What to do with miscarriage tissue
What Should Be Done with the Remains of Miscarried Fetuses?
Photo via Flickr user Konstantinos Koukopoulos
In 2014, a British investigation discovered that more than 15,000 miscarried and aborted fetuses had been incinerated at UK hospitals over the previous two years. They had been mixed in with other medical waste, and in some cases their incineration helped heat and power the same hospitals at which those fetuses were miscarried. "Thousands of unborn foetuses incinerated to heat UK hospitals," was the headline splashed across the country's papers.
Advertisement
Suddenly, one of society's longest-standing taboos—miscarriage—had been suddenly pushed to the forefront of a nation's consciousness. That attention was long overdue: In the UK, as in the US, there was no national standard for handling miscarried fetuses.
As with all matters concerning pregnancy, there are a number of ways a woman may want to handle her miscarriage. Some women find comfort in burying or cremating the remains of the miscarried fetus; others don't consider their fetus something to be mourned, and prefer that it be handled alongside other medical waste. But the status quo in America often robs women of these choices altogether.
In the words of Erica and Joshua Raef, miscarriage "may be one of the least discussed, yet most common, sources of heartbreak." Like thousands of parents across America, they know that heartbreak all too well. Erica's pregnancy last year ended in a miscarriage.
In an interview with VICE, the Raefs described how, after seeing their baby's heartbeat weeks earlier, they were told at their next visit that it no longer had one. This was 13 weeks into Erica's pregnancy. As they sat down to work out how to manage the miscarriage, they were told that if they went into the hospital they would not be able to take the remains home for burial. This information, provided to the Raefs' doctor, later turned out to be incorrect, but it nevertheless led them to choose to wait out the miscarriage at home, in the hopes that they would be able to inter the remains of the fetus themselves.
Advertisement
It took ten days, but eventually Erica's body went into labor, and in her words, they "were able to see and hold [their] tiny and perfect little baby. " Later that night, Erica began to bleed out and Joshua rushed her, unconscious, to the ER.
" Later that night, Erica began to bleed out and Joshua rushed her, unconscious, to the ER.
Some 18 months later, in April 2015, the Raefs stood up and testified about their experience in the Public Health Committee of the Texas House of Representatives in support of HB 635, a bill that came into effect at the beginning of this month and ensures that Texas parents will have the right to choose what happens to the remains of a pregnancy after a miscarriage. Already, Representative Four Price, the author of the bill, has seen the impact that this change in the law may have. Price told VICE, "After [HB 635] passed, many couples have called or sent letters saying how they had experienced similar circumstances and how thankful they were that this was now going to be the law."
A miscarriage is not, despite confusion in popular discourse, the same thing as a stillbirth. Every year in the United States there are more than 23,000 stillbirths—fetuses which die in utero after 20 weeks or longer of gestation. These babies are required by law to be either buried or cremated. In 34 states, parents may also receive a "Certificate of Birth Resulting in Stillbirth" or something similar alongside the obligatory death certificate. For a pregnancy loss prior to 20 weeks it is much more likely that the fetus, will be incinerated along with the rest of the day's medical waste or cremated and buried in an unmarked plot.
These babies are required by law to be either buried or cremated. In 34 states, parents may also receive a "Certificate of Birth Resulting in Stillbirth" or something similar alongside the obligatory death certificate. For a pregnancy loss prior to 20 weeks it is much more likely that the fetus, will be incinerated along with the rest of the day's medical waste or cremated and buried in an unmarked plot.
Advertisement
Yet the number of stillbirths in America is dwarfed by the number of miscarriages. Estimates vary due to lack of reporting, but the number may be close to 1 million a year; close to 30 percent of pregnancies end in a miscarriage.
As of 2014, in 27 states there was no explicit right for the mother (or her designee) to opt for a burial or cremation of a fetus which dies before the 20-week mark. In a further seven, one can opt for a burial or cremation but there is no duty to inform the mother of this power. This leaves grieving families in legal limbo and for many adds to their grief and suffering in the wake of a sudden loss. In the worst cases, it can lead to the dangerous situations like the Reafs'.
In the worst cases, it can lead to the dangerous situations like the Reafs'.
According to Tanya Marsh, a professor of law at Wake Forest University specializing in funeral and cemetery law, "the fundamental legal problem is that it never occurred to anybody until fairly recently, on the law-making side, that this is anything that they should care about." This is hardly surprising when one considers the lack of public understanding of miscarriage. In a recent paper in the journal Obstetrics and Gynecology, researchers found that more than half of respondents radically underestimated how often miscarriages occur. Representative Four Price said that even at the legislative level, a lot of education was needed. Price told VICE that while pushing their bill forward, legislators needed "to spend quite a bit of time educating members and staff members in the legislative offices in the House and the Senate as to why this was even necessary. Most individuals really had no personal experience or understanding of why this might be a good thing. " Indeed, it was not an issue that Representative Price had considered himself until the Raefs visited with him. Price said, "That [visit] really was the catalyst for the bill."
" Indeed, it was not an issue that Representative Price had considered himself until the Raefs visited with him. Price said, "That [visit] really was the catalyst for the bill."
Advertisement
It is hard to say when most miscarriages take place during a pregnancy, although the vast majority occur very early; in the first few weeks, many miscarriages may go unnoticed.
The 20-week mark distinguishing a miscarriage from a stillbirth is open to accusations of arbitrariness. According to Kristen Swanson, RN PhD, the reasoning behind that division doesn't make sense. In an interview with VICE, Swanson said, "The legal definition supposedly relies on the medical definition, which is, 'A stillbirth is the loss of a pregnancy past the point of expected fetal viability.' The legal breakoff tends to be 20 weeks. In most regards, we consider the medical breakoff to be 24 weeks. We use a legal definition of 20 weeks based on a medical definition that doesn't even apply."
It would be wrong to think that women who suffer miscarriages suffer less than women whose pregnancy loss is classified as a stillbirth. The area is little researched, but the experience of miscarriage has changed a lot since Irv Leon, a clinical psychologist and adjunct professor at University of Michigan, began working in the area of pregnancy loss in 1985.
The area is little researched, but the experience of miscarriage has changed a lot since Irv Leon, a clinical psychologist and adjunct professor at University of Michigan, began working in the area of pregnancy loss in 1985.
"Then, miscarriage was not experience as loss of a baby, it was considered more as the loss of a pregnancy," he told VICE. According to Leon, the way in which women now experience an early-stage pregnancy as a baby is in part due to "the use of ultrasounds, especially early on, and the greater sharpness and clarity of the images."
Advertisement
"At around eight weeks, when one has the experience of the ultrasound where one sees the heartbeat, very often that is the beginning of the process of experiencing the pregnancy as a baby," said Leon. "Whereas before that, the pregnancy would usually be a quickening, when the mother experienced the baby 'move' in the second trimester." According to a June study in Obstetrics and Gynecology, 37 percent of women surveyed who had experienced a miscarriage conceived it as the loss of a child.
But the loss of a pregnancy can have different meanings to different people. As Joanne Cacciatore, PhD, an assistant professor at Arizona State University and founder of the MISS Foundation notes, "For a woman who has, perhaps, had trouble with infertility, and has been trying to get pregnant for five years, and finally gets pregnant, and she's so excited, and she's told everyone…and at 12 weeks she's miscarried—that's a devastating loss for her."
Martha Diamond, PhD, says that based on her research, "what effects the level of grief is the meaning of the loss to the individual or the couple. A very early loss can be absolutely devastating, or it can not [be]." For Cacciatore, and Diamond this means it is important to give parents control and choice over what happens after the loss of a pregnancy. This is, according to Leon, as much for psychological reasons as for moral ones. Providing choices in a situation of helplessness can psychologically assist parents by limiting and coping with what can be the overwhelming experience of pregnancy loss.
Advertisement
Like many parents across America, the Raefs were not given the chance to choose the method of final disposition for the remains of their pregnancy. This led them to extreme medical risk, but in the end it gave them what they wanted: the chance to bury their baby, which they had named Liam, following a small service on a family plot. This was something which gave them, in their own words, "a profound sense of closure." Cacciatore says that being allowed to mark the loss with a service and a burial—a ritual—is crucial to the grieving process.
"Ritual is very important for us to enact our emotions, for us to be able to socially connect to others around the loss," Cacciatore told VICE. "In some ways, parents use that ritual to be able to embody that love and connection that they so often hear doesn't matter, even if it is not explicit. Culturally, in an implicit way, we do hear it."
This ritualizing can be important even in the absence of a body, according to Kristen Swanson, Dean of the College of Nursing at Seattle University, who has done extensive research and clinical work with women who experienced a pregnancy loss. "People talk about 'making ceremony,' but I don't remember people talking too much about using the products of conception," Swanson told VICE. "It's more like they have a proper burial of the memory and have a proper ceremony surrounding that."
"People talk about 'making ceremony,' but I don't remember people talking too much about using the products of conception," Swanson told VICE. "It's more like they have a proper burial of the memory and have a proper ceremony surrounding that."
But Cacciatore emphasizes that however a family chooses to mark the loss of a pregnancy due to miscarriage—if they do so at all—is something which must remain an individual choice, and something that should not be forced on parents. "It is very important that ritual not be forced on people. Especially with very early losses, because for some women that may not be a child," she said.
Advertisement
Any legislation dealing with remains of a pregnancy has the potential to be incredibly fraught. While it is a separate issue, the closeness to the debate around abortion was very much in the mind of Representative Four Price when he and his staff were drafting the Texas legislation.
"We were very careful and deliberate with the language that we utilized, because any time you start to get into a debate or an area of law or proposed law where you are dealing with fetal remains, very quickly the assumption may be that you are entering into a pro-life/pro-choice issue, and that can immediately polarize folks," Price told VICE. "This bill had nothing to with that issue, what we were intent on doing was making sure that parents who had a miscarriage… had an absolute right to control the disposition of their child's remains."
"This bill had nothing to with that issue, what we were intent on doing was making sure that parents who had a miscarriage… had an absolute right to control the disposition of their child's remains."
"I don't remember people talking too much about the products of conception. It's more like they have a proper burial of the memory." —Kristen Swanson
In the UK, which has in general adopted a more liberal attitude to the myriad ethical issues surrounding embryos and fetuses, the Human Tissue Authority, a government agency, has issued revised guidance in the wake of the 2014 scandal. Now anyone disposing of pregnancy remains (pre-24th week) must provide the patient with clear verbal or written information about the disposal options available (which include cremation and burial), along with providing the option for a woman to opt out of receiving the information, thereby allowing the hospital to choose a method of disposal. It also explicitly bans mixing pregnancy remains with clinical waste for joint incineration. In the UK, this only occurred after a national outcry in the light of a scandal. Meanwhile, change in America is currently being driven by occasional legislative efforts—often encouraged by personal rather than national trauma.
In the UK, this only occurred after a national outcry in the light of a scandal. Meanwhile, change in America is currently being driven by occasional legislative efforts—often encouraged by personal rather than national trauma.
Advertisement
Even once legislation is in place, the decision to dispose of fetal remains in one way or another may not, in fact, be a choice. Marsh told VICE, "If the hospital disposes of the remains, then the hospital pays for it. If parents have a choice, now the parents have to go find a funeral home and a funeral director [at their own expense]."
Nebraska residents Stephanie Hopp and her husband Andrew found themselves in a situation much like this. Last year, Hopp suffered a miscarriage at ten weeks. Hopp told VICE, "The day before surgery, when I called, I asked what happens to the remains after. [The hospital] told me that typically they take all of the fetal remains together and every so often they cremate them. They said that they would not be able to disclose where they would put [the cremated remains] after that. " When Hopp pushed for her right to control the final disposition of her own pregnancy remains, she says she was told, "'You can set up your own funeral home costs and pay everything yourself, or you can do what the hospital is offering for free.'" When her husband called around local funeral homes, they found that a cremation was going to cost them around $1,000, a prohibitive sum for many families.
" When Hopp pushed for her right to control the final disposition of her own pregnancy remains, she says she was told, "'You can set up your own funeral home costs and pay everything yourself, or you can do what the hospital is offering for free.'" When her husband called around local funeral homes, they found that a cremation was going to cost them around $1,000, a prohibitive sum for many families.
This was a concern that Price was well aware of when drafting the Texas legislation. While there is no standard procedure for either hospitals or funeral homes, he explained to VICE that "many funeral homes will handle such remains very inexpensively or sometimes for free. I am very hopeful that [this] will not result in a situation where only the more economically-advantaged can take advantage of the law. I think that hospitals and funeral homes will often accommodate parents."
Indeed, the hospital eventually accommodated Stephanie Hopp's request: "It wasn't until the day of surgery that I got a call and they said, 'You know what, we worked it out with the funeral home we contract with and we will pay for everything. "
"
For many others in America, this kind of choice—and the resulting compassion—are not the case. In Connecticut, where there is no statutory provision for parents to choose, the charity Hope After Loss has been supporting individuals grieving a pregnancy loss for almost 20 years. Since 2010 the group, in collaboration with the Kelly Ryan Foundation, has been providing funding for disposal of remains according with the wishes of parents. So far, they have helped over 60 families across Connecticut. In their experience, the cost differs "depending on how much you want what it will cost, and that really does vary from funeral home to funeral home."
There is no rule book for how to handle a miscarriage, and the situation raises difficult decisions: not least, whether and how to mourn. The most important thing, in the words of Joshua and Erica Raef, is "giving parents the right to make that choice." In Texas and 16 other states this is now a reality—but across America much more needs to be done. But even when that right is secured, it can only be the first step; situations like the Hopps' will only become more common unless hospitals ensure, by policy or by law, that a woman's ability to bury or cremate what she understands to be her baby is not contingent upon her ability to pay up.
But even when that right is secured, it can only be the first step; situations like the Hopps' will only become more common unless hospitals ensure, by policy or by law, that a woman's ability to bury or cremate what she understands to be her baby is not contingent upon her ability to pay up.
Follow Jonathan on Twitter.
What Happens After a Miscarriage? An Ob-Gyn Discusses the Options.
Miscarriage, the loss of a pregnancy that’s in the uterus, is common. It happens in about 1 in 10 women who know they’re pregnant. But many people don’t know what to expect afterward.
The vast majority of miscarriages happen in the first trimester, before 13 weeks of pregnancy. Most occur before 10 weeks. In this article, I’ll discuss the treatment options for first-trimester miscarriage, also called early pregnancy loss. Second-trimester miscarriage usually requires different treatments.
Here’s what to know about care and recovery.
There are three main treatments for early pregnancy loss. The goal for all three is to remove any pregnancy tissue left in the uterus. There are two nonsurgical treatments: expectant management (letting the tissue pass on its own) and medication. The third treatment is a surgical procedure called dilation and curettage (also known as D&C or suction curettage).
The goal for all three is to remove any pregnancy tissue left in the uterus. There are two nonsurgical treatments: expectant management (letting the tissue pass on its own) and medication. The third treatment is a surgical procedure called dilation and curettage (also known as D&C or suction curettage).
In many cases, patients can choose the option they prefer.
Expectant management is giving your body time to pass the tissue on its own. This doesn’t involve medication or surgery. Some women choose this because it’s the most natural option, but it is more unpredictable than other treatments.
Most women pass the tissue within 2 weeks of a miscarriage diagnosis, but it can take longer. If it takes too long, your ob-gyn may recommend medication to start the process. (Once the process starts and cramping and bleeding begin, most of the tissue passes within a few hours. More on that below.)
Sometimes, the body doesn’t pass all the tissue. When this happens, another treatment is recommended, usually a D&C. Expectant management is most likely to work when you already have some bleeding and cramping. This means your body has begun the process of passing the tissue.
When this happens, another treatment is recommended, usually a D&C. Expectant management is most likely to work when you already have some bleeding and cramping. This means your body has begun the process of passing the tissue.
Medication works faster and is more predictable. Some women choose medication that helps their body remove any leftover tissue. These drugs are absorbed through the cheek in the mouth or through the vagina. Cramping or bleeding usually starts within a few hours. Most women pass the tissue within 48 hours and don’t need any other treatment. (Some women may still not pass all the tissue and may need a surgical procedure.)
Medication gives you more control over the timing of the tissue passing. And it’s often quicker than waiting for the tissue to pass on its own.
Some women like to take the medication in the morning, so the process doesn’t start overnight. And some women like to have a support person, such as a friend or family member, with them when they take the medication.
You’ll have a similar experience whether the tissue passes on its own or you take medication. You’ll have bleeding and cramping that are heavier than your normal period. The pregnancy tissue may look like large blood clots, or it may look white or gray. It does not look like a baby. The process can be painful, and ob-gyns may prescribe medication to help with this discomfort. Your ob-gyn may also suggest over-the-counter pain medication. Talk with your ob-gyn about pain relief options.
Most of the tissue passes within 2 to 4 hours after the cramping and bleeding start. Cramping usually stops within a day. Light bleeding or spotting can go on for 4 to 6 weeks. Two weeks after the tissue passes, your ob-gyn may do an ultrasound exam or other tests to make sure all the tissue has passed.
A D&C is the most predictable treatment. During a D&C, your ob-gyn passes a small tool through the cervix and into the uterus to remove the tissue. Some women choose this option because they want a faster, more certain treatment. And if you’re already bleeding heavily, it’s the safest option.
Some women choose this option because they want a faster, more certain treatment. And if you’re already bleeding heavily, it’s the safest option.
Some ob-gyns do D&Cs in an operating room using general anesthesia, which means you’ll be asleep. Some offer a form of pain relief called sedation, where you will be awake but comfortable. Others do the procedure in a normal exam room, with an injection of drugs that block pain in a specific area. Women often have some bleeding and intense cramping during a D&C. They usually have little discomfort afterward.
Light spotting or bleeding can last up to a month. An antibiotic is prescribed to prevent infection. Other complications are rare, and most women don’t need any follow-up appointments.
Whichever option you choose, call your ob-gyn if you have very heavy bleeding, a fever, or feel unwell. Dangerous bleeding and infection are a risk of all treatments, but these problems are rare. Call your ob-gyn right away if you have any of these symptoms:
-
Your bleeding soaks through more than two large pads in an hour for 2 hours or more.
 This much bleeding is dangerous and needs immediate care.
This much bleeding is dangerous and needs immediate care. -
You have a temperature higher than 100 °F.
-
You have chills, severe pain, or any other symptoms that concern you.
Physical recovery is usually quick. Most women resume their regular activities a day or two after they pass the tissue or have a D&C. For some, nausea and other pregnancy symptoms stop before their ob-gyn diagnoses a miscarriage. For others, these symptoms go away a few days after the tissue passes.
To keep your infection risk low, don’t put anything into your vagina for a week—no douching (which is never a good idea at any time), vaginal sex, tampons, or menstrual cups. You can use pads to absorb the bleeding. Most women have their first period about 2 weeks after any spotting or light bleeding ends, which is usually about 2 to 3 months after you pass the tissue or have a D&C.
People have different emotional reactions.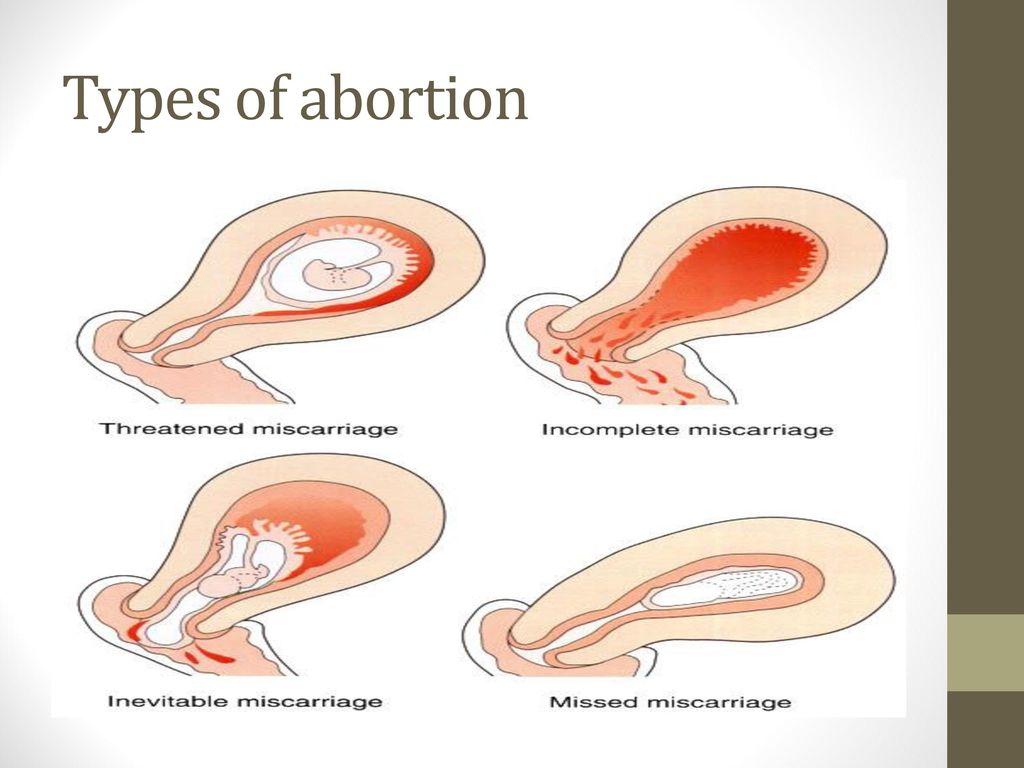 Some women feel sadness or grief. Others may feel relief. Some may feel a mixture of emotions. All these feelings are normal, and it’s important to allow yourself time to process them.
Some women feel sadness or grief. Others may feel relief. Some may feel a mixture of emotions. All these feelings are normal, and it’s important to allow yourself time to process them.
Talking about these feelings with friends, family, your ob-gyn, or a mental health professional can help. If you feel depressed or are thinking of hurting yourself, tell your ob-gyn or another doctor right away. Support groups and resources, such as Share Pregnancy & Infant Loss Support, may be helpful too.
Miscarriage isn’t your fault. Women often worry that they somehow caused their miscarriage. This is not the case. Physical activity, stress, and sex don’t cause miscarriages. Most happen because the pregnancy wasn’t developing normally. Often, the egg or sperm develops with more or fewer chromosomes than normal, which can lead to miscarriage. This is a random event that you cannot control.
Most women can have a healthy pregnancy after a miscarriage. Talk with your ob-gyn if you have concerns. Your ob-gyn can help ease your fears, answer any questions, and talk about preparing for your next pregnancy.
Talk with your ob-gyn if you have concerns. Your ob-gyn can help ease your fears, answer any questions, and talk about preparing for your next pregnancy.
Published: June 2022
Last reviewed: June 2022
Copyright 2023 by the American College of Obstetricians and Gynecologists. All rights reserved. Read copyright and permissions information.
This information is designed as an educational aid for the public. It offers current information and opinions related to women's health. It is not intended as a statement of the standard of care. It does not explain all of the proper treatments or methods of care. It is not a substitute for the advice of a physician. Read ACOG’s complete disclaimer.
Miscarriage. What to do after a miscarriage?
When a woman finds out about her pregnancy, she changes her rhythm of life, especially if the pregnancy is desired. However, depending on many circumstances, miscarriage , that is, a natural termination of pregnancy, may occur. Statistics say that up to 20 percent of pregnancies end in pathological abortions. Often a woman may not know that she was pregnant, as a miscarriage sometimes occurs at a very early stage and seems to be just a normal delay in menstruation followed by heavy discharge.
Statistics say that up to 20 percent of pregnancies end in pathological abortions. Often a woman may not know that she was pregnant, as a miscarriage sometimes occurs at a very early stage and seems to be just a normal delay in menstruation followed by heavy discharge.
If a woman finds out that she is pregnant and wants to become a mother, she should be very attentive to her condition. The threat of miscarriage often occurs in the early stages of pregnancy and therefore it is necessary to know what symptoms and signs precede a sudden miscarriage.
Signs
The main sign of a suspected miscarriage is bleeding from the uterus. They happen not abundant, pale scarlet or gray-brown. The discharge most often gradually increases and is characterized by sudden spasms or pulling pains in the lower abdomen. These symptoms may last for some time.
The pains are often so mild that the woman simply does not pay attention to them.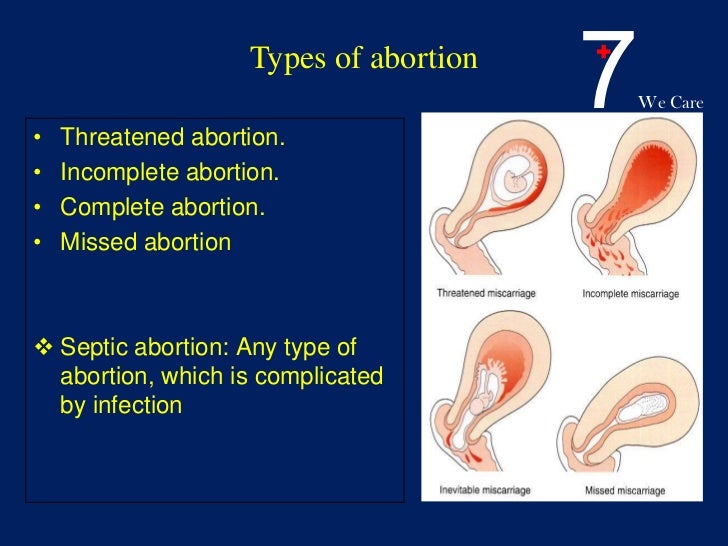 They are able to be interrupted, and the woman simply forgets about them, especially if the discharge also stopped, and before that they were insignificant. Meanwhile, the very first symptoms should alert you and you should urgently go to the gynecologist for examination and consultation. Even if the process has stopped, after a few days you can feel a sharp deterioration in health, and then you can no longer save the life of the unborn child. Be sure to pay attention to what exactly comes out with the discharge, if there are tissue fragments, it means that miscarriage has already occurred. Therefore, one should not hesitate to go to the doctor, the fetus may come out, in whole or in parts, there may be white particles or a round gray bubble. When the body is completely cleansed, the pain will subside, but before that it may continue for some time.
They are able to be interrupted, and the woman simply forgets about them, especially if the discharge also stopped, and before that they were insignificant. Meanwhile, the very first symptoms should alert you and you should urgently go to the gynecologist for examination and consultation. Even if the process has stopped, after a few days you can feel a sharp deterioration in health, and then you can no longer save the life of the unborn child. Be sure to pay attention to what exactly comes out with the discharge, if there are tissue fragments, it means that miscarriage has already occurred. Therefore, one should not hesitate to go to the doctor, the fetus may come out, in whole or in parts, there may be white particles or a round gray bubble. When the body is completely cleansed, the pain will subside, but before that it may continue for some time.
Terms of miscarriages
A miscarriage is classified as early if it occurred before twelve weeks from the onset of pregnancy. Starting from the 22nd week, if a spontaneous miscarriage has occurred, it is considered late. If the termination of pregnancy occurred before thirty-seven weeks, then this is already called premature birth. All subsequent fetal rejections are called term births and are generally considered normal, since during this period, mostly able-to-survive children are born. In modern medicine, children born after 22 weeks are nursed and subsequently do not differ from those born at term with normal weight.
Starting from the 22nd week, if a spontaneous miscarriage has occurred, it is considered late. If the termination of pregnancy occurred before thirty-seven weeks, then this is already called premature birth. All subsequent fetal rejections are called term births and are generally considered normal, since during this period, mostly able-to-survive children are born. In modern medicine, children born after 22 weeks are nursed and subsequently do not differ from those born at term with normal weight.
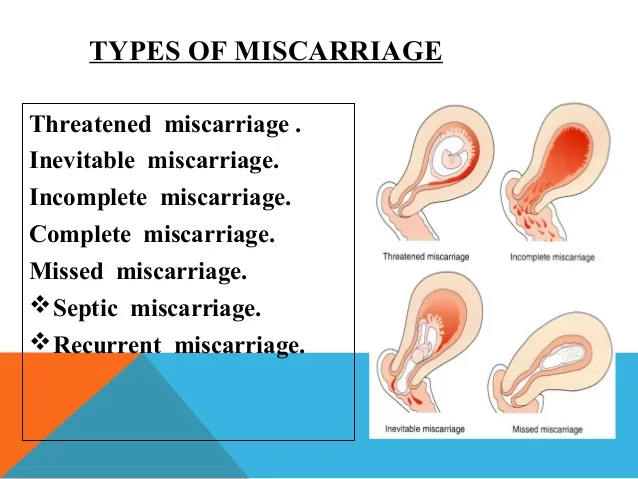
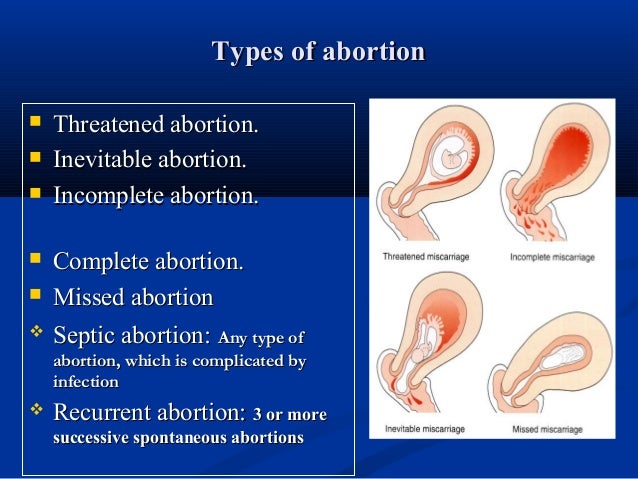
Types of miscarriages
Specialists have identified several types of miscarriages.
- Complete or inevitable - characterized by pain in the lower back and dilatation of the cervix, hemorrhages from it. The fetal membrane necessarily bursts, and the pregnancy is terminated. The fetus comes out of the uterus, and all discomfort in the form of pain and bleeding stops.
- Miscarriage is different in that the fetus died, but remained in the mother's body.
 This can be detected by a doctor when examining a woman and when listening to the fetal heartbeat.
This can be detected by a doctor when examining a woman and when listening to the fetal heartbeat. - Repeated miscarriage is rare, it occurs only some time after the first and can occur up to three times in a row in the early stages.
Causes of spontaneous abortion
The vast majority of women, having learned about their pregnancy, want to give birth to a healthy baby. And if there is a spontaneous miscarriage , then for a failed mother this is a real tragedy. Many, having experienced an abortion, try to conceive a child faster again, but first you need to know the reasons for what happened in order to save the fetus in the future. According to statistics, the largest number of miscarriages occurs precisely in the early stages.
There are several reasons for this:
- Violations in genetics.
This is the most common cause of miscarriage. This is not due to heredity, it is a consequence of the mutation of parent germ cells, which accidentally ended up in unfavorable conditions. This is also the influence of radiation, poisoning, viruses, that is, temporary situations that affected the quality of germ cells. The body thus gets rid of a weak non-viable fetus. It is impossible and unnecessary to prevent such spontaneous abortion. It is only necessary, having decided to become pregnant, to try to cleanse your body of possible harmful influences.
This is not due to heredity, it is a consequence of the mutation of parent germ cells, which accidentally ended up in unfavorable conditions. This is also the influence of radiation, poisoning, viruses, that is, temporary situations that affected the quality of germ cells. The body thus gets rid of a weak non-viable fetus. It is impossible and unnecessary to prevent such spontaneous abortion. It is only necessary, having decided to become pregnant, to try to cleanse your body of possible harmful influences.
- Hormonal disorders
The cause of miscarriage at a very early stage also lies in the lack of the hormone progesterone, or in the fact that a woman has an excess of male sex hormones that suppress the production of estrogen and progesterone in her body. In this case, the fetus can be saved medically by administering the necessary medicines to the woman. The work of the adrenal glands, as well as the thyroid gland, affects the production of hormones, so a lot depends on the work of these glands throughout the pregnancy process.
- Immunological causes .
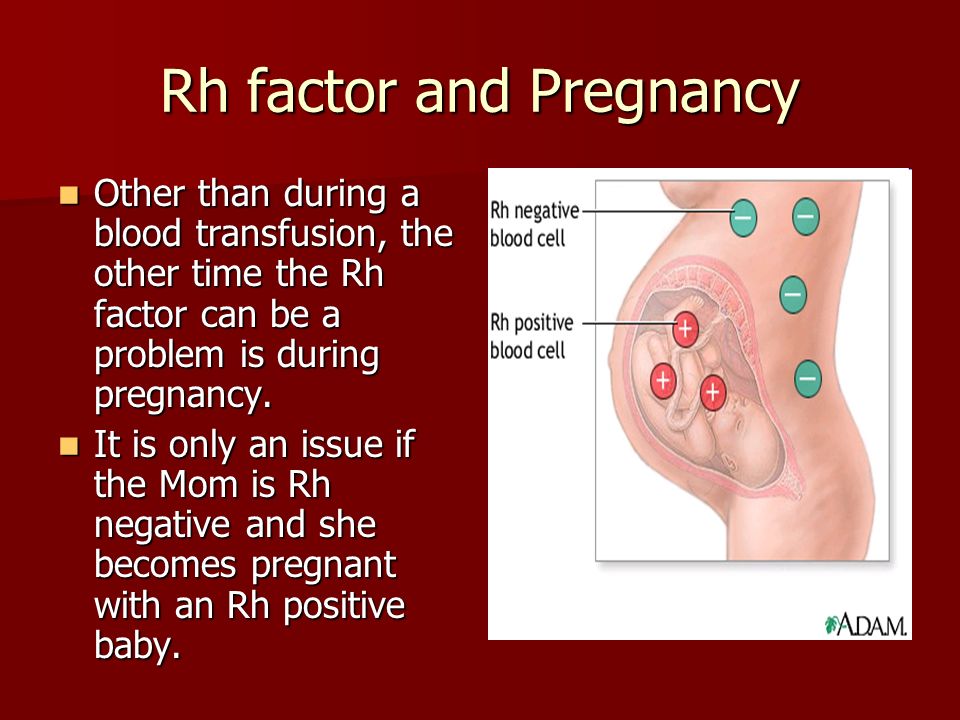
In this case, the vitality of the fetus is directly affected by the Rh conflict. The embryo will inherit the positive Rh of the man, and if the partner has a negative Rh, then her body simply rejects cells that are foreign to him. A similar situation can be prevented by injecting the expectant mother with a variety of progesterone, a process called immunomodulation.
Sexually transmitted infections such as toxoplasmosis, syphilis, trichomoniasis, chlamydia and others are of great danger. External infection: bacteria and viruses infect the fetal membranes, and the body will inevitably reject the embryo. Therefore, before becoming pregnant, you should be examined to know for sure that there are no infections, and if the result is positive, undergo treatment.
In addition, all inflammatory processes, various diseases of the internal organs, which are accompanied by a persistent high temperature, can also lead to unexpected rejection of the fetus. Rubella is especially dangerous, and viral hepatitis is common. But even a sore throat, mild pneumonia, appendicitis sometimes play a key role and lead to a miscarriage, so the expectant mother must undergo a thorough examination even before the child is conceived, and then beware of all kinds of infections and weakening of the body.
Rubella is especially dangerous, and viral hepatitis is common. But even a sore throat, mild pneumonia, appendicitis sometimes play a key role and lead to a miscarriage, so the expectant mother must undergo a thorough examination even before the child is conceived, and then beware of all kinds of infections and weakening of the body.
- Medical abortion.
If a woman had an abortion in a hospital and then became pregnant and decided to give birth, there is a danger that she will have a miscarriage. Abortion is a stress factor for the body, ovarian dysfunction is often observed, inflammatory processes in the female genital organs can begin, and all this will lead, at best, to miscarriage and subsequent repeated miscarriages, and at worst, to infertility. Therefore, you need to think very seriously before going for an abortion.
- Medicines and certain herbs.
It is advisable for a pregnant woman not to take any medication at all, especially during the first three calendar months. Medicines and herbs can cause various defects in the fetus, which in turn will lead to its rejection. Analgesics and uncontrolled hormonal contraceptives are especially dangerous. Parsley and nettle should be eaten with caution - they cause a high tone of the uterus, which in turn can reject the fetus.
Medicines and herbs can cause various defects in the fetus, which in turn will lead to its rejection. Analgesics and uncontrolled hormonal contraceptives are especially dangerous. Parsley and nettle should be eaten with caution - they cause a high tone of the uterus, which in turn can reject the fetus.
- Stress.
It is no coincidence that in ancient times, pregnant women were protected from unrest, they were created comfortable conditions, and they tried to give as many positive emotions as possible. Now the direct dependence of the health of the unborn baby on the mental state during pregnancy has already been proven. Any stress, fear and overstrain can cause an unexpected termination of pregnancy. If you have a problem (death of a loved one, divorce, etc.), you need to find sedatives with the help of a doctor, they will help you cope with this period.
- Unhealthy lifestyle.
Of course, the intake of alcoholic beverages, an unhealthy lifestyle, smoking, even coffee consumption in large quantities, improper diet - all this can lead to a transient miscarriage. Therefore, the expectant mother should prioritize and change her rhythm of life in advance in order to give birth to a healthy child.
Therefore, the expectant mother should prioritize and change her rhythm of life in advance in order to give birth to a healthy child.
- Sexual intercourse, falling, heavy lifting.
All of these factors can affect the fetus, so you should protect yourself and your baby by avoiding these activities.
What to do after a miscarriage?
Having experienced the tragedy of losing a child, parents often intend to immediately conceive a new baby, but they are afraid that everything will happen again. In this case, you do not need to make independent decisions, but consult a doctor. And first of all, it is necessary to identify the cause that led to the miscarriage. For this, the expectant mother needs to undergo as thorough an examination as possible.
If no obvious cause is found, the fetus most likely has a chromosomal abnormality. In this case, you should not worry, since the next conception will occur with a different set of chromosomes, which means that there will be no repeated miscarriage. If the miscarriage was repeated, it is necessary to contact a geneticist and conduct a study of the set of chromosomes of both parents. If it turns out that the cause was an infection, then it is necessary to fully recover. If we are talking about sexual infections, then both parents need to undergo therapy. It is necessary to take tests for hormonal studies, hemostasis systems and determine the immune status.
If the miscarriage was repeated, it is necessary to contact a geneticist and conduct a study of the set of chromosomes of both parents. If it turns out that the cause was an infection, then it is necessary to fully recover. If we are talking about sexual infections, then both parents need to undergo therapy. It is necessary to take tests for hormonal studies, hemostasis systems and determine the immune status.
After a miscarriage, should be treated, if necessary, and pause between conceptions. During pregnancy, you should not take medications to prevent re-spontaneous pathological termination of pregnancy. Therefore, you can become pregnant only after the end of the course of treatment. If the cause was hormonal abnormalities, then the expectant mother should take special drugs to stabilize the background, and at this time she should never become pregnant. During the pause, you need to choose contraceptives with the help of a doctor. You can go to a specialized clinic where you will be prescribed a full course of rehabilitation.
The first week after a miscarriage women often experience pain in the lower abdomen, heavy bleeding, so you should refrain from sexual intercourse with a man. If there is severe bleeding, acute pain in the lower abdomen, convulsions, high fever, palpitations, nausea, vomiting, then you should immediately consult a doctor to identify the cause of this condition. It is necessary to plan a subsequent pregnancy not earlier than three months after this situation, but preferably six months later. Until that time, it is worth reconsidering your outlook on life, giving up hard work, eating right and wisely, taking vitamins, exercising, losing weight if you are overweight, stop smoking, drinking alcohol, think over your daily routine.
It is very important during this recovery period to have a positive attitude and confidence that the next attempt will be successful. This is harder to do than to say, because after a miscarriage the woman is in a depressed state and is afraid of a repetition of the situation. You can’t get hung up on your problem, during this period it’s better to do some favorite thing, relax, change the situation, travel, visit the city more often. The modern ecological situation in cities has a bad effect on women's health, so private trips to nature, a trip to the sea, to friends in another city can distract from painful thoughts. An important role in this case is played by the woman's relatives and, above all, the husband, who can surround her with care and attention, creating peace of mind.
You can’t get hung up on your problem, during this period it’s better to do some favorite thing, relax, change the situation, travel, visit the city more often. The modern ecological situation in cities has a bad effect on women's health, so private trips to nature, a trip to the sea, to friends in another city can distract from painful thoughts. An important role in this case is played by the woman's relatives and, above all, the husband, who can surround her with care and attention, creating peace of mind.
You may need to contact a counseling psychologist or psychotherapist. Yoga classes, self-education, visiting theaters, exhibitions and temples have a very beneficial effect on the psyche of a woman and help to distract from her problems. Helping others who have a difficult life situation, caring for the sick can also have a beneficial psychological effect and help you look at your problems from the outside.
Remember, the human body is a self-healing system, it just needs a little help.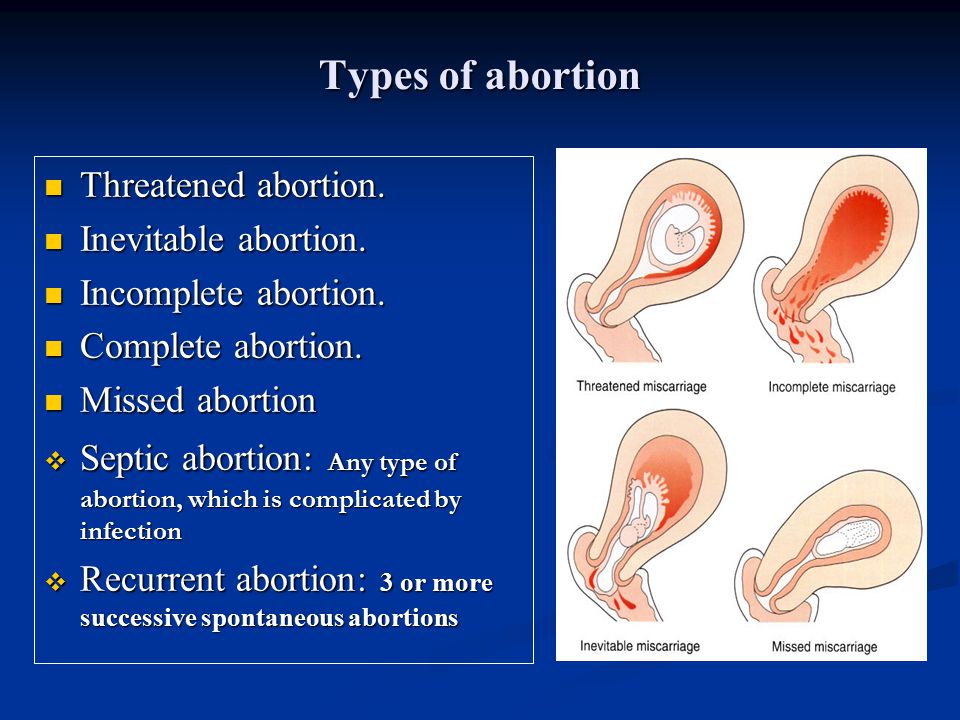
What to do after a miscarriage
If a woman has a miscarriage, it is important to take competent measures to restore her health. This will help to cope mentally and prepare the ground for a new pregnancy. According to medical statistics, 15-20% of pregnancies end in spontaneous termination for various reasons. The symptoms of what happened rarely go unnoticed, which makes it possible to diagnose the pathology in time, consult a gynecologist, undergo adequate treatment and plan the birth of a child for the future.
Experts classify spontaneous abortion into two categories:
1. Termination of biochemical pregnancy - the embryo leaves the uterine cavity in the first or third weeks after conception. A woman during this period most often does not suspect that she is carrying a child. Pregnancy becomes known only when testing for the content of hCG in the urine and blood. The blood that has left the body is usually perceived as menstruation, which, for unknown reasons, began outside the scheduled time.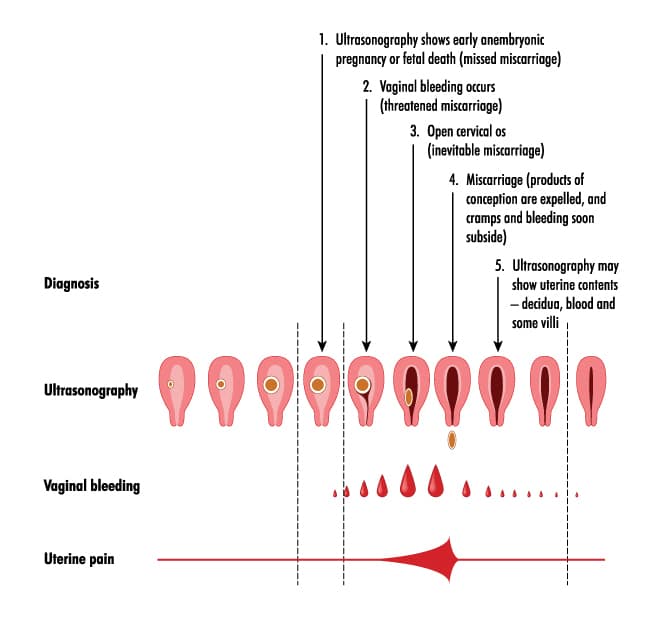 Units who carefully monitor their health go to the doctor.
Units who carefully monitor their health go to the doctor.
2. Spontaneous abortion or miscarriage in early pregnancy - up to 22 weeks, when the weight of the embryo does not reach 0.4 kg.
Medical therapy
Any method is useful to maintain pregnancy. A qualified doctor develops an individual treatment protocol based on the available diagnostic data. Drugs used may include:
- sedatives;
- restorative therapy;
- hormone stabilizing drugs;
- uterine antispasmodics;
- vitamin and mineral supplements.
The specialist eliminates the threat of miscarriage in the early stages, tells how to prevent a relapse. In the later stages, the cervix is fixed with a special suturing (usually for a period of 16-25 weeks, if there is an ICI).
If an attempt to stop a spontaneous abortion fails, the following treatment tactics are used:
- Waiting – an organism freed from an embryo on its own does not require specialized treatment.
- Drug therapy - the patient is prescribed drugs that complete the removal of foreign tissues from the body. By causing severe spasms of the muscular walls of the uterus, the tablets provoke the expulsion of residues from the cavity.
- Surgery - is used in case of complications or inconvenient for the independent exit of the fetus, the bending of the uterus.
Curettage
Having symptoms of a miscarriage in early pregnancy and faced with the need for a curettage (gynecological cleansing), a woman worries about the state of her reproductive system. It is not worth doing this, the operation takes place in a gentle mode, with maximum delicacy in relation to the patient's childbearing ability. Curettage is performed when there is a risk of incomplete exit of the embryo from the uterine cavity and the development of infection in the pelvic organs due to the elements remaining in it. Ignoring the procedure can lead to blood poisoning and the formation of a pathology that prevents re-conception.
Vacuum aspiration, however, is performed more frequently and is more gentle. The complex application of the method with hysteroscopy allows you to carefully examine the internal contents of the uterus in order to prevent poorly cleaned areas on the mucous membrane.
Preparation for gynecological cleaning (curettage)
Gynecological cleaning is carried out for diagnostic and therapeutic purposes for various indications :
- after childbirth;
- in missed pregnancy, miscarriages;
- for menstrual irregularities;
- for accurate diagnosis of gynecological disorders.
Curettage is recommended a few days before the onset of menstruation. In this case, blood loss decreases and a favorable prognosis is given for rapid tissue recovery. The operation requires a preliminary examination, testing. This is :
- complete blood count;
- blood coagulation test;
- smear for examination of the bacteriological environment;
- analysis for STIs.

Before curettage, you stop taking any medications, dietary supplements that have not been discussed with a specialist. Even plant components that can affect blood clotting and provoke blood loss during surgery can be dangerous. Your healthcare provider should be made aware of the medications you are taking so that they know what risks may arise.
Rules for preparing for the procedure:
- refrain from sexual intercourse three days before the operation;
- avoid using intimate hygiene products (gels, creams, ointments, liquids), suppositories, tablets and vaginal sprays;
- Do not douche;
- Do not eat or drink 10 hours before surgery. This is necessary for high-quality anesthesia.
Cleansing
Curettage is carried out in a hospital, the woman is placed on the gynecological chair of the operating room. The doctor removes the upper layer of the mucous lining the uterine cavity from the inside. The exclusion of pain involves anesthesia. If there were signs of miscarriage in the early stages of pregnancy or at a later period, after which it spontaneously terminated, the dilated cervix allows for curettage without anesthesia. For anesthesia, intravenous administration of the drug is used, selected individually, taking into account the characteristics of the patient's body. A few seconds after the injection, the woman falls into a shallow sleep, the discomfort disappears, which makes the doctor's actions painless.
If there were signs of miscarriage in the early stages of pregnancy or at a later period, after which it spontaneously terminated, the dilated cervix allows for curettage without anesthesia. For anesthesia, intravenous administration of the drug is used, selected individually, taking into account the characteristics of the patient's body. A few seconds after the injection, the woman falls into a shallow sleep, the discomfort disappears, which makes the doctor's actions painless.
A dilator inserted into the cervix straightens the walls of the organ, facilitating access to the internal cavity. Holding the neck, the specialist inserts a rounded probe with a small diameter, after which he replaces it with a more voluminous analogue. A special video camera attached to the end of the probe allows for hysteroscopy - examination of the cavity before curettage. Cleaning is done with a curette, shaped like a small spoon on a long handle. Carefully collected tissues are stored in a specialized sterile tube, which is later sent to the laboratory for histological examination.
The procedure rarely takes more than one hour, usually 20 minutes is enough for the doctor. Together with the cavity, the cervical canal is cleaned. Manipulations are called RDV - separate diagnostic curettage. Collected samples are placed separately. Histology is used to identify the structure of tissues in order to exclude the presence of atypical cells in them, indicating cancerous lesions, precancerous conditions. The study is carried out within two weeks, after receiving the results, the woman revisits the gynecologist for a follow-up examination.
Curettage is often carried out for diagnostic purposes to determine the symptoms of pathological conditions in the functioning of the organs of the reproductive system. These can be:
- irregular cycle;
- voluminous discharge and painful menstruation;
- bleeding during menopause;
- difficulties in conceiving in the absence of visible causes of pathology;
- suggestion of developing uterine cancer.

Possible complications
Complications can occur, as after any surgical intervention. A serious consequence is the discovery of uterine bleeding. In order to prevent it, oxytocin is used - injections stimulate the cessation of abnormal blood flow. Oxytocin will help if the bleeding is due to insufficient contraction of the uterus. In violation of blood clotting, it is ineffective.
Another complication of is hematometra, when blood clots accumulate in the uterine cavity, which can cause an inflammatory process in the tissues. It is caused by a spasm of the cervix that occurred immediately after cleaning, which interferes with the evacuation of blood. Experts recommend the use of antispasmodics that relax the muscles of the organ and contribute to the normal outflow of blood. A woman should be alerted by pulling pains in the lower abdomen and a sharp cessation of discharge.
After cleansing, endometritis may occur when inflammation affects the lining of the uterus. A measure of therapy for a dangerous diagnosis is a course of antibiotics. Pain in the abdomen and a sharp increase in body temperature testify to the pathology. Any dangerous change in condition should be reported to the doctor immediately. In this case, countermeasures will be taken in a timely manner, which will eliminate the risks of developing more formidable complications.
A measure of therapy for a dangerous diagnosis is a course of antibiotics. Pain in the abdomen and a sharp increase in body temperature testify to the pathology. Any dangerous change in condition should be reported to the doctor immediately. In this case, countermeasures will be taken in a timely manner, which will eliminate the risks of developing more formidable complications.
How to behave after a miscarriage
A miscarriage that has occurred requires a certain tactic of behavior. Among the measures recommended by doctors:
- It is advisable to postpone a new pregnancy attempt for 3-6 months . Otherwise, the risk of repeating the undesirable development of events is high. If pregnancy occurs before the expiration date, there is no need to panic. The main thing is the supervision of a specialist.
- If you are waiting for , ask for advice on effective contraception.
- Follow your doctor's advice .

- Pass the necessary examinations , take tests.
Consult what effect the medicines you take will have on the fetus if you become pregnant during therapy. Find out after what period of time you can fearlessly try to conceive a child.
How to detect genetic pathologies during repeated pregnancy
If a miscarriage of the first pregnancy occurs due to a genetic factor, it is especially scary to decide on a second one. But you should not be afraid of this, with a well-designed therapy, the chances of success are more than great. Diagnostic procedures today are highly accurate and allow you to identify pathology in the early stages. Examination in this case is mandatory, as well as the following:
- who are over 35;
- has screening changes;
- who had markers of chromosomal pathologies and malformations of the embryo;
- who already have children with chromosomal abnormalities.
Ultrasound diagnostics can detect malformations in 80-85% of cases.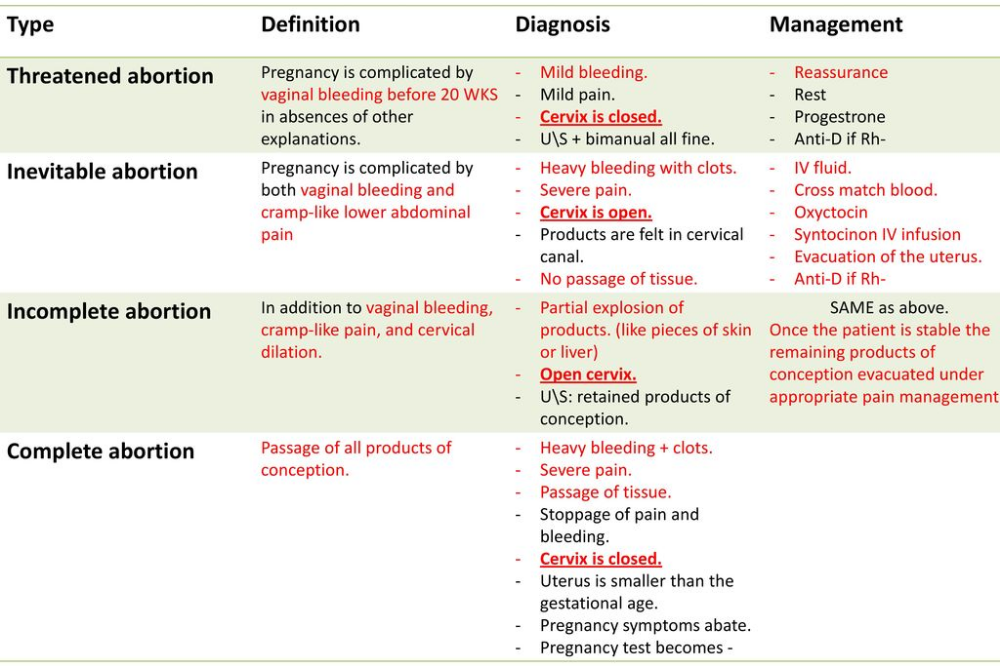 However, the technology is not impeccably reliable, as it misses pathologies in 20% of situations. Biochemical screening, invasive examinations have valid data. The latest version of the study allows you to identify up to 99% anomalies.
However, the technology is not impeccably reliable, as it misses pathologies in 20% of situations. Biochemical screening, invasive examinations have valid data. The latest version of the study allows you to identify up to 99% anomalies.
When planning a new pregnancy, it is imperative to visit a geneticist. Screening diagnostics for the detection of abnormal genes will help eliminate the risks of possible pathologies, the factor of heredity and genetic failure during conception. Sometimes the threat of miscarriage in the early stages exists in almost healthy carriers. The examination will allow you to find out about the anomaly in advance and undergo treatment.
What is a miscarriage like
A miscarriage that has occurred is complete when all parts of the embryo come out of the uterine cavity together with membranes and amniotic fluid. If parts of the fetus remain in the uterus, they speak of an incomplete miscarriage, which occurs more often in the early stages of pregnancy. To neutralize the negative consequences, to prevent the development of an infectious process in the tissues, the product of conception is evacuated from the uterine cavity by the methods of medical interruption, gynecological curettage, and vacuum aspiration. Therapy may include the use of drugs aimed at contracting the uterus and pushing the contents out. Ultrasound examination is considered to be the control method of diagnostics.
To neutralize the negative consequences, to prevent the development of an infectious process in the tissues, the product of conception is evacuated from the uterine cavity by the methods of medical interruption, gynecological curettage, and vacuum aspiration. Therapy may include the use of drugs aimed at contracting the uterus and pushing the contents out. Ultrasound examination is considered to be the control method of diagnostics.
Why the body rejects the embryo
The causes of miscarriage often lie in the presence of chromosomal abnormalities in the fetus. Among the factors provoking rejection of embryos are also:
- Heredity and genetic failure at the stage of fertilization of the egg by the sperm.
- A non-viable fetus may appear as a result of various risk factors - environmental conditions, occupational hazards, viral illness of parents. It is impossible to neutralize these factors. The only way out of the situation is to reduce the likelihood of their manifestation by protecting the expectant mother from dangers during gestation.
- Hormonal imbalance caused by disruption of the endocrine system. The situation can be affected by an insufficient amount of progesterone in the mother's body or an excess of testosterone. With early detection of a failure of the hormonal system, a woman undergoes specially organized therapy before pregnancy.
- The presence of tumors , neoplasms in the pelvic organs.
- Isthmic-cervical insufficiency when the isthmus and cervix dilate prematurely, unable to cope with the increasing pressure caused by the growing fetus in the body.
- There is a risk of miscarriage in the presence of anomalies in the work of the cardiovascular and renal systems.
- Drug addiction , alcohol addiction, substance abuse of mother and father.
- Depressive conditions , stress, nervous stress of a pregnant woman.
- Mechanical stress , blows, bruises, excessive physical labor of the future woman in labor.
- X-ray examination - radiation can cause miscarriage.
- Drug use . In the first trimester, you can not use potent medicinal formulas. Drugs can cause the development of defects in the embryo. Some decoctions of herbs are also contraindicated - parsley, tansy, cornflower, nettle, St. John's wort. It is forbidden to self-medicate. Each drug is agreed with the attending physician.
- Infectious and viral process in the body. Any sexually transmitted infection can provoke a miscarriage, which must be cured before pregnancy, otherwise there is a high risk of infection of the fetus in the womb. A great threat of miscarriage in the early stages exists due to viral infections and inflammation of the internal organs. A dangerous symptom is the high temperature of the mother, accompanied by intoxication of the body. At the stage of pregnancy planning, it is important to stop chronic diseases.
- History of abortion , unsuccessful surgery, unprofessionalism of the doctor and unfortunate circumstances.

- Immunological factors .
The list of causes of miscarriage in the early stages of pregnancy and in the later period may be more extensive, in each case, doctors identify the pathology individually.
Isthmic-cervical insufficiency (ICI)
One of the most common causes of spontaneous miscarriage during pregnancy is CSI - dilatation of the cervix and isthmus of the uterus as a result of increasing pressure from the growing fetus. Pre-pregnancy manipulations with the uterus (cervical dilation due to abortion, childbirth or curettage) affect the condition of the muscle ring. Damaged areas are tightened by scar tissue that does not have elasticity, is not amenable to stretching and contraction. ICI also has a functional nature when there is a hormonal imbalance.
ICI occurs in the period from the 11th to the 27th week after conception, when the embryo begins to produce androgens in the mother's body with the launch of the adrenal glands. Taking into account the mother's hormones, their indicator can be exceeded - this softens the cervix, opens and shortens it. Harmful bacteria and microorganisms penetrate into the formed channel, infecting the fetal egg. The initial stages of ICI do not have obvious symptoms, since they do not entail the tone of the uterine muscles. With the loss of strength of the membranes, amniotic fluid pours out. There are no pain sensations.
Taking into account the mother's hormones, their indicator can be exceeded - this softens the cervix, opens and shortens it. Harmful bacteria and microorganisms penetrate into the formed channel, infecting the fetal egg. The initial stages of ICI do not have obvious symptoms, since they do not entail the tone of the uterine muscles. With the loss of strength of the membranes, amniotic fluid pours out. There are no pain sensations.
If a woman has had a miscarriage that started with amniotic fluid, she should report it to her doctor when monitoring a subsequent pregnancy.
Treatment of isthmic-cervical insufficiency
Endocrine disorders are corrected by prescribing hormonal drugs. An assessment of the condition of the uterus is carried out by a doctor a couple of weeks after the start of taking medications. They say about positive dynamics when the opening is suspended and no further expansion of the neck is observed. In the absence of the planned effect, surgical intervention is prescribed. Similar measures are used for the traumatic nature of the neck deformity. You should not be afraid of the operation, the doctor acts delicately, without causing additional injuries to the patient, without causing discomfort to the baby growing in the womb. The procedure is most effective in the early stages of pregnancy. Suturing can significantly reduce the risk of infection of the embryo through the lower edge of the cavity.
Similar measures are used for the traumatic nature of the neck deformity. You should not be afraid of the operation, the doctor acts delicately, without causing additional injuries to the patient, without causing discomfort to the baby growing in the womb. The procedure is most effective in the early stages of pregnancy. Suturing can significantly reduce the risk of infection of the embryo through the lower edge of the cavity.
Surgical intervention takes place in a hospital setting. Before the operation, the pregnant woman is examined. After the procedure, the vagina is sanitized, for which the suturing site is treated with chlorhexidine and furatsilin for three days. The patient needs to undergo a weekly follow-up examination with the attending physician, where he assesses the situation, making adjustments to the therapeutic protocol if necessary. The sutures are removed at the 38th week of pregnancy. During this time, the neck matures, preparing the birth canal for the passage of the fetus. Many women in labor worry that they will need a caesarean section if they have stitches, but this is not true. In most cases, women give birth on their own.
Many women in labor worry that they will need a caesarean section if they have stitches, but this is not true. In most cases, women give birth on their own.
Immediate action is recommended if the amniotic sac prolapses (falls out) into the cervix between 16 and 24 weeks. The suturing of the neck obliges the woman to observe bed rest, strictly follow the daily routine, avoid physical exertion, and do not skip taking medications. In rare cases, complications occur. Among them, the eruption of sutures through the tissues, provoked by the frequent tension of the muscles of the uterus. To prevent tone, tocolytics are prescribed - medicines to prevent premature birth. The expectant mother should be prepared for frequent examinations and smears, which may be caused by the likelihood of accumulation of pathological microflora on the suture threads.
It is also important to conduct psychological therapy, where a woman is taught relaxation techniques. The behavior of the future mother is a decisive factor in the successful bearing of the fetus in case of pregnancy complications. Panic and fuss create an unfavorable prognosis in stabilizing the situation. If a spontaneous abortion occurred for reasons of ICI, when you can get pregnant after a miscarriage, the doctor will say. Ideally, the period should be at least two years. The specialist must also take measures to prevent a repeated situation of losing a child.
In addition to the suture, ICI correction is also carried out using an obstetric pessary. An alternative method is the imposition of a special ring of hypoallergenic materials on the cervix. Silicone is the most commonly used. The ring creates additional support, preventing the opening of the neck.
Uterine hypertonicity - risk prevention
Uterine contractions before natural delivery is called hypertonicity. The condition is not an independent disease, it signals a malfunction in the body, often manifesting itself in the early stages of pregnancy. The causes of the pathological phenomenon are:
- Hormonal imbalances caused by insufficient function of the placenta, ovaries, problems with the adrenal glands causing imbalance.
- Genital infantilism , organ defects.
- Neoplasms , tumors in the uterus that are not necessarily malignant (eg, fibroids).
- During pregnancy infectious processes, viral diseases.
- CCI - opening of the neck under increasing pressure created by the growing embryo.
- Immunological problems .
- Chronic diseases of the body (cardiovascular disorders, renal insufficiency).
- Past miscarriages early pregnancy, symptoms of which may recur, induced abortions.
In addition to physiological causes, psychological factors are of no small importance. A woman who is in a depressed state can provoke hypertonicity in herself.
You can feel the tension of the muscles of the uterus on your own, without the help of a specialist. This is evidenced by the heaviness that appears in the lower abdomen, pulling pains in the lumbar region. Symptoms are similar to painful menstruation. Arising in the first trimester, the condition provokes spontaneous abortion, missed pregnancy, death of the fetal egg. In the subsequent period, premature birth due to hypertonicity is likely.
Why does tension in the walls of the uterus cause irreversible consequences? The reason is the disturbed blood supply to the placental tissues, the occurrence of hypoxia of the embryo and the slowdown in the development of the emerging child. Following the contraction of the muscles of the uterus, the placenta does not contract, which causes its detachment and provoking the release of the fetal bladder.
Hypertonicity is diagnosed during a scheduled visit to a specialist. Stabilization of the situation requires the appointment of sedative drugs and antispasmodics. A strengthening effect is provided by therapy with the inclusion of vitamin B6, magnesium. In most cases, the measures taken are sufficient to neutralize the risks. Self-treatment, which can cause irreversible consequences, is strictly prohibited. With hypertonicity, the main rule for a pregnant woman is calmness and lack of physical activity. Some women who have had a successful delivery say they "didn't get up" during their entire pregnancy. With hypertonicity, sexual intercourse is also excluded.
If the threat cannot be neutralized, hospitalization is recommended. It is especially dangerous when severe cramping pain is complemented by spotting. To lie down "for preservation" is an adequate measure in the struggle for the birth of a healthy and strong baby. In the hospital walls, a pregnant woman is prescribed a vaginal examination, ultrasound. If necessary, a woman takes urine and blood tests, checks the hormonal background, and is examined for the presence of STIs.
At the beginning of labor activity before the 34th week, the state is tried to be stabilized with tocolytics. The most dangerous period is from the 25th to the 28th week, when the woman is recommended the maximum possible bed rest. After that, the fetus has every chance of survival. In order to quickly form the pulmonary system of the embryo, allowing it to survive with an early birth, hormones are prescribed.
Having an unfavorable prognosis for miscarriage and the threat of miscarriage, it is necessary to take up prevention at the stage of conception planning.
Stages of spontaneous abortion
There are certain signs that attract attention and divide the course of a miscarriage into specific stages:
- Threat - having noticed factors threatening pregnancy, you can take measures to restore the situation, normalize the mother's well-being.
- Start of abortion - at this stage, the doctor can apply life-saving manipulations and give recommendations to the pregnant woman.
- Miscarriage in progress – the condition is irreversible, it is impossible to stop the pathology. The death of the fetal egg begins, which leaves the uterine cavity.
- Completed abortion – the uterus gets rid of the residual tissues of the embryo, is cleansed, and restores its original parameters.
It is important to prevent the remnants of foreign fibers inside, otherwise the organ becomes infected with decaying residues and toxins go into the bloodstream.
Symptoms of miscarriage - how not to miss the threat
If there is a threat of miscarriage in the early stages, the following symptoms may occur: The pain may be monotonous or come in waves.
A woman who does not know how an early miscarriage occurs should listen to her inner state.
Should alert:
- spasmodic pain impulses;
- Drawing pain in the lumbar region.
In the later stages, the above symptoms are added:
- liquid discharge from the vagina, which may indicate damage to the amniotic sac;
- pain when urinating;
- internal bleeding, which warns the deterioration of the general condition, fainting, dizziness, pallor of the skin.
All this is an indication for emergency hospitalization of a pregnant woman.
The beginning of an abortion is characterized by more pronounced symptoms of a miscarriage - contraction-like pain, severe dizziness, loss of strength. Instead of smearing discharges, clot-like ones appear, abundantly manifested during movement. Pregnancy can be saved if the area of detachment of the fetal egg is small and the fetal heartbeat is determined.
The third stage is useless to save the fetus. There is girdle pain in the lower back and abdomen. Together with abundant blood loss, a fetal egg comes out of the uterus. Incomplete miscarriage requires curettage of the uterine cavity if parts of the embryo or membranes of the fetal egg remain in it, otherwise there is a high risk of complications that will endanger the life of the mother.
In rare cases, complications and serious health consequences can occur after a spontaneous abortion. But in the majority of situations, the body independently copes with what happened, expelling the parts remaining in the uterine cavity with a natural contraction of the muscles. An early spontaneous miscarriage does not always occur, a dangerous condition can also occur in the later stages. Some women try to provoke the release of the fetus with decoctions of herbs and medications. This is fraught with complications, including sepsis, dysfunction of the reproductive organs, after which pregnancy becomes impossible.
Methods of diagnosis
The symptoms of a threatened miscarriage at an early stage will be determined by a doctor during a visit to the antenatal clinic. The specialist will check the size of the uterus, determine the tone of its muscles, the condition of the cervix, and examine the discharge from the genital organs. A reliable method to identify the existing threat is transvaginal ultrasound diagnostics. The doctor draws attention to segmental muscle contractions of the uterus, detachment of the fetal egg. Genetic testing will help analyze the likely causes of a miscarriage. The patient's history is carefully collected.
Planning a new pregnancy
The medical community is unanimous in the issue of planning a new pregnancy after a spontaneous abortion. Conception is not recommended for at least 3-6 months. During this period, the woman's body will recover and gain strength to bear the fetus. Observation by a doctor, harmonization of hormonal levels, examination of parents to identify possible pathologies are important. In order not to become pregnant in the first months, it is recommended to use contraceptive methods prescribed by your doctor.
Examination after a miscarriage includes blood and urine tests, examination of the microflora of the vagina with a smear, detection of overt and latent genital infections, glucose and hormone tests, examination of partners for biological compatibility. Planning is an important step towards having a healthy baby. After the studies, the woman is prescribed strengthening therapy. It is important to completely reconsider eating habits, to exclude factors that are harmful to well-being. Vitamins, folic acid are used. Fast food, food containing carcinogens and preservatives are excluded from the diet. Subject to the rules recommended by the doctor, a successful pregnancy with a favorable outcome is likely.
It is not uncommon for a pregnancy test to show two lines after a miscarriage. This is due to the restructuring of the body, the organs of the reproductive system. It is important to report the incident to your doctor. The presence of remnants of embryonic tissue in the uterus can provoke a positive test result. In this case, immediate curettage is necessary, which neutralizes the risk of inflammation and infection. To accurately determine her condition, a woman needs to undergo an ultrasound diagnosis, take tests to determine hCG in the blood.
The question of whether it is possible to get pregnant after a miscarriage worries many parents. The answer is unequivocal - yes, if you follow the recommendations of experts, carefully plan a new conception, monitor your well-being and state of your health.
Components of success after a miscarriage
Spontaneous abortion can provoke not only the health of the patient, but non-compliance with simple rules can be a threat. To reduce the risk of losing a child during pregnancy, you need to:
1. Keep calm – it is important for a mother to exclude from her life all the factors that make her nervous. Irritation is not the best way to normalize the condition. In order to stabilize the emotional background, rest is recommended, the use of soothing teas with the permission of the doctor. Good results are given by decoctions of chamomile, lemon balm, mint.
2. Avoid taking unnecessary medicines and preparations. But it is unacceptable to stop the therapy prescribed by the doctor on your own. Each step must be discussed with the gynecologist.
3. Eliminate harmful occupational factors. Work in the chemical industry and other hazardous facilities can create an undesirable background in the body, which prevents normal gestation. It is important to understand what is of great value to the mother - the birth of a healthy baby or a career factor. Many refuse to work to increase the chance of having a baby.
4. Eliminate bad habits. It is unacceptable for a woman who has experienced miscarriage to drink alcohol and smoke. It is forbidden to do this and the future father. This negatively affects the quality of spermatozoa, provokes difficulties with conception and risks of deviations in the development of the embryo.
5. Take vitamin complexes, specially designed to prepare the body for pregnancy, the formation of basic conditions for its favorable course.
6. Eat right. A complete, balanced diet works wonders. With a lack of weight, a nutritionist will develop an adequate diet for a woman with the inclusion of a large amount of protein foods rich in vitamins and trace elements of vegetables, fruits, and cereals. Recommended fats contained in fish, seeds, nuts, avocados, olives.
7. Get rid of extra pounds. Obesity adversely affects the development of pregnancy. Science has proven that enhanced nutrition during this period is not required. The main thing is its balance.
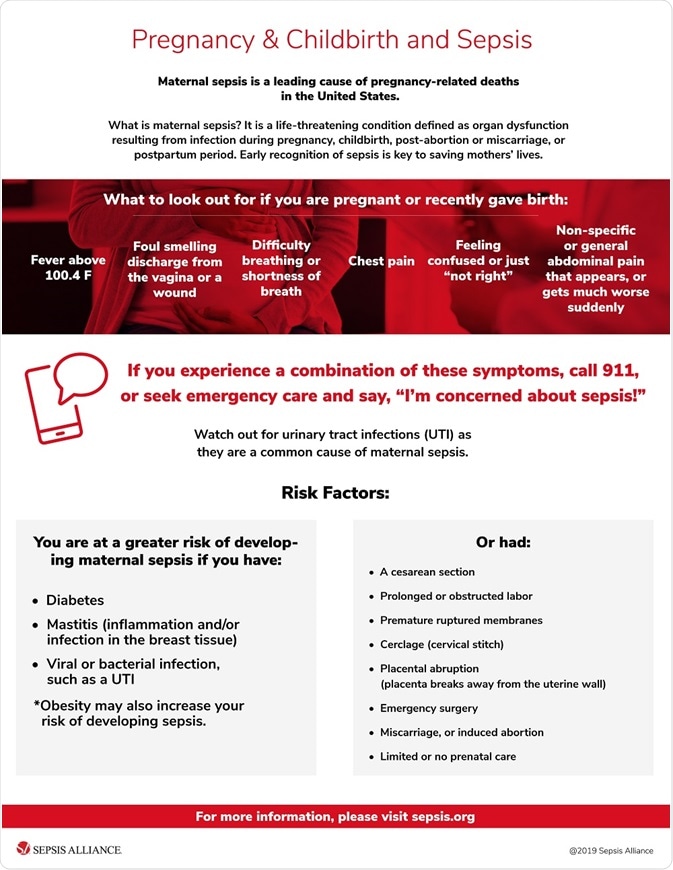
Infections during pregnancy
Infectious processes transferred before pregnancy develop immunity in the mother to similar agents of influence. Primary infection poses a great threat, so vaccination will be useful before planning conception. Perinatal diagnosis allows you to detect the infectious process at the initial stage and prevent its harmful effects. This is possible if the pregnant woman is registered from an early date.
Infection may develop due to an infection transmitted by airborne droplets. It is the most dangerous, since it is almost impossible to prevent it. This applies to mumps, measles, rubella. HIV and hepatitis infect the body through sexual contact, similar to chlamydia. Listeriosis is transmitted with poor-quality products. A pregnant woman can pass infections to a developing baby. Pathology is determined by profile tests of latent infection.
Routine pregnancy monitoring involves regular testing. Sexual infections are determined using a smear, ultrasound shows deviations in the development of the baby, and KGT is aimed at listening to the work of the fetal heart muscle. If there is a suspicion of a serious infection of the embryo, blood sampling from the umbilical cord and amniotic fluid analysis are practiced.
Infection of a child also depends on concomitant factors. The speed of diagnosis, the literacy of the treatment, the type of pathogen, the duration of the pregnancy are taken into account. The following infectious processes deserve special attention:
1. Viral etiology - a huge number of viruses pose a danger to a pregnant woman. The threat is genital herpes, rubella, infectious type erythema, cytomegalovirus, hepatitis B, measles, mumps, chickenpox.
2. Bacterial infections, detected during the analysis of biological materials (feces, urine, blood), examination of certain organs of the body. Active reproduction provokes a rapid growth in the number of bacteria in the vagina. Not all microorganisms pose a threat to the child. Dangerous candidiasis, streptococcus, chlamydia, bacterial vaginosis, cystitis.
The successful course of pregnancy is threatened by intestinal infections, often activated in the summer. Their carriers can be animals and poorly processed food before consumption. Of particular danger are listeriosis, salmonellosis, toxoplasmosis.
Prevention of infections during pregnancy
Infection of the mother poses a threat to the life of the fetus. From the 3rd to the 12th week, the infected organism responds with a miscarriage or the formation of malformations of the child. From the 11th to the 25th - developmental delay. At a later date, organs are deformed and prerequisites for premature birth are created. In order to prevent intrauterine infection, it is recommended to apply a number of rules:
- be examined for the detection of STIs;
- examine blood, determine the presence of antibodies to infection carriers, pathogens;
- avoid contact with sick people, visits to crowded places where there is a possibility of infection by airborne droplets;
- Examine pets for dangerous infections, treat them if necessary, or remove them from the home until the threat is eliminated;
- exclude fast food, store-bought semi-finished products from the diet, thoroughly heat treat meat, fish;
- remove from the diet sushi and other culinary delights purchased in restaurants, cafes;
- thoroughly wash hands, fruits, vegetables with special disinfectants that are not capable of harming a pregnant woman and a child;
- it is planned to visit a gynecologist, undergo examinations recommended by a doctor, take tests, take vitamins;
- register at the first sign of pregnancy;
- prepare for conception, cure infections, vaccinate.
It is also important for the child's father to follow most of the recommended rules. If only the mother undergoes treatment, a relapse is likely during sexual intercourse, neutralizing the beneficial effect of therapy.
A woman who has had a miscarriage in the past should be alert to any deviations from the norm in her state of health. It is important to pay attention to ailments, pain, weakness, dizziness. Accounting for an early consultation will create conditions for the bearing of the fetus and the birth of a child. There is no need to be afraid that a miscarriage will forever deprive the joy of motherhood.
After completing a course of examinations, passing tests and following the measures prescribed by the doctor to treat imbalances in the body, you will create all the conditions for a favorable outcome of pregnancy. Tune in to the positive, protect yourself from worries, worries, stress. Feel the support of loved ones, hope for the best! Get advice from good specialists to rule out any unfavorable prognosis before conception or take steps to neutralize them.