Child birth process
What happens to your body during childbirth
Childbirth is challenging and complications occur, but women's bodies are designed to give birth. The shape of the pelvis, hormones, powerful muscles and more all work together to help you bring your baby into the world - before, during and after childbirth.
How your body prepares for labour
Here are some of the ways your body will prepare both you and your baby for the birth ahead.
Braxton Hicks contractions
In the weeks or days before you start having proper contractions, you may experience Braxton Hicks contractions. This is your uterus tightening then relaxing. These contractions don't usually hurt and are thought to help your uterus and cervix get ready for labour.
Braxton Hicks contractions may become more regular as you get closer to the time of birth, but unlike labour contractions, they don't change the shape of the cervix and are sometimes referred to as 'false labour'. Your midwife can tell you if you're experiencing Braxton Hicks contractions or if you are in labour by doing a vaginal examination to look at your cervix.
Changes to the cervix
As labour gets closer, your cervix softens and becomes thinner, getting ready for the dilation (widening) that will allow the baby to enter the vagina. You may also see a 'show', which is a pinkish plug of mucus, stained with blood.
Engagement
Your baby may move further down your pelvis as the head engages, or sits in place over your cervix, ready for the birth. Some women feel they have more room to breathe after the baby has moved down. This is called 'lightening'.
Rupture of the membranes, or 'waters breaking'
Some women find the sac of amniotic fluid containing the baby breaks before labour, contractions start and the fluid runs (or gushes) out of the vagina. This is referred to as rupture of the membranes, or 'waters breaking'.
Let your maternity team know when your waters have broken and take notice of the colour of the fluid. It is usually light yellow. If it is green or red, tell your maternity team since this could mean the baby is having problems.
If your waters have broken but you have not started having regular contractions within 24 hours, you may need your labour to be induced because there is a risk of infection. Your midwife or doctor will talk to you about this.
How will you know when labour has started?
Movies often show women suddenly being struck by painful contractions and rushing to hospital. In real life, many women are not sure if they have actually started their labour.
You may feel restless, have back pain or period-like pain, or stomach disturbances such as diarrhoea.
Labour officially begins with contractions, which start working to open up the cervix. You should phone your midwife when your contractions start, although you probably won't be encouraged to come to the hospital or birthing centre until your contractions are closer together.
In preparation for labour, your baby may move further down your pelvis as the head engages, or sits in place over your cervix.How the pelvis is designed for childbirth
Your pelvis is located between your hip bones. Women typically have wider, flatter pelvises than men, as well as a wider pelvic cavity (hole) to allow a baby to pass through.
Women typically have wider, flatter pelvises than men, as well as a wider pelvic cavity (hole) to allow a baby to pass through.
The organs sitting in a woman's pelvis include the uterus, cervix and vagina, which are held together by a group of muscles. During childbirth, the muscles at the top of your uterus press down on the baby's bottom. Your baby's head then presses on your cervix which, along with the release of the hormone oxytocin (see 'How hormones help you give birth', below), brings on contractions. Your cervix should dilate so your baby can pass through it.
Your pelvis has bones and ligaments that move or stretch as the baby travels into the vagina. Your baby also has spaces between the skull bones called 'sutures', and the gaps where the sutures meet on the skull are called fontanelles. This allows for the baby's head to mould as the skull bones meet or overlap, allowing it to fit more easily as it travels through your pelvis.
How hormones help you give birth
Your body produces hormones that trigger changes in your body before, during and after childbirth. Here's how they work to help you deliver your baby.
Here's how they work to help you deliver your baby.
- Prostaglandin Before childbirth, a higher level of prostaglandin will help open the cervix and make your body more receptive to another important hormone, oxytocin.
- Oxytocin This hormone causes contractions during labour, as well as the contractions that deliver the placenta after the baby is born. These post-birth contractions, including more that can occur during breastfeeding, help your uterus shrink back to its normal size. Oxytocin and prolactin are the two main hormones that produce and let down breast milk for your baby. Skin-to-skin contact between a mother and baby helps to release more of these hormones.
- Relaxin The hormone relaxin helps soften and stretch the cervix for birth, while helping your waters break and stretching the ligaments in your pelvis to allow the baby to come through.
- Beta-endorphins During childbirth, this type of endorphin helps with pain relief and can cause you to feel joyful or euphoric.

- 'Baby blues' After birth, your hormone balance can change again, and this is believed to cause the ‘baby blues’ in some women. You may feel teary, anxious and irritable and your mood can go up and down.
When childbirth doesn’t go to plan
Sometimes, complications can occur before or during childbirth that mean things don’t go as expected.
Sometimes, labour needs to be induced or started. There are a few ways to induce labour, including the mother being offered synthetic prostaglandin. This is inserted into the vagina to soften the cervix and start contractions.
If contractions slow down or stop during labour, the mother may be offered synthetic oxytocin from a drip to increase the contractions. In both these cases contractions can come on strongly and more pain relief may be needed. Your maternity team should explain the benefits and risks of this with you before you agree to it.
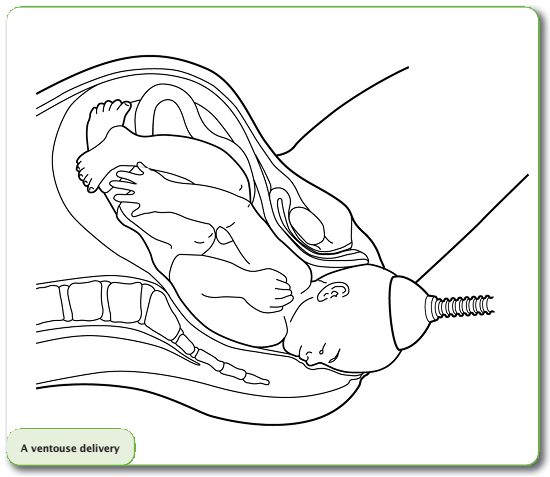
The baby could be in a posterior or breech position, not ideally placed above the cervix before the birth. Your maternity team may need to use forceps or a vacuum to help turn the baby or help the baby travel out of the vagina. Sometimes a caesarean is needed.
Your maternity team may need to use forceps or a vacuum to help turn the baby or help the baby travel out of the vagina. Sometimes a caesarean is needed.
In rare cases, a mother may experience cephalopelvic disproportion (CPD), which is when the baby’s head is too big to fit through the pelvis. A diagnosis of CPD is usually made when labour hasn’t progressed and synthetic oxytocin has not helped. A caesarean is usually the next step.
More information
If you have any questions about childbirth or pregnancy, you can call Pregnancy, Birth and Baby on 1800 882 436, 7 days a week, to speak to a maternal health nurse.
Learn more here about the development and quality assurance of healthdirect content.
Childbirth | Stages of Labor | Effacement
On this page
Basics
- Summary
- Start Here
- Diagnosis and Tests
- Treatments and Therapies
Learn More
- Related Issues
- Specifics
See, Play and Learn
- Images
- Videos and Tutorials
Research
- Statistics and Research
- Clinical Trials
- Journal Articles
Resources
- Find an Expert
For You
- Patient Handouts
When you are ready to have your baby, you'll go through labor. Labor is the process of giving birth. Signs that you might be going into labor include:
Labor is the process of giving birth. Signs that you might be going into labor include:
- Contractions that are regular then start to come closer together
- Leaking fluid or bleeding from the vagina
- Low, dull backache
- Abdominal cramps
Call your health care provider if you have any of these signs, even if it is before your due date. Preterm labor can start before 37 completed weeks of pregnancy.
Labor happens in three stages. The first stage begins with contractions. It continues until your cervix has become thinner and dilated (stretched) to about 4 inches wide. The second stage is the active stage, in which you begin to push downward. Crowning is when your baby's scalp comes into view. Shortly afterward, your baby is born. In the third stage, you deliver the placenta. The placenta is the organ that supplied food and oxygen to your baby during pregnancy.
Mothers and babies are monitored closely during labor. Most women are able to have a baby through normal vaginal delivery. If there are complications, the baby may need to be delivered surgically by a Cesarean section.
If there are complications, the baby may need to be delivered surgically by a Cesarean section.
NIH: National Institute of Child Health and Human Development
- Labor and Birth (Department of Health and Human Services, Office on Women's Health) Also in Spanish
- Stages of Labor (March of Dimes Birth Defects Foundation) Also in Spanish
- What Is Labor? (Eunice Kennedy Shriver National Institute of Child Health and Human Development) Also in Spanish
- Contractions and Signs of Labor (March of Dimes Birth Defects Foundation)
- Cord Blood Testing and Banking (National Library of Medicine) Also in Spanish
- Monitoring Baby's Heart Rate During Labor (American Academy of Family Physicians) Also in Spanish
- Water Breaking: Understand This Sign of Labor (Mayo Foundation for Medical Education and Research) Also in Spanish
- Dealing with Pain during Childbirth (Nemours Foundation) Also in Spanish
- Apgar Scores (American Academy of Pediatrics) Also in Spanish
- Birthing Centers and Hospital Maternity Services (Nemours Foundation) Also in Spanish
- Birthing Classes (American Academy of Family Physicians) Also in Spanish
- Elective Deliveries Before 39 Weeks: Is It Worth It? (American Academy of Pediatrics)
- Assisted Vaginal Delivery (American College of Obstetricians and Gynecologists)
- Cesarean Section: MedlinePlus Health Topic (National Library of Medicine) Also in Spanish
- Episiotomy: When It's Needed, When It's Not (Mayo Foundation for Medical Education and Research) Also in Spanish
- Induction of Labor at 39 Weeks (American College of Obstetricians and Gynecologists)
- Labor Pain (American Society of Anesthesiologists)
- Natural Childbirth (Nemours Foundation) Also in Spanish
- At Least 39 Weeks (March of Dimes Birth Defects Foundation)
- FastStats: Births -- Method of Delivery (National Center for Health Statistics)
- PeriStats: Perinatal Statistics (March of Dimes Birth Defects Foundation)
- ClinicalTrials.
 gov: Delivery, Obstetric (National Institutes of Health)
gov: Delivery, Obstetric (National Institutes of Health) - ClinicalTrials.gov: Labor, Obstetric (National Institutes of Health)
- Article: Evaluation efficacy and safety of epidural analgesia in second-trimester induced labor:.
 ..
.. - Article: Digital fetal scalp stimulation (dFSS) versus fetal blood sampling (FBS) to...
- Article: Maternal and perinatal effects with the use of floral therapy in.
 ..
.. - Childbirth -- see more articles
- Department of Health and Human Services, Office on Women's Health Also in Spanish
- Find an Ob-Gyn (American College of Obstetricians and Gynecologists)
The process of childbirth
This event must be approached with self-confidence, one's strengths, capabilities and reliability of information received about childbirth during pregnancy. Tuning in the right way and doing everything right, knowledge helps. It is incomparably easier for pregnant women who have a good idea of all the stages of the birth process and are psychologically prepared for the upcoming event than for those expectant mothers who are poorly aware of what will happen to them.
Tuning in the right way and doing everything right, knowledge helps. It is incomparably easier for pregnant women who have a good idea of all the stages of the birth process and are psychologically prepared for the upcoming event than for those expectant mothers who are poorly aware of what will happen to them.
Childbirth is divided into three periods:
- Disclosure period . As a result of regular contractions (involuntary contraction of the muscles of the uterus), the cervix opens.
- The period of expulsion of the fetus from the uterine cavity. Attempts are added to the contractions - arbitrary (that is, controlled by the woman in labor) contractions of the abdominal muscles. The baby moves through the birth canal and is born.
- Follow-up period . The placenta and membranes are born.
First stage of labor
The fact that labor has already begun or is about to begin is indicated by the appearance of regular contractions and / or the outflow of amniotic fluid. Contractions are involuntary periodic contractions of the muscles of the uterus, aimed at shortening and opening the cervix. Normally, the length of the cervix is 3-5 cm, and the diameter is only a few millimeters. And for the birth of a child, it is necessary that the cervix completely shorten and open up to 9-10 cm.
Contractions are involuntary periodic contractions of the muscles of the uterus, aimed at shortening and opening the cervix. Normally, the length of the cervix is 3-5 cm, and the diameter is only a few millimeters. And for the birth of a child, it is necessary that the cervix completely shorten and open up to 9-10 cm.
The period of dilation is the longest in the process of childbirth. In the natural course of childbirth, this period lasts 10-11 hours for primiparas, 6-7 hours for multiparous ones.
At the beginning of this period there are regular contractions that last 15-20 seconds with an interval of about 15 minutes. As the cervix dilates, the contractions intensify, become longer, and the intervals between them shorten. When the break between contractions is 10 minutes, you need to go to the maternity hospital.
During the opening period, it is recommended to walk, move, breathe properly, take a warm shower or bath. These measures contribute to a faster opening of the cervix, while reducing pain. You can ask your husband or midwife to massage the lumbar region - this will reduce the discomfort from contractions.
You can ask your husband or midwife to massage the lumbar region - this will reduce the discomfort from contractions.
Second stage of labor
Most women agree that the end of the dilation phase, before the onset of the second stage of labor, is the most difficult. Contractions become frequent and painful, anesthesia by this moment usually ceases to act, fatigue accumulates, it is still impossible to push. The state of many women at this moment is described by one single phrase: “That's it! I can not anymore!". The only consolation is that it doesn't last long.
After the cervix is fully dilated, the doctor allows the mother to push. A woman usually herself feels strong urges to "push" the child out of the birth canal. These urges are called pushes.
In order for pushing to be effective, you need to push properly and breathe properly. Before pushing, you need to get more air into the lungs, hold your breath and try to push effectively. It is important not to strain your face and legs during attempts, but on the contrary - to relax as much as possible. Between attempts, you also need to relax and rest.
Between attempts, you also need to relax and rest.
The second stage of labor lasts from 15 minutes to two hours, and in multiparous this stage is shorter than in primiparas. During this period, doctors especially carefully monitor the condition of the mother and fetus (they regularly listen to heartbeats, etc.).
Meanwhile, the baby is moving along the genital tract. At the height of one of the attempts from the genital slit, the lower pole of the head (or buttocks - in breech presentation) is shown, after the end of the attempt, the head is hidden in the genital slit. This process - cutting the head - continues for some time. At a certain moment, the pole of the head remains in the genital gap and in between attempts. Under the influence of continuing attempts, the eruption of the head begins, which continues until its full birth. There is very little left. A few more attempts - and the whole child is born.
The newborn is placed on the mother's belly (ideally) and they get to know each other for a while, resting after the birth. The midwife or doctor then cuts the umbilical cord and takes the baby away for proper treatment, bathing, weighing and examination by a pediatrician.
The midwife or doctor then cuts the umbilical cord and takes the baby away for proper treatment, bathing, weighing and examination by a pediatrician.
10-15 minutes after the birth of the baby can be applied to the breast. This promotes uterine contraction and milk production.
Third stage of labor
The last stage of labor - the birth of the placenta - is the shortest. Usually, the afterbirth is born 10-20 minutes after the birth of the baby. Mom might need to push a little for this.
If the placenta does not separate for more than 30 minutes, doctors diagnose the retention of the placenta in the uterus and begin to take emergency measures.
The delivered placenta is carefully examined for its integrity. If everything is fine, that is, the placenta has separated completely, the woman is sewn up with tears or incisions (if any). After that, a heating pad with ice is placed on her stomach and observed for some time in the delivery room (1.5-2 hours).
This is where the birth process ends and a new life begins for mother and baby.
References
- Florian S., Ichou M., Panico L. Parental migrant status and health inequalities at birth: The role of immigrant educational selectivity. // Soc Sci Med - 2021 - Vol278 - NNULL - p.113915; PMID:33905985
- Naja S., Al Kubaisi N., Singh R., Abdalla H., Bougmiza I. Screening for antenatal depression and its determinants among pregnant women in Qatar: revisiting the biopsychosocial model. // BMC Pregnancy Childbirth - 2021 - Vol21 - N1 - p.330; PMID:33902481
- Shchepin VO., Khabriev RU. [The characteristics of population mortality of the Russian Federation, the Central Federal Okrug and City of Moscow in 2020]. // Probl Sotsialnoi Gig Zdravookhranenniiai Istor Med - 2021 - Vol29 - N2 - p.189-193; PMID:332
- Saavedra LPJ., Prates KV., Gonçalves GD., Piovan S., Matafome P., Mathias PCF. COVID-19 During Development: A Matter of Concern.
 // Front Cell Dev Biol - 2021 - Vol9 - NNULL - p.659032; PMID:33898461
// Front Cell Dev Biol - 2021 - Vol9 - NNULL - p.659032; PMID:33898461 - Caparros-Gonzalez RA., Romero-Gonzalez B., Puertas-Gonzalez JA., Quirós-Fernandez S., Coca-Guzman B., Peralta-Ramirez MI. [Midwives and psychologists as professionals to screen and prevent pregnancy-specific stress.] // Rev Esp Salud Publica - 2021 - Vol95 - NNULL - p.; PMID:33896933
- Burakowska K., Gorka P., Penner GB. Effects of canola meal inclusion rate in starter mixtures for Holstein heifer calves on dry matter intake, average daily gain, ruminal fermentation, plasma metabolites, and total-tract digestibility. // J Dairy Sci - 2021 - Vol - NNULL - p.; PMID:33896627
- Toker E., Aktaş S. The childbirth experiences of Syrian refugee mothers living in Turkey: a qualitative study. // J Reprod Infant Psychol - 2021 - Vol - NNULL - p.1-17; PMID:33896296
- Mérillet L., Pavoine S., Kopp D., Robert M., Mouchet M. Biomass of slow life history species increases as local bottom trawl effort decreases in the Celtic sea.
 // J Environ Manage - 2021 - Vol290 - NNULL - p.112634; PMID:33895454
// J Environ Manage - 2021 - Vol290 - NNULL - p.112634; PMID:33895454 - Patskun E., Yevtushok L., Zymak-Zakutnia N., Lapchenko S., Akhmedzhanova D., Wertelecki W. A teratology information system in vernacular: Closing an information gap. // Birth Defects Res - 2021 - Vol - NNULL - p.; PMID:33893758
- Fu A., Liu C. Is Pregnancy Following a TRAM or DIEP Flap Safe? A Critical Systematic Review and Meta-analysis. // Aesthetic Plast Surg - 2021 - Vol - NNULL - p.; PMID:33893518
Important to know - St. Petersburg citizen's health
The total duration of childbirth and its course
The total duration of childbirth depends on many factors: age, physique and physical condition of the woman, her psychological mood, the speed of cervical dilatation, first pregnancy or repeated , the size of the child, the type of presentation and a number of other points.
Labor activity proceeds differently for all women, but the main periods of childbirth are clearly distinguished: 1st period - the period of contractions, the longest and most intense, 2nd period - the direct birth of a baby, 3rd period - the birth of the afterbirth (placenta).
First stage of labor (opening period)
As the name implies, during this period there is a gradual opening of the cervix as a result of regular contractions of the uterine muscles. Contractions occur with a decreasing interval, while they themselves become longer and more frequent.
The dilation period is the time elapsed from the onset of regular contractions to the full dilation of the cervix. During this period, the birth canal is prepared for the passage of the fetus through them with all the fetal formations.
Cervical dilatation occurs gradually: at first the cervix is smoothed out, then the pharynx opens up to 3-4 cm and at the end of the first stage of labor up to 10 cm. This is already a complete dilatation of the cervix. With it, during contractions, the fetal bladder becomes tense and bursts at the height of one of them, the anterior portion of amniotic fluid is poured out.
The first stage of labor is the longest and consists of three phases:
1. Latent phase (lasts 5-6 hours). It is characterized by the establishment of regular contractions, with an interval between them of 10-15 minutes. Latent, or hidden, this phase is called because the contractions of the uterus during it are painless or slightly painful. By the end of the phase, the cervix is completely flattened and opens about 4 cm.
Latent phase (lasts 5-6 hours). It is characterized by the establishment of regular contractions, with an interval between them of 10-15 minutes. Latent, or hidden, this phase is called because the contractions of the uterus during it are painless or slightly painful. By the end of the phase, the cervix is completely flattened and opens about 4 cm.
2. Active phase (lasts 3-4 hours). Contractions become more intense, last at least 20 seconds, and the interval between them is reduced to 5-6 minutes. Normally, during the active phase, amniotic fluid is poured out, which contributes to a faster full disclosure of the uterine pharynx. By the end of the phase, the uterus opens by 8 cm.
3. Transitional (transient) phase, or deceleration phase (lasts from 40 minutes to 2 hours, may be absent in multiparas). This phase is not always clearly manifested, but it is nevertheless distinguished due to the usual weakening of contractions during disclosure from 8 to 10 cm. The child's head descends and stands in the narrow part of the small pelvis, which necessitates a slower and smoother process. Already in the transitional phase, the woman in labor feels the desire to push, to push the baby out. But in order for the head to pass through the birth canal without the risk of injury, it is necessary to achieve cervical dilatation up to 10 cm.
Already in the transitional phase, the woman in labor feels the desire to push, to push the baby out. But in order for the head to pass through the birth canal without the risk of injury, it is necessary to achieve cervical dilatation up to 10 cm.
Second stage of labor (exile period)
The period of exile is the time from the moment of full opening of the pharynx until the birth of the fetus.
It is the second stage of childbirth that is their culmination, because in a short time (compared to contractions) the long-awaited birth of the baby takes place.
After the discharge of the amniotic fluid, contractions temporarily stop. The volume of the uterine cavity decreases, the uterine cavity and vagina appear as a single birth canal. Contractions reappear and become more intense. They are joined by attempts - contractions of the muscle press (abdominal wall, diaphragm and pelvic floor). The frequency and intensity of contractions and attempts are constantly increasing. The head descends and compresses the nerves of the sacral plexus. A woman has a strong desire to squeeze the head out of the birth canal, she is looking for supports for her arms and legs to strengthen her efforts.
The head descends and compresses the nerves of the sacral plexus. A woman has a strong desire to squeeze the head out of the birth canal, she is looking for supports for her arms and legs to strengthen her efforts.
Pushing is a lot of physical work. During attempts, a woman experiences maximum physical stress (blood pressure rises, pulse and respiration become more frequent). During the attempts, the woman holds her breath, and in the intervals between them she rests and "gathers her strength for a new attempt."
During one of the attempts, the head is born. Next, the shoulders are born (first the front, then the back) and the torso. Following the fetus, the posterior amniotic fluid is poured out with an admixture of cheese-like lubricant.
A woman in labor, having experienced severe fatigue, rests after hard work (pulse and respiration rate decrease).
Third stage of labor (postpartum period).
The afterbirth period is the time from the birth of the fetus to the birth of the placenta. During this period, the placenta separates from the walls of the uterus and the birth of the placenta (placenta with membranes and umbilical cord).
During this period, the placenta separates from the walls of the uterus and the birth of the placenta (placenta with membranes and umbilical cord).
In the process of separation of the placenta from the walls of the uterus, uteroplacental vessels are damaged, which is normally accompanied by blood loss in the amount of 100-200 ml, without adversely affecting the woman's condition. After the birth of the placenta, the uterus contracts sharply, becomes dense, which is necessary to stop bleeding in the area of the placental site; its bottom is in the middle between the womb and the navel.
During this period, the woman's pulse and respiration normalize. Her demeanor is calm. Chills can sometimes be observed (as a reaction to the transferred strong physical stress).
The third period is no longer as exciting and tense as the previous two. The child was born and the matter remains for the small - the separation of the placenta, or placenta. Nature provides for the resumption of contractions a few minutes after the birth of the baby, necessary for effective exfoliation from the uterus of tissues that nourished the fetus during pregnancy (placenta, membranes, umbilical cord).