Why is high blood pressure bad during pregnancy
High Blood Pressure During Pregnancy
- What are high blood pressure complications during pregnancy?
- What should I do if I have high blood pressure before, during, or after pregnancy?
- What are types of high blood pressure conditions before, during, and after pregnancy?
- More Information
Some women have high blood pressure during pregnancy. This can put the mother and her baby at risk for problems during the pregnancy. High blood pressure can also cause problems during and after delivery.1,2 The good news is that high blood pressure is preventable and treatable.
High blood pressure, also called hypertension, is very common. In the United States, high blood pressure happens in 1 in every 12 to 17 pregnancies among women ages 20 to 44.3
High blood pressure in pregnancy has become more common. However, with good blood pressure control, you and your baby are more likely to stay healthy.
The most important thing to do is talk with your health care team about any blood pressure problems so you can get the right treatment and control your blood pressure—before you get pregnant. Getting treatment for high blood pressure is important before, during, and after pregnancy.
What are high blood pressure complications during pregnancy?
Complications from high blood pressure for the mother and infant can include the following:
- For the mother: preeclampsia, eclampsia, stroke, the need for labor induction (giving medicine to start labor to give birth), and placental abruption (the placenta separating from the wall of the uterus).1,4,5
- For the baby: preterm delivery (birth that happens before 37 weeks of pregnancy) and low birth weight (when a baby is born weighing less than 5 pounds, 8 ounces).1,6 The mother’s high blood pressure makes it more difficult for the baby to get enough oxygen and nutrients to grow, so the mother may have to deliver the baby early.
Discuss blood pressure problems with your health care team before, during, and after pregnancy.
Learn what to do if you have high blood pressure before, during, or after pregnancy.
What should I do if I have high blood pressure before, during, or after pregnancy?
Before Pregnancy
- Make a plan for pregnancy and talk with your doctor or health care team about the following:
- Any health problems you have or had and any medicines you are taking. If you are planning to become pregnant, talk to your doctor.7 Your doctor or health care team can help you find medicines that are safe to take during pregnancy.
- Ways to keep a healthy weight through healthy eating and regular physical activity.1,7
During Pregnancy
- Get early and regular prenatal care. Go to every appointment with your doctor or health care professional.
- Talk to your doctor about any medicines you take and which ones are safe.
 Do not stop or start taking any type of medicine, including over-the-counter medicines, without first talking with your doctor.7
Do not stop or start taking any type of medicine, including over-the-counter medicines, without first talking with your doctor.7 - Keep track of your blood pressure at home with a home blood pressure monitor. Contact your doctor if your blood pressure is higher than usual or if you have symptoms of preeclampsia. Talk to your doctor or insurance company about getting a home monitor.
- Continue to choose healthy foods and keep a healthy weight.8
After Pregnancy
- Pay attention to how you feel after you give birth. If you had high blood pressure during pregnancy, you have a higher risk for stroke and other problems after delivery. Tell your doctor or call 9-1-1 right away if you have symptoms of preeclampsia after delivery. You might need emergency medical care.9,10
What are types of high blood pressure conditions before, during, and after pregnancy?
Your doctor or nurse should look for these conditions before, during, and after pregnancy:1,11
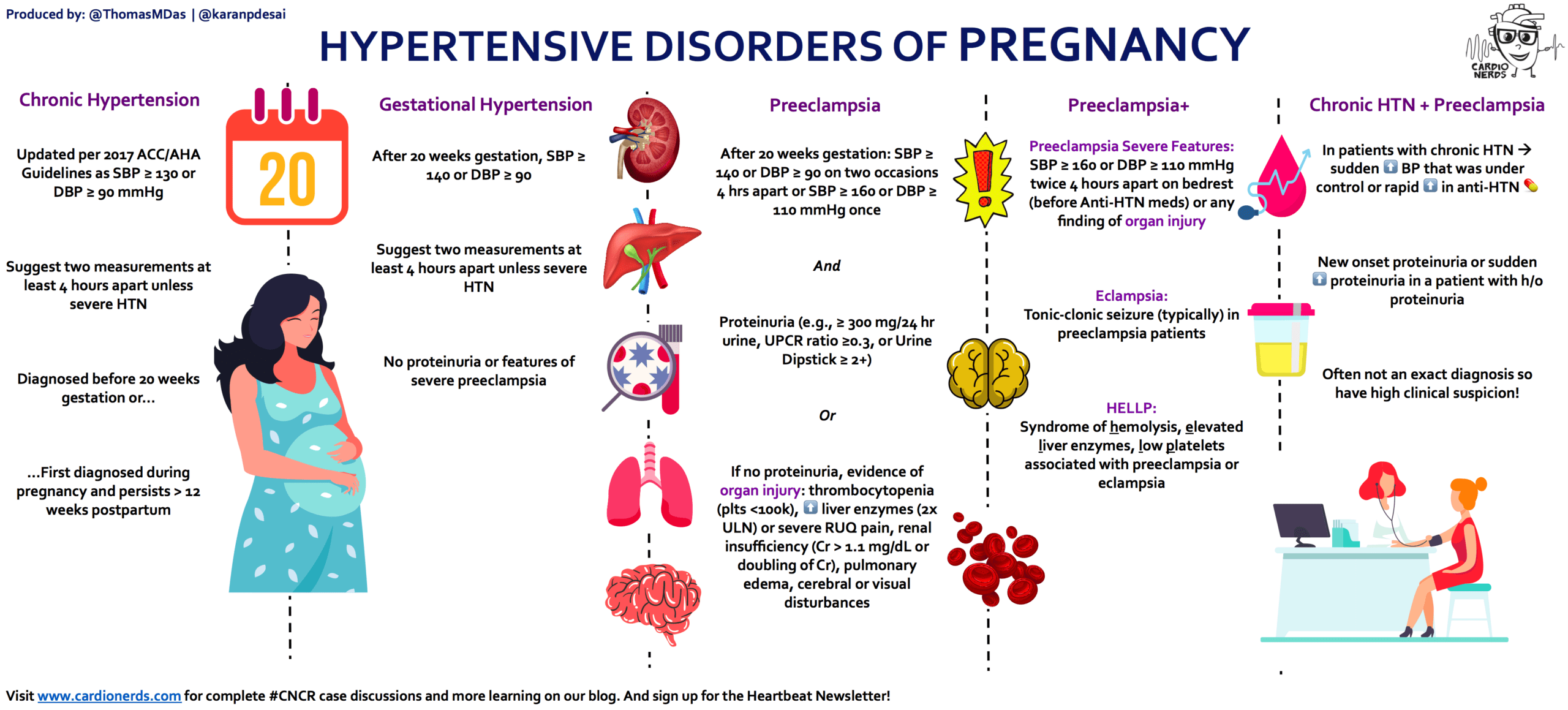
Chronic Hypertension
Chronic hypertension means having high blood pressure* before you get pregnant or before 20 weeks of pregnancy.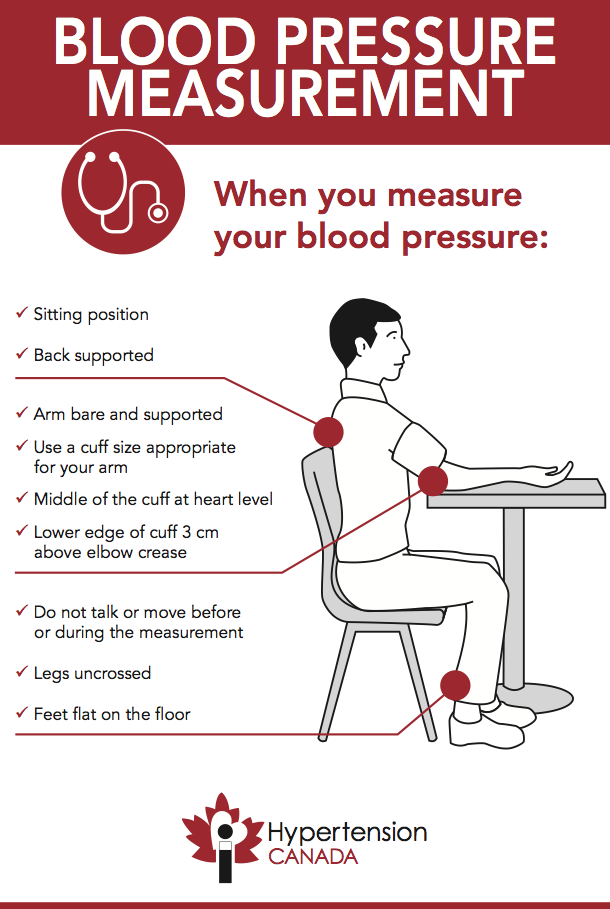 1 Women who have chronic hypertension can also get preeclampsia in the second or third trimester of pregnancy.1
1 Women who have chronic hypertension can also get preeclampsia in the second or third trimester of pregnancy.1
Gestational Hypertension
This condition happens when you only have high blood pressure* during pregnancy and do not have protein in your urine or other heart or kidney problems. It is typically diagnosed after 20 weeks of pregnancy or close to delivery. Gestational hypertension usually goes away after you give birth. However, some women with gestational hypertension have a higher risk of developing chronic hypertension in the future.1,12
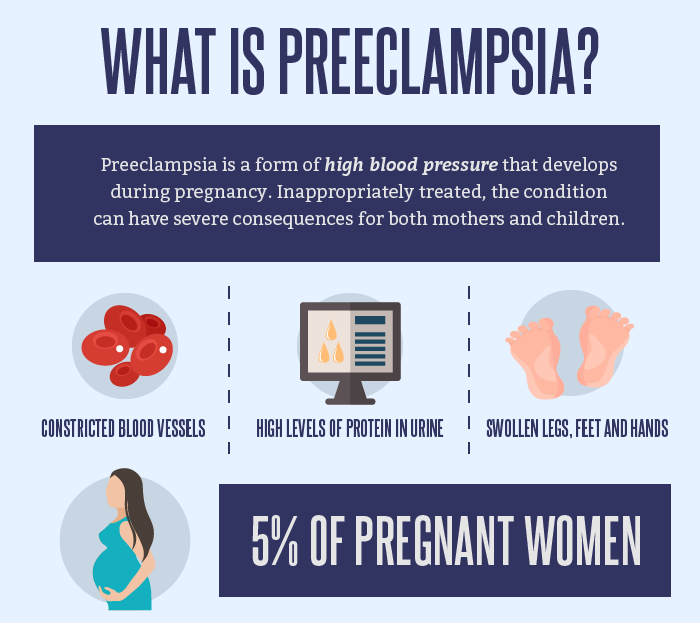
Preeclampsia/Eclampsia
Preeclampsia happens when a woman who previously had normal blood pressure suddenly develops high blood pressure* and protein in her urine or other problems after 20 weeks of pregnancy. Women who have chronic hypertension can also get preeclampsia.
Preeclampsia happens in about 1 in 25 pregnancies in the United States.1,13 Some women with preeclampsia can develop seizures. This is called eclampsia, which is a medical emergency.1,11
This is called eclampsia, which is a medical emergency.1,11
Symptoms of preeclampsia include:
- A headache that will not go away
- Changes in vision, including blurry vision, seeing spots, or having changes in eyesight
- Pain in the upper stomach area
- Nausea or vomiting
- Swelling of the face or hands
- Sudden weight gain
- Trouble breathing
Some women have no symptoms of preeclampsia, which is why it is important to visit your health care team regularly, especially during pregnancy.
You are more at risk for preeclampsia if:1
- This is the first time you have given birth.
- You had preeclampsia during a previous pregnancy.
- You have chronic (long-term) high blood pressure, chronic kidney disease, or both.
- You have a history of thrombophilia (a condition that increases risk of blood clots).
- You are pregnant with multiple babies (such as twins or triplets).
- You became pregnant using in vitro fertilization.
- You have a family history of preeclampsia.
- You have type 1 or type 2 diabetes.
- You have obesity.
- You have lupus (an autoimmune disease).
- You are older than 40.
In rare cases, preeclampsia can happen after you have given birth. This is a serious medical condition known as postpartum preeclampsia. It can happen in women without any history of preeclampsia during pregnancy.14 The symptoms for postpartum preeclampsia are similar to the symptoms of preeclampsia. Postpartum preeclampsia is typically diagnosed within 48 hours after delivery but can happen up to 6 weeks later.9
Tell your health care provider or call 9-1-1 right away if you have symptoms of postpartum preeclampsia. You might need emergency medical care.9,10
*In November 2017, the American College of Cardiology (ACC) and the American Heart Association (AHA) updated the definition of chronic stage 2 hypertension to mean having blood pressure at or above 140/90 mmHg.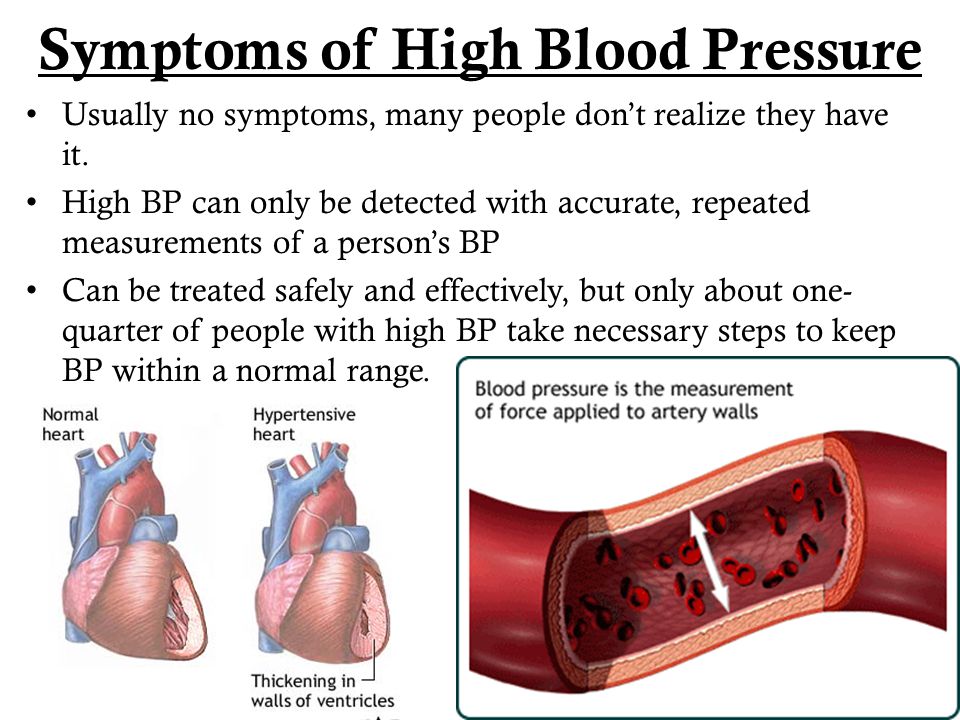 15 The American College of Obstetricians and Gynecologists’ recommendations on hypertension in pregnancy predate the 2017 ACC/AHA’s guideline and definition of hypertension and stage 2 hypertension.
15 The American College of Obstetricians and Gynecologists’ recommendations on hypertension in pregnancy predate the 2017 ACC/AHA’s guideline and definition of hypertension and stage 2 hypertension.
High blood pressure during pregnancy
High blood pressure can cause problems for you and your baby during pregnancy, including preeclampsia and premature birth.
High blood pressure usually doesn’t cause signs or symptoms. Go to all of your prenatal care visits so your provider can check your blood pressure.
If you need medicine to keep your blood pressure under control, take it every day.
If you’re at high risk for preeclampsia, your provider may want you to take low-dose aspirin to help prevent it.
What is high blood pressure?
Blood pressure is the force of blood that pushes against the walls of your arteries. Arteries are blood vessels that carry blood away from your heart to other parts of the body. Each time your heart beats, it pumps blood to the arteries. If the pressure in your arteries becomes too high, you have high blood pressure (also called hypertension). High blood pressure can put extra stress on your organs. This can lead to heart attack, heart failure, stroke and kidney failure.
Each time your heart beats, it pumps blood to the arteries. If the pressure in your arteries becomes too high, you have high blood pressure (also called hypertension). High blood pressure can put extra stress on your organs. This can lead to heart attack, heart failure, stroke and kidney failure.
Some women have high blood pressure before they get pregnant. Others have high blood pressure for the first time during pregnancy. About 8 in 100 women (8 percent) have some kind of high blood pressure during pregnancy. If you have high blood pressure, talk to your health care provider. Managing your blood pressure can help you have a healthy pregnancy and a healthy baby.
How do you know if you have high blood pressure?
Your blood pressure reading is given as two numbers:
- Systolic blood pressure. This is the upper (first) number in your reading. It’s the pressure when you heart contracts (gets tight). Your blood pressure is highest when your heart beats and pumps blood.

- Diastolic blood pressure. This is the lower (second) number in your reading. It’s the pressure when your heart relaxes. Your blood pressure falls because your heart is at rest between beats.
Your blood pressure reading fits into one of five categories:
- Normal. Your blood pressure is less than 120/80.
- Elevated. This is when your systolic blood pressure is between 120-129 and your diastolic pressure is less than 80.
- Stage 1 high blood pressure. This is when your systolic pressure is between 130-139 or your diastolic pressure is between 80-89.
- Stage 2 high blood pressure. This is when your systolic pressure is at least 140 or your diastolic is at least 90.
- Hypertensive crisis. This is when your systolic pressure is higher than 180 and/or your diastolic pressure is higher than 120. Call your health care provider right away if your blood pressure is this high.
At each prenatal care checkup, your provider checks your blood pressure. To do this, she wraps a cuff (band) around your upper arm. She pumps air into the cuff to measure the pressure in your arteries when the heart contracts and then relaxes. If you have a high reading, your provider can recheck it to find out for sure if you have high blood pressure. Your blood pressure can go up or down during the day.
What pregnancy complications can high blood pressure cause?
High blood pressure can cause problems for you and your baby during pregnancy, including:
Problems for moms include:
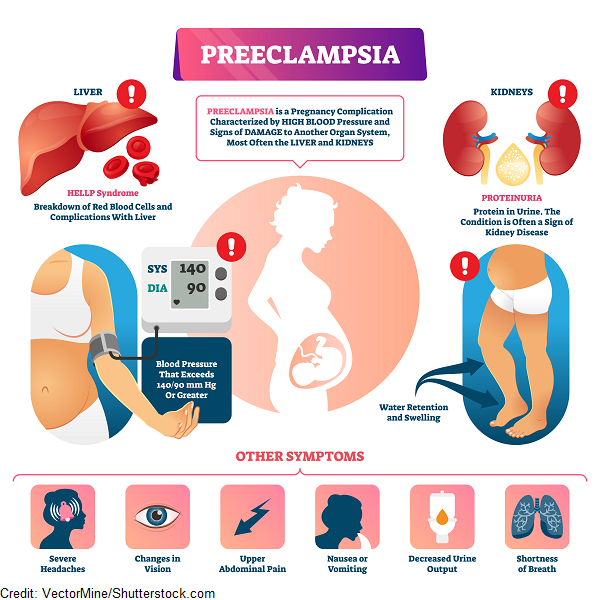
- Preeclampsia. This is when a pregnant woman has high blood pressure and signs that some of her organs, like her kidneys and liver, may not be working properly. Signs and symptoms of preeclampsia include having protein in the urine, changes in vision and severe headaches. Preeclampsia can be a serious medical condition. Even if you have mild preeclampsia, you need treatment to make sure it doesn’t get worse.
 Without treatment, preeclampsia can cause serious health problems, including kidney, liver and brain damage. In rare cases, it can lead to life-threatening conditions called eclampsia and HELLP syndrome. Eclampsia causes seizures and can lead to coma. HELLP syndrome is when you have serious blood and liver problems. HELLP stands for hemolysis (H), elevated liver enzymes (EL), low platelet count (LP).
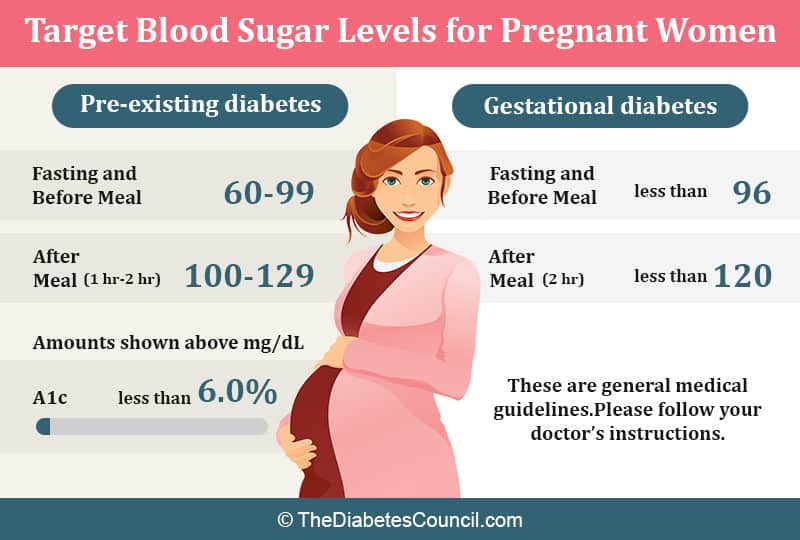
Without treatment, preeclampsia can cause serious health problems, including kidney, liver and brain damage. In rare cases, it can lead to life-threatening conditions called eclampsia and HELLP syndrome. Eclampsia causes seizures and can lead to coma. HELLP syndrome is when you have serious blood and liver problems. HELLP stands for hemolysis (H), elevated liver enzymes (EL), low platelet count (LP). - Gestational diabetes. This is a kind of diabetes that only pregnant women get. It’s a condition in which your body has too much sugar (also called glucose). Most women get a test for gestational diabetes at 24 to 28 weeks of pregnancy.
- Heart attack (also called myocardial infarction).
- Kidney failure. This is a serious condition that happens when the kidneys don’t work well and allow waste to build up in the body.
- Placental abruption. This is a serious condition in which the placenta separates from the wall of the uterus before birth.
 If this happens, your baby may not get enough oxygen and nutrients in the womb. You also may have serious bleeding from the vagina. The placenta grows in the uterus and supplies the baby with food and oxygen through the umbilical cord.
If this happens, your baby may not get enough oxygen and nutrients in the womb. You also may have serious bleeding from the vagina. The placenta grows in the uterus and supplies the baby with food and oxygen through the umbilical cord. - Postpartum hemorrhage (also called PPH). This is when a woman has heavy bleeding after giving birth. It’s a serious but rare condition. It usually happens 1 day after giving birth, but it can happen up to 12 weeks after having a baby.
- Pulmonary edema. This is when fluid fills the lungs and leads to shortness of breath.
- Stroke. This is when blood flow to your brain stops. Stroke can happen if a blood clot blocks a vessel that brings blood to the brain or when a blood vessel in the brain bursts open.
- Pregnancy related death. This is when a woman dies during pregnancy or within 1 year after the end of her pregnancy from health problems related to pregnancy.
If you have high blood pressure during pregnancy, you’re also more likely have a cesarean birth (also called c-section). This is surgery in which your baby is born through a cut that your doctor makes in your belly and uterus.
Problems for babies include:
- Premature birth. This is birth that happens too early, before 37 weeks of pregnancy. Even with treatment, a pregnant woman with severe high blood pressure or preeclampsia may need to give birth early to avoid serious health problems for her and her baby.
- Fetal growth restriction. High blood pressure can narrow blood vessels in the umbilical cord. This is the cord that connects the baby to the placenta. It carries food and oxygen from the placenta to the baby. If you have high blood pressure, your baby may not get enough oxygen and nutrients, causing him to grow slowly.
- Low birthweight. This is when a baby is born weighing less than 5 pounds, 8 ounces.
- Fetal death. When a baby dies spontaneously in the womb at any time during pregnancy.
- Neonatal death. This is when a baby dies in the first 28 days of life.
What kinds of high blood pressure can affect pregnancy?
Two kinds of high blood pressure that can happen during pregnancy:
- Chronic hypertension. This is high blood pressure that you have before you get pregnant or that develops before 20 weeks of pregnancy. It doesn’t go away once you give birth. About 1 in 4 women with chronic hypertension (25 percent) has preeclampsia during pregnancy. If you’re at high risk for preeclampsia, your provider may treat you with low-dose aspirin to prevent it.
If you have chronic hypertension, your provider checks your blood pressure and urine at each prenatal care visit. You may need to check your blood pressure at home, too. Your provider may use ultrasound and fetal heart rate testing to check your baby’s growth and health.
 Your provider also checks for signs of preeclampsia.
Your provider also checks for signs of preeclampsia.If you were taking medicine for chronic hypertension before pregnancy, your provider makes sure it’s safe to take during pregnancy. If it’s not, he switches you to a safer medicine. Some blood pressure medicines, called ACE inhibitors and angiotensin receptor blockers, can harm your baby during pregnancy.
During the first half of pregnancy, blood pressure often falls. If you have mild hypertension and took medicine for it before pregnancy, your provider may lower the dose of medicine you take. Or you may be able to stop taking medicine during pregnancy. Don’t stop taking any medicine before you talk to your health care provider. Even if you didn’t take blood pressure medicine in the past, you may need to start taking it during pregnancy.
- Gestational hypertension. This is high blood pressure that only pregnant women can get. It starts after 20 weeks of pregnancy and usually goes away after you give birth.
 It usually causes a small rise in blood pressure, but some women develop severe hypertension and may be at risk for more serious complications later in pregnancy, like preeclampsia.
It usually causes a small rise in blood pressure, but some women develop severe hypertension and may be at risk for more serious complications later in pregnancy, like preeclampsia.
During pregnancy, your provider checks your blood pressure and urine at every prenatal care checkup. She may use ultrasound and fetal heart rate testing to check your baby’s growth and health. Your provider may ask you to check your blood pressure at home and do kick counts to see when and how often your baby moves. Here are two ways to do kick counts:
- Every day, time how long it takes for your baby to move ten times. If it takes longer than 2 hours, tell your provider.
- See how many movements you feel in 1 hour. Do this three times each week. If the number changes, tell your provider.
We don’t know how to prevent gestational hypertension. But if you’re overweight or obese, getting to a healthy weight before pregnancy may lower your chances of having this condition. And even though gestational hypertension usually goes away after birth, you may be more likely to develop hypertension later in life. Healthy eating, staying active and getting to a healthy weight after pregnancy can help prevent high blood pressure in the future.
And even though gestational hypertension usually goes away after birth, you may be more likely to develop hypertension later in life. Healthy eating, staying active and getting to a healthy weight after pregnancy can help prevent high blood pressure in the future.
How can you manage high blood during pregnancy?
Here’s what you can do:
- Go to all your prenatal care checkups, even if you’re feeling fine.
- If you need medicine to control your blood pressure, take it every day. Your provider can help you choose one that’s safe for you and your baby.
- Check your blood pressure at home. Ask your provider what to do if your blood pressure is high.
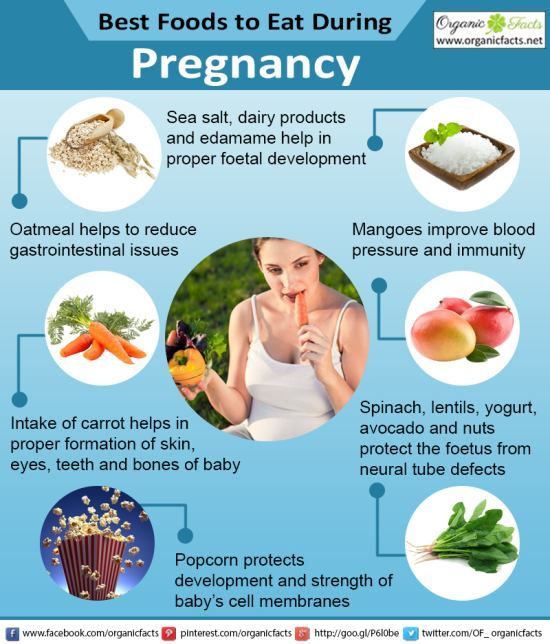
- Eat healthy foods. Don’t eat foods that are high in salt, like soup and canned foods. They can raise your blood pressure.
- Stay active. Being active for 30 minutes each day can help you manage your weight, reduce stress and prevent problems like preeclampsia.
- Don’t smoke, drink alcohol or use street drugs or abuse prescription drugs.

What can you do about high blood pressure before pregnancy?
Here’s what you can do:
- Get a preconception checkup. This is a medical checkup you get before pregnancy to take care of health conditions that may affect your pregnancy.
- Use birth control until your blood pressure is under control. Birth control is methods you can use to keep from getting pregnant. Condoms and birth control pills are examples of birth control.
- Get to a healthy weight. Talk to your provider about the weight that’s right for you.
- Eat healthy foods.
- Do something active every day.
- Don’t smoke. Smoking is dangerous for people with high blood pressure because it damages blood vessel walls.
Last reviewed: February, 2019
See also: Preeclampsia, HELLP syndrome
Hypertension in pregnancy
High blood pressure during pregnancy
Changes in blood pressure (BP) in women during pregnancy are observed quite often, which can adversely affect the mother and fetus. Blood pressure is one of the most important indicators of the functioning of the circulatory system in the body. During pregnancy, all organs and systems of the mother work with increased stress, especially the cardiovascular system. Therefore, it is necessary to regularly measure blood pressure to prevent the development of severe complications. At the beginning of pregnancy, blood pressure, as a rule, decreases slightly, which is associated with the action of hormones. In later pregnancy, as the fetus grows and blood flow increases to feed it, blood pressure may increase relative to pre-pregnancy physiological values. Hypertension is said to occur when a pregnant woman's blood pressure exceeds 140/9.0 mmHg However, in women with low blood pressure before pregnancy, arterial hypertension may be at blood pressure levels that are usually considered normal. Therefore, it is important to know your normal blood pressure.
Blood pressure is one of the most important indicators of the functioning of the circulatory system in the body. During pregnancy, all organs and systems of the mother work with increased stress, especially the cardiovascular system. Therefore, it is necessary to regularly measure blood pressure to prevent the development of severe complications. At the beginning of pregnancy, blood pressure, as a rule, decreases slightly, which is associated with the action of hormones. In later pregnancy, as the fetus grows and blood flow increases to feed it, blood pressure may increase relative to pre-pregnancy physiological values. Hypertension is said to occur when a pregnant woman's blood pressure exceeds 140/9.0 mmHg However, in women with low blood pressure before pregnancy, arterial hypertension may be at blood pressure levels that are usually considered normal. Therefore, it is important to know your normal blood pressure.
Why is high blood pressure dangerous during pregnancy?
High blood pressure during pregnancy poses a great danger to the mother and fetus. Against this background, vasoconstriction occurs and the blood supply to all vital organs, including the placenta, is disrupted. Due to the lack of essential nutrients and oxygen, the process of growth and development of the fetus slows down. There is a serious danger of placental abruption, which is accompanied by bleeding and threatens the life of the mother and fetus. High blood pressure during pregnancy can lead to the development of a dangerous pregnancy complication - preeclampsia. Edema, large weight gain, and the presence of protein in the urine can also be a manifestation of preeclampsia. Very dangerous symptoms of preeclampsia are: headache, blurred vision ("flies", "veil" before the eyes), pain in the upper abdomen. Deterioration of the general condition may be accompanied by dizziness, tinnitus, nausea, vomiting. Pre-eclampsia can provoke a formidable complication - eclampsia. In this condition, the pregnant woman loses consciousness and convulsions occur. nine0005
Against this background, vasoconstriction occurs and the blood supply to all vital organs, including the placenta, is disrupted. Due to the lack of essential nutrients and oxygen, the process of growth and development of the fetus slows down. There is a serious danger of placental abruption, which is accompanied by bleeding and threatens the life of the mother and fetus. High blood pressure during pregnancy can lead to the development of a dangerous pregnancy complication - preeclampsia. Edema, large weight gain, and the presence of protein in the urine can also be a manifestation of preeclampsia. Very dangerous symptoms of preeclampsia are: headache, blurred vision ("flies", "veil" before the eyes), pain in the upper abdomen. Deterioration of the general condition may be accompanied by dizziness, tinnitus, nausea, vomiting. Pre-eclampsia can provoke a formidable complication - eclampsia. In this condition, the pregnant woman loses consciousness and convulsions occur. nine0005
Register for pregnancy at the antenatal clinic as early as possible!
A very important feature of arterial hypertension during pregnancy is that often even with high blood pressure numbers, the patient feels normal. High blood pressure is detected by chance, at the next appearance in the antenatal clinic. The absence of clinical manifestations of elevated blood pressure does not exclude the development of dangerous complications.
High blood pressure is detected by chance, at the next appearance in the antenatal clinic. The absence of clinical manifestations of elevated blood pressure does not exclude the development of dangerous complications.
In order to detect unwanted deviations during pregnancy in time and prevent the development of complications in the mother and fetus, pregnant women need to regularly monitor their blood pressure. It is very important to register for pregnancy in a antenatal clinic in a timely manner. The doctor will promptly detect changes in blood pressure and prescribe the optimal therapy to maintain blood pressure in the normal range. If a woman had high blood pressure before pregnancy, and she is taking medications, it is necessary to adjust the treatment and individually select the drugs that can be taken during pregnancy. To prevent high blood pressure, a pregnant woman should eat a healthy and balanced diet, observe a drinking regimen, and monitor weight gain. The correct recommendations on these issues will also be given by the doctor of the antenatal clinic. A pregnant woman must follow the recommendations and not violate the prescribed therapy. nine0005
A pregnant woman must follow the recommendations and not violate the prescribed therapy. nine0005
What to do if a pregnant woman has high blood pressure?
If a pregnant woman regularly monitors blood pressure on her own and notes even a slight increase with good health, she should visit the doctor of the antenatal clinic as soon as possible (before the scheduled next visit). Self-administration of drugs in this case is strictly prohibited. Before visiting a doctor, you can reduce blood pressure by taking a mild sedative based on motherwort or valerian. nine0005
If necessary, you can consult with an obstetrician-gynecologist of the remote medical advisory panel of the Ambulance and Emergency Medical Care Station. A.S. Puchkov, Moscow by phone: (495) 620-42-44.
When is it necessary to call an ambulance?
If blood pressure rises suddenly, you feel unwell, urgent hospitalization is necessary, and it is advisable for the patient to immediately call an ambulance team. Such signs as: headache, feeling of flashing dots or "flies", a veil before the eyes, pain in the upper abdomen, nausea, vomiting, agitation or depression, along with this - an increase in blood pressure should alert. There may be a high convulsive readiness, which is manifested by twitching of the muscles of the face, neck, upper limbs, loss of consciousness, convulsions are possible. nine0005
Such signs as: headache, feeling of flashing dots or "flies", a veil before the eyes, pain in the upper abdomen, nausea, vomiting, agitation or depression, along with this - an increase in blood pressure should alert. There may be a high convulsive readiness, which is manifested by twitching of the muscles of the face, neck, upper limbs, loss of consciousness, convulsions are possible. nine0005
What to do before the ambulance arrives?
First of all, go to bed, if possible, eliminate all unwanted irritants (turn off all sources of noise, close the curtains), do not leave the pregnant woman alone, as convulsions may occur and help will be needed. Give it a position with a raised head end. It is possible to take pressure-lowering drugs prescribed by a doctor. If a woman has not previously taken antihypertensive drugs, then drugs should not be taken on the advice of others. nine0005
If an attack of convulsions occurs, the pregnant woman should be laid on a flat surface, turn her head to the side (to prevent aspiration of vomit), protect from damage (cover with a blanket), do not hold physically. After an attack, clean the oral cavity with a napkin from vomit, blood and mucus. Wait for the ambulance to arrive!
After an attack, clean the oral cavity with a napkin from vomit, blood and mucus. Wait for the ambulance to arrive!
The ambulance will arrive quickly and provide the necessary assistance. Hospitalization in this condition is mandatory. Only in a hospital is it possible to fully monitor the condition of the mother and child, complete therapy and determine the delivery plan. nine0005
We wish you health and happy motherhood!
Chief Specialist
in Obstetrics and Gynecology Arkhipova N.L.
High blood pressure during pregnancy
But its meaning is not always correctly controlled and interpreted. Let's see how to properly control blood pressure during pregnancy , what kind of blood pressure is considered elevated, why it can rise and what should be done with it, and what should not be done.
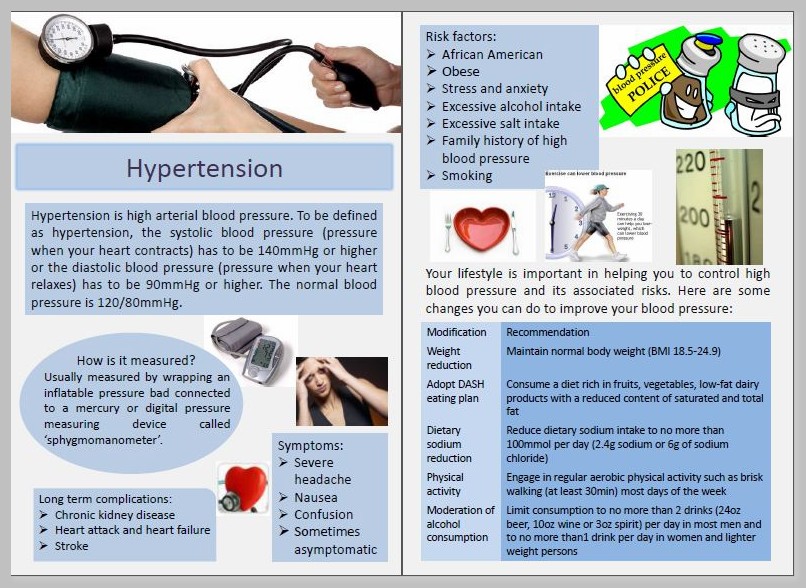
Blood pressure measurement
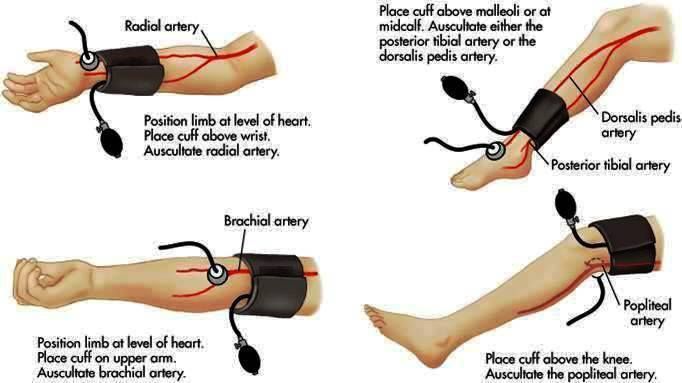
Blood pressure is monitored using a tonometer: electronic, semi-automatic or mechanical. You can buy any that you can handle and the cuff of which suits you in diameter. The only thing to consider is that the blood pressure cuff should be worn on the upper arm, carpal blood pressure monitors are too inaccurate and cannot be relied upon. nine0005
You can buy any that you can handle and the cuff of which suits you in diameter. The only thing to consider is that the blood pressure cuff should be worn on the upper arm, carpal blood pressure monitors are too inaccurate and cannot be relied upon. nine0005
Measurement of blood pressure is best done in a sitting position, and after you have spent about fifteen minutes in this position, in a state of physical and emotional rest, you do not need to talk while measuring blood pressure.
The cuff is worn on the shoulder freed from clothing, its lower edge should be a few centimeters above the elbow. The arm on which blood pressure is measured should be in a relaxed position, the cuff should be located approximately at the level of the heart. Measurement is performed on one arm, measurement on two arms, which was previously required for all pregnant women, is now excluded from all clinical recommendations. nine0005
When measuring with a mechanical sphygmomanometer , air is inflated into the cuff to the digits, approximately twenty to thirty mm.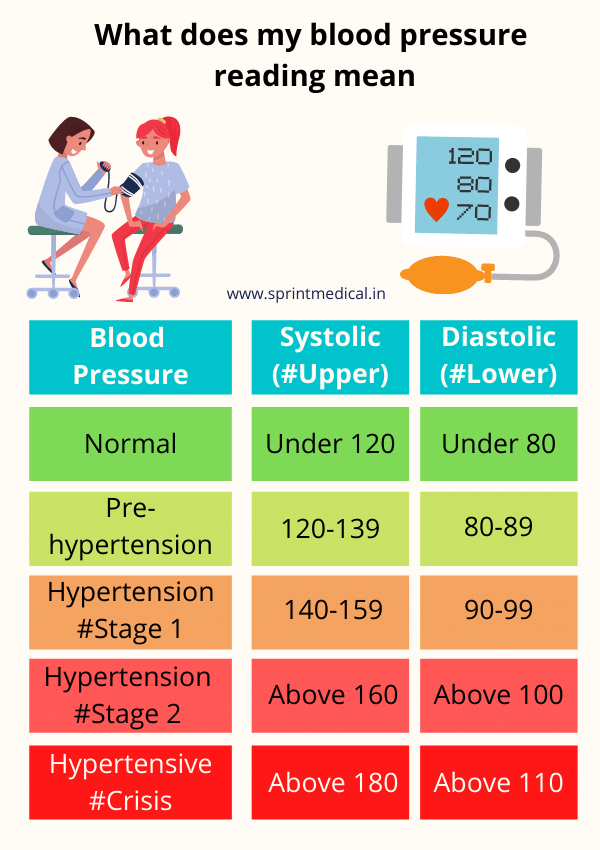 rt. Art. higher than expected blood pressure. The air from the cuff is released slowly, the appearance of sound marks the numbers of systolic blood pressure, the disappearance of the sound - diastolic. This is not "cardiac" and "renal" pressure, but - systolic and diastolic.
rt. Art. higher than expected blood pressure. The air from the cuff is released slowly, the appearance of sound marks the numbers of systolic blood pressure, the disappearance of the sound - diastolic. This is not "cardiac" and "renal" pressure, but - systolic and diastolic.
Measurement of blood pressure is carried out at each visit to the obstetrician-gynecologist - office measurement of blood pressure, at home of the pregnant woman herself or her relative - outpatient measurement of blood pressure. If necessary, the doctor may recommend that the patient keep a blood pressure diary - measure blood pressure several times a day for some time, writing down the numbers. Ceteris paribus, more reliable information is obtained from outpatient (at home) measurements. nine0005
If there is doubt about the correctness of the patient's blood pressure measurement or if there is a suspicion of an increase in blood pressure at night, the doctor may prescribe the patient 24-hour blood pressure monitoring (ABPM), in which blood pressure is measured automatically at certain intervals within one day.
In general, during pregnancy, blood pressure in the first trimester is lower than normal for the patient, in the second or third it returns to her usual numbers, by the third trimester it may be slightly higher, but within the normal range. Blood pressure below 140/9 is considered normal during pregnancy.0 mm. rt. Art.
If the patient is prone to arterial hypotension (low blood pressure), elevated blood pressure is still considered to be blood pressure above 140/90 mm. rt. Art., lower figures do not require any additional examination or treatment, even if they are higher than usual for the patient. None of the clinical guidelines for the treatment of arterial hypertension during pregnancy indicate the need for treatment with higher blood pressure than usual, but not reaching a value of 140/90 mm. rt. Art.
AD 140/90 mm. rt. Art. and above must be recorded 2 or more times with an interval between measurements of at least 4 hours to be considered hypertension.
Causes of high blood pressure
There are three causes of high blood pressure during pregnancy: chronic arterial hypertension, gestational arterial hypertension and preeclampsia.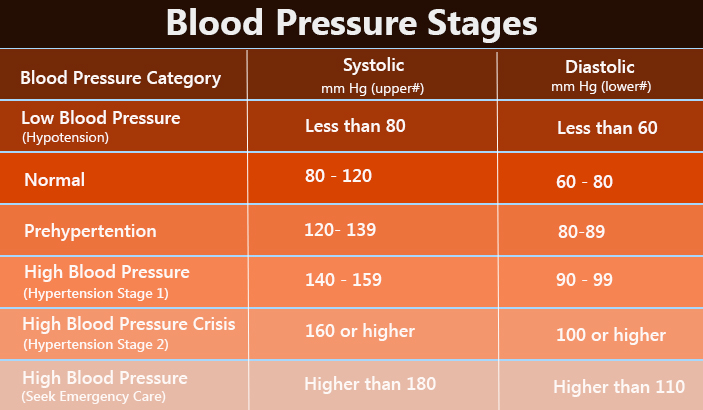
Chronic arterial hypertension is the general name for all cases of high blood pressure that existed before pregnancy. Chronic arterial hypertension is not divided into primary (due to unknown causes) and secondary (resulting from a disease), in contrast to arterial hypertension detected outside of pregnancy. Also, chronic arterial hypertension includes situations when a woman did not control blood pressure before pregnancy, and for the first time an increase in blood pressure was detected only in the first half (up to 20 weeks) of pregnancy. nine0005
Gestational hypertension occurs from the twentieth week until the end of the term, and is not accompanied by the excretion of protein in the urine.
Pre-eclampsia, in contrast to gestational hypertension, also develops after the 20th week of pregnancy, and is accompanied by the release of protein into the urine (proteinuria). Preeclampsia can also occur after delivery.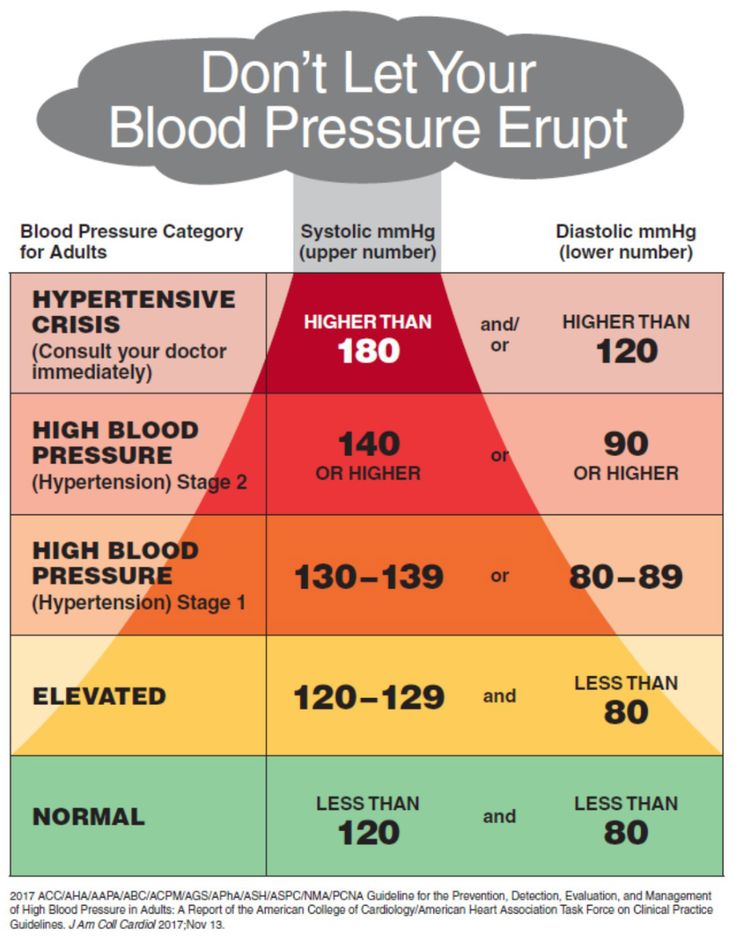 Signs of an increase in the severity of preeclampsia are the appearance of a headache, dizziness, visual disturbances, pain in the solar plexus and / or in the right hypochondrium, pain under the right shoulder blade, respiratory failure, and some changes in blood tests. These signs require urgent hospitalization. nine0005
Signs of an increase in the severity of preeclampsia are the appearance of a headache, dizziness, visual disturbances, pain in the solar plexus and / or in the right hypochondrium, pain under the right shoulder blade, respiratory failure, and some changes in blood tests. These signs require urgent hospitalization. nine0005
The extreme case of preeclampsia - eclampsia - is characterized by the occurrence of convulsions and threatens the life of both the mother and the child, therefore, it requires an emergency delivery, regardless of the gestational age, only in this way it becomes possible to save the life of the mother and child.
Since an increase in blood pressure may occur before proteinuria in preeclampsia, it is possible to distinguish gestational arterial hypertension from preeclampsia only in retrospect - if blood pressure increased, and protein did not appear in the daily urine, it can be said with certainty that this increase in blood pressure was due to specifically gestational hypertension. nine0107 Preeclampsia may be associated with chronic arterial hypertension that existed before pregnancy.
nine0107 Preeclampsia may be associated with chronic arterial hypertension that existed before pregnancy.
Treatment of Hypertensive Disorders
Hypertensive disorders are an important cause of maternal and perinatal death, increase the rate of preterm birth, and are indeed a serious problem and should not be ignored.
The only one to date proven effective in preventing preeclampsia drug is acetylsalicylic acid. It is prescribed starting from the 13th week of pregnancy at a low dose and at this dosage does not lead to impaired fetal development, unlike high doses.
Treatment of any arterial hypertension during pregnancy is prescribed only by a doctor.
In chronic arterial hypertension uncomplicated by damage to other organs, treatment is started at BP 150/90 mm. rt. Art. and more, with gestational arterial hypertension and preeclampsia - with blood pressure 140/90 mm. rt. Art. and more.
BP should be maintained at 130-150/80/95 mmHg during treatment. rt. Art., since a more radical decrease in blood pressure is fraught with impaired blood supply to the fetus and is not recommended.
rt. Art., since a more radical decrease in blood pressure is fraught with impaired blood supply to the fetus and is not recommended.
There are several groups of antihypertensive drugs, the use of which during pregnancy can lead to impaired fetal development or death, so they should not be used during pregnancy. These are angiotensin-converting enzyme inhibitors and angiotensin II receptor antagonists. Do not use during pregnancy and diuretics (drugs with a diuretic effect). nine0107 Treatment is usually initiated with methyldopa, but it is also possible to use certain drugs from the group of beta-blockers and some drugs from the group of calcium antagonists, which are best studied from the point of view of safety in pregnancy. It is possible to use combinations of these drugs.
Separately, a few words should be said about magnesium sulfate (magnesium sulphate). This drug has practically no antihypertensive effect, and its use during pregnancy is limited only to preeclampsia, which threatens the development of eclampsia. It is needed to prevent the development of seizures (neuroprotective effect). It should not be used to influence elevated blood pressure. nine0005
It is needed to prevent the development of seizures (neuroprotective effect). It should not be used to influence elevated blood pressure. nine0005
Hypertension during pregnancy, delivery is usually through the natural birth canal, except in cases of severe pre-eclampsia, eclampsia and their complications, requiring emergency delivery by caesarean section, regardless of the gestational age for health reasons.
Chronic arterial hypertension that persists during lactation and is not complicated by damage to other organs does not require medical treatment for blood pressure less than 150/95 mm. rt. Art. Arterial hypertension after childbirth does not require stopping breastfeeding; on the contrary, the protective effect of lactation in arterial hypertension has been proven.
If it is necessary to prescribe drug therapy , drugs are selected that are the least likely to be excreted into breast milk, the use of which has not been recorded serious side effects in the child.