What cause preeclampsia in pregnancy
Preeclampsia - Symptoms and causes
Overview
Preeclampsia is a complication of pregnancy. With preeclampsia, you might have high blood pressure, high levels of protein in urine that indicate kidney damage (proteinuria), or other signs of organ damage. Preeclampsia usually begins after 20 weeks of pregnancy in women whose blood pressure had previously been in the standard range.
Left untreated, preeclampsia can lead to serious — even fatal — complications for both the mother and baby.
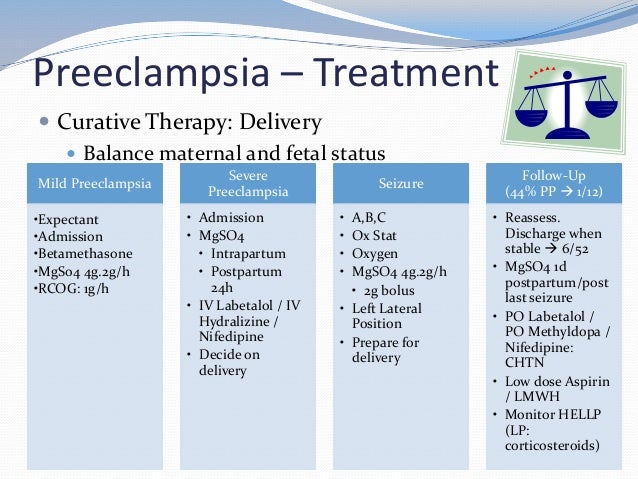
Early delivery of the baby is often recommended. The timing of delivery depends on how severe the preeclampsia is and how many weeks pregnant you are. Before delivery, preeclampsia treatment includes careful monitoring and medications to lower blood pressure and manage complications.
Preeclampsia may develop after delivery of a baby, a condition known as postpartum preeclampsia.
Products & Services
- Book: Mayo Clinic Guide to a Healthy Pregnancy
Symptoms
The defining feature of preeclampsia is high blood pressure, proteinuria, or other signs of damage to the kidneys or other organs. You may have no noticeable symptoms. The first signs of preeclampsia are often detected during routine prenatal visits with a health care provider.
Along with high blood pressure, preeclampsia signs and symptoms may include:
- Excess protein in urine (proteinuria) or other signs of kidney problems
- Decreased levels of platelets in blood (thrombocytopenia)
- Increased liver enzymes that indicate liver problems
- Severe headaches
- Changes in vision, including temporary loss of vision, blurred vision or light sensitivity
- Shortness of breath, caused by fluid in the lungs
- Pain in the upper belly, usually under the ribs on the right side
- Nausea or vomiting
Weight gain and swelling (edema) are typical during healthy pregnancies. However, sudden weight gain or a sudden appearance of edema — particularly in your face and hands — may be a sign of preeclampsia.
When to see a doctor
Make sure you attend your prenatal visits so that your health care provider can monitor your blood pressure.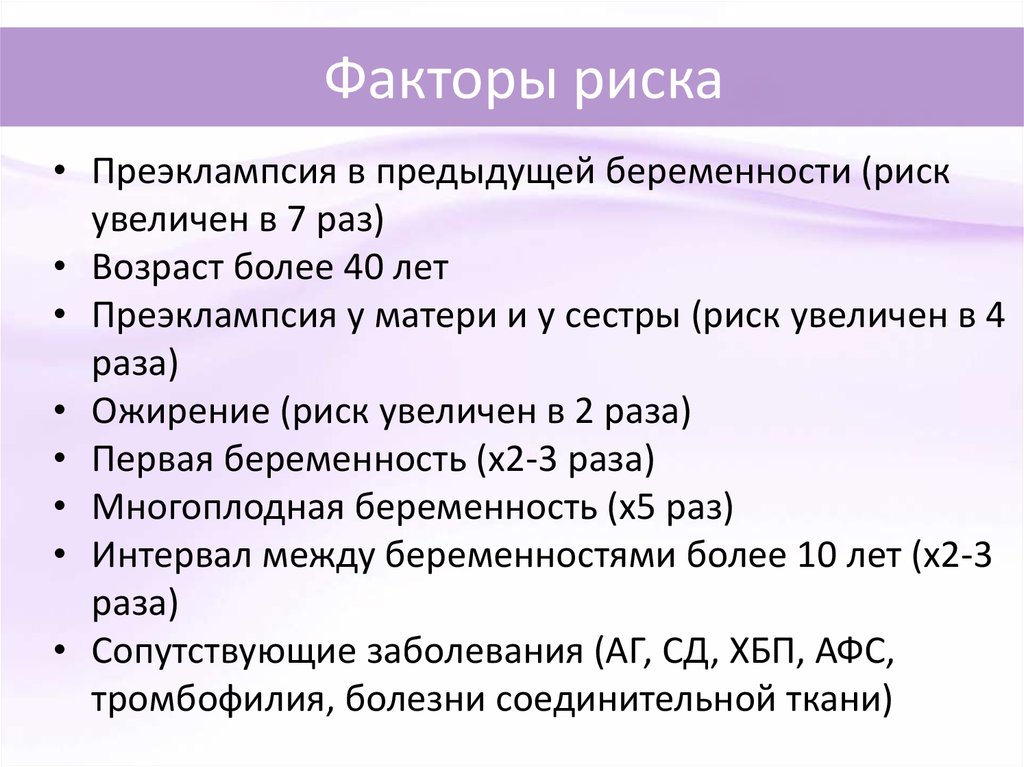 Contact your provider immediately or go to an emergency room if you have severe headaches, blurred vision or other visual disturbances, severe belly pain, or severe shortness of breath.
Contact your provider immediately or go to an emergency room if you have severe headaches, blurred vision or other visual disturbances, severe belly pain, or severe shortness of breath.
Because headaches, nausea, and aches and pains are common pregnancy complaints, it's difficult to know when new symptoms are simply part of being pregnant and when they may indicate a serious problem — especially if it's your first pregnancy. If you're concerned about your symptoms, contact your doctor.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which
information is beneficial, we may combine your email and website usage information with
other information we have about you.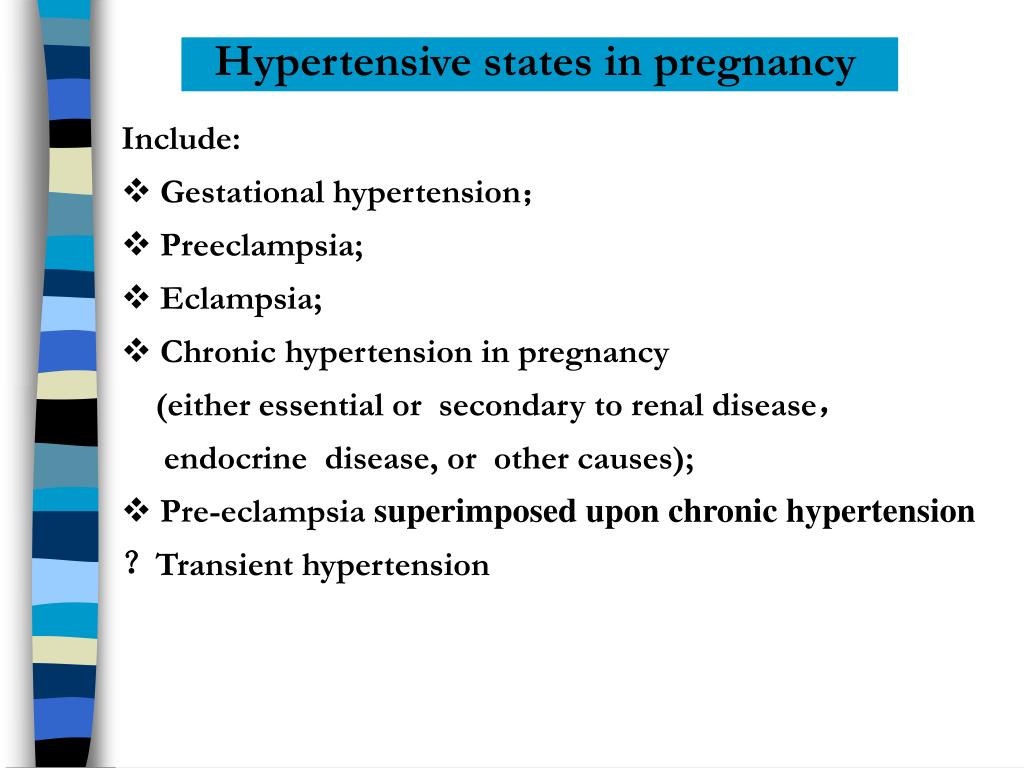 If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
Causes
The exact cause of preeclampsia likely involves several factors. Experts believe it begins in the placenta — the organ that nourishes the fetus throughout pregnancy. Early in a pregnancy, new blood vessels develop and evolve to supply oxygen and nutrients to the placenta.
In women with preeclampsia, these blood vessels don't seem to develop or work properly. Problems with how well blood circulates in the placenta may lead to the irregular regulation of blood pressure in the mother.
Problems with how well blood circulates in the placenta may lead to the irregular regulation of blood pressure in the mother.
Other high blood pressure disorders during pregnancy
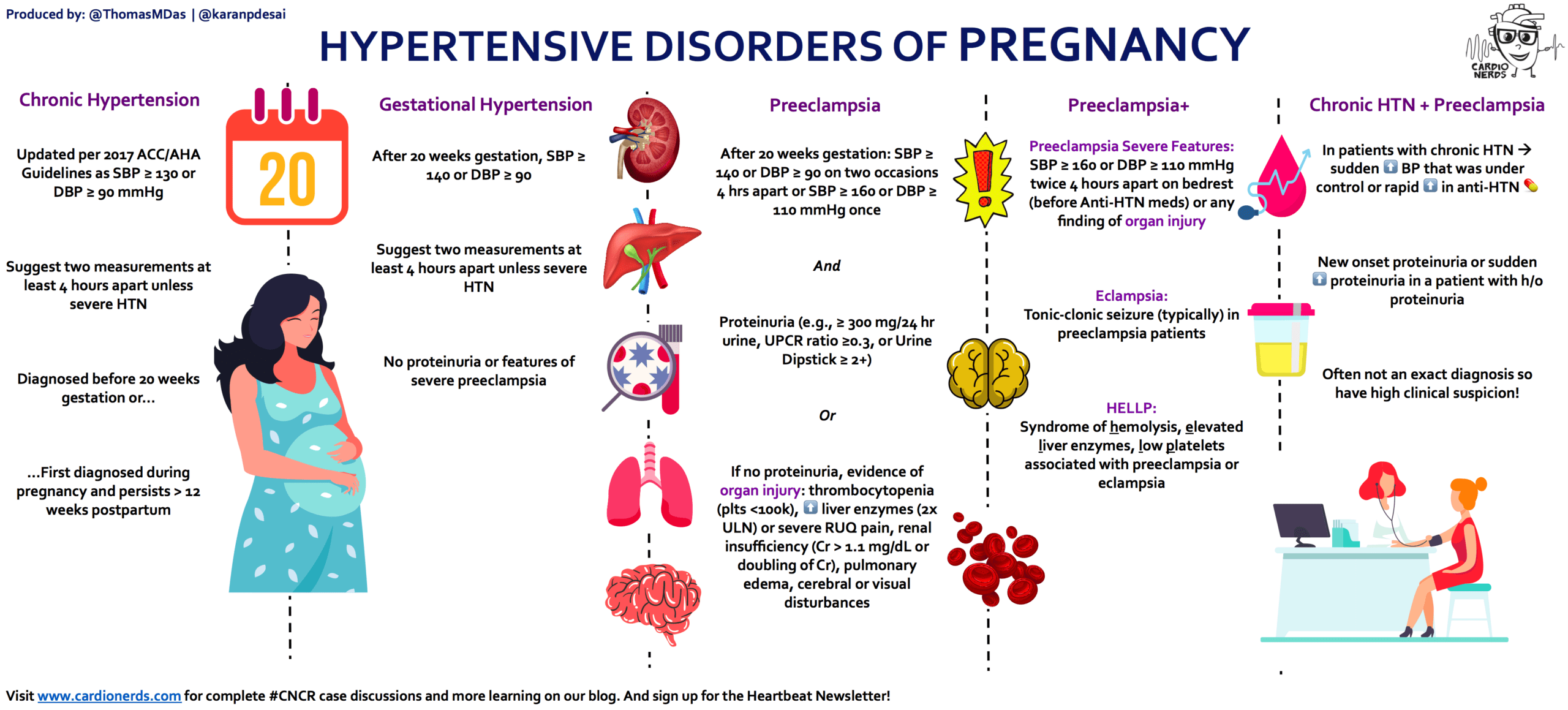
Preeclampsia is one high blood pressure (hypertension) disorder that can occur during pregnancy. Other disorders can happen, too:
- Gestational hypertension is high blood pressure that begins after 20 weeks without problems in the kidneys or other organs. Some women with gestational hypertension may develop preeclampsia.
- Chronic hypertension is high blood pressure that was present before pregnancy or that occurs before 20 weeks of pregnancy. High blood pressure that continues more than three months after a pregnancy also is called chronic hypertension.
- Chronic hypertension with superimposed preeclampsia occurs in women diagnosed with chronic high blood pressure before pregnancy, who then develop worsening high blood pressure and protein in the urine or other health complications during pregnancy.
Risk factors
Conditions that are linked to a higher risk of preeclampsia include:
- Preeclampsia in a previous pregnancy
- Being pregnant with more than one baby
- Chronic high blood pressure (hypertension)
- Type 1 or type 2 diabetes before pregnancy
- Kidney disease
- Autoimmune disorders
- Use of in vitro fertilization
Conditions that are associated with a moderate risk of developing preeclampsia include:
- First pregnancy with current partner
- Obesity
- Family history of preeclampsia
- Maternal age of 35 or older
- Complications in a previous pregnancy
- More than 10 years since previous pregnancy
Other risk factors
Several studies have shown a greater risk of preeclampsia among Black women compared with other women. There's also some evidence of an increased risk among indigenous women in North America.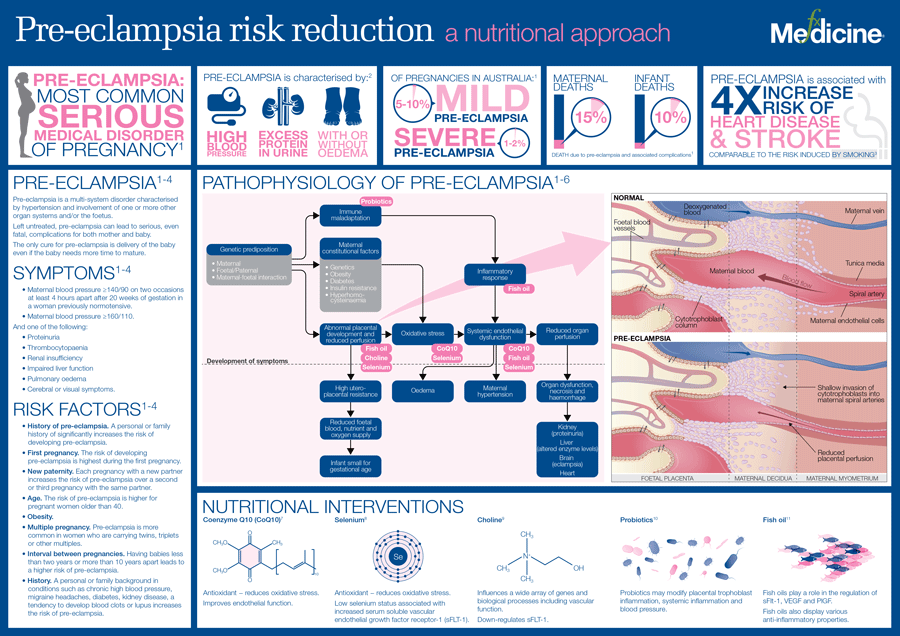
A growing body of evidence suggests that these differences in risk may not necessarily be based on biology. A greater risk may be related to inequities in access to prenatal care and health care in general, as well as social inequities and chronic stressors that affect health and well-being.
Lower income also is associated with a greater risk of preeclampsia likely because of access to health care and social factors affecting health.
For the purposes of making decisions about prevention strategies, a Black woman or a woman with a low income has a moderately increased risk of developing preeclampsia.
Complications
Complications of preeclampsia may include:
- Fetal growth restriction. Preeclampsia affects the arteries carrying blood to the placenta. If the placenta doesn't get enough blood, the baby may receive inadequate blood and oxygen and fewer nutrients. This can lead to slow growth known as fetal growth restriction.
- Preterm birth.
 Preeclampsia may lead to an unplanned preterm birth — delivery before 37 weeks. Also, planned preterm birth is a primary treatment for preeclampsia. A baby born prematurely has increased risk of breathing and feeding difficulties, vision or hearing problems, developmental delays, and cerebral palsy. Treatments before preterm delivery may decrease some risks.
Preeclampsia may lead to an unplanned preterm birth — delivery before 37 weeks. Also, planned preterm birth is a primary treatment for preeclampsia. A baby born prematurely has increased risk of breathing and feeding difficulties, vision or hearing problems, developmental delays, and cerebral palsy. Treatments before preterm delivery may decrease some risks. - Placental abruption. Preeclampsia increases your risk of placental abruption. With this condition, the placenta separates from the inner wall of the uterus before delivery. Severe abruption can cause heavy bleeding, which can be life-threatening for both the mother and baby.
-
HELLP syndrome. HELLP stands for hemolysis (the destruction of red blood cells), elevated liver enzymes and low platelet count.
 This severe form of preeclampsia affects several organ systems. HELLP syndrome is life-threatening to the mother and baby, and it may cause lifelong health problems for the mother.
This severe form of preeclampsia affects several organ systems. HELLP syndrome is life-threatening to the mother and baby, and it may cause lifelong health problems for the mother.Signs and symptoms include nausea and vomiting, headache, upper right belly pain, and a general feeling of illness or being unwell. Sometimes, it develops suddenly, even before high blood pressure is detected. It also may develop without any symptoms.
-
Eclampsia. Eclampsia is the onset of seizures or coma with signs or symptoms of preeclampsia. It is very difficult to predict whether a patient with preeclampsia will develop eclampsia. Eclampsia can happen without any previously observed signs or symptoms of preeclampsia.
Signs and symptoms that may appear before seizures include severe headaches, vision problems, mental confusion or altered behaviors.
 But, there are often no symptoms or warning signs. Eclampsia may occur before, during or after delivery.
But, there are often no symptoms or warning signs. Eclampsia may occur before, during or after delivery. - Other organ damage. Preeclampsia may result in damage to the kidneys, liver, lung, heart, or eyes, and may cause a stroke or other brain injury. The amount of injury to other organs depends on how severe the preeclampsia is.
- Cardiovascular disease. Having preeclampsia may increase your risk of future heart and blood vessel (cardiovascular) disease. The risk is even greater if you've had preeclampsia more than once or you've had a preterm delivery.
Prevention
Medication
The best clinical evidence for prevention of preeclampsia is the use of low-dose aspirin. Your primary care provider may recommend taking an 81-milligram aspirin tablet daily after 12 weeks of pregnancy if you have one high-risk factor for preeclampsia or more than one moderate-risk factor.
It's important that you talk with your provider before taking any medications, vitamins or supplements to make sure it's safe for you.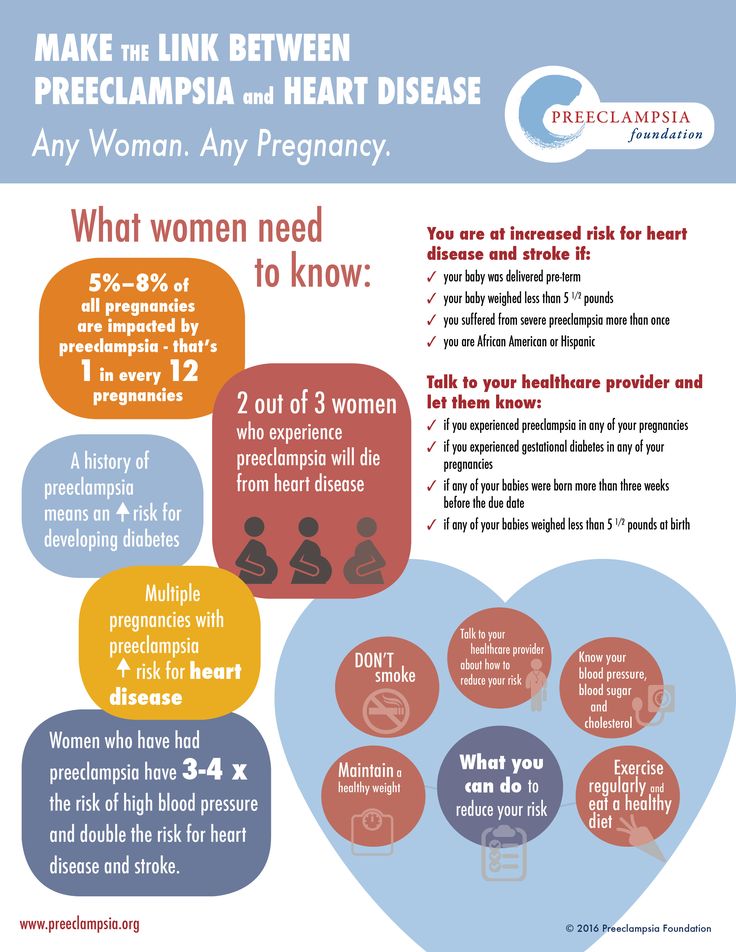
Lifestyle and healthy choices
Before you become pregnant, especially if you've had preeclampsia before, it's a good idea to be as healthy as you can be. Talk to your provider about managing any conditions that increase the risk of preeclampsia.
By Mayo Clinic Staff
Related
Associated Procedures
News from Mayo Clinic
Products & Services
Pre-eclampsia - NHS
Pre-eclampsia is a condition that affects some pregnant women, usually during the second half of pregnancy (from 20 weeks) or soon after their baby is delivered.
Symptoms of pre-eclampsia
Early signs of pre-eclampsia include having high blood pressure (hypertension) and protein in your urine (proteinuria).
It's unlikely that you'll notice these signs, but they should be picked up during your routine antenatal appointments.
In some cases, further symptoms can develop, including:
- severe headache
- vision problems, such as blurring or flashing
- pain just below the ribs
- vomiting
- sudden swelling of the face, hands or feet
If you notice any symptoms of pre-eclampsia, seek medical advice immediately by calling your midwife, GP surgery or NHS 111.
Although many cases are mild, the condition can lead to serious complications for both mother and baby if it's not monitored and treated.
The earlier pre-eclampsia is diagnosed and monitored, the better the outlook for mother and baby.
Video: what is pre-eclampsia and what are the warning signs?
In this video, a midwife explains the warning signs of pre-eclampsia.
Media last reviewed: 1 September 2020
Media review due: 1 September 2023
Who's affected?
There are a number of things that can increase your chances of developing pre-eclampsia, such as:
- having diabetes, high blood pressure or kidney disease before you were pregnant
- having an autoimmune condition, such as lupus or antiphospholipid syndrome
- having high blood pressure or pre-eclampsia in a previous pregnancy
Other things that can slightly increase your chances of developing pre-eclampsia include:
- a family history of pre-eclampsia
- being 40 years old or more
- it's more than 10 years since your last pregnancy
- expecting multiple babies (twins or triplets)
- having a body mass index (BMI) of 35 or more
If you have 2 or more of these together, your chances are higher.
If you're thought to be at a high risk of developing pre-eclampsia, you may be advised to take a 75 to 150mg daily dose of aspirin from the 12th week of pregnancy until your baby is born.
What causes pre-eclampsia?
Although the exact cause of pre-eclampsia is not known, it's thought to occur when there's a problem with the placenta, the organ that links the baby's blood supply to the mother's.
Treating pre-eclampsia
If you're diagnosed with pre-eclampsia, you should be referred for an assessment by a specialist, usually in hospital.
While in hospital, you'll be monitored closely to determine how severe the condition is and whether a hospital stay is needed.
The only way to cure pre-eclampsia is to deliver the baby, so you'll usually be monitored regularly until it's possible for your baby to be delivered.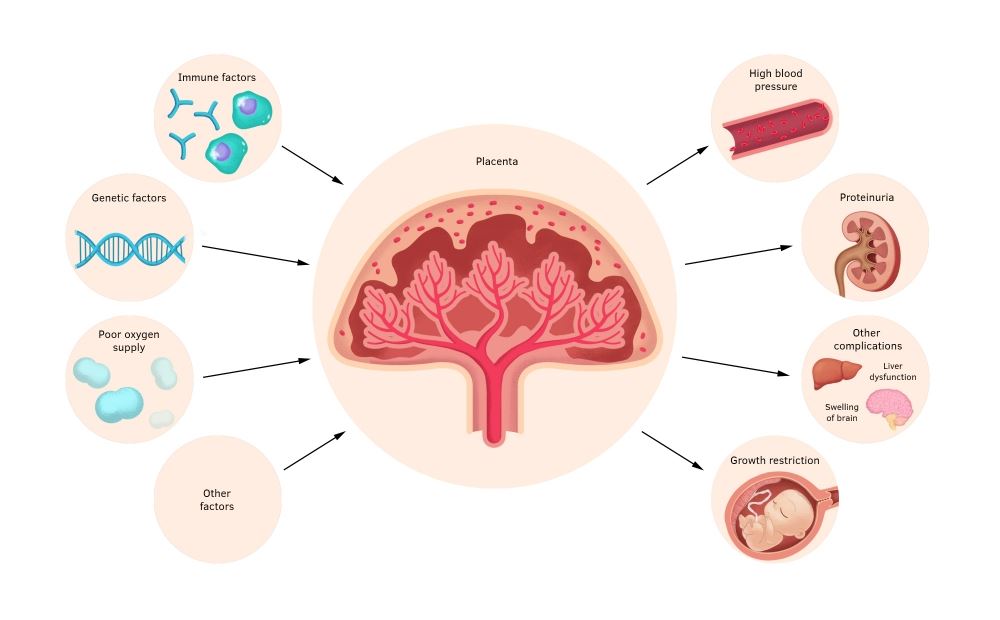
This will normally be at around 37 to 38 weeks of pregnancy, but it may be earlier in more severe cases.
At this point, labour may be started artificially (induced) or you may have a caesarean section.
You'll be offered medicine to lower your blood pressure while you wait for your baby to be delivered.
Complications
Although most cases of pre-eclampsia cause no problems and improve soon after the baby is delivered, there's a risk of serious complications that can affect both the mother and her baby.
There's a risk that the mother will develop fits called "eclampsia". These fits can be life threatening for the mother and baby, but they're rare.
Page last reviewed: 28 September 2021
Next review due: 28 September 2024
Preeclampsia and pregnancy | Ida-Tallinna Keskhaigla
The purpose of this leaflet is to provide the patient with information about the nature, occurrence, risk factors, symptoms and treatment of preeclampsia.
What is preeclampsia?
Pre-eclampsia is a disease that occurs during pregnancy and is characterized by high blood pressure and protein in the urine. Preeclampsia is one of the most common complications of pregnancy. Epilepsy-like seizures occur in severe preeclampsia and are life-threatening.
What symptoms may indicate the development of preeclampsia?
High blood pressure - blood pressure values are 140/90 mmHg. Art. or higher. If systolic (upper) or diastolic (lower) blood pressure rises by 30 mm Hg. Art. or more, then such an increase cannot be ignored.
Protein in urine - 300 mg in urine collected over 24 hours, or +1 value on a rapid test.
Swelling of the arms, legs or face , especially under the eyes or if the swelling leaves a depression in the skin when pressed. Edema can occur in all pregnant women and is generally harmless, but rapidly developing edema should be taken into account.
Edema can occur in all pregnant women and is generally harmless, but rapidly developing edema should be taken into account.
Headache that does not improve after taking pain medication.
Visual disturbances - double vision or blurred vision, dots or flashes before the eyes, auras.
Nausea or pain in the upper abdomen - These symptoms are often mistaken for indigestion or gallbladder pain. Nausea in the second half of pregnancy is not normal.
Sudden weight gain - 2 kg or more per week.
As a rule, there is a mild course of the disease that occurs at the end of pregnancy and has a good prognosis. Sometimes, preeclampsia can worsen quickly and be dangerous to both mother and fetus. In such cases, rapid diagnosis and careful monitoring of the mother and child are of paramount importance.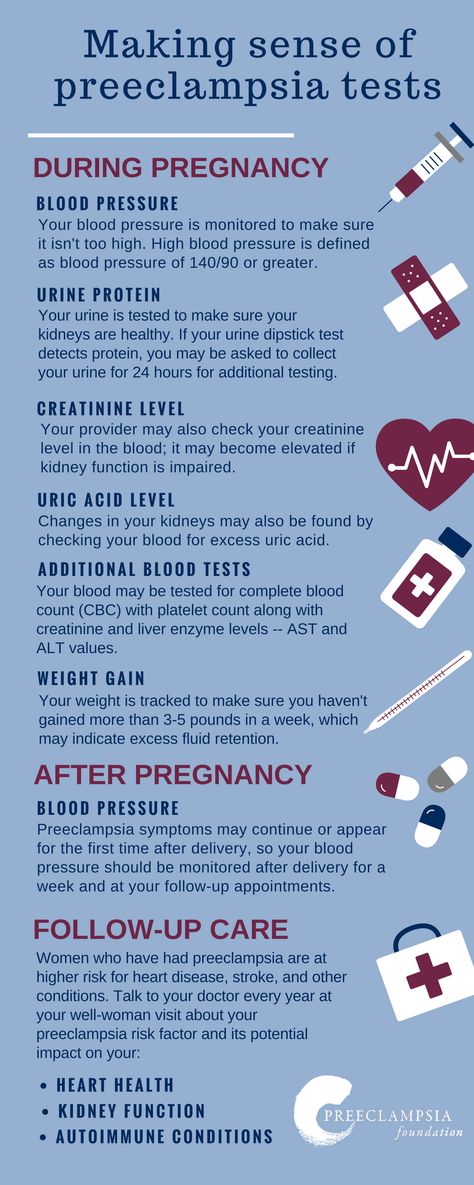
Unfortunately, most women show symptoms in the final stages of the disease. If you experience any of the above symptoms, you should contact your midwife, gynecologist, or the Women's Clinic emergency department.
Is preeclampsia called toxemia of pregnancy?
Previously, pre-eclampsia was really called toxicosis, or toxemia, since it was believed that the cause of the disease was toxins, that is, poisons in the blood of a pregnant woman.
What is the difference between preeclampsia and gestational hypertension?
Pregnancy hypertension is an increase in blood pressure above normal after the 20th week of pregnancy. With hypertension of pregnant women, protein in the urine is not observed.
What is HELLP syndrome?
HELLP syndrome is one of the most severe forms of preeclampsia.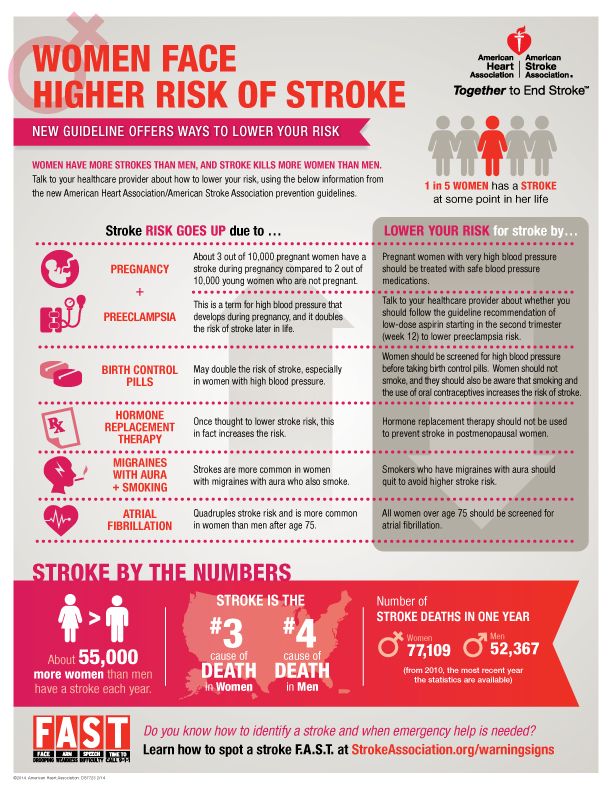 HELLP syndrome is rare and sometimes develops before symptoms of preeclampsia appear. Sometimes the syndrome is difficult to diagnose, as the symptoms resemble gallbladder colic or a cold.
HELLP syndrome is rare and sometimes develops before symptoms of preeclampsia appear. Sometimes the syndrome is difficult to diagnose, as the symptoms resemble gallbladder colic or a cold.
When does preeclampsia occur?
Preeclampsia usually occurs after the 20th week of pregnancy. As a rule, preeclampsia goes away after delivery, but complications can occur up to six weeks after delivery, during which careful monitoring of the condition is necessary. If by the sixth week after birth, blood pressure does not return to normal, then you need to contact a cardiologist, who will begin treatment against hypertension.
What is the cause of preeclampsia?
The causes of the disease are still not clear, there are only unproven hypotheses.
How does the disease affect pregnant women and pregnancy?
Most preeclamptic pregnancies have a favorable outcome and a healthy baby is born.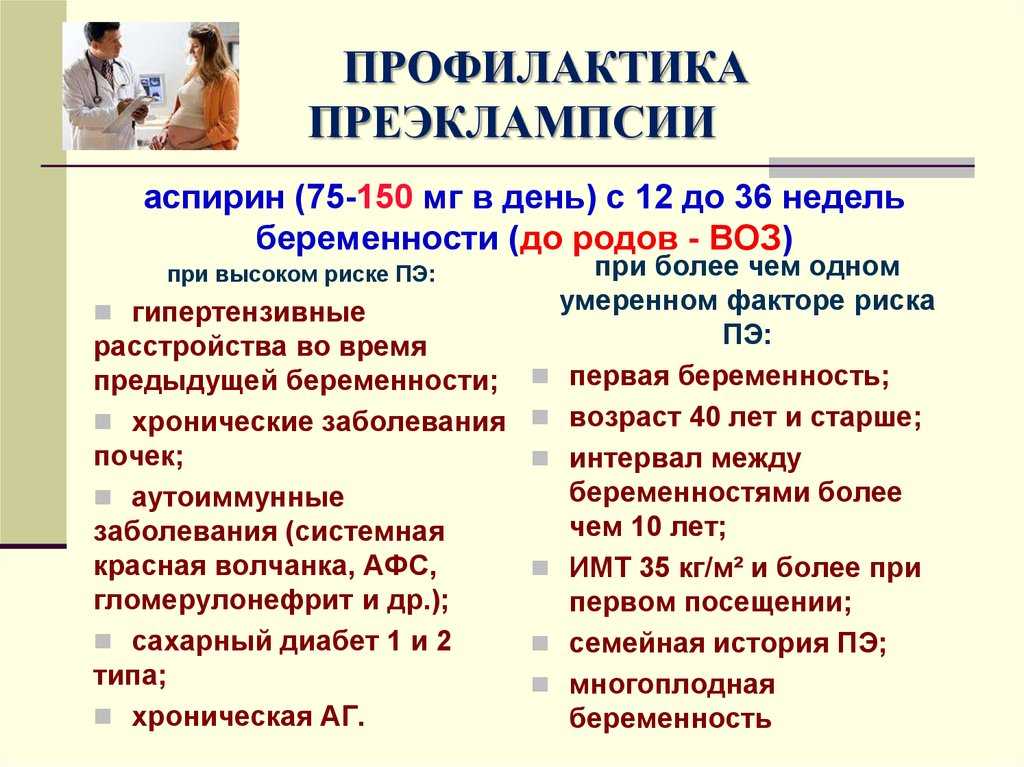 However, the disease is very serious and is one of the most common causes of death of the child and mother. Preeclampsia affects a woman's kidneys, liver, and other vital organs, and if left untreated, it can cause seizures (eclampsia), cerebral hemorrhage, multiple organ failure, and death.
However, the disease is very serious and is one of the most common causes of death of the child and mother. Preeclampsia affects a woman's kidneys, liver, and other vital organs, and if left untreated, it can cause seizures (eclampsia), cerebral hemorrhage, multiple organ failure, and death.
How does the disease affect the fetus?
In preeclampsia, the fetus does not receive enough oxygen and nutrients to grow, and intrauterine growth retardation may occur. In addition, the placenta may separate from the uterine wall before the baby is born. Since the only treatment for preeclampsia is childbirth, sometimes a pregnancy has to be terminated prematurely. Until the 34th week of pregnancy, the lungs of the fetus have not yet matured, and steroid hormones are administered intravenously to the pregnant woman to prepare her lungs. In addition to the immaturity of the lungs, the health of a premature baby is threatened by many other diseases.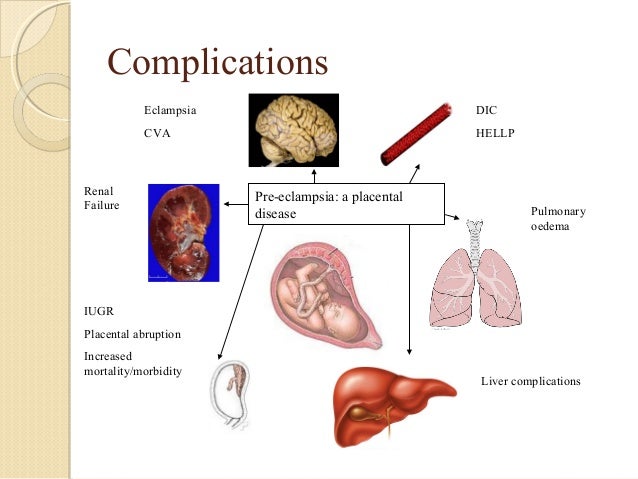
Who is at risk of developing preeclampsia?
Preeclampsia occurs in approximately 8% of pregnant women, many of whom have no known risk factors.
What are the risk factors for preeclampsia?
Patient-related risk factors
-
First pregnancy
-
Pre-eclampsia during a previous pregnancy
-
Age over 40 or under 18
-
High blood pressure before pregnancy
-
Diabetes before or during pregnancy
-
Multiple pregnancy
-
Overweight (BMI> 30)
-
Systemic lupus erythematosus or other autoimmune disease
-
Polycystic ovary syndrome
-
Long interval between two pregnancies
Risk factors associated with the patient's family
What is the prevention and treatment of preeclampsia
During the first trimester screening, or Oscar test, in addition to the most common chromosomal diseases, the risk of preeclampsia is also calculated.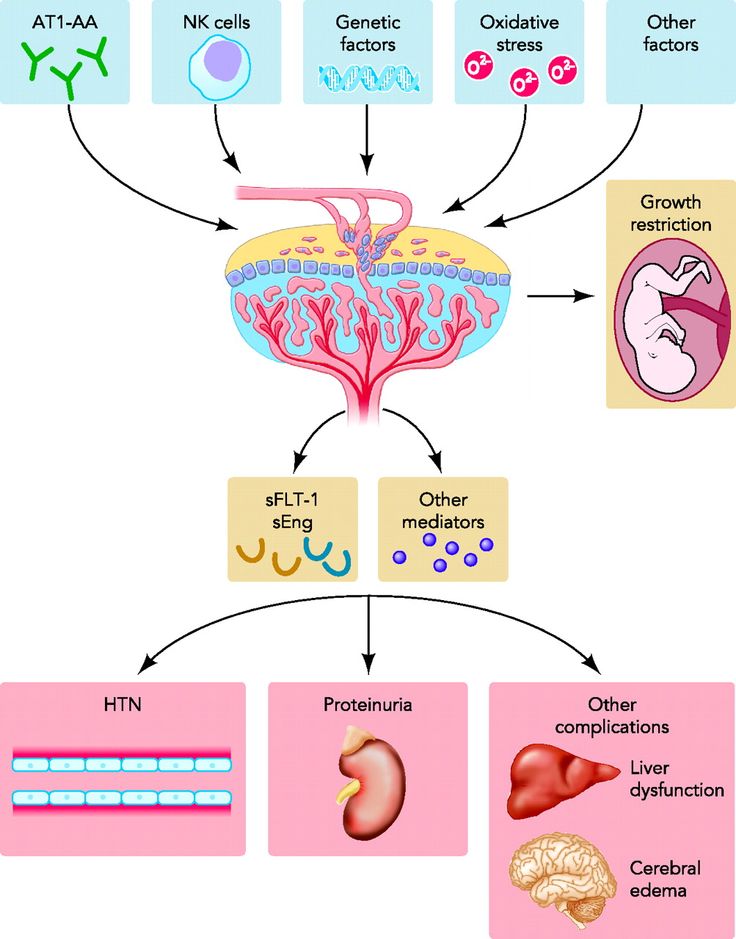 In case of high risk, pregnant women are advised to take aspirin (acetylsalicylic acid) at a dose of 150 mg in the evenings until the 36th week of pregnancy. This helps reduce the chance of preeclampsia by the 34th week of pregnancy by up to 80%.
In case of high risk, pregnant women are advised to take aspirin (acetylsalicylic acid) at a dose of 150 mg in the evenings until the 36th week of pregnancy. This helps reduce the chance of preeclampsia by the 34th week of pregnancy by up to 80%.
Childbirth is the only treatment for preeclampsia. Sometimes a child can be born naturally, but sometimes, if the disease is very acute, an emergency caesarean section is necessary. The best time to have a baby is after the 37th week of pregnancy. Bed rest, medications, and, if necessary, hospitalization can sometimes help bring the condition under control and prolong the pregnancy. Often, a doctor will refer a woman with preeclampsia to the hospital for observation, as the condition of the fetus and pregnant woman may suddenly worsen.
Does bed rest help?
Sometimes bed rest is enough to bring mild preeclampsia under control. In this case, the patient often visits a doctor who measures blood pressure, does blood and urine tests, and monitors the course of the disease. The condition of the fetus is also often examined using a cardiotocogram (CTG) and ultrasound.
In this case, the patient often visits a doctor who measures blood pressure, does blood and urine tests, and monitors the course of the disease. The condition of the fetus is also often examined using a cardiotocogram (CTG) and ultrasound.
Are drugs used to treat preeclampsia?
High blood pressure sometimes requires medication. The medications used have few side effects, the drugs prescribed do not have much effect on the fetus, but are very important in the treatment of maternal high blood pressure.
Seizures are a rare but very serious complication of preeclampsia. Magnesium sulfate is sometimes given intravenously to prevent seizures in a pregnant woman with preeclampsia both during and after childbirth. It is safe for the fetus, but the mother may experience side effects such as hot flashes, sweating, thirst, visual disturbances, mild confusion, muscle weakness, and shortness of breath.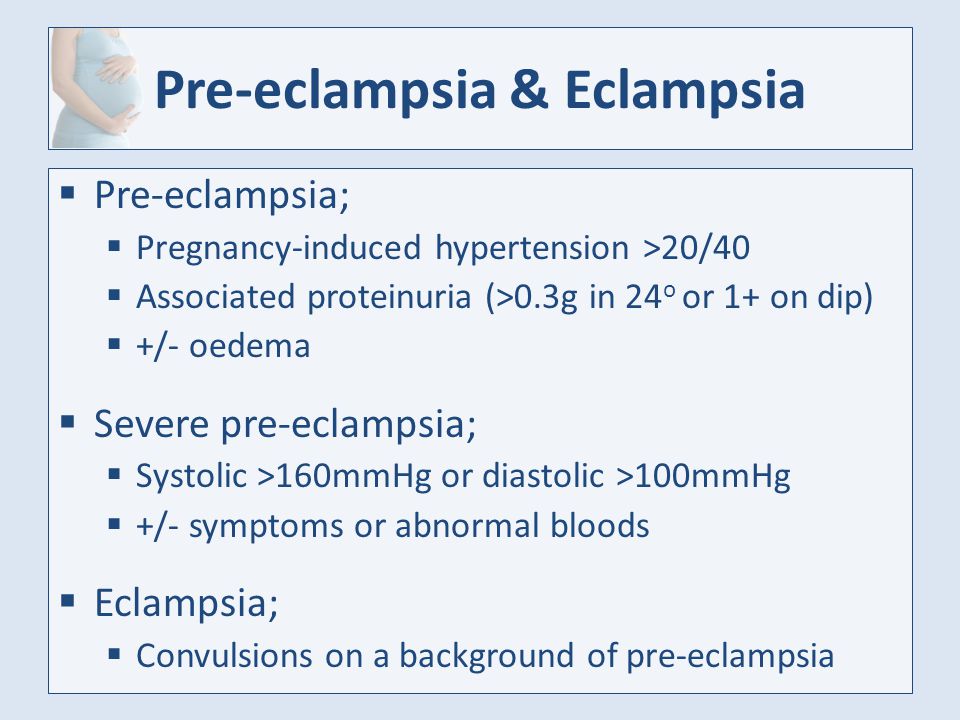 All these side effects disappear when the drug is discontinued.
All these side effects disappear when the drug is discontinued.
Can preeclampsia recur?
Preeclampsia does not necessarily recur in the next pregnancy, but the main risk factor for preeclampsia is the presence of preeclampsia in a previous pregnancy(s). Risk factors for relapse include the severity of the previous case and the woman's overall health during pregnancy. A woman who has previously had preeclampsia should consult a gynecologist during a new pregnancy or when planning a pregnancy.
ITK1013
The information material was approved by the Health Care Quality Committee of East-Tallinn Central Hospital on 27.01.2021 (Minutes No. 2-21).
pre-eclampsia
Every mother-to-be wants her pregnancy to be a time of joyful anticipation. But the fear of preeclampsia can darken the joy.
What is preeclampsia?
Pre-eclampsia is a potentially life-threatening disease that occurs during pregnancy and affects multiple organ systems and is characterized by high maternal blood pressure and protein in the urine, or in the absence of the latter, dysfunction of other organ systems. This can affect both you and your unborn child. If the risk of preeclampsia is known in advance, it can be prevented.
This can affect both you and your unborn child. If the risk of preeclampsia is known in advance, it can be prevented.
How common is preeclampsia?
Most women have a normal pregnancy. At the same time, pre-eclampsia is a relatively common disease during pregnancy, which occurs in two out of a hundred women in Estonia.
When does preeclampsia occur?
Pre-eclampsia occurs after the 20th week of pregnancy or up to six weeks after delivery. Most often, preeclampsia occurs between the 32nd and 36th weeks of pregnancy. The earlier in pregnancy the disease occurs, the more severe its course, and the more dangerous it is for the mother and child.
What causes preeclampsia?
The exact causes of preeclampsia are unknown, but it is believed that they lie in the violation of the attachment of the developing placenta to the uterus, as a result of which there is no reliable connection between the circulatory systems of the mother and child.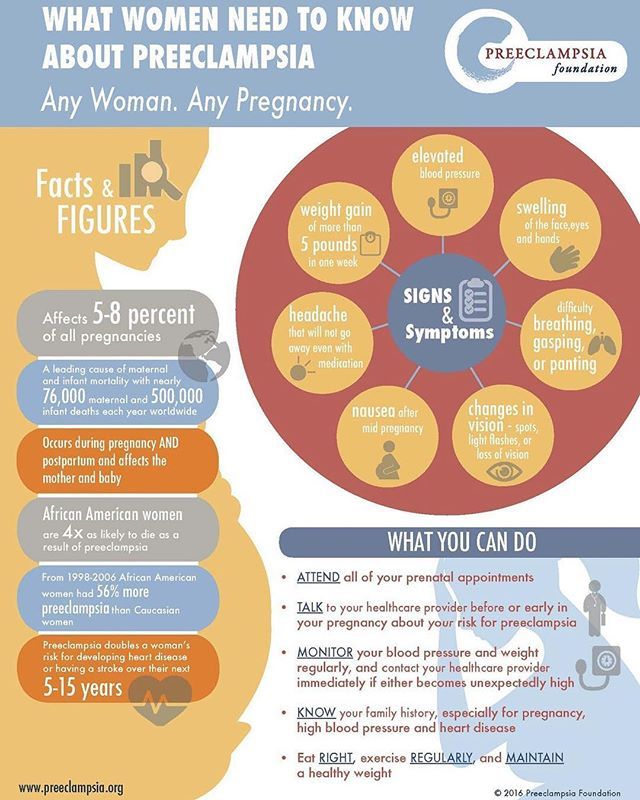 At the same time, a rapidly developing fetus requires oxygen and nutrients from the mother's circulatory system for its growth. If oxygen deficiency occurs in the developing placenta, toxic substances are released into the mother's circulatory system, which damage the lining of the mother's blood vessels. This is how a systemic lesion of the internal organs of the mother is formed. In order to save the lives of mother and child, the child must be born. If this happens at a very early stage of pregnancy, the baby is not yet ready for extrauterine life.
At the same time, a rapidly developing fetus requires oxygen and nutrients from the mother's circulatory system for its growth. If oxygen deficiency occurs in the developing placenta, toxic substances are released into the mother's circulatory system, which damage the lining of the mother's blood vessels. This is how a systemic lesion of the internal organs of the mother is formed. In order to save the lives of mother and child, the child must be born. If this happens at a very early stage of pregnancy, the baby is not yet ready for extrauterine life.
How will this affect me?
Mostly there is a mild form of the disease that occurs at the end of pregnancy and the prognosis for which is good. But sometimes pre-eclampsia can get worse very quickly and begin to threaten the lives of the mother and child. Preeclampsia also has a long-term effect on a woman's health, as it doubles the incidence of cardiovascular disease in the future. Most women with preeclampsia are hospitalized, and often their children have to be born prematurely.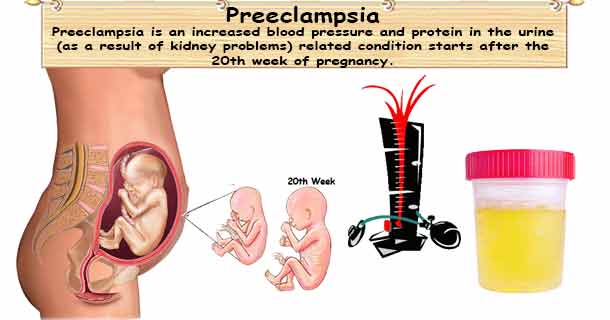 If the health of the mother or child is at risk, labor is induced or a caesarean section is performed.
If the health of the mother or child is at risk, labor is induced or a caesarean section is performed.
How will this affect my child?
Most children remain healthy even when their mothers have severe preeclampsia. But sometimes preeclampsia can threaten the life and health of both the fetus and the newborn. Maternal preeclampsia doubles the risk of a surviving child suffering from cerebral palsy, that is, brain damage that results in delayed physical and sometimes mental development. In addition, surviving children are more likely to develop cardiovascular disease, obesity and diabetes in the future. In preeclampsia, there is not enough oxygen and nutrients for the growth of the fetus, and intrauterine growth retardation occurs. Since the only treatment for preeclampsia is childbirth, sometimes the pregnancy has to be terminated. Until the 34th week of pregnancy, the lungs of the fetus have not yet fully developed, and steroid injections are given to the pregnant woman to stimulate them.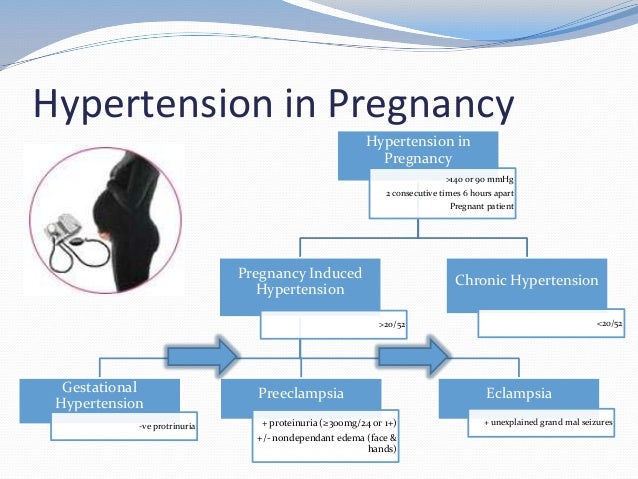
How to recognize preeclampsia?
Unfortunately, in most women, the symptoms of the disease appear only at an advanced stage.
- Chronic headache not responding to painkillers
- Severe nausea and vomiting
- Visual disturbances, tinnitus
- Pain in the right hypochondrium
- Feeling short of breath, shortness of breath
- Infrequent urge to urinate (less than 500 ml per day)
- Edema of hands, face and eyelids
- Rapid weight gain (more than 1 kg per week)
If you experience any of the above symptoms, contact your obstetrician, gynecologist or hospital doctor on call.
Am I at risk?
Although all pregnant women can develop preeclampsia, some women are more at risk than others.
You are at greater risk if
- this is your first pregnancy;
- you had preeclampsia during a previous pregnancy;
- your sister or mother had preeclampsia;
- Your body mass index is 35 kg/m 2 or more;
- You are at least 40 years old;
- the time between births was more than 10 years;
- You are expecting twins;
- You have become pregnant in vitro;
- you have any medical problem, such as hypertension, kidney problems, lupus, diabetes;
- You developed diabetes during this pregnancy.
At what stage of pregnancy is screening performed?
Screening for preeclampsia can be done in all three trimesters.
- First trimester, 11–13 weeks +6 weeks (as part of the OSCAR test)
- Second trimester, 19-21 weeks +6 weeks (as part of fetal anatomy screening)
- Third trimester, 34-36 weeks (as part of a growth and fetal study)
A three-stage screening test for preeclampsia can prevent it from occurring or move it to a later stage of pregnancy.
How reliable is screening for preeclampsia?
In the first trimester, the OSCAR test can identify women at risk of developing early preeclampsia with 76% accuracy before the 37th week of pregnancy. Among pregnant twins, all women who can develop early preeclampsia can be identified before the 37th week of pregnancy.
In the second trimester, fetal anatomy screening can identify women at risk of developing early preeclampsia with an accuracy of 85% before the 37th week of pregnancy.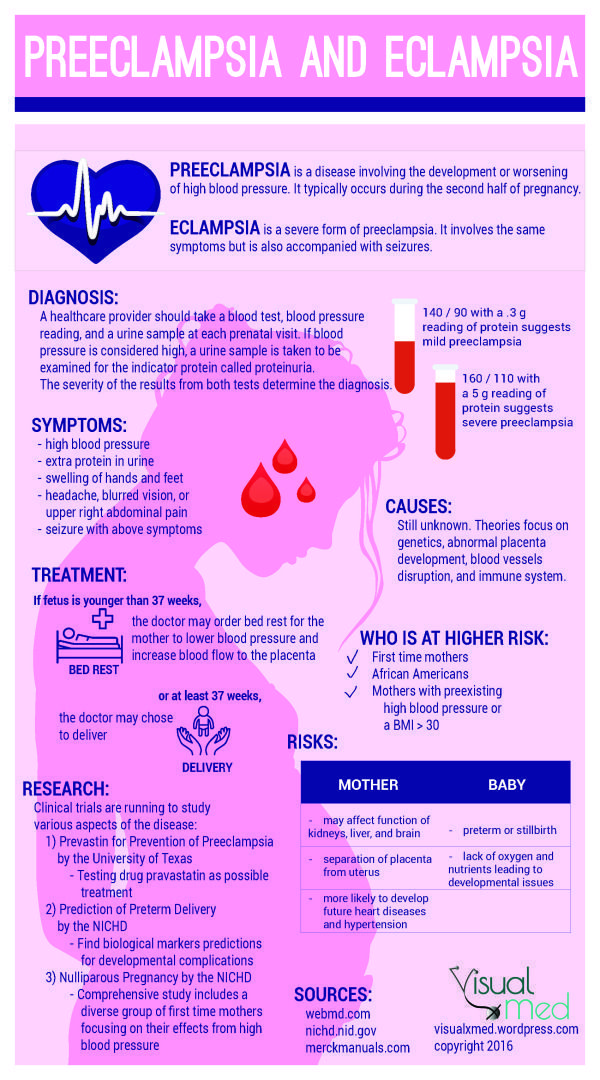
In the 3rd trimester, growth and fetal ultrasound can identify women at risk for developing late preeclampsia after 37 weeks of pregnancy with 85% accuracy.
Why should I assess my risk for preeclampsia?
The best way to assess the risk of early preeclampsia is in the first trimester with the OSCAR test, when at-risk women will benefit from the anti-preeclampsia effect of aspirin. Studies have shown that small doses of aspirin before the 16th week of pregnancy in 62% of cases reduce the risk of early preeclampsia, which may require delivery before the 37th week. Therefore, women with an increased risk of preeclampsia are advised to take 150 milligrams of aspirin once a day, in the evenings, until the 36th week of pregnancy. The goal of prophylactic treatment for women at high risk of preeclampsia is either to avoid the development of preeclampsia or to postpone its occurrence until later in pregnancy, when the child is ready for birth.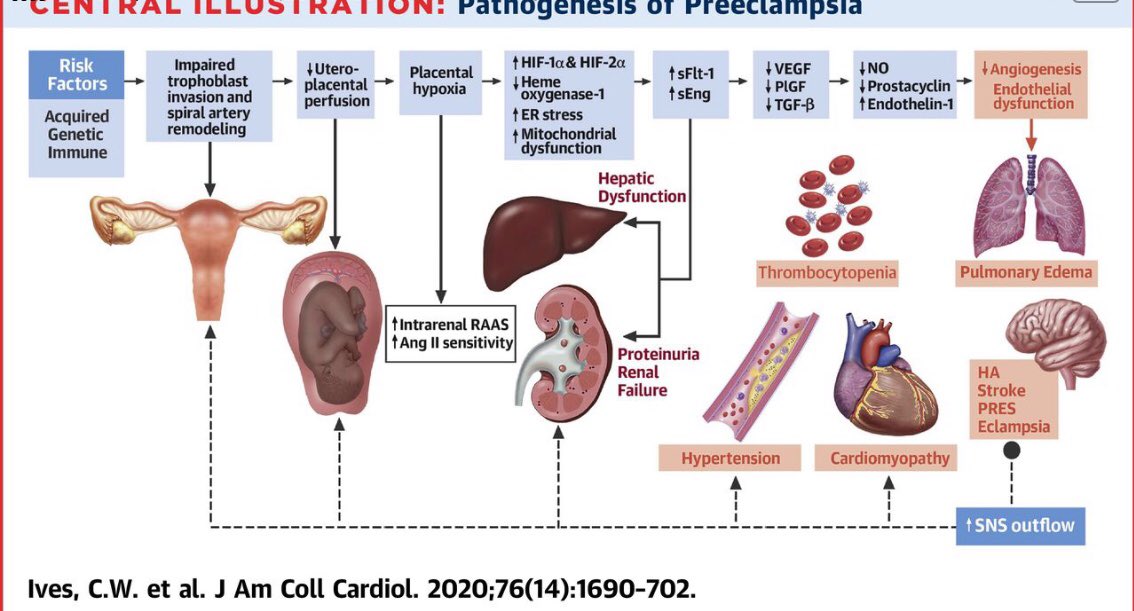
During the second trimester, fetal anatomy screening may reassess the OSCAR risk for preeclampsia or recommend screening for preeclampsia in women who were not assessed for preeclampsia by OSCAR.
In the third trimester, ultrasound examination of the growth and condition of the fetus can assess the risk of late preeclampsia. This is very important as 75% of preeclampsia cases develop after the 37th week of pregnancy. This makes it possible to more intensively examine women with an increased risk of preeclampsia and to detect the disease in a timely manner, as well as to prepare the baby's lungs for an early birth.
How is preeclampsia screened?
Screening for pre-eclampsia consists of an appointment with a nurse and an ultrasound examination by a gynecologist. The nurse interviews the pregnant woman, measuring her blood pressure, height and weight, and doing a blood test. The gynecologist performs an ultrasound examination and measures the blood flow indices of the uterine arteries feeding the placenta.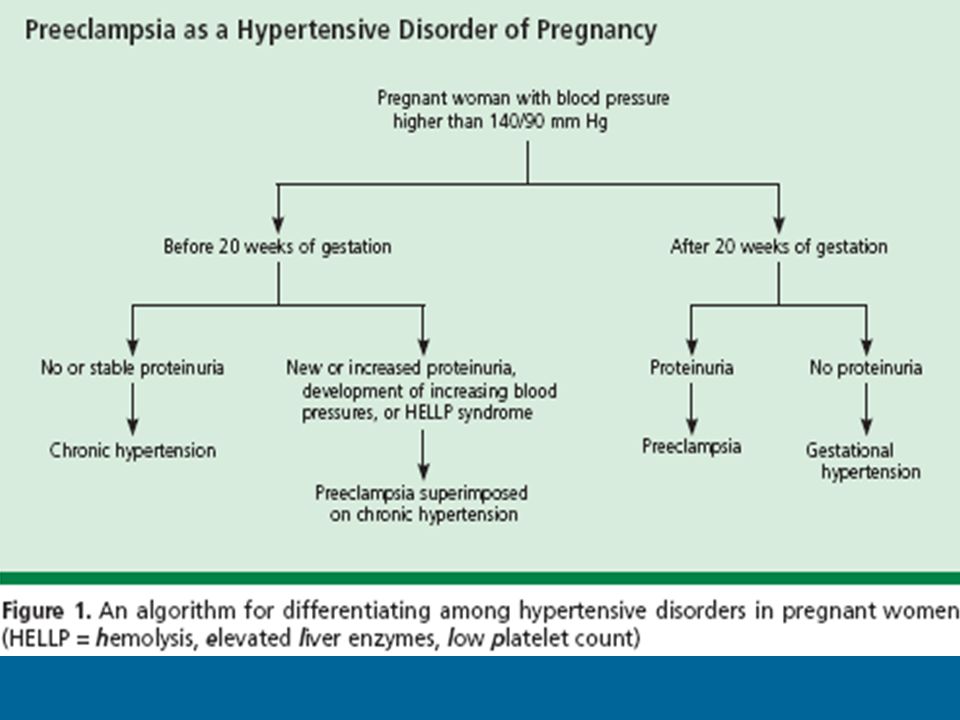 Based on the blood test values of hormone levels and associated risk factors for preeclampsia, blood pressure parameters, body mass index and uterine arterial blood flow indices, the gynecologist uses a special computer program to assess the individual risk of early or late preeclampsia.
Based on the blood test values of hormone levels and associated risk factors for preeclampsia, blood pressure parameters, body mass index and uterine arterial blood flow indices, the gynecologist uses a special computer program to assess the individual risk of early or late preeclampsia.
- The risk of preeclampsia can be assessed in one day.
- The risk of preeclampsia can also be assessed for women who are expecting twins.
Preeclampsia screening makes you feel safe
Most of the women who participate in preeclampsia screening are at low risk. At increased risk, a three-stage screening test for preeclampsia provides an opportunity, if necessary, to prevent its occurrence or shift it to a later stage of pregnancy. Reducing the risk of pre-eclampsia and careful, evidence-based monitoring of your health and that of your baby gives you the much-needed sense of security. So the child will be able to safely be born when he is ready for this, and you will enjoy a healthy child.