Preeclampsia care plan
Preeclampsia Nursing Diagnosis & Care Plan
Preeclampsia is a serious complication that occurs during pregnancy and affects 5-7% of pregnancies worldwide. It is characterized by high blood pressure and protein in the urine (proteinuria). The exact cause is unknown though research shows genetics or blood vessel abnormalities with the placenta could be a potential cause.
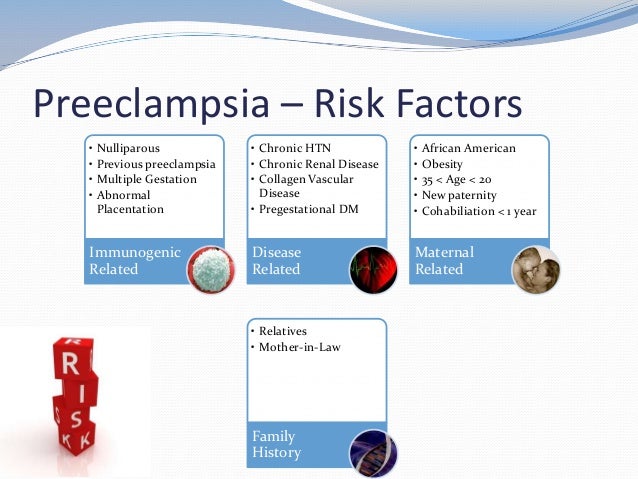
The following risk factors increase the chance of a woman developing preeclampsia:
- Multiple-gestation pregnancy
- Obesity
- Family history of preeclampsia
- Women giving birth for the first time
- Women younger than 20 years of age or older than 40 years of age
- Overproduction of amniotic fluid (polyhydramnios)
- Underlying diseases like hypertension, diabetes, renal disease, and autoimmune disorders
Hypertension, proteinuria, and edema are the classic triad symptoms of preeclampsia. Other symptoms include:
- Constant headaches
- Vision abnormalities
- Shortness of breath
- Epigastric pain
- Fluctuations in fetal heart rate
- Vaginal bleeding
Preeclampsia, if untreated, can hinder the baby’s growth and may develop into eclampsia. Eclampsia is a severe complication of preeclampsia that can lead to seizures.
The only way to treat preeclampsia is to deliver the baby. After delivery, preeclampsia usually resolves within days to weeks.
The Nursing Process
Nurses can first identify high-risk pregnancies to prevent preeclampsia. Focus on a thorough nursing assessment, education, and antenatal care.
The majority of cases are avoidable. Interventions include:
- Monitoring the patient’s blood pressure and symptoms
- Stress management
- Weight management
- Proper nutrition
- Monitoring fetal heart rate (FHR)
- Regular OB/GYN follow-ups and prenatal care
Risk for Imbalanced Fluid Volume Care Plan
Risk for imbalanced fluid volume associated with preeclampsia is caused by fluid shifts which can lead to overloading organs and tissues.
Nursing Diagnosis: Risk for Imbalanced Fluid Volume
- Plasma protein loss
- Decreased osmotic pressure
- Fluid shifting out of the vascular space
- Narrowing of the blood vessels
- Highly concentrated blood (Hemoconcentration)
- Elevated blood flow resistance
- Body cell degeneration (for pregnant mothers of older age)
- Decreased kidney filtration
- Sodium retention
As evidenced by:
A risk diagnosis is not evidenced by signs and symptoms as the problem has not yet occurred.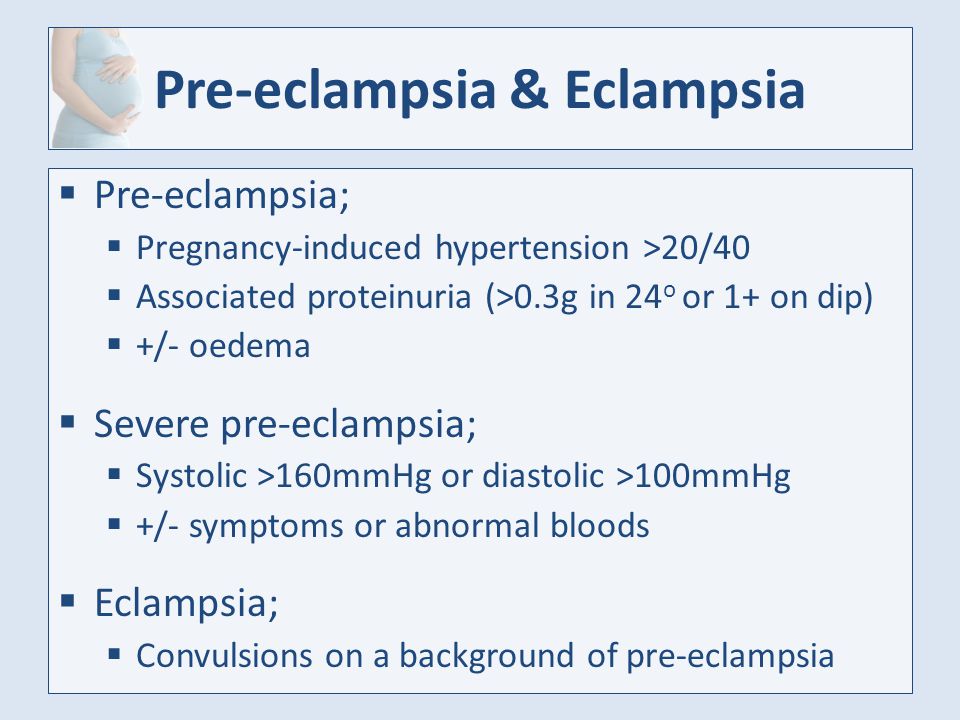 Nursing interventions are aimed at prevention.
Nursing interventions are aimed at prevention.
Expected outcomes:
- Patient will be able to maintain adequate fluid volume as evidenced by blood pressure within normal limits
- Patient will be able to demonstrate efficient fluid intake and output
- Patient will remain free from generalized or pulmonary edema
Imbalanced Fluid Volume Assessment
1. Monitor blood pressure.
High blood pressure during pregnancy causes a concern for preeclampsia. Increased blood pressure may cause the heart to have to work harder due to the additional fluid in the body.
2. Assess for edema, proteinuria, and weight gain.
Proteinuria, edema, and weight gain are symptoms of preeclampsia. Protein in the urine (proteinuria) occurs from impaired renal filtration. Weight gain is likely related to fluid retention.
Note the following symptoms:
- Proteinuria of 1+ to 2+ on a random sample
- Minor facial or upper extremity edema
- Weight gain of more than 2 pounds per week in the second trimester and less than 1 pound per week in the third trimester
3. Monitor fetal well-being and status.
Monitor fetal well-being and status.
Preeclampsia is a significant factor in fetal death. If fluid is not balanced, the fetus is at higher risk of hypoxia and growth retardation.
Imbalanced Fluid Volume Interventions
1. Manage preeclampsia.
Collaborate with the healthcare team in treating preeclampsia to manage symptoms of fluid volume imbalance and prevent further complications.
2. Administer fluids.
IV fluids are administered to expand the intravascular volume. Care must be taken to not worsen or cause pulmonary edema.
3. Instruct on diet recommendations.
Limiting sodium and taking calcium, magnesium, and potassium supplements prevent the progression of edema and hypertension in preeclampsia.
4. Monitor intake and output.
Oliguria or reduced urine output can signal decreased kidney function from poor circulatory blood volume.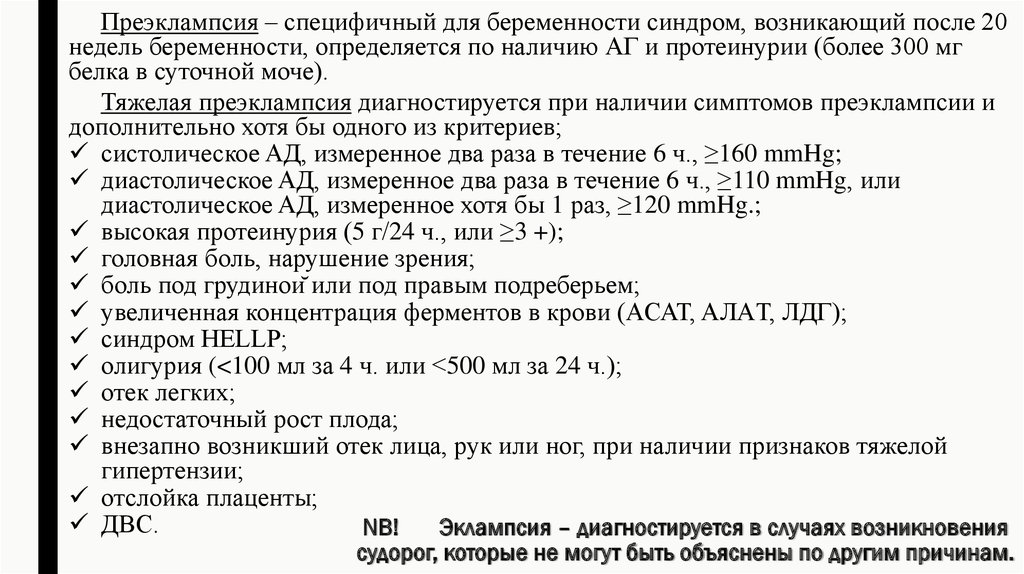
Decreased Cardiac Output Care Plan
Decreased cardiac output associated with preeclampsia can be caused by increased cardiac demands and decreased blood supply.
Nursing Diagnosis: Decreased Cardiac Output
- Hypovolemia
- Decreased venous return
- Increased systemic vascular resistance
As evidenced by:
- Alterations in blood pressure
- Alterations in hemodynamic readings
- Edema
- Dyspnea
- Alterations in mental status
Expected outcomes:
- Patient will be able to maintain adequate blood pressure within acceptable limits
Decreased Cardiac Output Assessment
1. Assess the patient’s blood pressure.
During pregnancy, hypertension is defined as blood pressure >140/90 mm Hg. Preeclampsia is diagnosed with new onset hypertension with proteinuria after 20 weeks of pregnancy.
2. Assess for indications of poor cardiac function and impending heart failure.
The nurse can assess for the following symptoms:
- Excessive fatigue
- Intolerance to exertion
- Sudden or rapid weight gain
- Edema in the extremities
- Progressive or worsening shortness of breath
4. Assess the patient’s platelet count.
In preeclamptic women, a low platelet count is linked to a higher risk of abnormal coagulation and decreased cardiac output.
5. Assess for fetal growth.
Preeclampsia reduces cardiac output and can affect the arteries that provide blood to the placenta. The fetus may not get enough oxygen or nutrients which may result in fetal growth restriction.
Decreased Cardiac Output Interventions
1. Position the patient comfortably on the left side-lying position.
Left side-lying promotes adequate circulation. This position makes it easier for nutrient-rich blood to flow from the heart to the placenta to support the fetus.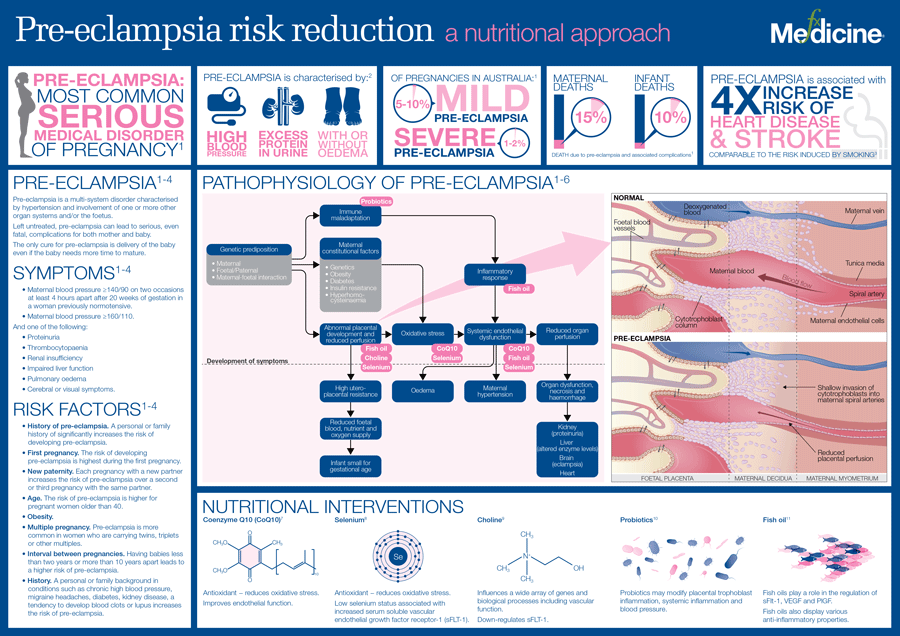
2. Administer oxygen as prescribed.
Increase the amount of oxygen available for heart function which will increase the blood supply to the placenta and fetus.
3. Administer antihypertensives.
Cardiac medications should be administered to reduce hypertension with precautions that are safe for the mother and the fetus.
4. Restrict fluids as ordered.
If there is the presence of edema and cardiopulmonary congestion, restrict fluid intake as ordered.
6. Encourage reduced activity.
Rest periods and reduced activity is recommended. Physical activity diverts blood away from the placenta. Complete bed rest is not necessary.
7. Prepare for cesarean section.
If complications of preeclampsia due to decreased cardiac output are present, an emergency cesarean section is performed. This is to prevent maternal and fetal death.
Deficient Knowledge Care Plan
Deficient knowledge associated with preeclampsia can result in delayed recognition and treatment and poorer outcomes.
Nursing Diagnosis: Deficient Knowledge
- Pathophysiology of preeclampsia
- Management of preeclampsia
- Risk factors for preeclampsia
- Self-care and nutritional needs of preeclampsia
- Complications of preeclampsia
- Lack of exposure to preeclampsia
- Inaccurate information about preeclampsia
- Misconceptions about preeclampsia
As evidenced by:
- Rapid progress of preeclampsia
- Development of preventable complications
- Unawareness of symptoms
- Inquiries about preeclampsia
- Misconceptions about preeclampsia
- Inaccurate or insufficient instructions in the prevention or management of preeclampsia
Expected outcomes:
- Patient will be able to verbalize understanding of preeclampsia and its management
- Patient will be able to verbalize possible complications and when to contact a healthcare provider
- Patient will be able to demonstrate behavior and lifestyle modifications in the prevention of preeclampsia
Deficient knowledge Assessment
1. Determine the patient’s knowledge level of preeclampsia.
Determine the patient’s knowledge level of preeclampsia.
Assessing the patient’s current knowledge and understanding of preeclampsia will help the nurse determine appropriate resources to guide learning.
2. Determine misconceptions about preeclampsia.
Preeclampsia can be misinterpreted by the patient due to past information or influences by family, friends, and cultures. Ask the patient directly about their understanding and clarify any questions as needed.
4. Assess readiness to learn.
Pregnancy can be an exciting and frightening journey, especially for first-time moms. Establish an uninterrupted time to provide information on preeclampsia that is not overwhelmed by other instructions.
Deficient knowledge Interventions
1. Instruct on symptoms to report.
Provide verbal and written instructions on symptoms to report to the healthcare provider such as blurred vision, headaches, epigastric pain, or difficulty breathing.
2. Involve the support system.
A mother requires support from her partner and family members. Information can be provided to support persons to monitor the patient and encourage healthy habits.
3. Encourage using positive reinforcement.
Positive reinforcement can be used to encourage behavior modification and teach new skills. It promotes motivation for further attempts at learning.
4. Instruct on appointments and tests.
Completing follow-up appointments, glucose monitoring, and blood pressure assessments will ensure a healthy pregnancy and delivery.
References and Sources
- Doenges, M. E., Moorhouse, M. F., & Murr, A. C. (2019). Nurse’s pocket guide: Diagnoses, interventions, and rationales (15th ed.). F A Davis Company.
- Moura, S. B., Lopes, L. M., Murthi, P., & Costa, F. D. (2012, December 17). Prevention of Preeclampsia. PubMed Central (PMC).
 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3534321/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3534321/ - Pillitteri, A., & Silbert-Flagg, J. (2015). Nursing Care of a Family Experiencing a Sudden Pregnancy Complication. In Maternal & child health nursing: Care of the childbearing & Childrearing family (8th ed., pp. 1210-1224). LWW.
- Silvestri, L. A., & CNE, A. E. (2019). Risk Conditions Related to Pregnancy. In Saunders comprehensive review for the NCLEX-RN examination (8th ed., pp. 687-688). Saunders.
Pregnancy- Induced Hypertension (PIH; preeclampsia and eclampsia) Nursing Care Plan & Management
Description
- Preeclampsia is a hypertensive disorder of pregnancy developing after 20 weeks’ gestation and characterized by edema, hypertension, and proteinuria.
- Eclampsia is an extension of preeclampsia and is characterized by the client experiencing seizures.
Etiology
- The cause of preeclampsia is unknown.
- Possible contributing factors include:
- Genetic or immunologic
- Primigravid status
- Conditions that create excess trophoblastic tissue, such as multiple gestation, diabetes, or hydatidiform mole.
- Age younger than 18 or older than 35 years.
Pathophysiology
- Preeclampsia is a multisystem, vasospatic disease process characterized by hemoconcentration, hypertension, and proteinuria.
Assessment Findings
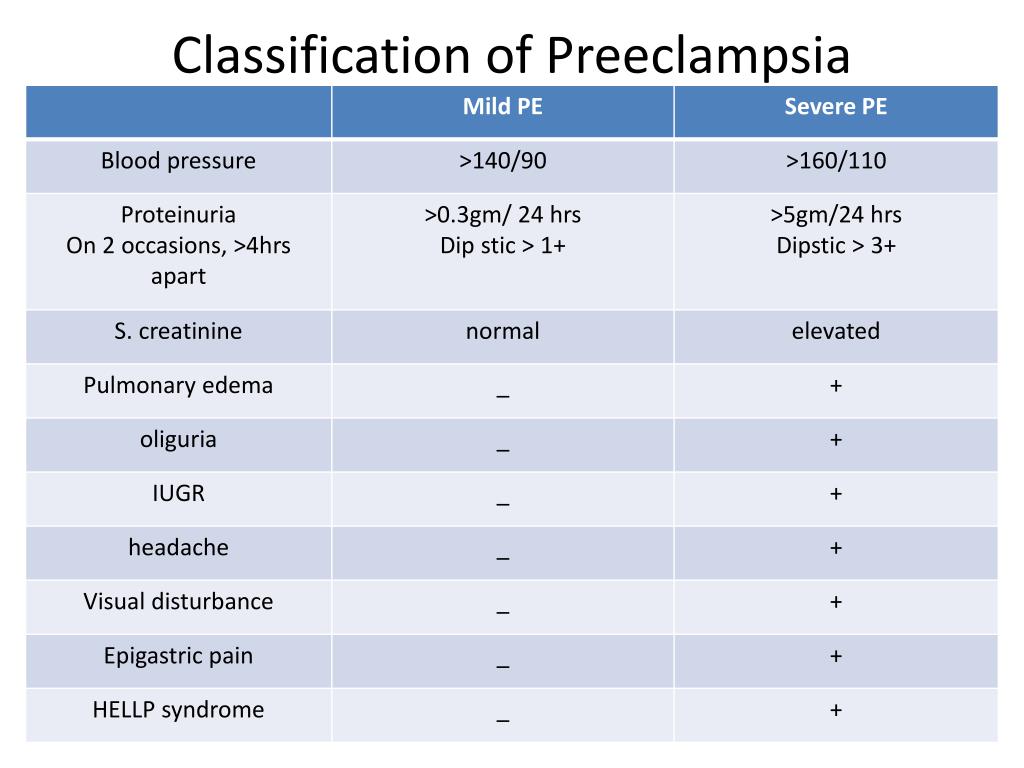
- Clinical manifestations of mild preeclampsia
- Blood pressure exceeding 140/90 mmHg; or increase above baseline of 30 mm Hg in systolic pressure or 15 mmHg in diastolic pressure on two readings taken 6 hours apart.
- Generalized edema in the face, hands, and ankles (a classic sign)
- Weight gain of about 1.5 kg (3.3 lb) per month in the second trimester or more than 1.3 to 2.3 kg (3 to 5 lb) per week in the third trimester
- Proteinuria 1+ to 2+, or 300 mg/dL, in a 24 hour sample
- Warning signs of worsening preeclampsia
- Rapid rise in blood pressure
- Rapid weight gain
- Generalized edema
- Increased proteinuria
- Epigastric pain, marked hyperreflexia, and severe headache, which usually precede convulsions in eclampsia
- Visual disturbances
- Oliguria (<120 mL in 4 hours)
- Irritability
- Severe nausea and vomiting
- Clinical manifestations of severe preeclampsia
- Blood pressure exceeding 160/110 mm Hg noted on two readings taken 6 hours apart with the client on bed rest.

- Proteinuria exceeding 5 g/24 hours
- Oliguria (less than 400 mL/24 hours)
- Headache
- Blurred vision, spots before eyes, and retinal edema
- Pitting edema of the sacrum, face, and upper extremities
- Dyspnea
- Epigastric pain
- Nausea and vomiting
- Hyperreflexia
- Blood pressure exceeding 160/110 mm Hg noted on two readings taken 6 hours apart with the client on bed rest.
- Eclampsia exists once the patient has experienced a grand mal seizure. The patient may progress o more serious complications such as cerebral hemorrhage, liver rupture, and coma.
- Laboratory and diagnostic study findings. Abdominal test results are provided in Table.
| TEST | FINDINGS |
| Blood Hematocrit | >40% |
| Renal Function Serum uric acid | >5.5 mg/dL >6.0 mg/dL (severe pregnancy-induced hypertension (PIH) |
| Creatinine | >1. 0 mg/dL 0 mg/dL2.0-3.0 mg/dL (severe PIH) |
| Creatinine clearance | <150 mL/min |
| BUN | 8-10 mg/dL 10-16 mg/dL (severe PIH) |
| Coagulation Platelets | <100,000 mL (severe PIH) >16 mg/mL (severe PIH) |
Classification Of Hypertensive Disorders Of Pregnancy
| Disorder | Symptoms | Onset |
| Gestational hypertension | Blood pressure elevated > 140/90 mm Hg | >20 weeks pregnancy |
| Preeclampsia | Blood pressure elevated >140/90 mmHg and +1 or greater proteinuria on dipstick | >20 weeks pregnancy |
| Eclampsia | Preeclampsia with neurologic symptoms/seizures | .20 weeks pregnancy |
| Chronic hypertension | Pre-existing hypertension | Exists prior to pregnancy |
| Preeclampsia/eclampsia superimposed on chronic hypertension | Blood pressure increases >30 mm Hg systolic or >15 mm Hg diastolic from baseline with onset of significant protenuria | >20 weeks pregnancy |
Nursing Management
1. Monitor for, and promote the resolution of, complications.
- Monitor vital signs and FHR.
- Minimize external stimuli; promote rest and relaxation.
- Measure and record urine output, protein level, and specific gravity.
- Assess for edema of face, arms, hands, legs, ankles, and feet. Also assess for pulmonary edema.
- Weigh the client daily.
- Assess deep tendon reflexes every 4 hours.
- Assess for placental separation, headache and visual disturbance, epigastric pain, and altered level of consciousness.
2. Provide treatment as prescribed.
- Mild preeclampsia treatment consists of bed rest in left lateral recumbent position, balanced diet with moderate to high protein and low to moderate sodium, and administration of magnesium sulfate.
- Severe preeclampsia treatment consist of complete bed rest, balanced diet with high protein and low to moderate sodium, administration of sulfate, fluid and electrolyte replacements, and sedative antihypertensives, such as diazepam or Phenobarbital, or an anticonvulsant such as phenytoin.
- Eclampsia treatment consists of administration of magnesium sulfate intravenously.
3. Institute seizure precautions. Seizures may occur up to 72 hours after delivery.
4. Address emotional and psychosocial needs.
Please wait while the activity loads. If this activity does not load, try refreshing your browser. Also, this page requires javascript. Please visit using a browser with javascript enabled.
If loading fails, click here to try again
Choose the letter of the correct answer. Good luck!
Congratulations - you have completed Pregnancy-Induced Hypertension Practice Exam (PM)*. You scored %%SCORE%% out of %%TOTAL%%. Your performance has been rated as %%RATING%%
Your answers are highlighted below.
Deficient Fluid Volume
Deficient Fluid Volume: It is defined as decreased intravascular, interstitial, and intracellular fluid.
May be related to
- Osmotic pressure
- Plasma protein loss
- Decreasing plasma colloid
- Allowing fluid shifts out of the vascular compartment
Possibly evidenced by
- Edema formation
- Sudden weight gain
- Decreased urine output
- Hemoconcentration
- Nausea/vomiting
- Epigastric pain
- Headaches
- Visual changes
Desired Outcomes
- Patient engages in therapeutic regimen and monitoring, as indicated.
- Patient verbalizes understanding of need for close monitoring of weight, BP, urine protein, and edema.
- Patient is free of signs of generalized edema (i.e., epigastric pain, cerebral symptoms, dyspnea, nausea/vomiting)
- Patient exhibits Hct WNL and physiological edema with no signs of pitting.
| Nursing Interventions | Rationale |
|---|---|
Weigh patient regularly. Tell patient to record weight at home in between visits. | Abrupt, notable weight gain (e.g., more than 3.3 lb (1.5 kg)/month in the second trimester or more than 1 lb (0.5 kg)/wk in the third trimester) reflects fluid retention. Fluid moves from the vascular to interstitial space, resulting in edema. |
| Differentiate physiological and pathological edema of pregnancy. Locate and determine degree of pitting. | The presence of pitting edema (mild, 1+ to 2+; severe, 3+ to 4+) of face, hands, legs, sacral area, or abdominal wall, or edema that does not disappear after 12hr of bedrest is vital. Note: Significant edema may actually be present in nonpre-eclamptic patient sand absent in patients with mild or moderated PIH. |
| Note signs of progressive or excessive edema i.e., epigastric/RUQ pain, cerebral symptoms, nausea, vomiting). Assess for possible eclampsia. | Edema and intravascular fibrin deposition (in HELLP syndrome) within the encapsulated liver are manifested by RUQ pain; dyspnea, indicating pulmonary involvement; cerebral edema, possibly leading to seizures; and nausea and vomiting, indicating GI edema.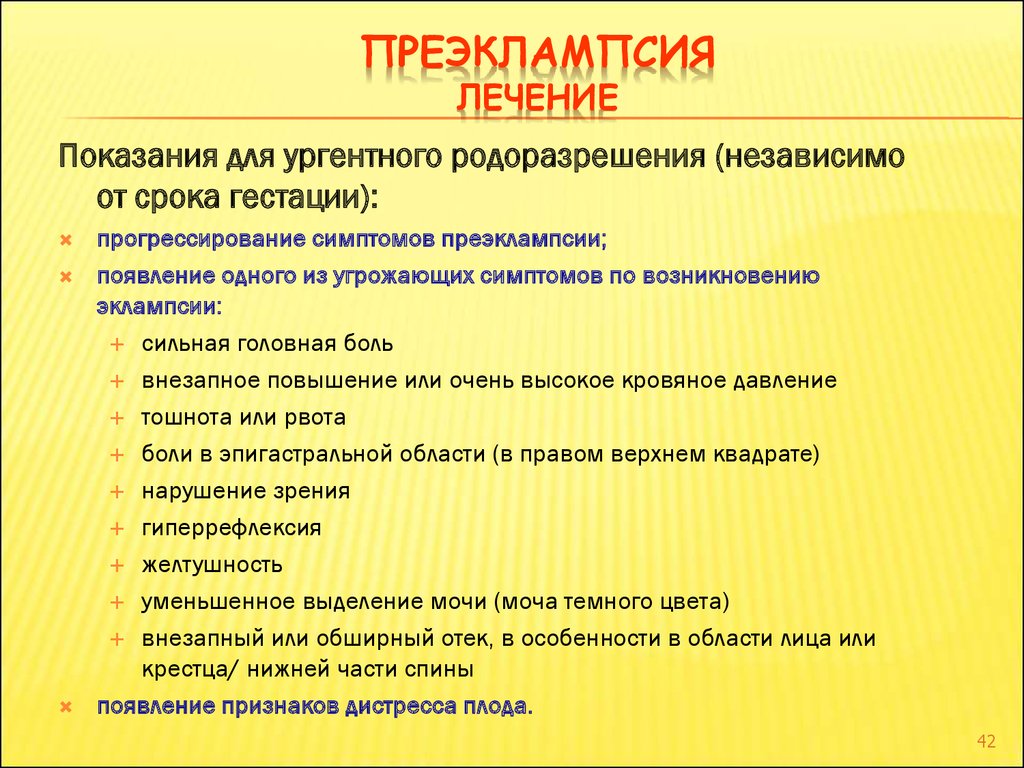 |
| Note alteration in Hct/Hb levels. | Identifies degree of hemoconcentration caused by fluid shift. If Hct is less than 3 times Hb level, hemoconcentration exists. |
| Check on dietary intake of proteins and calories. Give information as needed. | Proper nutrition decreases incidence of prenatal hypovolemia and hypoperfusion; insufficient protein/calories increases the risk of edema formation and PIH. Intake of 80–100 g of protein may be required daily to replace losses. |
| Monitor intake and output. Note urine color, and measure specific gravity as indicated. | Urine output is a sensitive indicator of circulatory blood volume. Oliguria and specific gravity of 1.040 indicate severe hypovolemia and kidney involvement. Note: Administration of magnesium sulfate (MgSO4)may cause transient increase in output. |
Examine clean, voided urine for protein each visit, or daily/hourly as appropriate if hospitalized. Report readings of 2+, or greater. | Aids in identifying degree of severity/progression of condition. A 2+ reading implies glomerular edema or spasm. Proteinuria affects fluid shifts from the vascular tree. Note: Urine contaminated by vaginal secretions may test positive for protein, or dilution may result in a false-negative result. In addition, PIH may be present without significant proteinuria. |
| Assess lung sounds and respiratory rate/effort. | Dyspnea and crackles may mean pulmonary edema, which needs immediate treatment. |
| Check BP and pulse. | Rise in BP may happen in response to catecholamines, vasopressin, prostaglandins, and, as recent findings suggest, decreased levels of prostacyclin. |
| Respond to questions and review rationale for avoiding use of diuretics to treat edema. | Diuretics further increase chances of dehydration by decreasing intravascular volume and placental perfusion, and they may cause thrombocytopenia, hyperbilirubinemia, or alteration in carbohydrate metabolism in fetus/newborn.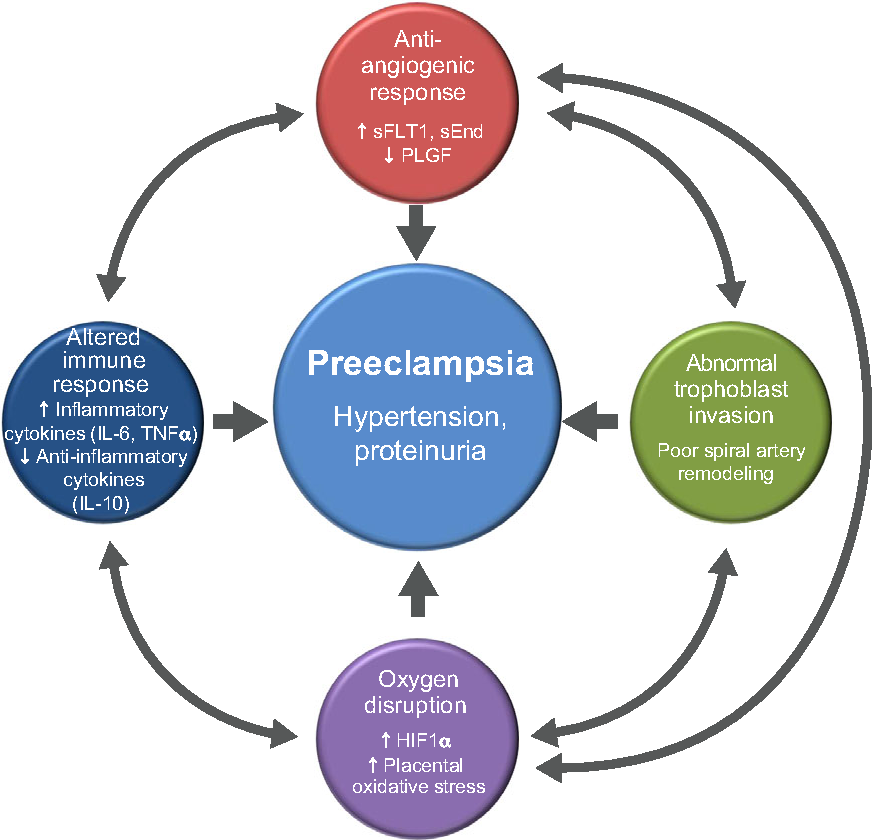 Note: May be useful in treating pulmonary edema. Note: May be useful in treating pulmonary edema. |
| Schedule prenatal visit every 1–2 wk if PIH is mild; weekly if severe. | Important to monitor changes more closely for the well-being of the patient and fetus. |
| Review moderate sodium intake of up to 6 g/day. Tell patient to read food labels and avoid foods high in sodium (e.g., bacon, luncheon meats, hot dogs, canned soups, and potato chips). | Some sodium intake is necessary because levels below 2–4 g/day result in greater dehydration in some patients. However, excess sodium may increase edema formation. |
| Collaborate with dietitian as indicated. | Nutritional consult may be beneficial in determining individual needs/dietary plan. |
| Place patient on strict regimen of bedrest; encourage lateral position. | Lateral recumbent position decreases pressure on the vena cava, increasing venous return and circulatory volume. This enhances placental and renal perfusion, reduces adrenal activity, and may lower BP as well as account for weight loss through diuresis of up to 4 lb in 24-hr period.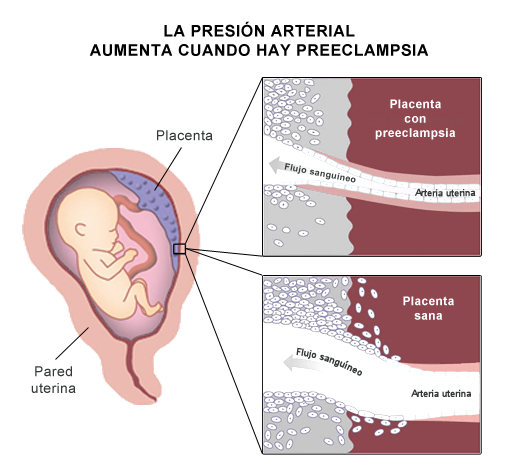 |
| Educate patient and family members or significant others on home monitoring/day-care program, as appropriate. | Some mildly hypertensive patients without proteinuria may be managed on an outpatient basis if adequate surveillance and support is provided and the patient/family actively participates in the treatment regimen. |
| Substitute fluids either orally or parenterally via infusion pump, as indicated. | Fluid replacement treats hypovolemia, yet must be given cautiously to prevent overload, especially if interstitial fluid is drawn back into circulation when activity is reduced. With renal involvement, fluid intake is restricted; i.e., if output is reduced (less than 700 ml/24 hr), total fluid intake is restricted to approximate output plus insensible loss. Use of infusion pump allows more accurate control delivery of IV fluids. |
| When fluid deficit is severe and patient is hospitalized: | |
| Allows more accurate monitoring of output/renal perfusion. |
| Gives a more precise measurement of fluid volume. In normal pregnancy, plasma volume increases by 30%–50%, yet this increase does not occur in the patient with PIH. |
| Elevated levels, especially of uric acid, indicate impaired kidney function, worsening of maternal condition, and poor fetal outcome. |
| Patients with HELLP syndrome awaiting delivery of the fetus may benefit from transfusion of platelets when count is below 20,000. |

Decreased Cardiac Output
Decreased Cardiac Output: Inadequate blood pumped by the heart to meet metabolic demands of the body.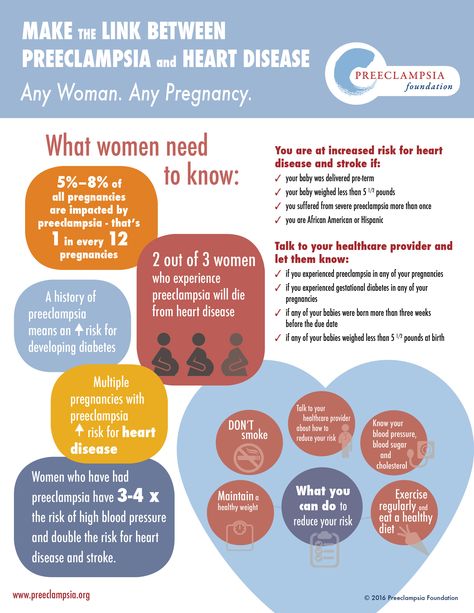
May be related to
- Hypovolemia/decreased venous return
- Increased systemic vascular resistance
Possibly evidenced by
- Change in blood pressure/hemodynamic readings
- Edema
- Shortness of breath
- Alteration in mental status
Desired Outcomes
- Patient remains normotensive throughout remainder of pregnancy.
- Patient reports absence and/or decreased episodes of dyspnea.
- Patient alters activity level as condition warrants.
| Nursing Interventions | Rationale |
|---|---|
| Record and graph vital signs especially BP and pulse. | The patient with PIH does not display the normal cardiovascular response to pregnancy (left ventricular hypertrophy, increase in plasma volume, vascular relaxation with decreased peripheral resistance). Hypertension (the second manifestation of PIH after edema) occurs owing to increased sensitization to angiotensin II, which increases BP, promotes aldosterone release to increase sodium/water reabsorption from the renal tubules, and constricts blood vessels.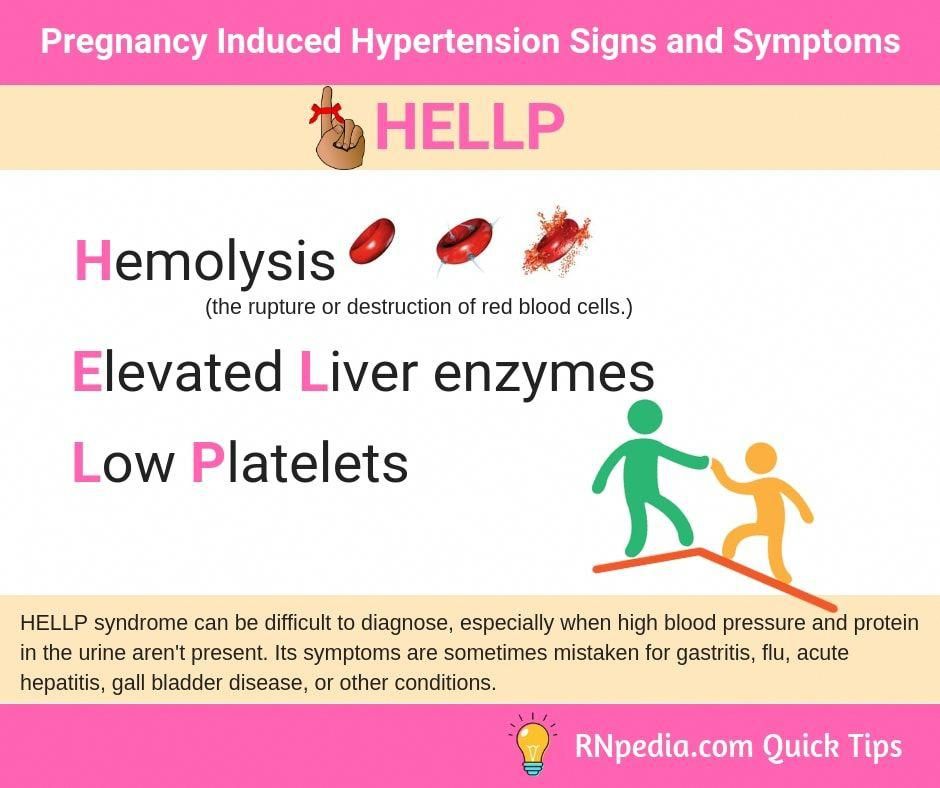 |
| Assess MAP at 22 weeks’ gestation. A pressure of 90 mm Hg is considered predictive of PIH. Assess for crackles, wheezes, and dyspnea; note respiratory rate/effort. | Pulmonary edema may transpire, with modification in peripheral vascular resistance and drop in plasma colloid osmotic pressure. |
| Institute bedrest with patient in lateral position. | Improves venous return, cardiac output, and renal/placental perfusion. |
| Check for invasive hemodynamic parameters. | Provides precise picture of vascular changes and fluid volume. Prolonged vascular constriction, increased hemoconcentration, and fluid shifts decrease cardiac output. |
| Give antihypertensive drug such as hydralazine (Apresoline) PO/IV, so that diastolic readings are between 90 and 105 mm Hg. Begin maintenance therapy as needed, e.g., methyldopa (Aldomet) or nifedipine (Procardia). | If BP does not respond to conservative measures, short-term medication may be needed in conjunction with other therapies, e.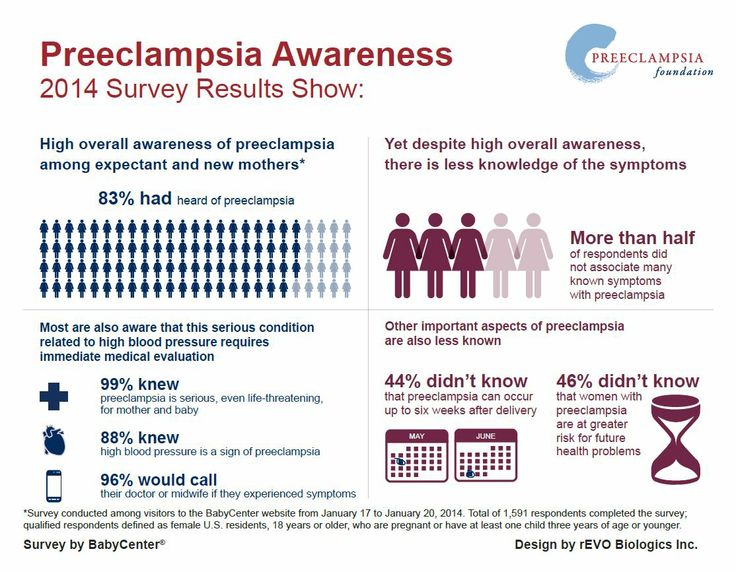 g., fluid replacement and MgSO4. Antihypertensive drugs work directly on arterioles to promote relaxation of cardiovascular smooth muscle and help increase blood supply to cerebrum, kidneys, uterus, and placenta. Hydralazine is the drug of choice because it does not produce effects on the fetus. Sodium nitroprusside is being used with some success to lower BP (especially in HELLP syndrome). g., fluid replacement and MgSO4. Antihypertensive drugs work directly on arterioles to promote relaxation of cardiovascular smooth muscle and help increase blood supply to cerebrum, kidneys, uterus, and placenta. Hydralazine is the drug of choice because it does not produce effects on the fetus. Sodium nitroprusside is being used with some success to lower BP (especially in HELLP syndrome). |
| Check on BP and side effects of antihypertensive drugs. Administer propranolol (Inderal), as appropriate. | Side effects such as tachycardia, headache, nausea, and vomiting, and palpitations may be treated with propranolol. |
| Prepare for birth of fetus by cesarean delivery, labor when severe PIH/eclamptic condition is stabilised, but vaginal delivery is not feasible. | If conservative treatment is ineffective and labor induction is ruled out, then surgical procedure is the only means of halting the hypertensive problems. |
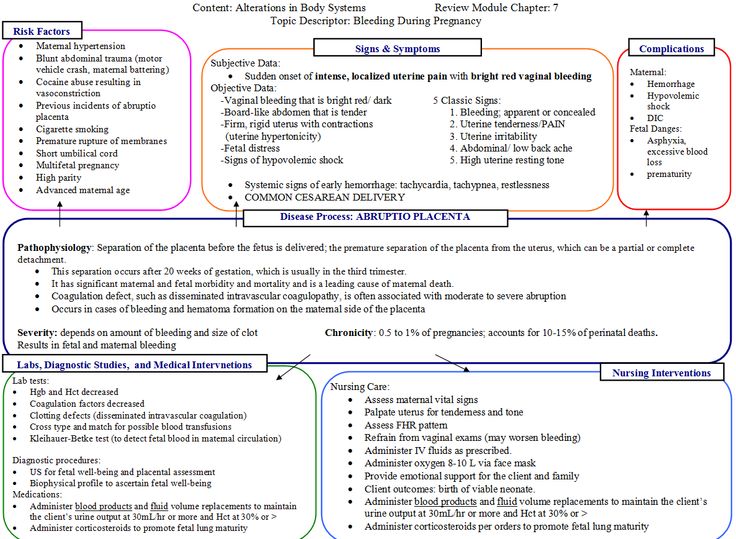
Altered Tissue Perfusion (Uteroplacental)
Impaired Tissue Perfusion: Decreased in the oxygen resulting in the failure to nourish the tissues at the capillary level.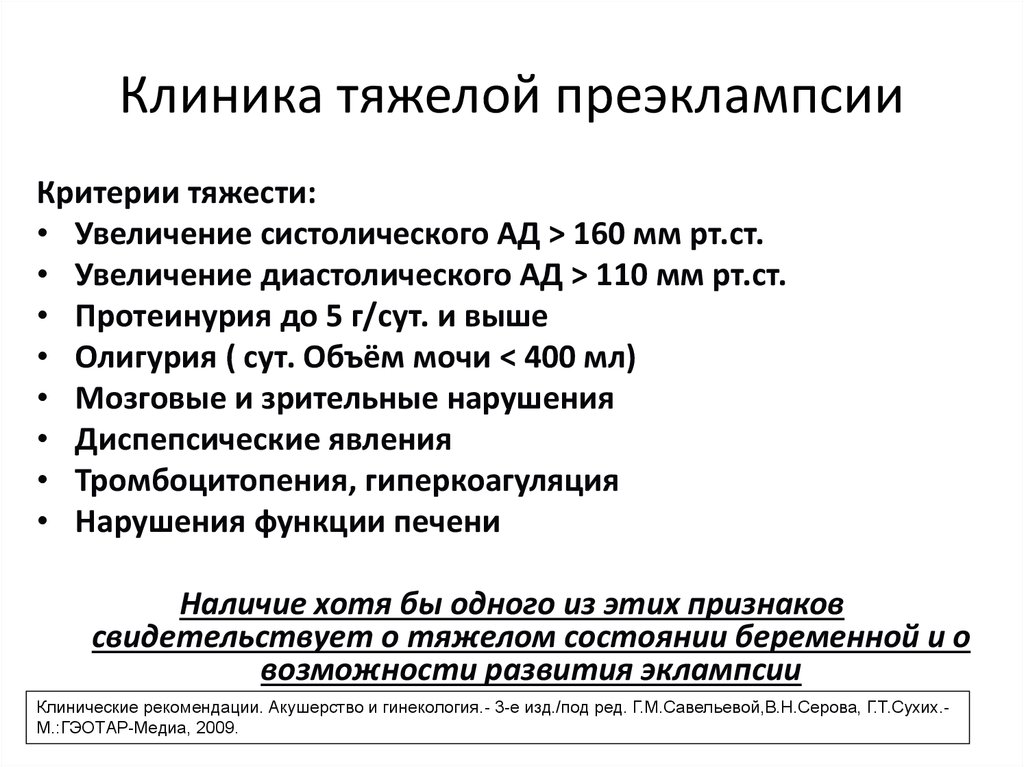
May be related to
- Maternal hypovolemia
- Interruption of blood flow (progressive vasospasm of spiral arteries)
Possibly evidenced by
- Intrauterine growth retardation
- Changes in fetal activity/heart rate
- Premature delivery
- Fetal demise
Desired Outcomes
- Patient demonstrates normal CNS reactivity on nonstress test (NST)
- Patient is free of late decelerations;
- Patient has no decrease in FHR on contraction stress test/oxytocin challenge test (CST/OCT).
- Patient is full-term, AGA.
| Nursing Interventions | Rationale |
|---|---|
| Present information to patient/couple concerning home assessment or noting daily fetal movements and when to seek immediate medical attention. | Decrease in placental blood flow results in reduced gas exchange and impaired nutritional functioning of the placenta. Potential outcomes of poor placental perfusion include a malnourished, LBW infant, and prematurity associated with early delivery, abruptio placentae, and fetal death. Reduced fetal activity means fetal compromise (occurs before detectable alteration in FHR and indicates demand for immediate evaluation/intervention. Reduced fetal activity means fetal compromise (occurs before detectable alteration in FHR and indicates demand for immediate evaluation/intervention. |
| Name factors affecting fetal activity. | Cigarette smoking, medication/drug use, serum glucose levels, environmental sounds, time of day,and sleep-wake cycle of the fetus can increase or decrease fetal movement. |
| Report signs of abruptio placentae (i.e., vaginal the bleeding, uterine tenderness, abdominal pain, and decreased fetal activity). | Immediate attention and intervention increases the likelihood of a positive outcome. |
| Present contact number for patient to direct questions, address changes in daily fetal movements, and so forth. | Provides chance to address concerns/misconceptions and intervene in a timely manner, as indicated. |
Evaluate fetal growth; measure progressive fundal accompany growth at each office visit or periodically during stress home visits, as appropriate. | Reduced placental functioning may accompany PIH, resulting in IUGR. Chronic intrauterine stress and uteroplacental insufficiency decrease amount of fetal contribution to amniotic fluid pool. |
| Note fetal response to medications such as MgSO4, phenobarbital, and diazepam. | Depressant effects of medication reduce fetal respiratory and cardiac function and fetal activity level, even though placental circulation may be adequate. |
| Check FHR manually or electronically, as indicated. | Helps evaluate fetal well-being. An elevated FHR may show a compensatory response to hypoxia, prematurity, or abruptio placentae. |
| Assess fetal response to BPP criteria or CST, as maternal status indicates. | BPP helps evaluate fetus and fetal environment on five specific parameters to assess CNS function and fetal contribution to amniotic fluid volume. CST assesses placental functioning and reserves. |
Assist with assessment of fetal maturity and well-being using L/S ratio, presence of PG, estriol levels, FBM, and sequential sonography beginning at 20–26 weeks’ gestation. | In the event of declining maternal/fetal condition, risks of delivering a preterm infant are weighed against the risks of continuing the pregnancy, using results from evaluative studies of lung and kidney maturity, fetal growth, and placental functioning. IUGR is associated with reduced maternal volume and vascular changes. |
| Assist with assessment of maternal plasma volume at 24–26 weeks’ gestation using Evans’ blue dye when indicated. | Identifies fetus at risk for IUGR or intrauterine fetal demise associated with reduced plasma volume and reduced placental perfusion. |
| Utilizing an ultrasonography, assist with assessment of placental size. | Reduced placental function and size are associated with PIH. |
| Give corticosteroid (dexamethasone, betamethasone) IM for at least 24–48 hr, but not more than 7 days before delivery, when severe PIH necessitates premature delivery between 28 and 34 weeks’ gestation. | Corticosteroids are thought to induce fetal pulmonary maturity (surfactant production) and prevent respiratory distress syndrome, at least in a fetus delivered prematurely because of condition or inadequate placental functioning.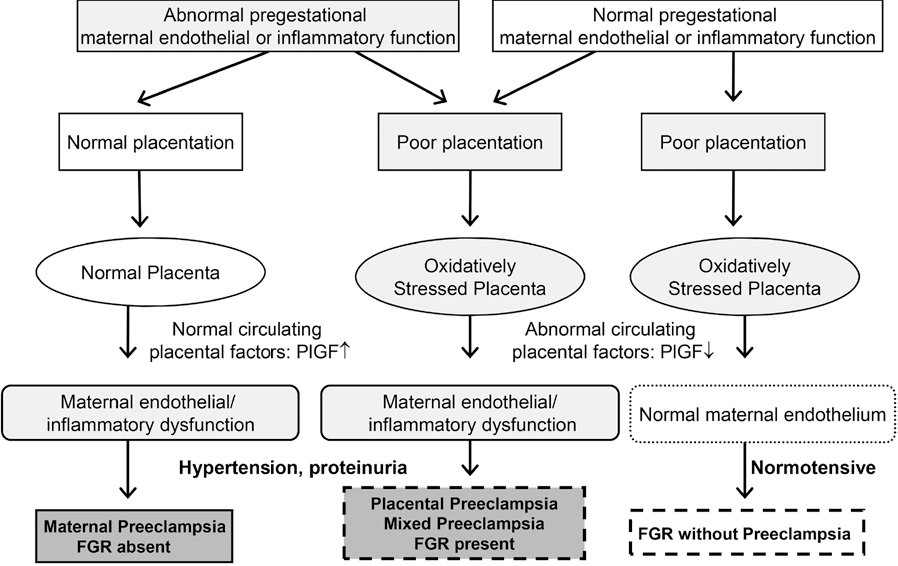 Best results are obtained when fetus is less than 34 weeks’ gestation and delivery occurs within a week of corticosteroid administration Best results are obtained when fetus is less than 34 weeks’ gestation and delivery occurs within a week of corticosteroid administration |
Risk for Maternal Injury
Risk for Injury: Vulnerable for injury as a result of environmental conditions interacting with the individual’s adaptive and defensive resources, which may compromise health.
May be related to
- Tissue edema/hypoxia
- Tonic-clonic convulsions
- Abnormal blood profile and/or clotting factors
Possibly evidenced by
- [Not applicable: Presence of signs/symptoms establishes an actual diagnosis]
Desired Outcomes
- Patient participates in treatment and/or environmental modifications to protect self and enhance safety.
- Patient is free of signs of cerebral ischemia (visual disturbances, headache, changes in mentation).
- Patient displays normal levels of clotting factors and liver enzymes
| Nursing Interventions | Rationale |
|---|---|
Check for CNS involvement (i. e., headache, irritability, visual disturbances or changes on funduscopic examination). e., headache, irritability, visual disturbances or changes on funduscopic examination). | Cerebral edema and vasoconstriction can be evaluated in terms of symptoms, behaviors, or retinal changes. |
| Emphasize importance of patient promptly reporting signs/symptoms of CNS involvement. | Delayed treatment or progressive onset of symptoms may result in tonic-clonic convulsions or eclampsia. |
| Check for alterations in level of consciousness. | In progressive PIH, vasoconstriction and vasospasms of cerebral blood vessels reduce oxygen consumption by 20% and result in cerebral ischemia. |
| Assess for signs of impending eclampsia: hyperactivity of deep tendon reflexes (3+ to 4+), ankle clonus, decreased pulse and respirations, epigastric pain, and oliguria (less than 50 ml/hr). | Generalized edema/vasoconstriction, manifested by severe CNS, kidney, liver, cardiovascular, and respiratory involvement, precede convulsive state. |
| Establish measures to lessen likelihood of seizures; i.e., keep room quiet and dimly lit, limit visitors, plan and coordinate care, and promote rest. | Lessens environmental factors that may stimulate irritable cerebrum and cause a convulsive state. |
| Enforce seizure precautions per protocol. | If seizure does occur, reduces risk of injury. |
In the event of a seizure:
| Maintains airway by reducing risk of aspiration and preventing tongue from occluding airway. Maximizes oxygenation. Note: Be cautious with use of airway/bite block, because attempts to insert when jaws are set may result in injury. |
| These signs may indicate abruptio placentae, especially if there is a preexisting medical problem, such as diabetes mellitus, or a renal or cardiac disorder causing vascular involvement. |
| Convulsions increase uterine irritability; labor may ensue. |
| During seizure activity, fetal bradycardia may occur. |
| Monitor for signs of DIC easy/spontaneous bruising, prolonged bleeding, epistaxis, GI bleeding. | Abruptio placentae with release of thromboplastin predisposes patient to DIC. |
| Hospitalize if CNS involvement is present. | Immediate introduction of therapy helps to ensure safety and limit complications. |
| Give MgSO 4 IM or IV using infusion pump. | MgSO4 a CNS depressant, decreases acetylcholine release, blocks neuromuscular transmission, and prevents seizures. It has a transient effect of lowering BP and increasing urine output by altering vascular response to pressor substances. Although IV administration of MgSO4 is easier to regulate and reduces the risk of a toxic reaction, some facilities may still use the IM route if continuous surveillance is not possible and/or if appropriate infusion apparatus is not available. Note: Adding 1 ml of 2% lidocaine to the IM injection may reduce associated discomfort. (Current research suggests the use of phenytoin infusion may be effective in the treatment of PIH without the adverse side effects, such as respiratory depression, and tocolytic effect on uterine smooth muscle, which can impede labor during intrapartum therapy.) It has a transient effect of lowering BP and increasing urine output by altering vascular response to pressor substances. Although IV administration of MgSO4 is easier to regulate and reduces the risk of a toxic reaction, some facilities may still use the IM route if continuous surveillance is not possible and/or if appropriate infusion apparatus is not available. Note: Adding 1 ml of 2% lidocaine to the IM injection may reduce associated discomfort. (Current research suggests the use of phenytoin infusion may be effective in the treatment of PIH without the adverse side effects, such as respiratory depression, and tocolytic effect on uterine smooth muscle, which can impede labor during intrapartum therapy.) |
| Monitor BP before, during, and after MgSO4 administration. Note serum magnesium levels in conjunction with respiratory rate, patellar/deep tendon reflex (DTRs), and urine output. | A therapeutic level of MgSO4is achieved with serum levels of 4.0–7.5 mEq/L or 6–8 mg/dL.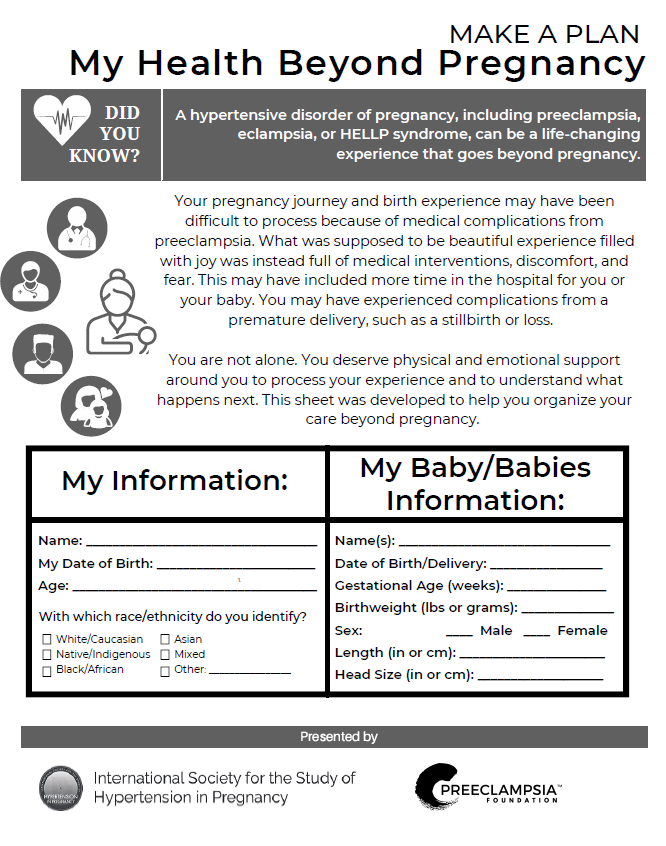 Adverse/toxic reactions develop above 10–12 mg/dL, with loss of DTRs occurring first, respiratory paralysis between 15–17 mg/dL, or heart block occurring at 30–35 mg/dL. Adverse/toxic reactions develop above 10–12 mg/dL, with loss of DTRs occurring first, respiratory paralysis between 15–17 mg/dL, or heart block occurring at 30–35 mg/dL. |
| Ready calcium gluconate. Give 10 ml (1 g/10 ml) over 3 min as indicated. | Serves as antidote to counteract adverse/toxic effects of MgSO4. |
| Administer amobarbital (Amytal) or diazepem (Valium), as indicated. | Depresses cerebral activity; has sedative effect when convulsions are not controlled by MgSO4. Not recommended as first-line therapy because sedative effect also extends to the fetus. |
| Perform funduscopic examination regulary. | Helps to evaluate changes or severity of retinal involvement. |
| Review test results of clotting time, PT, PTT, fibrinogen levels, and FPS/FDP. | Such tests can indicate depletion of coagulation factors and fibrinolysis, which suggests DIC. |
Scan sequential platelet count. Avoid amniocentesis if platelet count is less than 50,000/mm3. If thrombocytopenia is present during operative procedure, use general anesthesia. Transfuse with platelets, packed red blood cells, fresh frozen plasma, or whole blood, as indicated. Rule out HELLP syndrome. If thrombocytopenia is present during operative procedure, use general anesthesia. Transfuse with platelets, packed red blood cells, fresh frozen plasma, or whole blood, as indicated. Rule out HELLP syndrome. | Thrombocytopenia may arise because of platelet adherence to disrupted endothelium or reduced prostacyclin levels (a potent inhibitor of platelet aggregation). Invasive procedures or anesthesia requiring needle puncture (such as spinal/epidural) could result in excessive bleeding. |
| Monitor liver enzymes and bilirubin; note hemolysis and presence of Burr cells on peripheral smear. | Elevated liver enzyme (AST, ALT) and bilirubin levels, microangiopathic hemolytic anemia, and thrombocytopenia may indicate presence of HELLP syndrome, signifying a need for immediate cesarean delivery if condition of cervix is unfavorable for induction of labor. |
Prepare for cesarean birth if PIH is severe, placental functioning is compromised, and cervix is not ripe or is not responsive to induction.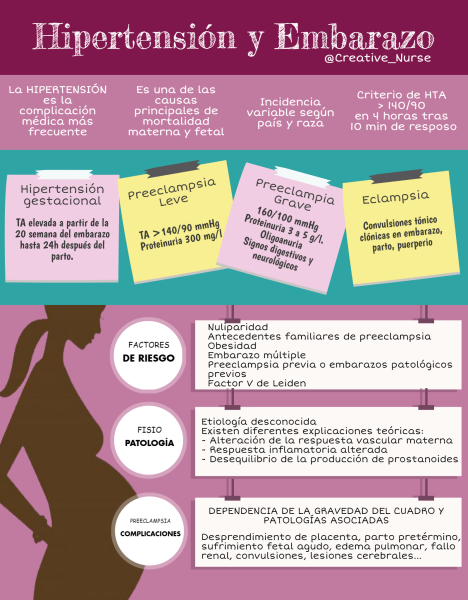 | When fetal oxygenation is severely reduced owing to vasoconstriction within malfunctioning placenta, immediate delivery may be necessary to save the fetus. |
 Review history of other medical problems.
Review history of other medical problems.
Risk for Imbalanced Nutrition: Less Than Body Requirements
Imbalanced Nutrition: Less Than Body Requirements: Intake of nutrients insufficient to meet metabolic needs.
May be related to
- Intake insufficient to meet metabolic demands and replace losses
Possibly evidenced by
- [Not applicable; presence of signs/symptoms establishes an
actual diagnosis]
Desired Outcomes
- Patient verbalizes understanding of individual dietary needs.
- Patient demonstrates knowledge of proper diet as evidenced by developing a dietary plan within own financial resources.
- Patient displays appropriate weight gain.
| Nursing Interventions | Rationale |
|---|---|
Determine patient’s nutritional status, condition of hair and nails, and height and pregravid weight.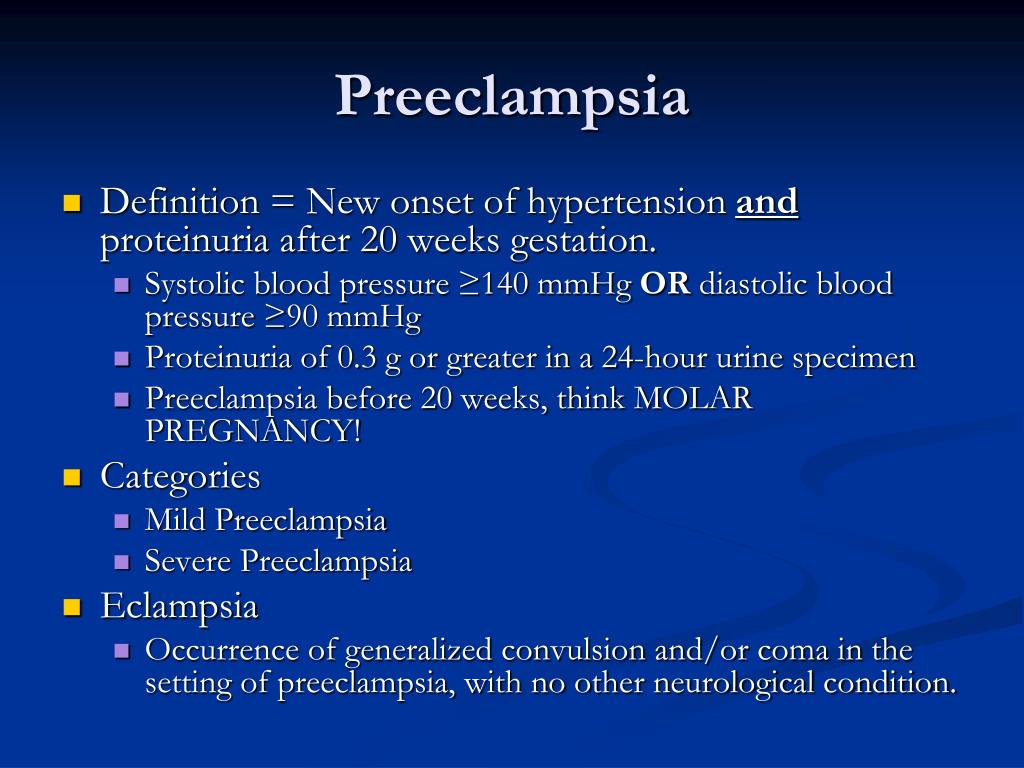 | Establishes guidelines for determining dietary needs and educating patient. Malnutrition may be a contributing factor to the onset of PIH, specifically when client follows a low-protein diet, has insufficient caloric intake, and is overweight or underweight by 20% or more before conception. |
| Provide information about normal weight gain in pregnancy, modifying it to meet client’s needs. | The underweight patient may need a diet higher in calories; the obese patient should avoid dieting because it places the fetus at risk for ketosis. |
| Present oral/written information about action and uses of protein and its role in development of PIH. | Regular intake of 80–100 g/day (1.5 g/kg) is sufficient to replace proteins lost in urine and allow for normal serum oncotic pressure. |
| Provide information regarding effect of bedrest and reduced activity on protein requirements. | Decreasing metabolic rate through bedrest and limited activity reduces protein needs. |
| Collaborate with dietitian, as indicated. | Helpful in creating individual dietary plan incorporating specific needs/restrictions. |
Deficient Knowledge
Deficient Knowledge: Absence or deficiency of cognitive information related to specific topic.
May be related to
- Lack of exposure
- Unfamiliarity with information resources
- Misinterpretation
Possibly evidenced by
- Request for information
- Statement of misconceptions
- Inaccurate follow-through of instructions
- Development of preventable complications
Desired Outcomes
- Patient identifies signs/symptoms requiring medical evaluation.
- Patient performs necessary procedures correctly.
- Patient verbalizes understanding of disease process and appropriate treatment plan.
- Patient initiate lifestyle/behavior changes as indicated.
| Nursing Interventions | Rationale |
|---|---|
| Assess patient’s/couple’s knowledge of the disease process. Provide information about pathophysiology of PIH, implications for mother and fetus; and the rationale for interventions, procedures, and tests, as needed. | Establishes data base and provides information. Provide information about areas in which learning is needed. Taking information can improve understanding and reduce fear, helping to facilitate the treatment plan for the client. Note: Current research in progress may provide additional treatment options, such as using low-dose (60 mg/day) aspirin to reduce thromboxane generation by platelets, limiting the severity/incidence of PIH. |
| Provide information about signs/symptoms indicating worsening of condition, and instruct patient when to notify healthcare provider. | Helps ensure that patient seeks timely treatment and may prevent worsening of preeclamptic state or additional complications.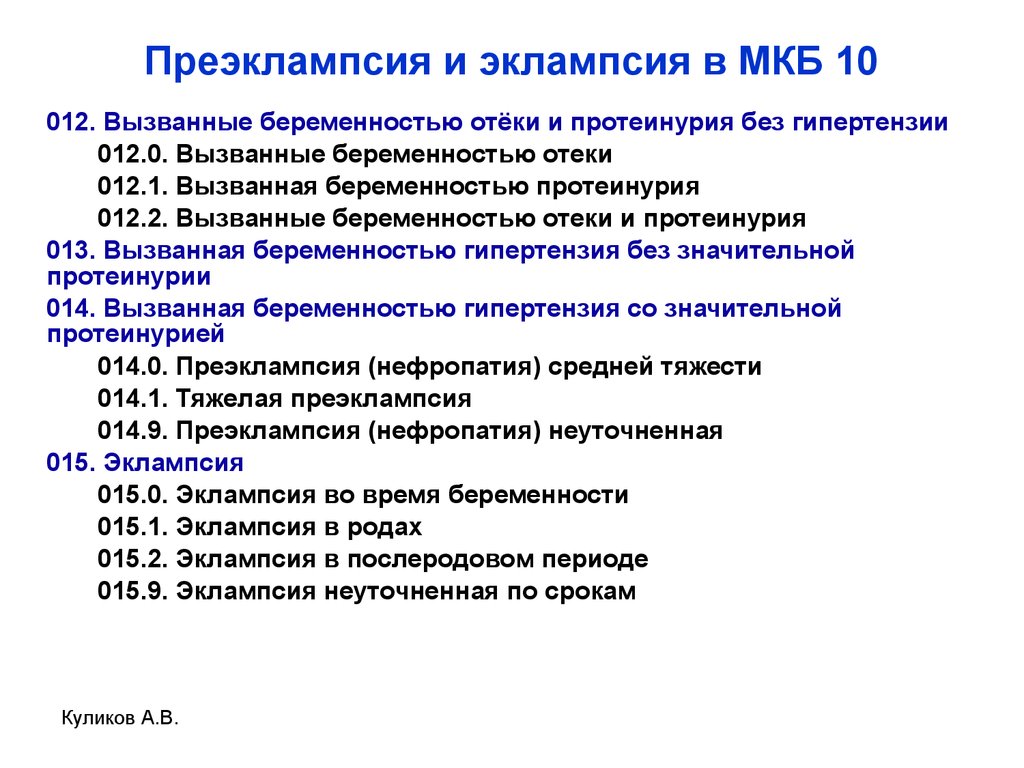 |
| Have patient informed of health status, results of when tests, and fetal well-being. | Fears and anxieties can be compounded when patient/couple does not have adequate information about the state of the disease process or its impact on patient and fetus. |
| Educate patient on how to monitor her own weight at home, and to notify healthcare provider if gain is in excess of 2 lb/wk, or 0.5 lb/day. | Gain of 3.3 lb or greater per month in second trimester or 1 lb or greater per week in third trimester is suggestive of PIH. |
| Educate and assist family members in learning the procedure for home monitoring of BP, as indicated. | Encourages cooperation in treatment regimen, allows immediate intervention as needed, and may provide reassurance that efforts are beneficial. |
| Review techniques for stress management and diet restriction. | Strengthens importance of patient’s responsibility in treatment. |
Provide information about ensuring enough protein in diet for patient with possible or mild preeclampsia.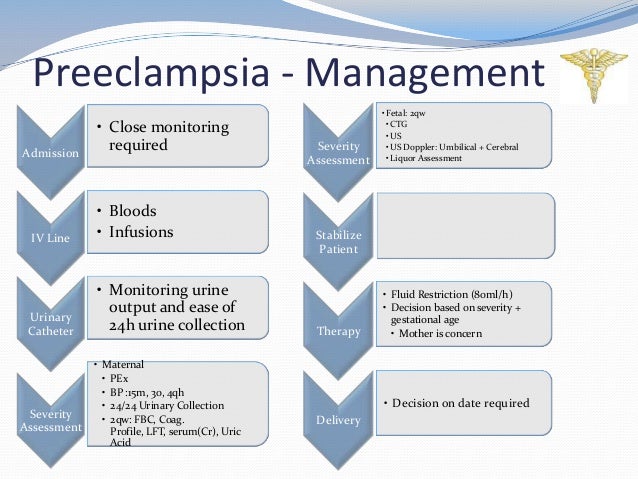 | Protein is essential for intravascular and extravascular fluid regulation. |
| Review self-testing of urine for protein. Reinforce rationale for and implications of testing. | A test result of 2+ or greater is vital and needs to be reported to healthcare provider. Urine specimen contaminated by vaginal discharge or RBCs may produce positive test result for protein. |
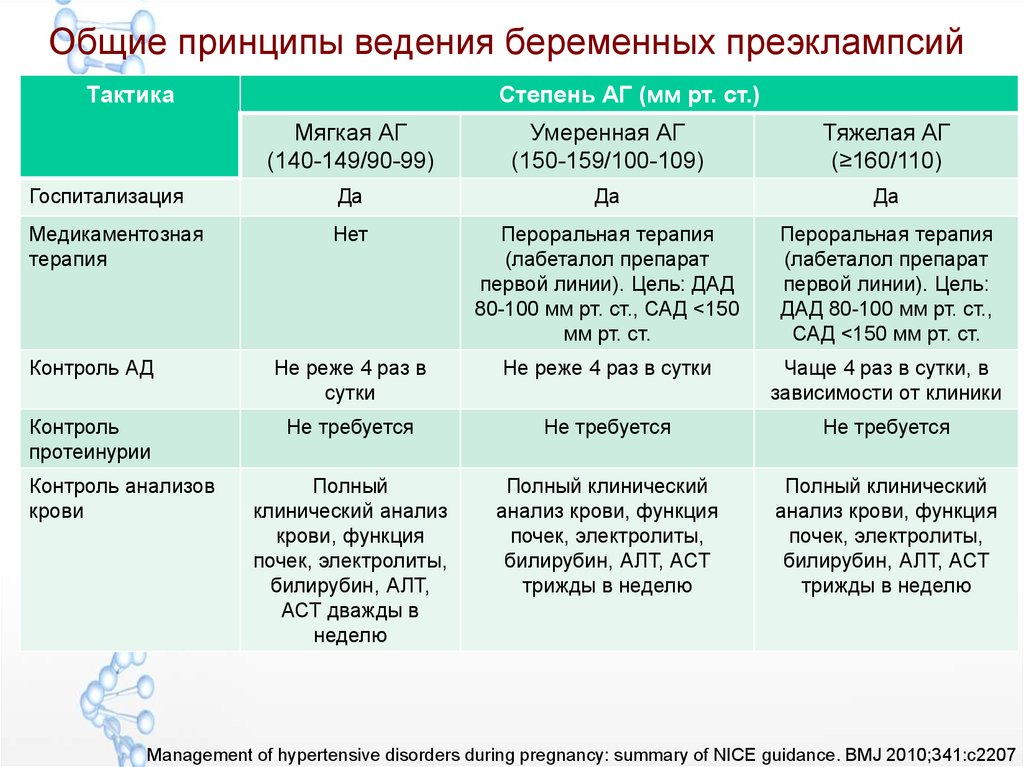
Preeclampsia. Part 2: Management, prevention of pre-eclampsia
How do we treat preeclampsia?
The only reliable treatment for preeclampsia is delivery! No placenta - no source of bad anti-angionic factors in the mother's bloodstream, no symptoms of preeclampsia. But! Management tactics will be determined by the gestational age and the severity of preeclampsia: in the absence of risks for the patient herself, we will try to prolong the pregnancy as much as possible in the interests of fetal maturation.
Treatment begins with magnesia therapy (intravenously we inject a solution of magnesia sulfate).
We select antihypertensive therapy (1st line drug - "Methyldopa", 2nd line - "Nifedipine" with slow release, 3rd line - B-blockers: "Metoprolol", "Bisoprolol", 4th line - "Clonidine"). Unfortunately, Labetalol, which is the first-line drug in the world, is not registered in Russia).
· Be sure to include sedative sedatives in the complex therapy of preeclampsia.
· In order to improve uteroplacental blood flow after lowering blood pressure numbers, we connect low molecular weight heparins.
· In the case of severe early preeclampsia, when we understand that preterm birth is inevitable, we carry out the prevention of fetal RDS (an injection for the maturation of the lungs).
Tactically we are moving in 3 directions:
· If we have selected therapy and the patient's condition has stabilized, then discharge with careful outpatient monitoring is possible.
If the condition has stabilized, but maximum doses of drugs are required for maintenance; or laboratory tests are very abnormal; or the condition of the fetus requires constant monitoring, then we stay in the hospital, prolong the pregnancy, but at any time we are ready for an emergency delivery.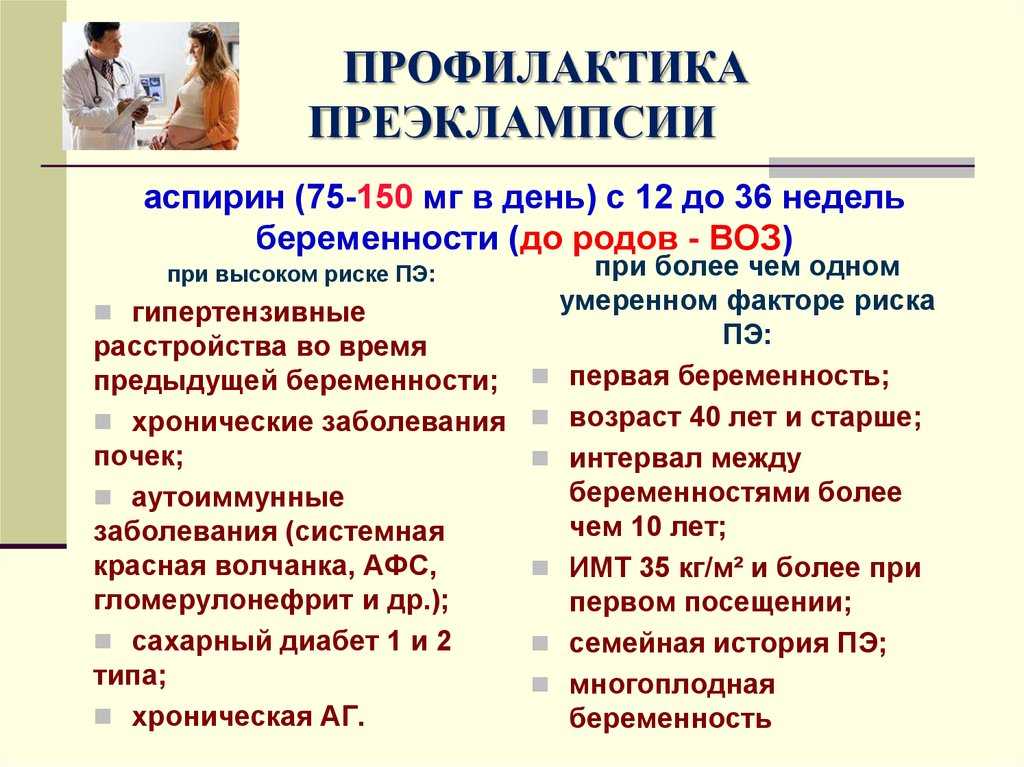
If antihypertensive drugs do not control blood pressure, laboratory tests progressively worsen, or critical symptoms of preeclampsia appear, then this may indicate that the patient's internal organs are working to the limit of their capabilities or the condition of the fetus is severely disturbed! In such a situation, patients are urgently delivered, further prolongation of pregnancy threatens their lives and / or the life of their child.
In cases of early (before 34 weeks) pre-eclampsia, while observing the safety conditions for the patient and the child, we prefer expectant management.
In cases of late preeclampsia (after 34 weeks), when the fetal lungs are almost mature, we prefer more active management tactics.
If preeclampsia overshadowed your pregnancy and did not allow you to fully enjoy the most beautiful period of a woman's life - pregnancy, do not despair! First, it is not necessary that preeclampsia will recur in the next pregnancy, since preeclampsia is usually the lot of the first pregnancy. But before planning your next pregnancy, make sure you don't have any risk factors for preeclampsia.
But before planning your next pregnancy, make sure you don't have any risk factors for preeclampsia.
So, the examination plan before the planned pregnancy after suffering preeclampsia is as follows:
Ultrasound of the kidneys with the study of renal blood flow
Abdominal Ultrasound
· ECHOCG
SMAD
· (MRI of the brain, depending on the variant of the course of preeclampsia)
· Blood chemistry
Coagulogram Ddimer
· General urine analysis
· Clinical blood test
Examination for APS (VA, antibodies to cardiolipin, beta-2-glycoprotein)
Examination for systemic autoimmune disease: antinuclear factor, antinuclear antibodies
Examination for genetic and acquired thrombophilias, including studies of protein C and S levels, VIII and von Willebrand factors, homocysteine
Pelvic ultrasound and, if chronic endometritis is suspected, paypel aspiration biopsy of the endometrium.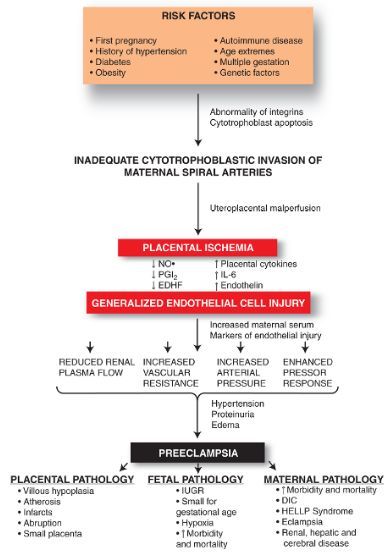
We involve specialists in preparation for pregnancy, depending on the identified pathology (cardiologist, nephrologist, rheumatologist, etc.).
What medications might we need?
This, of course, is aspirin and low molecular weight heparins. Antihypertensive drugs - in case of chronic hypertension, immunosuppressive drugs - in the presence of rheumatological problems, etc.
During pregnancy, patients who have had preeclampsia or who are at high risk for preeclampsia on first screening will receive aspirin 150mg. The need to prescribe other drugs is determined individually!
What is the saving power of aspirin?
Firstly, it has a positive effect on platelet aggregation (aspirin blocks the synthesis of thromboxane, a substance that increases platelet adhesion) and thus prevents thrombosis and heart attacks in the placenta.
Secondly, aspirin has angioprotective (vascular protection) and vasodilating effects due to the ability to increase the formation of nitric oxide.
The third and most important property of aspirin is immunomodulatory and anti-inflammatory, which today is given a central place in explaining the normalization of implantation, the formation of a rich vascular tree of the placenta and, thus, in the prevention of preeclampsia and other placenta-associated complications of pregnancy (fetal growth retardation, placental abruption).
So, according to studies, taking aspirin during pregnancy prevents the development of preeclampsia in more than 60% of cases!
Conclusions:
· Today it is possible to predict preeclampsia already from the end of the first trimester.
· There are ways to prevent the development of preeclampsia.
In case of suspected preeclampsia, hospitalization is necessary to assess the severity of preeclampsia, determine further management tactics, and select therapy.
· In preparation for the next pregnancy, all patients who have had preeclampsia need to conduct an examination and specific preconception preparation.
Special offer for the treatment of preeclampsia at the MD GROUP Clinical Hospital
Preeclampsia. What is Preeclampsia?
IMPORTANT
The information in this section should not be used for self-diagnosis or self-treatment. In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests. For diagnosis and proper treatment, you should contact your doctor.
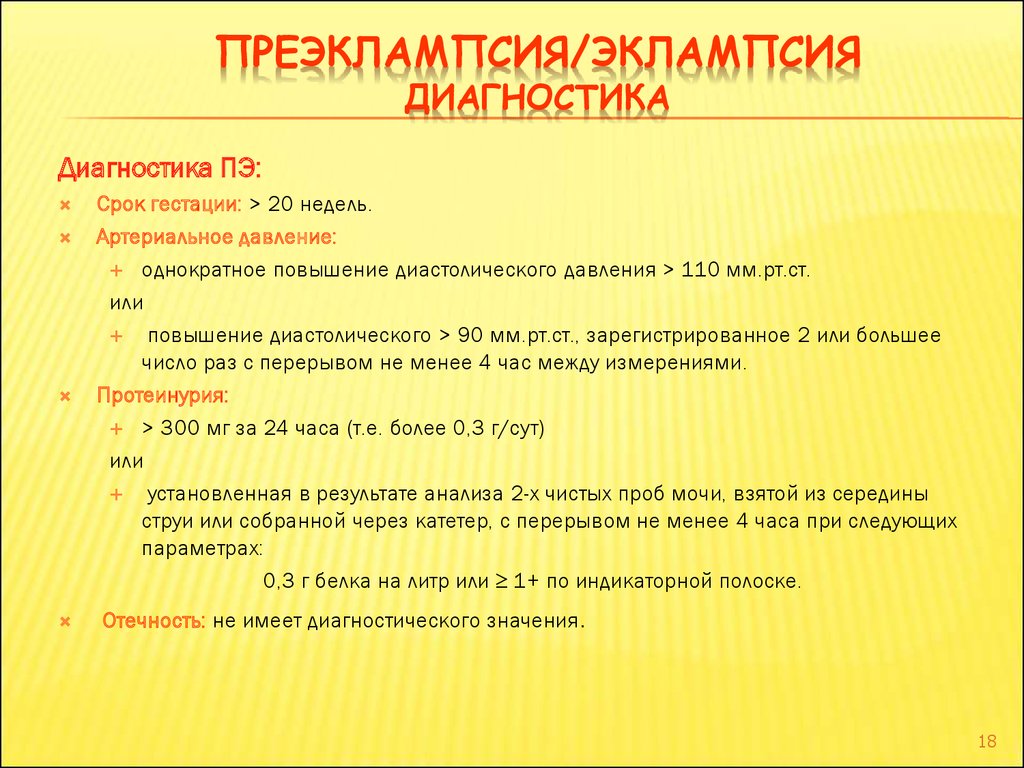
Preeclampsia is a severe variant of preeclampsia that occurs after the 20th week of gestational age, is characterized by multiple organ disorders with a primary lesion of the central nervous system, and precedes eclampsia. Manifested by headaches, nausea, vomiting, visual disturbances, hyperreflexia, lethargy, drowsiness or insomnia. It is diagnosed on the basis of data from daily monitoring of blood pressure, urinalysis, coagulogram, transcranial dopplerography. For treatment, infusion therapy, anticonvulsant, antihypertensive, anticoagulant, membrane stabilizing agents are used. With the ineffectiveness of appointments, an emergency caesarean section is indicated.
With the ineffectiveness of appointments, an emergency caesarean section is indicated.
ICD-10
O14 Pregnancy-induced hypertension with significant proteinuria
- Causes of pre-eclampsia
- Pathogenesis
- Symptoms of preeclampsia
- Complications
- Diagnostics
- Treatment of preeclampsia
- Prognosis and prevention
- Prices for treatment
General
Often, preeclampsia develops after the 28th week of gestation against the background of milder forms of preeclampsia. The preeclamptic state is observed in 5% of pregnant women, women in labor and puerperas. In 38-75% of patients, it occurs in the prenatal period, in 13-36% - in childbirth, in 11-44% - after childbirth. In 62% of cases, preeclampsia precedes eclampsia, although, according to some authors, in other patients, the disorder remains unrecognized due to the rapid development of convulsive syndrome. More often, the disease occurs in predisposed women during the first teenage, late, multiple pregnancy, repeated gestation with a history of preeclampsia, the presence of obesity, extragenital pathology (chronic arterial hypertension, diseases of the liver, kidneys, collagenoses, diabetes mellitus, antiphospholipid syndrome).
More often, the disease occurs in predisposed women during the first teenage, late, multiple pregnancy, repeated gestation with a history of preeclampsia, the presence of obesity, extragenital pathology (chronic arterial hypertension, diseases of the liver, kidneys, collagenoses, diabetes mellitus, antiphospholipid syndrome).
Preeclampsia
Causes of preeclampsia
The etiology of the disorder, as well as other forms of gestosis, has not been finally established to date. A likely factor contributing to the development of preeclampsia is the pathological reaction of the body of a predisposed woman to physiological changes during pregnancy. More than 30 reasoned etiopathogenetic theories of the onset of the disease have been proposed by specialists in the field of obstetrics, the main of which are:
- Hereditary. The role of genetic factors in the development of preeclampsia is confirmed by its more frequent diagnosis in patients whose mothers suffered from preeclampsia.
 Patients have defects in the genes 7q36-eNOS, 7q23-ACE, AT2P1, C677T. The mode of inheritance is presumably autosomal recessive.
Patients have defects in the genes 7q36-eNOS, 7q23-ACE, AT2P1, C677T. The mode of inheritance is presumably autosomal recessive. - Immune. Penetration into the maternal circulation of foreign antigens of the fetus is accompanied by the response production of antibodies. The deposition of the formed immune complexes in various tissues triggers complex protective mechanisms, which are manifested by the activation of endothelial cells and acute endotheliosis.
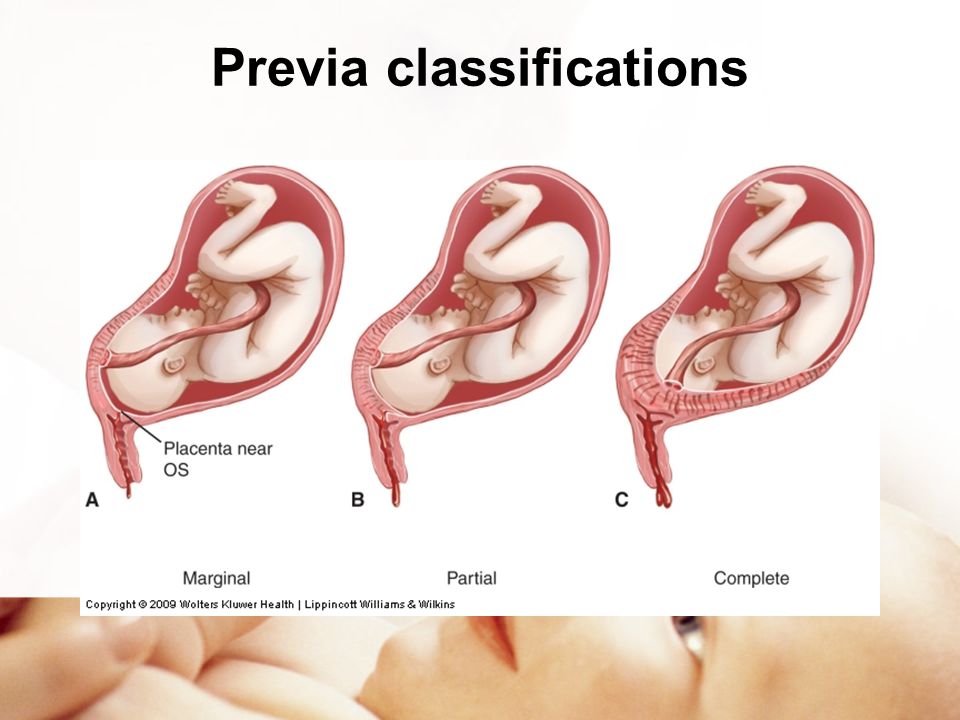
- Placental. Some authors associate preeclampsia with impaired cytotrophoblast invasion. As a result, there is no transformation of the smooth muscle layer of the uterine arteries, which subsequently leads to their spasm, deterioration of intervillous blood flow, hypoxia and, as a result, damage to the endothelium.
- Cortico-visceral. Proponents of the theory consider preeclampsia as a neurotic hemodynamic disorder caused by a violation of the relationship between the cortex and subcortical regions. This approach explains the provoking role of severe stress and is confirmed by functional changes in the EEG.
Since individual theories cannot fully explain all the clinical manifestations of the disease, it is justified to consider preeclampsia as a polyetiological condition with common mechanisms of pathogenesis. The immediate causes of the development of preeclampsia are improperly selected therapy for dropsy of pregnancy and nephropathy, non-compliance by the patient with medical recommendations, and high therapeutic resistance of milder variants of gestosis.
Pathogenesis
The key link in the mechanism of development of preeclampsia is the generalization of acute endotheliosis and vasoconstriction, initially localized in the placenta, with the involvement of brain tissues in the pathological process. Vascular dysfunction leads to damage to cell membranes, impaired metabolism of neurons with the occurrence of hypersensitivity and increased excitability of nerve cells. The defeat of the suprasegmental subcortical structures is accompanied by polysystemic autonomic disorders, detected in more than 90% of patients with severe forms of preeclampsia.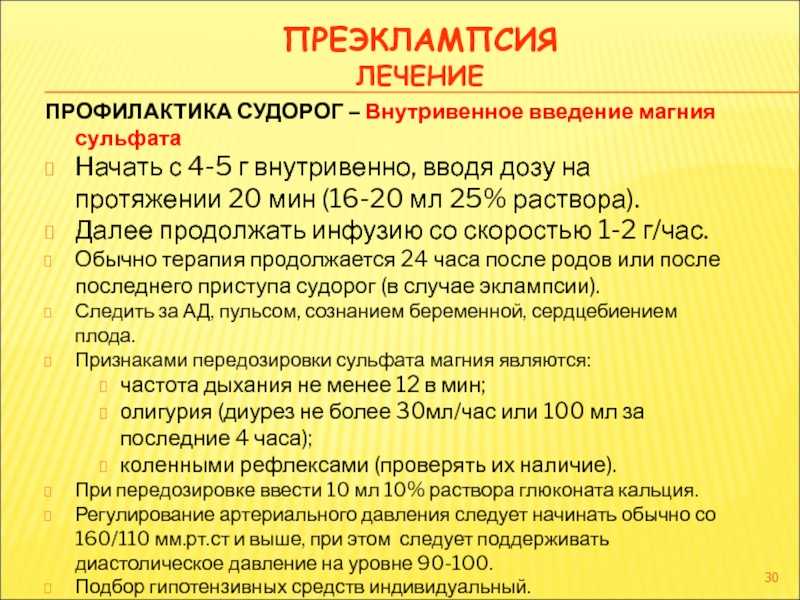
In parallel, pregnant women and women in labor with preeclampsia develop pyramidal insufficiency, which indicates a disorder at the level of the cortical sections and is manifested by tendon-periosteal hyperreflexia, anisoreflexia, the occurrence of pathological reflexes, and an increase in convulsive readiness. The last to be affected are the brain stem regions. Destructive processes caused by microcirculation disorders also occur in other organs - the liver, kidneys, lung tissue. The situation is aggravated by coagulopathic disorders characteristic of gestosis.
Symptoms of preeclampsia
Usually, the disorder occurs against the background of previous nephropathy. Existing edema, arterial hypertension, moderate astheno-vegetative symptoms (dizziness, weakness, insufficient sleep, meteotropism, emotional lability) are accompanied by signs of CNS damage and increased intracranial pressure. The patient complains of intense headache, heaviness in the back of the head, fatigue, looks lethargic, lethargic, indifferent, sometimes responds inappropriately. There is increased drowsiness or insomnia, trembling of outstretched fingers, sweating of the palms and feet.
There is increased drowsiness or insomnia, trembling of outstretched fingers, sweating of the palms and feet.
In 25% of women with a clinic of preeclampsia, visual disorders are detected - a feeling of blurred vision, flickering of sparks or flies, fear of light, double vision, loss of individual fields of vision. Perhaps the appearance of nausea, vomiting, pain in the epigastrium and right hypochondrium. In severe cases, there are muscle twitches, delirium, hallucinations, petechial rash, indicating a violation of blood clotting. The pre-eclamptic state is relatively short, lasting no more than 3-4 days, after which it is stopped by the correct therapy or passes into eclampsia.
Complications
The most formidable complication of preeclampsia is eclampsia, the most severe type of preeclampsia with high rates of maternal and perinatal mortality. In 1-3% of patients, there is a loss of vision (amaurosis) caused by edema, vascular changes, retinal detachment or ischemia of the occipital lobe of the cortex due to circulatory disorders in the posterior cerebral artery basin.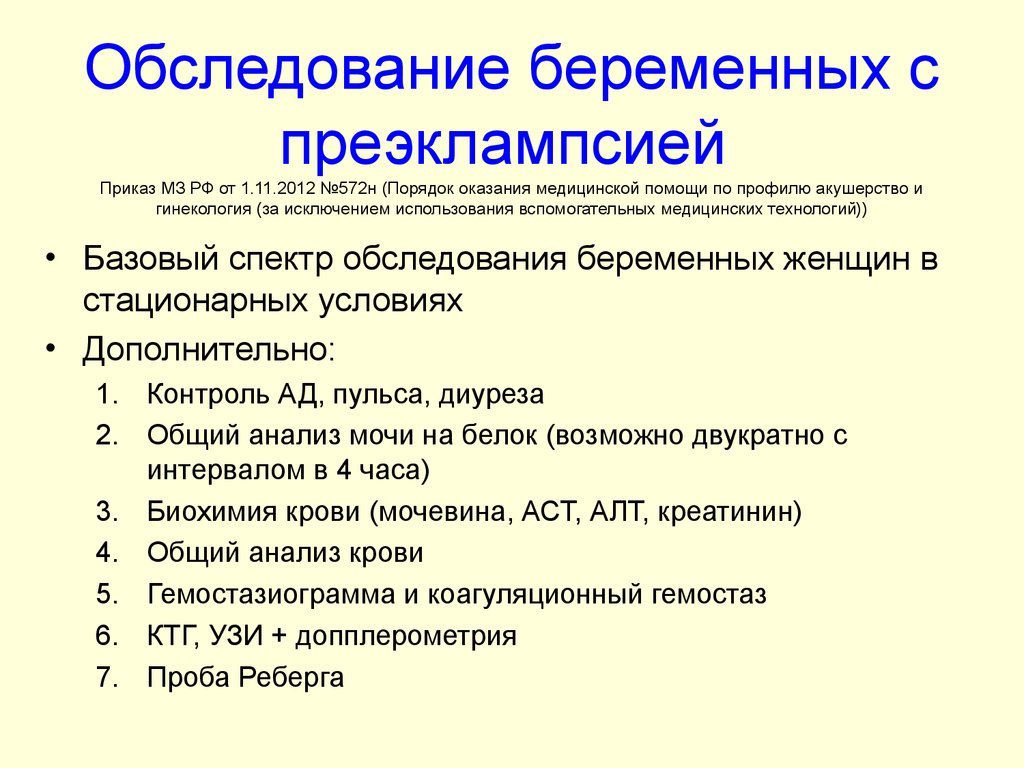 Perhaps the development of a hypertensive crisis, cerebral edema, stroke, HELLP-syndrome, detachment of a normally located placenta, the occurrence of postpartum coagulopathic bleeding and DIC. Fetoplacental insufficiency is usually aggravated, signs of intrauterine fetal hypoxia are growing.
Perhaps the development of a hypertensive crisis, cerebral edema, stroke, HELLP-syndrome, detachment of a normally located placenta, the occurrence of postpartum coagulopathic bleeding and DIC. Fetoplacental insufficiency is usually aggravated, signs of intrauterine fetal hypoxia are growing.
Women who have had preeclampsia are 4 times more likely to develop cardiovascular diseases (hypertension, angina pectoris, heart attacks, strokes, congestive heart failure) in the future, and the risk of developing type 2 diabetes mellitus doubles. In a third of patients, gestosis is diagnosed in subsequent pregnancies.
Diagnostics
Timely diagnosis of preeclampsia is usually not particularly difficult if the pregnant woman has been under the supervision of an obstetrician-gynecologist for a long time about previous nephropathy. At the initial visit of a patient with characteristic complaints, an examination plan is recommended with the identification of specific markers of preeclampsia:
- Blood pressure control.
 Daily monitoring with automatic measurement of blood pressure using a special device is shown. In patients with preeclampsia, blood pressure usually exceeds 180/110 mm Hg. Art. with a pulse amplitude of more than 40 mm Hg. Art. The arterial hypertension index is 50% or more.
Daily monitoring with automatic measurement of blood pressure using a special device is shown. In patients with preeclampsia, blood pressure usually exceeds 180/110 mm Hg. Art. with a pulse amplitude of more than 40 mm Hg. Art. The arterial hypertension index is 50% or more. - Evaluation of the hemostasis system. Preeclampsia is characterized by coagulopathy of consumption and activation of the fibrinolytic system. It is recommended to study the content of fibrinogen, its degradation products (RFMK), antithrombin III, endogenous heparin, to evaluate APTT, prothrombin (MHO), thrombin time.
- Urinalysis. Proteinuria is an important symptom of preeclampsia. The protein content in the urine exceeds 5 g / l, granular casts, leukocyturia can be detected. Hourly urine output is often reduced to 40 ml or less. To assess the severity of kidney damage, the daily amount of protein in the urine is determined.
- TKDG of cerebral vessels. It is used for an objective assessment of cerebral blood flow.
 In the course of transcranial Doppler sonography, the presence of signs of an increase in cerebral perfusion pressure and a decrease in vascular resistance, characteristic of preeclampsia, is confirmed.
In the course of transcranial Doppler sonography, the presence of signs of an increase in cerebral perfusion pressure and a decrease in vascular resistance, characteristic of preeclampsia, is confirmed.
Taking into account possible obstetric complications, the patient is shown ultrasound of the uterus and placenta, dopplerography of the uteroplacental blood flow, CTG, fetometry, and fetal phonocardiography. Differential diagnosis is carried out with diseases of the brain (thrombosis of the sinuses of the hard shell, meningitis, tumors, stroke), non-convulsive forms of epilepsy, retinal detachment. A pregnant woman is consulted by an anesthesiologist-resuscitator, therapist, neuropathologist, ophthalmologist, cardiologist, nephrologist.
Treatment of preeclampsia
The patient is urgently admitted to the intensive care unit of the nearest hospital with a delivery room. The main therapeutic task is to reduce reflex and central hyperreactivity, prevent convulsive syndrome, stabilize vital functions, and correct multiple organ disorders.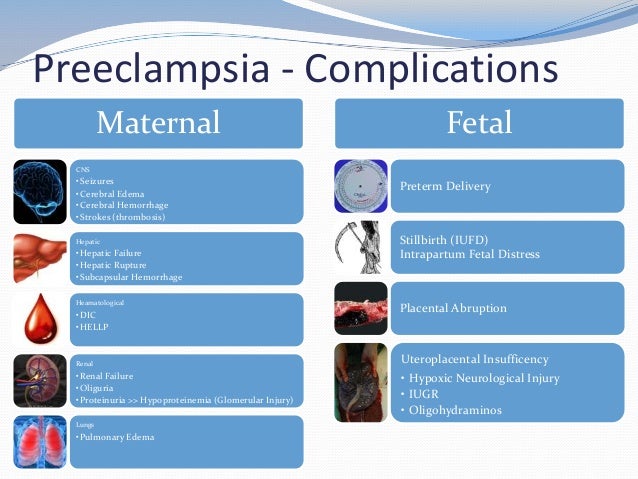 A pregnant woman with preeclampsia is shown a strict medical and protective regimen. The treatment regimen includes the appointment of the following groups of drugs:
A pregnant woman with preeclampsia is shown a strict medical and protective regimen. The treatment regimen includes the appointment of the following groups of drugs:
- Anticonvulsants. The “gold standard” is the introduction of magnesium sulfate through an infusomat. The drug has a sedative, anticonvulsant, antispasmodic, hypotensive effect, effectively reduces intracranial pressure. Simultaneously with the improvement of cerebral hemodynamics, it relaxes the myometrium and increases the intensity of blood flow in the uterus. If necessary, tranquilizers are additionally used.
- Antihypertensives. Imidazoline derivatives are preferred, which have a central α2-adrenomimetic effect, stimulate I1-imadazoline receptors in the nucleus of the solitary tract and thereby increase the parasympathetic effect on the myocardium. Perhaps parenteral administration of peripheral vasodilators, hybrid β- and α1-blockers with a rapid antihypertensive effect.
- Infusion formulations.
 To normalize oncotic and osmotic pressure, colloidal, protein, balanced crystalloid solutions are injected intravenously. Infusion therapy improves the rheological properties of blood, central and peripheral hemodynamics, tissue perfusion, reduces the severity of multiple organ disorders, and restores water and electrolyte balance.
To normalize oncotic and osmotic pressure, colloidal, protein, balanced crystalloid solutions are injected intravenously. Infusion therapy improves the rheological properties of blood, central and peripheral hemodynamics, tissue perfusion, reduces the severity of multiple organ disorders, and restores water and electrolyte balance.
According to indications, sedatives, direct-acting anticoagulants, antioxidants, membrane stabilizers, drugs to improve blood flow in tissues, and prevent fetal respiratory distress syndrome are used. With the ineffectiveness of intensive therapy within a day from the moment of hospitalization, emergency delivery by caesarean section is recommended. Patients with rapidly increasing symptoms of preeclampsia undergo surgery within 2-4 hours. Natural childbirth with high-quality anesthesia (long-term epidural anesthesia), perineotomy or episiotomy is possible only with a significant improvement in the patient's well-being, persistent stabilization of blood pressure, and laboratory parameters.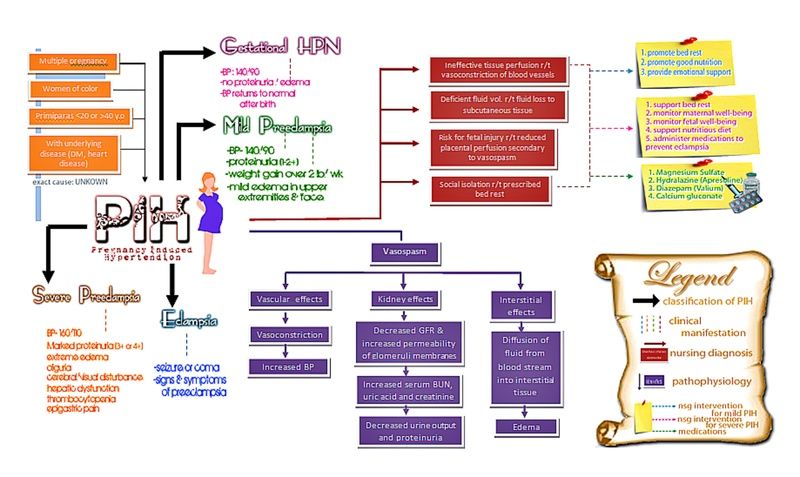
Prognosis and prevention
The outcome of gestation in pregnant women with symptoms of preeclampsia depends on the availability of medical care and the correct choice of management tactics. In any case, the prognosis for the mother and fetus is considered serious. The level of maternal mortality in recent years has been reduced to 0.07 per 1000 births, perinatal mortality ranges from 21 to 146 per 1000 observations. Prevention of preeclampsia involves regular examinations at the antenatal clinic, monitoring of pressure and laboratory parameters in patients with dropsy of pregnancy, nephropathies, careful implementation of all medical prescriptions, normalization of sleep and rest, psycho-emotional peace, control of weight gain, protein-enriched diet with low salt content.
Sources
- Emergency care for preeclampsia and its complications (eclampsia, HELLP syndrome). Clinical guidelines (treatment protocols). – 2014.