Help for pregnant teenagers
Supporting Expectant, Pregnant, and Parenting Youth in Foster Care
Expectant, pregnant, and parenting youth often face challenges balancing their school, work, and home lives with being a new parent. Young parents in foster care are at increased risk for dropping out of school, unemployment, poverty, mental health issues, and child care concerns. Ensuring that adolescent parents receive adequate social, emotional, medical, and academic support is essential to the parent's and the baby’s future. Child welfare caseworkers and others working with pregnant and parenting youth should provide guidance that is strength-based, consistent, and unbiased while presenting options for services and supports. On this page, find guidance on working with expectant and parenting youth in out-of-home care and ways to support them and their families.
- State and local examples
Addressing the Needs of Pregnant and Parenting Youth in Foster Care: A Primer on Interagency Collaboration for Children’s Bureau Grantees
Capacity Building Center for States (2019)
Explains the services offered to pregnant and parenting youth in out-of-home care by the John H. Chafee Foster Care Program for Successful Transition to Adulthood and the Adolescent Pregnancy and Parenting Program. This tip sheet provides strategies for using both programs together to improve outcomes for pregnant and parenting youth in out-of-home care.
Challenges, Benefits Found in Providing Home Visiting Services for Pregnant and Parenting Foster Youth
Chapin Hall (2021)
Presents the results of a study that shows adolescent parents in foster care needing additional support, and one way to provide this support is through community-based home visiting programs. Outcomes from these interventions show positive effects in the areas of parent-child attachment, child and maternal health and development, parenting skills, and social support.
Connecting the Dots: A Resource Guide for Meeting the Needs of Expectant and Parenting Youth, Their Children, and Their Families
Center for the Study of Social Policy (2019)
Offers information on interventions and services for expectant and parenting youth involved with the child welfare system to help improve parent and child well-being outcomes.
Expectant and Parenting Youth in Foster Care: Systems Leaders Data Tool Kit
Annie E. Casey Foundation (2019)
Explains how child welfare leaders can better support expectant, pregnant, and parenting youth in foster care and offers recommendations for improving policies around working with this population.
Family First Prevention Services Act: Pregnant & Parenting Youth FAQs
Center for the Study of Social Policy (2018)
Provides answers to frequently asked questions related to the Family First Prevention Services Act and the law’s impact on pregnant and parenting youth in foster care.
Having a Healthy Pregnancy
Nemours Children’s Health (2017)
Presents information on prenatal care, what to expect during a pregnancy, things to avoid, and how to have a healthy pregnancy overall.
Leveraging the Family First Prevention Services Act for Older Youth: Prevention Provisions
American Bar Association (2019)
Explains provisions of the Family First Prevention Services Act that will impact older youth, including the use of title IV-E funds to provide services to youth in foster care who are pregnant or parenting.
Promising Practices That Support Pregnant and Parenting Youth [Webinar]
Capacity Building Center for States (2017)
Reviews promising practices in services for expectant, pregnant, and parenting youth involved with child welfare and discusses evidence-based programs along with home visiting services.
Support and Resources for Expectant and Parenting Young People in Foster Care
Family Voices United (2021)
Shares responses from youth with foster care experience about supports needed for expectant and parenting youth in care or transitioning out of care. Mental health, peer connections, access to resources, support networks, and more are discussed.
What Are Some Strategies for Supporting Pregnant and Parenting Teens in Foster Care?
Casey Family Programs (2018)
Examines challenges faced by child welfare agencies that are working with pregnant and parenting teens in foster care and discusses effective programs for this population that aim to ensure the healthy development of the teen parent and the child.
WIC PreScreening Tool: Special Supplemental Nutrition Program for Women, Infants and Children (WIC)
United States Department of Agriculture Food and Nutrition Service
Presents a tool that caseworkers and others working with pregnant and parenting youth in foster care can use to assess whether youth are eligible to receive WIC benefits. Most young people may not be aware of this resource, so this is something an adult should help with. The tool takes approximately 15 minutes to complete.
(Back to Top)
Help Pregnant Teens Know Their Options: AAP Policy Explained
By: Elise D. Berlan, MD, MPH, FAAP
Teenage pregnancy rates have been declining for decades, recently dropping to their lowest point in more than 70 years in the United States. Still, many girls in their teens or younger become pregnant each year. To help sort through the life-changing and emotional decisions they face, pregnant adolescents need prompt and straightforward information and judgment-free medical guidance, support and care.
In our policy statement, "Options Counseling for the Pregnant Adolescent Patient," the American Academy of Pediatrics (AAP) explains how to help teens get prompt medical care and basic, accurate information about all their options—while respecting everyone's personal, spiritual and cultural perspectives. These options usually include having and raising the baby, making plans for relatives or an adoptive family to raise the baby or terminating the pregnancy.
Federal and state policies may threaten to restrict health care providers from providing pregnant teens with unbiased counseling that includes the full range of pregnancy options. However, our approach to this issue has not changed since our original policy statement on the issue in 1989.
When children have children
Most teenagers who become pregnant decide to continue the pregnancy. Adolescents, especially younger ones, are more likely than women in their 20s to have medical complications during pregnancy. Their babies are also more likely to be born preterm, with low birth weight, and are less likely to survive. It's important to connect pregnant teens with early prenatal care and to encourage a healthy lifestyle—a well-balanced diet, daily exercise and staying away from tobacco, alcohol and drugs.
Their babies are also more likely to be born preterm, with low birth weight, and are less likely to survive. It's important to connect pregnant teens with early prenatal care and to encourage a healthy lifestyle—a well-balanced diet, daily exercise and staying away from tobacco, alcohol and drugs.
If the teen decides to have and raise the baby, they may need help identifying a strong support system. Teens and young girls who have babies can certainly achieve their personal life goals and raise healthy successful children, but often they will have more challenges to overcome. See "Helping Teen Parents and Their Children Build Healthy Futures."
Kinship care or foster care
In
kinship care arrangements, which have become increasingly common in recent years, a grandparent or other relative serves as a parent to the infant. This may be through an informal, private arrangement or through child welfare systems, which vary by state. Some adolescents may choose foster care for their baby when kinship care is unavailable or not suitable.
Kinship care arrangements can give a teen an opportunity to be involved with raising their child, as well as the chance to take on responsibilities of parenthood in the future. Growing evidence also suggests that babies in kinship care arrangements fare better than those cared for by unrelated foster parents. However, kinship care arrangements face unique challenges.
If you are considering raising your grandchild, here are some things to keep in mind:
Most children living with relatives are in informal arrangements, and this creates a problem if the relatives do not have the authority to give legal consent for needed medical care, including immunizations and other non-emergency health services. Your pediatrician can help connect you with community legal resources to help you take steps to gain legal authority to help children get the medical care they need to stay healthy.
Older family caregivers who haven't parented an infant for several years may not be aware of changes to safety standards for sleep, car seats and injury prevention.

Raising an infant the second time around can be a deeply rewarding and invigorating experience. However, it's a good idea for older caregivers to have a plan in place for guardianship in the event they experience health declines.
Adoption
Adoption is another option for teens who want to have their baby but don't feel ready or able to become a parent. About one to two million families are currently waiting to adopt, love and care for a baby in the United States.
The decision to place a baby with an adoptive family is legal and binding. However, most states do allow the birth mother anywhere from several days to several months after the child is born to change their mind. Information about adoption laws can be found on the Child Welfare Information Gateway, which is a service of the Children's Bureau in the U.S. Department of Health and Human Services.
If your teen is considering adoption, here are some basic things to know:
The adoption process can take place through public or private channels and be closed or open.
In public adoptions, the child is placed in a family by an agency operated or contracted by the state.
In private or independent adoptions, the birth parents may work with an attorney, physician, clergy member, or a licensed or unlicensed facilitator.
In closed adoptions, the names of the birth mother and the adoptive parents are kept secret from each other.
In open adoptions, the birth parent may choose to personally select the adoptive parents, meet with them, and even maintain contact and an ongoing relationship. Open adoptions, research shows, may lessen feelings such as grief or guilt some birth parents who make an adoption plan for their child may experience.
Abortion
Because some pregnant teens will consider abortion, the AAP believes they should be offered accurate information free of judgment. Because of the harms of restrictive abortion laws and the dangers of unsafe abortions, adolescents should have access to legal abortion services. The AAP respects the diversity of beliefs about abortion and encourages any teenager considering an abortion talk to a parent or trusted adult before making such a big decision.
The AAP respects the diversity of beliefs about abortion and encourages any teenager considering an abortion talk to a parent or trusted adult before making such a big decision.
Teens who feel safe and are willing to involve their parents in their abortion decision, as most are, usually benefit from adult experience, wisdom, emotional and financial support. Parental notification laws exist and vary from state to state. See Confidentiality for Teens Considering Abortion: AAP Policy Explained for more information.
If your teen is considering abortion:
Talk to your pediatrician about local laws affecting the availability of pregnancy termination options and where to find trained and licensed providers in your community or region. Medical and surgical abortions are safe when performed by licensed and experienced physicians.
Out-of-pocket costs for abortion services can be a barrier for pregnant teens and their families.
 Lack of money can cause delays, which can lead to more complicated procedures further along in the pregnancy. Sources of financial assistance may be available in your community or state.
Lack of money can cause delays, which can lead to more complicated procedures further along in the pregnancy. Sources of financial assistance may be available in your community or state.Use caution before speaking with a "pregnancy crisis center." Many of these offices have an agenda and may not offer accurate, non-judgmental counseling. For accurate information, it is best to talk with your pediatrician, or someone recommended by your provider.
Remember, pregnant teens need access to all options available to them—not judgment.
Finding out they're pregnant is a sensitive and emotional time for a teen, their family, and their sexual partner. Whatever their decision—to become a parent, make an adoption or kinship care plan, or have an abortion—it will likely have life-changing consequences. Creating an accepting environment for a pregnant teen allows them to feel safe to explore their own feelings about the pregnancy and their future.
More information
-
Contraception Explained: Options for Teens & Adolescents
- Guttmacher Institute
- National Abortion Federation Hotline
- Repro Legal Helpline
- Plan C
- The National Campaign to Prevent Teen Pregnancy
About Dr.
 Berlan
BerlanDr. Berlan is a member of the AAP Committee on Adolescence and lead author of the updated policy statements, Options Counseling for the Pregnant Adolescent Patient, and The Adolescent's Right to Confidential Care When Considering Abortion.
The information contained on this Web site should not be used as a substitute for the medical care and advice of your pediatrician. There may be variations in treatment that your pediatrician may recommend based on individual facts and circumstances.
Early adolescent pregnancy
01/29/2020
Early pregnancy is a medical, psychological and acute social problem of modern society. The age of such pregnancy varies from 10 to 18 years. The most common age for teen pregnancy is 15-17 years old. Why is this happening? How to prevent early pregnancy
Causes of early pregnancy
The problem of teenage pregnancy occurs, as a rule, for several reasons at the same time and it is rarely possible to fix one specific
- Sexual education of the child, or rather its absence.
 In today's adolescents, puberty begins at the age of 12, and their sexual desire also occurs earlier. It is very important to psychologically prepare the child for the upcoming changes in his intimate life, and continue to engage in sexual education until it is fully established. Often, parents do not have time to talk with the child on this topic, which can lead to unpleasant consequences such as infections or sexually transmitted diseases. Adolescents do not have sufficient information about sexuality.
In today's adolescents, puberty begins at the age of 12, and their sexual desire also occurs earlier. It is very important to psychologically prepare the child for the upcoming changes in his intimate life, and continue to engage in sexual education until it is fully established. Often, parents do not have time to talk with the child on this topic, which can lead to unpleasant consequences such as infections or sexually transmitted diseases. Adolescents do not have sufficient information about sexuality. - Sexual promiscuity. This factor is more common in the so-called "bad companies", where children gather who do not have any extracurricular useful hobbies or responsibilities. The teenager wants to prove to friends from the "bad company" that he is already an adult and more experienced than his peers. We must not miss the point that the implementation of such actions often occurs under the influence of alcohol or drugs. Psychologists say that more active and aggressive children are more likely to experience early pregnancy.

- Lack of knowledge about contraceptives or lack of funds to purchase them. Lack of knowledge about contraceptives, fear when buying, inability to use them or embarrassment when storing them at home also lead to such serious consequences. Parents are obliged to explain to their growing child what a condom is, what it is for, how to use it and where to buy it. If a teenager is embarrassed to buy a product in a pharmacy, parents can take care of this by buying the package themselves and inform their son or daughter about this.
- Violence. Frequently, violent sexual acts occur within dysfunctional families where the perpetrator is a male relative. The reason for withholding this information from relatives is fear and shame. But, unfortunately, no one is immune from street rape.
Talk to your daughter about how to avoid dark alleys and streets at night, try not to be alone on the street at night, take care of the attacker's protective equipment (for example, buy a gas canister for her).
- Planned pregnancy. Adolescents overwhelmed with feelings consciously conceive at 14-17 years of age. Thus, a teenage girl is trying to keep a young man, to prove to adults that she is already ready for an independent life, to show everyone her convictions that the age has come when she can become a mother. In this case, parents need to be more attentive to their children in love, talk in a timely manner about the fact that early pregnancy can cause complications in the health of the expectant mother or child, cause gynecological diseases and further infertility.
Psychological problems
Pregnancy in a teenage girl does not have the best effect on her psycho-emotional state. Having learned about pregnancy, which usually happens with a significant delay, young pregnant women first experience shock and guilt, get scared, lost and start to panic. It is almost impossible for a teenager with his still unformed and childish psyche to assess the situation and solve the problem on his own.
Some plunge into depression, while others hope for self-elimination of the problem - what if the pregnancy resolves or I just made a mistake. An important role in providing psychological assistance and support can be played by an adult with whom the minor has a trusting relationship. It can be a mother or grandmother, a school teacher or a psychologist, an older friend (neighbor, friend of the parents).
It is on how an adult behaves in this situation, having heard about the shocking news, the further behavior of the teenager, his decision on the outcome of the pregnancy, and in the case of gestation, the correct attitude towards his position and attitude to motherhood depend.
Trying to hide their situation, teenagers lead an asocial lifestyle to the last, possibly even before giving birth, smoke, use drugs and alcohol, hide their stomachs in every possible way with tight clothes, do not want to visit a doctor and follow his recommendations, which cannot but affect the health of the born child and young mother.
The psychological unpreparedness of the girl for motherhood either forces her to abandon the child while still in the hospital, or completely withdraw from his upbringing. Such a child is perceived by the young mother as a living reproach and grows up in the absence of love and affection.
Prevention of early pregnancy
The sexual education of a child depends only on the parents, their ability to find a common language with a teenager, the ability to listen and hear. Do not be shy to talk to your child about intimate life. It is necessary to come from afar and gradually expand the horizons of the child in this matter with films, books or presentations. Do not be shy to talk with a teenager about contraception and the consequences of sexual intercourse.
It is better to always try to maintain friendly relations with the child in order to be aware of changes in his personal life and, if necessary, help with wise advice or moral support. All sorts of jokes and ridicule will be inappropriate.
All sorts of jokes and ridicule will be inappropriate.
Pregnancy in a teenager is not a terrible sentence. The chances of a favorable outcome of early pregnancy are quite high. The main thing to remember is that during this period, a teenager needs the support of relatives and friends more than ever, and then a healthy and beloved baby will be born.
Return to list
Teenage pregnancy. What is Teen Pregnancy?
IMPORTANT
The information in this section should not be used for self-diagnosis or self-treatment. In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests. For diagnosis and proper treatment, you should contact your doctor.
Teenage pregnancy is the state of carrying a developing embryo and fetus by an underage teenage girl. Clinically manifested by the same signs as gestation in adults: the absence of regular menstruation, causeless nausea and vomiting, changes in taste habits, engorgement of the mammary glands, hyperpigmentation of the areola and nipples, weight gain, and an increase in abdominal circumference. When making a diagnosis, they use the data of a gynecological examination, the results of a pregnancy test and ultrasound of the uterus. When the patient decides to keep the child, management tactics are aimed at the timely detection and correction of complications, the choice of an appropriate method of delivery.
When making a diagnosis, they use the data of a gynecological examination, the results of a pregnancy test and ultrasound of the uterus. When the patient decides to keep the child, management tactics are aimed at the timely detection and correction of complications, the choice of an appropriate method of delivery.
- Causes of teenage pregnancy
- Pathogenesis
- Classification
- Symptoms of teenage pregnancy
- Complications
- Diagnostics
- Management of teenage pregnancy
- Prognosis and prevention
- Prices for treatment
General
Teenage pregnancy is not only a medical problem, but also a social one. In developed countries, its prevalence reaches 12 cases per 1,000 adolescents, in Russia this figure is 8-9times higher. According to WHO, about 16 million girls aged 15-19 years old give birth to children every year, which is up to 11% of all births in the world. 95% of such cases are detected in countries with low and middle incomes. The level of teenage pregnancy is largely influenced by national and religious traditions - in Islamic states it is much less common. According to statistics, up to 30% of pregnancies in girls end in artificial interruption, 14% in miscarriage, and 56% in childbirth. Two thirds of minors give birth out of wedlock. According to the social status, 72% of patients study at school, vocational schools or are housewives.
95% of such cases are detected in countries with low and middle incomes. The level of teenage pregnancy is largely influenced by national and religious traditions - in Islamic states it is much less common. According to statistics, up to 30% of pregnancies in girls end in artificial interruption, 14% in miscarriage, and 56% in childbirth. Two thirds of minors give birth out of wedlock. According to the social status, 72% of patients study at school, vocational schools or are housewives.
Teenage pregnancy
Causes of teenage pregnancy
Physiological opportunities for fertilization of the egg arise in the girl after the onset of the first menstruation (menarche). However, the real causes of early pregnancy are not related to the biological, but to the social aspect. The provocative factors differ in different countries and are largely determined by the level of economic development, the organization of education and medical care, local norms and traditions. According to experts in the field of obstetrics and gynecology, the onset of pregnancy in adolescence is facilitated by:
According to experts in the field of obstetrics and gynecology, the onset of pregnancy in adolescence is facilitated by:
- Insufficient sexual education and education. Adolescents are not always fully aware of the consequences of unprotected sex, the need and rules for contraception. This is due to the lack of targeted programs for the sexual education of schoolchildren, the sanctimonious attitude of adults, and examples of the asocial lifestyle that parents lead.
- Sexual emancipation. 9 out of 10 girls have their first sexual experience before the age of 20. This is facilitated by the availability of low-alcohol drinks, narcotic substances, and pornographic materials. Studies have shown that teens who watch TV shows and movies with sex scenes are at twice the risk of early pregnancy.
- Contraceptive prejudice. There is still a persistent stereotype in society that the use of male barrier contraceptives reduces the severity of pleasure and affects the romanticism of relationships.
 As a result, some girls and young women, in fear of losing their partners, are embarrassed to ask them for condom protection.
As a result, some girls and young women, in fear of losing their partners, are embarrassed to ask them for condom protection. - Sexual abuse. About 10% of pregnant adolescents under the age of 15 report the forced nature of their first sexual relationship. Often, coercion to have sex is caused by the girl's being in an unfavorable social environment, much less often it is an element of blackmail by a partner who threatens to end the romantic relationship.
- Poor socio-economic situation. This reason is one of the most significant for low-income countries. For some adolescents, the financial allowance at the birth of a child and social assistance provided until they reach a certain age become a significant argument in favor of early motherhood, and sometimes the only source of income.
Some of these reasons are relevant for poor countries with high unemployment, inaccessibility of educational and medical services, and low incomes. However, the increase in the frequency of early pregnancy in developed countries indicates the shortcomings of the implemented state policy and the lack of targeted efforts aimed at solving this problem.
Pathogenesis
Although, in general, the development of teenage pregnancy is based on the same mechanisms as normal, it has a number of features that affect the course of the gestational period and childbirth. First of all, these features are associated with the functional immaturity of the genital organs and endocrine regulation systems. In adolescence, complications of pregnancy are more often noted, and the likelihood of traumatism in childbirth increases. The onset of gestation in a teenager leads to an acceleration of the processes of puberty and somatic maturation - the size of the bone pelvis increases to typical for 16-18-year-old girls, which, combined with sufficient hydrophilicity and elasticity of the ligamentous apparatus, makes the bone ring more pliable.
Classification
In order to predict the development and choose the optimal tactics for supporting teenage pregnancy, it is advisable to systematize, taking into account a number of medical, physiological and social factors. Such a classification allows you to identify the risks of the gestational period in advance, prevent possible complications and determine the optimal delivery option. The main criteria for systematizing teenage pregnancy are:
Such a classification allows you to identify the risks of the gestational period in advance, prevent possible complications and determine the optimal delivery option. The main criteria for systematizing teenage pregnancy are:
- Menstrual age (MW). Taking into account the time of onset of menarche, groups of pregnant adolescents with a menstrual age of up to 1 year, 2 years, 3 years and more are distinguished. The lower the MV, the more likely the pathological course of pregnancy, childbirth and the postpartum period.
- Age of the pregnant woman. Girls under 9 years of age with accelerated sexual development are called "super-young primiparas", at the age of 9-15 years with incomplete puberty - "young primiparas", at 15-18 years old - adolescents ready for the implementation of childbearing function.
- State of health. Depending on the presence of concomitant pathology, there are categories of completely healthy pregnant adolescents, young pregnant women suffering from extragenital diseases, and adolescent girls with complications of the gestational period.
- Circumstances of pregnancy. There are primiparous girls with a desired pregnancy from prosperous and complete families, young pregnant women with an unwanted pregnancy from dysfunctional and single-parent families, adolescents who become pregnant due to rape.
Symptoms of teenage pregnancy
The key sign of onset gestation is the absence of another menstruation, although girls with an irregular monthly cycle may underestimate the significance of this symptom. A possible pregnancy is evidenced by the appearance of unreasonable nausea and vomiting, a change in taste and food preferences, breast engorgement, soreness in the nipple-areolar zone. As the uterus grows, the urge to urinate becomes more frequent, weight gain and an increase in the circumference of the abdomen are observed. Adolescent pregnancies are characterized by sudden mood swings with emotional lability, tearfulness, and tantrums. Often girls complain of unusual drowsiness, general weakness and fatigue.
Complications
Pregnancy and childbirth put an increased burden on the immature teenage body. In addition, in recent years there has been a significant deterioration in the somatic and reproductive health of girls - up to 75-86% of adolescents suffer from chronic somatic diseases, from 10 to 15% have genital pathology that affects fertility. As a result, teenage pregnancy often has a complicated course. Underage pregnant women are three times more likely to suffer from treatment-resistant anemia. Every second girl has preeclampsia, which manifests on average 12-14 days earlier, mostly has a moderate or severe course. Due to the presence of concomitant genital infections in the adolescent age group, the likelihood of developing an ectopic pregnancy increases.
Fetoplacental insufficiency with hypoxia, antenatal distress and fetal growth retardation is more often formed in pregnant girls of menstrual age 1-2 years. Insufficient secretion of steroids by the fetoplacental system leads to anomalies in the birth forces. With a teenage pregnancy, the risk of spontaneous abortions and premature births increases. Hypoglobulinemia and insufficient reserve potential of phagocytes provoke immune failure, which is manifested by an increase in infectious and inflammatory processes at the gestational and postpartum stages.
With a teenage pregnancy, the risk of spontaneous abortions and premature births increases. Hypoglobulinemia and insufficient reserve potential of phagocytes provoke immune failure, which is manifested by an increase in infectious and inflammatory processes at the gestational and postpartum stages.
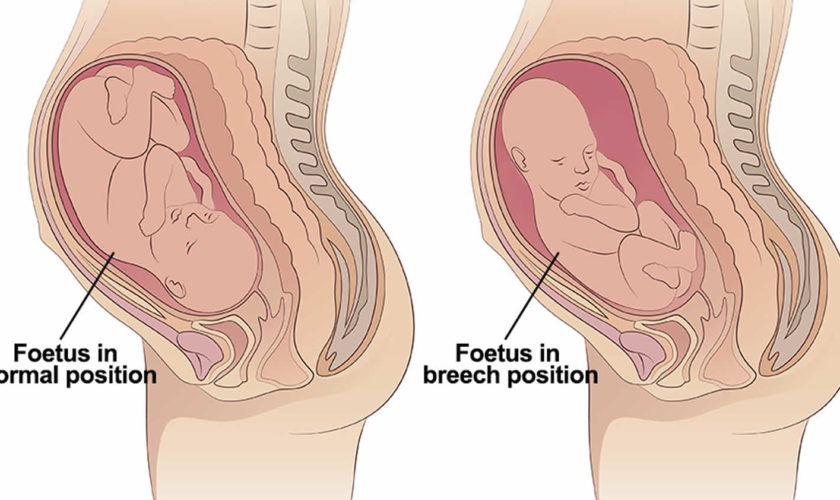
The course of childbirth directly depends on the menstrual age of the minor. With CF up to 1-2 years, anatomical or functional narrowing of the pelvis is observed in 50-66% of primiparas, breech presentation occurs more often, childbirth is complicated by spastic irregular contractions in the preliminary period, violent labor, primary weakness of the labor force, traumatization of soft tissues, hypotonic postpartum hemorrhage arising from pathological attachment of the placenta. Girls with 3-year-old CF often give birth quickly or rapidly, they have signs of primary weakness or incoordination of labor, there are ruptures of the birth canal, especially the perineum and cervix. After childbirth, postpartum endometritis, subinvolution of the uterus, hypogalactia and agalactia are detected twice as often in juvenile women in labor.
After childbirth, postpartum endometritis, subinvolution of the uterus, hypogalactia and agalactia are detected twice as often in juvenile women in labor.
Diagnostics
A feature of teenage pregnancy is its late diagnosis, due to the fact that up to 35-55% of girls do not suspect that they are carrying a child, or hide it. Often, adolescents turn to an obstetrician-gynecologist only at a later date, and 8-11% of underage pregnant women are not registered at all. The "gold" standard for diagnosing the condition is based on identifying the same presumptive, probable and reliable signs as in the adult reproductive group. To finally confirm pregnancy in a girl with a delay in menstruation, they carry out:
- Chair examination. With bimanual palpation, an increase in the uterus to the probable gestational age, softening of its isthmus, and increased mobility of the cervix are determined. Examination in the mirrors allows you to identify possible signs of a genital infection (inflammation of the vaginal mucosa, discharge from the cervical canal).

- Pregnancy test. Laboratory diagnostics is based on the determination of chorionic gonadotropin in the urine, a specific hormone that begins to be secreted from the time of implantation of a fertilized egg in the uterus. Modern inkjet tests are highly sensitive, and their reliability reaches 99%.
- Ultrasound of the uterus. Sonographic examination is the most popular and affordable method that reliably confirms the fact of pregnancy in a teenager. With the help of ultrasound in the uterine cavity, the fetus, placenta, membranes are detected. Regular screening allows you to dynamically monitor gestation, and fetometry - to assess the development of the fetus.
To exclude a possible infectious and inflammatory pathology of the genital organs, microscopy of a smear from the vagina, bacteriological seeding on nutrient media, TORCH-complex, RIF, ELISA, PCR diagnostics are performed. Subsequently, CTG is recommended for early detection of signs of fetoplacental insufficiency. Differential diagnosis is carried out with neoplasms of the abdominal cavity and small pelvis, malformations of the uterus, hypothalamic-pituitary disorders, primary ovarian insufficiency, metabolic and endocrine disorders in diabetes mellitus, hypofunction and hyperfunction of the thyroid gland, and other diseases accompanied by amenorrhea. According to the indications, the patient is consulted by an adolescent pediatrician, an endocrinologist, an infectious disease specialist, a dermatologist, a neuropathologist, a neurosurgeon, a psychologist, and a psychiatrist.
Differential diagnosis is carried out with neoplasms of the abdominal cavity and small pelvis, malformations of the uterus, hypothalamic-pituitary disorders, primary ovarian insufficiency, metabolic and endocrine disorders in diabetes mellitus, hypofunction and hyperfunction of the thyroid gland, and other diseases accompanied by amenorrhea. According to the indications, the patient is consulted by an adolescent pediatrician, an endocrinologist, an infectious disease specialist, a dermatologist, a neuropathologist, a neurosurgeon, a psychologist, and a psychiatrist.
Management of teenage pregnancy
After detecting gestation, a teenage girl, her relatives and employees of a medical institution need to decide on the advisability of bearing a child, patient management tactics and the optimal method of delivery. Possible options for solving the problem, taking into account all possible factors and the opinion of the pregnant woman, can be:
- Induced abortion.
 The girl and her relatives need to be explained that medical or surgical abortion performed at adolescence is more often complicated by traumatic injuries of the uterus, inflammation of the reproductive organs, and a violation of the ovarian cycle. In the future, such patients increase the likelihood of miscarriage and infertility. If a girl insists on terminating a pregnancy, it is important to intervene at an earlier date.
The girl and her relatives need to be explained that medical or surgical abortion performed at adolescence is more often complicated by traumatic injuries of the uterus, inflammation of the reproductive organs, and a violation of the ovarian cycle. In the future, such patients increase the likelihood of miscarriage and infertility. If a girl insists on terminating a pregnancy, it is important to intervene at an earlier date. - Pregnancy with natural delivery. The management of young primiparas does not differ significantly from standard protocols and involves the timely correction of emerging complications. In more than 90% of cases, a teenage girl is able to give birth to a child on her own. Even with an anatomically narrow pelvis, a clinical discrepancy between the size of the fetal head and the mother's pelvis is observed in only 10% of patients, which is associated with the frequent onset of preterm birth.
- Pregnancy and caesarean section. The decision to operate in each case is made individually, and the young age of the patient should not be taken as an obstacle to timely surgical intervention.
 Indications for operative delivery in adolescent women in labor are the same as in adult women. A caesarean section is performed when anomalies of labor activity that are resistant to conservative therapy, a clinically narrow pelvis, and signs of intranatal fetal hypoxia are detected.
Indications for operative delivery in adolescent women in labor are the same as in adult women. A caesarean section is performed when anomalies of labor activity that are resistant to conservative therapy, a clinically narrow pelvis, and signs of intranatal fetal hypoxia are detected.
When managing a girl carrying a child, an obstetrician-gynecologist pays attention to both the medical aspects of pregnancy and the correction of the patient's lifestyle. Since the adolescent age group often eat irregular and unbalanced meals, the importance of rational diet and food intake is being educated. Particular attention is paid to the discussion of smoking, alcohol and drug use, prevention of sexually transmitted infections, psychoprophylactic preparation for the upcoming birth. Given the increased risk of complications in childbirth, pregnant adolescents are shown hospitalization in highly qualified obstetric hospitals for 37-39week of gestational age.
Prognosis and prevention
The prognosis with proper management of teenage pregnancy and the choice of the optimal method of delivery is favorable.