Ivf pregnancy process
In vitro fertilization (IVF) - Mayo Clinic
Overview
In vitro fertilization
In vitro fertilization
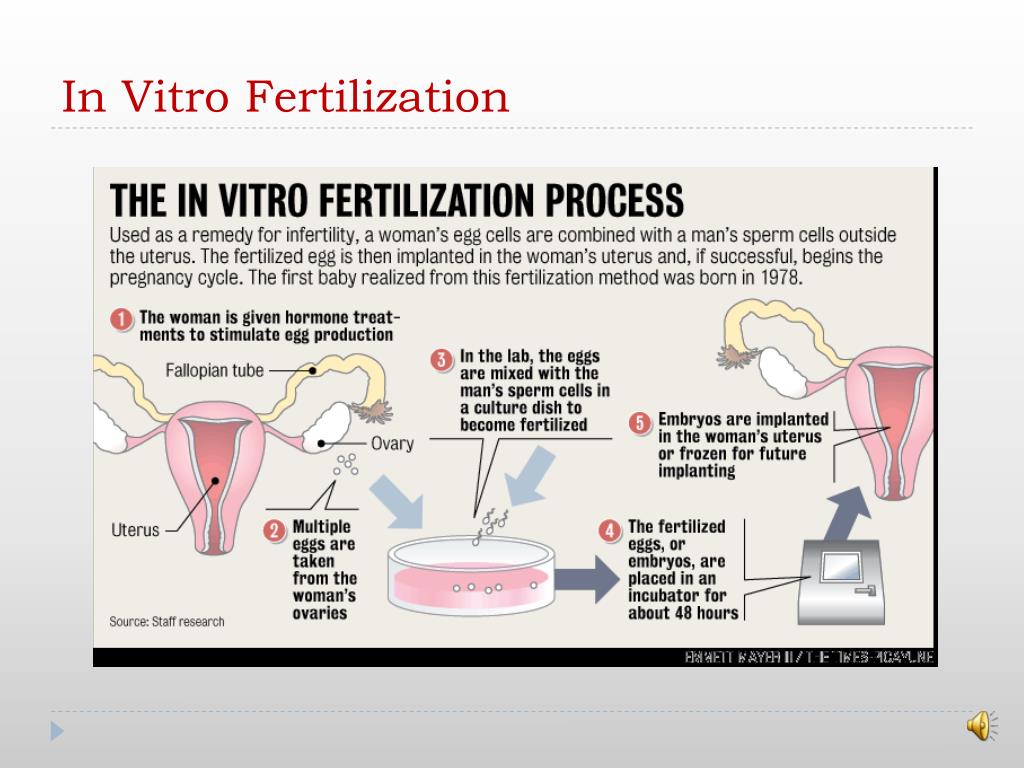
During in vitro fertilization, eggs are removed from mature follicles within an ovary (A). An egg is fertilized by injecting a single sperm into the egg or mixing the egg with sperm in a petri dish (B). The fertilized egg (embryo) is transferred into the uterus (C).
In vitro fertilization (IVF) is a complex series of procedures used to help with fertility or prevent genetic problems and assist with the conception of a child.
During IVF, mature eggs are collected (retrieved) from ovaries and fertilized by sperm in a lab. Then the fertilized egg (embryo) or eggs (embryos) are transferred to a uterus. One full cycle of IVF takes about three weeks. Sometimes these steps are split into different parts and the process can take longer.
IVF is the most effective form of assisted reproductive technology. The procedure can be done using a couple's own eggs and sperm. Or IVF may involve eggs, sperm or embryos from a known or anonymous donor. In some cases, a gestational carrier — someone who has an embryo implanted in the uterus — might be used.
Your chances of having a healthy baby using IVF depend on many factors, such as your age and the cause of infertility. In addition, IVF can be time-consuming, expensive and invasive. If more than one embryo is transferred to the uterus, IVF can result in a pregnancy with more than one fetus (multiple pregnancy).
Your doctor can help you understand how IVF works, the potential risks and whether this method of treating infertility is right for you.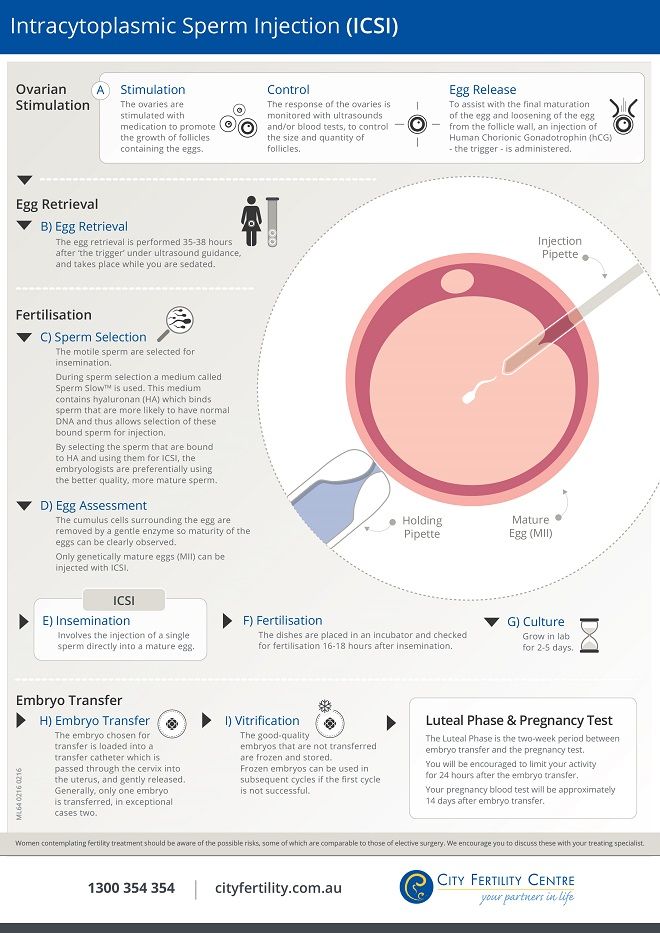
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Book: Mayo Clinic Guide to a Healthy Pregnancy
- Book: Mayo Clinic Guide to Fertility and Conception
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Why it's done
In vitro fertilization (IVF) is a treatment for infertility or genetic problems. If IVF is performed to treat infertility, you and your partner might be able to try less-invasive treatment options before attempting IVF, including fertility drugs to increase production of eggs or intrauterine insemination — a procedure in which sperm are placed directly in the uterus near the time of ovulation.
Sometimes, IVF is offered as a primary treatment for infertility in women over age 40. IVF can also be done if you have certain health conditions.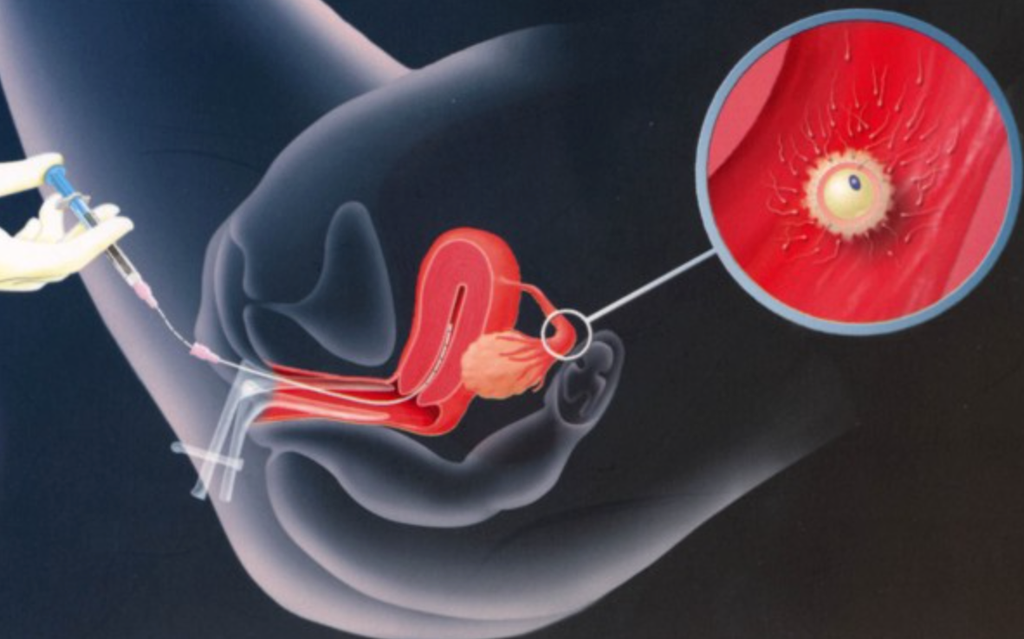 For example, IVF may be an option if you or your partner has:
For example, IVF may be an option if you or your partner has:
- Fallopian tube damage or blockage. Fallopian tube damage or blockage makes it difficult for an egg to be fertilized or for an embryo to travel to the uterus.
- Ovulation disorders. If ovulation is infrequent or absent, fewer eggs are available for fertilization.
- Endometriosis. Endometriosis occurs when tissue similar to the lining of the uterus implants and grows outside of the uterus — often affecting the function of the ovaries, uterus and fallopian tubes.
- Uterine fibroids. Fibroids are benign tumors in the uterus. They are common in women in their 30s and 40s. Fibroids can interfere with implantation of the fertilized egg.
- Previous tubal sterilization or removal. Tubal ligation is a type of sterilization in which the fallopian tubes are cut or blocked to permanently prevent pregnancy.
 If you wish to conceive after tubal ligation, IVF may be an alternative to tubal ligation reversal surgery.
If you wish to conceive after tubal ligation, IVF may be an alternative to tubal ligation reversal surgery. - Impaired sperm production or function. Below-average sperm concentration, weak movement of sperm (poor mobility), or abnormalities in sperm size and shape can make it difficult for sperm to fertilize an egg. If semen abnormalities are found, a visit to an infertility specialist might be needed to see if there are correctable problems or underlying health concerns.
- Unexplained infertility. Unexplained infertility means no cause of infertility has been found despite evaluation for common causes.
- A genetic disorder. If you or your partner is at risk of passing on a genetic disorder to your child, you may be candidates for preimplantation genetic testing — a procedure that involves IVF. After the eggs are harvested and fertilized, they're screened for certain genetic problems, although not all genetic problems can be found.
 Embryos that don't contain identified problems can be transferred to the uterus.
Embryos that don't contain identified problems can be transferred to the uterus. -
Fertility preservation for cancer or other health conditions. If you're about to start cancer treatment — such as radiation or chemotherapy — that could harm your fertility, IVF for fertility preservation may be an option. Women can have eggs harvested from their ovaries and frozen in an unfertilized state for later use. Or the eggs can be fertilized and frozen as embryos for future use.
Women who don't have a functional uterus or for whom pregnancy poses a serious health risk might choose IVF using another person to carry the pregnancy (gestational carrier). In this case, the woman's eggs are fertilized with sperm, but the resulting embryos are placed in the gestational carrier's uterus.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.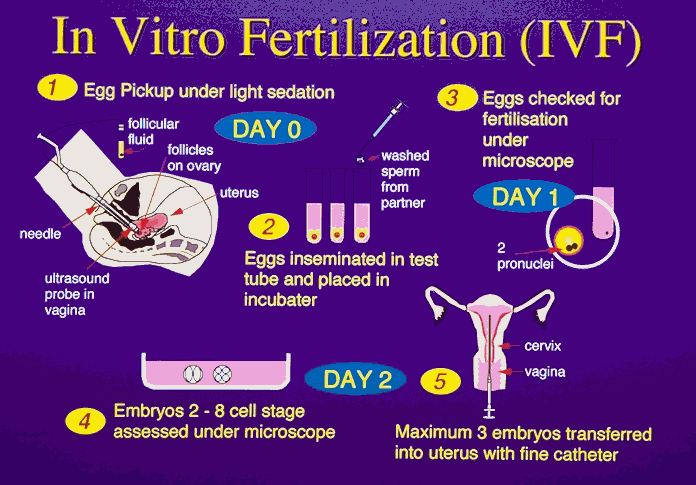
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Risks
Risks of IVF include:
- Multiple births.
 IVF increases the risk of multiple births if more than one embryo is transferred to your uterus. A pregnancy with multiple fetuses carries a higher risk of early labor and low birth weight than pregnancy with a single fetus does.
IVF increases the risk of multiple births if more than one embryo is transferred to your uterus. A pregnancy with multiple fetuses carries a higher risk of early labor and low birth weight than pregnancy with a single fetus does. - Premature delivery and low birth weight. Research suggests that IVF slightly increases the risk that the baby will be born early or with a low birth weight.
-
Ovarian hyperstimulation syndrome. Use of injectable fertility drugs, such as human chorionic gonadotropin (HCG), to induce ovulation can cause ovarian hyperstimulation syndrome, in which your ovaries become swollen and painful.
Symptoms typically last a week and include mild abdominal pain, bloating, nausea, vomiting and diarrhea. If you become pregnant, however, your symptoms might last several weeks. Rarely, it's possible to develop a more severe form of ovarian hyperstimulation syndrome that can also cause rapid weight gain and shortness of breath.

- Miscarriage. The rate of miscarriage for women who conceive using IVF with fresh embryos is similar to that of women who conceive naturally — about 15% to 25% — but the rate increases with maternal age.
- Egg-retrieval procedure complications. Use of an aspirating needle to collect eggs could possibly cause bleeding, infection or damage to the bowel, bladder or a blood vessel. Risks are also associated with sedation and general anesthesia, if used.
- Ectopic pregnancy. About 2% to 5% of women who use IVF will have an ectopic pregnancy — when the fertilized egg implants outside the uterus, usually in a fallopian tube. The fertilized egg can't survive outside the uterus, and there's no way to continue the pregnancy.
- Birth defects. The age of the mother is the primary risk factor in the development of birth defects, no matter how the child is conceived.
 More research is needed to determine whether babies conceived using IVF might be at increased risk of certain birth defects.
More research is needed to determine whether babies conceived using IVF might be at increased risk of certain birth defects. - Cancer. Although some early studies suggested there may be a link between certain medications used to stimulate egg growth and the development of a specific type of ovarian tumor, more-recent studies do not support these findings. There does not appear to be a significantly increased risk of breast, endometrial, cervical or ovarian cancer after IVF.
- Stress. Use of IVF can be financially, physically and emotionally draining. Support from counselors, family and friends can help you and your partner through the ups and downs of infertility treatment.
How you prepare
The Centers for Disease Control and Prevention and the Society for Assisted Reproductive Technology provide information online about U. S. clinics' individual pregnancy and live birth rates.
S. clinics' individual pregnancy and live birth rates.
A clinic's success rate depends on many factors. These include patients' ages and medical issues, as well as the clinic's treatment population and treatment approaches. Ask for detailed information about the costs associated with each step of the procedure.
Before beginning a cycle of IVF using your own eggs and sperm, you and your partner will likely need various screenings, including:
- Ovarian reserve testing. To determine the quantity and quality of your eggs, your doctor might test the concentration of follicle-stimulating hormone (FSH), estradiol (estrogen) and anti-mullerian hormone in your blood during the first few days of your menstrual cycle. Test results, often used together with an ultrasound of your ovaries, can help predict how your ovaries will respond to fertility medication.
- Semen analysis. If not done as part of your initial fertility evaluation, your doctor will conduct a semen analysis shortly before the start of an IVF treatment cycle.
- Infectious disease screening. You and your partner will both be screened for infectious diseases, including HIV.
- Practice (mock) embryo transfer. Your doctor might conduct a mock embryo transfer to determine the depth of your uterine cavity and the technique most likely to successfully place the embryos into your uterus.
- Uterine exam. Your doctor will examine the inside lining of the uterus before you start IVF. This might involve a sonohysterography — in which fluid is injected through the cervix into your uterus — and an ultrasound to create images of your uterine cavity. Or it might include a hysteroscopy — in which a thin, flexible, lighted telescope (hysteroscope) is inserted through your vagina and cervix into your uterus.
Before beginning a cycle of IVF, consider important questions, including:
-
How many embryos will be transferred? The number of embryos transferred is typically based on age and number of eggs retrieved.
 Since the rate of implantation is lower for older women, more embryos are usually transferred — except for women using donor eggs or genetically tested embryos.
Since the rate of implantation is lower for older women, more embryos are usually transferred — except for women using donor eggs or genetically tested embryos.Most doctors follow specific guidelines to prevent a higher order multiple pregnancy, such as triplets or more. In some countries, legislation limits the number of embryos that can be transferred. Make sure you and your doctor agree on the number of embryos that will be transferred before the transfer procedure.
-
What will you do with any extra embryos? Extra embryos can be frozen and stored for future use for several years. Not all embryos will survive the freezing and thawing process, although most will.
Having frozen embryos can make future cycles of IVF less expensive and less invasive. Or, you might be able to donate unused frozen embryos to another couple or a research facility. You might also choose to discard unused embryos.
- How will you handle a multiple pregnancy? If more than one embryo is transferred to your uterus, IVF can result in a multiple pregnancy — which poses health risks for you and your babies. In some cases, fetal reduction can be used to help a woman deliver fewer babies with lower health risks. Pursuing fetal reduction, however, is a major decision with ethical, emotional and psychological consequences.
- Have you considered the potential complications associated with using donor eggs, sperm or embryos, or a gestational carrier? A trained counselor with expertise in donor issues can help you understand the concerns, such as the legal rights of the donor. You may also need an attorney to file court papers to help you become legal parents of an implanted embryo.
What you can expect
IVF involves several steps — ovarian stimulation, egg retrieval, sperm retrieval, fertilization and embryo transfer. One cycle of IVF can take about two to three weeks. More than one cycle may be needed.
One cycle of IVF can take about two to three weeks. More than one cycle may be needed.
Ovulation induction
The start of an IVF cycle begins by using synthetic hormones to stimulate the ovaries to produce multiple eggs — rather than the single egg that typically develops each month. Multiple eggs are needed because some eggs won't fertilize or develop normally after fertilization.
Several different medications may be used, such as:
- Medications for ovarian stimulation. To stimulate your ovaries, you might receive an injectable medication containing a follicle-stimulating hormone (FSH), a luteinizing hormone (LH) or a combination of both. These medications stimulate more than one egg to develop at a time.
- Medications for oocyte maturation. When the follicles are ready for egg retrieval — generally after eight to 14 days — you will take human chorionic gonadotropin (HCG) or other medications to help the eggs mature.
- Medications to prevent premature ovulation. These medications prevent your body from releasing the developing eggs too soon.
- Medications to prepare the lining of your uterus. On the day of egg retrieval or at the time of embryo transfer, your doctor might recommend that you begin taking progesterone supplements to make the lining of your uterus more receptive to implantation.
Your doctor will work with you to determine which medications to use and when to use them.
Typically, you'll need one to two weeks of ovarian stimulation before your eggs are ready for retrieval. To determine when the eggs are ready for collection, you may have:
- Vaginal ultrasound, an imaging exam of your ovaries to monitor the development of follicles — fluid-filled ovarian sacs where eggs mature
- Blood tests, to measure your response to ovarian stimulation medications — estrogen levels typically increase as follicles develop, and progesterone levels remain low until after ovulation
Sometimes IVF cycles need to be canceled before egg retrieval for one of these reasons:
- Inadequate number of follicles developing
- Premature ovulation
- Too many follicles developing, creating a risk of ovarian hyperstimulation syndrome
- Other medical issues
If your cycle is canceled, your doctor might recommend changing medications or their doses to promote a better response during future IVF cycles.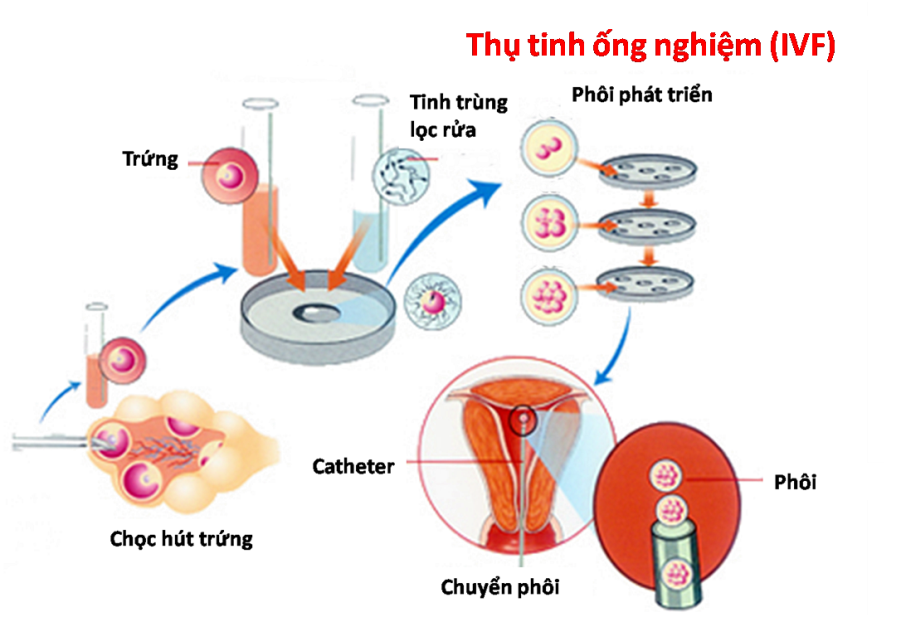 Or you may be advised that you need an egg donor.
Or you may be advised that you need an egg donor.
Egg retrieval
Egg retrieval can be done in your doctor's office or a clinic 34 to 36 hours after the final injection and before ovulation.
- During egg retrieval, you'll be sedated and given pain medication.
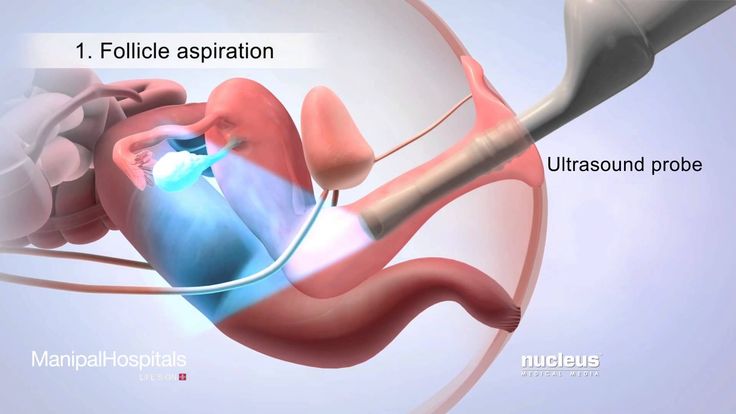
- Transvaginal ultrasound aspiration is the usual retrieval method. An ultrasound probe is inserted into your vagina to identify follicles. Then a thin needle is inserted into an ultrasound guide to go through the vagina and into the follicles to retrieve the eggs.
- If your ovaries aren't accessible through transvaginal ultrasound, an abdominal ultrasound may be used to guide the needle.
- The eggs are removed from the follicles through a needle connected to a suction device. Multiple eggs can be removed in about 20 minutes.
- After egg retrieval, you may experience cramping and feelings of fullness or pressure.
- Mature eggs are placed in a nutritive liquid (culture medium) and incubated.
 Eggs that appear healthy and mature will be mixed with sperm to attempt to create embryos. However, not all eggs may be successfully fertilized.
Eggs that appear healthy and mature will be mixed with sperm to attempt to create embryos. However, not all eggs may be successfully fertilized.
Sperm retrieval
If you're using your partner's sperm, a semen sample needs to be provided at your doctor's office or clinic the morning of egg retrieval. Typically, the semen sample is collected through masturbation. Other methods, such as testicular aspiration — the use of a needle or surgical procedure to extract sperm directly from the testicle — are sometimes required. Donor sperm also can be used. Sperm are separated from the semen fluid in the lab.
Fertilization
Fertilization can be attempted using two common methods:
- Conventional insemination. During conventional insemination, healthy sperm and mature eggs are mixed and incubated overnight.
- Intracytoplasmic sperm injection (ICSI). In ICSI, a single healthy sperm is injected directly into each mature egg.
 ICSI is often used when semen quality or number is a problem or if fertilization attempts during prior IVF cycles failed.
ICSI is often used when semen quality or number is a problem or if fertilization attempts during prior IVF cycles failed.
In certain situations, your doctor may recommend other procedures before embryo transfer.
- Assisted hatching. About five to six days after fertilization, an embryo "hatches" from its surrounding membrane (zona pellucida), allowing it to implant into the lining of the uterus. If you're an older woman, or if you have had multiple failed IVF attempts, your doctor might recommend assisted hatching — a technique in which a hole is made in the zona pellucida just before transfer to help the embryo hatch and implant. Assisted hatching is also useful for eggs or embryos that have been previously frozen as the process can harden the zona pellucida.
- Preimplantation genetic testing.
 Embryos are allowed to develop in the incubator until they reach a stage where a small sample can be removed and tested for specific genetic diseases or the correct number of chromosomes, typically after five to six days of development. Embryos that don't contain affected genes or chromosomes can be transferred to your uterus. While preimplantation genetic testing can reduce the likelihood that a parent will pass on a genetic problem, it can't eliminate the risk. Prenatal testing may still be recommended.
Embryos are allowed to develop in the incubator until they reach a stage where a small sample can be removed and tested for specific genetic diseases or the correct number of chromosomes, typically after five to six days of development. Embryos that don't contain affected genes or chromosomes can be transferred to your uterus. While preimplantation genetic testing can reduce the likelihood that a parent will pass on a genetic problem, it can't eliminate the risk. Prenatal testing may still be recommended.
Embryo transfer
Egg-retrieval technique
Egg-retrieval technique
Typically, transvaginal ultrasound aspiration is used to retrieve eggs. During this procedure, an ultrasound probe is inserted into your vagina to identify follicles, and a needle is guided through the vagina and into the follicles. The eggs are removed from the follicles through the needle, which is connected to a suction device.
ICSI
ICSI
In intracytoplasmic sperm injection (ICSI), a single healthy sperm is injected directly into each mature egg.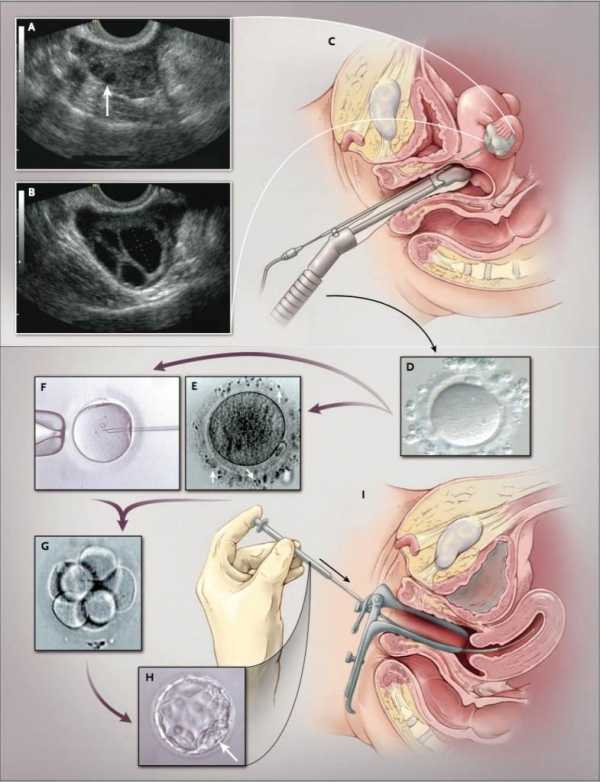 ICSI is often used when semen quality or number is a problem or if fertilization attempts during prior in vitro fertilization cycles failed.
ICSI is often used when semen quality or number is a problem or if fertilization attempts during prior in vitro fertilization cycles failed.
Blastocyst
Blastocyst
Three days after fertilization, a normally developing embryo will contain about six to 10 cells. By the fifth or sixth day, the fertilized egg is known as a blastocyst — a rapidly dividing ball of cells. The inner group of cells will become the embryo. The outer group will become the cells that nourish and protect it.
Embryo transfer is done at your doctor's office or a clinic and usually takes place two to five days after egg retrieval.
- You might be given a mild sedative. The procedure is usually painless, although you might experience mild cramping.
- The doctor will insert a long, thin, flexible tube called a catheter into your vagina, through your cervix and into your uterus.
- A syringe containing one or more embryos suspended in a small amount of fluid is attached to the end of the catheter.

- Using the syringe, the doctor places the embryo or embryos into your uterus.
If successful, an embryo will implant in the lining of your uterus about six to 10 days after egg retrieval.
After the procedure
After the embryo transfer, you can resume your usual daily activities. However, your ovaries may still be enlarged. Consider avoiding vigorous activity, which could cause discomfort.
Typical side effects include:
- Passing a small amount of clear or bloody fluid shortly after the procedure — due to the swabbing of the cervix before the embryo transfer
- Breast tenderness due to high estrogen levels
- Mild bloating
- Mild cramping
- Constipation
If you develop moderate or severe pain after the embryo transfer, contact your doctor. He or she will evaluate you for complications such as infection, twisting of an ovary (ovarian torsion) and severe ovarian hyperstimulation syndrome.
Results
About 12 days to two weeks after egg retrieval, your doctor will test a sample of your blood to detect whether you're pregnant.
- If you're pregnant, your doctor will refer you to an obstetrician or other pregnancy specialist for prenatal care.
- If you're not pregnant, you'll stop taking progesterone and likely get your period within a week. If you don't get your period or you have unusual bleeding, contact your doctor. If you're interested in attempting another cycle of in vitro fertilization (IVF), your doctor might suggest steps you can take to improve your chances of getting pregnant through IVF.
The chances of giving birth to a healthy baby after using IVF depend on various factors, including:
- Maternal age. The younger you are, the more likely you are to get pregnant and give birth to a healthy baby using your own eggs during IVF.
 Women age 41 and older are often counseled to consider using donor eggs during IVF to increase the chances of success.
Women age 41 and older are often counseled to consider using donor eggs during IVF to increase the chances of success. - Embryo status. Transfer of embryos that are more developed is associated with higher pregnancy rates compared with less-developed embryos (day two or three). However, not all embryos survive the development process. Talk with your doctor or other care provider about your specific situation.
- Reproductive history. Women who've previously given birth are more likely to be able to get pregnant using IVF than are women who've never given birth. Success rates are lower for women who've previously used IVF multiple times but didn't get pregnant.
- Cause of infertility. Having a normal supply of eggs increases your chances of being able to get pregnant using IVF.
 Women who have severe endometriosis are less likely to be able to get pregnant using IVF than are women who have unexplained infertility.
Women who have severe endometriosis are less likely to be able to get pregnant using IVF than are women who have unexplained infertility. - Lifestyle factors. Women who smoke typically have fewer eggs retrieved during IVF and may miscarry more often. Smoking can lower a woman's chance of success using IVF by 50%. Obesity can decrease your chances of getting pregnant and having a baby. Use of alcohol, recreational drugs, excessive caffeine and certain medications also can be harmful.
Talk with your doctor about any factors that apply to you and how they may affect your chances of a successful pregnancy.
Clinical trials
Explore Mayo Clinic studies of tests and procedures to help prevent, detect, treat or manage conditions.
By Mayo Clinic Staff
Related
Products & Services
What Is In-Vitro-Fertilization (IVF)?
In This Section
- Fertility Treatments
- What is IVF?
- What is IUI?
In vitro fertilization (IVF) helps with fertilization, embryo development, and implantation, so you can get pregnant.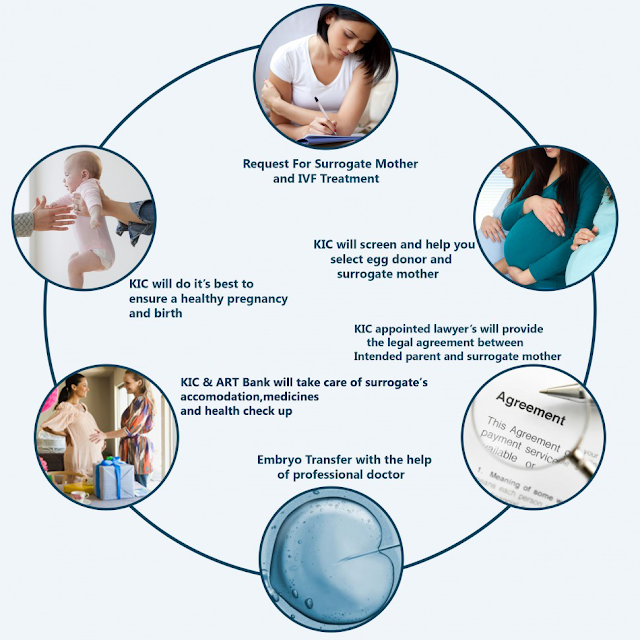
How does IVF work?
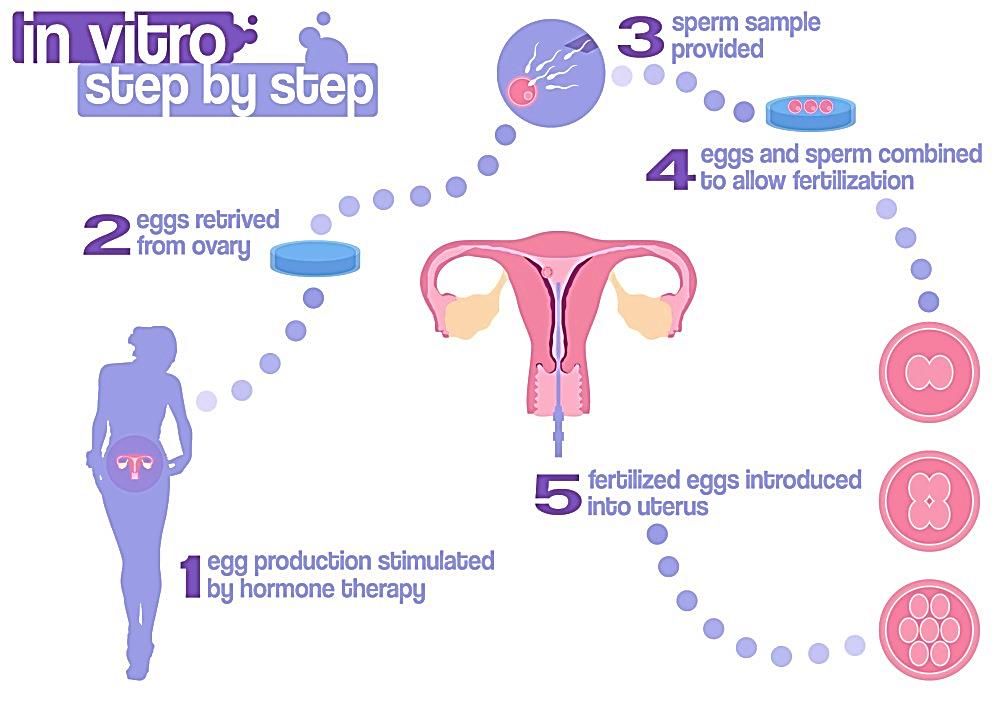
IVF stands for in vitro fertilization. It’s one of the more widely known types of assisted reproductive technology (ART). IVF works by using a combination of medicines and surgical procedures to help sperm fertilize an egg, and help the fertilized egg implant in your uterus.
First, you take medication that makes several of your eggs mature and ready for fertilization. Then the doctor takes the eggs out of your body and mixes them with sperm in a lab, to help the sperm fertilize the eggs. Then they put 1 or more fertilized eggs (embryos) directly into your uterus. Pregnancy happens if any of the embryos implant in the lining of your uterus.
IVF has many steps, and it takes several months to complete the whole process. It sometimes works on the first try, but many people need more than 1 round of IVF to get pregnant. IVF definitely increases your chances of pregnancy if you’re having fertility problems, but there’s no guarantee — everyone’s body is different and IVF won’t work for everyone.
What’s the IVF process?
The first step in IVF is taking fertility medications for several months to help your ovaries produce several eggs that are mature and ready for fertilization. This is called ovulation induction. You may get regular ultrasounds or blood tests to measure your hormone levels and keep track of your egg production.
Once your ovaries have produced enough mature eggs, your doctor removes the eggs from your body (this is called egg retrieval). Egg retrieval is a minor surgical procedure that’s done at your doctor’s office or at a fertility clinic.
You’ll get medicine to help you be relaxed and comfortable during the procedure. Using an ultrasound to see inside your body, the doctor puts a thin, hollow tube through your vagina and into the ovary and follicles that hold your eggs. The needle is connected to a suction device that gently pulls the eggs out of each follicle.
In a lab, your eggs are mixed with sperm cells from your partner or a donor — this is called insemination. The eggs and sperm are stored together in a special container, and fertilization happens. For sperm that have lower motility (don’t swim as well), they may be injected directly into the eggs to promote fertilization. As the cells in the fertilized eggs divide and become embryos, people who work at the lab monitor the progress.
The eggs and sperm are stored together in a special container, and fertilization happens. For sperm that have lower motility (don’t swim as well), they may be injected directly into the eggs to promote fertilization. As the cells in the fertilized eggs divide and become embryos, people who work at the lab monitor the progress.
About 3-5 days after the egg retrieval, 1 or more embryos are put into your uterus (this is called embryo transfer). The doctor slides a thin tube through your cervix into your uterus, and inserts the embryo directly into your uterus through the tube.
Pregnancy happens if any of the embryos attach to the lining of your uterus. Embryo transfer is done at your doctor’s office or at a fertility clinic, and it’s usually not painful.
Plan on resting for the rest of the day after your embryo transfer. You can go back to your normal activities the next day. You may also take pills or get daily shots of a hormone called progesterone for the first 8-10 weeks after the embryo transfer.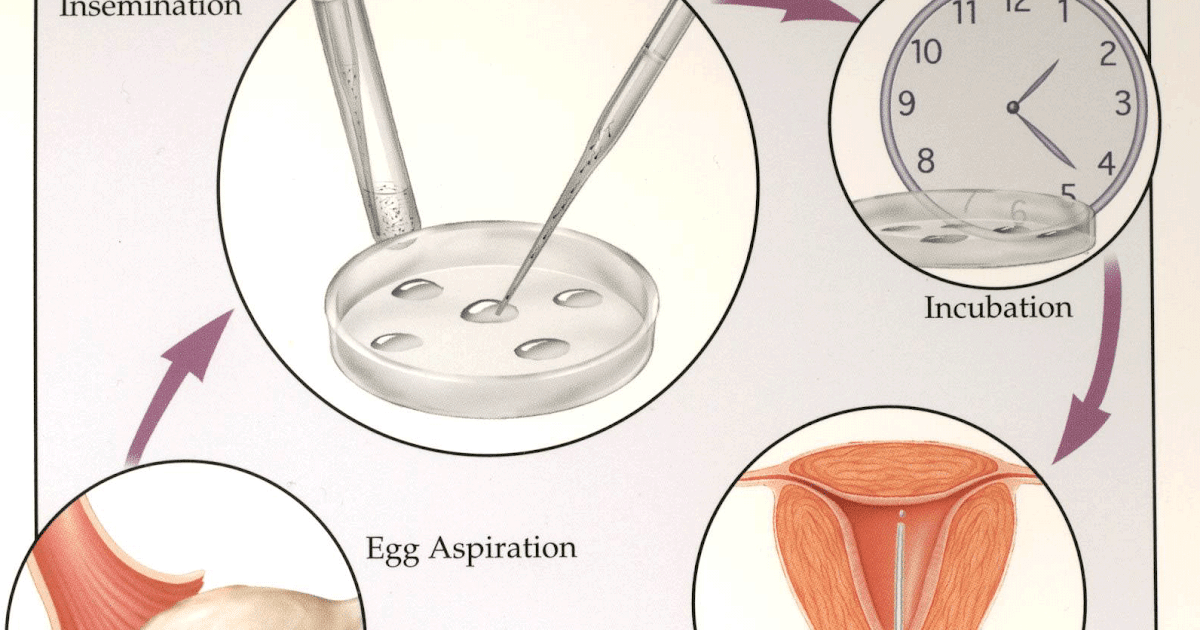 The hormones make it easier for the embryo to survive in your uterus.
The hormones make it easier for the embryo to survive in your uterus.
What are the side effects of IVF?
Like all medications and medical procedures, IVF has some risks and possible side effects. These include:
Your doctor can talk with you about any questions or concerns you have about IVF risks and side effects.
IVF can also be difficult emotionally, both for the person having the procedures and for their partner and/or family. Many people doing IVF treatments struggle with depression and anxiety throughout the process.
Talking with people who’ve been through fertility struggles and IVF can be really helpful if you’re feeling overwhelmed or discouraged. Online and in-person communities are also good places to meet people who understand what you’re going through and can offer advice and support. Counselors and therapists can also be sources of comfort.
You can find more information on support groups and coping with the stress of fertility treatments at RESOLVE: The National Infertility Association. Your doctor, fertility specialist, or local Planned Parenthood health center may also be able to offer you other resources and tips on finding therapists or support groups in your area.
Your doctor, fertility specialist, or local Planned Parenthood health center may also be able to offer you other resources and tips on finding therapists or support groups in your area.
How much does IVF cost?
IVF tends to be pretty expensive. A few states have laws that say health insurance companies must cover some or all of the costs of infertility treatment if you meet certain requirements. But many insurance plans don’t offer any fertility treatment coverage at all.
You can find more information about insurance coverage of IVF and other fertility treatments at The National Infertility Association.
The fees for 1 cycle of IVF include medicines, procedures, anesthesia, ultrasounds, blood tests, lab work, and embryo storage. The exact cost of a single IVF cycle varies, but it can be up to $15,000 or more.
Was this page helpful?- Yes
- No
Help us improve - how could this information be more helpful?
How did this information help you?
Please answer below.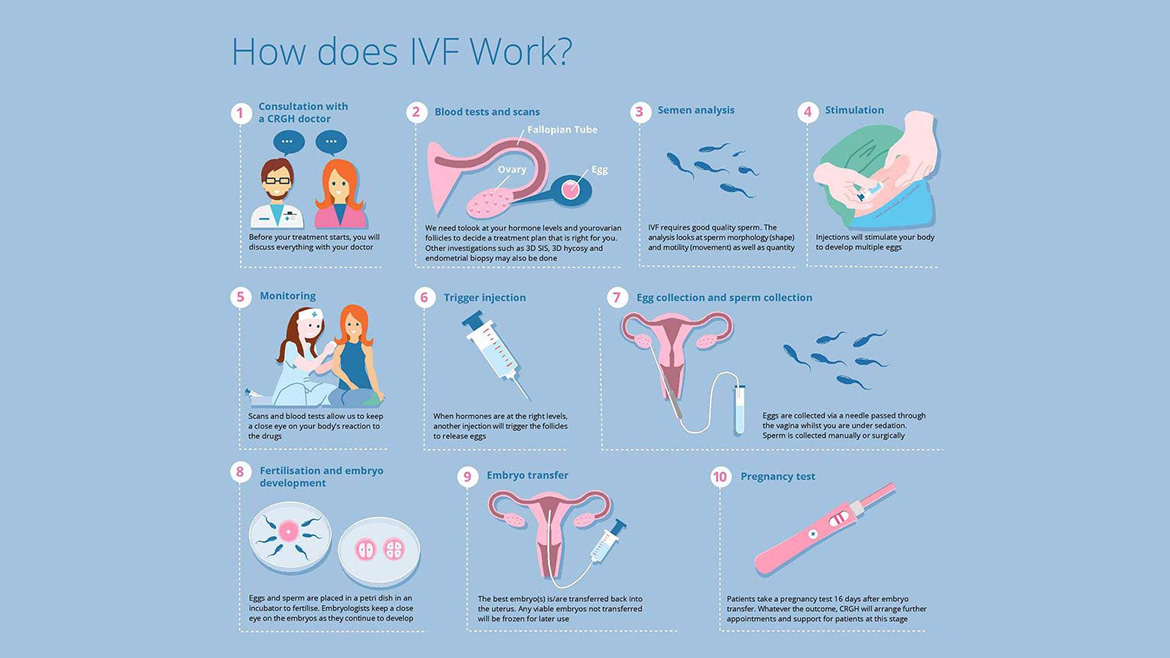
Are you human? (Sorry, we have to ask!)
Please don't check this box if you are a human.
You’re the best! Thanks for your feedback.
Thanks for your feedback.
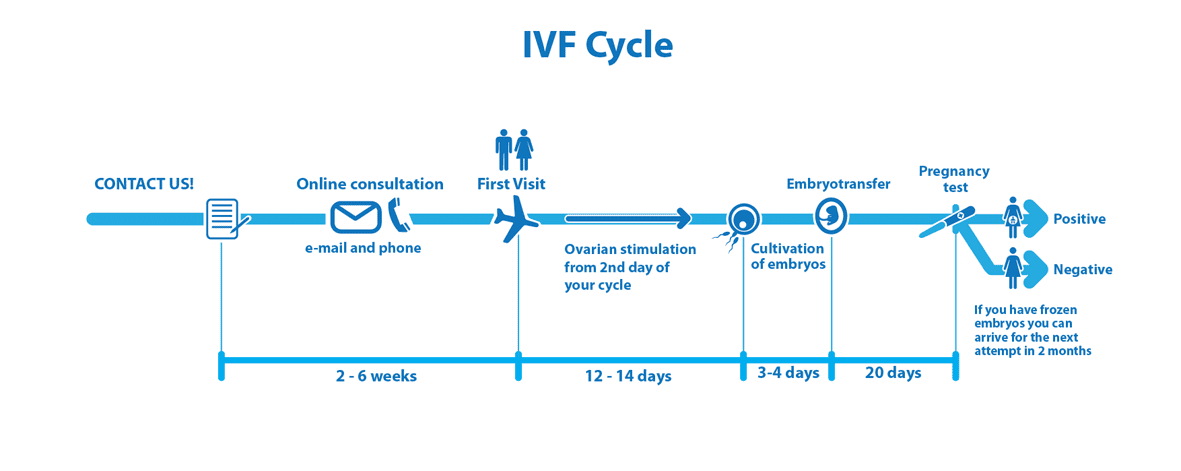
IVF procedure: all stages - from examination to confirmation of the fact of pregnancy
The first stage of IVF is a visit to a reproductive specialist - a doctor who specializes in the treatment of infertility.
The process of conception involves a man and a woman. If, as a result of sexual intimacy, pregnancy does not occur, then the reason for this may be both from the side of the man and from the side of the woman. Therefore, it is advisable to come to the reception together.
If pregnancy does not occur within 6-12 months of sexual life without contraception, then we can talk about infertility. Timely contacting a specialized clinic will solve the problem as efficiently as possible.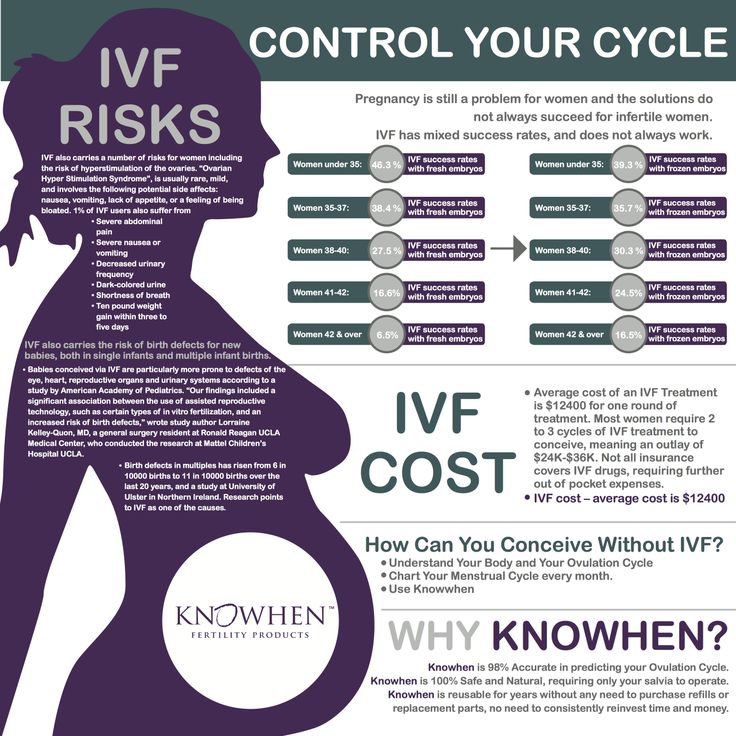
At the first appointment, the doctor will talk to the couple, take an anamnesis, examine the woman and assess her ovarian reserve using ultrasound. Then he will schedule an examination.
Basic examinations for women:
- Ultrasound of the pelvic organs
- Evaluation of the patency of the fallopian tubes
- Folliculometry
- Ultrasound of the thyroid gland (according to indications)
- Ultrasound of the mammary glands (according to indications)
- laboratory tests.
A man will definitely need to pass a spermogram and undergo an appointment with a urologist-andrologist. The results of complex diagnostics determine the indications for a particular treatment method. If there are indications for IVF, then the stage of preparation for the protocol begins.
The IVF protocol is a scheme that takes into account the sequence, duration, frequency and types of drugs administered, as well as their dosages.There are 2 main types of IVF protocols: short and long. There is also such a type of protocol as segmented with cryopreservation. To date, they are the most effective.
Quite often, before the IVF program, a woman is shown weight correction. Optimal body weight increases the effectiveness of the procedure.
So let's get into the protocol.
FIRST STAGE: superovulation stimulation
For this, a woman is prescribed special hormonal drugs. They cause the simultaneous maturation of several follicles in the ovaries, which increases the chances of pregnancy. One ovum matures in each follicle. Egg retrieval is carried out by puncture of the follicle.
Compliance with the exact schedule of injections of drugs is extremely important to obtain the result - a sufficient number of quality eggs. Therefore, be precise and obligatory, do not miss the scheduled dates and times of visits.
The first ultrasound monitoring after the start of the IVF program is usually carried out on the 5th or 6th day of superovulation stimulation.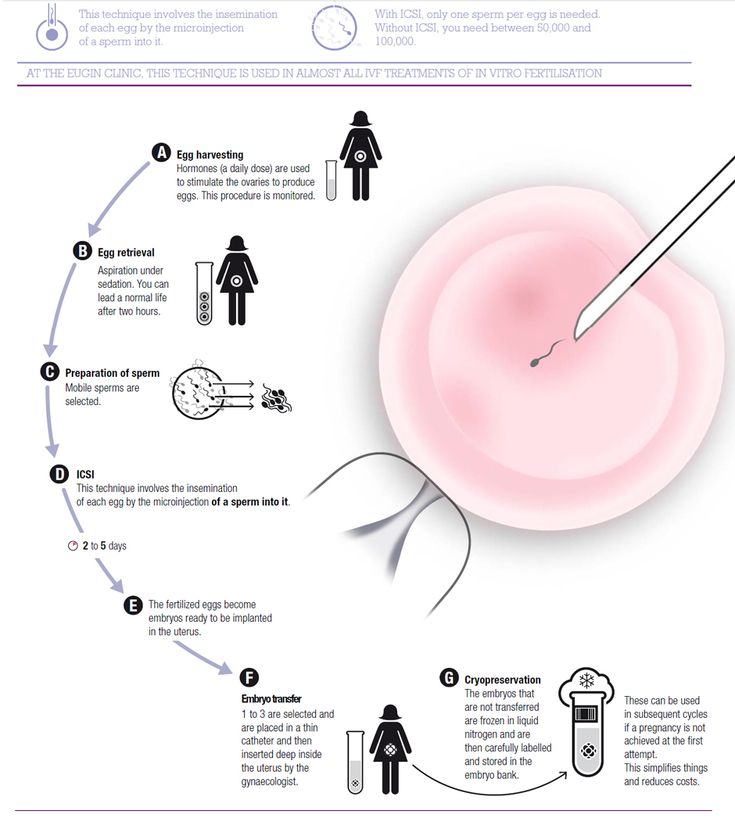 Its task is to assess the response of the ovaries (follicle growth dynamics) and the thickness of the endometrium (uterine lining). Before the active growth of follicles begins (until they reach a size of 10 mm or more), ultrasound is performed once every 4-5 days, then the ovaries are examined more often - once every 2-3 days.
Its task is to assess the response of the ovaries (follicle growth dynamics) and the thickness of the endometrium (uterine lining). Before the active growth of follicles begins (until they reach a size of 10 mm or more), ultrasound is performed once every 4-5 days, then the ovaries are examined more often - once every 2-3 days.
SECOND STAGE: follicle puncture
After the ovarian stimulation is completed, it is necessary to obtain eggs from the follicles. For this, a puncture is performed, 34-35 hours after the introduction of the trigger (hCG). The procedure takes place under ultrasound control in the operating room and under intravenous anesthesia, and lasts an average of 10-15 minutes.
After graduation, you will remain in the clinic under observation for at least 2 hours. Sperm collection is carried out on the same day and time as the puncture. In cases where it is impossible to use the cells of the parents, donor material comes to the rescue (IVF with a donor egg)
THIRD STAGE: egg fertilization and embryo culture
In the laboratory, after 3-4 hours, the embryologist fertilizes the received eggs with processed sperm. The day of the beginning of the cultivation of embryos is considered the next day after the puncture of the follicles.
The day of the beginning of the cultivation of embryos is considered the next day after the puncture of the follicles.
FERTILIZATION
It takes place in a Petri dish. In classical IVF, an egg is placed there and then specially processed sperm is added.
"Genome" mainly uses the ICSI method, in which the sperm is injected into the egg, which increases the likelihood of fertilization. PICSI is also used - an improved ICSI technique with additional selection of spermatozoa based on biochemical criteria.
Embryos obtained as a result of fertilization are cultivated up to 5-6 days, the blastocyst stage. They are then either transferred to the uterus or cryopreserved (frozen). To increase the chance of successful implantation, the shell of the embryo is sometimes thinned, a procedure called assisted hatching.
STAGE FOUR: Embryo Transfer
Technically, the embryo transfer procedure is quite simple and is carried out under ultrasound control, which allows you to track the course of the catheter with embryos. A set of embryos for transfer is carried out in the laboratory. Then the doctor exposes the cervix in the mirrors and inserts a catheter with embryos through the cervical canal into the uterine cavity. With the help of a syringe, the embryos are ''expelled'' from the catheter. Embryo transfer is the final stage of the IVF program. In "Genome" one embryo is usually transferred to the uterus, this tactic avoids the complications of multiple pregnancy.
A set of embryos for transfer is carried out in the laboratory. Then the doctor exposes the cervix in the mirrors and inserts a catheter with embryos through the cervical canal into the uterine cavity. With the help of a syringe, the embryos are ''expelled'' from the catheter. Embryo transfer is the final stage of the IVF program. In "Genome" one embryo is usually transferred to the uterus, this tactic avoids the complications of multiple pregnancy.
HCG blood test
A test indicating the onset of pregnancy is carried out 10-14 days after the embryo transfer. The first fetal ultrasound is recommended a week after the test.
The next important stage, but after IVF, is the observation of pregnancy.
Share information:
Previous news
Go back
Make an appointment with the specialists of the clinic "Genome"
in Rostov-on-Don:
Phone: +7 (863) 295-35-80
WhatsApp: ask a question, make an appointment
call Navigator Request a call
Volgograd
Kaliningrad
Moscow
Nur-Sultan (Astana)
Rostov-on-Don
Tomsk
Ulyanovsk
Cherepovets
Remember my choice
Choose a convenient clinic for you
Volgograd
Kaliningrad
Moscow
Nur Sultan (Astana)
Rostov-on-Don
Tomsk
Cherepovets
9000 IVF - articles from the specialists of the clinic "Mother and Child"
Voronova Nina Zinovievna
Obstetrician-gynecologist
Clinic "Mother and Child" Khodynskoye Pole
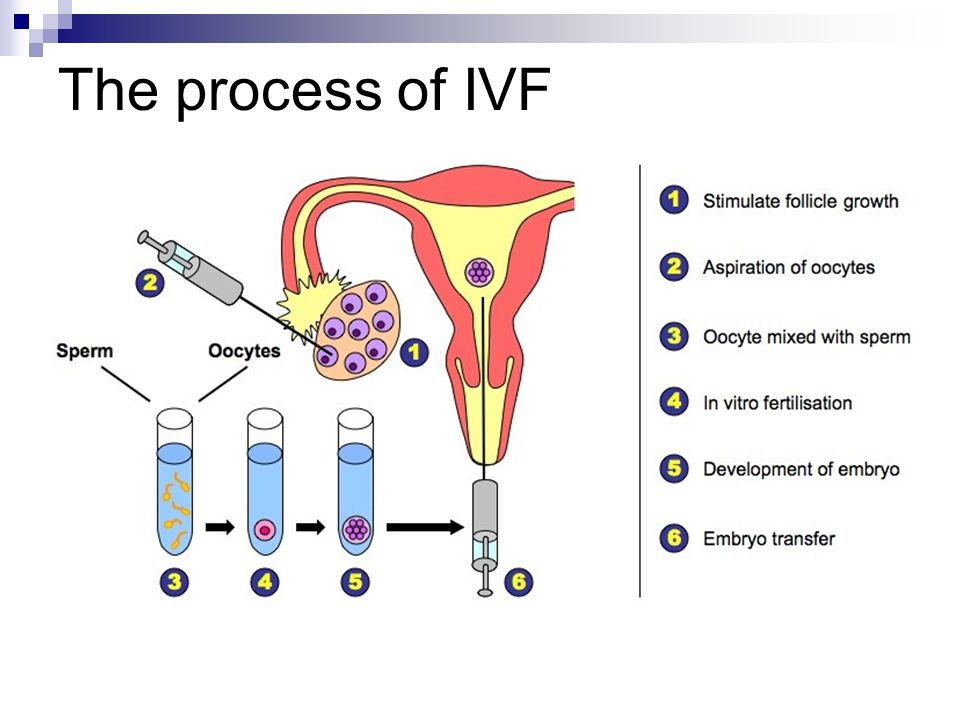
The IVF method is a complex process.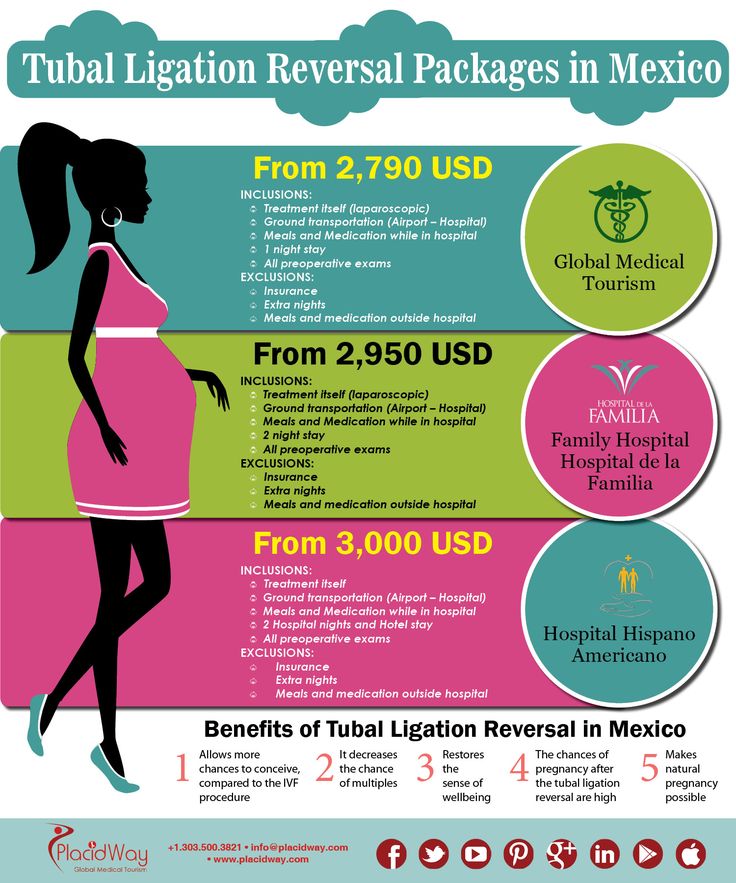 Schematically, it can be represented by the following steps:
Schematically, it can be represented by the following steps:
Stage 1 - monitoring the growth and maturation of follicles using ultrasound and (if indicated) hormonal studies. At this stage, superovulation is induced (that is, stimulation of the maturation of several eggs in one menstrual cycle). For the successful implementation of IVF, it is necessary to obtain several mature eggs at once during one menstrual cycle. This opportunity, which provides more chances for success, is provided by the use of hormonal drugs - triptorelin (decapeptyl / diferelin), buserelin or orgalutran; puregon/gonal or menopur; prerot/horagon or ovitrel. These drugs allow you to control the course of the menstrual cycle and calculate the time of egg maturation with the utmost accuracy. However, for the introduction of these drugs, as well as for any other drug, there may be an allergic reaction, both local (redness, infiltration) and general. These groups of hormonal drugs (GnRH agonists, urinary or recombinant gonadotropins) are analogues of human hormones involved in the process of growth and maturation of the egg. They have a narrowly focused action (ensure the maturation of eggs), with virtually no other side effects.
They have a narrowly focused action (ensure the maturation of eggs), with virtually no other side effects.
The day of the start of monitoring (the first stage of the IVF program) depends on the woman's age, the functional state of the ovaries. Women under the age of 35, as a rule, are included in the treatment cycle from 19–21 days of the menstrual cycle preceding the stimulation cycle (superovulation induction). From this time, the introduction of drugs (decapeptyl / diphereline / buserel) begins, which prepare the ovaries for stimulation. From the 1st-3rd day of the next menstrual cycle, drugs (Puregon / Gonal / Menopur, Pregnyl and their analogues) are used that directly stimulate the growth of follicles and the maturation of eggs, as well as the growth of the endometrium - the inner layer of the uterus, where the embryo will be implanted later. Women over 35-40 years old, as a rule, are included in the treatment cycle from day 1 of the menstrual cycle. The menstrual cycle is counted from the first day of menstruation.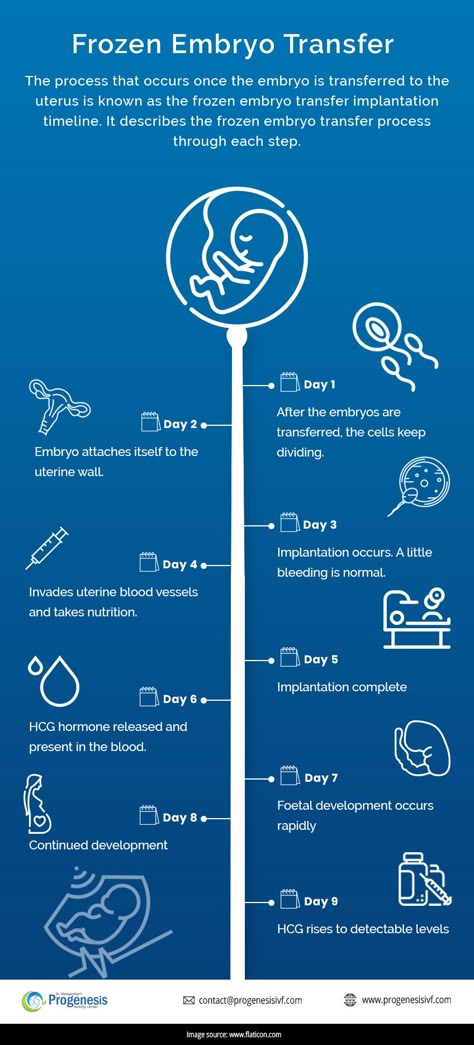 The day of arrival (the beginning of the treatment cycle) is always agreed with the doctor of the clinic (possibly by phone). All procedures are performed on an outpatient basis.
The day of arrival (the beginning of the treatment cycle) is always agreed with the doctor of the clinic (possibly by phone). All procedures are performed on an outpatient basis.
The introduction of drugs is performed by trained paramedical personnel. Treatment room services are provided according to the schedule all days of the week, including weekends and holidays (by appointment). When visiting the treatment room, please use changeable shoes.
Stage 2 - puncture or aspiration of follicular fluid containing mature eggs. The follicle puncture is performed transvaginally (through the vaults of the vagina) under ultrasound control. Due to its minimal trauma, transvaginal ovarian puncture is performed on an outpatient basis. At the request of patients, pain relief can be carried out with the help of drugs that cause drug-induced sleep. Ovarian puncture is performed on an empty stomach. On the day of the puncture, both spouses come to the medical center.
Stage 3 - embryological. The eggs obtained during the puncture of the follicles are placed in special cups with a nutrient medium. During the embryological stage, the culture dishes are in the incubator, where conditions are maintained similar to those in the mother's body (exactly the same temperature and the content of carbon dioxide, oxygen). After receiving eggs from a woman, the husband donates sperm.
The eggs obtained during the puncture of the follicles are placed in special cups with a nutrient medium. During the embryological stage, the culture dishes are in the incubator, where conditions are maintained similar to those in the mother's body (exactly the same temperature and the content of carbon dioxide, oxygen). After receiving eggs from a woman, the husband donates sperm.
For IVF, only spermatozoa that make forward movements are selected. Fertilization of eggs is carried out 4-6 hours after follicle puncture. Only one sperm cell out of tens of thousands is needed to fertilize one egg.
A prerequisite before donating sperm is prior abstinence from sexual activity for 2-7 days. In most men, with 3-5 days of abstinence, the composition of sperm and the quality of spermatozoa are the best.
Spermatogenesis largely depends on the impact of adverse factors. The quality of sperm deteriorates significantly under the influence of nicotine, alcohol, occupational hazards, stressful situations, nervous and general overwork, acute and chronic diseases. When planning treatment at an IVF medical center, it is necessary to exclude the influence of harmful factors or reduce it to a minimum. It must be remembered that the composition of spermatozoa is completely renewed within three months. Therefore, the longer a man manages to maintain a healthy lifestyle, the better the result.
When planning treatment at an IVF medical center, it is necessary to exclude the influence of harmful factors or reduce it to a minimum. It must be remembered that the composition of spermatozoa is completely renewed within three months. Therefore, the longer a man manages to maintain a healthy lifestyle, the better the result.
Stage 4 - transfer of embryos into the uterine cavity. Embryo transfer is carried out with a special atraumatic catheter, without resorting to expansion of the cervical canal, so this procedure is painless and does not require anesthesia.
It is recommended to transfer no more than 2 embryos into the uterine cavity, since if a larger number is transferred, the probability of a multiple pregnancy is higher.
Embryo transfer can be performed already on the second or third day after fertilization. If there are more than 3 high-quality embryos by the third day of cultivation, transfer can also be performed at later stages, up to the formation of a morula or blastocyst (pre-implantation stages of embryo development), that is, on the fourth or fifth day after fertilization.