Pcos natural pregnancy
How to Get Pregnant with PCOS
Polycystic ovary syndrome, or PCOS, is a hormonal condition that tampers with more than just your fertility, but you might first receive a diagnosis when you’re trying to get pregnant. This is because it’s a common — and treatable — cause of infertility in women.
According to the Centers for Disease Control (CDC), up to 12 percent of women in the United States have difficulty getting pregnant because of untreated PCOS. In reality, this number might be bigger because almost 50 percent of women with this syndrome don’t know they have it or are not diagnosed correctly.
Having PCOS doesn’t mean you can’t get pregnant. It just might be a bit trickier and you may need extra help. There is plenty that you can do at home and with medical treatment to keep PCOS symptoms at bay and raise your chances for a healthy pregnancy.
Getting pregnant with PCOS involves some of the same steps that women without PCOS should take for a healthy pregnancy.
- Have your weight and body mass index (BMI) measured by your doctor. Your BMI shows whether you have a healthy body weight and how much of your body composition is fat. If you are carrying extra weight, talk to your doctor about how much weight you need to lose before you get pregnant.
- Start a healthy diet and exercise plan. Get into the habit of choosing healthier food choices and being more active.
- Use an ovulation calendar or app to track when you have your period. This helps you make a better guess about which days of the month you are more likely to get pregnant.
- Check your blood sugar levels. See your doctor to make sure your blood sugar levels are balanced. Your blood sugar levels are important in getting pregnant, having a healthy pregnancy, and even in your baby’s future health.
Being overweight has been linked to PCOS, but many women who have this condition are not overweight at all. Still, if you are carrying extra weight, you may improve your fertility and reduce other PCOS symptoms by losing just 5 percent of your weight.
Still, if you are carrying extra weight, you may improve your fertility and reduce other PCOS symptoms by losing just 5 percent of your weight.
Exercise daily by going for a walk and getting in your steps. Use a standing desk rather than sitting down while you’re working. Lift light weights while watching TV as building more muscle helps bring down PCOS symptoms and improves your health.
Any woman who is trying to get pregnant needs to have the right levels of nutrients. Switch out sugary foods, simple carbs, and unhealthy fats for healthier choices, including:
- fresh and cooked fruit and vegetables
- whole grains like brown rice, oats, and barley
- beans and lentils
- chicken
- fish
Certain vitamins and minerals are important for a healthy pregnancy and a growing baby. Ask your doctor about the best supplements for you. Supplements that may help fertility include:
- folic acid (vitamin B9)
- vitamin B6
- vitamin B12
- vitamin C
- vitamin D
- vitamin E
- coenzyme Q10
Your doctor will test your blood sugar levels if you’re having trouble getting pregnant. PCOS sometimes leads to high blood sugar levels or type 2 diabetes. This may cause fertility problems.
PCOS sometimes leads to high blood sugar levels or type 2 diabetes. This may cause fertility problems.
This happens because PCOS may change how your body uses insulin. This important hormone moves sugar (glucose) out of the blood and into the muscles and cells where it is burned for energy. PCOS makes your body less sensitive to insulin — making it harder for it to do its job.
Balancing your blood sugar levels may help you get pregnant. Eat a healthy diet with more fiber, protein, and healthy fats. Getting plenty of daily exercise and strength training can also help your body use insulin better.
In some cases, your doctor might recommend medications to help balance your blood sugar levels. A common type 2 diabetes drug called metformin (or Glucophage) makes your body use insulin better to help lower high blood sugar. This can also help you get pregnant with PCOS.
You might need to take metformin in low doses and only temporarily, depending on your blood sugar levels. For best results, eat a healthy diet and exercise regularly along with taking any prescribed medications to help you get pregnant.
For best results, eat a healthy diet and exercise regularly along with taking any prescribed medications to help you get pregnant.
If you have high blood sugar levels or type 2 diabetes, it’s important to check your blood sugar levels with a home monitor every day.
Your doctor will check your blood sugar levels with tests, including:
- random blood sugar test
- overnight fasting blood sugar test
- oral glucose tolerance tests (after fasting and drinking a sugary drink)
- hemoglobin A1C test (checks your blood sugar levels for the last two to three months)
If you have PCOS your body might make more of both the male hormone testosterone and the female hormone estrogen. Too much (or too little) of these hormones can make it tricky to get pregnant. Your doctor might recommend prescription medications to help balance your hormones.
Medications to help you get pregnant with PCOS include:
- metformin to balance insulin levels
- clomiphene citrate (or Clomid) to help balance estrogen levels
- birth control pills to balance estrogen and testosterone levels (before beginning fertility treatment)
- fertility medications to jump-start the ovaries to send out more eggs
You may need in vitro fertilization (IVF) treatment to help you get pregnant with PCOS. Your fertility doctor will give you a checkup that may include more blood tests, ultrasounds scans, and a physical exam.
Your fertility doctor will give you a checkup that may include more blood tests, ultrasounds scans, and a physical exam.
IVF is a process that can take months or even years whether you have PCOS or not. However, medical research shows that women with PCOS have a high success rate of getting pregnant with IVF treatment.
Some clinical studies found that women with PCOS who took birth control pills before the IVF treatment had better results. You may also need other mediations to help balance hormones and get your body ready for the IVF treatment.
For all women, the first step in IVF treatment is to eat a balanced diet and get plenty of exercise to reach a healthy weight. Women with PCOS who are a healthy weight are twice as likely to get pregnant with IVF than women with PCOS who are obese.
Before exploring IVF, your doctor might suggest a less-costly alternative called intrauterine insemination (IUI). This process increases the chance of pregnancy because it directly injects a high concentration of sperm closer to the egg.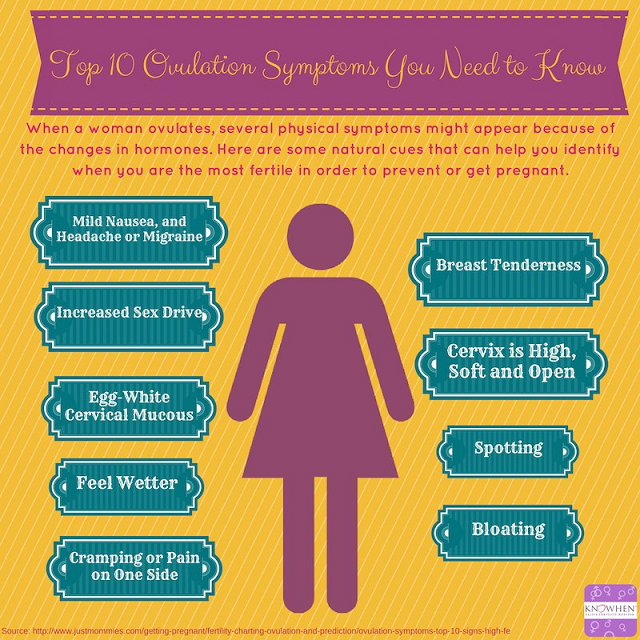
PCOS may make it harder to get pregnant because it can impact your menstruation cycle (your monthly period). Symptoms include:
- too few menstrual periods
- having your period for longer than usual
- not getting your period
- very heavy periods
- higher levels of male hormones like testosterone
- acne breakouts
- getting facial hair and extra hair in other places
- small cysts or bundles of fluid in the ovaries
- fewer eggs released from the ovaries
If you don’t get treated for PCOS, it also raises your risk for other health conditions, like:
- type 2 diabetes
- sleep apnea (snoring)
- heart disease
- high blood pressure
- high cholesterol
- stroke
No one knows why some women get PCOS. Nothing you did — or didn’t do— caused you to have this condition. But getting an early diagnosis and treatment along with making other lifestyle changes may help you get pregnant and prevent health complications from PCOS.
If you are trying to get pregnant with PCOS, you may only need treatment with medications. A medical study found that almost 80 percent of women with PCOS treated with the drug clomiphene citrate successfully ovulated. Out of these, half of the women got pregnant naturally within six period cycles.
If medications don’t help you get pregnant, your doctor may recommend IVF treatments. Most women with PCOS have a 20 to 40 percent chance of getting pregnant with IVF treatment. Women who are 35 years old and older or who are overweight have a lower chance of getting pregnant.
You can get pregnant with PCOS. You will likely need to have moderate weight, balance your blood sugar levels, and treat other PCOS symptoms with healthy lifestyle changes and medications.
In some cases, fertility medications alone will help you get pregnant. If that doesn’t work, you may need IVF treatment.
But regardless of what treatment you explore, don’t lose hope. Success rates are optimistic. In time you may be smiling, positive pregnancy test in hand.
In time you may be smiling, positive pregnancy test in hand.
11 Tips That Actually Work
This post was updated on October 12th, 2022
By Kym Campbell, BSc. | Updated October 12th, 2022
Medically Reviewed by Dr. Sarah Lee, M.D & Dr. Jessica A McCoy, Ph.D
Polycystic ovary syndrome or PCOS is one of the most common causes of female infertility.
PCOS impairs ovulation [1, 2], reduces egg quality [3, 4], and makes the womb less receptive during implantation [5, 6]. Women with PCOS also tend to experience higher rates of miscarriage as a result of this syndrome [7].
Yet despite these disadvantages, you can still get pregnant with PCOS. It just requires a little more work.
I’ve done it, and so have thousands of other women, after completing my free 30-Day PCOS Diet Challenge.
If you want to get pregnant with PCOS, then here are 11 tips that help. The interventions covered range from simple dietary changes to advanced reproductive technology.
1. Measure Your Metabolic Health
No one should ever feel ashamed of their weight. But the harsh reality is that both obesity and insulin resistance reduce fertility in women with PCOS [8-10]. Because of this, your metabolic health can tell you a lot about your reproductive potential.
Obesity has many negative effects on reproductive processes. This includes reduced egg quality [11], disrupted embryo development, and impaired receptivity of the uterus [12]. For overweight women with PCOS, reducing body fat is one of the best ways to improve fertility and pregnancy outcomes [13]. Even modest weight loss of 5-10% can help [14-17] (see how to lose weight with PCOS here).
Insulin resistance is one of the primary causes of both weight gain and infertility in women with PCOS [18, 19]. This means that it can tell us a lot about our reproductive health. Physicians will often use fasting plasma glucose and A1C as indicators of insulin sensitivity. For women wanting to conceive, changes to these biomarkers can be monitored for progress over time.
Overweight women are often insulin resistant. But this diagnosis is often missed in normal-weight women with PCOS. Excess stomach fat is a common sign of insulin resistance in otherwise lean women. Having a waist-to-hip ratio higher than 0.85 is also used to assess this problem.
Hanna is a textbook case study of a lean woman with PCOS. She once suffered from insulin resistance and infertility. After realizing she had insulin resistance, Hanna made significant changes to her diet and lifestyle. By doing so, she was able to fall pregnant within a few months.
This was also my own experience after transforming my diet. Following over four years of failed fertility treatments, I was able to regulate my cycle and fall pregnant naturally.
2. Eat a PCOS-Friendly Diet
Scientists say that an unhealthy diet forms part of a “deadly quartet” of PCOS risk factors [20]. Together with insulin resistance, elevated androgen levels, and low-grade inflammation, high carbohydrate consumption contributes to infertility and poor metabolic health.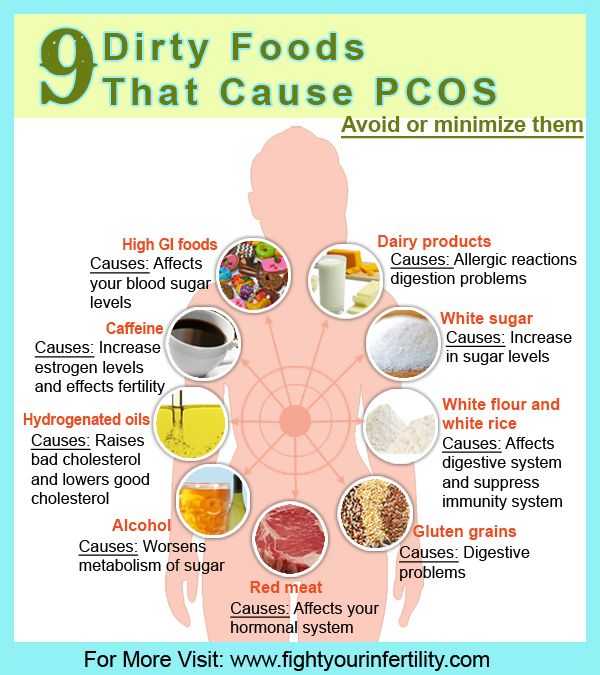
This is why a PCOS diet is one of the best fertility treatments. Dietary changes are often all that’s required to achieve a healthy, successful pregnancy. This is especially true if you’re overweight or insulin resistant. By improving insulin sensitivity and reducing inflammation, the right diet resolves both of these fertility-reducing factors. This can also improve other PCOS symptoms like unwanted hair, acne, anxiety, and depression. The best thing about eating for fertility though is that you can do it alongside any other treatment.
This was certainly Jamie’s experience. After participating in my free 30-Day PCOS Diet Challenge, Jamie lost weight, regulated her cycle, and soon fell pregnant.
If you want to test things out before making a 30-day commitment, this free 3-Day Meal Plan is a great place to start.
3. Consider Supplements
Certain minerals and vitamins can help with fertility. As explained in my article Vitamin D for PCOS, vitamin D supplementation is often warranted in women with PCOS. Vitamin D status impacts both fertility and pregnancy through a range of mechanisms [51-56]. Women with PCOS are also more likely to be deficient in this important nutrient. Methylated folate and iron are also among the most important supplements when trying to conceive.
Vitamin D status impacts both fertility and pregnancy through a range of mechanisms [51-56]. Women with PCOS are also more likely to be deficient in this important nutrient. Methylated folate and iron are also among the most important supplements when trying to conceive.
Others worth considering include:
- Vitamins A, C, E, and K
- Various B vitamins, especially B6 and B12
- Calcium, iodine, magnesium, zinc, selenium, copper, and chromium
Prenatal vitamins aside, when it comes to fertility, myo-inositol is one of the most promising candidates for women with PCOS. This natural, vitamin-like sugar has a notable effect on fertility.
For women with PCOS, myo-inositol has been shown to improve ovarian function [21] and egg quality [22, 23]. During IVF trials, myo-inositol has increased the yield of mature eggs [24]. It’s improved pregnancy rates [25, 26], and reduced the risk of ovarian hyperstimulation syndrome [23]. Other studies have found that myo-inositol may be more effective than birth control at regulating ovarian function [27]. It may also be better than metformin for boosting pregnancy rates [28].
It may also be better than metformin for boosting pregnancy rates [28].
Learn more about inositol for PCOS and fertility here.
4. Exercise Regularly
You might know it already, but there’s strong scientific evidence showing that exercise is good for fertility. In overweight women with PCOS, exercise can lead to the resumption of ovulation [29]. This effect is independent of changes to your diet. Improvements in insulin sensitivity are the pivotal factor. The mechanism is different though from that which comes about through diet [30].
Both resistance (strength) training and aerobic activity are effective PCOS treatments [31-33]. This suggests that almost any kind of exercise is likely to be good for improving fertility.
5. Manage Your Stress
While it’s a cliché, stress can indeed play a significant role in preventing pregnancy in women with PCOS.
Studies have shown that women with PCOS produce unusually high levels of cortisol when stressed [34]. his reduces our capacity to cope. It also promotes insulin resistance and causes fat to accumulate on our stomachs and thighs [35, 36].
his reduces our capacity to cope. It also promotes insulin resistance and causes fat to accumulate on our stomachs and thighs [35, 36].
In a first-of-its-kind trial, US researchers found a two-fold increased risk of infertility in women that had the highest stress levels compared to those who were the least stressed [37]. This was a high-quality analysis that controlled for many confounding factors. This included age, race, income, alcohol, caffeine, and cigarette use.
Mindfulness meditation is one of the best direct stress-management tools. Similar practices like guided relaxation exercises and cognitive behavioral therapy are also helpful. Physical activity is another powerful way to reduce anxiousness [38].
Other, less direct stress management practices can help too. Referred to as “self-care” (for want of a better term), anything that helps you relax or let go of your stress, can have a small but real effect.
6. Track Your Cycle
Getting pregnant is all about timing which is why tracking your menstrual cycle is so important. By monitoring changes in your basal body temperature and cervical mucus, you can know when you’re at your most fertile. Ovulation predictor kits can also be a valuable addition to your preconception toolkit.
By monitoring changes in your basal body temperature and cervical mucus, you can know when you’re at your most fertile. Ovulation predictor kits can also be a valuable addition to your preconception toolkit.
Cycle tracking can be difficult for women with PCOS because they have irregular periods or they don’t ovulate. But a PCOS diet and other positive lifestyle changes can overcome these issues. Once a more regular period is achieved, ovulation becomes a lot more predictable.
7. Get Medical Help When Needed
For young women with PCOS, diet and lifestyle changes are often all that is needed to restart ovulation. But these natural treatments can take between a couple of months to more than a year to work. If time is of the essence, then seeking fertility treatment may be warranted.
Besides male factor infertility, for women with PCOS, age is the key variable when deciding to advance to fertility treatments.
As the figure below shows, egg quality peaks in your late twenties, and then declines rapidly after your mid-thirties. This has a direct effect on your chances of getting pregnant.
This has a direct effect on your chances of getting pregnant.
Figure 1. Percentage of embryos produced by women that have the correct number of chromosomes i.e. “good quality” eggs [39].
What this means for our “natural” fertility is that for the average woman, things start to get difficult once you hit 40.
Knowing that fertility treatments can also take time, it’s important to consider how long you’ll try on your own, before seeking help.
As you enter your mid to late 40s, using donor eggs will greatly improve your chances of success. For younger women though, this shouldn’t be needed unless surgical treatments of PCOS have reduced ovarian reserves [50].
Figure 2. Changes in relative “natural” fertility rates with age from historical population data [40].
8. Skip Metformin & Birth Control
When seeking fertility treatment, it’s just as important to know what not to do, as it is to know which treatments are best. Metformin is a great example of this.
Metformin is a great example of this.
Metformin is still commonly used for infertility in women with PCOS, yet, it’s not an effective treatment. Older studies that show metformin improves menstrual frequency, ovulation, and clinical pregnancy rates. But more recent reviews of the evidence are less supportive of this approach.
A 2019 Cochrane database systematic review, challenged the idea that metformin increases live-birth rates. The strength of the effect was found to be small and the quality of the evidence was low. Gastrointestinal side effects from this medication are significant though [41].
There are simply better alternatives to metformin for fertility.
Even the Endocrine Society Clinical Practice Guidelines state that “…metformin is beneficial for improving menstrual irregularities, but it has limited or no benefit in treating hirsutism, acne, or infertility” [42].
Learn more about metformin for PCOS here.
Another outdated practice is the use of hormonal birth control as a short-term PCOS preconception treatment. The idea here is that the pill suppresses the overproduction of androgens. In theory, this should then also kick-start ovulation once discontinued.
The idea here is that the pill suppresses the overproduction of androgens. In theory, this should then also kick-start ovulation once discontinued.
The problem with this approach is that it may do more harm than good. Preconception birth control has no benefit to your chances of ovulation. It’s been shown to worsen metabolic health and may be detrimental to your fertility [43, 44]. See my PCOS birth control article for nine reasons to avoid this treatment.
9. Start with Clomid and/or Letrozole
When you need more help beyond diet and lifestyle changes, ovulation induction drugs are the obvious next step. Clomid and letrozole are the first-line therapies recommended by the World Health Organization [45]. Clomid has traditionally been the go-to first treatment. But many experts now believe that doctors should skip this step and head straight for letrozole instead. This is because letrozole has been shown to result in better outcomes for women with PCOS [46-48].
Interestingly, this recommendation may soon be further updated. A randomized control trial found that clomid and letrozole used together were better than letrozole on its own [49].
A randomized control trial found that clomid and letrozole used together were better than letrozole on its own [49].
In Karima’s case, Clomid + dietary change was the combination that worked for her. It was only after doubling down on the seven foods to avoid for PCOS that she fell pregnant on her seventh cycle.
10. Advance to Gonadotropins
If Clomid or letrozole fails to achieve pregnancy, most fertility specialists will recommend the use of injectable gonadotropin products. These are used either with timed intercourse, intrauterine insemination (IUI), or in-vitro fertilization (IVF).
Follicle-stimulating hormone (FSH), luteinizing hormone (LH), or a combination of the two, are the active ingredients in the most commonly used gonadotropin brands. This includes products such as Gonal-F, Follistim, Ovidrel, Bravelle, and Menopur. Gonadotropins can be used either on their own or in combination with oral fertility treatments like letrozole (Femara).
The biggest hazard with gonadotropins is their potential to over-stimulate the ovary. This can cause ovarian hyperstimulation syndrome (OHSS). IVF egg collection is when the most gonadotropins are used, increasing the chances of OHSS. Studies show that myo-inositol can mitigate this risk [23]. But it remains important to establish the lowest effective gonadotropin dose required.
This can cause ovarian hyperstimulation syndrome (OHSS). IVF egg collection is when the most gonadotropins are used, increasing the chances of OHSS. Studies show that myo-inositol can mitigate this risk [23]. But it remains important to establish the lowest effective gonadotropin dose required.
11. Add in IUI or IVF if Needed
Intrauterine insemination (IUI) is a type of artificial insemination that’s used to treat infertility. Sperm is first washed and concentrated. It’s then placed into the uterus with the hope that it’ll swim up into the fallopian tube to fertilize a waiting egg. This can be done with a “normal” cycle, or after ovulation induction.
IUI is a limited procedure that still relies on the sperm and egg to do a lot of the “work”. By comparison, during in-vitro fertilization (IVF), every step of the process is controlled and monitored.
IVF starts with ovulation induction. But unlike natural conception or IUI, IVF uses a lot more gonadotropins. The goal is to mature and collect 12 – 20 eggs for fertilization in the lab.
Fertilization can occur by introducing the sperm into the same petri dish as the egg. Alternatively, one lucky sperm and be injected into the egg. This process is known as intracytoplasmic sperm injection (ICSI). ICSI is an optional technology. It increases fertilization rates and helps overcome male infertility.
Once the eggs are fertilized, they’re then grown for a few days under controlled lab conditions. After they’ve matured, these fertilized embryos can be placed back into the uterus as a “fresh embryo transfer”. They can also be cryogenically preserved for later use.
Somewhat ironically, women with PCOS may have an advantage over other women when it comes to IVF. This may be because PCOS women have higher ovarian reserve than age-matched controls. This enables more embryos to be produced during IVF. This allows for more cycles which leads to better cumulative birth rates [57, 58].
In non-PCOS women, success rates go down significantly with age. But a 2011 study found that birth rates held stable between 22 and 41 years old in IVF patients with PCOS [59]. A similar study found that peak fertility was maintained until 38 years of age using IVF [60]. Others have found that PCOS women over 40 years have comparable success rates to those aged 35 to 40.
A similar study found that peak fertility was maintained until 38 years of age using IVF [60]. Others have found that PCOS women over 40 years have comparable success rates to those aged 35 to 40.
Just when you thought that it was all bad news!
The Bottom Line
Women with PCOS face a lot of extra obstacles when it comes to starting and growing their families. But that doesn’t mean you can’t get pregnant with PCOS. You just need to work harder at it.
Diet and lifestyle changes can address the underlying root causes of PCOS. If required, assisted reproductive technologies also have outstanding success rates.
Whichever path you choose to go down, if you’re trying to conceive with PCOS, make sure to include diet and lifestyle changes as a core part of your fertility plan. You can get started today with this free 3-Day Meal Plan. Or sign-up for my next free 30-Day PCOS Diet Challenge.
Ready to Take Action?
 This is a live program where you’ll receive weekly meal plans and helpful video lessons. You’ll also be part of a motivated and inspiring community of like-minded women.
This is a live program where you’ll receive weekly meal plans and helpful video lessons. You’ll also be part of a motivated and inspiring community of like-minded women.Author
Kym Campbell
Since 2010, Kym Campbell has used evidence-based diet and lifestyle interventions to manage her PCOS. After getting her symptoms under control and falling pregnant naturally, Kym now advocates for dietary change as part of any PCOS treatment plan. Combining rigorous science and clinical advice with a pragmatic approach to habit change, Kym is on a mission to show other women how to take back control of their health and fertility. Read more about Kym and her team here.
Combining rigorous science and clinical advice with a pragmatic approach to habit change, Kym is on a mission to show other women how to take back control of their health and fertility. Read more about Kym and her team here.
Co-Authors
Dr. Jessica A McCoy, Ph.D
This blog post has been critically reviewed to ensure accurate interpretation and presentation of the scientific literature by Dr. Jessica A McCoy, Ph.D. Dr McCoy has a master’s degree in cellular and molecular biology, and a doctorate in reproductive biology and environmental health. She currently serves as a University professor at the College of Charleston, South Carolina.
LinkedIn | Google Scholar | Researchgate
Dr. Sarah Lee, M.D
This blog post has also been medically reviewed and approved by Dr. Sarah Lee, M.D. Dr. Lee is a board-certified Physician practicing with Intermountain Healthcare in Utah. She obtained a Bachelor of Science in Biology from the University of Texas at Austin before earning her Doctor of Medicine from UT Health San Antonio.
Back to Top
References
1Patil, K., et al., Compromised Cumulus-Oocyte Complex Matrix Organization and Expansion in Women with PCOS. Reprod Sci, 2021.
2Chang, R.J. and H. Cook-Andersen, Disordered follicle development. Mol Cell Endocrinol, 2013. 373(1-2): p. 51-60.
3Palomba, S., J. Daolio, and G.B. La Sala, Oocyte Competence in Women with Polycystic Ovary Syndrome. Trends Endocrinol Metab, 2017. 28(3): p. 186-198.
4Patel, S.S. and B.R. Carr, Oocyte quality in adult polycystic ovary syndrome. Semin Reprod Med, 2008. 26(2): p. 196-203.
5Giudice, L.C., Endometrium in PCOS: Implantation and predisposition to endocrine CA. Best Pract Res Clin Endocrinol Metab, 2006. 20(2): p. 235-44.
6Schulte, M.M., J.H. Tsai, and K.H. Moley, Obesity and PCOS: the effect of metabolic derangements on endometrial receptivity at the time of implantation. Reprod Sci, 2015. 22(1): p. 6-14.
Reprod Sci, 2015. 22(1): p. 6-14.
7Luo, L., et al., Early miscarriage rate in lean polycystic ovary syndrome women after euploid embryo transfer – a matched-pair study. Reprod Biomed Online, 2017. 35(5): p. 576-582.
8Silvestris, E., et al., Obesity as disruptor of the female fertility. Reprod Biol Endocrinol, 2018. 16(1): p. 22.
9Al-Jefout, M., N. Alnawaiseh, and A. Al-Qtaitat, Insulin resistance and obesity among infertile women with different polycystic ovary syndrome phenotypes. Sci Rep, 2017. 7(1): p. 5339.
10He, F.F. and Y.M. Li, Role of gut microbiota in the development of insulin resistance and the mechanism underlying polycystic ovary syndrome: a review. J Ovarian Res, 2020. 13(1): p. 73.
11Snider, A.P. and J.R. Wood, Obesity induces ovarian inflammation and reduces oocyte quality. Reproduction, 2019. 158(3): p. R79-r90.
12Broughton, D. E. and K.H. Moley, Obesity and female infertility: potential mediators of obesity’s impact. Fertil Steril, 2017. 107(4): p. 840-847.
E. and K.H. Moley, Obesity and female infertility: potential mediators of obesity’s impact. Fertil Steril, 2017. 107(4): p. 840-847.
13Cena, H., L. Chiovato, and R.E. Nappi, Obesity, Polycystic Ovary Syndrome, and Infertility: A New Avenue for GLP-1 Receptor Agonists. J Clin Endocrinol Metab, 2020. 105(8): p. e2695-709.
14Thomson, R.L., et al., The effect of a hypocaloric diet with and without exercise training on body composition, cardiometabolic risk profile, and reproductive function in overweight and obese women with polycystic ovary syndrome. J Clin Endocrinol Metab, 2008. 93(9): p. 3373-80.
15Stamets, K., et al., A randomized trial of the effects of two types of short-term hypocaloric diets on weight loss in women with polycystic ovary syndrome. Fertil Steril, 2004. 81(3): p. 630-7.
16Tolino, A., et al., Evaluation of ovarian functionality after a dietary treatment in obese women with polycystic ovary syndrome. Eur J Obstet Gynecol Reprod Biol, 2005. 119(1): p. 87-93.
Eur J Obstet Gynecol Reprod Biol, 2005. 119(1): p. 87-93.
17Kuchenbecker, W.K., et al., In women with polycystic ovary syndrome and obesity, loss of intra-abdominal fat is associated with resumption of ovulation. Hum Reprod, 2011. 26(9): p. 2505-12.
18Marshall, J.C. and A. Dunaif, Should all women with PCOS be treated for insulin resistance? Fertil Steril, 2012. 97(1): p. 18-22.
19Wang, J., et al., Hyperandrogenemia and insulin resistance: The chief culprit of polycystic ovary syndrome. Life Sciences, 2019. 236.
20Barrea, L., et al., Source and amount of carbohydrate in the diet and inflammation in women with polycystic ovary syndrome. Nutr Res Rev, 2018. 31(2): p. 291-301.
21Gerli, S., et al., Randomized, double blind placebo-controlled trial: effects of myo-inositol on ovarian function and metabolic factors in women with PCOS. Eur Rev Med Pharmacol Sci, 2007. 11(5): p. 347-54.
11(5): p. 347-54.
22Ciotta, L., et al., Effects of myo-inositol supplementation on oocyte’s quality in PCOS patients: a double blind trial. Eur Rev Med Pharmacol Sci, 2011. 15(5): p. 509-14.
23Papaleo, E., et al., Myo-inositol may improve oocyte quality in intracytoplasmic sperm injection cycles. A prospective, controlled, randomized trial. Fertil Steril, 2009. 91(5): p. 1750-4.
24Garg, D. and R. Tal, Inositol Treatment and ART Outcomes in Women with PCOS. Int J Endocrinol, 2016. 2016: p. 1979654.
25Zheng, X., et al., Inositol supplement improves clinical pregnancy rate in infertile women undergoing ovulation induction for ICSI or IVF-ET. Medicine (Baltimore), 2017. 96(49): p. e8842.
26Artini, P.G., et al., Endocrine and clinical effects of myo-inositol administration in polycystic ovary syndrome. A randomized study. Gynecol Endocrinol, 2013. 29(4): p. 375-9.
27Ozay, A.C., et al., Different Effects of Myoinositol plus Folic Acid versus Combined Oral Treatment on Androgen Levels in PCOS Women. Int J Endocrinol, 2016. 2016: p. 3206872.
28Raffone, E., P. Rizzo, and V. Benedetto, Insulin sensitiser agents alone and in co-treatment with r-FSH for ovulation induction in PCOS women. Gynecol Endocrinol, 2010. 26(4): p. 275-80.
29Hakimi, O. and L.C. Cameron, Effect of Exercise on Ovulation: A Systematic Review. Sports Med, 2017. 47(8): p. 1555-1567.
30Palomba, S., et al., Structured exercise training programme versus hypocaloric hyperproteic diet in obese polycystic ovary syndrome patients with anovulatory infertility: a 24-week pilot study. Hum Reprod, 2008. 23(3): p. 642-50.
31Covington, J.D., et al., Higher circulating leukocytes in women with PCOS is reversed by aerobic exercise. Biochimie, 2016. 124: p. 27-33.
32Almenning, I. , et al., Effects of High Intensity Interval Training and Strength Training on Metabolic, Cardiovascular and Hormonal Outcomes in Women with Polycystic Ovary Syndrome: A Pilot Study. PLoS One, 2015. 10(9): p. e0138793.
, et al., Effects of High Intensity Interval Training and Strength Training on Metabolic, Cardiovascular and Hormonal Outcomes in Women with Polycystic Ovary Syndrome: A Pilot Study. PLoS One, 2015. 10(9): p. e0138793.
33Kogure, G.S., et al., Resistance Exercise Impacts Lean Muscle Mass in Women with Polycystic Ovary Syndrome. Med Sci Sports Exerc, 2016. 48(4): p. 589-98.
34Benson, S., et al., Disturbed stress responses in women with polycystic ovary syndrome. Psychoneuroendocrinology, 2009. 34(5): p. 727-35.
35Black, P.H., The inflammatory response is an integral part of the stress response: Implications for atherosclerosis, insulin resistance, type II diabetes and metabolic syndrome X. Brain Behav Immun, 2003. 17(5): p. 350-64.
36Pasquali, R., et al., The hypothalamic-pituitary-adrenal axis activity in obesity and the metabolic syndrome. Ann N Y Acad Sci, 2006. 1083: p. 111-28.
37Lynch, C. D., et al., Preconception stress increases the risk of infertility: results from a couple-based prospective cohort study–the LIFE study. Hum Reprod, 2014. 29(5): p. 1067-75.
D., et al., Preconception stress increases the risk of infertility: results from a couple-based prospective cohort study–the LIFE study. Hum Reprod, 2014. 29(5): p. 1067-75.
38Wegner, M., et al., Effects of exercise on anxiety and depression disorders: review of meta- analyses and neurobiological mechanisms. CNS Neurol Disord Drug Targets, 2014. 13(6): p. 1002-14.
39Franasiak, J.M., et al., The nature of aneuploidy with increasing age of the female partner: a review of 15,169 consecutive trophectoderm biopsies evaluated with comprehensive chromosomal screening. Fertil Steril, 2014. 101(3): p. 656-663.e1.
40Menken, J., J. Trussell, and U. Larsen, Age and infertility. Science, 1986. 233(4771): p. 1389-94.
41Sharpe, A., et al., Metformin for ovulation induction (excluding gonadotrophins) in women with polycystic ovary syndrome. Cochrane Database Syst Rev, 2019. 12(12): p. Cd013505.
42Legro, R. S., et al., Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab, 2013. 98(12): p. 4565-92.
S., et al., Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab, 2013. 98(12): p. 4565-92.
43Legro, R.S., et al., Randomized Controlled Trial of Preconception Interventions in Infertile Women With Polycystic Ovary Syndrome. J Clin Endocrinol Metab, 2015. 100(11): p. 4048-58.
44Legro, R.S., et al., Benefit of Delayed Fertility Therapy With Preconception Weight Loss Over Immediate Therapy in Obese Women With PCOS. J Clin Endocrinol Metab, 2016. 101(7): p. 2658-66.
45Balen, A.H., et al., The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update, 2016. 22(6): p. 687-708.
46Legro, R.S., et al., Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med, 2014. 371(2): p. 119-29.
119-29.
47Klement, A.H. and R.F. Casper, The use of aromatase inhibitors for ovulation induction. Curr Opin Obstet Gynecol, 2015. 27(3): p. 206-9.
48Amer, S.A., et al., Double-blind randomized controlled trial of letrozole versus clomiphene citrate in subfertile women with polycystic ovarian syndrome. Hum Reprod, 2017. 32(8): p. 1631-1638.
49Mejia, R.B., et al., A randomized controlled trial of combination letrozole and clomiphene citrate or letrozole alone for ovulation induction in women with polycystic ovary syndrome. Fertil Steril, 2019. 111(3): p. 571-578.e1.
50Al-Hussaini, T.K., et al., Premature ovarian failure/dysfunction following surgical treatment of polycystic ovarian syndrome: A case series. Middle East Fertility Society Journal, 2017. 22(3): p. 233-235.
51Moridi, I., et al., The Association between Vitamin D and Anti-Müllerian Hormone: A Systematic Review and Meta-Analysis. Nutrients, 2020. 12(6).
Nutrients, 2020. 12(6).
52Fang, F., et al., Effect of vitamin D supplementation on polycystic ovary syndrome: A systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract, 2017. 26: p. 53-60.
53Shojaei-Zarghani, S. and M. Rafraf, Resveratrol and Markers of Polycystic Ovary Syndrome: a Systematic Review of Animal and Clinical Studies. Reprod Sci, 2021.
54Chu, J., et al., Vitamin D and assisted reproductive treatment outcome: a systematic review and meta-analysis. Hum Reprod, 2018. 33(1): p. 65-80.
55Zhang, H., et al., Meta-analysis of the effect of the maternal vitamin D level on the risk of spontaneous pregnancy loss. Int J Gynaecol Obstet, 2017. 138(3): p. 242-249.
56Pilz, S., et al., The Role of Vitamin D in Fertility and during Pregnancy and Lactation: A Review of Clinical Data. Int J Environ Res Public Health, 2018. 15(10).
57Mai, Z., et al., Comparison of Cumulative Live Birth Rate Between Aged PCOS Women and Controls in IVF/ICSI Cycles. Front Endocrinol (Lausanne), 2021. 12: p. 724333.
58Tannus, S., et al., Prevalence, clinical characteristics, and reproductive outcomes of polycystic ovary syndrome in older women referred for tertiary fertility care. Arch Gynecol Obstet, 2018. 297(4): p. 1037-1042.
59Mellembakken, J.R., et al., Sustained fertility from 22 to 41 years of age in women with polycystic ovarian syndrome. Hum Reprod, 2011. 26(9): p. 2499-504.
60Hwang, Y.I., et al., Fertility of patients with polycystic ovary syndrome undergoing in vitro fertilization by age. Int J Gynaecol Obstet, 2016. 135(1): p. 91-5.
How to get pregnant with polycystic ovaries?
Polycystic disease is a common hormonal disease that affects the functioning of a woman's ovaries. The dangers of PCOS include irregular menstrual periods, excessive hair growth, acne, weight gain, and other problems. Left untreated, PCOS can even lead to infertility. In this article, we will tell you more about causes of polycystic , polycystic ovaries and pregnancy , and also give an answer to the question: “ Is it possible to give birth with polycystic ovaries? ".
Left untreated, PCOS can even lead to infertility. In this article, we will tell you more about causes of polycystic , polycystic ovaries and pregnancy , and also give an answer to the question: “ Is it possible to give birth with polycystic ovaries? ".
What is polycystic ovary syndrome?
Polycystic ovary syndrome (PCOS) is a hormonal disorder common among women of reproductive age. Women with PCOS may have menstrual irregularities and elevated levels of male hormones (androgens). Numerous small collections of fluid (follicles) may form in the ovaries, and an egg may not be released regularly. This condition should not be confused with multifollicular ovaries, because with multifollicular ovaries, ovulation and a normal menstrual cycle can persist, unlike polycystic disease.
50-75% of cases of endocrine infertility. 20-22% of marital infertility. It is detected in 5-16% of women of reproductive age. These are the figures for the diagnosis of "Polycystic Ovary".
These are the figures for the diagnosis of "Polycystic Ovary".
Symptoms of polycystic ovary syndrome
Polycystic ovary syndrome is accompanied by characteristic symptoms, upon noticing which it is necessary to seek advice from an endocrinologist or gynecologist. For some women, symptoms begin around the time of their first menstrual period. Others discover symptoms of PCOS only after they have gained a lot of weight or have problems getting pregnant. In some cases, PCOS may be asymptomatic.
The most common symptoms of PCOS:
- Irregular periods. Lack of ovulation prevents the lining of the uterus from falling off every month. Some women with PCOS have fewer than eight periods a year, or none at all.
- Severe bleeding. The lining of the uterus builds up over a longer period of time, so menstruation may be heavier than usual.
- Hair growth . More than 70 percent of women with this condition grow hair on their face and body, including on their back, abdomen, and chest.
 Excess hair growth is called hirsutism.
Excess hair growth is called hirsutism. - Acne . Male hormones can make the skin more oily than normal and cause breakouts on areas such as the face, chest, and upper back.
- Weight gain. Up to 80 percent of women with PCOS are overweight or obese.
- Male pattern baldness. The hair on the scalp becomes thinner and may fall out.
- Darkening of the skin. Dark patches of skin may develop in body folds, such as the neck, groin area, and under the breasts.
- Headaches. Hormonal changes may cause headaches in some women.
Irregular periods
Infrequent, irregular periods, long or no periods are the most common symptom of PCOS. For example, with PCOS, you may have fewer than nine periods a year, more than 35 days between periods, and abnormally heavy periods.
Hyperandrogenism
Hyperandrogenism is a disease characterized by high levels of androgens. It is more common in women than in men. Symptoms of hyperandrogenism may include acne, seborrhea (inflammation of the skin), hair loss on the scalp, increased body or facial hair, and infrequent or absent periods.
It is more common in women than in men. Symptoms of hyperandrogenism may include acne, seborrhea (inflammation of the skin), hair loss on the scalp, increased body or facial hair, and infrequent or absent periods.
Hyperandrogenism is a defining feature of women and young girls with PCOS. Polycystic disease causes a malfunction of the ovaries or adrenal glands, which leads to the production of excess androgens (male sex hormones).
Anovulation
Anovulation occurs when an egg is not released from the ovary during the menstrual cycle. The egg is essential for pregnancy. Since several hormones are involved in ovulation, there are many causes of anovulation, one of which is PCOS. Chronic anovulation is a common cause of infertility.
Diagnosis
There is no test to definitively diagnose polycystic ovary syndrome (PCOS). The doctor will likely begin by discussing your medical history, including menstrual periods and weight changes. A physical exam will include checking for signs of excessive hair growth, acne, and weight gain.
Your doctor may recommend:
- Gynecological examination. A physician visually and manually examines the reproductive organs for growths or other abnormalities.
- Blood tests. A blood test is given to determine the level of hormones. This will help rule out possible causes of menstrual irregularities or excess androgens that mimic PCOS. An additional blood test may also be needed to measure insulin resistance as well as fasting cholesterol and triglyceride levels.
- Ultrasound examination (ultrasound). The doctor will check the appearance of the ovaries and the thickness of the lining of the uterus. A rod-shaped device (sensor) (transvaginal ultrasound) is inserted into the vagina, which emits sound waves and converts them into images on a computer screen.
Is it possible to get pregnant with PCOS
How to get pregnant with PCOS? Getting pregnant with PCOS can be difficult, but that doesn't mean it's impossible.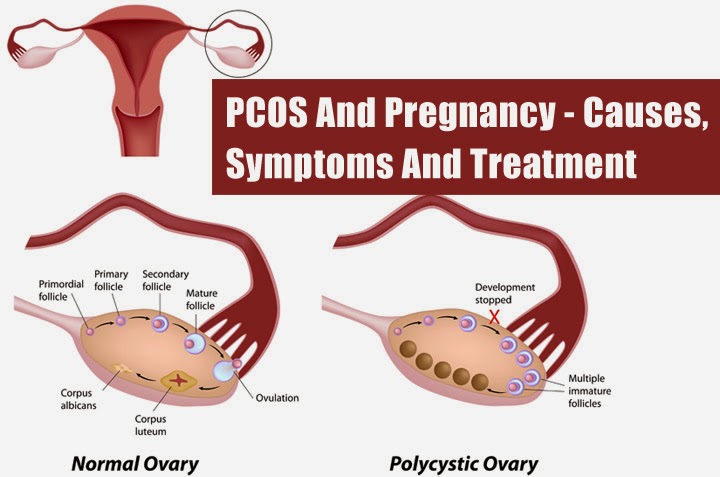 While PCOS can affect your hormones and therefore your fertility, there are medical treatments and lifestyle changes you can make to improve your chances of pregnancy.
While PCOS can affect your hormones and therefore your fertility, there are medical treatments and lifestyle changes you can make to improve your chances of pregnancy.
Is it possible to get pregnant with polycystic ovaries? To get pregnant, you must ovulate, which PCOS most often prevents. Women who do not ovulate regularly with PCOS do not release enough eggs for fertilization. Pregnancy with PCOS is further complicated by the fact that PCOS causes a hormonal imbalance that changes the quality of cervical fluid, making it difficult for sperm to survive.
It is impossible to say categorically that PCOS is infertility, but PCOS is one of the main causes of infertility in women.
Is it possible to get pregnant with PCOS? And although there are no exact statistics on the chances of pregnancy, 70 to 80 percent of women with PCOS have fertility problems. PCOS disrupts the normal menstrual cycle and makes it difficult to conceive.
Is it possible to get pregnant with PCOS? Polycystic ovary syndrome is not a sentence and it is possible to get pregnant, albeit problematic. However, if PCOS is left untreated, the chances of getting pregnant decrease with age.
However, if PCOS is left untreated, the chances of getting pregnant decrease with age.
It is possible to get pregnant with polycystic disease, but most often pregnancy with polycystic disease is difficult. This condition can increase the risk of pregnancy complications. Women with PCOS are twice as likely to have a preterm birth than women without. They are also at greater risk of miscarriage, high blood pressure, and gestational diabetes. However, by managing the symptoms, many women with PCOS can become pregnant and have a healthy baby.
How to get pregnant with PCOS? Women with PCOS can become pregnant using fertility treatments that improve ovulation. Losing weight and lowering your blood sugar can increase your chances of a healthy pregnancy.
Pregnancy planning for PCOS
How to get pregnant with PCOS? While your chances of getting pregnant with PCOS may be lower, there are a few things you can do to increase those chances.
- Call your doctor.
 How to get pregnant with polycystic ovaries? Normalization of hormones and menstruation is the first step. Your doctor may prescribe medications to help your body deal with insulin better and regulate your menstrual cycle.
How to get pregnant with polycystic ovaries? Normalization of hormones and menstruation is the first step. Your doctor may prescribe medications to help your body deal with insulin better and regulate your menstrual cycle. - Maintain a healthy weight. Is it possible to get pregnant with PCOS? Weight loss can lower insulin levels, androgen levels, and restore ovulation. Ask your doctor about a weight management program and meet with a nutritionist regularly for help with your weight loss goals.
- Eat right. Polycystic Ovarian Diet includes sugary foods, simple carbohydrates and unhealthy fats. Add to your menu: fresh and cooked fruits and vegetables, whole grains such as brown rice, oats and barley, beans and lentils, chicken, fish.
- Be active. Exercise helps lower blood sugar levels. How to get pregnant with insulin resistance? If you have PCOS, increasing daily activity such as walking, exercising, walking can help treat or even prevent insulin resistance, control your weight, and avoid developing diabetes.

- Lead a healthy lifestyle. Follow a healthy lifestyle with PCOS, give up bad habits, unhealthy diet, lack of sports and irregular sleep.
Treatment for PCOS
Treatment for PCOS focuses on your individual problems such as infertility, acne or obesity. Also, the direction of PCOS treatment largely depends on whether a woman is planning a pregnancy or not. Specific treatment may include lifestyle changes or medications.
How to treat PCOS?
Lifestyle changes
Your doctor may recommend weight loss through a low-calorie diet combined with moderate exercise. Even small weight loss - like losing 5 percent of your body weight - can improve your condition. Can you get pregnant with PCOS? Losing weight can also increase the effectiveness of medications your doctor recommends to treat PCOS and help with infertility.
Treatment with drugs for polycystic ovaries
To regulate the menstrual cycle, the doctor may recommend:
Combination birth control pills. Estrogen and progestin tablets reduce androgen production and regulate estrogen. Hormone regulation can reduce the risk of endometrial cancer and correct abnormal bleeding, excess hair growth, and acne. Instead of pills, you can use a skin patch or vaginal ring containing a combination of estrogen and progestin.
Estrogen and progestin tablets reduce androgen production and regulate estrogen. Hormone regulation can reduce the risk of endometrial cancer and correct abnormal bleeding, excess hair growth, and acne. Instead of pills, you can use a skin patch or vaginal ring containing a combination of estrogen and progestin.
Progestin therapy. Daily progestin may: restore normal hormonal balance, regulate ovulation, stop excessive hair growth, protect against endometrial cancer, and help get pregnant with sleep deprivation.
How to induce ovulation in PCOS? To help induce ovulation in PCOS, your doctor may recommend:
Clomiphene is a fertility medication that can help women with PCOS get pregnant.
Metformin is a drug used to treat type 2 diabetes. It also treats PCOS by increasing insulin levels.
Operation
How to get pregnant with PCOS? Surgery may be an option to improve fertility if other treatments don't work. Ovarian drilling is a procedure in which tiny holes are made in the ovary using a laser or a thin, heated needle to restore normal ovulation and the possibility of pregnancy with PCOS.
Ovarian drilling is a procedure in which tiny holes are made in the ovary using a laser or a thin, heated needle to restore normal ovulation and the possibility of pregnancy with PCOS.
Important! To determine the right treatment and choose the right drug, you need to consult a doctor!
Help Doc.ua: you can make an appointment with a gynecologist-endocrinologist on the website.
Polycystic ovary syndrome and infertility
What is polycystic ovary syndrome?
- Polycystic ovary syndrome (PCOS) is the most common cause of anovulation and female infertility
- Sometimes the state of anovulation is determined by polycystic or multifollicular ovaries
Women with polycystic ovaries:
- do not ovulate regularly
- have ovaries containing a large number of small antral follicles from 2-9 mm in diameter
How does normal ovulation occur?
- In a normal menstrual cycle, a mature (dominant) follicle grows.
 The size of a mature follicle ready for ovulation reaches 18-22 mm in diameter
The size of a mature follicle ready for ovulation reaches 18-22 mm in diameter - Approximately 14 days after ovulation, a woman gets her period if she is not pregnant
- The difference between polycystic and normal ovaries is that, despite the presence of many small antral follicles with eggs in them, the proper development and maturation of the follicles does not occur and ovulation is absent
- If a woman with polycystic ovaries does not ovulate regularly, she does not have regular periods
Symptoms of polycystic ovary syndrome
- Irregular menstrual cycle (oligomenorrhea), sometimes absence of periods (amenorrhea)
- Hirsutism - excessive male-pattern hair growth beginning in adolescence or around 20 years of age
- Elevated levels of male sex hormones, LH (luteonizing hormone)
- Sometimes lipid disorders and insulin resistance
Frequency of polycystic ovary syndrome
About 8-10% of women of reproductive age suffer from this disease.