Contractions before scheduled c section
Planned or elective caesarean | Pregnancy Birth and Baby
Planned or elective caesarean | Pregnancy Birth and Baby beginning of content5-minute read
Listen
What is a planned or elective caesarean?
A caesarean section (C-section) is an operation to deliver a baby through a cut in your tummy.
Caesarean sections may be planned before the birth. This is known as an elective caesarean. This may happen if there are pregnancy complications that prevent your baby being born by vaginal birth. In some cases, an elective caesarean is requested by the mother.
There are some important things to think about if you plan to or want to have a caesarean.
Why have a planned caesarean?
About 3 out of every 5 caesarean births in Australia are planned (elective).
Sometimes health problems or pregnancy complications mean that a caesarean birth would be safer than a vaginal birth.
Your doctor might recommend a planned, or elective, caesarean section for the following reasons:
- you have already had one or more caesarean sections
- your baby is in an abnormal position (such as bottom or feet first, or lying sideways)
- you are carrying more than one baby (for example, a twin pregnancy)
- your placenta is covering all or part the cervix (the opening to the uterus) - this is called placenta praevia
- you have a health problem, such as a heart problem, high blood pressure or fibroids (growths in the uterus)
- you have an infection that could be passed to your baby during a vaginal birth
- you or your baby have other medical complications
Some women may prefer a caesarean section to a vaginal birth for non-medical reasons. There are some risks and benefits to this decision for both mother and baby. It can also affect future pregnancies.
It can also affect future pregnancies.
You have a right to be involved in making decisions about the type of birth you will have. If you are having a planned caesarean section, talk with your doctor about the risks and benefits.
A caesarean section is major surgery. Complications are rare but can be serious. It is important to make an informed decision. So, make sure you ask questions and discuss concerns with your doctor and midwife.
How do I prepare for a planned caesarean?
Your doctor or midwife will arrange any tests and medical reviews that may be needed before your surgery. You will be asked to sign a consent form for the operation.
The timing of your caesarean birth will depend on your health, your baby’s health and the caesarean team’s schedule. Where possible, planned caesarean sections are often done at around 39 weeks. If there are problems or if you are having multiple babies (for example, twins), your caesarean may be done earlier than this.
Remember to take a bag for your stay in hospital, containing the things you and your baby will need. If you would like to take photos of the birth, ask your doctor whether it is OK for your partner or support person to bring a camera.
What will happen before a caesarean?
You will need to stop eating and drinking for about 6 hours before the operation.
Before the surgery, your pubic hair may be shaved and your tummy will need to be cleaned with antiseptic wash. You will be fitted with compression stockings on your legs. These help to reduce the risk of blood clots in your legs.
You will then be prepared for the anaesthetic. Many women having an elective caesarean will have an epidural anaesthetic or spinal block.
You will have intravenous (IV) lines put into your arm to give you fluids and medicines.
A doctor will place a catheter (a thin flexible tube) into your bladder. This will likely be removed once sensation returns to your legs and you can sit out of bed and walk.
What happens during and after a caesarean?
A screen is usually put across your chest so you cannot see what is happening. Some doctors now offer a ‘maternal assisted caesarean section’ so mothers can help deliver their baby. This is under the guidance of the doctor and is not always possible.
Your partner or support person can usually be with you during your planned caesarean birth. You will also usually have a midwife that stays with you. They will look after you and your baby in the operating theatre and recovery area.
If your baby is well, it is a good idea for you or your partner or support person to hold them straight away after the birth. Skin to skin contact keeps the baby warm and helps with bonding.
If you are choosing to breastfeed, your midwife may be able to assist you to do so once in the recovery room.
Remember that you will need time to recover after a caesarean. If possible, plan to have plenty of help at home in the weeks after the surgery.
What happens if I go into labour first?
About 1 in 10 women whose planned caesareans are scheduled for 39 weeks will go into labour first. That means their waters break or their contractions start. If this happens, you will have an emergency rather than a planned caesarean.
Call your hospital's maternity unit or delivery suite immediately if you are booked to have a planned caesarean and you go into labour.
Sources:
The Royal Women's Hospital (Caesarean birth), Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Caesarean section), Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Timing of elective caesarean section at term)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: May 2022
Back To Top
Related pages
- Vaginal birth after caesarean (VBAC)
- Recovery after a caesarean
- Emergency caesarean
Need more information?
Vaginal birth after caesarean (VBAC)
If you've delivered a baby by caesarean (C-section), you may have a choice with your next pregnancy - a vaginal birth after caesarean (VBAC) or a planned (elective) caesarean.
Read more on Pregnancy, Birth & Baby website
Vaginal Birth after Caesarean Section
Read more on RANZCOG - Royal Australian and New Zealand College of Obstetricians and Gynaecologists website
Emergency caesarean
Sometimes birth doesn't go as expected. If you or your baby are at risk, there might be a need to do an emergency caesarean.
Read more on Pregnancy, Birth & Baby website
Having a caesarean
A caesarean is an operation to deliver a baby through a cut in the abdomen (tummy) and uterus (womb). It might be planned (elective) or an emergency procedure.
Read more on Pregnancy, Birth & Baby website
Caesarean section - Better Health Channel
A caesarean section is usually performed when it is safer for the mother or the baby than a vaginal birth.
Read more on Better Health Channel website
Recovery after a caesarean
Recovery after a caesarean section - whether it's an emergency or planned - will take several weeks. Find out what to expect after you have had your baby.
Read more on Pregnancy, Birth & Baby website
Elective caesarean birth: what to expect | Raising Children Network
Having a planned or elective caesarean birth? As with any major surgery, it helps to know what to expect during a caesarean section. Our guide explains.
Read more on raisingchildren.net.au website
Caesarean Section - Birth Trauma
Being abdominal surgery, pain in the early months is very common after a caesarean section (C-section) and needs to be managed with rest, pain relief, and
Read more on Australasian Birth Trauma Association website
Breastfeeding after a caesarean birth | Australian Breastfeeding Association
Many mothers ask, "Can I breastfeed after a caesarean birth?" The answer is YES! There is no reason why you should not be able to breastfeed successfully.
Read more on Australian Breastfeeding Association website
Your Next Birth after Caesarean Section - Maternal, child and family health
Consumer brochure with information on birth options available to women planning their next birth after caesarean section.
Read more on NSW Health website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Signs of Labor | Frequently Asked Labor Questions
Video Transcription:Hi, I’m Andi, I’m a nurse here at Moreland OB-GYN--here today to answer some frequent questions about how to identify when you are in labor. Today I’m providing guidelines for a typical labor, but please follow the guidelines provided by your doctor.
 How will I know when I’m in labor? You will begin to notice that contractions will start at the top of your uterus or the top of your belly, and those contractions over time will become more and more frequent. Initially, those contractions might come at maybe 10 or 20-minute intervals, and throughout a duration of time, those contractions will eventually become every 1 to 2 minutes. Initially, you may be distracted from what you are doing throughout your day, but eventually, those contractions will be strong enough that no matter what you are doing you will have to stop and take time and breathe with them. Another sign of labor can be the rupture of membranes. For some women, this is a slow trickle of fluid where you just can’t feel clean no matter what you do. For other women, it’s a large gush of fluid like in the movies where it’s running down your legs. If that is occurring, make note of the time the rupture occurs, the color of the fluid, and the quantity of the fluid you are experiencing.
How will I know when I’m in labor? You will begin to notice that contractions will start at the top of your uterus or the top of your belly, and those contractions over time will become more and more frequent. Initially, those contractions might come at maybe 10 or 20-minute intervals, and throughout a duration of time, those contractions will eventually become every 1 to 2 minutes. Initially, you may be distracted from what you are doing throughout your day, but eventually, those contractions will be strong enough that no matter what you are doing you will have to stop and take time and breathe with them. Another sign of labor can be the rupture of membranes. For some women, this is a slow trickle of fluid where you just can’t feel clean no matter what you do. For other women, it’s a large gush of fluid like in the movies where it’s running down your legs. If that is occurring, make note of the time the rupture occurs, the color of the fluid, and the quantity of the fluid you are experiencing. The next step is to contact your doctor. As women get closer to their due date, they may experience false labor. False labor are bouts of contractions that can occur. These are contractions though that you may experience several of them. Say you are active, you are walking around, you experience contractions, you think that this might be it, but then you stop, you sit, and they go away. It can be very frustrating, especially as you are anticipating your due date approaching. You get excited, you get ready to go to the hospital, and sure enough, you stop, you sit, you drink a big glass of water or you lay down, and they dissolve and they go away. False labor is not uncommon—it’s not meant to feel defeating or discouraging but it’s very normal as your body is preparing for labor in and of itself. What Should I do if I’m in Labor? For first-time moms, if you’re contracting for every five minutes or less for at least an hour, each contraction is at least 60 seconds or longer, they are taking your breath away, all you can do is breathe with them, you’re distracted from any other activity, we want to know about it.
The next step is to contact your doctor. As women get closer to their due date, they may experience false labor. False labor are bouts of contractions that can occur. These are contractions though that you may experience several of them. Say you are active, you are walking around, you experience contractions, you think that this might be it, but then you stop, you sit, and they go away. It can be very frustrating, especially as you are anticipating your due date approaching. You get excited, you get ready to go to the hospital, and sure enough, you stop, you sit, you drink a big glass of water or you lay down, and they dissolve and they go away. False labor is not uncommon—it’s not meant to feel defeating or discouraging but it’s very normal as your body is preparing for labor in and of itself. What Should I do if I’m in Labor? For first-time moms, if you’re contracting for every five minutes or less for at least an hour, each contraction is at least 60 seconds or longer, they are taking your breath away, all you can do is breathe with them, you’re distracted from any other activity, we want to know about it. Or if your bag of waters has broken, you are having any bright red bleeding more than a period, or if your baby’s not moving, please contact our office. If this is not your first baby, and you have been experiencing contractions every 5 to 10 minutes, lasting at least 60 to 90 seconds for at least an hour, if you are having any bright red bleeding more than a period, if you think your bag of waters has ruptured, or your baby is not moving like normal, you should also be evaluated. Another question is what if I’m scheduled for a C-Section and I think I have gone into labor? What we would want you to do is contact us as soon as you think your labor has started, and stop eating or drinking. The reason for that is we would want to prepare for your surgery and know as soon as possible. During operating hours, triage nurses are always available to answer your questions. After hours, holidays, and weekends, physicians are available on-call to answer any of your questions.
Or if your bag of waters has broken, you are having any bright red bleeding more than a period, or if your baby’s not moving, please contact our office. If this is not your first baby, and you have been experiencing contractions every 5 to 10 minutes, lasting at least 60 to 90 seconds for at least an hour, if you are having any bright red bleeding more than a period, if you think your bag of waters has ruptured, or your baby is not moving like normal, you should also be evaluated. Another question is what if I’m scheduled for a C-Section and I think I have gone into labor? What we would want you to do is contact us as soon as you think your labor has started, and stop eating or drinking. The reason for that is we would want to prepare for your surgery and know as soon as possible. During operating hours, triage nurses are always available to answer your questions. After hours, holidays, and weekends, physicians are available on-call to answer any of your questions. Please DO NOT send MyChart messages with any questions regarding labor, rupture of membranes, or any concerns regarding the well-being of your baby. And do not hesitate, no questions are considered foolish. We hope you found this video helpful today. Our goal is the lead women to better health. When should I expect to go into labor?
Please DO NOT send MyChart messages with any questions regarding labor, rupture of membranes, or any concerns regarding the well-being of your baby. And do not hesitate, no questions are considered foolish. We hope you found this video helpful today. Our goal is the lead women to better health. When should I expect to go into labor? Labor normally starts when your baby is full grown or as we call it “term.” This can be as early as two weeks before your due date to as late as two weeks after your due date. If labor begins earlier than two weeks ahead of your due date, your baby can be born too early or premature. If it doesn’t happen until later than two weeks after your due date, your baby can be born overdue or post maturely.
How will I know that I'm in labor?Labor occurs when your uterus begins to tighten over and over again in an effort to push the baby out. This tightness or contractions are usually felt at the back and spread over the whole belly area. They last from about 45 to 60 seconds and occur about every 10 to 20 minutes. After an hour or two, these contractions usually become stronger and closer together.
They last from about 45 to 60 seconds and occur about every 10 to 20 minutes. After an hour or two, these contractions usually become stronger and closer together.
Sometimes a small amount of thick blood streaked mucous may come from the cervix, through the vagina during labor. This mucous plug is normal. Some women experience a sudden gush or slow leaking of clear fluid (amniotic fluid) from their vagina. This is the liquid that has surrounded and cushioned the baby so far. Usually, this fluid is forced out toward the end of labor, but sometimes it occurs earlier. You should call your doctor if this happens to you.
What is false labor?These are pains that are often felt in the low belly which don’t follow a regular time pattern or become more intense over time. They usually go away in a few hours. Often times if you lay down on your side for about an hour and drink a large glass of water, they will go away.
What should I do if I'm really in labor?First, use a clock to check how far apart the contractions are and how long they last. When they are strong and occurring about 10 minutes apart, call us and we will tell you the best time to go to the hospital. A physician is available 24 hours a day and can be reached at 262-544-4411—when calling after office hours, the answering service 1-800-446-3274 will direct your call.
When they are strong and occurring about 10 minutes apart, call us and we will tell you the best time to go to the hospital. A physician is available 24 hours a day and can be reached at 262-544-4411—when calling after office hours, the answering service 1-800-446-3274 will direct your call.
Let us know as soon as your labor begins, since you will need to get to the hospital very soon and we will want to be ready for surgery when you arrive.
What are the warning signs in labor that tell me I need to call the doctor or go to the hospital as soon as possible?- Decreased fetal movement
- Vaginal bleeding
- Rupture of membranes (bag of water)
We eat in childbirth! - articles from the specialists of the clinic "Mother and Child"
Artsybysheva Ludmila Romanovna
Obstetrician-gynecologist
Clinical hospital Lapino-1 "Mother and Child", Clinic KG "Lapino" in Odintsovo (branch)
yes or no
did not even arise, the doctors believed that with the onset of contractions, food and drink should be forgotten.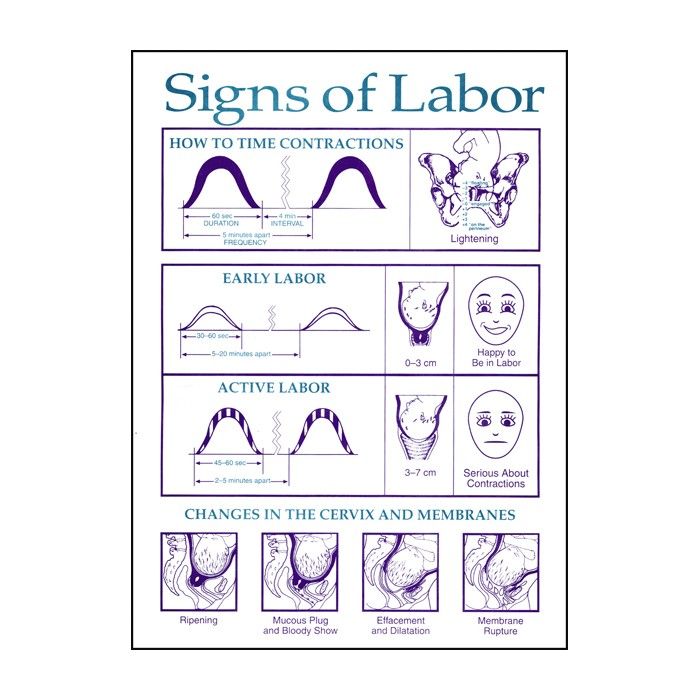 This was explained by the fact that if suddenly, for some reason, an emergency caesarean section is required, then general anesthesia will be needed, and before this anesthesia, you can’t drink, let alone eat (during such anesthesia, food residues can be thrown from the stomach into the lungs) . The only thing allowed was a few sips of water. But now everything has changed: childbirth has ceased to be a medical event, but has moved into the category of natural processes, no one thinks about “you never know what will happen”. In addition, even if a caesarean section is needed, then it (even an emergency one) is done almost everywhere with the help of epidural anesthesia (and eating does not affect it). So now doctors are not so categorical in relation to food in childbirth and even believe that food and water will help a woman avoid dehydration and maintain strength for experiencing contractions.
This was explained by the fact that if suddenly, for some reason, an emergency caesarean section is required, then general anesthesia will be needed, and before this anesthesia, you can’t drink, let alone eat (during such anesthesia, food residues can be thrown from the stomach into the lungs) . The only thing allowed was a few sips of water. But now everything has changed: childbirth has ceased to be a medical event, but has moved into the category of natural processes, no one thinks about “you never know what will happen”. In addition, even if a caesarean section is needed, then it (even an emergency one) is done almost everywhere with the help of epidural anesthesia (and eating does not affect it). So now doctors are not so categorical in relation to food in childbirth and even believe that food and water will help a woman avoid dehydration and maintain strength for experiencing contractions.
Therefore, if the birth is going well and you suddenly want to eat, then a light snack is allowed. Well, if you don’t even want to think about food, you don’t need to force yourself. In general, everything should be as desired.
Well, if you don’t even want to think about food, you don’t need to force yourself. In general, everything should be as desired.
when there is
Very often, on the day of childbirth, a woman notices that she does not feel like eating at all, at most - she would eat something light and simple. The same is possible with the onset of contractions: the body is not up to the digestive processes now, so there will be no strong appetite during childbirth. But, nevertheless, you don’t need to go to give birth on an empty stomach either, it will take strength in childbirth, and we take energy for them just from food. Therefore, with the onset of contractions, doctors recommend a woman to have a light snack - this is the best time to eat. Firstly, when the contractions are still weak and rare, you can eat without being distracted by painful sensations. Secondly, there is still a lot of time before the height of labor and the food has time to be digested, and this is important, because often during strong contractions, the woman in labor experiences nausea.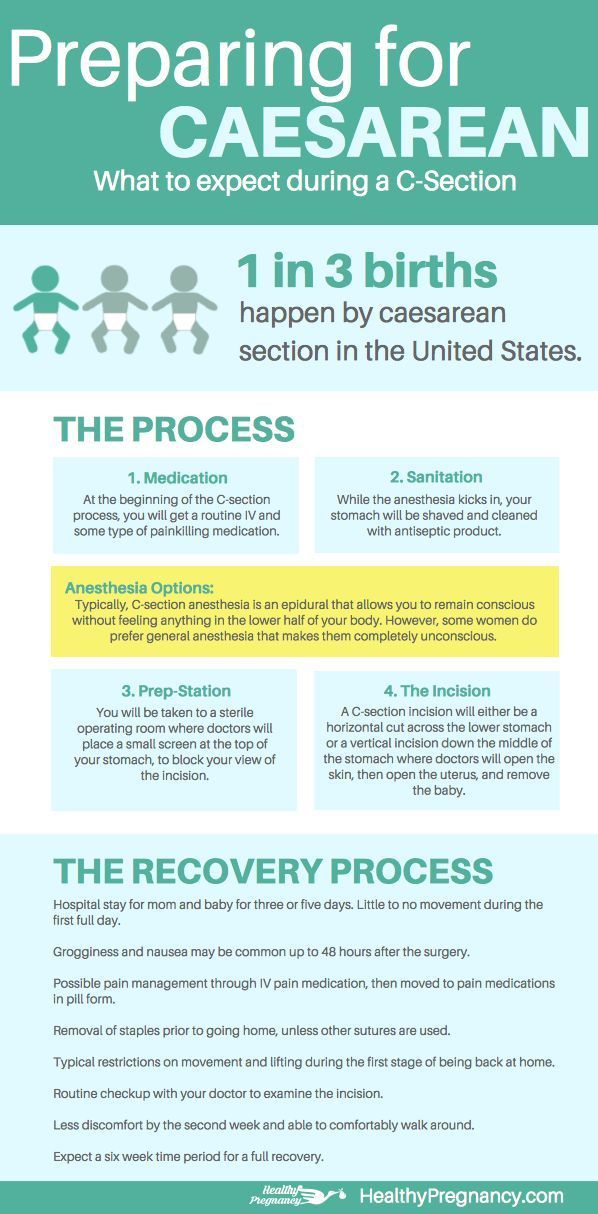 Thirdly, at the beginning of labor, a woman is usually at home, where, of course, there is food, then there will simply be no place to take it in the rodblok.
Thirdly, at the beginning of labor, a woman is usually at home, where, of course, there is food, then there will simply be no place to take it in the rodblok.
what to eat
Which dish or product to choose? There are no special prohibitions for food, and you can focus on your wishes, but still it is worth considering that fatty foods are out of place now: it is also heavy for the stomach, and nausea in labor can increase. The same can be said about protein: it does not provide energy and is hard and slow to digest. It is best to eat something from carbohydrates - they are just digested easily and, most importantly, provide the necessary energy. For example, banana, crispbread, toast, cereal, crackers, fruit puree, broth, soup, or yogurt will do.
what to drink
Contractions are physical work, they are like running a long distance, so during childbirth there is almost always thirst. Another reason why women in labor are thirsty is that it is often too warm or even hot in the birthing room, and the air in it is very dry. So drinking during childbirth is not only possible, but necessary. What is the best choice? Plain water, clarified juice and weak tea will do. Soda, especially sweet, should not be drunk: gas and sugar can irritate the stomach and provoke or increase nausea. You need to drink little by little, but often (sometimes even the usual amount of liquid also causes vomiting).
So drinking during childbirth is not only possible, but necessary. What is the best choice? Plain water, clarified juice and weak tea will do. Soda, especially sweet, should not be drunk: gas and sugar can irritate the stomach and provoke or increase nausea. You need to drink little by little, but often (sometimes even the usual amount of liquid also causes vomiting).
caesarean section
As we have already said, now almost everywhere a planned caesarean section is done under epidural anesthesia, and then eating and drinking is not prohibited. But if the operation is done under general anesthesia, then there will be restrictions on food intake. The last time you will be allowed to eat somewhere 8-12 hours before the operation. Since a planned caesarean section is usually performed in the morning, it turns out that the last meal is dinner. It should be light - the same bread, toast, yogurt, broth will do. Meat (even low-fat), cheeses, nuts, fatty cottage cheese - in general, it is better not to eat all foods that take a long time to digest.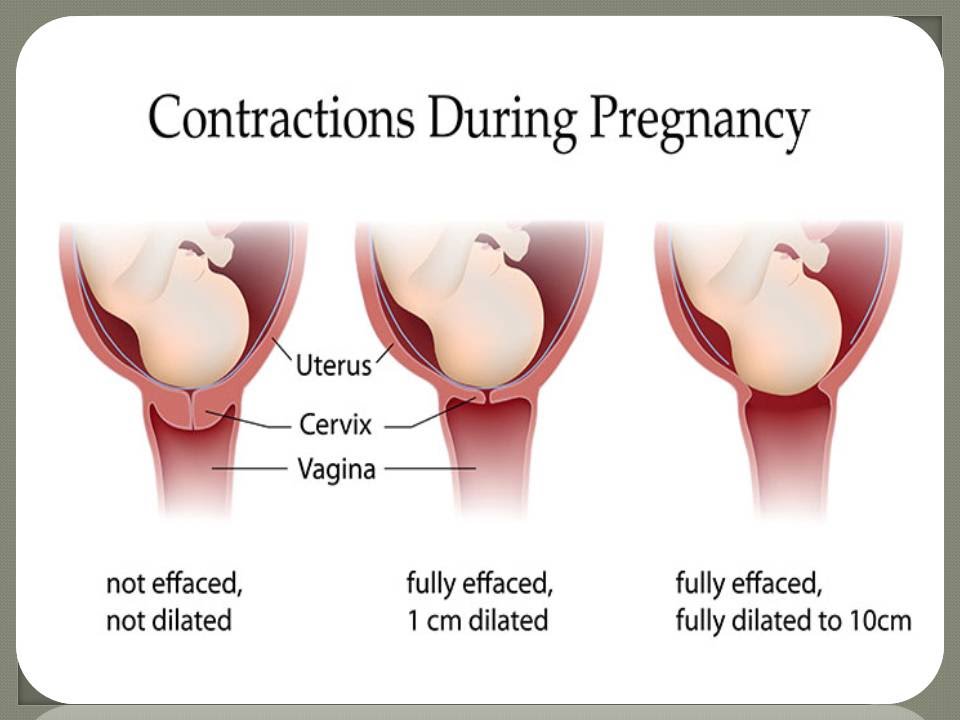 Also, do not eat a lot of fiber (vegetables and fruits) - it can affect bowel function.
Also, do not eat a lot of fiber (vegetables and fruits) - it can affect bowel function.
If you suddenly need general anesthesia during childbirth, and the woman has recently eaten, you should definitely tell the anesthesiologist about this. The doctor will more closely monitor that, under anesthesia, the contents of the stomach do not enter the respiratory tract.
some nuances
– Today, you can take water with you to childbirth in almost all maternity hospitals. Better if it is in a plastic bottle.
– Can I take some food with me to the hospital? Everything here will depend on the rules of the hospital. Usually, it is not allowed to bring food directly into the maternity unit itself, and this is understandable: a woman is already in it during active contractions, when she is not at all up to eating. But there are exceptions, somewhere they are allowed to bring the same toast, bread, chocolate to the rodblok. In any case, you can put some non-perishable products in the bag for the maternity hospital: what if the birth is delayed, or the baby will be born late in the evening, when dinner is already over, and breakfast is still far away? This is where you can have a bite to eat.
– If a partner (husband, sister, girlfriend) is present at the birth, then in a few hours he will also want to eat. Therefore, something to eat will have to be taken for him.
Ask the midwife or doctor who will be attending the delivery about food and drink. Or just call the maternity hospital and find out what food you can take with you. Then it will be easier for you to prepare and reschedule the birth.
Make an appointment
to the doctor - Artsybysheva Lyudmila Romanovna
Clinical Hospital Lapino-1 "Mother and Child" Clinic KG "Lapino" in Odintsovo (branch)
Pregnancy
By clicking on the send button, I consent to the processing of personal data
WHO: Women in labor and doctors increasingly opt for caesarean section |
According to the World Health Organization, modern surgical approaches, effective painkillers and antibiotics make it possible to perform surgery with minimal risk to mother and child. A new WHO study in this area has shown that in countries where at least 10% of women undergo this operation, maternal and child mortality is reduced. However, caesarean section certainly has its downsides.
A new WHO study in this area has shown that in countries where at least 10% of women undergo this operation, maternal and child mortality is reduced. However, caesarean section certainly has its downsides.
“My doctor almost immediately recommended a caesarean section. He explained it by my age. Although this was the second birth for me, but I was already 44 years old. And when I came to the hospital at the appointed time, they said: why, actually, a caesarean? according to what evidence? But my doctor insisted, he didn't want to risk anything. And then, after the birth, he told me that the child had an entanglement of the umbilical cord, and during childbirth this loop could tighten around the child’s neck.
More and more women choose caesarean section as the most painless, quick and safe way to give birth. Caesarean section is especially popular in developed and developing countries. The numbers are impressive. For example, in Brazil, 45% of women choose a caesarean section. In European countries, this figure has increased from 15% to 22% over the past 20 years. WHO spokeswoman Dr. Marlene Temmerman says:
In European countries, this figure has increased from 15% to 22% over the past 20 years. WHO spokeswoman Dr. Marlene Temmerman says:
In Brazil, 45% of women opt for a caesarean section. In European countries, this figure has grown from 15% to 22% over the past 20 years
“In many developing and developed countries, there is a real epidemic of caesarean sections. A cesarean is done even when there is no medical need for it. You may be wondering: so what? If women choose caesarean section and it is safe, why not? Yes, in modern conditions it is really safe. But do not forget that this is still an operation, a surgical intervention.
A caesarean section can cause serious complications for both the baby and the mother. Marlene Temmerman explains:
“Women who have a cesarean are at a higher risk of bleeding. Also, do not forget about the scars that remain from previous births that have passed with the help of surgical intervention. Serious complications may arise. And even in some developed countries, where caesareans are often performed, a higher level of maternal mortality has been reported compared to other developed countries. Of course, this operation is not the main cause of death among women in childbirth, but the connection certainly exists.
However, the preference for caesarean is made, of course, not only by women, but also by doctors. And they are partly understandable. It is better to perform a scheduled operation at a prearranged time than to receive a call from a patient in the middle of the night and then deal with this or that unforeseen situation during childbirth:
adjust your schedule. The doctor sees patients at a certain time. He can do two surgeries a day. No unexpected calls, no late night work, no emergencies, no added stress. The quality of life of doctors thanks to caesarean section is significantly improved.”
At the same time, experts emphasize that in many cases, caesarean section really saves lives.