Where is the baby held during pregnancy
Anatomy of pregnancy and birth - uterus
Anatomy of pregnancy and birth - uterus | Pregnancy Birth and Baby beginning of content5-minute read
Listen
What does the uterus look like?
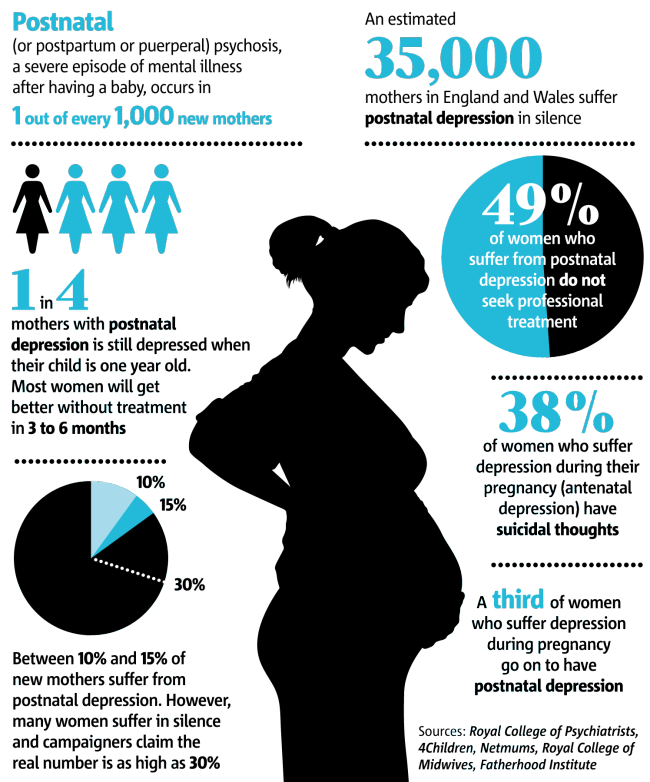
One of the most recognised changes in a pregnant woman’s body is the appearance of the ‘baby bump’, which forms to accommodate the baby growing in the uterus. The primary function of the uterus during pregnancy is to house and nurture your growing baby, so it is important to understand its structure and function, and what changes you can expect the uterus to undergo during pregnancy.
The uterus (also known as the ‘womb’) has a thick muscular wall and is pear shaped. It is made up of the fundus (at the top of the uterus), the main body (called the corpus), and the cervix (the lower part of the uterus ). Ligaments – which are tough, flexible tissue – hold it in position in the middle of the pelvis, behind the bladder, and in front of the rectum.
The uterus wall is made up of 3 layers. The inside is a thin layer called the endometrium, which responds to hormones – the shedding of this layer causes menstrual bleeding. The middle layer is a muscular wall. The outside layer of the uterus is a thin layer of cells.
Illustration showing the female reproductive system.The size of a non-pregnant woman's uterus can vary. In a woman who has never been pregnant, the average length of the uterus is about 7 centimetres. This increases in size to approximately 9 centimetres in a woman who is not pregnant but has been pregnant before. The size and shape of the uterus can change with the number of pregnancies and with age.
How does the uterus change during pregnancy?
During pregnancy, as the baby grows, the size of a woman’s uterus will dramatically increase. One measure to estimate growth is the fundal height, the distance from the pubic bone to the top of the uterus. Your doctor (GP) or obstetrician or midwife will measure your fundal height at each antenatal visit from 24 weeks onwards. If there are concerns about your baby’s growth, your doctor or midwife may recommend using regular ultrasound to monitor the baby.
Your doctor (GP) or obstetrician or midwife will measure your fundal height at each antenatal visit from 24 weeks onwards. If there are concerns about your baby’s growth, your doctor or midwife may recommend using regular ultrasound to monitor the baby.
Fundal height can vary from person to person, and many factors can affect the size of a pregnant woman’s uterus. For instance, the fundal height may be different in women who are carrying more than one baby, who are overweight or obese, or who have certain medical conditions. A full bladder will also affect fundal height measurement, so it’s important to empty your bladder before each measurement. A smaller than expected fundal height could be a sign that the baby is growing slowly or that there is too little amniotic fluid. If so, this will be monitored carefully by your doctor. In contrast, a larger than expected fundal height could mean that the baby is larger than average and this may also need monitoring.
As the uterus grows, it can put pressure on the other organs of the pregnant woman's body. For instance, the uterus can press on the nearby bladder, increasing the need to urinate.
For instance, the uterus can press on the nearby bladder, increasing the need to urinate.
How does the uterus prepare for labour and birth?
Braxton Hicks contractions, also known as 'false labour' or 'practice contractions', prepare your uterus for the birth and may start as early as mid-way through your pregnancy, and continuing right through to the birth. Braxton Hicks contractions tend to be irregular and while they are not generally painful, they can be uncomfortable and get progressively stronger through the pregnancy.
During true labour, the muscles of the uterus contract to help your baby move down into the birth canal. Labour contractions start like a wave and build in intensity, moving from the top of the uterus right down to the cervix. Your uterus will feel tight during the contraction, but between contractions, the pain will ease off and allow you to rest before the next one builds. Unlike Braxton Hicks, labour contractions become stronger, more regular and more frequent in the lead up to the birth.
How does the uterus change after birth?
After the baby is born, the uterus will contract again to allow the placenta, which feeds the baby during pregnancy, to leave the woman’s body. This is sometimes called the ‘after birth’. These contractions are milder than the contractions felt during labour. Once the placenta is delivered, the uterus remains contracted to help prevent heavy bleeding known as ‘postpartum haemorrhage‘.
The uterus will also continue to have contractions after the birth is completed, particularly during breastfeeding. This contracting and tightening of the uterus will feel a little like period cramps and is also known as 'afterbirth pains'.
Read more here about the first few days after giving birth.
Sources:
The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Labour and birth), StatPearls Publishing (Anatomy, Abdomen and Pelvis), Department of Health (Clinical practice guidelines: Pregnancy care), Better Health Channel Victoria (Pregnancy stages and changes), Mater Mother's Hospital (Labour and birth information), Royal Australian and New Zealand College of Obstetricians and Gynaecologists (The First Few Weeks Following Birth), Queensland Health (Queensland Clinical Guidelines – maternity and neonatal), King Edward Memorial Hospital (Fundal height: Measuring with a tape measure), Royal Hospital for Women (Fetal growth assessment (clinical) in pregnancy), MSD Manual (Female internal genital organs)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: October 2020
Back To Top
Related pages
- Anatomy of pregnancy and birth - perineum and pelvic floor
- Anatomy of pregnancy and birth - pelvis
- Anatomy of pregnancy and birth - cervix
- Anatomy of pregnancy and birth - abdominal muscles
- Anatomy of pregnancy and birth
Need more information?
Prolapsed uterus - Better Health Channel
The pelvic floor and associated supporting ligaments can be weakened or damaged in many ways, causing uterine prolapse.
Read more on Better Health Channel website
Uterus, cervix & ovaries - fact sheet | Jean Hailes
This fact sheet discusses some of the health conditions that may affect a woman's uterus, cervix and ovaries.
Read more on Jean Hailes for Women's Health website
Dilatation and curettage (D&C)
A D&C is an operation to lightly scrape the inside of the uterus (womb).
Read more on WA Health website
Ectopic pregnancy
An ectopic pregnancy occurs when a fertilised egg implants outside the uterus (womb)
Read more on WA Health website
Placental abruption - Better Health Channel
Placental abruption means the placenta has detached from the wall of the uterus, starving the baby of oxygen and nutrients.
Read more on Better Health Channel website
Placenta previa - Better Health Channel
Placenta previa means the placenta has implanted at the bottom of the uterus, over the cervix or close by.
Read more on Better Health Channel website
Pelvic Floor | Family Planning NSW
The pelvic floor is a group of muscles in the pelvic area that support the bladder, bowel and uterus (womb).
Read more on Family Planning NSW website
Mirena IUD | Hormonal IUD Mirena | IUD Mirena insertion | IUD Mirena cost | Mirena IUD Melbourne - Sexual Health Victoria
The hormonal intrauterine device (IUD) is a small contraceptive device that is put into the uterus (womb) to prevent pregnancy.
Read more on Sexual Health Victoria website
Contraception - intrauterine devices (IUD) - Better Health Channel
An intrauterine device (IUD) is a small contraceptive device that is put into the uterus (womb) to prevent pregnancy.
Read more on Better Health Channel website
Endometriosis | Your Fertility
Endometriosis is a condition where the tissue that lines the uterus also grows in other areas of the body
Read more on Your Fertility website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Anatomy of pregnancy and birth - cervix
Anatomy of pregnancy and birth - cervix | Pregnancy Birth and Baby beginning of content5-minute read
Listen
Where is the cervix?
The cervix plays a critical role throughout a woman’s life, but never more so than during conception, pregnancy and childbirth. The cervix changes during these events, so it’s important to understand the role of this organ and what these changes mean for you and your baby.
The cervix changes during these events, so it’s important to understand the role of this organ and what these changes mean for you and your baby.
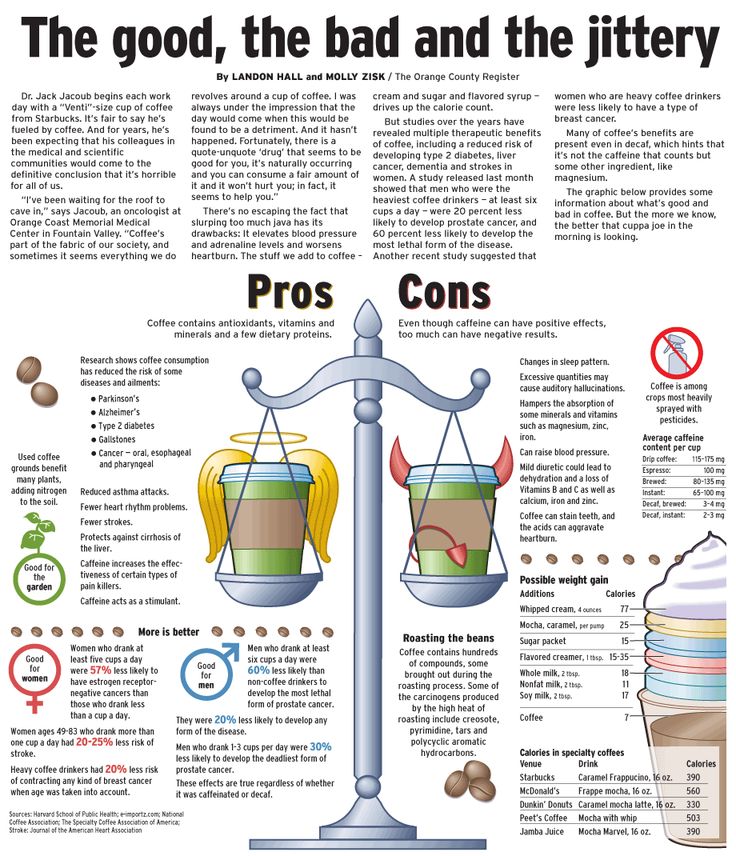
The cervix is the muscular channel or opening that runs between the uterus (also known as the womb) and the vagina. The cervix is located in the pelvis and lies behind the bladder and near the front of the rectum. It is held in its position by tough, flexible ligaments.
Illustration showing the female reproductive system.What does the cervix do in women who are not pregnant?
In women who are not pregnant, the cervix is narrow and firm. Its size, shape and lining undergo subtle changes throughout a woman’s menstrual cycle.
For instance, the cervix has a smooth covering of mucus. When a woman is ovulating, the mucus becomes stretchy and elastic, which helps sperm move and survive following intercourse, and is known as ‘fertile mucus’. When a woman is not ovulating, the mucus takes on a more creamy texture and can be milky or yellow in colour. This change in consistency indicates that sperm are less likely to reach the uterus after intercourse at this time in the menstrual cycle.
This change in consistency indicates that sperm are less likely to reach the uterus after intercourse at this time in the menstrual cycle.
The cervix contains a channel, referred to as the 'cervical canal', which also has an important role in women who are not pregnant. Sperm enters the uterus after intercourse and menstrual blood leaves the uterus during menstruation through this channel.
What is the function of the cervix during conception and pregnancy?
The cervix has several important functions during conception. After a woman conceives, the mucus on the surface of the cervix becomes sticky and thick. This stops new sperm and microorganisms, such as bacteria and viruses, from entering the uterus and potentially harming the fetus.
The cervix also plays a crucial role during pregnancy. From conception until just before birth, the cervix protects the growing baby by increasing in size and strength, helping to keep the baby safe and secure in the uterus.
How does the cervix change during labour?
The cervix undergoes dramatic changes during labour in a process known as ‘effacement’ or ‘ripening’.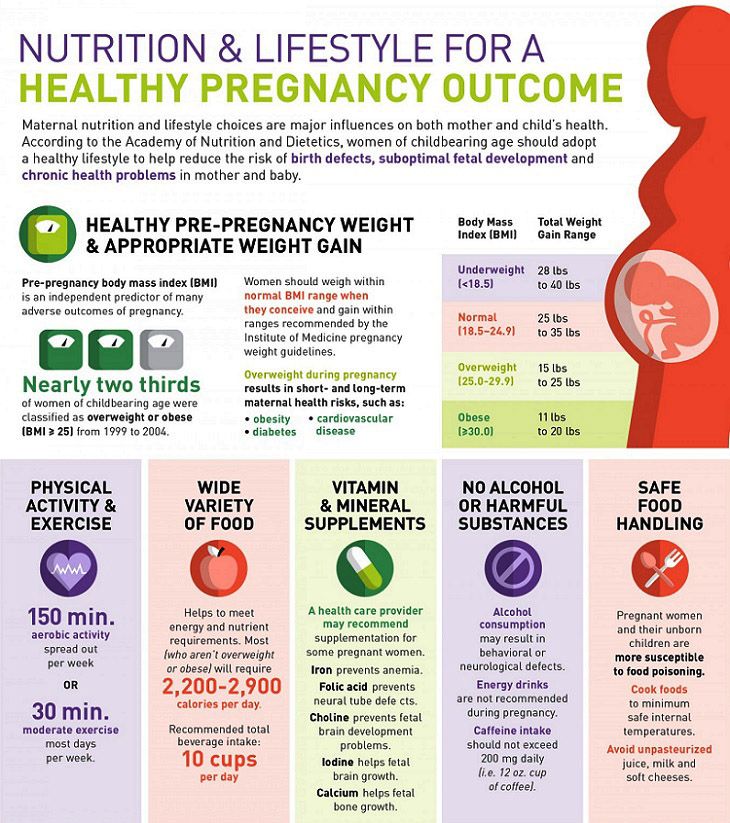 It starts out long and firm, and as labour progresses, it softens, widens and becomes more elastic.
It starts out long and firm, and as labour progresses, it softens, widens and becomes more elastic.
Changes to the cervix are partly triggered by contractions of the muscles of the uterus, which help open the cervix. As the cervix begins to open, you may see a clear, pink, or slightly bloody discharge (sometimes referred to as the 'show'). This is the release of the mucus plug, that sits over the cervical canal during pregnancy.
The first stage of labour begins when you feel contractions — your cervix will start to soften and to open. The time it takes for the cervix to open (or dilate) will vary from woman to woman and can range from several hours to days or even weeks. Once the cervix is dilated more than 3cm, and contractions are strong and regular, labour is said to be ‘established’.
Established labour is also known as the 'active phase'. This phase continues until the cervix dilates to approximately 7cm, with the contractions being strong, painful and around every 3 or 4 minutes.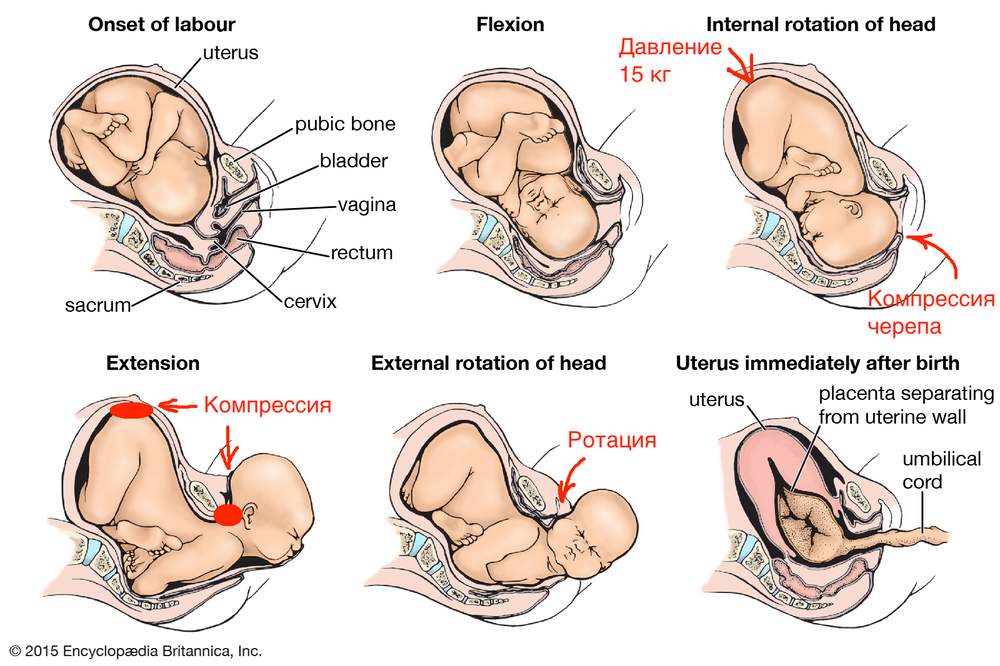
This is followed by the ‘transition phase’, when the cervix continues to fully open. There is now less time to rest in between contractions.
First stage of labour is complete when the cervix is fully open (referred to as 'fully dilated'), the baby moves through the pelvis and the mother can begin pushing the baby out. Being fully dilated might not actually be a 10cm opening of the cervix. Rather it is when the doctor or midwife cannot feel any cervix when they perform a vaginal examination.
The second stage of labour is when your baby is being born and the third stage is when the placenta is delivered.
What problems can occur with the cervix during pregnancy, labour, or birth?
The cervix is monitored throughout pregnancy, labour and birth to identify any problems. For instance, if the cervix is weak, it might be difficult to keep the baby in the uterus for the whole pregnancy. This can lead to premature labour and birth.
During labour, contractions might not be regular or strong enough to fully open the cervix, which slows labour down. In these situations, the doctor or midwife might intervene by breaking the mother's waters or using a hormone to increase contractions and speed up the dilation of the cervix.
In these situations, the doctor or midwife might intervene by breaking the mother's waters or using a hormone to increase contractions and speed up the dilation of the cervix.
It is important that the mother does not begin pushing the baby out until the cervix is fully dilated. This is because pushing too soon might swell the cervix, which can slow down the birth.
Read more here about complications in labour, and how they are managed.
Sources:
MSD Manual (Female internal genital organs), Translational Research in Anatomy (March 2016) (The structure and function of the cervix during pregnancy), Women's Health (Understanding your menstrual cycle fact sheet), Mater Mother's Hospital (Labour and birth information), The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Labour and birth), Royal Women's (Stages of labour), King Edward Memorial Hospital (Second stage of labour and birth), SA Health (Induction of labour techniques), Queensland Health (Vaginal examinations in labour)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: October 2020
Back To Top
Related pages
- Anatomy of pregnancy and birth - uterus
- Anatomy of pregnancy and birth - perineum and pelvic floor
- Anatomy of pregnancy and birth - pelvis
- Anatomy of pregnancy and birth - abdominal muscles
- Anatomy of pregnancy and birth
Need more information?
Uterus, cervix & ovaries - fact sheet | Jean Hailes
This fact sheet discusses some of the health conditions that may affect a woman's uterus, cervix and ovaries.
Read more on Jean Hailes for Women's Health website
Placenta previa - Better Health Channel
Placenta previa means the placenta has implanted at the bottom of the uterus, over the cervix or close by.
Read more on Better Health Channel website
Diaphragm - how effective is the diaphragm - Sexual Health Victoria
A diaphragm is a shallow, cup-shape made of silicone inserted inside the cervix. In Australia there is one size diaphragm available sold as Caya®.
Read more on Sexual Health Victoria website
Pap smear tests - MyDr.com.au
Pap smear tests are currently used in Australia as a screening test for cervical cancer. A Pap smear test can detect changes in the cells of the cervix that may develop into cancer.
Read more on myDr website
Labour & birth: what to expect | Raising Children Network
Early labour signs include a show, waters breaking and pain. During labour, your contractions increase and your cervix dilates, so you can birth your baby.
Read more on raisingchildren.net.au website
Induction of labour
Inducing labour allows women to deliver their baby normally by stimulating labour contractions. There are several medical and surgical techniques which can be used.
Read more on Parenthub website
What happens to your body in childbirth
During childbirth, your body's hormones, ligaments and muscles, as well as the shape of your pelvis, all work together to bring your baby safely into the world.
Read more on Pregnancy, Birth & Baby website
Dilatation and curettage (D&C) - Better Health Channel
A dilatation and curettage (D&C) is an operation performed on women to lightly scrape away the womb lining.
Read more on Better Health Channel website
Asherman Syndrome
Read more on RANZCOG - Royal Australian and New Zealand College of Obstetricians and Gynaecologists website
Cervical Screening | Pap Smear | Jean Hailes
All you need to know about cervical screening tests and how they differ from pap smears. Learn why and when you should have one and how they work.
Read more on Jean Hailes for Women's Health website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Life before birth – Dixion Medical Center in Orel
The author of the article is
Olga Mikhailovna Khoreva,
psychologist of the clinic "Dixion"
In modern society, we no longer treat pregnant women with such trepidation, but at the same time we still know little about the life of a person in the womb of a mother. We have little idea what it feels like to happen. Perinatal psychology reveals these mysteries.
This kind of psychology appeared not so long ago, about forty years ago. This science studies the mental life of a baby in the womb or a newborn, his connection with his mother, the influence of her psychological state on him.
Many scientists claim that the fetus has a long-term memory and mental life.
The perinatal period has a great influence on the future of a person. It turns out that what happened to him in the womb, as well as during and after childbirth, is stored in his subconscious. In the future, these events affect how a person will become, how he will behave in certain situations.
The events of the perinatal period can be divided into three stages: pregnancy, childbirth and the postpartum period.
Stage 1: Pregnancy
At this time, a person's life potential is formed, the ability to adapt to various conditions. Dear mothers, learn to love your baby in the tummy, even if his appearance was not a very pleasant surprise for you!
According to scientists, the basic physical and mental potential of the desired child is much higher. Otherwise, children do not sleep well, are easily upset, and cannot calm down for a long time. Often they are physically weaker than desired children.
The baby in the mother's belly is very sensitive to her mood. He hears, sees, tastes and touches. The child "sees the world" through the eyes of the mother, perceives it through her emotions. Therefore, pregnant women are asked to avoid stress, not to worry.
The child succeeds in all this with the help of hormones that come to the child through the placenta, and with the help of the mother's electromagnetic field. Scientists believe that mother and child communicate by means of millimeter-wave electromagnetic waves.
It is possible that some of the information is transmitted to the child through the aquatic environment of the mother's body. But the baby still in the womb can show independence. From about the tenth week, the fetus feels touch, that is, it has a sense of touch. From the eighteenth week - begins to distinguish the taste and drink amniotic fluid.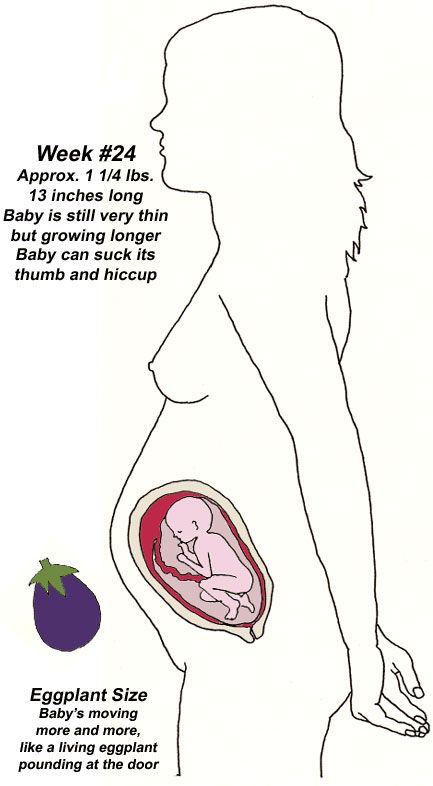 At this time, you need to carefully monitor your menu - you can teach your child to eat "not right."
At this time, you need to carefully monitor your menu - you can teach your child to eat "not right."
Hearing develops around the 22nd week, but children do not hear external noise well. They are disturbed by the sound of the work of the internal organs of the mother. But they hear their mother perfectly. So we recommend expectant mothers to sing songs, read aloud and just talk to your baby.
This is best done when the baby is awake. This time is easy to determine. Usually during this period the child is actively moving. It will be great if every day during this period you communicate with him like this: touch your tummy and say something, for example: “Hello, baby.” Over time, the conversations will become longer, and the child will respond to touches by pushing. It is advisable to involve older children and dad in this game. Just keep in mind that each family member should have a “own” part of the tummy for touching and their own “sound code”. In this way, the baby's sense of touch and hearing are developed, and it also has a positive effect on the emotional development of the child.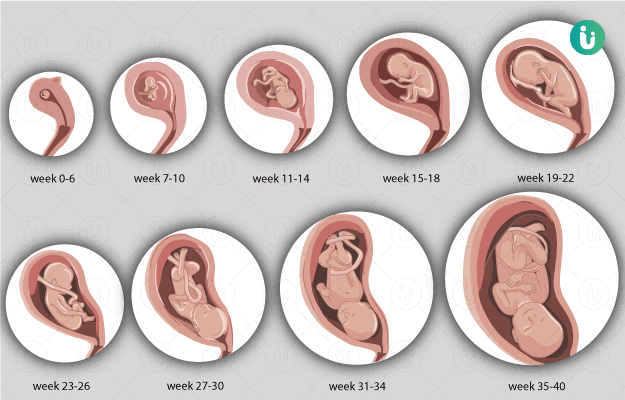
By the twenty-fourth week, the child's pupils are able to react to light. Some scientists believe that complete darkness reigns in the womb, others that the red part of the spectrum enters the uterus. The baby will learn to distinguish smells only when he is born - being in the womb, he will trust the mother's sense of smell.
Stage 2: Birth
Who will be the child in the "big" life - will he be a "winner" or "victim", how will he fight for a place under the sun - this is determined during this perinatal period.
Scientists believe that natural childbirth has the best effect on the future of the baby. Stimulation of childbirth has a negative impact on the mother and child - it breaks their interaction, speeds up the process against their will, so it is worth resorting to it only for medical reasons. Despite the fact that with a planned caesarean section, everything happens painlessly for the baby, many scientists believe that in this case your child will not become a fighter, and they do not recommend resorting to cesarean section unnecessarily.
If you want your child to be a fighter, behave properly when pushing, and then the mouse will become more assertive in the performance of the tasks assigned to him, act accordingly and perceive various situations objectively.
Breathing will help to behave properly during contractions and efforts, and it will also help reduce pain. You can learn how to breathe correctly during childbirth on your own or in courses for pregnant women. During childbirth, listen carefully to what the midwife says and try to follow her advice.
Husband, mother or other close person can provide great support and assistance during childbirth. The so-called joint births have a number of advantages: during contractions, the mother will not be alone with pain, there will be a loved one nearby who can distract her, support and help in this difficult situation; besides this close person is easier to perceive than a stranger, so the words of the midwife, repeated by the husband, will reach your consciousness faster.
Stage 3: Postpartum
According to scientists, at this perinatal stage, a person's attitude to freedom, their capabilities and strengths is formed. Therefore, during natural childbirth, the child is immediately placed on the mother's stomach. He sees his mother, feels her warmth, that is, he feels protected. Immediately after birth, the baby looks at his mother's face - he seems to get to know her again. This process of "gazing" is called bonding.
Psychologists say that during this process a stable emotional bond is formed between mother and child. If the father, whom the baby had only heard before, is next to the newborn and the mother, it will be just great - he will also be involved in the bonding process. It will be great if dad takes the baby in his arms, hugs him, talks to him. The presence of the father is especially important in the case of a caesarean section. While the doctors are "conjuring" over the mother, the baby will be in the hands of the father.
If it happens that a child cannot be with his mother for a long time after giving birth, then in life independence may become a burden for him. But with good care, breastfeeding for up to a year, tenderness and love, this state of affairs can be corrected.
Breastfeeding is a very important moment that affects both the emotional and physical development of the child.
The composition of breast milk is individual and ideal for just one baby. This composition changes during the day and days of a newborn's life.
Emotions are the thread that connects mother and child - they still form a single whole, but in the psycho-emotional, and not in the physical plane. The newborn is very sensitive to the mood of the mother. If the mother is upset, then the baby also behaves restlessly.
An important factor influencing the emotional development of a child is the attentive, sensitive attitude of his parents both to him and to each other. You need to spend as much time as possible together, smile, hold the child in your arms more often.
It has been proven that the baby develops faster if he has a lot of contact with his parents from birth. Of great importance are touches at every change of clothes, bathing, carrying on hands, feeding, massage.
It may be that some of the hypotheses of perinatal psychology seem dubious. But this science makes you think that inside a pregnant woman is not just a fetus, but a developing personality.
A baby inside the womb is not a physiological thing, it is a person who has his own mental life, and his future largely depends on the woman, on how she behaved during pregnancy, childbirth and the first hours after them.
By using our website, you agree to our use of cookies
How to hold your baby correctly
Bagdasaryan Kristina Genrihovna
Obstetrician-gynecologist, Ultrasound doctor
Clinic "Mother and Child" St. Petersburg
So, how to take the child from the supine position. Grasp his chest with both hands - thumbs in front, and the rest hold the back. If the baby is not yet able to hold his head, support it with your index fingers. Gently lift your baby up. Do not forget, your face turned to the child should always express the kindest feelings. Talk to the baby, tell him what you are doing, the voice should not be very loud, gentle.
Grasp his chest with both hands - thumbs in front, and the rest hold the back. If the baby is not yet able to hold his head, support it with your index fingers. Gently lift your baby up. Do not forget, your face turned to the child should always express the kindest feelings. Talk to the baby, tell him what you are doing, the voice should not be very loud, gentle.
Those who take a small child in their arms are divided into two categories: relatives who live with him under the same roof, and visitors. You should not allow a visitor to the child who has not taken off his outerwear, hat, street shoes, has not washed his hands with soap, has not freed his hands from rings, rings, watches, bracelets. The baby can be frightened by sharp extraneous odors, for example, the smell of tobacco, alcohol, perfume.
Sick people should not be allowed near the child - coughing, sneezing, as well as complaining of indigestion, suffering from skin diseases.
Even if loving relatives have come a long way on trains and planes to visit the baby, be persistent and keep the guests “in quarantine” for several days - will the infection picked up on the road show up? They may be offended, but the child will remain healthy! In order to more reliably protect the psyche and immune system of the child, it is useful in his first six months of life to limit the circle of people admitted to him. These are the rules, and no one - neither the formidable mother-in-law, nor the neighbor, nor the beloved boss - deserves an exception.
These are the rules, and no one - neither the formidable mother-in-law, nor the neighbor, nor the beloved boss - deserves an exception.
Some parents take the baby in their arms with unthinkable precautions, others, on the contrary, snatch it from the crib so famously. All these are extremes. So how should it be?
- do not make sudden movements when holding the baby
- never take it with one hand - only with both
- do not raise or lower the baby quickly, rapidly
- do not take him out of the crib by pulling on the handles
The position of the baby in the arms of the mother (or another adult), first of all, depends on his age, as well as on whether he will sleep or be awake. Up to 2-2.5 months (and sometimes longer), the baby’s head must be supported, so in a horizontal position (face up), arrange the baby on your arm so that the back of his head lies on your elbow, the back rests on your forearm, and your hands should support the buttocks and hips of the baby. You can put the baby on your forearm and stomach. In this case, the baby's head should be in the crook of the elbow, and your hands will close on the baby's stomach, and one hand will pass between the legs of the little one. If you want to hold the child in an upright position, for example, in order for him to burp excess air, then support his head and back: put one of your palms on the back of the baby’s head, with your forearm firmly press his body to you. With the other hand, fix the buttocks of the crumbs. In no case do not sit the child on your arm until he has confidently mastered the skill of sitting, which happens on average at the age of 6 months. From 2.5-3 months, you can already carry the baby, turning him away from you, holding him with one hand at chest level, with the other at hip level.
You can put the baby on your forearm and stomach. In this case, the baby's head should be in the crook of the elbow, and your hands will close on the baby's stomach, and one hand will pass between the legs of the little one. If you want to hold the child in an upright position, for example, in order for him to burp excess air, then support his head and back: put one of your palms on the back of the baby’s head, with your forearm firmly press his body to you. With the other hand, fix the buttocks of the crumbs. In no case do not sit the child on your arm until he has confidently mastered the skill of sitting, which happens on average at the age of 6 months. From 2.5-3 months, you can already carry the baby, turning him away from you, holding him with one hand at chest level, with the other at hip level.
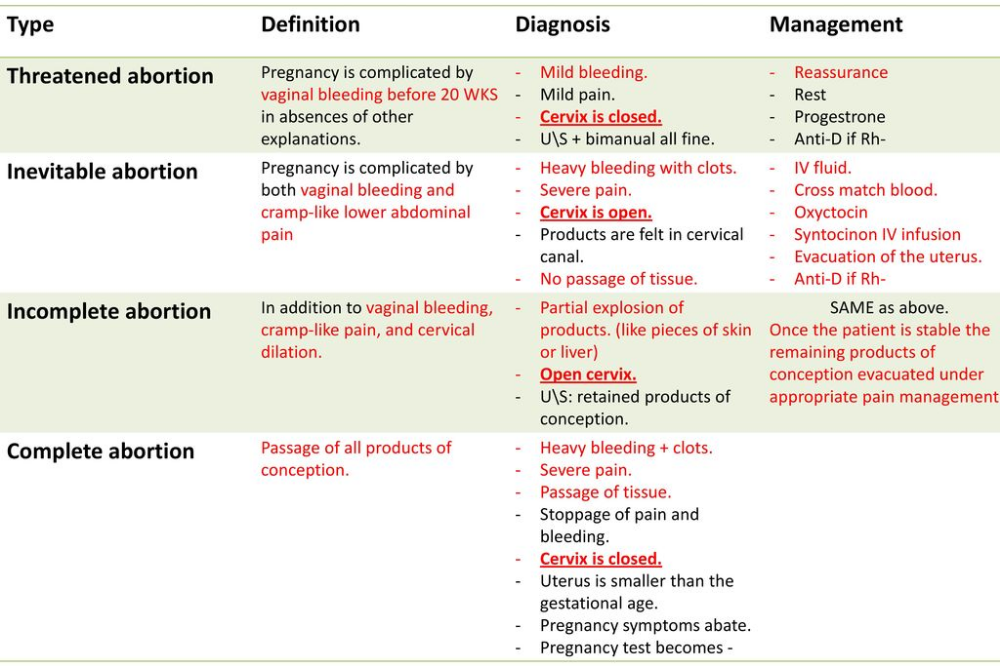
Depending on the age of the child, there are 6 ways to hold him in your arms.
Hanging. This method is good for babies up to 3 months old, when they still have trouble holding their head. With one hand support the neck and back of the baby's head, with the other - the buttocks, while his torso may be slightly bent, and his face turned towards you. This situation opens up scope for the much-needed emotional contact with the mother and other loved ones for a small child. Do not forget that in order to avoid the development of one-sidedness, the baby's head must be supported either with the left or with the right hand - periodically changing them.
With one hand support the neck and back of the baby's head, with the other - the buttocks, while his torso may be slightly bent, and his face turned towards you. This situation opens up scope for the much-needed emotional contact with the mother and other loved ones for a small child. Do not forget that in order to avoid the development of one-sidedness, the baby's head must be supported either with the left or with the right hand - periodically changing them.
On the arm. Ideal for babies aged 3-6 months, although you can keep your baby this way almost from birth. He rests his head on your shoulder, you hold his feet with your hand, and your arms with your forearm. With your other hand, you support the baby under the buttocks. At the same time, the child's legs should be bent at the knee and hip joints and bred. Don't forget to alternate hands.
In front of bust . Starting from 6 months, this way of holding the baby provides him with the same position as in the position on the back. The baby leans back against your chest, his legs are bent and divorced, the soles are in contact. Hold the baby's shins with your thumbs, the feet with the index, middle and ring fingers, and the buttocks with the little fingers. This position is useful for the development of the child: as well as on the back, he can play with his legs, improving movements, mastering his body and gaining an idea of \u200b\u200bspace.
The baby leans back against your chest, his legs are bent and divorced, the soles are in contact. Hold the baby's shins with your thumbs, the feet with the index, middle and ring fingers, and the buttocks with the little fingers. This position is useful for the development of the child: as well as on the back, he can play with his legs, improving movements, mastering his body and gaining an idea of \u200b\u200bspace.
In front of the stomach . In children from 7 months old, this method allows you to reproduce crawling in a plastunsky way - a motor skill that they just need to master at this age. With one hand, take the child under the chest, and pass the other between the legs, supporting the stomach. Don't forget to switch hands.
On the side. Suitable for babies from 10 months, when they are already sitting confidently. Take the child so that he wraps his legs around your side, and rests his back on your forearm. You should support the baby's knee with your hand, giving it a slightly bent position.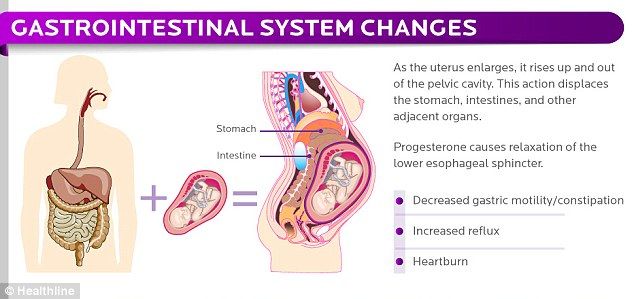 One arm of the child is on your chest, the other is free. Please note: you need to wear a child in this position alternately from one side to the other.
One arm of the child is on your chest, the other is free. Please note: you need to wear a child in this position alternately from one side to the other.
And, finally, a universal and completely international way to carry children of any age. Holding the palm of your right hand under the breast of the baby, firmly press his back to your chest. With your left hand, grasp the child's right thigh, bending his legs at the hip joints. Please note: the weight of a child under 6 months should not fall on your hand supporting the baby's pelvis - this is harmful to his spine and can ruin his posture in the future.
The baby grows, his body weight increases, and it becomes difficult to carry the baby in his arms for a long time (especially after 3 months of age, when the weight of the child reaches an average of 7 kg). Here, assistive devices for carrying children, such as a baby sling and a kangaroo backpack, can help out for a while. A baby sling is a modern modification of a piece of fabric that provides close physical contact between mother and child. In addition, with it, if necessary, it is easier to breastfeed a child while on the street or in another public place. You can use a baby sling from birth to a year and a half. It all depends on the weight of the baby and your physical capabilities. It is also very important to find the optimal position for the child and for the mother, which would provide both with maximum comfort. The basic positions of the baby in a baby sling are horizontal, with support for the spine, and (for older children) raised vertical or sitting, when the baby is tightly pulled by the fabric. A kangaroo backpack can be used only after the baby learns to hold his head confidently and his back muscles get stronger. Preference should be given to backpacks with a rigid back. But, nevertheless, you should not get too carried away with a baby sling and a kangaroo backpack. Firstly, it is still more useful for the baby to lie on the hard mattress of the crib or stroller. Secondly, it is unlikely that the child will like to sleep while sitting in a backpack.
In addition, with it, if necessary, it is easier to breastfeed a child while on the street or in another public place. You can use a baby sling from birth to a year and a half. It all depends on the weight of the baby and your physical capabilities. It is also very important to find the optimal position for the child and for the mother, which would provide both with maximum comfort. The basic positions of the baby in a baby sling are horizontal, with support for the spine, and (for older children) raised vertical or sitting, when the baby is tightly pulled by the fabric. A kangaroo backpack can be used only after the baby learns to hold his head confidently and his back muscles get stronger. Preference should be given to backpacks with a rigid back. But, nevertheless, you should not get too carried away with a baby sling and a kangaroo backpack. Firstly, it is still more useful for the baby to lie on the hard mattress of the crib or stroller. Secondly, it is unlikely that the child will like to sleep while sitting in a backpack. And, thirdly, a long stay of a child in the same position, which causes an uneven load on different parts of the spine, can provoke a pathology of the musculoskeletal system. Therefore, it is not recommended to keep the baby in a baby sling and "kangaroo" for more than 40 minutes a day. When the child grows up a little, you can practice the pose when the baby sits on his mother's side, facing her. The advantages of this position: the mother has one hand free, and the child has an excellent view. If the mother, for health reasons, is not recommended to take the baby in her arms, then you can often put him on her stomach, put him on her knees.
And, thirdly, a long stay of a child in the same position, which causes an uneven load on different parts of the spine, can provoke a pathology of the musculoskeletal system. Therefore, it is not recommended to keep the baby in a baby sling and "kangaroo" for more than 40 minutes a day. When the child grows up a little, you can practice the pose when the baby sits on his mother's side, facing her. The advantages of this position: the mother has one hand free, and the child has an excellent view. If the mother, for health reasons, is not recommended to take the baby in her arms, then you can often put him on her stomach, put him on her knees.
And, finally, many parents are concerned about the question, is it possible, often taking the baby in her arms, to spoil him? If the needs of the child are not ignored, they are not denied affection and tactile contact, then this does not mean at all that he is spoiled and poorly educated. Love is not a synonym for bad parenting, especially if we are talking about a baby who is only a few weeks or months old. There is an opinion that it is impossible to spoil a child up to 12 months - until this age, all his "whims" are justified by needs, so an adult should indulge the baby in everything. And only when the baby reaches the year, parents should selectively treat his requests - based on what they are caused by. From this age, it is already possible to instill in the baby the concept that not only he, but also the people around him have needs.
There is an opinion that it is impossible to spoil a child up to 12 months - until this age, all his "whims" are justified by needs, so an adult should indulge the baby in everything. And only when the baby reaches the year, parents should selectively treat his requests - based on what they are caused by. From this age, it is already possible to instill in the baby the concept that not only he, but also the people around him have needs.
Rigid parenting methods, according to which taking a child in your arms means pampering him, ignore the natural need of the baby for the constant presence of the mother (or the one who cares for him). While promoting the principle of early formation of "independence", they have significant negative features. Firstly, a child who is deliberately separated from his mother does not develop a trusting, kind attitude towards the world, and this will certainly have a negative impact in his adult life. Secondly, the restriction of bodily contact between mother and baby does not contribute to the emergence of mutual feelings between them. It is not surprising that the child in such cases is perceived as a hindrance to the usual way of life and ordinary affairs. And the baby constantly needs communication and his crying is a call to everyone, and first of all to his mother. Indeed, even in those cases when, it would seem, there are no reasons for tears, the baby may burst into offended or angry crying - because he is not yet ready for loneliness, his biological connection with his mother is still too strong. Thirdly, it should be borne in mind that a strict attitude towards a child, when adults try not to show their feelings and emotions in relation to a child, is not a guarantee of a good upbringing of a child and his further success. Most often, a young mother has a lot of chores around the house. Therefore, if she often takes the baby in her arms, she will have to sacrifice some things. In addition, carrying a child in her arms is also physically not very easy. In general, if desired, there are many reasons for minimizing physical contact with a child.
It is not surprising that the child in such cases is perceived as a hindrance to the usual way of life and ordinary affairs. And the baby constantly needs communication and his crying is a call to everyone, and first of all to his mother. Indeed, even in those cases when, it would seem, there are no reasons for tears, the baby may burst into offended or angry crying - because he is not yet ready for loneliness, his biological connection with his mother is still too strong. Thirdly, it should be borne in mind that a strict attitude towards a child, when adults try not to show their feelings and emotions in relation to a child, is not a guarantee of a good upbringing of a child and his further success. Most often, a young mother has a lot of chores around the house. Therefore, if she often takes the baby in her arms, she will have to sacrifice some things. In addition, carrying a child in her arms is also physically not very easy. In general, if desired, there are many reasons for minimizing physical contact with a child.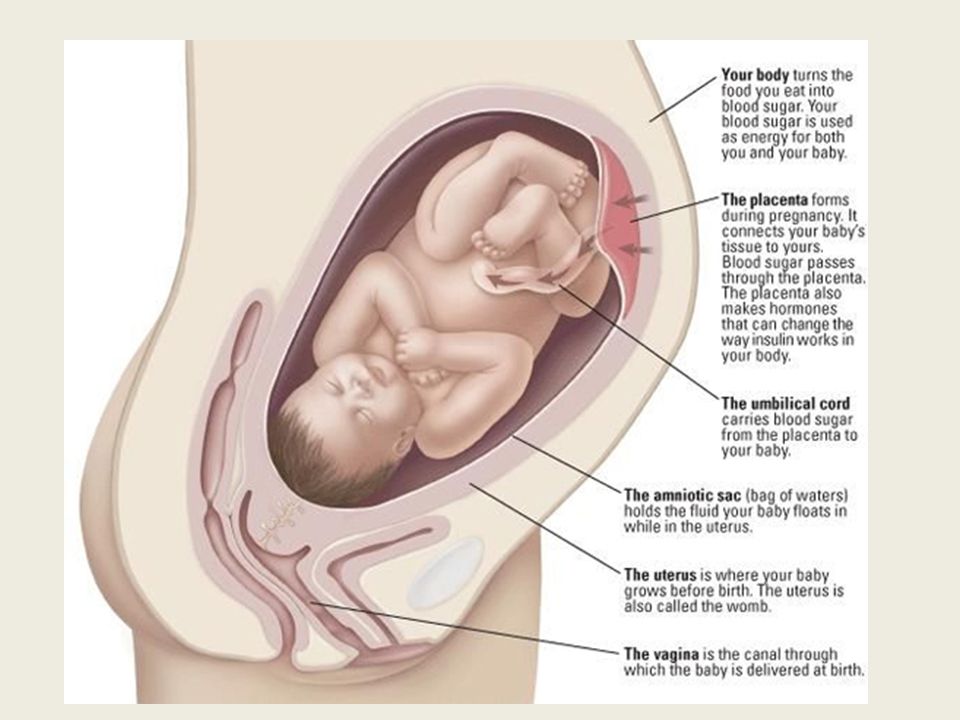 Here you need to prioritize and decide what is more important for you - the daily routine or the development of the child. If you want to properly take care of the child and at the same time not start life, look for helpers-allies with whom you can do everything.
Here you need to prioritize and decide what is more important for you - the daily routine or the development of the child. If you want to properly take care of the child and at the same time not start life, look for helpers-allies with whom you can do everything.
Make an appointment
to the doctor - Bagdasaryan Kristina Genrihovna
Clinic "Mother and Child" St. Petersburg
PregnancyManagement of pregnancyManagement of pregnancy after IVFManagement of pregnancy in Rh-conflictGynecologyPregnancy diaryImmunological causes of miscarriageConservative gynecologyConservative treatment of cervical pathologyContracts for the management of pregnancyTreatment of miscarriagePlanning pregnancyHLA compatibility
By clicking on the send button, I consent to the processing of personal data
Attention! Prices for services in different clinics may vary. To clarify the current cost, select a clinic
All areasSpecialist consultations (children)Therapeutic research
01.