Underweight baby in womb
Intrauterine Growth Restriction (IUGR) (for Parents)
What Is Intrauterine Growth Restriction (IUGR)?
Intrauterine growth restriction, or IUGR, is when a baby in the womb (a fetus) does not grow as expected. The baby is not as big as would be expected for the stage of the mother's pregnancy. This timing is known as an unborn baby's "gestational age."
The two types of IUGR are:
- symmetrical IUGR: all parts of the baby's body are similarly small in size
- asymmetrical IUGR: the baby's head and brain are the expected size, but the rest of the baby's body is small
What Causes IUGR?
Often, IUGR happens because the fetus doesn't get enough nutrients and nourishment. This can happen if there is a problem with:
- the placenta, the tissue that brings nutrients and oxygen to the developing baby
- the blood flow in the umbilical cord, which connects the baby to the placenta
Intrauterine growth restriction also can happen if a pregnant woman:
- smokes, drinks alcohol, or uses drugs
- has an infection, such as cytomegalovirus, German measles (rubella), toxoplasmosis, or syphilis
- takes some types of medicines, such as some seizure treatments
- has a medical condition such as lupus, anemia, or clotting problems
- has high blood pressure (hypertension)
- is carrying a baby that has a genetic disorder or birth defect
- is pregnant with multiples (such as twins or triplets)
How Is IUGR Diagnosed?
Before babies are born, doctors check their growth by measuring the mother's belly from the top of the pubic bone to the top of the uterus. This is called the uterine fundal height.
They also can do a prenatal ultrasound, which is how IUGR often is diagnosed. A technician coats the woman's belly with a gel and then moves a probe (wand-like instrument) over it. High-frequency sound waves create pictures of the baby on a computer screen. These pictures help doctors estimate the baby's size and weight. These estimates aren't exact, but they do help health care providers track the baby's growth and see if there's a problem. Ultrasounds also can help find other issues, such as problems with the placenta or a low level of amniotic fluid (the fluid surrounding the fetus). Doctors will also use ultrasounds to check the blood flow to the placenta and through the umbilical cord.
If they think a baby has IUGR, doctors also might do such tests as:
- fetal monitoring to track the baby's heart rate and movements
- screening the mother for infections that could affect the baby
- amniocentesis to look for genetic causes of IUGR (and sometimes to help them see how mature the baby's lungs are)
How Is IUGR Treated?
Treatment for intrauterine growth restriction depends on how far along the pregnancy is and how the baby is doing. Doctors will watch a baby with IUGR closely during prenatal visits. They'll do ultrasounds, keep track of growth, and watch for other problems.
Doctors will watch a baby with IUGR closely during prenatal visits. They'll do ultrasounds, keep track of growth, and watch for other problems.
If the baby's mother has a condition, doctors will help her manage it. This might include making sure she eats a healthy and nutritious diet and gains the right amount of weight during her pregnancy. Some women might go on bed rest to try to improve blood flow to the baby.
Sometimes, doctors will recommend inducing labor and delivery early. They might do this if the baby seems to have stopped growing, or if there's a problem with the placenta or the blood flow in the umbilical cord.
A woman might have a cesarean section (C-section) if the stress of a vaginal delivery is considered too risky for the baby.
What Problems Can Happen?
Babies with IUGR are more at risk for some kinds of health problems. Those born early or who are very small at birth are more likely to need to stay in the hospital for a longer time. They also might need special care in the neonatal intensive care unit (the NICU).
Other problems that can be related to intrauterine growth restriction include:
- problems with breathing and feeding
- trouble keeping a steady body temperature
- abnormal blood cell counts
- low blood sugar level (hypoglycemia)
- problems fighting off infections
- neurological problems
The long-term effects of IUGR on a baby may depend on the condition that caused the problem.
What Can I Do if My Baby Has IUGR?
If your baby might have IUGR, follow your doctor's advice and go to all prenatal visits and testing appointments. This helps your doctor see how your baby is developing and growing.
Take good care of yourself by:
- eating a healthy diet
- getting enough sleep
- avoiding alcohol, drugs, and tobacco
Reviewed by: Larissa Hirsch, MD
Date reviewed: July 2020
IUGR—Why Is My Baby Small and What Can Be Done About It?
What is IUGR?
IUGR stands for intrauterine growth retardation. This means that your baby is growing slowly and doesn't weigh as much as your doctor expected for this stage of pregnancy. If your unborn baby weighs less than most babies at this stage, your baby might have IUGR. IUGR is also used to describe a baby who weighs less at birth than most babies at the same stage. For babies who are born near their due date (meaning, they aren't premature), the dangerous weight is anything less than 5 pounds, 8 ounces.
This means that your baby is growing slowly and doesn't weigh as much as your doctor expected for this stage of pregnancy. If your unborn baby weighs less than most babies at this stage, your baby might have IUGR. IUGR is also used to describe a baby who weighs less at birth than most babies at the same stage. For babies who are born near their due date (meaning, they aren't premature), the dangerous weight is anything less than 5 pounds, 8 ounces.
Your doctor might suspect IUGR if he or she thinks your baby is growing slightly less than would be expected. IUGR is usually diagnosed during an ultrasound examination. Doctors most often find it during the 6th, the 7th or the 8th months of pregnancy.
It's important to know that IUGR only means slowed growing. These small babies aren't mentally slow or retarded. Most small babies grow up to be healthy children and adults.
Why is my baby small?
Doctors know many of the causes of IUGR but are only able to be sure about the cause in about one half of babies who have IUGR. The most common reasons for a baby to be small are the following:
The most common reasons for a baby to be small are the following:
The mother smoked cigarettes during pregnancy.
The mother drank alcohol during pregnancy.
The mother had high blood pressure during pregnancy.
The mother had infections during pregnancy.
The baby has chromosomal abnormalities (like Down syndrome).
The mother used certain medicines during pregnancy.
The mother is small (less than 5 feet tall or weighing less than 110 pounds).
Why is my baby's size important?
The best predictor of a baby's survival and good health is its birth weight. Babies born with low birth weight might have problems near the time of birth. Because of the danger of some of these problems—such as difficulty holding a normal body temperature or fighting infection—your doctor will do some tests to find out if your baby is growing well, both before and after birth.
What tests might be done on my baby?
Two tests can find out if your baby has IUGR and keep track of your baby's growth in the womb. These tests are the ultrasound exam and the nonstress test. The first kind of test, the ultrasound exam, is used to find out if your baby has IUGR. This exam is done every three to four weeks to make sure your baby is still growing right. The ultrasound exams let your doctor look at your baby's internal organs and measure the amount of fluid around the baby.
Special ultrasound exams are called biophysical profiles. During a biophysical profile, the person who does the exam will also watch your baby's breathing, muscle tone and movements.
The other test is the nonstress test. This test is usually done in the doctor's office, but it might be done in a hospital. A nonstress test measures how fast your baby's heart is beating. A healthy baby normally has a heartbeat that gets faster as the baby moves around. A nonstress test takes about 20 to 30 minutes to do.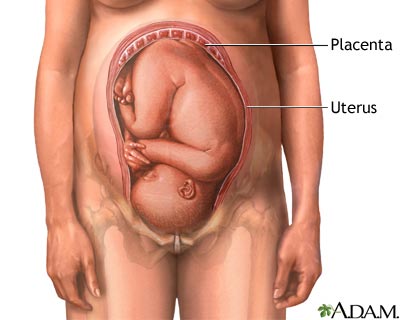 It might take longer if your baby is asleep.
It might take longer if your baby is asleep.
Sometimes your doctor wants to watch your baby's heartbeat while your uterus contracts (squeezes together). This is called a contraction stress test. There are two ways to help you have contractions for just a little while. First, your nipples will be warmed up. Sometimes this makes your uterus start contracting for a little while. If that doesn't work, you could take a special medicine (either oxytocin or pitocin), to make your uterus contract just for a little while.
What happens if a test isn't normal?
If one of the tests isn't normal, your doctor may want to do other tests. Your doctor may also try to start your labor early (induce labor) if you might have a problem.
What will the doctor do to help my baby?
If your baby is very small when it's born, your doctor can give it oxygen through a nose tube, fluids through a tube in a vein and, sometimes, antibiotics.
What can I do to help my baby?
You can do five important things to help your baby grow big enough before it's born:
If you smoke—quit now.
 Cigarettes hurt the placenta, which is your baby's only way to get “food.” It's never too late to quit smoking. Babies gain one half of their weight in the last three months before being born.
Cigarettes hurt the placenta, which is your baby's only way to get “food.” It's never too late to quit smoking. Babies gain one half of their weight in the last three months before being born.If you drink alcohol—quit now. Even one drink a day makes it more likely that you will have a small baby. You could even have a baby with brain damage caused by the alcohol. This can happen in all months of pregnancy.
If you use illegal drugs—quit now. Almost all illegal drugs make babies too small to be strong and healthy. You may need your doctor's help to quit so you don't have withdrawal problems.
Eat a good diet. Ask your doctor to tell you the best foods to eat.
Keep all your appointments for doctor visits and tests.
Fetal growth retardation (FGR)
Gynecology
It happens that expectant mothers hear a frighteningly incomprehensible abbreviation - ZRP at the appointment with the attending physician or in the ultrasound room. Its decoding is even more frightening: "delayed fetal development." A pregnant woman faced with a similar diagnosis is tormented by many questions. How dangerous is this condition? How will it affect the health of the baby? Will he be able to catch up?
Its decoding is even more frightening: "delayed fetal development." A pregnant woman faced with a similar diagnosis is tormented by many questions. How dangerous is this condition? How will it affect the health of the baby? Will he be able to catch up?
The weight of a child at birth is very important for his development, especially in the first year of life, and affects his health later on. Children born with low body weight (up to 2500 grams) are more prone to obstetric complications: they tolerate childbirth worse, they develop hypoxia and even asphyxia more often than children with normal weight, and neurological disorders also occur.
Children born with low body weight (up to 2500 grams) are more prone to obstetric complications: they tolerate childbirth worse, they develop hypoxia and even asphyxia more often than children with normal weight, and neurological disorders also occur.
As a result, these babies do not adapt well to a new life. In infancy, they suffer from hyperexcitability, increased or, conversely, decreased muscle tone, sluggishly suck and often spit up food, gain weight poorly, and may lag behind their peers in psychomotor development. Even at the age of 7-8 years, such children are hyperactive, clumsy and do not know how to concentrate on the necessary subject for a long time. The difference between healthy babies and small babies only blurs by 9-10 years, although in height and weight they catch up with their peers by the age of two. However, the consequences of the transferred condition can “come around” already in adulthood. Recent studies have shown an association between low birth weight and an increased risk of developing cardiovascular disease, obesity, diabetes mellitus and elevated blood lipids, all of which are associated with congenital endocrine disorders seen in low birth weight infants. Therefore, such a pathology as " Fetal growth retardation " (FGR or fetal malnutrition) deserves special attention.
Therefore, such a pathology as " Fetal growth retardation " (FGR or fetal malnutrition) deserves special attention.
FGR can be symmetrical, when all organs are evenly reduced, and asymmetric, when the brain and skeleton correspond to the gestational age, and the internal organs lag behind in development. The reasons for this are smoking, alcohol consumption, chromosomal abnormalities, infections, but most often - fetoplacental insufficiency and other conditions that lead to circulatory disorders: high or low blood pressure, toxicosis of the second half of pregnancy, diabetes mellitus with vascular damage, kidney disease, etc. nine0003
The development of fetal malnutrition is influenced by the age of the mother . The fact is that the body of very young mothers (16-18 years old) is simply not yet ready for the upcoming stresses, while older mothers (32-40 years old) most often already have a “baggage” of chronic diseases. Smoking, addiction to alcohol and any drugs clearly contribute to the development of malnutrition, as they cause pronounced vasoconstriction and reduce uteroplacental blood flow. Alas, quite often hypotrophy is observed during multiple pregnancies, since two or even three twins have to share, literally brotherly, the nutrients received from the mother. nine0003
Alas, quite often hypotrophy is observed during multiple pregnancies, since two or even three twins have to share, literally brotherly, the nutrients received from the mother. nine0003
One of the simplest methods of monitoring fetal development is to measure the size of the uterus. As soon as it can be easily felt above the womb - approximately at the fourth month of pregnancy, at each visit, the doctor will measure the height of the fundus of the uterus, and in the second half of pregnancy, the circumference of the abdomen at the level of the navel. This will allow the doctor to roughly judge the size of the fetus. Obviously, these indicators are not objective enough, because their value is influenced by the thickness of the anterior abdominal wall, the amount of amniotic fluid, and the physique of the woman. nine0003
The most accurate diagnostic method is the ultrasound biometry used in our Clinic , which measures and evaluates several fetal parameters. The most traditional is the measurement of the head, tummy and femur, but if the doctor has doubts, he will also take additional measurements. The first signs of IGR can be detected in such a study as early as 24-26 weeks, and its symmetrical form is more often noted. The occurrence of malnutrition after 32 weeks is more typical for the asymmetric form, and fetal hypoxia usually also joins it. Identified fetal growth retardation should be treated. The goal of treatment in this case is not to “fatten the baby”, but to normalize metabolic processes and support the vital functions of the fetus. Of course, the success of treatment largely depends on how timely it is started. A large arsenal of medicines is used to treat malnutrition. It should be individual, taking into account the cause that caused IGR in this particular case and aimed at treating both the woman's diseases and pregnancy complications. For expectant mothers who are carrying a small child, it is very important to have a good diet rich in vitamins and animal proteins, as well as a regimen with limited physical activity. Depending on the severity of the condition of the fetus, the treatment is carried out on an outpatient basis, for example, in our day hospital, or in the maternity hospital. Although, as you know, houses and walls help, but in severe cases it is better not to refuse hospitalization. In the hospital, it is easier to monitor the condition of the mother and baby, and therefore provide more effective assistance. The effect of therapeutic measures must be constantly monitored using ultrasound and CTG, which are usually prescribed at intervals of 2 weeks, and if necessary, more often. FGR treatment almost always produces good results. In most cases, it is possible to observe adequate fetal growth: for example, in 7-10 days, the size of the fetus increases accordingly, and does not lag even further, which is considered a completely satisfactory result. The method and timing of delivery largely depend on the condition of the fetus. If the treatment of FGR is successful and the baby is growing, then it makes no sense to rush things, because by the end of pregnancy it can reach quite a decent size. If, despite all efforts, the child does not gain weight or has any other problems, then they resort to early delivery. At a gestational age close to full-term and ready-made birth canal, natural labor is usually stimulated. At the same time, childbirth is carried out under close medical supervision. However, if the baby is so weak that ordinary childbirth will be too big a test for him, then they resort to a caesarean section. Women who are diagnosed with fetal hypotrophy need to choose a maternity hospital, on the basis of which a modern nursing service for small children is organized, because it is important for such a child to provide qualified assistance from the first minutes of life. nine0003 But the best way to prevent this problem is prevention. The birth of a small child is not uncommon today. Often, such babies are born on time or a little earlier, but due to a lack of weight, they can significantly lag behind their peers in development. Pediatricians and neuropathologists closely monitor the child's condition, because a child's body weight deficiency is a risk factor for changes in the neurological status, functional disorders of the cardiovascular and autonomic nervous systems. But because of their weakness, underweight children do not eat well, and the rate of weight gain in children born with low body weight determines their further physical and psychomotor development and the formation of the immune system. To assess the development of your child and the compliance with the norm of the main indicators (height, weight), you can contact a pediatrician or independently - according to existing tables. In the first months, the child is actively growing, adding up to 25-60 grams per day. Small children with adequate nutrition can increase body weight more intensively than their peers. For the first month of life, children should gain up to 1.3-1.7 kg. After 5-6 months of life, the intensity of weight gain decreases somewhat - in 30 days, the increase can be only 400-700 grams. nine0003 The length of the child's body during the first month increases by 4-7 cm, and after 5-6 months of life, growth is added less intensively - by 2-3 cm. But parents should understand that these figures are approximate. Each child is individual. Its weight and height depend on many factors: heredity, the quality of the mother's nutrition, the state of health of the newborn, the severity of childbirth. The main cause of underweight in the neonatal period is the baby's refusal to breastfeed. Small children have poor appetite and spend most of the day sleeping. Often, parents have to wake up the child for a long time, and after a few minutes of sucking on the breast or a bottle of formula, the newborn falls asleep again. Children are especially sleepy, in whom pronounced physiological jaundice was observed in the first days of life. nine0003 As a result, after the next weighing, the doctor can tell the mother that the newborn has not gained weight at all or the increase is insignificant. If the situation does not improve for several months, the mother and baby may be hospitalized for a comprehensive examination and tube feeding in a hospital setting. Sometimes the cause of low weight gain lies in non-compliance with breastfeeding tactics. Pediatricians recommend applying the baby to only one breast during feeding so that it sucks out the "hind" milk, which is of particular energy value and rich in nutrients. If the baby has had an infectious disease, has been ill for a long time, suffered from a high temperature or an intestinal disorder, then the monthly weight gain may be significantly less than usual. In this case, the timing of the introduction of complementary foods is also shifted, and during the period of illness, in general, many children practically refuse to eat, which is reflected in their weight. Parents should actively communicate with the pediatrician, if necessary, ask him questions of interest and adhere to all recommendations. If you are breastfeeding, pay special attention to your diet. Drink as much liquid as possible: low-fat milk, compotes, hypoallergenic juices. But sometimes women's milk is produced in insufficient quantities or the baby does not have enough strength to suck it out. In this case, it is necessary to start supplementing with special infant formula as soon as possible. For children prone to allergic reactions, special hypoallergenic products are intended, which can be bought at a pharmacy, having previously discussed the mixture option with a pediatric nutritionist or pediatrician. Small babies are not adapted to intensive sucking, so the nipple on the bottle must be soft and pliable so that the child can fill up without problems. nine0003 In addition, in order to increase the rate of weight gain and, accordingly, for the proper growth and development of the child, it is recommended to give courses of preparations containing L-carnitine (levorcarnitine), an essential vitamin-like substance that has anabolic properties and has proven itself to normalize body weight in case of its deficiency. In children, in contrast to the adult body, where levocarnitine is among the substances produced, the synthesis of this compound covers only 1% of the required amount. Of course, the required amount of L-carnitine is found in breast milk, but if natural feeding is impaired or impossible, the drug must be added to the diet. In underweight children, psychomotor development is often retarded, which can subsequently manifest itself in the form of speech defects, instability of the nervous system. Elcar improves the energy supply of brain activity, which will help to avoid or reduce the degree of development of functional failure in various areas of the child's neuropsychic response (motor, emotional-motivational, vegetative, cognitive spheres). The accuracy of the diagnosis is ensured by the high qualification of the doctor conducting the study, the excellent resolution of our Sonix OP ultrasound scanner and the possibility of conducting a Doppler study. Ultrasound also controls the amount of amniotic fluid, reveals signs of placental dysfunction, as well as changes in blood flow in it, which helps the doctor to accurately make a preliminary diagnosis and begin treatment. To clarify the diagnosis, we carry out Doppler study of the vessels of the placenta, umbilical cord and large vessels of the fetus, as well as cardiotocography (CTG), , which allows you to register the fetal heartbeat and the nature of changes in the frequency of its heartbeats in response to movements or uterine contractions. It is important that normal Doppler and CTG data - even in the presence of low weight, indicate the well-being of the baby. If the examination did not reveal any deviations, then it becomes clear that we are talking about a healthy, low-weight fetus.
The accuracy of the diagnosis is ensured by the high qualification of the doctor conducting the study, the excellent resolution of our Sonix OP ultrasound scanner and the possibility of conducting a Doppler study. Ultrasound also controls the amount of amniotic fluid, reveals signs of placental dysfunction, as well as changes in blood flow in it, which helps the doctor to accurately make a preliminary diagnosis and begin treatment. To clarify the diagnosis, we carry out Doppler study of the vessels of the placenta, umbilical cord and large vessels of the fetus, as well as cardiotocography (CTG), , which allows you to register the fetal heartbeat and the nature of changes in the frequency of its heartbeats in response to movements or uterine contractions. It is important that normal Doppler and CTG data - even in the presence of low weight, indicate the well-being of the baby. If the examination did not reveal any deviations, then it becomes clear that we are talking about a healthy, low-weight fetus. In this case, we simply observe the woman without any therapy. nine0003
In this case, we simply observe the woman without any therapy. nine0003  Although you should not overeat, remembering that excesses in the diet do not at all lead to a proportional increase in the amount of nutrients taken by the placenta for the fetus. nine0003
Although you should not overeat, remembering that excesses in the diet do not at all lead to a proportional increase in the amount of nutrients taken by the placenta for the fetus. nine0003  nine0003
nine0003  When planning a pregnancy, it is necessary to undergo a thorough examination by specialists, sanitize foci of chronic infection, and say goodbye to bad habits. Sometimes for pregnant women at high risk for FGR, we recommend courses of drug prophylaxis for up to 12 weeks, at 20-23 and 30-32 weeks, which include vasodilators and vitamins.
When planning a pregnancy, it is necessary to undergo a thorough examination by specialists, sanitize foci of chronic infection, and say goodbye to bad habits. Sometimes for pregnant women at high risk for FGR, we recommend courses of drug prophylaxis for up to 12 weeks, at 20-23 and 30-32 weeks, which include vasodilators and vitamins. how to help them develop?
 nine0003
nine0003 How much should a newborn gain in weight?
Why is the child not gaining weight well?
 Due to their inexperience, mothers offer both breasts to newborns. In this case, the child sucks the upper milk without making any effort and quickly falls asleep, slightly satisfying his hunger. nine0003
Due to their inexperience, mothers offer both breasts to newborns. In this case, the child sucks the upper milk without making any effort and quickly falls asleep, slightly satisfying his hunger. nine0003 How to help a child gain weight and catch up with their peers in their development?
 Your diet must include boiled or baked meat. Take extra vitamins (as advised by the doctor). Breastfeed your baby immediately after waking up, when he is active, in a good mood and does not want to sleep. nine0003
Your diet must include boiled or baked meat. Take extra vitamins (as advised by the doctor). Breastfeed your baby immediately after waking up, when he is active, in a good mood and does not want to sleep. nine0003  In addition, by increasing the secretory and enzymatic activity of gastric and intestinal juices, appetite and digestion improve. One of these drugs is Elkar, containing an aqueous solution of L-carnitine. Elkar is included in the "National program for optimizing the feeding of children in the first year of life" as a means of correcting malnutrition of the II degree. nine0003
In addition, by increasing the secretory and enzymatic activity of gastric and intestinal juices, appetite and digestion improve. One of these drugs is Elkar, containing an aqueous solution of L-carnitine. Elkar is included in the "National program for optimizing the feeding of children in the first year of life" as a means of correcting malnutrition of the II degree. nine0003