Pelvic pain left side early pregnancy
Pelvic pain in pregnancy - NHS
Some women may develop pelvic pain in pregnancy. This is sometimes called pregnancy-related pelvic girdle pain (PGP) or symphysis pubis dysfunction (SPD).
PGP is a collection of uncomfortable symptoms caused by a stiffness of your pelvic joints or the joints moving unevenly at either the back or front of your pelvis.
Symptoms of PGP
PGP is not harmful to your baby, but it can be painful and make it hard to get around.
Women with PGP may feel pain:
- over the pubic bone at the front in the centre, roughly level with your hips
- across 1 or both sides of your lower back
- in the area between your vagina and anus (perineum)
- spreading to your thighs
Some women may feel or hear a clicking or grinding in the pelvic area.
The pain can be worse when you're:
- walking
- going up or down stairs
- standing on 1 leg (for example, when you're getting dressed)
- turning over in bed
- moving your legs apart (for example, when you get out of a car)
Most women with PGP can have a vaginal birth.
Non-urgent advice: Call your midwife or GP if you have pelvic pain and:
- it's hard for you to move around
- it hurts to get out of a car or turn over in bed
- it's painful going up or down stairs
These can be signs of pregnancy-related pelvic girdle pain.
Treatments for PGP
Getting diagnosed as early as possible can help keep pain to a minimum and avoid long-term discomfort.
You may be referred to a physiotherapy service that specialises in obstetric pelvic joint problems.
Physiotherapy aims to relieve or ease pain, improve muscle function, and improve your pelvic joint position and stability.
This may include:
- exercises to strengthen your pelvic floor, stomach, back and hip muscles
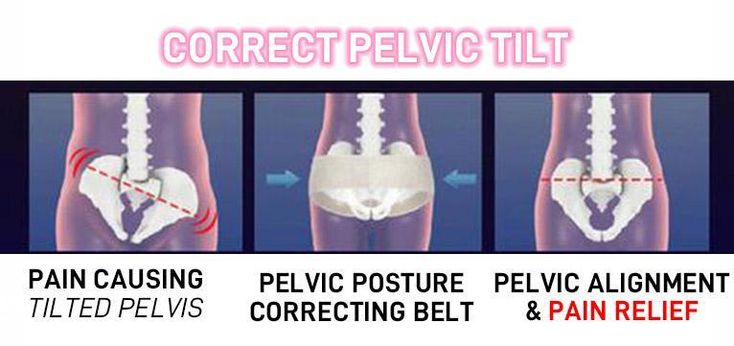
- equipment, if necessary, such as crutches or pelvic support belts
These problems tend not to get completely better until the baby is born, but treatment from an experienced practitioner can improve the symptoms during pregnancy.
Coping with pelvic pain in pregnancy
Your physiotherapist may recommend a pelvic support belt to help ease your pain, or crutches to help you get around.
It can help to plan your day so you avoid activities that cause you pain. For example, do not go up or down stairs more often than you have to.
For example, do not go up or down stairs more often than you have to.
The Pelvic, Obstetric & Gynaecological Physiotherapy (POGP) network also offers this advice:
- be as active as possible within your pain limits, and avoid activities that make the pain worse
- rest when you can
- ask your family, friends or partner, if you have one, to help with everyday activities
- wear flat, supportive shoes
- sit down to get dressed – for example, do not stand on 1 leg when putting on jeans
- keep your knees together when getting in and out of the car – a plastic bag on the seat can help you swivel
- sleep in a comfortable position – for example, on your side with a pillow between your legs
- try different ways of turning over in bed – for example, turning over with your knees together and squeezing your buttocks
- take the stairs 1 at a time, or go upstairs backwards or on your bottom
- if you're using crutches, have a small backpack to carry things in
- if you want to have sex, consider different positions, such as kneeling on all fours
POGP suggests that you avoid:
- standing on 1 leg
- bending and twisting to lift, or carrying a baby on 1 hip
- crossing your legs
- sitting on the floor, or sitting twisted
- sitting or standing for long periods
- lifting heavy weights, such as shopping bags, wet washing or a toddler
- vacuuming
- pushing heavy objects, such as a supermarket trolley
- carrying anything in only 1 hand (try using a small backpack)
The physiotherapist should be able to provide advice on coping with the emotional impact of living with chronic pain, such as using relaxation techniques. If your pain is causing you considerable distress, then you should let your GP or midwife know. You may require additional treatment.
If your pain is causing you considerable distress, then you should let your GP or midwife know. You may require additional treatment.
Find out more on the Pelvic, Obstetric & Gynaecological Physiotherapy (POGP) website.
Labour and birth with pelvic pain
Many women with pelvic pain in pregnancy can have a normal vaginal birth.
Plan ahead and talk about your birth plan with your birth partner and midwife.
Write in your birth plan that you have PGP, so the people supporting you during labour and birth will be aware of your condition.
Think about birth positions that are the most comfortable for you, and write them in your birth plan.
Being in water can take the weight off your joints and allow you to move more easily, so you might want to think about having a water birth. You can discuss this with your midwife.
You can discuss this with your midwife.
Who gets pelvic pain in pregnancy?
It's estimated that PGP affects up to 1 in 5 pregnant women to some degree.
It's not known exactly why pelvic pain affects some women, but it's thought to be linked to a number of issues, including previous damage to the pelvis, pelvic joints moving unevenly, and the weight or position of the baby.
Factors that may make a woman more likely to develop PGP include:
- a history of lower back or pelvic girdle pain
- previous injury to the pelvis (for example, from a fall or accident)
- having PGP in a previous pregnancy
- a physically demanding job
- being overweight
Further information
Find support and advice from other women with PGP at the Pelvic Partnership.
Listen to women’s experiences of pain and discomfort in pregnancy, including PGP, on healthtalk.org.
Read more about coping with common health problems in pregnancy, including nausea, heartburn, tiredness and constipation.
Find maternity services or physiotherapy services near you.
Community content from HealthUnlockedOvary Pain in Early Pregnancy: Causes, Management, and More
Pregnancy causes a lot of changes to the body. Some of those changes can cause mild discomfort or light cramping in the area around your ovaries. Ovary pain may cause pain on one side of your lower abdominal or pelvic area. It can also sometimes cause pain in the back or thigh.
Ovary pain may be a sign that implantation is occurring, or it could be a response to the change in hormones that you’ll experience in early pregnancy.
Any serious ovary pain should be reported to your doctor. Seek immediate medical attention if you’re pregnant and experience sharp or long-lasting pain accompanied by:
Seek immediate medical attention if you’re pregnant and experience sharp or long-lasting pain accompanied by:
- nausea
- vaginal bleeding
- fever
- feeling faint
- vomiting
Read on to learn more about causes for ovary pain in early pregnancy and when to seek medical help.
The following may cause pain in the area of your ovaries in early pregnancy.
Ectopic pregnancy
Ectopic pregnancy occurs when a fertilized egg attaches itself in a place other than the inside of the uterus, usually in the fallopian tubes.
Symptoms include:
- sharp or stabbing pain, usually on one side of the pelvis or abdomen
- vaginal bleeding that’s heavier or lighter than your normal period
- weakness, dizziness, or fainting
- gastrointestinal or stomach discomfort
Seek medical help right away if you think you’re experiencing an ectopic pregnancy. Ectopic pregnancies are not viable, and, left untreated, may result in a ruptured fallopian tube or other serious complications.
Miscarriage
A miscarriage is the loss of a pregnancy before 20 weeks.
Possible symptoms include:
- vaginal bleeding
- pelvic pain, low back pain, or abdominal pain
- passing tissue or discharge through the vagina
Let your doctor know if you’re experiencing miscarriage symptoms. There’s no way to stop a miscarriage, but in some cases, medication or surgery is needed to prevent complications.
Ovarian cyst
Most ovarian cysts are asymptomatic and harmless. But cysts that continue to grow can rupture or twist, or cause complications during pregnancy and delivery.
Symptoms may include:
- pelvic pain, which may be isolated to one side
- abdominal fullness, heaviness, or bloating
- pain with fever or vomiting
Seek medical help if you have sharp or stabbing pain, especially with fever or vomiting. You should also let your OB-GYN know if you have a known ovarian cyst. They may want to monitor the cyst throughout your pregnancy.
Ovarian rupture and torsion
An ovarian rupture is a medical emergency. It can cause internal bleeding.
Ovarian torsion is also a medical emergency where a large cyst causes an ovary to twist or move from its original position. This can cut off blood supply to the ovary.
Symptoms of a rupture or torsion may include:
- severe or sharp pelvic pain, sometimes isolated to one side
- fever
- dizziness
- rapid breathing
Always let the hospital staff know if you’re pregnant and all your symptoms. You may need an ultrasound or MRI. Your doctor can then determine if surgery is necessary or recommend alternative treatment options.
Other possible causes
Other causes of pain near your ovaries during early pregnancy may include:
- gastrointestinal or stomach issues
- stretching of the uterus
- fibroids
Let your doctor know about your symptoms at your first pregnancy appointment.
Is it a sign of implantation?
Implantation occurs when a fertilized egg attaches to the interior lining of the uterus. It typically occurs 6 to 12 days after conception. Implantation occurs before you are far enough along to have a positive pregnancy test.
It typically occurs 6 to 12 days after conception. Implantation occurs before you are far enough along to have a positive pregnancy test.
Cramps around the time when implantation would occur could be an early sign of pregnancy, but until you’ve had a positive pregnancy test, it’s impossible to know if the cramps are a sign of pregnancy or an impending menstrual period.
If your period doesn’t start when expected, take a pregnancy test three days to one week later to confirm pregnancy.
Let your doctor know if you have sharp or chronic ovarian pain on one or both sides that doesn’t go away on its own. You may need emergency medical care, especially if you have sharp or chronic pain along with one or more of the following symptoms:
- nausea
- vaginal bleeding
- high fever
- feeling faint
- vomiting
Ovarian pain during pregnancy that doesn’t go away on its own may need to be treated by a doctor.
But if your doctor does not recommend any medical treatment for your pain, you may be able to manage mild discomfort at home.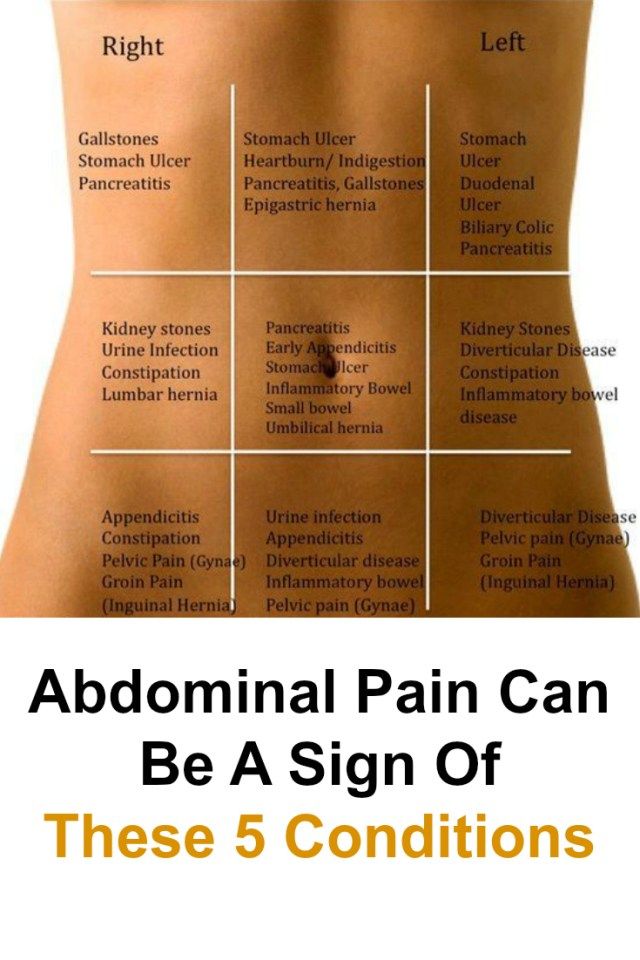
- Change positions slowly, especially when going from sitting to standing. That can help reduce incidence of pain.
- Get plenty of rest, and change or reduce your workout routine if you experience discomfort related to exercise.
- Soak in a warm (not hot) bath.
- Drink plenty of water.
- Apply gentle pressure to the sore area.
Many pain relievers aren’t safe to take during early pregnancy. Talk to your doctor before taking medication to manage pain.
You should also talk to you doctor before applying heat, such as from a hot compress. Too much heat could cause serious birth defects.
Treatment will depending on the underlying cause. In some cases, you may not need treatment.
For treatment of an ovarian cyst, your doctor will take into account factors like the size of the cyst, whether or not it has ruptured or twisted, and how far along you are in your pregnancy. They will make a treatment recommendation that will give you and your baby the healthiest outcome possible.
In some cases, surgery can be safely performed during pregnancy. Your healthcare team will tell you about the risks and possible outcomes based on your circumstances.
If your pain is caused by an ectopic pregnancy, your doctor will likely prescribe the medication methotrexate. This drug can stop the growth of rapidly dividing cells, such as the cells of the ectopic mass. If medication doesn’t work, surgery may be necessary.
If you are having a miscarriage, you may be able to pass the pregnancy at home. In other cases, you may need medication to help you pass the tissue from the pregnancy loss or you may need a procedure known as dilation and curettage (D and C). D and C is a minor surgery that can be used to remove the tissue from the lost pregnancy.
Always let your doctor know if you are experiencing ovarian pain during pregnancy.
Seek emergency medical care for sharp or stabbing pain that doesn’t go away on its own, and let the hospital staff know you are pregnant. Your doctor and healthcare team can come up with a treatment plan for the healthiest outcome.
Your doctor and healthcare team can come up with a treatment plan for the healthiest outcome.
Pelvic pain in early pregnancy | Symptoms
Ectopic pregnancy
Signs: Abdominal or pelvic pain that is often sudden and persistent (not crampy), localized, and may or may not be accompanied by vaginal bleeding. If an ectopic pregnancy is terminated, fainting, dizziness, or palpitations may occur.
Miscarriage (threatened miscarriage or ongoing spontaneous abortion)
Signs: Spasmodic pain in the pelvic area, often radiating to the abdominal cavity. Often vaginal bleeding, sometimes with the release of fragments of fetal tissue.
Septic abortion (infection of the contents of the uterus before, during or after a miscarriage)
Signs: Usually in women who have already had an abortion (usually performed by an inexperienced doctor or by the women themselves). Fever and chills, persistent abdominal or pelvic pain, and pus-filled vaginal discharge.
Normal changes during pregnancy (includes distension and growth of the uterus in early pregnancy)
Signs: Cramping or burning sensation in the lower abdomen, pelvis and/or lower back.
Uterine fibroma degeneration
Signs: Pelvic pain that starts suddenly and is usually accompanied by nausea, vomiting, and fever. Sometimes vaginal bleeding.
Torsion (twisting) of the epididymis
Signs: Pain in the pelvic area that starts suddenly, may be with colic, which is often mild if the ovary uncoils on its own, often with nausea or vomiting.
Rupture of the corpus luteum cyst (forms in the ovary from which the egg is released after ovulation)
Signs: Abdominal or pelvic pain that originates in a specific area, sometimes resembling pain due to ovarian torsion;
usually occurs suddenly. Vaginal bleeding.
Pelvic inflammatory disease
Signs: Pain in the pelvic area that lasts a long time, usually develops gradually, as a rule, is felt on both sides.
Vaginal discharge containing pus. Sometimes fever or chills. It is more common in women who have sex with new partners and do not use condoms or diaphragms.
Appendicitis
Signs: As a rule, continuous pain and tenderness in the lower abdomen on the right. There may be pain in a different place (higher in the abdomen) or a different nature of pain (weaker and more crampy) compared to non-pregnant women.
Urinary tract infections
Signs: Discomfort that is felt just above the pubic bone. Often burning during urination, frequent urge to urinate, and the need to urinate immediately. Sometimes blood in the urine.
Inflammatory bowel disease (Crohn's disease, ulcerative colitis)
Signs: Pain, which may be spasmodic or continuous, may occur in multiple locations. Often diarrhea, sometimes with mucus or blood. As a rule, in women who have already been diagnosed with this disease.
Intestinal obstruction (intestinal obstruction)
Signs: Spasmodic pain that recurs periodically, vomiting. Lack of bowel movements or gas (flatulence), bloating. As a rule, in women who have undergone surgery in the abdominal cavity.
Lack of bowel movements or gas (flatulence), bloating. As a rule, in women who have undergone surgery in the abdominal cavity.
Gastroenteritis
Signs: Usually vomiting and diarrhea.
Pain in the pubic region during pregnancy
Subscribe to our Instagram! Useful information about pregnancy and childbirth from leading obstetrician-gynecologists in Moscow and foreign experts: https://www.instagram.com/roddompravda/
Advice and opinions from leading children's specialists: https://www.instagram.com/emc.child/
The pubic bone is one of the three bones that make up the pelvic bone. Two pubic bones, forming the pubic articulation (symphysis), form the anterior wall of the pelvis. The pubic bone in women with a regular physique has the form of a roller about the thickness of the thumb, which is curved and forms a pubic eminence. This bone hangs in a kind of arch over the entrance to the vagina.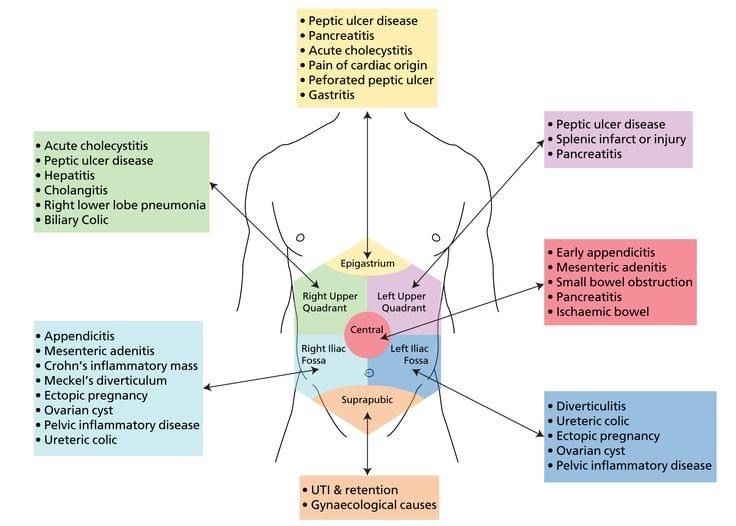
The main cause of pain in the pubic bone is the divergence and increased mobility of the pubic symphysis. To refer to pathological changes in the pubic symphysis of the pelvis during pregnancy and after childbirth, the following terms are used: symphysiopathy, symphysitis, arthropathy of pregnant women, divergence and rupture of the pubic symphysis, dysfunction of the pubic symphysis. The most commonly used terms are "symphysitis" or "symphysiopathy".
So, symphysiopathy is a disease associated with a pronounced softening of the pubic joint under the influence of the hormone relaxin, which is produced during pregnancy. The process of softening the interosseous joints is natural, it helps the child to pass more easily through the bone pelvis during childbirth. The diagnosis of "symphysiopathy" is made when severe pain appears, the pubic joint swells, greatly stretches, becomes mobile, and the pubic bones diverge excessively. One of the striking, characteristic symptoms of this pathology is that it is impossible to raise the leg in the prone position.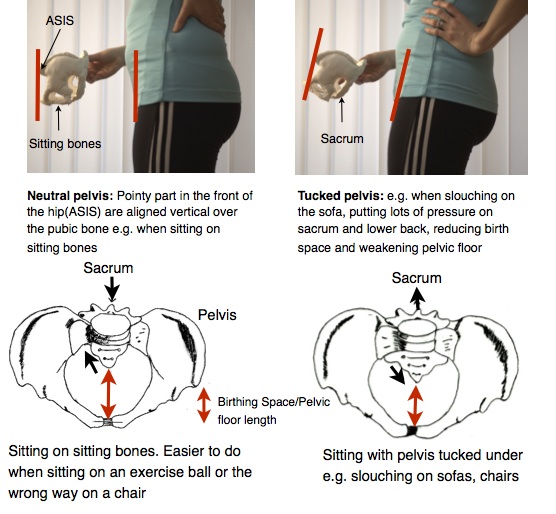 In addition to acute pain in the pubis, there are difficulties when walking up the stairs, it becomes difficult to turn from side to side on the bed and get up from the sofa, and the gait changes and becomes like a "duck". According to most doctors, the cause of symphysiopathy is a lack of calcium, an increased concentration of the hormone relaxin, and increased physical activity on the bones of the pelvic region. In addition, the development of symphysiopathy can be provoked by a serious sports injury or a fracture of the pelvic bones.
In addition to acute pain in the pubis, there are difficulties when walking up the stairs, it becomes difficult to turn from side to side on the bed and get up from the sofa, and the gait changes and becomes like a "duck". According to most doctors, the cause of symphysiopathy is a lack of calcium, an increased concentration of the hormone relaxin, and increased physical activity on the bones of the pelvic region. In addition, the development of symphysiopathy can be provoked by a serious sports injury or a fracture of the pelvic bones.
At what stage of pregnancy do they occur?
The disease begins gradually or suddenly during pregnancy, childbirth or after childbirth. Most often, women begin to feel pain in the area of the pubic joint in the third trimester of pregnancy. This is due to the fact that the places of adhesions of the pubic bones, their ligaments and cartilage, soften under the influence of the hormone relaxin. This hormone of pregnancy naturally softens the bony joints, which is necessary to facilitate the passage of the child's bone pelvis and birth canal at the time of childbirth.
Some women begin to complain of pain in the pelvic bones some time after giving birth. This may be the result of traumatic childbirth (imposition of obstetrical forceps, shoulder dystocia, excessive separation of the hips during childbirth, etc.) or physical exertion (lifting a heavy baby stroller up the stairs, prolonged motion sickness in the arms of a well-fed baby, etc.). It is recommended to limit physical activity, wear an orthopedic bandage, consult a traumatologist. Complaints usually recur after the next pregnancy. In a small proportion of patients, pain persists for a long time.
When can this be considered the norm, and when not?
Obstetricians-gynecologists do not consider a slight soreness of the pubic joint to be a pathology, but if the pain is acute, restricting the movements of the pregnant woman, accompanied by edema, then we can talk about pathology. Pain can be quite strong and especially manifest itself while walking, turning the body to the right and left in a sitting position and even lying down.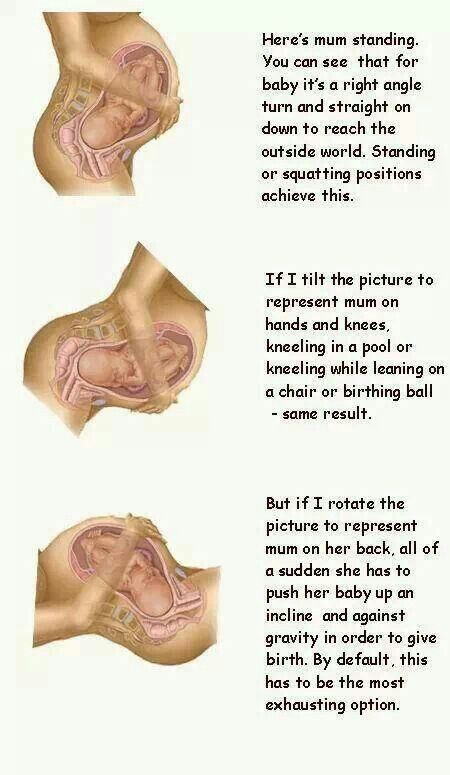 In this case, you need to urgently consult a doctor and undergo an ultrasound diagnosis (ultrasound) to determine the size of the divergence of the pubic bones. Magnetic resonance imaging (MRI) is also used, which allows assessing the state of the symphysis, the state of the bone tissue, as well as soft tissues.
In this case, you need to urgently consult a doctor and undergo an ultrasound diagnosis (ultrasound) to determine the size of the divergence of the pubic bones. Magnetic resonance imaging (MRI) is also used, which allows assessing the state of the symphysis, the state of the bone tissue, as well as soft tissues.
With ultrasound, the degree of divergence (diastasis) of the pubic bones is determined. The severity of the clinical picture largely depends on the degree of divergence of the pubic bones, and therefore there are three degrees of divergence of the pubic branches: in the first degree - by 6-9 mm, in the second - by 10-20 mm, in the third - more than 20 mm. The severity of the symptoms of the disease varies from mild discomfort to unbearable pain.
How can pain be relieved?
There are some recommendations that will help reduce bone pain during pregnancy, if the cause of its occurrence is the divergence of the pubic bones. Be sure to wear a bandage, especially in later pregnancy.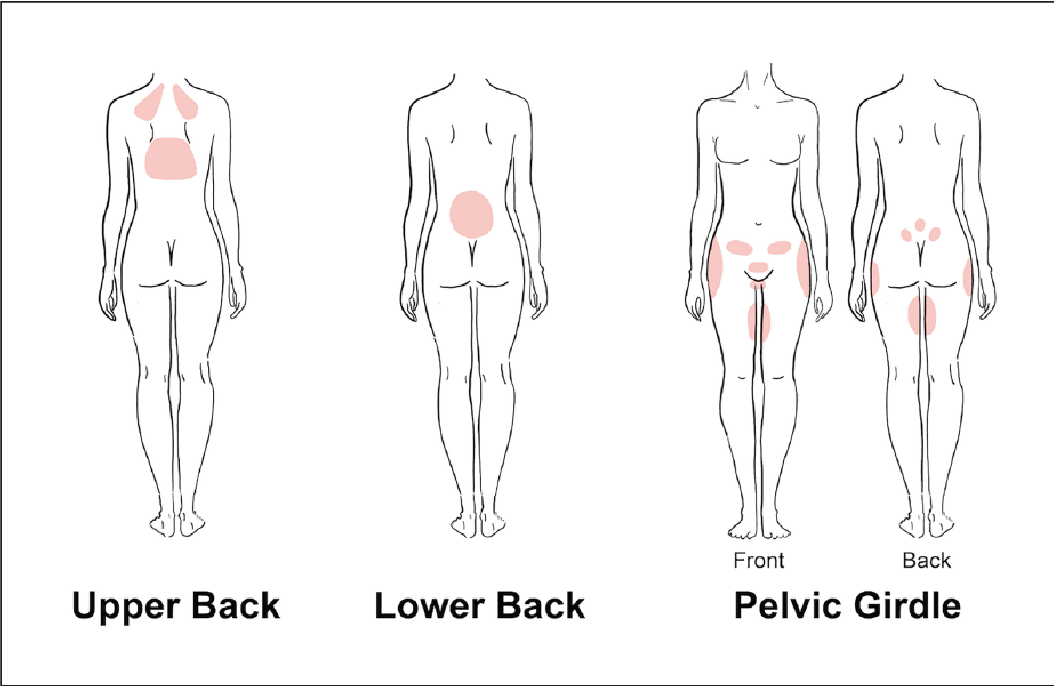 The bandage takes on most of the load, thereby releasing pressure from the pubic joint. Limitation of heavy physical exertion is indicated for any manifestations of pain, lying down more often, walking less and being in a sitting position for no longer than 30-40 minutes. In severe cases, before and sometimes after childbirth, a woman may be shown strict bed rest. Moreover, the bed should not be hard and flat.
The bandage takes on most of the load, thereby releasing pressure from the pubic joint. Limitation of heavy physical exertion is indicated for any manifestations of pain, lying down more often, walking less and being in a sitting position for no longer than 30-40 minutes. In severe cases, before and sometimes after childbirth, a woman may be shown strict bed rest. Moreover, the bed should not be hard and flat.
Since the appearance of symphysiopathy is associated not only with a large production of the hormone relaxin, but also with a lack of calcium in the body, the expectant mother is prescribed calcium preparations and complex vitamins for pregnant women, which contain all the necessary vitamins and trace elements in the right amount and proportions. There is evidence that pain is reduced during acupuncture and physiotherapy.
In especially severe cases of symphysiopathy, the pregnant woman is hospitalized.
What is the danger of this condition?
The occurrence of symphysiopathy is due to several reasons. This is a lack of calcium in the body of the future mother, and an excess amount of the hormone relaxin, and the individual structural features of the woman's body, and possible hereditary or acquired problems of the musculoskeletal system.
This is a lack of calcium in the body of the future mother, and an excess amount of the hormone relaxin, and the individual structural features of the woman's body, and possible hereditary or acquired problems of the musculoskeletal system.
With an unexpressed clinical picture of the disease, with an expansion of the pubic fissure up to 10 mm, normal pelvic sizes, a small fetus, childbirth can be carried out through the birth canal, avoiding the use of physical force, such as the Christeller maneuver. With a pronounced stretching of the pubic symphysis, pain syndrome, especially with anatomical narrowing of the pelvis, a large fetus, there is a danger of rupture of the pubic symphysis, and the method of choice in this case is caesarean section. This is due to the fact that during natural delivery, the bones can disperse even more and the woman subsequently will not be able to walk at all.
Prevention
The body of a healthy woman is able to independently cope with all the difficulties of the pregnancy period.