Women hip bone
Anatomy, Function of Bones, Muscles, Ligaments
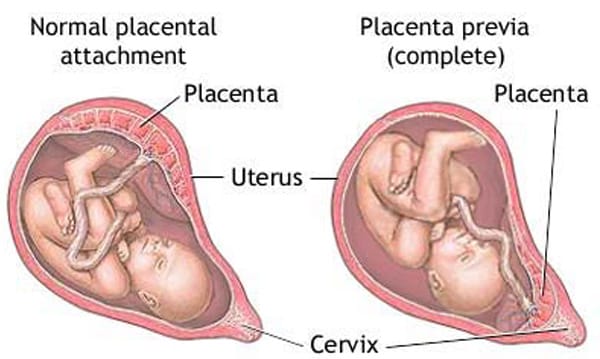
What is the female pelvis?
The pelvis is the lower part of the torso. It’s located between the abdomen and the legs. This area provides support for the intestines and also contains the bladder and reproductive organs.
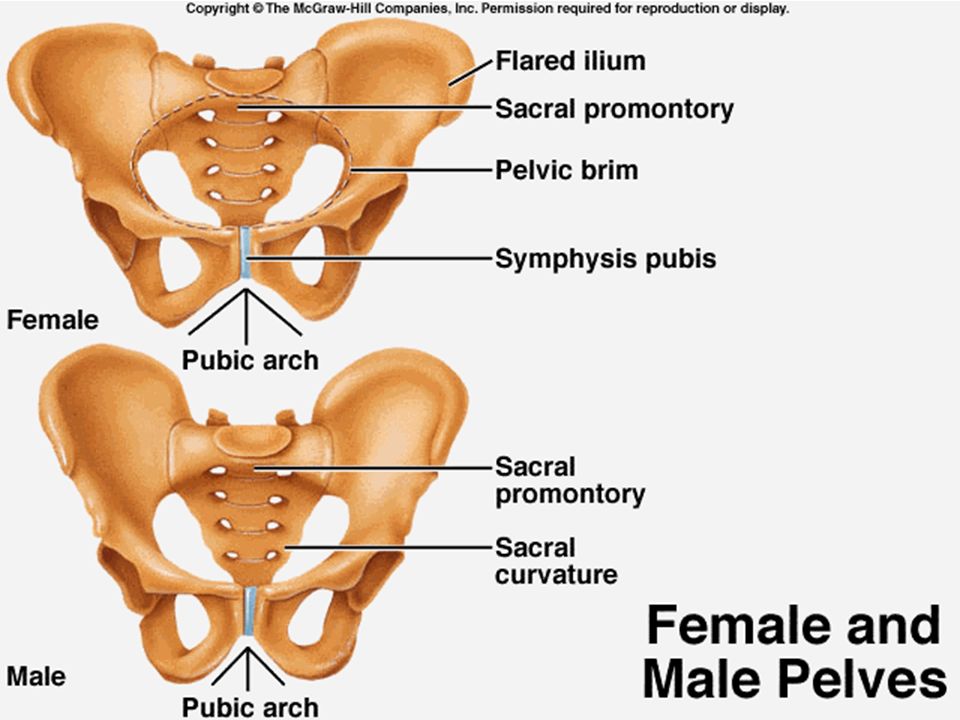
There are some structural differences between the female and the male pelvis. Most of these differences involve providing enough space for a baby to develop and pass through the birth canal of the female pelvis. As a result, the female pelvis is generally broader and wider than the male pelvis.
Below, learn more about the bones, muscles, and organs of the female pelvis.
Female pelvis anatomy and function
Female pelvis bones
Hip bones
There are two hip bones, one on the left side of the body and the other on the right. Together, they form the part of the pelvis called the pelvic girdle.
The hip bones join to the upper part of the skeleton through attachment at the sacrum. Each hip bone is made of three smaller bones that fuse together during adolescence:
- Ilium. The largest part of the hip bone, the ilium, is broad and fan-shaped. You can feel the arches of these bones when you put your hands on your hips.
- Pubis. The pubis bone of each hip bone connects to the other at a joint called the pubis symphysis.
- Ischium. When you sit down, most of your body weight falls on these bones. This is why they’re sometimes called sit bones.
The ilium, pubis, and ischium of each hip bone come together to form the acetabulum, where the head of the thigh bone (femur) attaches.
Sacrum
The sacrum is connected to the lower part of the vertebrae. It’s actually made up of five vertebrae that have fused together. The sacrum is quite thick and helps to support body weight.
Coccyx
The coccyx is sometimes called the tailbone. It’s connected to the bottom of the sacrum supported by several ligaments.
The coccyx is made up of four vertebrae that have fused into a triangle-like shape.
Female pelvis muscles
Levator ani muscles
The levator ani muscles are the largest group of muscles in the pelvis. They have several functions, including helping to support the pelvic organs.
The levator ani muscles consist of three separate muscles:
- Puborectalis. This muscle is responsible for holding in urine and feces. It relaxes when you urinate or have a bowel movement.
- Pubococcygeus. This muscle makes up most of the levator ani muscles. It originates at the pubis bone and connects to the coccyx.
- Iliococcygeus. The iliococcygeus has thinner fibers and serves to lift the pelvic floor as well as the anal canal.
Coccygeus
This small pelvic floor muscle originates at the ischium and connects to the sacrum and coccyx.
Female pelvis organs
Uterus
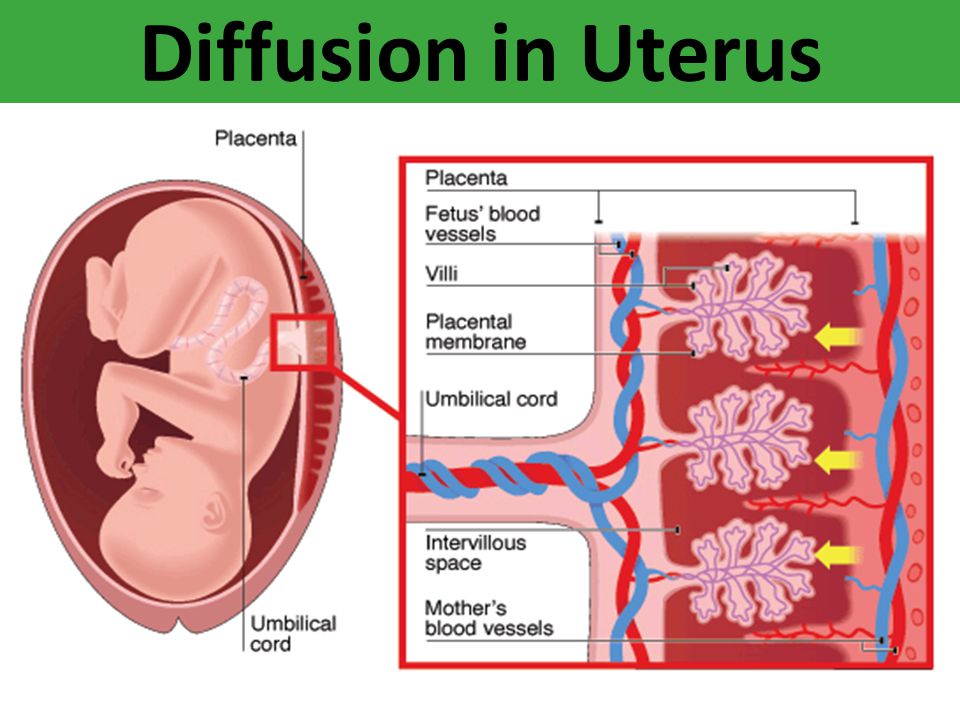
The uterus is a thick-walled, hollow organ where a baby develops during pregnancy.
During the reproductive years, the lining of the uterus sheds every month during menstruation if you don’t become pregnant.
Ovaries
There are two ovaries located on either side of the uterus. The ovaries produce eggs and also release hormones, such estrogen and progesterone.
Fallopian tubes
The fallopian tubes connect each ovary to the uterus. Specialized cells in the fallopian tubes use hair-like structures called cilia to help direct eggs from the ovaries toward the uterus.
Cervix
The cervix connects the uterus to the vagina. It’s able to widen, allowing sperm to pass into the uterus.
In addition, thick mucus produced in the cervix can help to prevent bacteria from reaching the uterus.
Vagina
The vagina connects the cervix to the exterior female genitalia. It’s also called the birth canal, as the baby passes through the vagina during delivery.
Rectum
The rectum is the lowest part of the large intestine.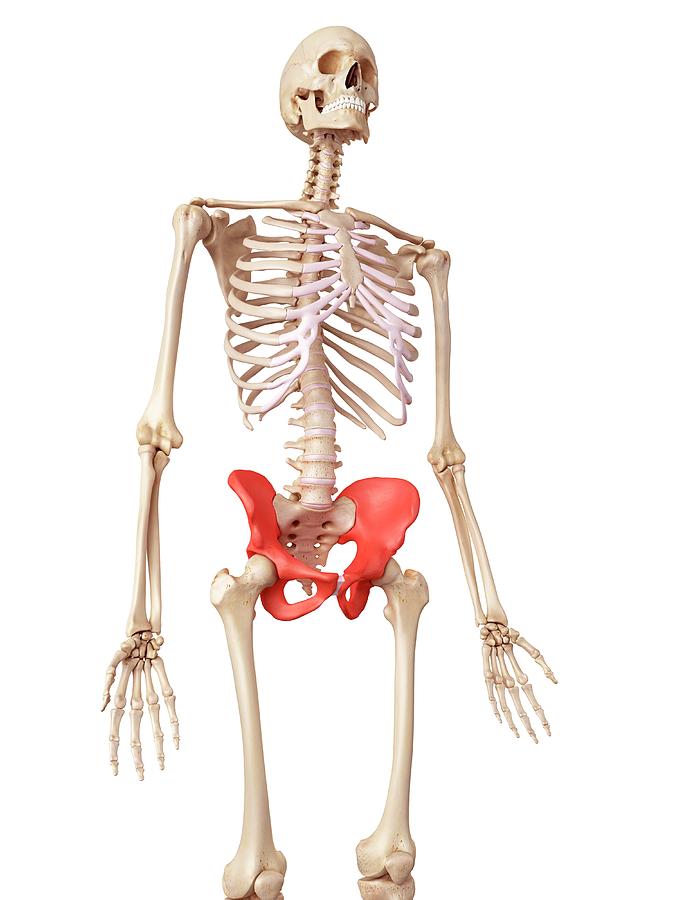 Feces collects here until exiting through the anus.
Feces collects here until exiting through the anus.
Bladder
The bladder is the organ that collects and stores urine until it’s released. Urine reaches the bladder through tubes called ureters that connect to the kidneys.
Urethra
The urethra is the tube that urine travels through to exit the body from the bladder. The female urethra is much shorter than the male urethra.
Female pelvis ligaments
Broad ligament
The broad ligament supports the uterus, fallopian tubes, and ovaries. It extends to both sides of the pelvic wall.
The broad ligament can be further divided into three components that are linked to different parts of the female reproductive organs:
- mesometrium, which supports the uterus
- mesovarium, which supports the ovaries
- mesosalpinx, which supports the fallopian tubes
Uterine ligaments
Uterine ligaments provide additional support for the uterus. Some of the main uterine ligaments include:
Some of the main uterine ligaments include:
- the round ligament
- cardinal ligaments
- pubocervical ligaments
- uterosacral ligaments
Ovarian ligaments
The ovarian ligaments support the ovaries. There are two main ovarian ligaments:
- the ovarian ligament
- the suspensory ligament of the ovary
Female pelvis diagram
Explore this interactive 3-D diagram to learn more about the female pelvis:
Female pelvis conditions
The pelvis contains a large number of organs, bones, muscles, and ligaments, so many conditions can affect the entire pelvis or parts within it.
Some conditions that can affect the female pelvis as a whole include:
- Pelvic inflammatory disease (PID). PID is an infection that occurs in the female reproductive system. While it’s often caused by a sexually transmitted infection, other infections can also cause PID. Untreated PID can lead to complications, such as infertility or ectopic pregnancy.
- Pelvic organ prolapse. Pelvic organ prolapse occurs when the muscles in the pelvis can no longer support its organs, such as the bladder, uterus, or rectum. This can cause one or more of these organs to press down on the vagina. In some cases, this can cause a bulge to form outside of the vagina.
- Endometriosis. Endometriosis occurs when the tissue that lines the inside walls of the uterus (endometrium) begins to grow outside of the uterus. The ovaries, fallopian tubes, and other tissues in the pelvis are typically affected by the condition. Endometriosis can lead to complications, including infertility or ovarian cancer.
Symptoms of a pelvic condition
Some common symptoms of a pelvic condition can include:
- pain in the lower abdomen or pelvis
- a feeling of pressure or fullness in the pelvis
- unusual or foul-smelling vaginal discharge
- pain during sex
- bleeding in between periods
- painful cramping during or before periods
- pain during bowel movements or when urinating
- a burning feeling when urinating
Tips for a healthy pelvis
The female pelvis is a complex, important part of the body. Follow these tips to keep it in good health:
Follow these tips to keep it in good health:
Stay on top of your reproductive health
See a gynecologist for a yearly health screen. Things like pelvic exams and Pap smears can aid in identifying pelvic conditions or infections early.
You can get a free or low-cost pelvic exam at your local Planned Parenthood clinic.
Practice safe sex
Use barriers — such as condoms or dental dams — during sexual activity, especially with a new partner, to avoid infections that could lead to PID.
Try pelvic floor exercises
These types of exercises can help to strengthen the muscles in the pelvis, including those around the bladder and vagina.
Stronger pelvic floor muscles can aid in preventing things like incontinence or organ prolapse. Here’s how to get started.
Never ignore unusual symptoms
If you’re experiencing anything unusual in your pelvic area, such as bleeding between periods or unexplained pelvic pain, make an appointment with your doctor. Left untreated, some pelvic conditions can have lasting impacts on your health and fertility.
Left untreated, some pelvic conditions can have lasting impacts on your health and fertility.
Anatomy, Bony Pelvis and Lower Limb, Pelvic Bones - StatPearls
Matthew D. Burgess; Forshing Lui.
Author Information
Last Update: July 25, 2022.
Introduction
The bones of the pelvis are a critical part of the central portion of the skeleton. They serve as a transition from the axial skeleton and the appendicular skeleton of the lower body, serving as an attachment point for some of the strongest muscles in the human body while withstanding the forces generated by them. The curved nature of the pelvic bone creates a closed structure, itself lined with various muscles and housing various blood supplies, lymphatic structures, nerves, and organs, including the intestines, urinary bladder, and internal sex organs.
Structure and Function
The pelvis is comprised of the large hip bone, the os coxae, on each side. The os coxae itself is composed of the ilium (the flat superior protuberance), ischium (the curved anterior protuberance), and pubis bones (the curved inferior protuberance).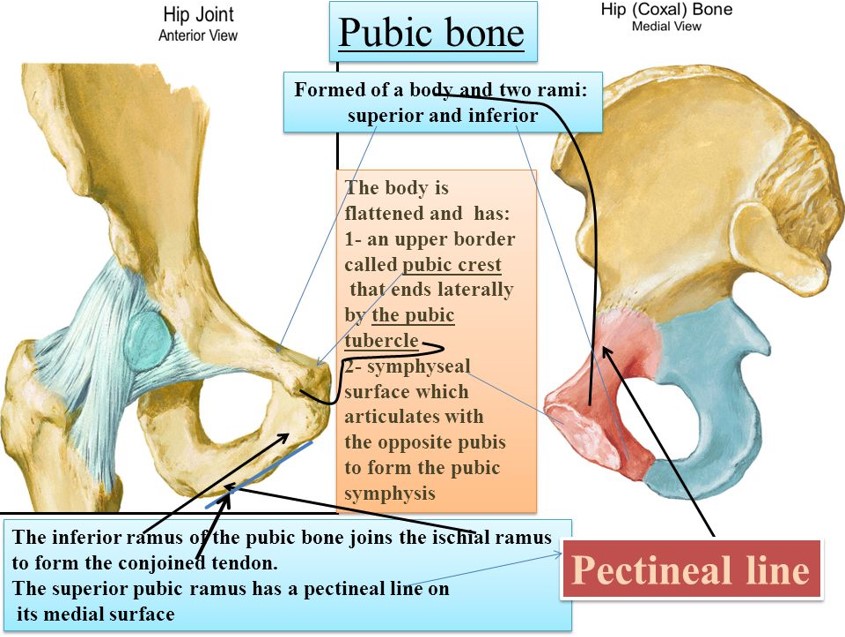 The os coxae attach anteriorly to each other at the pubic symphysis and posteriorly to each side of the sacrum, creating the sacroiliac joint. These three os coxae bones meet each other at the acetabulum, a medial structure that serves as an attachment point for the head of the femur. The pubis and ischium also articulate inferiorly at the ramal epiphyses, with their curving nature leaving an opening between them known as the obturator foramen. This foramen allows the obturator nerve to leave the pelvic cavity. Each of the pelvic bones also has many landmarks (i.e., tuberosities, notches) unique to the specific bone. The superior edge of the ilium is named the crest of the ilium, or, more commonly, the iliac crest, with a tuberosity below it on the ilium’s anterior edge known as the anterior inferior iliac spine. The ilium also has a posterior-inferior landmark known as the greater sciatic notch on it, with a subsequent lesser sciatic not being on the posterior-inferior side of the ischium.
The os coxae attach anteriorly to each other at the pubic symphysis and posteriorly to each side of the sacrum, creating the sacroiliac joint. These three os coxae bones meet each other at the acetabulum, a medial structure that serves as an attachment point for the head of the femur. The pubis and ischium also articulate inferiorly at the ramal epiphyses, with their curving nature leaving an opening between them known as the obturator foramen. This foramen allows the obturator nerve to leave the pelvic cavity. Each of the pelvic bones also has many landmarks (i.e., tuberosities, notches) unique to the specific bone. The superior edge of the ilium is named the crest of the ilium, or, more commonly, the iliac crest, with a tuberosity below it on the ilium’s anterior edge known as the anterior inferior iliac spine. The ilium also has a posterior-inferior landmark known as the greater sciatic notch on it, with a subsequent lesser sciatic not being on the posterior-inferior side of the ischium. On the anterior side of the same edge of the ischium is the tuberosity of the ischium.[1][2]
On the anterior side of the same edge of the ischium is the tuberosity of the ischium.[1][2]
The primary function of the pelvic bones is to transfer the load of the upper body onto the lower limbs while standing or walking. This function takes place through the connection of the axial and appendicular skeletons at the sacroiliac joint. When a man stands upright, the center of gravity lies in the center of the body. The pelvis transmits the weight to the femur and both lower extremities. The rigid structure of these bones also protects the organs that lie within their confinements. Such organs include the bladder, rectum, urethra, and uterus in females.[3]
Embryology
Pelvic bones begin their development as mesenchymal tissue of the embryonic lower limb buds. This mesenchyme begins extending out in three directions, corresponding to each of the three bones of the os coxae. The ischial and pubic masses migrate around the obturator nerve, fusing inferiorly to form the obturator foramen. Each pubic mass migrates medially to meet at the future pubic symphysis, while interactions with the primitive spinal column draw the iliac mass toward the sacrum derived from notochord mesenchyme. These mesenchymal masses then undergo endochondral ossification, with ilium, ischium, and pubis beginning primary ossification at third, fourth-to-fifth, and fifth-to-sixth months of gestation, respectively. Each bone’s primary center of ossification is near the future acetabulum, with the ossification process fanning out superiorly, inferiorly, and anteriorly in the direction of each bone. Sacral ossification begins in the third month, with each of the vertebrae having three centers of ossification. Secondary ossification occurs during the first year of life. Secondary ossification centers are at the articulation of the three pelvic bones in the acetabulum, the crest of the ilium, anterior inferior iliac spine, tuberosity of the ischium, symphysis pubis, and ramal epiphyses. These growth plates close during mid-puberty.
Each pubic mass migrates medially to meet at the future pubic symphysis, while interactions with the primitive spinal column draw the iliac mass toward the sacrum derived from notochord mesenchyme. These mesenchymal masses then undergo endochondral ossification, with ilium, ischium, and pubis beginning primary ossification at third, fourth-to-fifth, and fifth-to-sixth months of gestation, respectively. Each bone’s primary center of ossification is near the future acetabulum, with the ossification process fanning out superiorly, inferiorly, and anteriorly in the direction of each bone. Sacral ossification begins in the third month, with each of the vertebrae having three centers of ossification. Secondary ossification occurs during the first year of life. Secondary ossification centers are at the articulation of the three pelvic bones in the acetabulum, the crest of the ilium, anterior inferior iliac spine, tuberosity of the ischium, symphysis pubis, and ramal epiphyses. These growth plates close during mid-puberty. [1]
[1]
Blood Supply and Lymphatics
Many blood vessels are contained within the cavity created by the pelvic bones. These vessels include the common iliac artery, external and internal iliac artery, superior and inferior gluteal artery, obturator artery, superior vesical artery, and internal pudendal artery, along with their accompanying veins. Some of these arteries and their branches, such as the internal iliac, remain within the pelvic cavity while others travel out, such as the gluteals and external iliac, to supply regions such as the buttocks and lower limbs, respectively. The gonadal and uterine arteries will also run through and into the pelvic cavity, respectively, depending upon sex. Major lymph nodes in this region include the obturator, common iliac, external and internal iliac, hypogastric, superior rectal, presacral, presacral, promontory, and perirectal nodes. Nodes with the corresponding vasculature appear in pairs, one being on the anatomical left and the other on the anatomical right.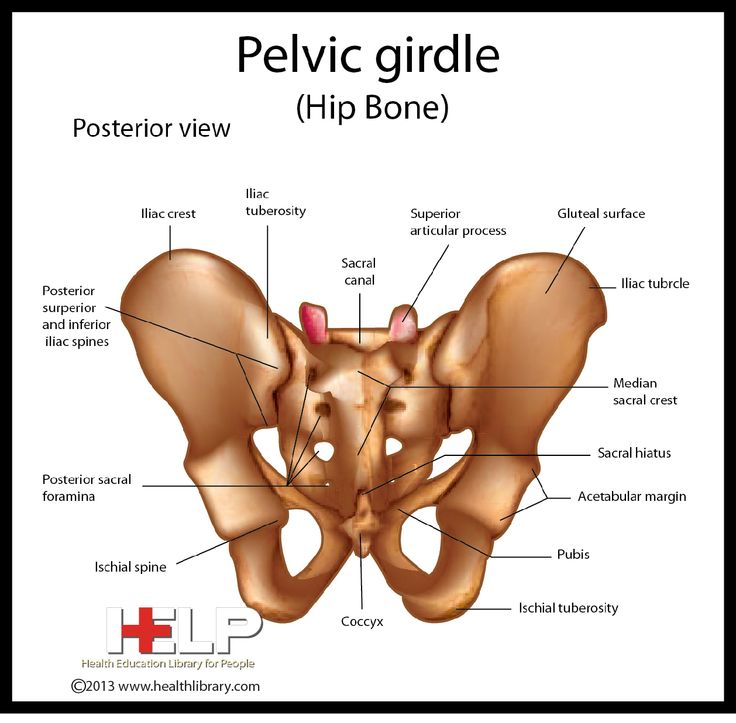 Pelvic lymph nodes are a common site of prostatic and gynecologic cancer metastasis.[4][5][6][7]
Pelvic lymph nodes are a common site of prostatic and gynecologic cancer metastasis.[4][5][6][7]
Nerves
The pelvic bones, and the girdle made by them, house nerves from the lumbar and sacral plexuses. Nerves of the lumbar plexus contained in the pelvis include the genitofemoral, lateral femoral cutaneous, obturator, and femoral nerves. The genitofemoral pierces through the psoas muscle posterior-to-anterior to reach the genital region on the anterior face of the pelvis. The lateral femoral cutaneous nerve leaves the spine and transverses the pelvis exiting under the anterior brim of the crest of the ilium to reach the thigh. The obturator nerve descends medially to the psoas to leave the pelvis through the obturator foramen. The femoral nerve runs between the psoas and the iliacus, emerging from the pelvis above the pubis to continue into the anterior thigh.[2][8]
Sacral plexus nerves of the pelvis include the sciatic, superior, and inferior gluteal, posterior femoral, and pudendal nerves.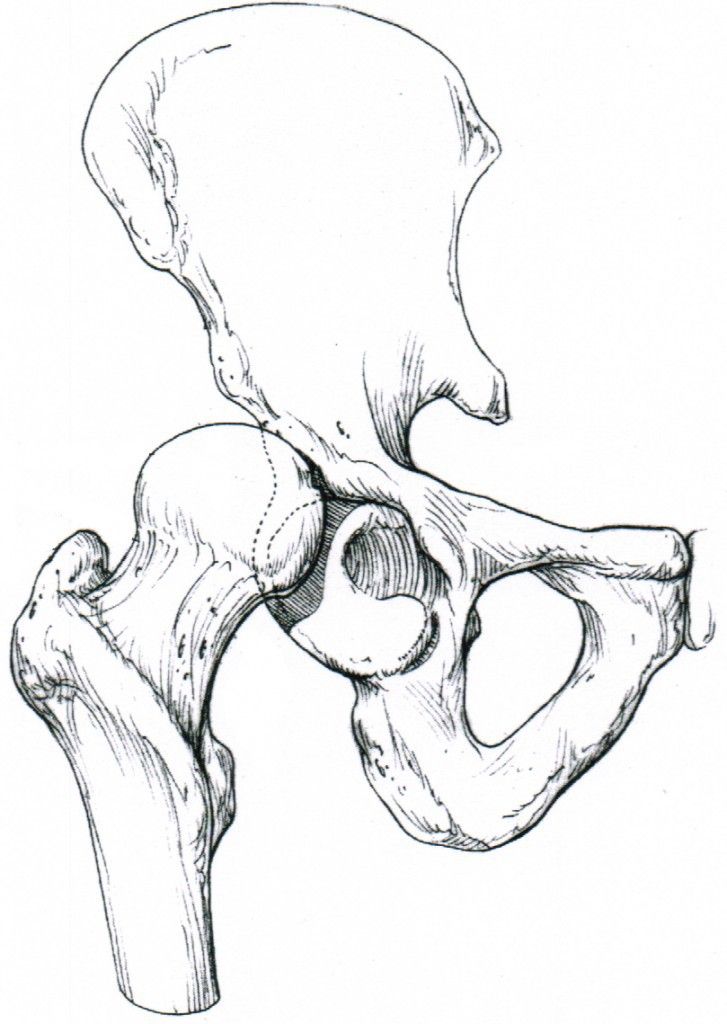 The first four of these nerves all leave the pelvis traveling under the greater sciatic notch, serving innervations on the posterior gluteal and thigh regions. The superior gluteal nerve gives innervations to the gluteus minimus and medius, while the inferior gluteal innervated the gluteus maximus, which extends the hip. The pudendal nerve travels within the pelvic girdle, sending interventions to various sphincters and genitalia structures. This nerve commonly gets injured during the vaginal delivery of children.[9]
The first four of these nerves all leave the pelvis traveling under the greater sciatic notch, serving innervations on the posterior gluteal and thigh regions. The superior gluteal nerve gives innervations to the gluteus minimus and medius, while the inferior gluteal innervated the gluteus maximus, which extends the hip. The pudendal nerve travels within the pelvic girdle, sending interventions to various sphincters and genitalia structures. This nerve commonly gets injured during the vaginal delivery of children.[9]
Muscles
The muscles around the pelvis are essential in maintaining the stability of the pelvic girdle, maintaining an erect posture, and assisting the movement of the trunk and lower extremities.
The internal iliac crest serves as the origin of the Iliacus muscle, which travels inferiorly and meets with the psoas, which originates above the pelvis but travels down through it, to make the iliopsoas. This muscle eventually exits the pelvis and inserts itself upon the femur. The piriformis is another muscle that originates inside of the pelvis and inserts externally on the femur.[10]
The piriformis is another muscle that originates inside of the pelvis and inserts externally on the femur.[10]
The pubic symphysis serves as an attachment point for both abdominal muscles, including the rectus abdominis, internal and external obliques, and transversus abdominis, as well as muscles of the adductor compartment of the leg, including the adductor brevis/longus/magnus, gracilis, and pectineus. Attached along the inferior edges of the pubis running posteriorly to the sacrum are the pelvic floor muscles, which include the puborectalis, iliococcygeal, ischiococcygeus, pubococcygeus, external anal sphincter muscles, and levator ani. The obturator internus muscles also have insertions on the internal side of the pubis and travel on the pelvic floor muscles, eventually leaving the greater sciatic notch and inserting on the posterior surface of the femur. The obturator externus travels from the anterior face of the pubis posteriorly to insert on the backside of the femur as well. The gluteal muscles, quadratus femoris, and semitendinosus muscles all also have attachments on the pelvic bones. The inguinal ligament, a common anatomical landmark involved with a hernia, runs from the anterior portion of the iliac spine to the front of the pubic symphysis.[11][12][13][14]
The gluteal muscles, quadratus femoris, and semitendinosus muscles all also have attachments on the pelvic bones. The inguinal ligament, a common anatomical landmark involved with a hernia, runs from the anterior portion of the iliac spine to the front of the pubic symphysis.[11][12][13][14]
Physiologic Variants
The pelvis in females is very different from that of males; this is very important for females to provide an adequate birth canal for the large head of the fetus during birth. To achieve these means, the female pelvis is generally broader and shallower (gynecoid shape). The birth canal has to be rounded and more spacious. The sciatic notch is much wider with shorter symphysis pubis, and the pubic bones have a much broader angle with each other. The female coccyx is more mobile, and the sacrum is shorter and less curved.
Clinical Significance
A weakness of muscles of the pelvis, such as in limb-girdle muscular dystrophy, will result in an abnormal waddling type of gait.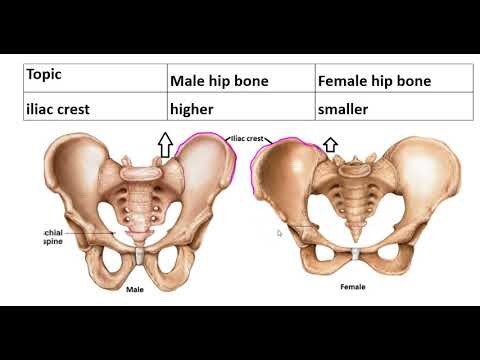 A unilateral weakness of the hip abductor muscles or subluxation of a hip joint will cause a Trendelenburg gait. An analysis of how a patient walks can give clues to the underlying problems related to the structure and function of the pelvis.
A unilateral weakness of the hip abductor muscles or subluxation of a hip joint will cause a Trendelenburg gait. An analysis of how a patient walks can give clues to the underlying problems related to the structure and function of the pelvis.
Surgeries performed on pelvic structures may be complicated by excessive bleeding or hematoma formation. Surgery may also be complicated by infection and abscess formation. In the pelvis, hematoma or abscess usually remains localized in the retroperitoneal space just in front of the iliopsoas muscles. The presentation is often related to compression of the femoral plexus or the femoral nerve in the retroperitoneal space. The patient will present with postoperative weakness of the hip flexors and knee extensors with or without the involvement of the obturator muscles, depending on whether it is compression of the femoral plexus or the femoral nerve.
A female with a male type (android) of the pelvis will encounter problems during childbirth, which is one of the most prevalent indications for a caesarian section. [15]
[15]
Review Questions
Access free multiple choice questions on this topic.
Comment on this article.
Figure
Pelvis, Male, Ilium, Arcuate Line, Pubis, Ischium, Pubis Arch, Sacrum,. Contributed by Gray's Anatomy Plates
Figure
Pelvis, Female, Pubic Arch, Brim of lesser Pelvis,. Contributed by Gray's Anatomy
Figure
Compilation of 6 images detailing anatomy of female pelvic cavity. Contributed by Gray's Anatomy Plates (Public Domain)
Figure
Pelvic nerves. Image courtesy S Bhimji MD
Figure
Pelvic bones. Image courtesy O.Chaigasame
References
- 1.
Verbruggen SW, Nowlan NC. Ontogeny of the Human Pelvis. Anat Rec (Hoboken). 2017 Apr;300(4):643-652. [PubMed: 28297183]
- 2.
Navarro-Zarza JE, Villaseñor-Ovies P, Vargas A, Canoso JJ, Chiapas-Gasca K, Hernández-Díaz C, Saavedra MÁ, Kalish RA. Clinical anatomy of the pelvis and hip. Reumatol Clin.
 2012 Dec-2013 Jan;8 Suppl 2:33-8. [PubMed: 23228531]
2012 Dec-2013 Jan;8 Suppl 2:33-8. [PubMed: 23228531]- 3.
DeLancey JO. What's new in the functional anatomy of pelvic organ prolapse? Curr Opin Obstet Gynecol. 2016 Oct;28(5):420-9. [PMC free article: PMC5347042] [PubMed: 27517338]
- 4.
Spratt DE, Vargas HA, Zumsteg ZS, Golia Pernicka JS, Osborne JR, Pei X, Zelefsky MJ. Patterns of Lymph Node Failure after Dose-escalated Radiotherapy: Implications for Extended Pelvic Lymph Node Coverage. Eur Urol. 2017 Jan;71(1):37-43. [PMC free article: PMC5571898] [PubMed: 27523595]
- 5.
Ohashi H, Kikuchi S, Aota S, Hakozaki M, Konno S. Surgical anatomy of the pelvic vasculature, with particular reference to acetabular screw fixation in cementless total hip arthroplasty in Asian population. J Orthop Surg (Hong Kong). 2017 Jan 01;25(1):2309499016685520. [PubMed: 28498719]
- 6.
Lawton CA, Michalski J, El-Naqa I, Buyyounouski MK, Lee WR, Menard C, O'Meara E, Rosenthal SA, Ritter M, Seider M.
 RTOG GU Radiation oncology specialists reach consensus on pelvic lymph node volumes for high-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2009 Jun 01;74(2):383-7. [PMC free article: PMC2905150] [PubMed: 18947938]
RTOG GU Radiation oncology specialists reach consensus on pelvic lymph node volumes for high-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2009 Jun 01;74(2):383-7. [PMC free article: PMC2905150] [PubMed: 18947938]- 7.
Charoenkwan K, Kietpeerakool C. Retroperitoneal drainage versus no drainage after pelvic lymphadenectomy for the prevention of lymphocyst formation in women with gynaecological malignancies. Cochrane Database Syst Rev. 2017 Jun 29;6:CD007387. [PMC free article: PMC6353272] [PubMed: 28660687]
- 8.
O'Rahilly R, Müller F, Meyer DB. The human vertebral column at the end of the embryonic period proper. 4. The sacrococcygeal region. J Anat. 1990 Feb;168:95-111. [PMC free article: PMC1256893] [PubMed: 2182589]
- 9.
Xiaoqiang L, Xuerong Z, Juan L, Mathew BS, Xiaorong Y, Qin W, Lili L, Yingying Z, Jun L. Efficacy of pudendal nerve block for alleviation of catheter-related bladder discomfort in male patients undergoing lower urinary tract surgeries: A randomized, controlled, double-blind trial.
 Medicine (Baltimore). 2017 Dec;96(49):e8932. [PMC free article: PMC5728874] [PubMed: 29245259]
Medicine (Baltimore). 2017 Dec;96(49):e8932. [PMC free article: PMC5728874] [PubMed: 29245259]- 10.
Cho JY, Moon H, Park S, Lee BJ, Park D. Isolated injury to the tibial division of sciatic nerve after self-massage of the gluteal muscle with massage ball: A case report. Medicine (Baltimore). 2019 May;98(19):e15488. [PMC free article: PMC6531083] [PubMed: 31083184]
- 11.
Lee SC, Endo Y, Potter HG. Imaging of Groin Pain: Magnetic Resonance and Ultrasound Imaging Features. Sports Health. 2017 Sep/Oct;9(5):428-435. [PMC free article: PMC5582693] [PubMed: 28850315]
- 12.
Otcenasek M, Krofta L, Baca V, Grill R, Kucera E, Herman H, Vasicka I, Drahonovsky J, Feyereisl J. Bilateral avulsion of the puborectal muscle: magnetic resonance imaging-based three-dimensional reconstruction and comparison with a model of a healthy nulliparous woman. Ultrasound Obstet Gynecol. 2007 Jun;29(6):692-6. [PubMed: 17523155]
- 13.
Nacion AJD, Park YY, Yang SY, Kim NK.
 Critical and Challenging Issues in the Surgical Management of Low-Lying Rectal Cancer. Yonsei Med J. 2018 Aug;59(6):703-716. [PMC free article: PMC6037599] [PubMed: 29978607]
Critical and Challenging Issues in the Surgical Management of Low-Lying Rectal Cancer. Yonsei Med J. 2018 Aug;59(6):703-716. [PMC free article: PMC6037599] [PubMed: 29978607]- 14.
Reiner CS, Weishaupt D. Dynamic pelvic floor imaging: MRI techniques and imaging parameters. Abdom Imaging. 2013 Oct;38(5):903-11. [PubMed: 22349892]
- 15.
Abitbol MM. The shapes of the female pelvis. Contributing factors. J Reprod Med. 1996 Apr;41(4):242-50. [PubMed: 8728076]
Scientists told how the shape of the female pelvis changes during life
Scientists told how the shape of the female pelvis changes during lifeThe next potential opponent of the Russian national team was named in the RFU 08:34
State Department spokesman O'Brien: US sanctions against Russia affected the course of the fighting... 08:32
Helena Bonham Carter Says She 'Hates Cancellation Culture' 08:31
The EU criticized Poland's proposal for a price ceiling for Russian oil 08:30
The United States allowed further contacts with Russia 08:30
Labor market experts announced new schemes for paying salaries to employees.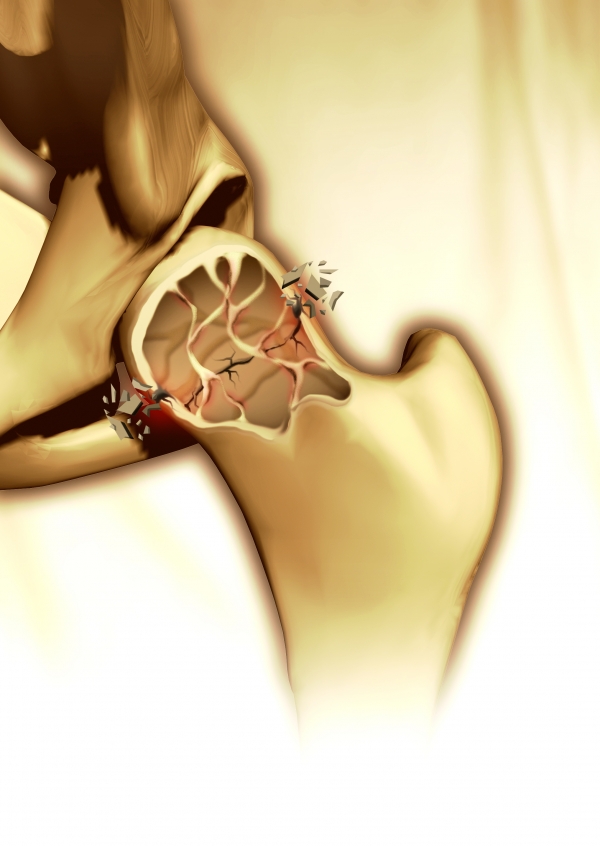 .. 08:25
.. 08:25
The construction industry announced a growing shortage of qualified specialists 08:25
In a kindergarten in Kazan, a house on a playground went underground 08:23
Actress "Margosha" Maria Berseneva will become a mother for the second time 08:22
In Krasnoyarsk, an ex-policeman who killed two pensioners was sentenced to 18 years 08:21
Science
close
100%
At the optimal age for the birth of a child, the structure of the female pelvis may change somewhat, scientists have found. Is there a solution to the "obstetric dilemma" and when the female body is most prepared for procreation, says the science department of Gazeta.Ru.
No matter how much scientists struggle to study nature, constantly improving their methods, it still remains the biggest mystery. Researchers still do not cease to be amazed at how everything is thought out and organized in the living world.
Jealousy is a reason for a medical examination
A 43-year-old Turkish woman unreasonably began to be jealous of her faithful husband, with whom she was married 20...
April 25 11:10
Anthropologists and biologists from Switzerland and Belgium, in a collaborative study, have found evidence that the shape and size of a woman's pelvis can change to adapt to having offspring. Research progress and data analysis published in the latest edition of Proceedings of the National Academy of Sciences.
The structure of the human pelvis is classified as sexually dimorphic, that is, it distinguishes males and females from each other. As a rule, the hips of women are wider and more rounded than those of men.
Studying the structure of the female skeleton, scientists put forward the hypothesis of the so-called obstetric dilemma. On the one hand, the female pelvis should be relatively wide in order to facilitate the birth of babies, which, when properly positioned in the womb, go head first. On the other hand, a narrow pelvis makes it easier for a person to walk upright. Recently, this hypothesis has been challenged on the basis of biomechanical and biocultural parameters, as well as metabolic processes. However, until the emergence of recent studies by Swiss and Belgian scientists, it remained unclear which factors are responsible for the differences in the shape and size of the pelvis in adult men and women.
On the other hand, a narrow pelvis makes it easier for a person to walk upright. Recently, this hypothesis has been challenged on the basis of biomechanical and biocultural parameters, as well as metabolic processes. However, until the emergence of recent studies by Swiss and Belgian scientists, it remained unclear which factors are responsible for the differences in the shape and size of the pelvis in adult men and women.
Weekends are not for childbirth
Tuesday is the most favorable day for the birth of a child, but on Thursday, Saturday and Sunday babies ...
November 26 14:28
Starting their scientific work, the researchers put forward the following assumption: during the course of life, the structure of the pelvis in women specially changes, facilitating the birth of children. To test their own hypothesis, a group of scientists invited 275 women of different ages up to 95 years to participate in the research. The authors of the work used the methods of computed tomography, and also engaged in geometric morphometry, that is, they analyzed the ratio of the sizes and shapes of the parts of the pelvis. The obtained data were compared with the already available data on the structure of the pelvis in men.
The obtained data were compared with the already available data on the structure of the pelvis in men.
The results obtained showed that before the onset of puberty, the structure of the pelvis in boys and girls practically does not differ, and all changes proceed in the same way.
With the onset of active sexual development, which in some girls occurs already at the age of 10 years, the change in the shape and size of the female pelvis occurs according to its own unique laws.
The processes that prepare the female body for the birth of children are completed by about 25 years. Scientists note that the period when differences in the structure of the pelvis in women and men are most noticeable coincides with the peak of fertility. According to the researchers, in women this age occurs on average from 25 to 30 years. Biologists have noticed a curious feature: at the age of 40 to 45 years, the structure of the female pelvis continues to develop, but the changes again proceed by analogy with men.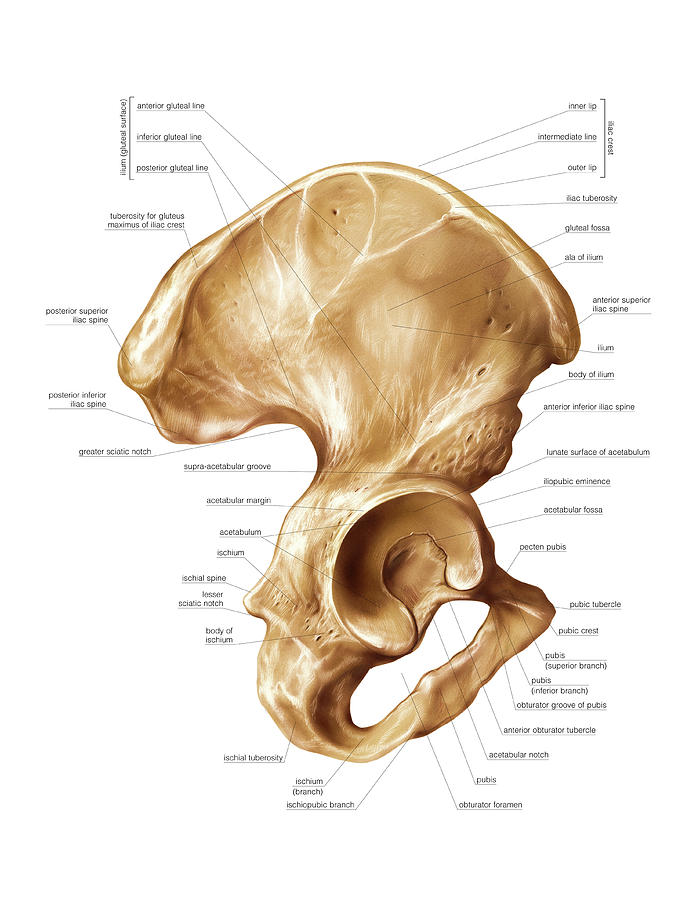 Transformations lead to a reduction in the size of the birth canal (the birth canal is a canal formed by the bones of the small pelvis and soft tissues located in it, through which the fetus and placenta pass during childbirth).
Transformations lead to a reduction in the size of the birth canal (the birth canal is a canal formed by the bones of the small pelvis and soft tissues located in it, through which the fetus and placenta pass during childbirth).
Swiss and Belgian scientists suggest that all changes in the shape and size of the female pelvis, depending on age, may be associated with the production of hormones during puberty and before menopause. According to biologists, estradiol, which is part of the group of female sex hormones - estrogen, takes the most active part. It depends on him how rounded the outlines of the female figure will be. Often, estradiol is called the "hormone of pregnancy", as it regulates blood circulation in the pelvic cavity, directs the increase in the size of the uterus, and is also responsible for the formation of the placenta.
Subscribe to Gazeta.Ru in News, Zen and Telegram.
To report a bug, select the text and press Ctrl+Enter
News
Zen
Telegram
Picture of the day
Russian military operation in Ukraine.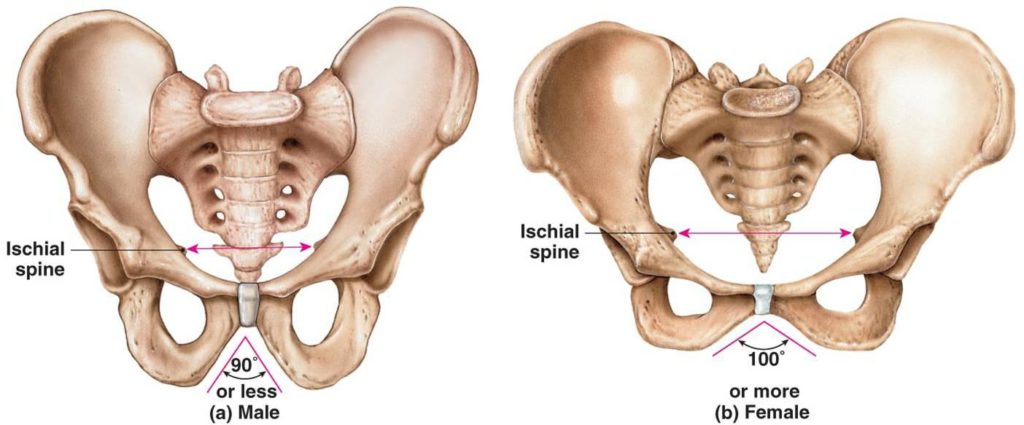 Day 278
Day 278
Online broadcast of the military special operation in Ukraine — Day 278
Eight adults, 15 children. Mass poisoning in a Polish center for Ukrainian refugees
Dozens of Ukrainians hospitalized after being poisoned in a refugee center in Poland
"Xi Jinping, go away!" People in China staged mass protests
Protests are taking place in China against the policy of zero tolerance for coronavirus
French politician accused Zelensky of wanting to start World War III
The Guardian: Kyiv risks losing US and EU support due to problems in the West
"Kommersant": citizens had difficulties with credit holidays
Congress warned of a possible collapse of the US economy due to the railroad strike
News and materials
The RFU named the next potential rival of the Russian national team
State Department spokesman O'Brien: US sanctions against Russia affected the course of fighting in Ukraine
Helena Bonham Carter said she "hates cancellation culture"
The EU criticized Poland's proposal for a price ceiling for Russian oil
The USA allowed further contacts with Russia
Labor market experts announced new schemes for paying salaries to employees abroad
The construction industry announced a growing shortage of qualified specialists
In a kindergarten in Kazan, a house on the playground went underground
Actress "Margosha" Maria Berseneva will become a mother for the second time
In Krasnoyarsk, an ex-policeman who killed two pensioners was sentenced to 18 years
Mitya Fomin was hiding in a Saturn suit at the Mask.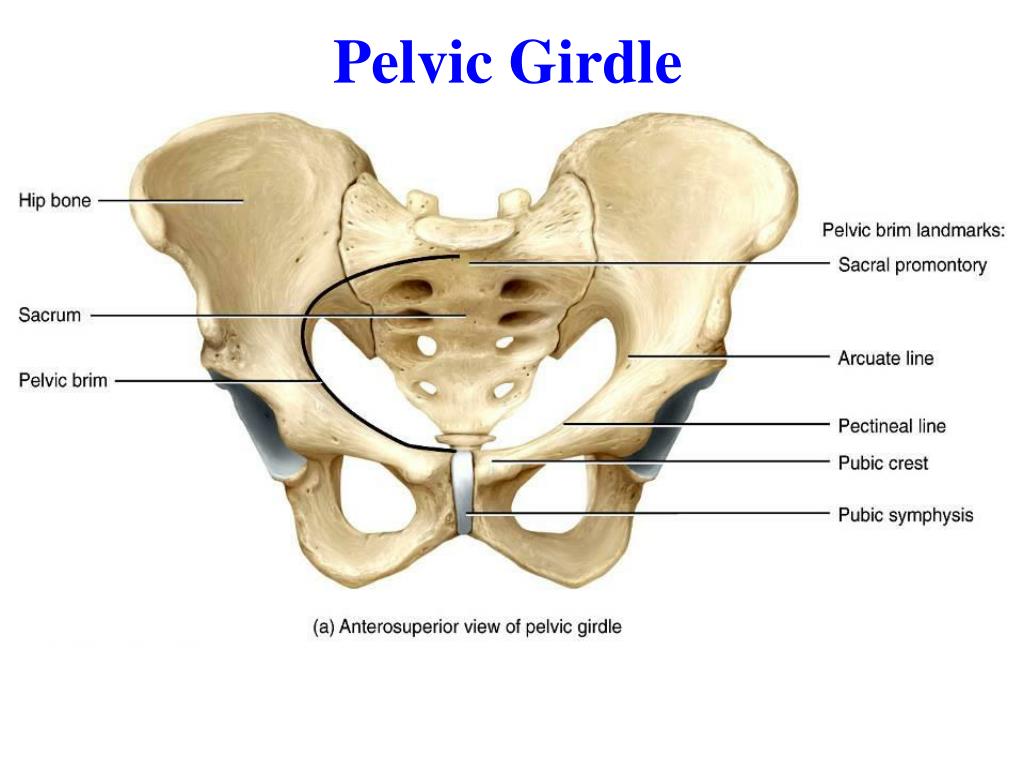 Dancing»
Dancing»
Imagine Dragons leader Dan Reynolds sparked romance rumors with 'Euphoria' actress
Laima Vaikule announced a tour of Israel
Skater Semenenko reported that he could run onto the ice in a fur coat
The State Duma Control Committee complained about the delay in the development of by-laws
"Kommersant": "Gazprom" will mothball the gas pumping equipment of "Nord Streams"
Yegor Druzhinin is not sure about the return of Alla Pugacheva to the Russian stage
In the RPL, Lovren, who plays at the World Cup, was trolled for skipping a fight in the Zenit-Spartak match
All news
“Lebanon is no longer an independent state”
How the USA and Syria deprived Beirut of its independence
“Look at yourself more often in the mirror without clothes”: how to avoid prostate cancer and impotence
Urologist Korolev dispelled the myth about the connection between prostatitis and impotence
"Professional and not corrupt.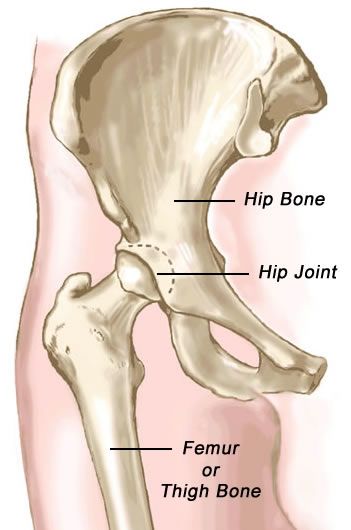 " Zhukov may replace Kudrin as head of the Accounts Chamber
" Zhukov may replace Kudrin as head of the Accounts Chamber
First Vice Speaker of the State Duma Zhukov may head the Accounts Chamber
"Significant destruction." Trains stopped for a long time in Krivoy Rog
Train traffic was stopped in Krivoy Rog after rocket attacks
Tim Burton's Wednesday: Chilling Adventures Addams
Review of Tim Burton's Wednesday series based on The Addams Family
"Almost zero". 20 out of 30 NATO countries have exhausted their resources to supply weapons to Kyiv
NYT: Most NATO countries have run out of stocks to supply weapons to Ukraine
Spartak and Zenit football players staged a mass brawl during the match
“I was told that my daughter would remain a plant, but now she is studying at the university”
Stories of foster mothers of children with developmental disabilities who would not survive in an orphanage
Hernia has nothing to do with it: how to get rid of back pain that lasts for more than a year
Doctors explained which method to choose to fight back pain
“Russia could destroy Ukraine in a day without the use of nuclear weapons”
Former White House employee Roberts: Russia can defeat Ukraine in a day without nuclear weapons
Test: Guess whose famous mother or daughter it is
Remember what celebrity mothers and daughters look like
For them, a penny, for us - a fortune: why I will not pay my friends for what my child broke
A teacher from the Moscow region - about class differences
Russian military operation in Ukraine. Day 277
Online broadcast of a military special operation in Ukraine - Day 277
Georgy Bovt
Almost like in a movie
About the fact that the methods and customs of diplomacy during the Tehran Conference can no longer be returned
Yakov Peer
Russian-style hamburger
About the new Russian fast food
Vladimir Tregubov
Who are you, Mr. Mask?
Mask?
About the Tesla creator's business path
Maria Degtereva
Abracadabra
New business vocabulary in Russian
Dmitry Samoilov
Holy World Cup
About the importance of the World Cup in Qatar
-->
See also
Error found?
Close
Thank you for your message, we will fix it soon.
Continue reading
The pelvis as a whole, its dimensions are
Updated: 11/27/2022
The pelvis (pelvis) in the form of a bone ring formed by the connection of the pelvic bones with each other and with the sacrum, serves to connect the trunk with the free lower limbs. It is divided into 2 sections: the upper, wide - the large pelvis and the lower, narrow - the small pelvis.
It is divided into 2 sections: the upper, wide - the large pelvis and the lower, narrow - the small pelvis.
Large pelvis is part of the abdominal cavity, bounded laterally by the deployed wings of the ilium. In front, it has no bony walls, and behind it is limited by the lumbar vertebrae.
The greater pelvis is separated from the lesser pelvis by a boundary line formed by the promontory, the arched edge of the ilium, the superior branches of the pubic bones, and the superior margin of the pubic symphysis. The opening thus limited is called the entrance or the upper aperture of the small pelvis, below which lies its cavity.
Anteriorly, the wall of the small pelvis is short and is formed by the pubic bones and their joints, as well as the obturator membranes. Behind the wall is long and consists of the sacrum and coccyx. The lateral walls of the small pelvis are formed by the bodies of three bones adjacent to the acetabulum, branches of the pubic and ischial bones, as well as ligaments that run from the sacrum to the ischial tuberosities and awns. The exit from the cavity of the small pelvis or the lower aperture is closed by the muscles and fascia of the perineum.
The exit from the cavity of the small pelvis or the lower aperture is closed by the muscles and fascia of the perineum.
Sex differences begin to appear at puberty. The bones of the female pelvis are smoother and thinner. The wings of the ilium in women are deployed to the sides. The upper aperture of the small female pelvis has a transverse-oval shape, while in the male pelvis it is longitudinally oval. The cape of the male pelvis protrudes more forward. The pelvic surface of the sacrum is more concave, while in women, on the contrary, the sacrum is relatively wider and at the same time more flat. The exit from the small pelvis in men is much narrower than in women. The ischial tubercles, which limit the lower aperture in women, are further apart, and the coccyx protrudes less forward. The subpubic angle in women is obtuse and arch-shaped, while in men it is more acute. The pelvic cavity in men is funnel-shaped, in women the pelvis is cylindrical.
Skeleton of the free lower limb
The free lower limb consists of the following parts: femur, tibia and foot. The skeleton of these departments is formed by the femur, two bones of the lower leg and the bones of the foot. On the lower limb is the largest sesamoid bone - the patella.
The skeleton of these departments is formed by the femur, two bones of the lower leg and the bones of the foot. On the lower limb is the largest sesamoid bone - the patella.
Femur
The femur (femur) is the largest tubular bone in the human skeleton. It refers to the long levers of movement.
At the proximal end of the femur is the articular head, which has a round shape. There is a small rough fossa on it - the place of attachment of the ligament of the femoral head. Lateral to the head is the neck, which forms an obtuse angle with the axis of the femoral body. On the border of the neck and body of the femur, there are two bony protrusions called the greater and lesser skewers. Muscles are attached to them. In front, the skewers are connected by an intertrochanteric line, and behind - by an intertrochanteric ridge. The body of the femur is somewhat convex anteriorly and has a triangular-rounded shape; on its back side there is a trace of attachment of the thigh muscles - a rough line consisting of two lips - lateral and medial.![]()
The distal end of the femur is thickened and bears two round, folded back, lateral and medial condyles. With a strictly vertical position of the femur, the medial condyle protrudes more downward than the lateral one. But, since in its natural position the femur is oblique, and its lower end is closer to the midline than the upper one, the condyles are on the same level. On the anterior surface of the condyles is a slight concavity for the patella. Posteriorly and inferiorly, the condyles are separated by a deep intercondylar fossa. On the side of each condyle above its articular surface is a rough epicondyle.
Pelvic bones, their structure, connections. Taz in general. age and gender characteristics. dimensions.
The pelvic bones and the sacrum, connecting with the help of the sacroiliac joints and the pubic symphysis, form the pelvis, pelvis. . The pelvis is a bone ring, inside of which there is a cavity containing internal organs: the rectum, bladder, etc. With the participation of the pelvic bones, the trunk is also connected to the free lower limbs.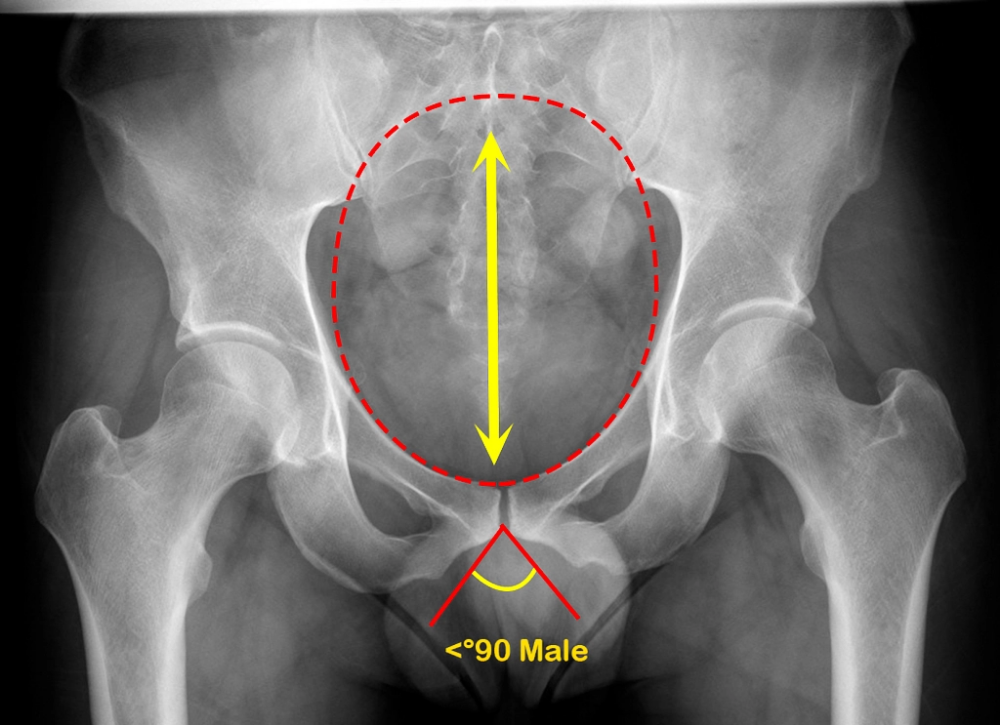 The pelvis is divided into two sections: upper and lower. The upper section is the large pelvis, and the lower section is the small pelvis. The large pelvis is separated from the small pelvis by a boundary line, which is formed by the cape of the sacrum, the arcuate line of the ilium, the crests of the pubic bones and the upper edges of the pubic symphysis.
The pelvis is divided into two sections: upper and lower. The upper section is the large pelvis, and the lower section is the small pelvis. The large pelvis is separated from the small pelvis by a boundary line, which is formed by the cape of the sacrum, the arcuate line of the ilium, the crests of the pubic bones and the upper edges of the pubic symphysis.
The large pelvis, pelvis major, is bounded behind by the body of the fifth lumbar vertebra, on the sides by the wings of the ilium. In front, the large pelvis has no bony walls. The pelvic cavity is the lower part of the abdominal cavity.
The small pelvis, pelvis minor, is a narrowed downward bone canal (cavity). The upper opening of this canal, the upper pelvic aperture, apertura pelvis superior, is the entrance to the small pelvis and is limited by the boundary line. The exit from the small pelvis is the lower pelvic aperture, apertura pelvis inferior, limited behind by the coccyx, on the sides by the sacrotuberous ligaments, ischial tubercles, branches of the ischial bones, lower branches of the pubic bones, and in front by the lower branches of the pubic bones. The posterior wall of the pelvic cavity is formed by the pelvic surface of the sacrum and the anterior surface of the coccyx. The anterior wall is represented by the lower and upper branches of the pubic bones and the pubic symphysis. From the sides, the cavity of the small pelvis is limited by the inner surface of the pelvic bones below the border line, sacrotuberous and sacrospinous ligaments. On the right and on the left there are obturator openings, each closed by a fibrous plate - the obturator membrane, membrdna obturatoria, which is the ligament of the pelvic bone itself.
The posterior wall of the pelvic cavity is formed by the pelvic surface of the sacrum and the anterior surface of the coccyx. The anterior wall is represented by the lower and upper branches of the pubic bones and the pubic symphysis. From the sides, the cavity of the small pelvis is limited by the inner surface of the pelvic bones below the border line, sacrotuberous and sacrospinous ligaments. On the right and on the left there are obturator openings, each closed by a fibrous plate - the obturator membrane, membrdna obturatoria, which is the ligament of the pelvic bone itself.
Connected by the pubic symphysis, the lower branches of the pubic bones close the pelvic ring in front.
In the structure of the pelvis of an adult, sexual characteristics are clearly expressed. The pelvis in women is lower and wider than in men. The distance between the spines and iliac crests in women is greater, since the wings of the iliac bones are more deployed to the sides. Thus, the cape in women protrudes less than in men, so the upper aperture of the female pelvis is more rounded than that of the male. In women, the sacrum is wider and shorter than in men, the ischial tuberosities are turned to the sides, the distance between them is greater than in men. The angle of convergence of the lower branches of the pubic bones in women is more than 90° (pubic arch), and in men it is 70-75° (subpubic angle).
In women, the sacrum is wider and shorter than in men, the ischial tuberosities are turned to the sides, the distance between them is greater than in men. The angle of convergence of the lower branches of the pubic bones in women is more than 90° (pubic arch), and in men it is 70-75° (subpubic angle).
The size and shape of the pelvis are of great importance for the birth process. Knowing the average size of the entrance and exit from the small pelvis is necessary to predict the course of labor. Direct The size of the entrance to the small pelvis - true, or gynecological, conjugate, conjugdta vera, seu conjugata gyneco-°gi-ca (Fig. 93, 94), usually equal to 11 cm, is the distance between the cape and the most protruding posterior point pubic symphysis.
The transverse diameter, diameter transversa, of the entrance to the small pelvis is the distance between the most distant points of the boundary line that delimits the small pelvis from the large one. This size is about 13 cm. The oblique diameter, diameter obliqua, of the entrance to the small pelvis is 12 cm. It is the distance between the sacroiliac joint, on the one hand, and the iliopubic eminence, on the other.
The oblique diameter, diameter obliqua, of the entrance to the small pelvis is 12 cm. It is the distance between the sacroiliac joint, on the one hand, and the iliopubic eminence, on the other.
The right direction and size of the exit from the cavity of the small pelvis is equal to the distance between the inner edges of the ischial tuberosities (11 cm). The dimensions of the large pelvis are also of practical importance, namely the distance between the two upper anterior iliac spines - distantia spindrum, which is 25-27 cm, and the distance between the most distant points of the wings of the ilium - distantia cristarum - 28-30 cm.
Pelvis as a whole. Age and sex differences, the size of the female pelvis.
The pelvis is generally divided into large and small along the border through the sacral promontory (formed by the anterior part of the base of the sacrum and the body of the Y lumbar vertebra), through the arcuate lines of the ilium, crests of the pubic bones and the upper edge of the pubic symphysis - the entire border is called the boundary line.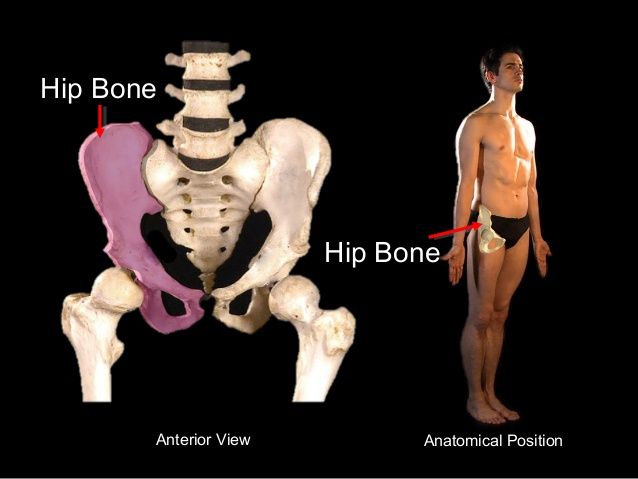 The cavity the pelvis is occupied by internal organs and muscles, from below it is limited by the pelvic and urogenital diaphragms. Outside the pelvis are the muscles of the lower girdle.
The cavity the pelvis is occupied by internal organs and muscles, from below it is limited by the pelvic and urogenital diaphragms. Outside the pelvis are the muscles of the lower girdle.
In the small pelvis, there are: the upper aperture (inlet), the cavity with wide and narrow parts, the lower aperture (outlet). The upper aperture coincides with the borderline, the lower one passes behind through the top of the coccyx, on the sides through the sacrotuberous ligaments, ischial tubercles, ischial branches, in front along the edge of the inferior pubic branches and the lower edge of the pubic symphysis. On the front wall of the small pelvis there are obturator openings with the same canals, on the side walls - large and small ischial openings, limited by the same bone notches and sacrotuberous, sacrospinous ligaments.
Age differences in the structure of the pelvis are determined by changes in the angle of inclination and the degree of curvature of the sacrum and coccyx. Individual fluctuations in the angle of inclination of the pelvis (for men - within 50-55 o, for women - 55-60 o) vary depending not only on gender, but also on the position of the body. In a sports or military stance, the angle of inclination increases as much as possible, in a sitting position it decreases as much as possible. Significant age-related fluctuations are also observed in terms of ossification of the bones of the pelvic ring.
Individual fluctuations in the angle of inclination of the pelvis (for men - within 50-55 o, for women - 55-60 o) vary depending not only on gender, but also on the position of the body. In a sports or military stance, the angle of inclination increases as much as possible, in a sitting position it decreases as much as possible. Significant age-related fluctuations are also observed in terms of ossification of the bones of the pelvic ring.
Gender differences are manifested in the following:
female pelvis, and especially its cavity, wide and low, with a cylindrical shape; male - narrow and high with a conical cavity;
· women's promontory protrudes slightly into the cavity, forming an oval-shaped entrance; the cape in men protrudes strongly, forming an entrance in the form of a card heart;
female sacrum is wide and short with a slightly concave, almost flat pelvic surface; male - narrow and long, strongly curved along the pelvic surface;
subpubic angle in women - more than 90 degrees, in men - 70-75 degrees;
· the wings of the ilium in women are more turned outward, and in men they have a more vertical position;
The linear dimensions of the female pelvis predominate over those of men.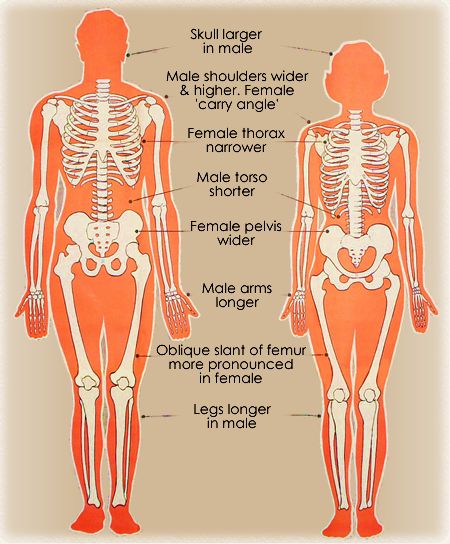
In the large pelvis in women, three transverse and one longitudinal dimensions are distinguished:
· interspinous dimension, as a direct distance of 23-25 cm between the anterior superior iliac spines;
intercrest dimension, as a straight distance of 26-28 cm between the most distant points of the iliac crests;
intertrochanteric size, as a straight distance of 30-33 cm between the most distant points of the greater trochanters;
All dimensions of the large pelvis are measured with a thickness caliper in a living woman, since these bone formations are easily palpable. By the size of the large pelvis and its shape, one can indirectly judge the shape of the small pelvis.
In the small pelvis, transverse, oblique, longitudinal dimensions (diameters) are distinguished, which in each part of the pelvis (upper, lower apertures, cavity) are also measured between certain bone landmarks. So, for example, the transverse diameter of the entrance is the distance of 12-13 cm between the most distant points of the arcuate line on the ilium; oblique diameter - a distance of 12 cm between the sacroiliac joint of one side and the iliac-pubic eminence of the opposite side; direct size of 11 cm, as the distance between the cape and the most protruding posterior point of the pubic symphysis.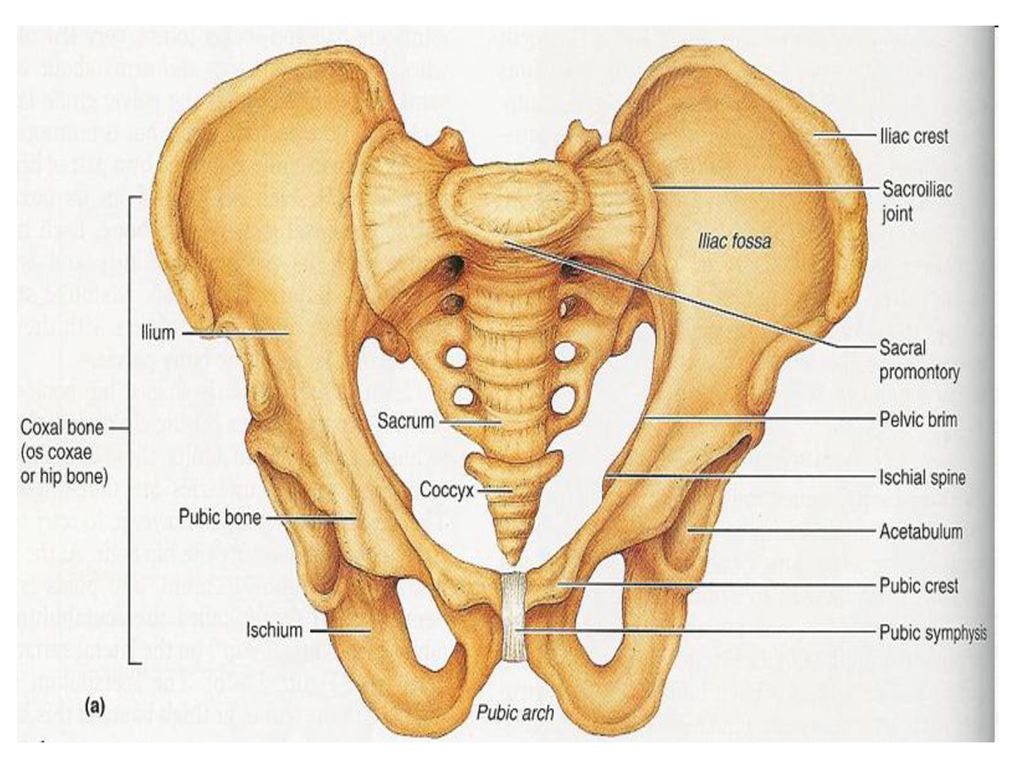 Direct exit size of 9cm is the distance between the tip of the coccyx and the lower edge of the pubic symphysis; the transverse size of the outlet is 11 cm - the distance between the ischial tubercles. If you connect the midpoints of all direct sizes, you get a wire axis of the small pelvis - a gentle curve, concave facing the symphysis. This is the direction of movement of the child being born.
Direct exit size of 9cm is the distance between the tip of the coccyx and the lower edge of the pubic symphysis; the transverse size of the outlet is 11 cm - the distance between the ischial tubercles. If you connect the midpoints of all direct sizes, you get a wire axis of the small pelvis - a gentle curve, concave facing the symphysis. This is the direction of movement of the child being born.
The pelvis as a whole
The pelvis (Fig. . 9) is formed by two pelvic bones, the sacrum with the coccyx and their joints. It is a container and protection for many internal organs: the uterus, bladder, rectum, etc. The pelvis is divided by the boundary line into the small and large pelvis. The large pelvis is bounded by the wings of the ilium, the small pelvis by the ischium and pubic bones, sacrum, coccyx, pubic symphysis, ligaments of the pelvis and obturator membranes. Allocate age and sex differences in the structure of the pelvis. The female pelvis is much wider and shorter than the male. This is achieved by the development of the wings of the ilium, a flatter sacrum, an increase in the subpubic angle (obtuse in women), etc. Anatomical data on the structural features and dimensions of the female pelvis are taken into account in obstetrics.
This is achieved by the development of the wings of the ilium, a flatter sacrum, an increase in the subpubic angle (obtuse in women), etc. Anatomical data on the structural features and dimensions of the female pelvis are taken into account in obstetrics.
9. Dimensions of the female pelvis (cut in the sagittal plane): 1 - straight diameter (exit from the small pelvis), 2 - pelvic tilt angle, 3 - diagonal conjugate, 4 - straight diameter (pelvic cavity), 5 - true (gynecological) conjugate , 6 - anatomical conjugate (direct size of the entrance to the small pelvis), 7 - large sciatic foramen, 8 - sacrospinous ligament, 9 - small sciatic foramen, 10 - sacrotuberous ligament.
Hip joint (art. coxae) - fig. 10.
10. Hip joint, opened frontally: 1 - femoral head, 2 pelvic bone, 3 - articular cartilage, 4 - articular cavity, 5 - femoral head ligament, 6 - transverse acetabular ligament, 7 - articular capsule, 8 - circular zone , 9 - acetabular lip.
Classification. Simple, bowl-shaped, multi-axial joint.
Structure. Formed by the acetabulum of the pelvis and the head of the femur. Articular cavity increases cartilaginous lip, labrum acetabulare. The capsule is attached along the circumference of the acetabulum, and on the femur - along the intertrochanteric line (in front) and along the neck of the femur parallel to the intertrochanteric crest (rear). Inside the joint cavity is located a ligament of the femoral head , which connects the head with the notch of the acetabulum, strengthens the joint, softens shocks during movement, conducts blood vessels to the femoral head. External ligaments of the joint: iliofemoral, pubic-femoral, ischio-femoral, circular zone (ligg. iliofemorale, pubofemorale, ischiofemorale, zona orbicularis).
Functions .It allows movements around three axes, but their volume is less than in the shoulder joint. Flexion and extension are possible around the frontal axis: when flexed, the thigh moves forward and presses against the stomach (such maximum flexion is possible due to the features of the fastening of the synovial membrane of the joint capsule - it does not attach to the femur from behind), while extending the thigh moves back.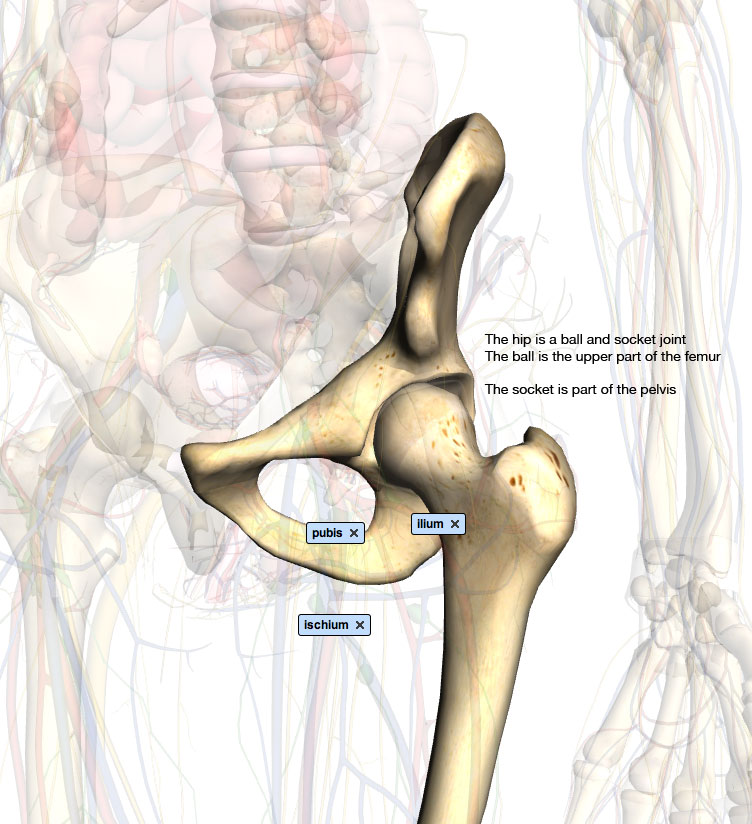 Around the sagittal axis, the leg is adducted and abducted relative to the midline of the body. Rotation (inward and outward) is possible around the vertical axis.
Around the sagittal axis, the leg is adducted and abducted relative to the midline of the body. Rotation (inward and outward) is possible around the vertical axis.
Knee joint (art. genus) - fig. 11.
Classification. The joint is complex, complex, condylar in shape, biaxial.
Structure. One of the largest and most complex human joints. It is formed by the articular surfaces of the condyles and the patella surface of the femur, the upper articular surface of the tibia and the articular surface of the patella, articulating only with the femur. The capsule is attached along the edges of the articular surfaces of the patella, condyles of the femur and tibia. The joint is supplemented with intra-articular cartilage: lateral and medial menisci (meniscus lateralis et medialis). The shape of the lateral and medial menisci is different, they increase the congruence of the articulating bones, provide reliability in support, and improve the biomechanical capabilities of the joint.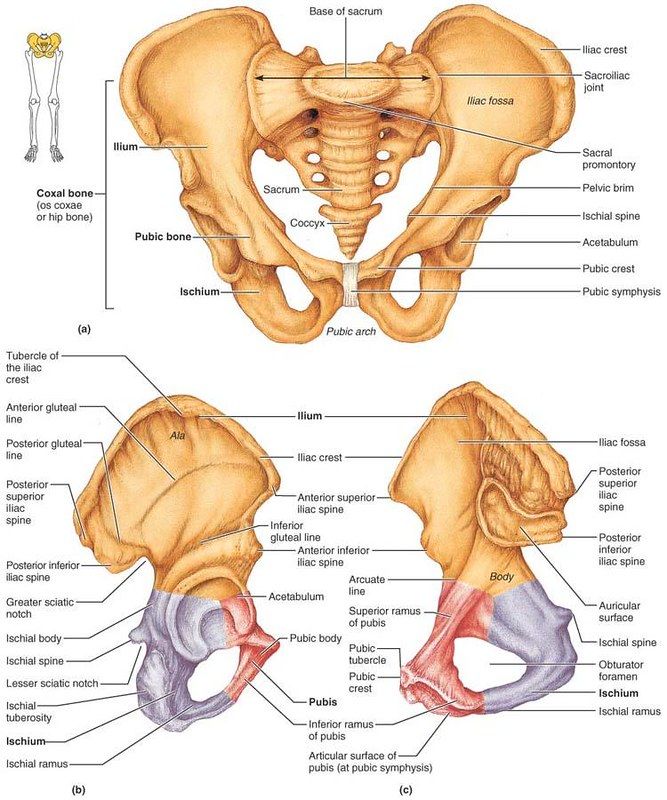 The anterior horns of the menisci are interconnected by transverse ligament of the knee, lig. transversum genus . The knee joint has many synovial bags, the main of which are suprapatellar, deep subpatellar and prepatellar bursae complex. Strengthened by ligaments: internal - anterior and posterior cruciate (ligg. cruciata genus anterius et posterius) and external - collateral tibia and fibula (ligg. collaterale tibiale et fibulare). The patella has its own ligament - lig. patellae.
The anterior horns of the menisci are interconnected by transverse ligament of the knee, lig. transversum genus . The knee joint has many synovial bags, the main of which are suprapatellar, deep subpatellar and prepatellar bursae complex. Strengthened by ligaments: internal - anterior and posterior cruciate (ligg. cruciata genus anterius et posterius) and external - collateral tibia and fibula (ligg. collaterale tibiale et fibulare). The patella has its own ligament - lig. patellae.
11. Knee joint, right. Opened. Front view. The joint capsule has been removed. 1 - patellar surface, 2 - lateral condyle, 3 - medial condyle, 4 - posterior cruciate ligament, 5 - anterior cruciate ligament, 6 - transverse ligament of the knee, 7 - medial meniscus, 8 - tibial collateral ligament, 9- ligament of the patella, 10 - patella, 11 - head of the fibula, 12 - tibiofibular joint (anterior ligament of the head of the patella), 13 - lateral condyle of the tibia, 14 - lateral meniscus, 15 - peroneal collateral ligament.
Functions .The joint can move around two axes: frontal and vertical. Around the frontal axis, flexion and extension of the lower leg occurs. Around the vertical axis (subject to knee flexion), rotation of the lower leg is possible.
Anatomy: The pelvis as a whole, its dimensions
In the formation of the pelvis, pelvis, the pelvic bones, the sacrum with the coccyx and the ligamentous apparatus take part (see Fig. 40). The pelvis is divided into large, pelvis major, and small, pelvis minor. The border between them is the border line, linea terminalis, running from the cape to the arcuate line and further to the pubic tubercle. The small pelvis has two openings: the upper one, apertura pelvis superior, limited by the boundary line, and the lower one, apertura pelvis inferior, bounded behind by the coccyx, from the sides by the ischial tubercles, sacrotuberous and sacrospinous ligaments, in front by the branches of the ischial and pubic bones.
There are two extreme forms of the structure of the female pelvis: one form is characterized by a predominance of the longitudinal size, the other - the transverse. The size of the male pelvis is 1.5-2 cm smaller than the female one. Deviations in the size of the pelvis depend on the age, body type and size of the subject. Individual features of the external differences in the pelvis may relate to the shape and size of the sacrum, innominate bones, the degree of severity of the cape of the sacrum, etc. Various painful conditions have a great influence on the shape of the pelvis - rickets, spinal deformity, etc. Age-related differences in the pelvis depend on the angle of inclination of the pelvis and degree of curvature of the sacrum.
The size of the male pelvis is 1.5-2 cm smaller than the female one. Deviations in the size of the pelvis depend on the age, body type and size of the subject. Individual features of the external differences in the pelvis may relate to the shape and size of the sacrum, innominate bones, the degree of severity of the cape of the sacrum, etc. Various painful conditions have a great influence on the shape of the pelvis - rickets, spinal deformity, etc. Age-related differences in the pelvis depend on the angle of inclination of the pelvis and degree of curvature of the sacrum.
See also:
- Insulin in myocardial infarction and diabetes mellitus. The value of glucose-insulin mixture in diabetes and heart attack
- Access, subchondroplasty technique of the knee
- Problems of the organization of pulmonary surgery. Relationship between thoracic surgery and oncology
- Economic evaluation in medicine. Healthcare inputs and outputs
- Bay oil benefits for hair.