Labor not progressing
Slow progress in labour | Pregnancy Birth and Baby
Slow progress in labour | Pregnancy Birth and Baby beginning of content4-minute read
Listen
Slow progress in labour – sometimes referred to as failure to progress in labour or prolonged labour – refers to when labour doesn’t go as quickly as expected. It’s one of the main reasons that interventions are used in labour, but there are other things to consider before doctors recommend an intervention.
What is slow progress in labour?
Slow progress in labour refers to when the first or second of the 3 stages of labour does’t go as planned.
The first stage is when your contractions increase and your cervix begins to dilate (open up). There is no limit to how long this stage might be, and it often stops and starts. However, sometimes contractions aren’t strong enough to dilate the cervix fully. If the cervix doesn’t dilate by about 1cm every hour, or if the labour stops altogether, the doctor may discuss with you the options to get labour moving along.
The second stage is when your cervix is fully open and you push the baby out through your vagina. Normally this can take up to 2 hours. But sometimes the baby’s position means the head doesn’t descend as it’s supposed to. If you have been pushing for more than 2 hours, your doctor will consider intervening.
Slow progress in labour can be risky. You may experience more pain and are more likely to have birth interventions. For the baby, it can increase the risk of low oxygen levels, abnormal heart rhythm, meconium in the amniotic fluid and infection.
What are the causes of slow progress in labour?
Slow progress may result if:
- the baby is large
- the baby has a large head
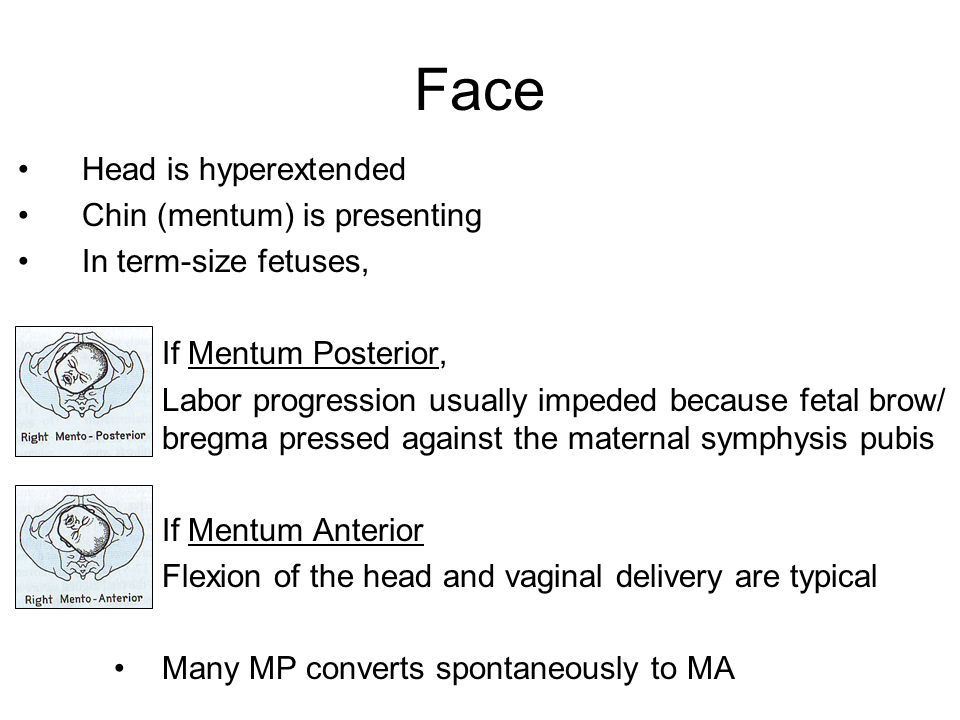
- the baby is in a difficult position (posterior, when the baby is facing your front rather than your back; or transverse, when they are lying across your abdomen)
- your contractions aren’t strong enough and the cervix doesn’t open
- your pelvis is too small to fit the baby through
You are also at greater risk of slow progress if you are overweight or have gained a lot of weight during the pregnancy, or if this is your first baby.
How is slow progress managed?
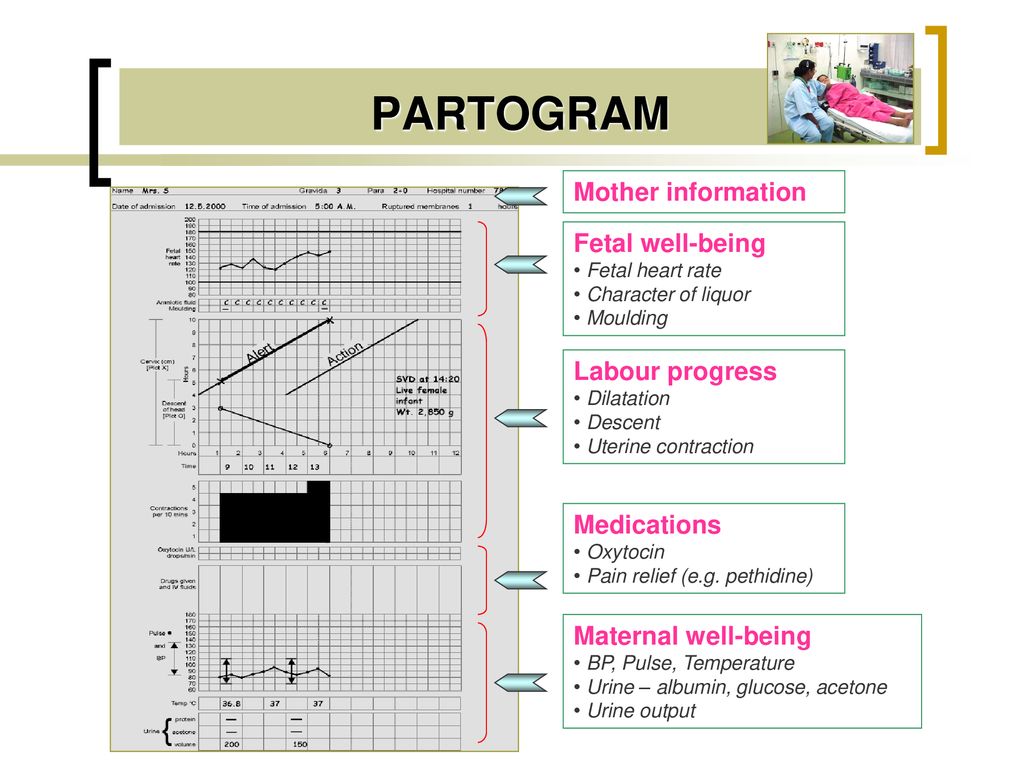
If you are experiencing slow progress, your midwife and doctor will monitor you closely. They will measure how quickly your cervix is dilating, how long your contractions last and how often you are having them. They will also continuously monitor the baby’s heart rate.
If you are in the first stage of labour, your midwife and doctor may decide to break your waters or give you the medication oxytocin to speed up your contractions or make them stronger. You will probably be given pain medication and asked to change position, which might speed things up.
If your baby has already entered the birth canal, your doctor or midwife might deliver them by using forceps or ventouse. If the baby is in distress, you may give birth by emergency caesarean.
What are the risks of slow progress?
Slow progress in labour can cause injury to both the mother and the baby.
If your doctor uses either forceps or ventouse to help you have your baby, there is a risk they may have some swelling or marks on their head, but these usually fade quite quickly.
If meconium is found in the amniotic fluid, your baby may have difficulty breathing when they are born and may require special care. Meconium is your baby’s first poo and is very sticky and tar-like. Babies usually have their first poo after they are born, but some babies who are stressed during delivery pass meconium when they are still in the womb and can inhale it.
Low oxygen levels or an abnormal heart rate might also require your baby to need have special care after the birth.
Assisted delivery can also result in injury to the mother. Most injuries will be temporary and will heal over time, but occasionally the injury can be more long lasting and may require further treatment.
Your medical team may recommend an emergency caesarean if other interventions don’t work. As with any type of surgery, there are some risks, but a caesarean is usually the safest option if you or your baby are at risk.
You won’t necessarily experience slow progress in your next pregnancy. Every pregnancy is different. If you’re worried about future pregnancies, however, it can help to talk to your doctor or midwife so they can explain what happened.
Every pregnancy is different. If you’re worried about future pregnancies, however, it can help to talk to your doctor or midwife so they can explain what happened.
Women whose labour didn’t go to plan can sometimes feel quite negative about their birth experience. They can feel stressed and experience anxiety about future motherhood. If you feel sad, disappointed or traumatised about what happened to you, it’s important to talk to someone. Those you might want to consider contacting include:
- Your doctor
- PANDA on 1300 726 306
- Australasian Birth Trauma Association
- Beyond Blue on 1300 22 4636
- Call Pregnancy, Birth and Baby to speak to a maternal child health nurse on 1800 882 436
Sources:
Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Labour and birth), Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Provision of routine intrapartum care in the absence of pregnancy complications), BMC Pregnancy and Childbirth (Diverse definitions of prolonged labour and its consequences with sometimes subsequent inappropriate treatment), WebMD (Prolonged labour), Medscape (Abnormal labor), Birth (The effect of medical and operative birth interventions on child health outcomes in the first 28 days and up to 5 years of age)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: January 2020
Back To Top
Related pages
- Labour complications
- Interventions during labour
- Induced labour
- Giving birth - stages of labour
Need more information?
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Tips for Labor Progress - Spinning Babies
If labor is progressing on its own, don’t try and make it progress more. It is distracting and leads you away from your natural process.
If, on the other hand, labor is not progressing well on its own, and one of the following is occurring:
- Labor seems to start and stop, or just doesn’t pick up at all
- Labor pauses unexpectedly in the middle
- Contractions are strong without bringing any dilation
You may greatly benefit from some of the following suggestions.
Pre-Labor
(Contractions are irregular and last roughly 20-40 seconds, but are inconsistent.)When the baby isn’t fitting well, these contractions can be 60-120 seconds with no dilation. One sign can be that the labor pattern is erratic, but just don’t make an assumption. It can be difficult to tell this situation from a transition without a vaginal exam. See Comparing OA and OP Labor Patterns for more details.
In this phase, the following things can really help:
- Relax the abdomen with Rebozo sifting.
- Sit smart, with your back straight or a little forward to help the baby settle in the front of your abdomen.
- Abdominal and sacral releases
- Acupressure and acupuncture
- Chiropractic adjustment
- Warm chamomile tea
- Plenty of laughter and love!
Try and go about your day as normally as you can. Take a nap (but don’t forget to Rest Smart).
Take a nap (but don’t forget to Rest Smart).
Is your abdominal wall loose? Does your uterus hang forward and make a crease underneath at the front of your panty line? Then use a pregnancy belt or a Rebozo to lift your uterus and allow the baby to come down on your cervix. Wear it until the baby is out to prevent a stall in labor after the head is born. Check-in with your provider(s) if any special needs present themselves.
Early Labor
(Contractions are regular and last 20-45 seconds with a frequency of 4-10 minutes apart. Things may begin to get bloody at this stage, which is normal.)In this early stage, the following tips can help:
- Relax the abdomen with the same things listed above in Pre-Labor.
- Maintain your regular daily routine. (Take into special consideration if your water broke.)
- Eat every two hours and drink lots of water, electrolyte drinks, and/or a little grape juice or hibiscus tea (for example) every hour.
- Rest Smart when you’re tired.
- Get up and walk or slow dance. Get down on your hands and knees and “wash the floor.”
- Use gravity to your advantage with the Abdominal Lift.
- Kneel over the back of a couch or hospital bed. Or, kneel on pillows and rest your arms in a comfy chair.
- Try some lively hula-hoop circles on the Birth Ball for 20 minutes.
- Stand and lean forward in the shower if sitting is too painful. Do some pelvic circles while standing.
- Check-in with your provider(s) to let them know your potential for labor. If you have a doula, call them! Doula-supported labors are statistically proven to be shorter than labors without one.

Active Labor I
(Beginning around 4 cm dilation. Contractions last 60-75 seconds with a frequency of 3-6 minutes apart.)In this phase, the following advice can help:
- You may want quiet, dark privacy.
- Continue to Rest Smart when tired and use the relaxation methods above. Massage between contractions as well.
- Do more Rebozo sifting for serious relaxation.
- Walking can help contractions continue to come.
- Be sure to eat!
- Do more circles on the birth ball.
- Continue to lunge for one-sided pain.
- Try an inversion of one type or another (your preference).
- Then, do the Trochanter Roll (Walcher’s Maneuver) if the baby isn’t in the brim before now.
Are you confined to bed?
Some providers persuade or direct all their moms to stay in bed during labor. Sometimes a woman’s health is such that she has to stay in bed.
If this is the case, try the following techniques to help:
- Keep rotating the pelvis.
- Lay on your left side with a pillow between your knees, or lift your right knee high up on a stack of pillows and shift your left hip back behind you so your belly aims into the mattress. Use pillows to support what needs support. Switch to your right side and try each of the different variations.
- If you can kneel and lean over a birthing ball or the raised head of the bed, do so for 30 minutes between sides.
 Change positions every 30 minutes.
Change positions every 30 minutes. - If your labor starts progressing rapidly, don’t worry too much about position changes for the purpose of labor progress. If labor doesn’t continue to progress, try to keep your back straight, not curled.
Active Labor II
(Beginning around 5 cm dilation. Contractions last 60-85 seconds with a frequency of 3-5 minutes apart.)If you can cope through 5 cm, you’re likely to have a natural birth! Continue to follow these tips:
- Relax your involuntary muscles as described before. Or, if you have a loose, pendulous womb, wear a pregnancy belt during your entire labor.
- Rest Smart℠ when tired.
- At any time during active labor (through the next three described phases), you can:
- 1.
 ) Do a sacral release
) Do a sacral release - 2.) Do the inversion through three contractions
- 3.) Do a pelvic floor release
- 1.
- Afterward, you will probably want to sink in a full tub or take a warm shower to mentally relax after those three techniques, which can be rather challenging this far into labor, but amazingly effective.
- Abdominal lift and tuck as before to take advantage of gravity. Do this for 10 contractions in a row, resting in between.
- Lunge for 6 contractions on each side. I like to do 3 contractions on one side, then switch knees and repeat, rather than all 6 on one side.
- Stand and hang onto your partner’s neck, or onto a sheet thrown over the bathroom door.
 (Tie a knot in one end and throw the knot over the door, then shut the door with the knot on the other side. Now the sheet won’t slip off the door and you can hang on and bend your knees and move to the contractions.)
(Tie a knot in one end and throw the knot over the door, then shut the door with the knot on the other side. Now the sheet won’t slip off the door and you can hang on and bend your knees and move to the contractions.) - Lift one hip and put one foot up. For instance, when sitting on the toilet, put one foot on a stool (or anything of a similar height) for three contractions. Stand for one with your other foot up on something. Then sit for three, stand for one, and repeat.
- Slow dance or slow dance in the shower while your partner sprays your back with a warm stream of water from the shower hose.
Active Labor III
(Dilation has advanced to 6-8 cm. Contractions last 60-85 seconds with a frequency of 3-4 minutes apart.)If you’re not at your birth site yet, now is a good time to go! Once there, continue to follow these tips:
- Balance as before, then relax the throat by “cooing.
 ” Deep, low tones are usually better than high-pitched ones.
” Deep, low tones are usually better than high-pitched ones. - Lots of moms like to be low to the ground, as they feel grounded with their knees deeply bent. Try kneeling on the floor while leaning forward, for example.
- Need to speed things up? Sit on a toilet for three contractions, then stand for three, and then sit for three again.
- Birth balls are rarely desired this late in labor, but if you’re up for it, give it a try.
- Lunge if you haven’t before, or try again for three contractions on each side and repeat.
- Walking can still be helpful, but may not be practical.
- Put one foot up on something when standing. Have your knee out diagonally and a foot on a stool (or other item).

- You will know what you need as your body feels progress. If you feel lost or frustrated, return to a calm state and do a Side-lying Release on both sides, followed by shake the apple tree.
- Make the pelvis open on one side by putting one foot on a stool. (Or, anything else you happen to have handy!)
Active Labor IV
(Dilation increases to 8-10 cm. Contractions last 75-120 seconds with a frequency of 2.5-4 minutes apart. Likely to be plenty of blood present now.)In this stage, the following tips can help:
- Continue balancing as before. Inversions are a common success for the stall in posterior labor.
- Use of a doula or face-to-face support is commonly appreciated.
- Loud moaning to a rhythm and a cool cloth can also help.
- Stand and lean forward to utilize gravity.
- Continue to Rest Smart℠ when in bed.
- Stand and hang on to the Rebozo or give a squat bar a try through 3-6 contractions.
- Lunge, holding a Rebozo or a sheet and straightening the back. Bend your knees with contractions and move freely.
- Is the baby still too high? Try another Trochanter Roll with Walcher’s Maneuver.
- Follow that up with a side-lying pelvic floor release.
Pushing or Releasing
(The second stage has begun. Contractions are now 45-75 seconds long with a frequency of 3-5 minutes.)In this final stage, the following advice can help:
- Be upright, with your back long and extended—don’t curl your back! When labor is not progressing readily, let your back be straight the way it naturally wants to lengthen.
- Sit up on a toilet (the porcelain birthing stool), lay on your side with your back arched instinctually, or stand and lift your arms to hang onto something sturdy above you.
- Relax as best you can in between contractions. Let the contraction get started before pushing voluntarily. If you need to push, use exhale pushing to conserve your strength and mental stamina. At the end of each contraction, take several deep cleansing breaths. Smile and feel the joy.
- Make deep vocalizations, vowel sounds, or roaring as desired.
- Kiss your partner.
- Know that your baby is helping you by pressing that pain out of your body. Work as a team. Let the baby rock back and forth in your pelvis. This relaxes the tissues in the perineum.
- Use vertical positions or side-lying on the bed to open the pelvis.
- Do some “towel pull” squats for 3-6 contractions.
- Use a hot washcloth on the perineum, and a cold, wet washcloth on the anus to prevent or soothe hemorrhoids.
- Rock forward and back while kneeling and leaning over a birth ball or the raised head of the bed.
- Keep lunging if the baby is asynclitic.
Childbirth is not progressing. The most comprehensive guide to a healthy pregnancy from top OB/GYNs
Labor does not progress
If the birth does not progress as it should, this phenomenon is called dystocia - it means that something is wrong with one of the components of the birth process. The progress of labor is measured by the degree of dilatation of the cervix and the descent of the baby in the pelvic area. This requires the following:
This requires the following:
• Regular and strong contractions.
• The size of the baby to pass through the pelvis and the correct position.
• The width of the pelvis, sufficient for the passage of the child.
If your contractions are not strong enough to open your cervix, you will be given medicine to make your uterus contract. Sometimes regular contractions suddenly stop in the middle of labor. If this happens and labor stops for several hours, the doctor may suggest rupturing the amniotic sac if it hasn't already, or inducing labor with oxytocin.
Problems during childbirth may include the following:
Protracted early stage of labor. This occurs if the cervix has not dilated to 3 cm despite regular contractions, after 20 hours if this is the first birth, and after 14 hours if the birth is not the first.
Sometimes progress is slow because it is not a real birth. You have false contractions that do not contribute to the opening of the cervix. Some pain medications used during labor can have the undesirable effect of slowing down the birth process, especially if taken too early.
Some pain medications used during labor can have the undesirable effect of slowing down the birth process, especially if taken too early.
Treatment . Whatever the reason, if your cervix hasn't dilated when you arrive at the hospital and your contractions aren't very strong, your doctor may suggest certain steps to speed up the delivery process. You may be asked to go back home and rest. Often, for a protracted first stage of labor, rest is the best medicine. You may be given some kind of sedative.
BABEL INTERVENTION
If labor is delayed or complications develop, medical intervention may be required. Tools - forceps or a vacuum extractor - can be used if the cervix is fully opened, the child has descended, but there are difficulties with his birth. Intervention may also be necessary if the baby's head is in the wrong position and may become stuck in the pelvic area. If the baby's heart is beating weakly and needs to be removed quickly, if you are too exhausted to continue pushing, labor can be expedited with forceps or a vacuum. This is the fastest and safest way to remove the baby.
This is the fastest and safest way to remove the baby.
Application of forceps . The tongs are shaped like two spoons connected like a lettuce spreader. They are gently inserted one by one into the vagina and cover the baby's head. When the uterus contracts and you push, the doctor carefully guides the baby through the birth canal, and he can come out at the next contraction.
Forceps are only used today if the baby's head is well down and close to the exit from the pelvis. If the head is not down enough, a caesarean section may be needed.
Vacuum application . Vacuum may be used instead of forceps if the baby's head has sunk into the pelvis. A rubber or plastic cap is placed over the baby's head, the suction is turned on, and the doctor gently guides the baby through the birth canal as the mother pushes. The vacuum extractor takes up less space than forceps and causes less trauma to the mother. But for a child, its use is somewhat more risky.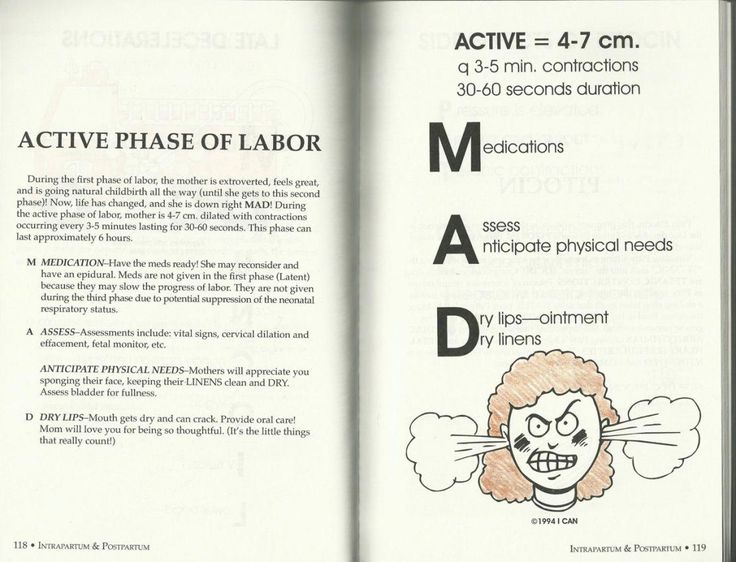
What to expect . This delivery is short, but it will take 30-45 minutes to get you ready for the procedure. You will need an epidural or spinal anesthetic and a catheter to empty your bladder. Incisions may be made to widen the vagina to make it easier for the baby to come out.
Tools to help the baby exit are very important and generally safe. Be aware that forceps can leave abrasions and red marks on the baby's head. The vacuum device may leave an abrasion or bump on the top of the head and hematomas under the scalp. The abrasions will disappear in about a week. Bump and redness - after a few days. In any case, serious damage is rare.
The decision whether to use forceps or a vacuum is best left to your doctor. Experience in using tools is the best guarantee against complications.
Prolonged active labor. The early stage of labor may go smoothly, but the process will slow down during the active phase. Labor is considered prolonged if the cervix does not dilate by about 1 cm within an hour after dilatation has reached 4-5 cm. The process may go on, but too slowly or stop altogether. Abrupt termination of the process after good contractions may mean that the size of your pelvis does not match the size of the baby's head.
The process may go on, but too slowly or stop altogether. Abrupt termination of the process after good contractions may mean that the size of your pelvis does not match the size of the baby's head.
Treatment . If the active stage progresses, the doctor may leave your labor to continue naturally. You may be asked to walk or change position to help the process. If you have a prolonged labor, you may be given intravenous fluids to keep you hydrated.
However, if active labor hasn't progressed within a few hours, your doctor may administer oxytocin, rupture of the amniotic sac, or both to speed up the process. Sometimes this is enough to restart contractions and allow you to give birth without complications.
Prolonged attempts. Sometimes attempts to expel the baby through the birth canal are slow or ineffective, which drains the mother's strength. If this is the first child, pushing for more than three hours is usually considered protracted. If you already had children, attempts are considered prolonged for more than two hours.
If you already had children, attempts are considered prolonged for more than two hours.
Treatment . The doctor will evaluate how far into the birth canal the baby has passed and whether the problem can be corrected by changing the position of the head. If you still have the strength and the child does not show signs of distress, you may be allowed to continue pushing. Sometimes, if the baby has gone far enough, the head can be gently released with forceps or a vacuum (see Birth Intervention, p. 472). You may be asked to assume a reclining, squatting or all fours position to help push the baby out. If the baby is too high in the birth canal and other measures fail, a caesarean section may be necessary.
This text is an introductory fragment.
Childbirth
childbirth • Arrival at the hospital. • Periods of childbirth. • How twins are born. • Postures during childbirth. • Fear of childbirth. • Natural childbirth. Childbirth is the expulsion of the fetus and afterbirth from the uterus - the baby's place, membranes, umbilical cord. Normal childbirth usually occurs after 40 weeks
• Periods of childbirth. • How twins are born. • Postures during childbirth. • Fear of childbirth. • Natural childbirth. Childbirth is the expulsion of the fetus and afterbirth from the uterus - the baby's place, membranes, umbilical cord. Normal childbirth usually occurs after 40 weeks
12.5. Preterm birth
12.5. preterm birth Preterm births are those that occur at 28-37 weeks of gestation, and the fetal weight is from 1000 to 2500 g. However, at present, according to the definition of the World Health Organization (WHO), if the pregnancy is terminated at
How is childbirth
How is childbirth A woman's body prepares for childbirth throughout pregnancy. Hormones appear in the blood, the action of which on the uterus leads to its muscle contractions, as a result of which the cervix opens and the baby moves down. In soft tissues
In soft tissues
Childbirth
childbirth Childbirth (medical birth act, delivery, Geburl, accouchement, partus) - represent a physiological process that takes place with the help of the contractile activity of the uterus and the assistance of the abdominal press, and the fetus and its
Prematurity
preterm birth It is very important to know the main signs of preterm labor (spit three times and knock on wood) so that they cannot take anyone by surprise. Preterm labor occurs somewhat more often in the summer months, which, apparently, is explained by
Childbirth and vision
Childbirth and vision Do not ignore the examination by medical specialists. This is a very important step in monitoring a pregnant woman. It is specialists who can identify or exclude diseases that affect the course of pregnancy and childbirth. In the first and third trimester
In the first and third trimester
Partner births
Partner births Not every appearance of the father of the child within the walls of the maternity hospital can be called participation in childbirth. Many men are ready to accompany their wife only to the delivery room, that is, to be with her in the prenatal ward, while helping in everything. This option is also not allowed
Childbirth
childbirth Any woman in anticipation of childbirth experiences anxiety, even if the child is not the first. But, if you are aware of how they will proceed, this will give you self-confidence, help you overcome fear. During the nine months of pregnancy, a whopping
Alternative births
Alternative births Obstetrician-gynecologists, along with classical childbirth, when women give birth in the prone position, began to use "vertical childbirth". The classic position of the woman in labor lying down leads to the passivity of the woman and is not optimal in physiological
The classic position of the woman in labor lying down leads to the passivity of the woman and is not optimal in physiological
partus, us m - childbirth
partus, us m - childbirth Approximate pronunciation: parArtus.Z: The girl is just right for the DESK, And she has the second PARTUS. The thing is that this "aunt" Taught from childhood sex education. She's still in elementary school unable to read, Instilled gender roles And offered
Prematurity
preterm birth A pregnancy is considered full-term if delivery occurs between the 37th and 42nd week after the start of the last monthly cycle. Preterm labor - when contractions begin to open the cervix before the end of the 37th week. Babies born this early are often
Weak labor activity: causes, diagnosis, treatment
What is weakness in labor?
Cervical dilatation slows down and labor is delayed. This is a pathological course of childbirth, in which contractions do not increase over time, but weaken and become shorter, and the cervix opens too slowly or does not open at all. In recent years, many obstetricians believe that the diagnosis of "weak labor" is often unjustified, and most women are able to give birth without medical stimulation - they just need more time for this.
This is a pathological course of childbirth, in which contractions do not increase over time, but weaken and become shorter, and the cervix opens too slowly or does not open at all. In recent years, many obstetricians believe that the diagnosis of "weak labor" is often unjustified, and most women are able to give birth without medical stimulation - they just need more time for this.
Causes of weakness of labor activity
- insufficient readiness of the body for childbirth;
- past inflammatory diseases of the genital organs, abortions;
- obesity;
- various complications of pregnancy;
- woman's fatigue during childbirth.
- Often, weakness complicates childbirth, which began after prolonged (for several days) pain in the lower abdomen, accompanied by irregular contractions, which leads to severe fatigue of the woman (pathological preliminary period).
Diagnosis and treatment of weakness of labor
Weakness of labor can be detected on the basis of the study of the nature of contractions, according to the results of the examination - the absence of cervical dilatation, and according to monitoring monitoring of the strength of contractions.
Treatment depends on the identified causes. Women in labor are allowed to rest, painkillers, sedatives and hypnotics are administered. After a few hours of sleep, women usually develop a good labor activity.
If labor does not intensify, then drugs are administered intravenously that increase uterine contractions (oxytocin, prostaglandins) - labor is stimulated. The introduction of drugs is carried out against the background of anesthesia, more often epidural anesthesia, and under careful monitoring of the condition of the fetus.
If labor does not increase within a few hours, then a caesarean section is performed.
References
- Westeneng HJ., van Veenhuijzen K., van der Spek RA., Peters S., Visser AE., van Rheenen W., Veldink JH., van den Berg LH. Associations between lifestyle and amyotrophic lateral sclerosis stratified by C9orf72 genotype: a longitudinal, population-based, case-control study. // Lancet Neurol - 2021 - Vol20 - N5 - p.373-384; PMID:33894192
- Xu A.
 , Sun C., Metcalf R., Limaye V. Health-related quality of life and work impairment in idiopathic inflammatory myopathies in South Australia. // Int J Rheum Dis - 2021 - Vol - NNULL - p.; PMID:33881230
, Sun C., Metcalf R., Limaye V. Health-related quality of life and work impairment in idiopathic inflammatory myopathies in South Australia. // Int J Rheum Dis - 2021 - Vol - NNULL - p.; PMID:33881230 - Luo J., Zhang D., Tang W., Dou LY., Sun Y. Impact of Frailty on the Risk of Exacerbations and All-Cause Mortality in Elderly Patients with Stable Chronic Obstructive Pulmonary Disease. // Clin Interv Aging - 2021 - Vol16 - NNULL - p.593-601; PMID:33880018
- Harrison CA., Parks RM., Cheung KL. The impact of breast cancer surgery on functional status in older women - A systematic review of the literature. // Eur J Surg Oncol - 2021 - Vol - NNULL - p.; PMID:33875285
- Coleman SA., Cunningham CJ., Murphy N., Feaheny J., Robinson D., Lannon R., McCarroll K., Casey M., Harbison J., Horgan NF. Progressive resistance training in a post-acute, older, inpatient setting: A randomized controlled feasibility study. // J Frailty Sarcopenia Falls - 2021 - Vol6 - N1 - p.14-24; PMID:33817447
- Espinoza G.