Being induced what to expect
I’m Being Induced! What Should I Expect?
Home / Community / News Releases / Maternity / I’m Being Induced! What Should I Expect?
Posted on
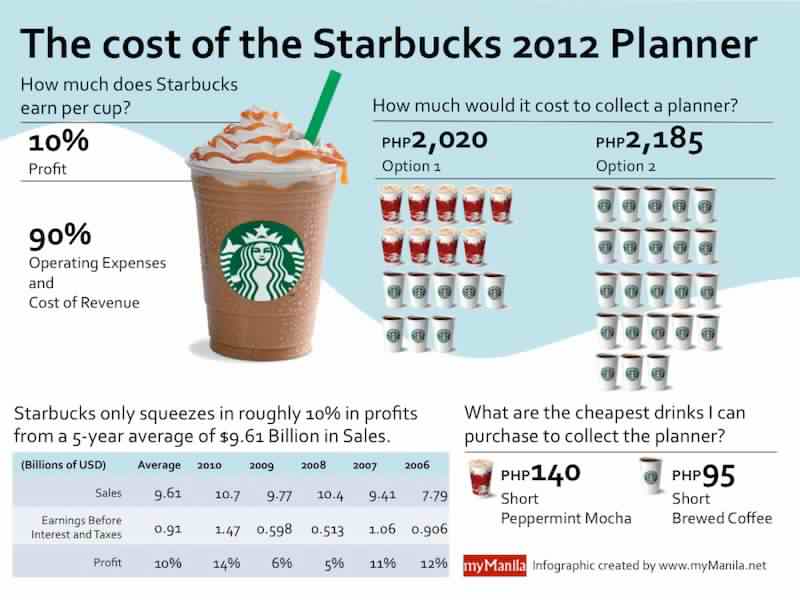
The goal of any healthcare practitioner is to carry all pregnancies to term, or 39 weeks. This means that generally speaking, labor shouldn’t be induced electively before that time—however, certain situations can come up when your body’s natural processes need a little nudge in the right direction.
What Does It Mean to be Induced?Being induced simply means that your labor contractions are started using medications or other methods because they aren’t starting naturally. There are a series of steps your doctor will follow to try to induce your labor, and most women don’t have to go through all of them!
Reasons Your Doctor Might Induce LaborYour baby is overdue.
If it’s time for your baby to make their debut, but there are no signs of action from your body, your doctor might induce labor around the 42-week mark.
You’re experiencing complications.
Conditions like preeclampsia, diabetes or gestational diabetes, issues with your placenta, or problems with your amniotic fluid make it risky to keep carrying your pregnancy. Your doctor may choose to induce your labor as soon as it’s safe to reduce the effects of these risks.
Broken water, but no contractions.
If your water has broken, but your contractions don’t start on their own within 24 hours, your doctor might need to get them started for you.
You live far from the hospital.
If you live far away from your hospital, your doctor might choose to induce labor to minimize the risk of not making it in time. On average, second-time moms experience much shorter labor than they did during their first time—so if your first baby came very quickly, your doctor might decide to induce your second to make sure you’re at the hospital when you need to be. This is known as an elective induction because it’s planned ahead of time and occurs no earlier than 39 weeks.
As mentioned above, there are a series of steps your doctor will go through to induce your labor. It’s fairly rare that a doctor has to go through every step to jumpstart your labor, but it is possible.
The first thing your doctor will try is ripening your cervix. Typically in natural labor, your cervix will open up, soften, and thin out in preparation for your baby. Your doctor might have to move things alone themselves, and they’ll do this by applying a topical form of the hormone prostaglandin to your cervix. After a few hours, labor could be well on its way—if it isn’t, your doctor will continue down the chain of steps toward successfully inducing your labor.
If your amniotic sac is still intact, meaning your water hasn’t broken, your doctor may get things started by swiping their finger across the fine membranes that connect it—the goal here isn’t to break your water, although that’s a possibility. Your doctor’s goal is to encourage your uterus to release prostaglandin as you would naturally if your labor was starting. This should cause your cervix to soften, and your contractions to start. This is called “membrane stripping.”
This should cause your cervix to soften, and your contractions to start. This is called “membrane stripping.”
If your cervix has started dilating, but your water hasn’t broken yet, your doctor might break it artificially. They’ll do this with an instrument that looks like a long crochet hook with a sharp tip—but don’t worry, while it might not be the most comfortable experience, it shouldn’t be painful.
If nothing your doctor tries is bringing on regular contractions, they will slowly start to give you Pitocin via IV. Pitocin is a synthetic form of the naturally occurring hormone oxytocin and should induce contractions. Contractions typically start about 30 minutes after you’ve been given the medication, and they’re usually stronger, more regular, and more frequent than natural labor contractions. If you’d like an epidural, you should ask your doctor about getting that started while the Pitocin is being administered, so that it’s ready to go once your labor starts.
When is a C-Section the Best Option?There are exceptions to every rule when it comes to pregnancy and the human body, which means that there are certain situations where labor shouldn’t be induced—in these situations, your doctor will recommend a c-section instead. Here are a few reasons you might have a c-section instead of being induced:
Here are a few reasons you might have a c-section instead of being induced:
- If there’s a need for immediate delivery, i.e. there’s no time to waste
- If there’s any doubt at all that your baby can fit through your pelvis
- If you’ve had a c-section before, and now you’re attempting a vaginal birth
- If the placenta is near or covering your cervix
- If there’s a prolapsed cord, i.e. it has slipped down into the vagina before the baby’s head
- If you’re experiencing a genital herpes outbreak
- If you’re carrying multiple babies
- If your baby is breech
Keep in mind that your doctor’s goal is to minimize interventions as best they can, and will only induce your labor or recommend a c-section if they decide it’s necessary.
Looking for more pregnancy advice? Visit our website today.
What to Expect and What to Ask
Labor induction, also known as inducing labor, is the jumpstarting of uterine contractions before natural labor occurs, with the goal of a healthy vaginal delivery.
Healthcare providers, doctors, and midwives might suggest inducing labor for a number of reasons — both medical and nonmedical (elected).
Here’s what you need to know in order to prepare for labor induction.
A healthcare provider, doctor, or midwife will evaluate your health and the health of your baby at all prenatal appointments. This includes examining your baby’s gestational age, size, weight and position in your uterus.
At later appointments, this may include checking your cervix and considering the overall picture to determine whether or not you or baby are at risk and labor induction is needed.
How does your cervix rate?
The cervix begins to ripen (soften), thin out, and open as it prepares for labor and delivery. To determine the readiness of the cervix, some doctors use the Bishop score. Rating the readiness on a scale from 0 to 13, your cervix gains points based on dilation, texture, placement, angle, and length.
A labor induction may be suggested if there’s cause for concern regarding the health of you or your baby. Or perhaps you live a far distance from your hospital, and it would be prudent to control the timing of your labor and delivery.
Or perhaps you live a far distance from your hospital, and it would be prudent to control the timing of your labor and delivery.
Other reasons include:
- Predicted due date has come and gone.
- Gestational diabetes.
- Chorioamnionitis (an infection in the uterus).
- Baby is growing too slowly.
- Oligohydramnios (low or leaking amniotic fluid).
- Placental obstruction or abruption.
- Broken water, but no contractions.
- History of speedy, short deliveries.
Women with certain medical conditions should not be recommended for induction, so it’s important to ask questions (see below) and discuss all of the options, benefits, and potential risks of a labor inducing procedure with your healthcare provider.
Did you know?Women spend more time in labor now than they did 50 years ago!
There are many methods of labor induction, and what works for one woman or one delivery, may not work for another.
In addition to natural inducing methods (both proven and unproven), such as sexual intercourse, castor oil, hot baths, breast and nipple stimulation, acupuncture, herbal supplements, and eggplant casseroles, there are many medical/surgical techniques too.
A doctor or midwife can use medicines and other means to assist in opening the cervix and stimulate contractions. Some methods include:
- Amniotomy, or “breaking the water,” where your healthcare provider pokes a small hole in your amniotic sac. This will also make your uterine contractions stronger.
- Pitocin, also called oxytocin, which is a hormone that speeds up labor. Pitocin is delivered through an IV in your arm.
- Cervical ripening, performed by taking medicine orally or by inserting a medicine (prostaglandin analogs) into the vagina to stretch, soften, and expand the cervix.
- Insertion of catheter or balloon by your healthcare provider, which then expands, such as a Foley bulb induction.
- Stripping membranes, where your healthcare provider uses a gloved finger to separate the thin tissue of amniotic sac from the uterine wall.
From time to time, a doctor will use more than one method to induce labor and delivery.
Every labor progresses at its own pace. If your cervix is soft and ripe, a gentle push may be all you need to jumpstart those contractions. If your cervix needs more time, it may take days before delivery occurs.
An induced labor can last anywhere from a few hours to a few days. Sometimes, labor induction doesn’t work at all, or the method used has to be repeated. It all depends on how ripe the cervix is at time of induction and how well your body responds to the method chosen for induction.
Contractions can start within 30 minutes of taking oxytocin, and most women will begin labor within hours after their water breaks.
All healthcare providers should allow you 24 hours or more of the early phase of labor before considering the induction a bust and moving forward with other interventions.
If you and your baby are healthy and doing well after a failed induction, you might be sent home and asked to reschedule the induction for a later date. (Yes, that can actually happen.)
As with everything in life, labor induction comes with some risks.
- You may experience stronger, more painful and frequent contractions.
- You may have increased risk of postpartum depression, according to one 2017 study.
- You may have a failed induction and need a cesarean delivery (this comes with its own list of concerns, including a longer recovery time).
A first-time mother whose cervix is not ready for labor has an increased chance of the induction leading to a cesarean delivery, according to the American College of Obstetricians and Gynecologists. This is why asking questions (see below) — especially about the condition of your cervix — is so important.
Throughout the induction process, your healthcare provider, doctor, or midwife will monitor you and your baby to determine whether or not an assisted vaginal delivery or cesarean delivery is necessary.
Other potential risks of induction include:
- Infection. Certain methods of induction, such as rupturing membranes, pose an increased risk for infection in both mom and baby.
- Uterine rupture. This is especially true for women who have had a previous cesarean delivery or another uterine surgery.
- Complications with fetal heart rate. Too many contractions can lead to changes in the baby’s heart rate.
- Fetal death.
It’s important to discuss the potential risks for you and your baby during induction in detail with a healthcare provider, doctor, or midwife before agreeing to any procedure.
Ask questions
Before you agree to be induced, consider finding out the following from your healthcare provider:
- What’s the reason for the induction?
- What are the signs that make you a good candidate for induction?
- What types of induction is your healthcare provider considering?
- What’s your due date? (Confirm that the induction date is indeed set for after the 39th week of pregnancy.
 )
) - What’s the condition of your cervix?
- What is the baby’s position?
- How many times has your doctor or midwife performed this procedure?
- Will you be able to move around?
- What are the risks and benefits of each induction procedure being considered?
- Will it require constant or occasional monitoring?
- Will it hurt? What are your options for pain relief?
- What is the doctor or midwife’s plan if the chosen method for induction fails?
- At what point might you be sent home, with another induction rescheduled?
- Will your doctor or midwife be available during the entire procedure?
- If the procedure takes a very long time, will you be able to use the restroom?
- Do you have a prior medical condition or consideration that will affect this induction?
You’ll also want to know where the labor induction will take place, typically a hospital or birthing center. However, a home delivery with natural induction methods may sometimes be an option.
Set realistic expectations
Maybe an induction isn’t what you had in mind. Well… try to keep an open mind! Induced labor is very different than a naturally occurring labor, but that doesn’t mean you have to throw your entire birth plan out the window.
Take a moment to consider how you think and feel about your labor and delivery plan. The mental and emotional aspects of labor and delivery are complicated enough, and getting induced has its own benefits and risks.
Pack entertainment
This may be happening, but it’s not always fast.Don’t let the waiting time get to you. Load an electronic device with movies, on-demand shows, and books and add them to your hospital bag.
Pack a journal and plan on taking a few minutes to jot down your in-the-moment labor and delivery thoughts. Make a playlist of music for when you need calming and for the You Can Do This Oomph and Push.
Don’t forget to pack chargers for all electronic devices, a pair of headphones, and comfortable, loose clothing.
Eat something light and then try to go poo
Most practitioners say no food once contractions begin. Don’t stop at your favorite fast food place on the way to the hospital. You don’t want the runs during this business.
Before heading to the hospital, eat a light meal at home… and then give the ol’ porcelain bowl a good visit. You’ll feel much better.
Give your partner permission to scoot
If the induction lasts longer than 12 to 24 hours, consider allowing your partner some fresh air. A bored induction partner can turn into an annoying labor and delivery companion, so allow your partner to pack their own hospital bag.
Tell them to pack some snacks (nothing smelly!) and a good pillow. Once at the hospital, communicate your feelings as best as possible, and then tell them to go find you some ice cream for after.
Accept that it may take longer than you’d like, and may be more challenging than you imagine. It will be okay! Talk with friends and family members who have had induced labors and at some point, and try to stop googling. It’s normal to feel excited and nervous.
It’s normal to feel excited and nervous.
Just remember: You have options and choices.
What to expect in 2022?
No one should be surprised if we say that 2021 has been one of the most turbulent years in the history of the information security industry. There were several high-profile cyber-attacks during the year. Many believe that cybercriminals led to the first death of a person caused directly by a ransomware attack - in the summer, the Wall Street Journal reported the first death from a ransomware in a hospital in Alabama (USA). In addition, many companies around the world have lost hundreds of billions of dollars due to ransomware. The number of data breaches that have been publicly reported has surpassed that of 2020, and this year is close to being the year of record breaches in history. Information about the next data breach in any company or organization, regardless of its size (small, medium or large), often made headlines in the media. And, according to WatchGuard experts, 2022 is likely to be as turbulent as 2021 .
State Sponsored Attacks
2021 has shown us that cyberattacks against critical infrastructure can impact masses of people and have real catastrophic consequences. In 2021, for example, cyber-attacks triggered a fuel buying panic on the US East Coast and temporary meat supply issues with the world's largest meat producer. State-sponsored hackers are aware of their potential and will most likely look for ways to strike critical infrastructure in 2022 . Such cyber-attacks are capable of triggering a war without firing a single live bullet. In this regard, the governments of all countries of the world must monitor their basic infrastructure.
Space cyber attacks
Leading countries have been very active lately when it comes to space. For example, less than two years ago, the US even founded the United States Space Force (USSF). With so much attention being paid to the outside world, WatchGuard draws attention to the fact that in 2022 the probability of "hacking in space" will be very high . Both private organizations and government agencies are involved in the space race, and one way or another, hackers may find their way there too. Some of the satellites that fly over the Earth are relatively outdated and their ability to meet today's protection and safety requirements is questionable.
Both private organizations and government agencies are involved in the space race, and one way or another, hackers may find their way there too. Some of the satellites that fly over the Earth are relatively outdated and their ability to meet today's protection and safety requirements is questionable.
SMSishing or SMS phishing
SMS phishing has been around for quite some time. Experts believe that 2022 will be no exception to this threat. Many believe that attacks will become even more sophisticated . Over the next year, cybercriminals will continue to impersonate other people to trick unsuspecting users into clicking on malicious links. More and more companies are relying on messaging apps to interact with employees. Many people share sensitive information in these messengers, so it is necessary to ensure that mobile phones are well protected. Don't leave an open door for cyber-attackers and avoid clicking on links that look suspicious. This can cost you dearly, both personally and professionally.
Failures in passwordless authentication methods
Many companies, including Microsoft, have begun implementing ways for users to interact with services and platforms without the use of passwords. As with any new technology, the start will not be easy, and the more companies that adopt similar practices, the more likely we are to see such practices fail. Of course, pioneers can always be admired, but, unfortunately, they are the ones to blame if something goes wrong. It won't be a surprise if in 2022 we see hackers who somehow find way to cause damage bypassing such authorization methods .
Cryptocurrencies and mobile wallets
It looks like cryptocurrencies will be with us for a long time . The adoption of mobile wallets will continue and crypto may even become mainstream eventually. This will no doubt continue to attract the attention of cyber criminals. Attacks can take many forms: users may be prompted to download malicious mobile applications or infected after visiting an insecure site. Hackers can be very creative and explore other routes, but the end goal is usually the same - to gain access to their victims' digital wallets. Cryptocurrencies are not easy to track, so the theft of this kind of funds is even a priority for cyber criminals . In 2022, we will most likely see an increase in the number of cyber attacks related to cryptocurrencies and digital wallets.
Hackers can be very creative and explore other routes, but the end goal is usually the same - to gain access to their victims' digital wallets. Cryptocurrencies are not easy to track, so the theft of this kind of funds is even a priority for cyber criminals . In 2022, we will most likely see an increase in the number of cyber attacks related to cryptocurrencies and digital wallets.
The coming year 2022 will indeed be as turbulent as 2021 . Will we see more high-profile hacks and attacks on ordinary people? Maybe yes. Especially in the context of the ongoing Covid 19 coronavirus pandemic, humanity will continue to rely on the Internet in daily life. While the remote nature of communication may be safer as all people avoid contracting the new virus, more people going digital will also mean more opportunities for troublemakers to attack.
Cloud solutions
[email protected]https://www.cloudav.ru
The world is going crazy, but it's not too late to fix it. Subscribe to the SecLabnews channel and do your part to prevent the cyber apocalypse!
Subscribe to the SecLabnews channel and do your part to prevent the cyber apocalypse!
Breastfeeding in the first month: what to expect
Not sure how to establish lactation and increase milk production? If you need help, support, or just want to know what to expect, read our First Month Breastfeeding Recommendations
Share this information
The first weeks of breastfeeding are a very stressful period. If at times you feel like you can't handle it, know that you are not alone. Feeding your baby all day long is completely natural and helps produce breast milk, but can be quite tiring at times. Be patient, think about yourself and remember: after the first month, when milk production stabilizes, it will become easier.
How often should a baby be breastfed?
Babies are born with a small stomach that grows rapidly as milk production increases: in the first week it is no larger than an apricot, and after two weeks it is already the size of a large hen's egg. 1.2 Let the child eat as much as he wants and when he wants. This will help him quickly regain the weight lost after birth and grow and develop further.
1.2 Let the child eat as much as he wants and when he wants. This will help him quickly regain the weight lost after birth and grow and develop further.
“Be prepared to feed every two to three hours throughout the day. At night, the intervals between feedings can be longer: three to four or even five hours, says Cathy Garbin, a recognized international expert on breastfeeding. Some eat quickly and are satiated in 15 minutes, while others take an entire hour to feed. Do not compare your breastfeeding regimen with that of other mothers - it is very likely that there will be nothing in common between them.
At each feed, give your baby a full meal from one breast and then offer a second one, but don't worry if the baby doesn't take it. When the baby is full, he lets go of his chest and at the same time looks relaxed and satisfied - so much so that he can immediately fall asleep. The next time you feed, start on the other breast. You can monitor the order of the mammary glands during feeding using a special application.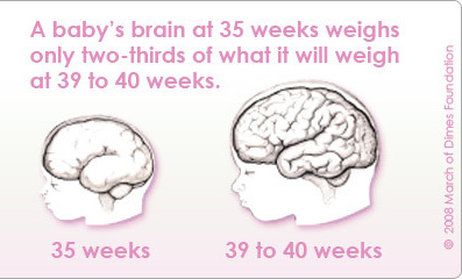
Why does the child always ask for a breast?
The first month is usually the hardest time to breastfeed. But do not think that because the baby is constantly hungry and asks for a breast almost every 45 minutes, then you do not have enough milk.
In the first month, the baby needs to eat frequently to start and stimulate the mother's milk production. It lays the foundation for a stable milk supply in the future. 3
In addition, we must not forget that the child needs almost constant contact with the mother. The bright light and noise of the surrounding world at first frighten the baby, and only by clinging to his mother, he can calm down.
Sarah, mother of three from the UK, confirms: “Crying is not always a sign of hunger. Sometimes my kids just wanted me to be around and begged for breasts to calm them down. Use a sling. Place the cradle next to the bed. Don't look at the clock. Take advantage of every opportunity to relax. Forget about cleaning. Let those around you take care of you. And not three days, but six weeks at least! Hug your baby, enjoy the comfort - and trust your body."
Let those around you take care of you. And not three days, but six weeks at least! Hug your baby, enjoy the comfort - and trust your body."
Do I need to feed my baby on a schedule?
Your baby is still too young for a strict daily routine, so
forget about breastfeeding schedules and focus on his needs.
“Volumes have been written about how to feed a baby on a schedule, but babies don't read or understand books,” Cathy says. - All children are different. Some people can eat on a schedule, but most can't. Most often, over time, the child develops his own schedule.
Some mothers report that their babies are fine with scheduled feedings, but they are probably just the few babies who would eat every four hours anyway. Adults rarely eat and drink the same foods at the same time of day - so why do we expect this from toddlers?
Offer your baby the breast at the first sign of hunger. Crying is already the last stage, so be attentive to early signs: the baby licks his lips, opens his mouth, sucks his fist, turns his head with his mouth open - looking for the breast. 4
4
What is a “milk flush”?
At the beginning of each feed, a hungry baby actively sucks on the nipple,
thereby stimulating the milk flow reflex - the movement of milk through the milk ducts. 5
“Nipple stimulation triggers the release of the hormone oxytocin,” Cathy explains. “Oxytocin is distributed throughout the body and causes the muscles around the milk-producing glands to contract and the milk ducts to dilate. This stimulates the flow of milk.
If the flushing reflex fails, milk will not come out. This is a hormonal response, and under stress it may not work at all or work poorly. Therefore, it is so important that you feel comfortable and calm when feeding.
“Studies show that each mother has a different rhythm of hot flashes during one feed,” Katie continues, “Oxytocin is a short-acting hormone, it breaks down in just 30-40 seconds after formation. Milk begins to flow, the baby eats, the effect of oxytocin ends, but then a new rush of milk occurs, the baby continues to suckle the breast, and this process is repeated cyclically. That is why, during feeding, the child periodically stops and rests - this is how nature intended.
That is why, during feeding, the child periodically stops and rests - this is how nature intended.
The flow of milk may be accompanied by a strong sensation of movement or tingling in the chest, although 21% of mothers, according to surveys, do not feel anything at all. 5 Cathy explains: “Many women only feel the first rush of milk. If you do not feel hot flashes, do not worry: since the child eats normally, most likely, you simply do not understand that they are.
How can you tell if your baby is getting enough milk?
Since it is impossible to track how much milk a baby eats while breastfeeding, mothers sometimes worry that the baby is malnourished. Trust your child and your body.
After a rush of milk, the baby usually begins to suckle more slowly. Some mothers clearly hear how the baby swallows, others do not notice it. But one way or another, the child himself will show when he is full - just watch carefully. Many babies make two or three approaches to the breast at one feeding. 6
6
“When a child has had enough, it is noticeable almost immediately: a kind of “milk intoxication” sets in. The baby is relaxed and makes it clear with his whole body that he is completely full, says Katie, “Diapers are another great way to assess whether the baby is getting enough milk. During this period, a breastfed baby should have at least five wet diapers a day and at least two portions of soft yellow stool, and often more.”
From one month until weaning at six months of age, a baby's stool (if exclusively breastfed) should look the same every day: yellow, grainy, loose, and watery.
When is the child's birth weight restored?
Most newborns lose weight in the first few days of life. This is normal and should not be cause for concern. As a rule, weight is reduced by 5-7%, although some may lose up to 10%. One way or another, by 10–14 days, almost all newborns regain their birth weight. In the first three to four months, the minimum expected weight gain is an average of 150 grams per week. But one week the child may gain weight faster, and the next slower, so it is necessary that the attending physician monitor the health and growth of the baby constantly. 7.8
But one week the child may gain weight faster, and the next slower, so it is necessary that the attending physician monitor the health and growth of the baby constantly. 7.8
At the slightest doubt or signs of dehydration, such as
dark urine, no stool for more than 24 hours, retraction of the fontanel (soft spot on the head), yellowing of the skin, drowsiness, lethargy, lack of appetite (ability to four to six hours without feeding), you should immediately consult a doctor. 7
What is "cluster feeding"?
When a baby very often asks for a breast for several hours, this is called cluster feeding. 6 The peak often occurs in the evening between 18:00 and 22:00, exactly when many babies are especially restless and need close contact with their mother. Most often, mothers complain about this in the period from two to nine weeks after childbirth. This is perfectly normal and common behavior as long as the baby is otherwise healthy, eating well, gaining weight normally, and appears content throughout the day. 9
9
Cluster feeding can be caused by a sharp jump in the development of the body - during this period the baby especially needs love, comfort and a sense of security. The growing brain of a child is so excited that it can be difficult for him to turn off, or it just scares the baby. 9 If a child is overworked, it is often difficult for him or her to calm down on his own and the help of adults is needed. And breastfeeding is the best way to calm the baby, because breast milk is not only food, but also pain reliever and a source of happiness hormones. 10
“No one told me about cluster feeding, so for the first 10 days I just went crazy with anxiety - I was sure that my milk was not enough for the baby,” recalls Camille, a mother from Australia, “It was a very difficult period . I was advised to pump and supplement until I finally contacted the Australian Breastfeeding Association. There they explained to me what was happening: it turned out that it was not about milk at all.
Remember, this is temporary. Try to prepare dinner for yourself in the afternoon, when the baby is fast asleep, so that in the evening, when he begins to often breastfeed, you have the opportunity to quickly warm up the food and have a snack. If you are not alone, arrange to carry and rock the baby in turns so that you have the opportunity to rest. If you have no one to turn to for help and you feel that your strength is leaving you, put the baby in the crib and rest for a few minutes, and then pick it up again.
Ask your partner, family and friends to help you with household chores, cooking and caring for older children if you have any. If possible, hire an au pair. Get as much rest as possible, eat well and drink plenty of water.
“My daughter slept a lot during the day, but from 23:00 to 5:00 the cluster feeding period began, which was very tiring,” recalls Jenal, a mother from the USA, “My husband tried his best to make life easier for me — he washed, cleaned, cooked, changed diapers, let me sleep at every opportunity and never tired of assuring me that we were doing well.
If you are concerned about the frequency of breastfeeding, it is worth contacting a specialist. “Check with a lactation consultant or doctor to see if this is indicative of any problems,” recommends Cathy. “Resist the temptation to supplement your baby with formula (unless recommended by your doctor) until you find the cause. It may not be a matter of limited milk production at all - it may be that the child is inefficiently sucking it.
When will breastfeeding become easier?
This early stage is very special and does not last long. Although sometimes it seems that there will be no end to it, rest assured: it will get easier soon! By the end of the first month, breast milk production will stabilize, and the baby will become stronger and learn to suckle better. 2.3 Any problems with latch on will most likely be resolved by this time, and the body will be able to produce milk more efficiently, so inflammation and leakage of milk will begin to subside.
“The first four to six weeks are the hardest, but then things start to get better,” Cathy assures. It just needs to be experienced!”
The longer breastfeeding continues, the more benefits it brings, from saving on formula and improving sleep quality 11-13 to boosting your baby's immune system 14 and reducing your risk of developing certain types of cancer. 15
“When you feel like you're on your limit, try to go from feed to feed and day to day,” advises Hannah, a UK mom. “I was sure I wouldn’t make it to eight weeks. And now I have been breastfeeding for almost 17 weeks, and I dare say it is very easy.”
Read the resource Breastfeeding After the First Month: What to Expect
Readings
1 Naveed M et al. An autopsy study of relationship between perinatal stomach capacity and birth weight. Indian J Gastroenterol .1992;11(4):156-158. - Navid M. et al., "Relationship between prenatal gastric volume and birth weight. Autopsy." Indian J Gastroenterol. 1992;11(4):156-158.
et al., "Relationship between prenatal gastric volume and birth weight. Autopsy." Indian J Gastroenterol. 1992;11(4):156-158.
2 Neville MC et al. Studies in human lactation: milk volumes in lactating women during the onset of lactation and full lactation. Am J Clinl Nutr . 1988;48(6):1375-1386. - Neville M.S. et al., "Female Lactation Study: Milk Quantity in Lactating Women at the Beginning and Peak of Lactation." Am F Clean Nutr. 1988;48(6):1375-1386.
3 Kent JC et al. Principles for maintaining or increasing breast milk production. J Obstet , Gynecol , & Neonatal Nurs . 2012;41(1):114-121. - Kent J.S. et al., "Principles for Maintaining and Increasing Milk Production". J Obstet Ginecol Neoneutal Nurs. 2012;41(1):114-121.
4 Australian Breastfeeding Feeding cues ; 2017 Sep [ cited 2018 Feb ]. - Australian Breastfeeding Association [Internet], Feed Ready Signals; September 2017 [cited February 2018]
- Australian Breastfeeding Association [Internet], Feed Ready Signals; September 2017 [cited February 2018]
5 Kent JC et al. Response of breasts to different stimulation patterns of an electric breast pump. J Human Lact . 2003;19(2):179-186. - Kent J.S. et al., Breast Response to Different Types of Electric Breast Pump Stimulation. J Human Lact (Journal of the International Association of Lactation Consultants). 2003;19(2):179-186.
6) Kent JC Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics. 2006;117(3): e 387-395. - Kent J.S. et al., "Amount and frequency of breastfeeding and fat content of breast milk during the day." Pediatrix (Pediatrics). 2006;117(3):e387-95.
7 Lawrence RA, Lawrence RM. Breastfeeding: A guide for the medical profession. 7th ed. Maryland Heights MO, USA: Elsevier Mosby; 2010. 1128 p . - Lawrence R.A., Lawrence R.M., "Breastfeeding: A guide for healthcare professionals." Seventh edition. Publisher Maryland Heights , Missouri, USA: Elsevier Mosby; 2010. P. 1128.
7th ed. Maryland Heights MO, USA: Elsevier Mosby; 2010. 1128 p . - Lawrence R.A., Lawrence R.M., "Breastfeeding: A guide for healthcare professionals." Seventh edition. Publisher Maryland Heights , Missouri, USA: Elsevier Mosby; 2010. P. 1128.
8 World Health Organization. [Internet]. Child growth standards; 2018 [cited 2018 Feb] - World Health Organization. [Internet]. Child Growth Standards 2018 [cited February 2018].
9 Australian Breast feeding Association . [ Internet ]. Cluster feeding and fussing babies ; Dec 2017 [ cited 2018 Feb ] - Australian Breastfeeding Association [Internet], Cluster Feeding and Screaming Babies; December 2017 [cited February 2018].
10 Moberg KU, Prime DK. Oxytocin effects in mothers and infants during breastfeeding. Infant . 2013;9(6):201-206.- Moberg K, Prime DK, "Oxytocin effects on mother and child during breastfeeding". Infant. 2013;9(6):201-206.
Oxytocin effects in mothers and infants during breastfeeding. Infant . 2013;9(6):201-206.- Moberg K, Prime DK, "Oxytocin effects on mother and child during breastfeeding". Infant. 2013;9(6):201-206.
11 U.S. Department of Health & Human Services [Internet]. Surgeon General Breastfeeding factsheet; 2011 Jan 20 [cited 2017 Feb] - Department of Health and Human Services [Internet], "Breastfeeding Facts from the Chief Medical Officer", Jan 20, 2011 [cited Feb 2017]
12 Kendall-Tackett K et al. The effect of feeding method on sleep duration, maternal well-being, and postpartum depression. clinical lactation. 2011;1;2(2):22-26. - Kendall-Tuckett, K. et al., "Influence of feeding pattern on sleep duration, maternal well-being and the development of postpartum depression." Clinical Lactation. 2011;2(2):22-26.
13 Brown A, Harries V. Infant sleep and night feeding patterns during later infancy: Association with breastfeeding frequency, daytime complementary food intake, and infant weight. Breast Med . 2015;10(5):246-252. - Brown A., Harris W., "Night feedings and infant sleep in the first year of life and their association with feeding frequency, daytime supplementation, and infant weight." Brest Med (Breastfeeding Medicine). 2015;10(5):246-252.
Breast Med . 2015;10(5):246-252. - Brown A., Harris W., "Night feedings and infant sleep in the first year of life and their association with feeding frequency, daytime supplementation, and infant weight." Brest Med (Breastfeeding Medicine). 2015;10(5):246-252.
14 Hassiotou F et al. Maternal and infant infections stimulate a rapid leukocyte response in breastmilk. Clin Transl immunology. 2013;2(4). - Hassiot F. et al., "Infectious diseases of the mother and child stimulate a rapid leukocyte reaction in breast milk." Clean Transl Immunology. 2013;2(4):e3.
15 Li DP et al. Breastfeeding and ovarian cancer risk: a systematic review and meta-analysis of 40 epidemiological studies. Asian Pac J Cancer Prev . 2014;15(12):4829-4837. - Lee D.P. et al., "Breastfeeding and the risk of ovarian cancer: a systematic review and meta-analysis of 40 epidemiological studies.