How can you tell if your child has down syndrome
Facts about Down Syndrome | CDC
Down syndrome is a condition in which a person has an extra chromosome.
What is Down Syndrome?
Down syndrome is a condition in which a person has an extra chromosome. Chromosomes are small “packages” of genes in the body. They determine how a baby’s body forms and functions as it grows during pregnancy and after birth. Typically, a baby is born with 46 chromosomes. Babies with Down syndrome have an extra copy of one of these chromosomes, chromosome 21. A medical term for having an extra copy of a chromosome is ‘trisomy.’ Down syndrome is also referred to as Trisomy 21. This extra copy changes how the baby’s body and brain develop, which can cause both mental and physical challenges for the baby.
Even though people with Down syndrome might act and look similar, each person has different abilities. People with Down syndrome usually have an IQ (a measure of intelligence) in the mildly-to-moderately low range and are slower to speak than other children.
Some common physical features of Down syndrome include:
- A flattened face, especially the bridge of the nose
- Almond-shaped eyes that slant up
- A short neck
- Small ears
- A tongue that tends to stick out of the mouth
- Tiny white spots on the iris (colored part) of the eye
- Small hands and feet
- A single line across the palm of the hand (palmar crease)
- Small pinky fingers that sometimes curve toward the thumb
- Poor muscle tone or loose joints
- Shorter in height as children and adults
How Many Babies are Born with Down Syndrome?
Down syndrome remains the most common chromosomal condition diagnosed in the United States. Each year, about 6,000 babies born in the United States have Down syndrome. This means that Down syndrome occurs in about 1 in every 700 babies.1
Types of Down Syndrome
There are three types of Down syndrome. People often can’t tell the difference between each type without looking at the chromosomes because the physical features and behaviors are similar.
- Trisomy 21: About 95% of people with Down syndrome have Trisomy 21.2 With this type of Down syndrome, each cell in the body has 3 separate copies of chromosome 21 instead of the usual 2 copies.
- Translocation Down syndrome: This type accounts for a small percentage of people with Down syndrome (about 3%).2 This occurs when an extra part or a whole extra chromosome 21 is present, but it is attached or “trans-located” to a different chromosome rather than being a separate chromosome 21.
- Mosaic Down syndrome: This type affects about 2% of the people with Down syndrome.2 Mosaic means mixture or combination. For children with mosaic Down syndrome, some of their cells have 3 copies of chromosome 21, but other cells have the typical two copies of chromosome 21. Children with mosaic Down syndrome may have the same features as other children with Down syndrome. However, they may have fewer features of the condition due to the presence of some (or many) cells with a typical number of chromosomes.

Causes and Risk Factors
- The extra chromosome 21 leads to the physical features and developmental challenges that can occur among people with Down syndrome. Researchers know that Down syndrome is caused by an extra chromosome, but no one knows for sure why Down syndrome occurs or how many different factors play a role.
- One factor that increases the risk for having a baby with Down syndrome is the mother’s age. Women who are 35 years or older when they become pregnant are more likely to have a pregnancy affected by Down syndrome than women who become pregnant at a younger age.3-5However, the majority of babies with Down syndrome are born to mothers less than 35 years old, because there are many more births among younger women.6,7
Diagnosis
There are two basic types of tests available to detect Down syndrome during pregnancy: screening tests and diagnostic tests. A screening test can tell a woman and her healthcare provider whether her pregnancy has a lower or higher chance of having Down syndrome.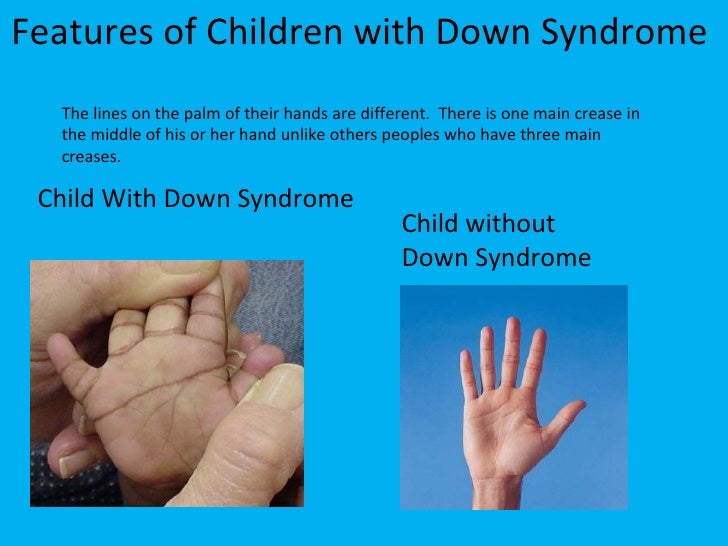 Screening tests do not provide an absolute diagnosis, but they are safer for the mother and the developing baby. Diagnostic tests can typically detect whether or not a baby will have Down syndrome, but they can be more risky for the mother and developing baby. Neither screening nor diagnostic tests can predict the full impact of Down syndrome on a baby; no one can predict this.
Screening tests do not provide an absolute diagnosis, but they are safer for the mother and the developing baby. Diagnostic tests can typically detect whether or not a baby will have Down syndrome, but they can be more risky for the mother and developing baby. Neither screening nor diagnostic tests can predict the full impact of Down syndrome on a baby; no one can predict this.
Screening Tests
Screening tests often include a combination of a blood test, which measures the amount of various substances in the mother’s blood (e.g., MS-AFP, Triple Screen, Quad-screen), and an ultrasound, which creates a picture of the baby. During an ultrasound, one of the things the technician looks at is the fluid behind the baby’s neck. Extra fluid in this region could indicate a genetic problem. These screening tests can help determine the baby’s risk of Down syndrome. Rarely, screening tests can give an abnormal result even when there is nothing wrong with the baby. Sometimes, the test results are normal and yet they miss a problem that does exist.
Diagnostic Tests
Diagnostic tests are usually performed after a positive screening test in order to confirm a Down syndrome diagnosis. Types of diagnostic tests include:
- Chorionic villus sampling (CVS)—examines material from the placenta
- Amniocentesis—examines the amniotic fluid (the fluid from the sac surrounding the baby)
- Percutaneous umbilical blood sampling (PUBS)—examines blood from the umbilical cord
These tests look for changes in the chromosomes that would indicate a Down syndrome diagnosis.
Other Health Problems
Many people with Down syndrome have the common facial features and no other major birth defects. However, some people with Down syndrome might have one or more major birth defects or other medical problems. Some of the more common health problems among children with Down syndrome are listed below.8
- Hearing loss
- Obstructive sleep apnea, which is a condition where the person’s breathing temporarily stops while asleep
- Ear infections
- Eye diseases
- Heart defects present at birth
Health care providers routinely monitor children with Down syndrome for these conditions.
Treatments
Down syndrome is a lifelong condition. Services early in life will often help babies and children with Down syndrome to improve their physical and intellectual abilities. Most of these services focus on helping children with Down syndrome develop to their full potential. These services include speech, occupational, and physical therapy, and they are typically offered through early intervention programs in each state. Children with Down syndrome may also need extra help or attention in school, although many children are included in regular classes.
Other Resources
The views of these organizations are their own and do not reflect the official position of CDC.
- Down Syndrome Research Foundation (DSRF)external icon
DSRF initiates research studies to better understand the learning styles of those with Down syndrome. - Global Down Syndrome Foundationexternal icon
This foundation is dedicated to significantly improving the lives of people with Down syndrome through research, medical care, education and advocacy.
- National Association for Down Syndromeexternal icon
The National Association for Down Syndrome supports all persons with Down syndrome in achieving their full potential. They seek to help families, educate the public, address social issues and challenges, and facilitate active participation. - National Down Syndrome Society (NDSS)external icon
NDSS seeks to increase awareness and acceptance of those with Down syndrome.
References
- Mai CT, Isenburg JL, Canfield MA, Meyer RE, Correa A, Alverson CJ, Lupo PJ, Riehle‐Colarusso T, Cho SJ, Aggarwal D, Kirby RS. National population‐based estimates for major birth defects, 2010–2014. Birth Defects Research. 2019; 111(18): 1420-1435.
- Shin M, Siffel C, Correa A. Survival of children with mosaic Down syndrome. Am J Med Genet A. 2010;152A:800-1.
- Allen EG, Freeman SB, Druschel C, et al. Maternal age and risk for trisomy 21 assessed by the origin of chromosome nondisjunction: a report from the Atlanta and National Down Syndrome Projects.
 Hum Genet. 2009 Feb;125(1):41-52.
Hum Genet. 2009 Feb;125(1):41-52. - Ghosh S, Feingold E, Dey SK. Etiology of Down syndrome: Evidence for consistent association among altered meiotic recombination, nondisjunction, and maternal age across populations. Am J Med Genet A. 2009 Jul;149A(7):1415-20.
- Sherman SL, Allen EG, Bean LH, Freeman SB. Epidemiology of Down syndrome. Ment Retard Dev Disabil Res Rev. 2007;13(3):221-7.
- Adams MM, Erickson JD, Layde PM, Oakley GP. Down’s syndrome. Recent trends in the United States. JAMA. 1981 Aug 14;246(7):758-60.
- Olsen CL, Cross PK, Gensburg LJ, Hughes JP. The effects of prenatal diagnosis, population ageing, and changing fertility rates on the live birth prevalence of Down syndrome in New York State, 1983-1992. Prenat Diagn. 1996 Nov;16(11):991-1002.
- Bull MJ, the Committee on Genetics. Health supervision for children with Down syndrome. Pediatrics. 2011;128:393-406.
What are Congenital Heart Defects?
Congenital heart defects (CHDs) are the most common type of birth defect. As medical care and treatment have advanced, babies with a CHD are living longer and healthier lives. Learn more facts about CHDs below.
As medical care and treatment have advanced, babies with a CHD are living longer and healthier lives. Learn more facts about CHDs below.
What are Congenital Heart Defects (CHDs)?
CHDs are present at birth and can affect the structure of a baby’s heart and the way it works. They can affect how blood flows through the heart and out to the rest of the body. CHDs can vary from mild (such as a small hole in the heart) to severe (such as missing or poorly formed parts of the heart).
About 1 in 4 babies born with a heart defect has a critical CHD (also known as critical congenital heart defect).1 Babies with a critical CHD need surgery or other procedures in the first year of life.
Piper was born with a congenital heart defect (CHD). Read her story as well as other stories from families affected by a congenital heart defect »
Types
Listed below are examples of different types of CHDs. The types marked with a star (*) are considered critical CHDs.
- Atrial Septal Defect
- Atrioventricular Septal Defect
- Coarctation of the Aorta*
- Double-outlet Right Ventricle*
- d-Transposition of the Great Arteries*
- Ebstein Anomaly*
- Hypoplastic Left Heart Syndrome*
- Interrupted Aortic Arch*
- Pulmonary Atresia*
- Single Ventricle*
- Tetralogy of Fallot*
- Total Anomalous Pulmonary Venous Return*
- Tricuspid Atresia*
- Truncus Arteriosus*
- Ventricular Septal Defect
Signs and Symptoms
Signs and symptoms for CHDs depend on the type and severity of the particular defect. Some defects might have few or no signs or symptoms. Others might cause a baby to have the following symptoms:
- Blue-tinted nails or lips
- Fast or troubled breathing
- Tiredness when feeding
- Sleepiness
Diagnosis
Some CHDs may be diagnosed during pregnancy using a special type of ultrasound called a fetal echocardiogram, which creates ultrasound pictures of the heart of the developing baby. However, some CHDs are not detected until after birth or later in life, during childhood or adulthood. If a healthcare provider suspects a CHD may be present, the baby can get several tests (such as an echocardiogram) to confirm the diagnosis.
However, some CHDs are not detected until after birth or later in life, during childhood or adulthood. If a healthcare provider suspects a CHD may be present, the baby can get several tests (such as an echocardiogram) to confirm the diagnosis.
Treatment
Treatment for CHDs depends on the type and severity of the defect present. Some affected infants and children might need one or more surgeries to repair the heart or blood vessels. Some can be treated without surgery using a procedure called cardiac catheterization. A long tube, called a catheter, is threaded through the blood vessels into the heart, where a doctor can take measurements and pictures, do tests, or repair the problem. Sometimes the heart defect can’t be fully repaired, but these procedures can improve blood flow and the way the heart works. It is important to note that even if their heart defect has been repaired, many people with CHDs are not cured. See more information about living with a CHD below.
Causes
The causes of CHDs among most babies are unknown. Some babies have heart defects because of changes in their individual genes or chromosomes. CHDs also are thought to be caused by a combination of genes and other factors, such as things in the environment, the mother’s diet, the mother’s health conditions, or the mother’s medication use during pregnancy. For example, certain conditions a mother has, like pre-existing diabetes or obesity, have been linked to heart defects in the baby.2,3 Smoking during pregnancy as well as taking certain medications have also been linked to heart defects.2,3
Some babies have heart defects because of changes in their individual genes or chromosomes. CHDs also are thought to be caused by a combination of genes and other factors, such as things in the environment, the mother’s diet, the mother’s health conditions, or the mother’s medication use during pregnancy. For example, certain conditions a mother has, like pre-existing diabetes or obesity, have been linked to heart defects in the baby.2,3 Smoking during pregnancy as well as taking certain medications have also been linked to heart defects.2,3
Learn more about research on CHDs »
Living with a CHD
As medical care and treatment have advanced, infants with CHDs are living longer and healthier lives. Many children with CHDs are now living into adulthood. It is estimated that more than two million individuals in the United States are living with a CHD. Many people with a CHD lead independent lives with little or no difficulty. Others might develop disability over time. Some people with a CHD have genetic problems or other health conditions that increase their risk for disability.
Some people with a CHD have genetic problems or other health conditions that increase their risk for disability.
Even with improved treatments, many people with a CHD are not cured, even if their heart defect has been repaired. People with a CHD can develop other health problems over time, depending on their specific heart defect, the number of heart defects they have, and the severity of their heart defect. For example, some other health problems that might develop include irregular heart beat (arrhythmias), increased risk of infection in the heart muscle (infective endocarditis), or weakness in the heart (cardiomyopathy). People with a CHD need routine checkups with a cardiologist (heart doctor) to stay as healthy as possible. They also might need further operations after initial childhood surgeries. It is important for people with a CHD to visit their doctor on a regular basis and discuss their health, including their specific heart condition, with their doctor.
Learn more about living with a CHD »
References
- Oster M, Lee K, Honein M, Colarusso T, Shin M, Correa A.
 Temporal trends in survival for infants with critical congenital heart defects. Pediatrics. 2013;131(5):e1502-8.
Temporal trends in survival for infants with critical congenital heart defects. Pediatrics. 2013;131(5):e1502-8. - Jenkins KJ, Correa A, Feinstein JA, Botto L, Britt AE, Daniels SR, Elixson M, Warnes CA, Webb CL. Noninherited risk factors and congenital cardiovascular defects: current knowledge: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young: endorsed by the American Academy of Pediatrics. Circulation. 2007;115(23):2995-3014.
- Patel SS, Burns TL. Nongenetic risk factors and congenital heart defects. Pediatr Cardiol. 2013;34(7):1535-55.
from 0 to 19 months
The presence of an additional, 47th, chromosome affects the development of the internal organs of the child, his abilities for mental and physical development. However, statistics say: 4 out of 5 children with this genomic pathology are trained, and some may well achieve significant success in life. There are a huge number of variations of the syndrome that have a different effect on the potential of the child - sometimes he does not need to draw up special programs at all, and his development is within the limits applicable to age.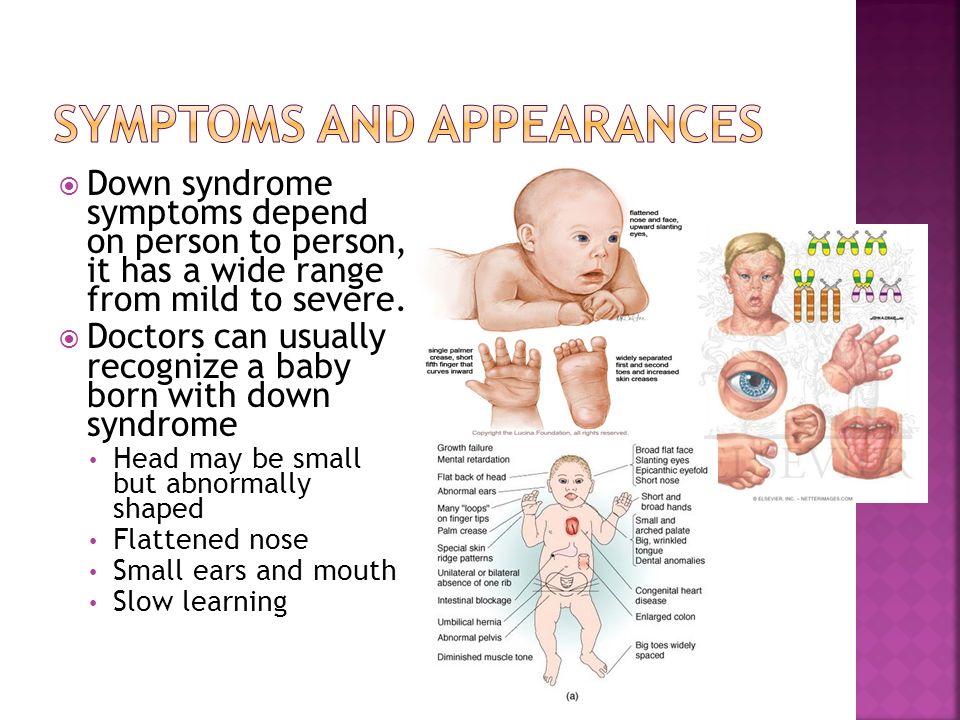
And yet, in most cases, children have problems with speech - for example, a delay between understanding and producing a word. Also common is the slow development of fine motor skills, which is inferior to other motor qualities in the pace of their improvement. Such children can stand up later - from 2 to 4 years. Therefore, doctors adhere to an early intervention approach: it is noticed that the earlier physical therapy and special classes are prescribed, the earlier examinations reveal limiting factors (for example, hearing problems), the faster the child develops and the less he lags behind his peers.
Causes of Down syndrome
Excess genetic material correlates with the age of the mother, father, and even maternal grandmother. However, it is impossible to predict whether a child will be born healthy or sick - his parents almost always turn out to be healthy people, and pathology is detected only at the stage of fetal screening. Indirectly affect the development of the syndrome can:
- conception in a closely related marriage;
- presence among relatives of a person with this mutation;
- late delivery with mother over 35 years of age and father over 40 years of age;
- the presence of bad habits, unhealthy diet and lifestyle.

The syndrome is not related to the sex of the fetus and is diagnosed using invasive and non-invasive techniques. At birth, the development of the child is almost always normal, with the exception of minor delays. At the same time, brothers and sisters with the disease are similar to each other, but not like their parents.
Differences since the early days:
- affected children have a flattened face and shortened nose;
- on the shortened neck there is a characteristic fold;
- at the inner corner of the eye, an epicanthus is noticeable, which is unusual for children of non-Mongoloid races;
- the corners of the eyes have different heights, which is often accompanied by strabismus;
- the tongue is enlarged, making it difficult for the child to keep his mouth closed;
- there is a curvature of the little finger, clinodactyly;
- in 20% or more, congenital leukemia, epilepsy, problems with the genitourinary system are also diagnosed.
Features of development
At the age of 3 months, a child with Down syndrome is characterized by the following level of development:
- expresses a feeling of hunger by crying, and satiety - by joy;
- reacts emotionally to the attention and appearance of significant adults;
- no problems with sucking and swallowing milk;
- when lying on his back, actively moves his arms and legs;
- lifting the head not lower than 4-6 cm from the surface, holding the head - 8-12 seconds;
- when lying down, holds the head for about a minute;
- compresses and unclenches well;
- can touch his own face with his fingers;
- actively observes interesting items;
- recognizes and responds to mother's voice;
- recognizes familiar people and emotionally expresses this.
At the age of 4-6 months:
- makes attempts to communicate with relatives, coos and babbles;
- knows how to laugh;
- shows apprehension and doubt at the sight of strangers;
- actively pulls pens into his mouth;
- sits and holds the head without much difficulty;
- observes interesting objects;
- well distinguishes acquaintances, up to frequent guests, from strangers;
- keeps track of favorite toys and other items of interest.
Older than 6 - up to 10 months:
- responds to tickling with laughter;
- smiles when playing or in response to affection;
- learns to speak short words of a couple of syllables;
- knows that if an object is dropped, it will be picked up;
- cries or shows other negative emotions if a toy is taken from him;
- knows how to eat from hands, drink from a mug held by an adult;
- begins to crawl and stand up independently with the support of an adult;
- passes objects with one or two hands;
- shows curiosity about the world around him, cognitive attempts.
At the age of 10-12 months:
- responds by crying to scolding or swearing;
- understands that items may be given in response to a request;
- eats independently;
- hugs parents;
- rolls over from back to stomach at will;
- walks with adult support;
- begins the development of fine motor skills in games;
- understands when spoken to.

13 to 15 months:
- waves and claps as appropriate;
- can respond with affirmative or negative head movements;
- gets up and walks independently;
- plays with a ball, a constructor, cars, a pyramid;
- makes the first drawings.
16-19 months of age:
- understands simple instructions from adults and does them on his own or with help from others;
- gives items to adults upon request;
- learns to take clothes off by himself;
- washes himself;
- can go up and down stairs with the help of an adult.
Contact us to receive an individual Vojta therapy program for your child!
Return to list
Don't know who to sign up for?
+7 (843) 202-26-27
Leave your contacts and the clinic administrator will call you soon and make an appointment with a specialist. Or call the indicated number
Or call the indicated number
Call me
Down syndrome: signs, causes, statistics. Help
https://ria.ru/20091124/195284093.html
Down syndrome: signs, causes, statistics. Help
Down syndrome: signs, causes, statistics. Help - RIA Novosti, 24.11.2009
Down syndrome: signs, causes, statistics. Help
Down's Syndrome is caused by a genetic abnormality. For the first time, the signs of people with Down syndrome were described in 1866 by the English doctor John ... RIA Novosti, 11/24/2009
2009-11-24T15:18
2009-11-24T15:18
2009-11-24T15:18
/html/head/meta[@name='og:title']/@content
/html/head/meta[@name='og:description']/@contenthttps://cdnn21.img.ria.ru/images/sharing/article/195284093.jpg?1957835221259065119
RIA Novosti
1
5
4.7
96
7 495 645-6601
Rossiya Segodnya
https: //xn---c1acbl2abdlkab1og. xn--p1ai/Awards/
xn--p1ai/Awards/
2009
RIA Novosti
1
5
4.7
9000 90004 -6601
FSUE MIA Rossiya Segodnya
https://xn--c1acbl2abdlkab1og.xn--p1ai/awards/
News
ru-RU
https://ria.ru/docs/about/ copyright.html
https://xn--c1acbl2abdlkab1og.xn--p1ai/
RIA Novosti
1
5
4.7
96 9000
7 495 645-6603
FSUE MIA today
https: // XN-C1ACBL2ABDLKab1G. XN-P1AI/ Awards/
RIA Novosti
1
5
4.7
9000
7 495 645-6601
FSUE MIA Russia Today
HTTPS ://xn--c1acbl2abdlkab1og.xn--p1ai/awards/
RIA Novosti
1,000 .xn--p1ai/awards/
society, references, life without barriers
Society, references, life without barriers
Down's Syndrome ( Down's Syndrome ) occurs as a result of a genetic anomaly. For the first time, the signs of people with Down syndrome were described in 1866 by the English physician John Langdon Down, whose name served as the name for this syndrome. The cause of the syndrome was found only in 1959 by the French scientist Jérôme Lejeune.
For the first time, the signs of people with Down syndrome were described in 1866 by the English physician John Langdon Down, whose name served as the name for this syndrome. The cause of the syndrome was found only in 1959 by the French scientist Jérôme Lejeune.
The syndrome occurs due to the process of chromosome segregation during the formation of gametes (eggs and spermatozoa), as a result of which the child receives from the mother (in 90% of cases) or from the father (in 10% of cases) an extra 21st chromosome. Most people with Down syndrome have three 21st chromosomes instead of two; in 5-8% of cases, the anomaly is associated with the presence not of a whole extra chromosome, but of its fragments.
Of the characteristic external signs of the syndrome, a flat face with slanting eyes (as in the Mongoloid race, so earlier this disease was called mongolism), wide lips, a wide flat tongue with a deep longitudinal furrow on it are noted. The head is round, sloping narrow forehead, auricles are reduced in the vertical direction, with adherent lobe, eyes with spotted iris (Brushfield's spots). The hair on the head is soft, sparse, straight with a low growth line at the neck. For people with Down syndrome, changes in the limbs are characteristic - shortening and widening of the hands and feet (acromicria). The little finger is shortened and curved, it has only two flexion grooves. On the palms there is only one transverse furrow (four-fingered). There are abnormal growth of teeth, high palate, changes in the internal organs, especially the alimentary canal and the heart.
The hair on the head is soft, sparse, straight with a low growth line at the neck. For people with Down syndrome, changes in the limbs are characteristic - shortening and widening of the hands and feet (acromicria). The little finger is shortened and curved, it has only two flexion grooves. On the palms there is only one transverse furrow (four-fingered). There are abnormal growth of teeth, high palate, changes in the internal organs, especially the alimentary canal and the heart.
In Russia, the term "Down's disease" is most often used. Some experts argue that there are even two diagnoses: Down's disease and Down's syndrome, but most scientists believe that this is not a disease, but a genetic disorder that determines the characteristics of a child's development at an early age. "Syndrome" means a specific set of features or characteristics.
According to the statistics of the World Health Organization, every 700-800th baby in the world is born with a diagnosis of Down syndrome. This ratio is the same in different countries, climatic zones and social strata. Genetic failure occurs regardless of the lifestyle of parents, their health, habits and education.
This ratio is the same in different countries, climatic zones and social strata. Genetic failure occurs regardless of the lifestyle of parents, their health, habits and education.
It is known that the risk of having a child with Down syndrome depends on the age of the mother. For women under the age of 25, the probability of having a sick child is 1/1400, up to 30 - 1/1000, at 35 years old the risk increases to 1/350, at 42 years old - up to 1/60, and at 49 years old - up to 1/1000. 12. However, because young women in general have many more children, the majority (80%) of all children with Down syndrome are actually born to young women under the age of 30.
A study conducted by scientists at the University of Mysore (India) identified four factors that affect the likelihood of Down syndrome in a child. This is the age of the mother, the age of the father, consanguineous marriages, and, oddly enough, the age of the maternal grandmother. Moreover, the last of the four factors was the most significant. The older the grandmother was when she gave birth to a daughter, the higher the likelihood that she would give birth to her grandson or granddaughter with Down syndrome. This probability increases by 30% with every year "missed" by the future grandmother.
The older the grandmother was when she gave birth to a daughter, the higher the likelihood that she would give birth to her grandson or granddaughter with Down syndrome. This probability increases by 30% with every year "missed" by the future grandmother.
For a study published online in the British Medical Journal (British Medical Journal), experts analyzed data from a national register that contained information on 26,000 identified cases of Down syndrome in England and Wales, diagnosed in both prenatal and postnatal stages of development. They found that the number of children diagnosed with this disease has increased by three-quarters since 1989, but the number of children born has decreased. Visually it looks like this: in 1989–1990 years - 1075 diagnosed cases, in 2007-2008 - 1843 diagnosed cases, the number of births decreased by 1%: from 752 to 743. . On average, 9 out of 10 women decide to terminate a pregnancy after they find out that their child is sick. Studies show that around 1,100 babies in England and Wales are not born each year due to Down syndrome.