Recurrent yeast infections in pregnancy
Yeast Infections and Pregnancy: Causes, Symptoms & More
What’s a yeast infection?
Vulvovaginal candidiasis, or moniliasis, is a yeast infection of the vulva and vagina. Yeast is a type of fungus. The yeast that most often causes these infections is Candida albicans, but other types of yeast — including Candida glabrata and Candida tropicalis — can also be responsible.
About three out of every four women will have at least one yeast infection in their lifetime, according to American Family Physician. Up to 45 percent will get two or more infections.
During pregnancy, Candida (and the infections it causes) is even more common. According to one study, about 20 percent of women have Candida yeast in their vagina normally. That number goes up to 30 percent during pregnancy. Yeast is more likely to cause infection during pregnancy due to hormone fluctuations.
Because you can pass the yeast to your baby during delivery, it’s important to get treated.
What causes candidiasis?
Candidiasis occurs when the normal number of fungi that reside in the vagina increases enough to cause symptoms. The most common factors that make a woman more likely to get yeast infections include:
- pregnancy
- diabetes
- use of birth control pills, antibiotics, or corticosteroids such as prednisone (Rayos)
- disorders that weaken the immune system, such as HIV
During pregnancy, shifting hormone levels change the pH balance in the vagina. This creates an environment that’s more favorable for yeast to grow.
What complications are associated with yeast infections?
In nonpregnant women who have a normal immune system, yeast infections rarely lead to serious complications.
Even in pregnancy, yeast infections don’t usually cause harmful effects in the mother. However, you can pass the yeast to your baby during delivery.
Most babies who develop a yeast infection have it just in their mouths or diaper area. However, though rare, a yeast infection in babies can become very serious, because their immune systems aren’t yet well-developed. It can spread through the infant’s body and affect breathing and heart rhythm, for example. This happens most often in babies who have other things affecting their immune systems, such as prematurity or an underlying infection.
However, though rare, a yeast infection in babies can become very serious, because their immune systems aren’t yet well-developed. It can spread through the infant’s body and affect breathing and heart rhythm, for example. This happens most often in babies who have other things affecting their immune systems, such as prematurity or an underlying infection.
Yeast infections can also cause body-wide infections and serious complications in women who have a weakened immune system because of conditions such as HIV.
What are the signs and symptoms of candidiasis?
With candidiasis, you’ll most likely have itching in your vagina and vulva. You may also notice a white vaginal discharge. This discharge may look similar to cottage cheese and shouldn’t have an odor.
Other symptoms include:
- soreness or pain in the vagina or vulva
- burning when you urinate
- a rash on the vulva and the skin around it, which sometimes appears on the groin and thighs as well
These symptoms may last for a few hours, days, or weeks.
In newborn babies and in women who have a weakened immune system, candidiasis may occur in the mouth. This condition is known as thrush.
Other conditions can cause symptoms similar to a yeast infection, including:
- an allergic reaction to a product you’ve used in the vaginal area, such as soap or a condom
- sexually transmitted diseases (STDs) such as chlamydia and gonorrhea
- bacterial vaginosis, a type of infection
How can I prevent a yeast infection?
You can reduce your risk of future yeast infections by:
- keeping the vaginal area dry
- avoiding bubble baths, feminine hygiene sprays, and douches
- wearing cotton underwear
Although candidiasis isn’t an STD, oral sex may make your condition worse and affect your sexual partner.
How is candidiasis diagnosed?
Your doctor will ask about your symptoms and do a physical exam. To confirm the diagnosis, your doctor will use a cotton swab to take a sample of the vaginal discharge. The sample will be checked under a microscope for signs of the yeasts that cause infections.
The sample will be checked under a microscope for signs of the yeasts that cause infections.
In certain cases, your doctor may want to culture — or grow in a lab — a sample of your vaginal discharge. Cultures help them rule out other types of yeast, such as C. glabrata and C. tropicalis.
How is candidiasis treated?
Most of the time, vulvovaginal candidiasis is easy to treat with an antifungal cream or suppository. The medicine should relieve your symptoms within seven days. However, during pregnancy, you should see your doctor before starting treatment. They can confirm that you actually have a yeast infection and ensure you get a treatment that’s safe to use during pregnancy.
Both oral and topical antifungal drugs are used to treat yeast infections in nonpregnant women. However, oral drugs may not be safe to use during pregnancy. A 2016 study in JAMA found an association between higher risk of miscarriage and oral fluconazole (Diflucan) use during pregnancy. Oral antifungal drugs have also been linked to birth defects.
Oral antifungal drugs have also been linked to birth defects.
Topical antifungal drugs that are safe to use during pregnancy include:
How should repeat yeast infections be treated?
During pregnancy, you’re more likely to have repeated yeast infections. Four or more yeast infections in one year is called recurrent vulvovaginal candidiasis.
If you keep getting yeast infections, talk to your doctor. You may need to be evaluated for risk factors such as diabetes or an immune disorder. If pregnancy is the cause, the infections should stop after you deliver.
Research finds that taking an oral “azole” drug for six months reduces your chance of a repeat infection. However, oral antifungal medicines might not be safe to use during your pregnancy. You may have to wait until after you deliver to go on this treatment.
Yeast Infections During Pregnancy - American Pregnancy Association
Yeast infections during pregnancy are more common than any other time in a woman’s life, especially during the second trimester of pregnancy. You may be noticing an increase in the amount of thin, white, odd smelling discharge. This is common and a normal symptom in the second trimester.
You may be noticing an increase in the amount of thin, white, odd smelling discharge. This is common and a normal symptom in the second trimester.
If you think you may be experiencing a yeast infection, the following information will prepare you to discuss the possibility with your doctor. Though yeast infections have no major negative effect on pregnancy, they are often more difficult to control during pregnancy, causing significant discomfort for you. Don’t wait to seek treatment!
What is a yeast infection?
Yeast infection occurs when the normal levels of acid and yeast in the vagina are out of balance, which allows the yeast to overgrow causing an uncomfortable, but not serious, a condition called a yeast infection.
If you have never been diagnosed or treated by a physician for a yeast infection and have some of the symptoms, you should see your physician first for accurate diagnosis and treatment. Other infections have similar symptoms, so you want to make sure that you are treating the infection correctly. There are also treatments that are not appropriate during pregnancy.
There are also treatments that are not appropriate during pregnancy.
What causes yeast infections during pregnancy?
A yeast infection can be caused by one or more of the following:
- Hormonal changes that come with pregnancy or before your period
- Taking hormones or birth control pills
- Taking antibiotics or steroids
- High blood sugar, as in diabetes
- Vaginal intercourse
- Douching
- Blood or semen
Why are yeast infections more common during pregnancy?
Your body is going through so many changes right now, and it is difficult for your body to keep up with the chemical changes in the vagina. There is more sugar in vaginal secretions on which the yeast can feed, causing an imbalance which results in too much yeast.
What are the symptoms of yeast infections?
The symptoms of a yeast infection may include one or more of the following:
- Discharge that is usually white/tan in color, similar to cottage cheese and may smell like yeast/bread
- Other discharge may be greenish or yellowish, also similar to cottage cheese and may smell like yeast/bread
- An increase in discharge
- Redness, itching, or irritation of the lips of the vagina
- Burning sensation during urination or intercourse
What else could I be experiencing?
If you are experiencing symptoms similar to a yeast infection, but a physician has ruled this diagnosis out, you may have one of the following:
- Sexually Transmitted Diseases (STDs) like Chlamydia, Gonorrhea, & Trichomoniasis
- A vaginal infection called bacterial vaginosis
How do I know for sure if I have a yeast infection?
At your doctor’s office or medical clinic, a clinician will use a simple, painless swab to remove the discharge or vaginal secretions and examine it through a microscope. Usually, upon a simple examination of the vagina, a physician can diagnose a yeast infection. In rare cases, the culture may be sent to a lab.
Usually, upon a simple examination of the vagina, a physician can diagnose a yeast infection. In rare cases, the culture may be sent to a lab.
How are yeast infections treated during pregnancy?
During pregnancy, physicians recommend vaginal creams and suppositories only. The oral medication, Diflucan (a single-dose medication), has not been proven safe during pregnancy and lactation. Not all vaginal creams and suppositories are okay to use during pregnancy, so it is best to consult your doctor or pharmacist to get the right one. If left untreated, yeast infections can pass to your baby’s mouth during delivery. This is called “thrush” and is effectively treated with Nystatin.
It may take 10-14 days to find relief or completely clear up the infection while you are pregnant. After the infection has cleared up and any sores have healed, it may be helpful to use a starch-free drying powder, or Nystatin powder to prevent a recurring infection.
How can I prevent a yeast infection or recurring yeast infections?
Most yeast infections can usually be avoided by doing the following:
- Wear loose, breathable cotton clothing and cotton underwear.

- After regular, thorough washing (using unscented, hypoallergenic or gentle soap), use your blow dryer on a low, cool setting to help dry the outside of your genital area.
- Always wipe from front to back after using the restroom.
- Shower immediately after you swim. Change out of your swimsuit, workout clothes, or other damp clothes as soon as possible.
- Do NOT:
- douche
- use feminine hygiene sprays
- use sanitary pads and tampons that contain deodorant
- take a bubble bath/use scented soaps
- use colored or perfumed toilet paper
- Include yogurt with “lactobacillus acidophilus” in your diet.
- Limit sugar intake, as sugar promotes the growth of yeast.
- Get plenty of rest to make it easier for your body to fight infections.
When should I contact my doctor?
If you are experiencing the symptoms described in this article, call your doctor now. Yeast infections have similar symptoms of other infections, such as STDs. Proper diagnosis every time you experience these symptoms is vital for the most effective, immediate treatment, or your condition may worsen/not go away.
Proper diagnosis every time you experience these symptoms is vital for the most effective, immediate treatment, or your condition may worsen/not go away.
If you see no improvement within three days, or if symptoms worsen or come back after treatment, you should contact your healthcare provider again.
Want to Know More?
- Pregnancy Nutrition
- Medication and Pregnancy
Compiled using information from the following sources:
1. American Academy of Family Physicians
https://familydoctor.org
1. Mayo Clinic Complete Book of Pregnancy & Babys First Year. Johnson, Robert V., M.D., et al, Ch. 11.
Influence of candidiasis of pregnant women on morbidity in children of the first year of life
Authors: O.M. Kantin, N.I. Syuch, I.M. Korsunskaya, Moscow Regional Perinatal Center, Center for Theoretical Problems of Physicochemical Pharmacology RAS
03/27/2015
Currently, there is an increase in infectious and inflammatory diseases caused by opportunistic Candida fungi (in particular, Candida albicans in the vast majority of cases).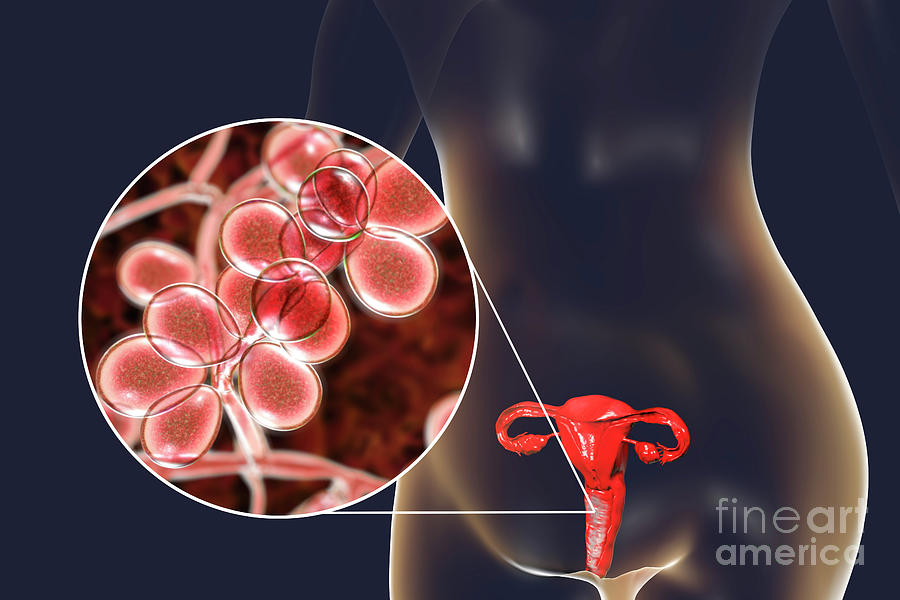
According to various authors, vulvovaginal candidiasis is 3-4 times more common in pregnant women due to changes in the immunological and hormonal status, increased susceptibility to various infectious influences.
The relevance of the problem of vaginal candidiasis in obstetrics is due to the high incidence of pregnancy complications (miscarriage, stillbirth), the risk of antenatal and intranatal infection of the fetus, as well as the development of pyoinflammatory complications in the postpartum period. The death of fetuses and newborns ranges from 17 to 36% of the total perinatal mortality. Despite the fact that fungi of the genus Candida are not causative agents of endometritis, they significantly reduce the colonization resistance of the vaginal mucosa, which contributes to the additional colonization of its opportunistic flora, which can cause an ascending infection. That is why a candidal infection during pregnancy, occurring with pronounced changes in the microbiocenosis of the vagina, is almost always mixed. Isolated candidal infection practically does not occur, and if there are clinical signs of inflammation of the vaginal mucosa, then monoinfection is in principle excluded. Perhaps as a result of all the cumulative causes, this infection in pregnant women, as a rule, is recurrent, poorly amenable to conventional methods of treatment and presents great difficulties for obstetricians and gynecologists, and poses a serious threat to the health of the mother, fetus and unborn child.
Isolated candidal infection practically does not occur, and if there are clinical signs of inflammation of the vaginal mucosa, then monoinfection is in principle excluded. Perhaps as a result of all the cumulative causes, this infection in pregnant women, as a rule, is recurrent, poorly amenable to conventional methods of treatment and presents great difficulties for obstetricians and gynecologists, and poses a serious threat to the health of the mother, fetus and unborn child.
The most frequent infection of the fetus occurs during childbirth when passing through the birth canal - the intranatal route (61.1%). The disease that occurred in newborns during the first 7 days after birth most often indicates a post-natal route of infection and reaches 28.9%. In cases of congenital candidiasis (the antenatal form of infection is 10%), fungi penetrate the fetus through the circulatory and lymphatic system of the placental barrier. Evidence of this is the detection of fungi in the tissues of the placenta, umbilical cord during cesarean section, as well as the presence of clinical and laboratory signs of candidiasis at the time of birth in newborns (manifestations of thrush in the mouth, a rash on the skin, in large folds, sowing scrapings from the oral mucosa, the surface of the lips , original lubrication, from the skin of large folds and external genitalia).
The neonatal period is characterized by insufficient maturity of the mechanisms of the immune system, in connection with which
infection with fungi of the genus Candida poses a significant danger in the outcome of the candidal process (the formation of chronic and granulomatous candidiasis, the occurrence of visceral forms, as well as candidal sepsis).
The facts of the development of candidal vulvovaginitis during pregnancy are also well known. The first episode of vulvovaginal candidiasis occurs in many women during pregnancy. The frequency of candidal vulvovaginitis in pregnant women reaches 40-46%. Such high rates are due to changes in hormonal balance during pregnancy. The highest degree of colonization is noted in the last trimester and in primiparas.
In pregnant women, the frequency of detection of fungi of the genus Candida is high and, according to various authors, ranges from 19.9 to 50.8%. It is known that such a high incidence of vaginal candidiasis during pregnancy is due to changes in hormonal balance. By increasing the level of both estrogens and progesterone, an increase in the adhesive properties of vaginal epitheliocytes is noted. Steroid hormones are able to influence the adhesion of fungi and indirectly, changing some indicators of immune defense. In addition, hyperestrogenemia contributes to increased proliferation of vaginal epithelial cells and an increase in the amount of glycogen in them, the breakdown of which produces glucose - an excellent nutrient medium for fungi.
By increasing the level of both estrogens and progesterone, an increase in the adhesive properties of vaginal epitheliocytes is noted. Steroid hormones are able to influence the adhesion of fungi and indirectly, changing some indicators of immune defense. In addition, hyperestrogenemia contributes to increased proliferation of vaginal epithelial cells and an increase in the amount of glycogen in them, the breakdown of which produces glucose - an excellent nutrient medium for fungi.
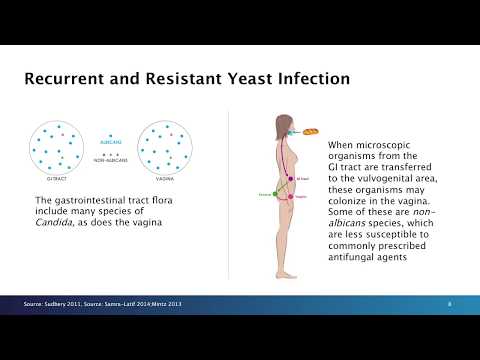
There is evidence that in recurrent vaginal candidiasis, the gastrointestinal tract serves as a reservoir of fungi and a source of reinfection of the vagina. When fungi are found in the vagina, they are very often found in feces, while in most patients the vaginal and intestinal strains are identical. In women, the sexual route of infection with fungi of the genus Candida is of secondary importance, and autoinfection from the intestines and other extragenital foci, as well as household or professional exogenous infection, comes to the fore.
Practice shows that often the contact of fungi of the genus Candida and mucous membranes forms a transient candidiasis that does not require the appointment of antifungal therapy. However, with changes in the resistance system of the macroorganism, intensive growth of fungi and stable colonization of the mucous membranes can occur. According to the results of comparative studies, treatment with local antimycotics does not help to reduce the number of relapses of the disease, since their use does not exclude the possibility of the existence of a source of reinfection in the intestine.
Increasingly, the literature discusses the issue of reducing the sensitivity of fungi of the genus Candida to antifungal drugs. The increase in the frequency of erased and atypical forms of the disease, as well as chronic, therapy-resistant cases of vulvovaginal candidiasis dictates the need to search for new, more effective drugs for the treatment of this disease.
We examined 41 women in labor and 42 newborns. The material for culture was taken from women in the first stage of labor (not later than 30 minutes after the outflow of water and the duration of the anhydrous period was not more than 4 hours). In newborns, crops were made from the skin of the presenting area, while simultaneously sowing the contents of the upper respiratory tract. Repeated cultures from the upper respiratory tract were performed on the 1st and 4th days with a swab administered sublingually. Growth intensity was assessed after 24, 48 and 96 hours and the degree of seeding was determined by the number of colonies. Under microscopy, the morphological composition of the colonies was assessed, and after obtaining a pure culture, pathogens were identified. Candiselect nutrient medium was used to identify yeast-like fungi.
The material for culture was taken from women in the first stage of labor (not later than 30 minutes after the outflow of water and the duration of the anhydrous period was not more than 4 hours). In newborns, crops were made from the skin of the presenting area, while simultaneously sowing the contents of the upper respiratory tract. Repeated cultures from the upper respiratory tract were performed on the 1st and 4th days with a swab administered sublingually. Growth intensity was assessed after 24, 48 and 96 hours and the degree of seeding was determined by the number of colonies. Under microscopy, the morphological composition of the colonies was assessed, and after obtaining a pure culture, pathogens were identified. Candiselect nutrient medium was used to identify yeast-like fungi.
During the examination of the discharged urogenital tract, Candida fungi were found in 71% of women in labor in the first stage of labor. In 80% of cases, Candida albicans was identified, in 20% - Candida tropicalis. In 40% of cases, yeast-like fungi were found in one localization (vagina), in 20% - in two (urethra and vagina), in 40% - in three (simultaneously in the urethra, vagina and rectum).
In 40% of cases, yeast-like fungi were found in one localization (vagina), in 20% - in two (urethra and vagina), in 40% - in three (simultaneously in the urethra, vagina and rectum).
We also examined 42 infants (with two of the twins) born by these women. Candida fungi were found in 41% of the examined children, in all cases on the skin (41%), in the contents of the upper respiratory tract - in 16.5% of newborns, simultaneously on the skin and in the contents of the upper respiratory tract - in 16.5% of cases . All newborns were identified Candida albicans. In the case of monolocalization of Candida (vagina), no signs of candidal infection were observed in newborns.
When re-examining the contents of the upper respiratory tract on the 1st and
On the 4th day, yeast-like fungi were found in 7.65% of newborns. It is important to note that in these cases, Candida albicans were detected during the initial examination both on the skin and in the contents of the upper respiratory tract at the same time.
Taking into account the results obtained, for the prevention of infection of newborns, women (20 people) who during pregnancy (including in the third trimester) were found to have yeast-like fungi of the genus Candida in the discharge of the urogenital tract and rectum, for
2 days before delivery, Pimafucin was prescribed 100 mg 4 times a day and 1 Pimafucin suppository (100 mg) 1 time per day.
Pimafucin (natamycin) is an antifungal polyene macrolide antibiotic with a wide spectrum of action. Having a fungicidal effect, natamycin binds sterols of cell membranes, violating their integrity
and function, which leads to the death of microorganisms. Most pathogenic yeast fungi are sensitive to natamycin, especially Candida albicans. Resistance to natamycin does not occur in clinical practice. Natamycin is practically not absorbed from the gastrointestinal tract, is not subject to systemic absorption when applied to intact skin and mucous membranes.
Vaginal suppositories dissolve quickly under the influence of body temperature, forming a foamy mass, which contributes to a uniform distribution of the active substance along the birth canal. Pimafucin is approved for use in pregnant women and newborns.
Pimafucin is approved for use in pregnant women and newborns.
In the postpartum period, Candida was detected in 18 women in labor. The predominant localization of yeast-like fungi is the rectum (18 observations), somewhat less often - the vagina and cervical canal (12), and the urethra (7). Combined localization of Candida was noted (simultaneously in the rectum, vagina, cervical canal and urethra - 7 observations).
In half of the women in labor, a high degree of contamination with yeast-like fungi of the genus Candida with altered morphological properties was observed. Microscopy showed large, homogeneous yeast-like cells, poorly perceiving dyes. The growth qualities of these cells were also changed. While exhibiting high growth activity on blood agar, these cells remained completely inert to Sabouraud's medium.
In newborns born to mothers who took prophylactic treatment for candidiasis in the third trimester of pregnancy, yeast-like fungi of the genus Candida were found in three cases, mainly on the skin. Fungi of the genus Candida were not isolated from the oral mucosa in any of the observed children.
Fungi of the genus Candida were not isolated from the oral mucosa in any of the observed children.
Yeast-like cells in the upper respiratory tract were observed in the same newborns 24 hours later and on the 4th day after birth (3 cases).
In 2 newborns in the absence of signs of candidal lesions of the skin and upper respiratory tract after delivery, Candida albicans was detected on the 1st (2 observations) and 4th (1) days after birth. At the same time, morphologically altered yeast-like cells were revealed.
Compared with the children of mothers who received Pimafucin therapy 2 days before childbirth, observed during the first year of life, in the group of children whose mothers did not receive preventive treatment, the incidence of diaper dermatitis (candidiasis of smooth skin) was significantly (2 times) higher (Table .), more than 20% higher incidence of atopic dermatitis, and dysbacteriosis developed 4 times more often. It should be noted that the children in both groups were breastfed and under constant supervision of a pediatrician.
For statistically reliable conclusions, further research in a larger sample of patients is required.
The results obtained by us correspond to the data of N.M. Gerasimova and G.A. Samsygina et al. and show that the therapy of candidiasis in mothers during pregnancy and childbirth is the prevention of the development of candidiasis in children; intravaginal therapy of candidiasis is insufficient to prevent infection of newborns, while combined therapy using Pimafucin tablets for 2 days before delivery and Pimafucin intravaginal suppositories reliably protects newborns from infection.
In the absence of therapy and preventive measures, the risk of developing candidiasis in newborns increases significantly, therapeutic measures in sick children require significant material costs, and with the development of generalized forms, candidiasis can lead to the death of a child.
References are under revision.
Gynecology, Vol. 9, No. 5, 2007
- Number:
- No.
 10/1 June - Pediatrics
10/1 June - Pediatrics
04.11.2022 Infectious illnessMolnupiravir, or "Dressing bug" for outpatient ailments on COVID‑19
This autumn, the incidence of illness on COVID‑19 increased againlike in the world, so it is in Ukraine. The peculiarities of the current treatment of COVID‑19 were examined at the scientific and practical conference “The Art of Liberation: Treatment and Prevention of Infectious and Non-Infectious Ills”, which was held on April 15 of the VGO “Association for Prevention of Mediation”. Dekilka dopovіdey, presented on this visit, was assigned to the peculiarities of the daily etiotropic therapy of COVID-19, based on the data of evidence-based medicine. We invite our readers to get to know the main provisions of Professor Viktor Volodymyrovich Mavrutenkov’s “COVID‑19. Minimization of risks in the development of an aggravated disease ....
We invite our readers to get to know the main provisions of Professor Viktor Volodymyrovich Mavrutenkov’s “COVID‑19. Minimization of risks in the development of an aggravated disease ....
04.11.2022 NeurologyCiticoline for improving memory in older people
Antiquity is characterized by the development of a wide range of pathologies, traditionally viewed as a natural process, and then, not like a disease. If old age is not aggravated by neurological or psychiatric ailments, cognitive functions do not break down, but rather calm down. Zokrema, in the middle of that frail age, the memory of those warehouses that are respected by physiological ones is commemorated. Mayzhe skin is subjectively aware of the memory of the memory of old times, which manifests itself, in the middle, like an hour later, necessary for memorizing new information and guessing information, as it was guessed earlier. ...
...
03.11.2022 Neurology Post-traumatic stress disorder: symptoms, risks, algorithm of primary care
Experiences of traumatic experiences can cause the development of post-traumatic stress disorder (PTSD). Associate Professor of the Department of Neurology, Psychiatry and Narcology, Faculty of Medicine, Kharkiv National University. V. N. Karazina, PhD, Doctor of Philosophy Andriy Volodymyrovich Gaydabrus kindly waited for the opinion of the ZU correspondent on the diagnosis of PTSD as a diagnosis, the cause of the risk and potential consequences of PTSD, as well as in the text of the primary management syndrome ..
Ecofucin for the treatment of thrush during pregnancy.
Thrush is a disease of the vaginal and vulvar mucosa caused by yeast-like fungi of the genus Candida, which affects 35% of women during pregnancy 1 .
At risk for the occurrence of a recurrent form of thrush are those pregnant women who have already had episodes of thrush in their anamnesis the level of estrogens rises, in connection with which glycogen accumulates in the vaginal mucosa - a nutrient medium for yeast-like fungi of the genus Candida.
Lactobacilli are the predominant microorganisms in the vaginal microflora of a healthy woman. A normal concentration of lactobacilli provides the necessary acidity in the vagina, which inhibits the growth of fungi. Lactobacilli also participate in the formation of local immunity
In addition, during thrush, the vaginal microflora is disturbed - the number of lactobacilli decreases sharply. These changes lead to the growth and reproduction of pathogenic fungi of the genus Candida, which leads to an increase in the number of manifestations of acute and recurrent forms of thrush.
Symptoms of thrush in a pregnant woman:
- itching and burning in the vulva and/or vagina, swelling and irritation in the vulva
- vaginal discharge of a "curdled character", sometimes with an unpleasant odor
- pain during and after intercourse
- urination disorder and pain
The appearance of at least one of the symptoms is a reason for an unscheduled visit to the doctor.
Why is it important to diagnose and treat thrush in a pregnant woman in time?
Some women are asymptomatic carriers of yeast-like fungi of the genus Candida and do not experience any discomfort or manifestation of the disease throughout the entire period of pregnancy 2
A pregnant woman with thrush (including an asymptomatic carrier) is a source of infection for her unborn child. Infection from mother to child occurs in 75-80% of cases 3 . Infection of a newborn occurs when passing through the birth canal (the skin of the child comes into contact with the infected mucous membranes of the mother's birth canal). In newborns, candidiasis is manifested by lesions of the mucous membranes and skin 2 , which can lead to negative consequences. Premature babies are particularly susceptible to Candida infection 2 .
Timely and effective treatment of thrush in a pregnant woman is an important task
Treatment of thrush
Safety and efficacy are the main criteria for choosing a drug in the treatment of thrush in pregnant women
The earlier a pregnant woman is diagnosed and treated for thrush, the less the risk of negative consequences and complications for the course of pregnancy and for the health of the mother and her unborn child. In the treatment of thrush, experts recommend an integrated approach to therapy.
In the treatment of thrush, experts recommend an integrated approach to therapy.
It is important to follow the recommendations of a specialist, following the prescribed dosage and regimen.
Comprehensive treatment should be aimed at solving two problems: eliminating the cause of thrush (fungi of the genus Candida) and restoring the vaginal microflora. It is important to know that not all drugs are approved for use during pregnancy. For example, most oral (systemic) drugs and some topical drugs for treating thrush are contraindicated during pregnancy.
Ecofucin
® in the treatment of thrush in pregnancyEcofucin
® is allowed at all stages of pregnancy and lactation 4
Natamycin
- practically not absorbed into the blood and has no systemic effect
- has a fungicidal effect - causes the death of fungal cells
- resistance to it does not develop
- does not inhibit the growth of natural microflora
+
Prebiotic 5
- actively fermented by the normal microflora of the vagina, stimulating the growth of lactobacilli 6
- causes restoration of the vaginal microflora, stimulates local immunity 6
The active substance 7 of Ecofucin ® eliminates the cause of thrush, and the prebiotic 5 in the composition of Ecofucin ® helps to restore the vaginal microflora and strengthen local immunity 6 .
Efficacy and safety of the drug Ecofucin proven by clinical studies
Ecofucin promotes faster recovery of patients with thrush.
More details
For pregnant women
Moscow 40 patients
For non-pregnant women
St. Petersburg 36 patients
Clinical cure occurred significantly earlier in the group of patients who used Ecofucin.
Kuzmin V.N., Bogdanova M.N. Ecofucin® is the first drug for the eradication of Candida fungi with the effect of stimulating the growth of lactobacilli in pregnant women. breast cancer. 2020; one; 28-33
Ecofucin helps to increase the number of own lactobacilli in the vagina and reduce the risk of recurrence of thrush.
More details
For pregnant women
Moscow 40 patients
For non-pregnant women
St. Petersburg 36 patients
Clinical cure occurred significantly earlier in the group of patients who used Ecofucin.
Kuzmin V.N., Bogdanova M.N. Ecofucin® is the first drug for the eradication of Candida fungi with the effect of stimulating the growth of lactobacilli in pregnant women. breast cancer. 2020; one; 28-33
Dosage and Administration
The regimen for the use of Ecofucin ® in a pregnant woman is prescribed by the attending physician individually.
Additional conditions for effective treatment of thrush are: giving up bad habits, a carbohydrate-restricted diet, wearing underwear made from natural fabrics, etc.
It is important to consult a gynecologist in a timely manner and exclude self-medication.
1. Tikhomirov A.L., Sarsania S.I. Features of candidal vulvovaginitis in pregnant women at the present stage. // Pharmateka № 9, 2009, p. 64-70.
2. Prilepskaya V.N., Mirzabalaeva A.K., Kira E.F., Gomberg M.A., Apolikhina I.A., Bairamova G.R. Federal clinical guidelines "Urogenital candidiasis". // 2013.