Baby three months premature
the long-term impacts of being born extremely early
Scientists are watching out for the health of adults born extremely premature, such as these people who took part in a photography project.Credit: Red Méthot
They told Marcelle Girard her baby was dead.
Back in 1992, Girard, a dentist in Gatineau, Canada, was 26 weeks pregnant and on her honeymoon in the Dominican Republic.
When she started bleeding, physicians at the local clinic assumed the baby had died. But Girard and her husband felt a kick. Only then did the doctors check for a fetal heartbeat and realize the baby was alive.
The couple was medically evacuated by air to Montreal, Canada, then taken to the Sainte-Justine University Hospital Center. Five hours later, Camille Girard-Bock was born, weighing just 920 grams (2 pounds).
Babies born so early are fragile and underdeveloped. Their lungs are particularly delicate: the organs lack the slippery substance, called surfactant, that prevents the airways from collapsing upon exhalation. Fortunately for Girard and her family, Sainte-Justine had recently started giving surfactant, a new treatment at the time, to premature babies.
After three months of intensive care, Girard took her baby home.
Today, Camille Girard-Bock is 27 years old and studying for a PhD in biomedical sciences at the University of Montreal. Working with researchers at Sainte-Justine, she’s addressing the long-term consequences of being born extremely premature — defined, variously, as less than 25–28 weeks in gestational age.
Families often assume they will have grasped the major issues arising from a premature birth once the child reaches school age, by which time any neurodevelopmental problems will have appeared, Girard-Bock says. But that’s not necessarily the case. Her PhD advisers have found that young adults of this population exhibit risk factors for cardiovascular disease — and it may be that more chronic health conditions will show up with time.
Camille Girard-Bock, born at 26 weeks of gestation, is now studying the effects of prematurity for a PhD. Credit: Red Méthot
Credit: Red Méthot
Girard-Bock doesn’t let these risks preoccupy her. “As a survivor of preterm birth, you beat so many odds,” she says. “I guess I have some kind of sense that I’m going to beat those odds also.”
She and other against-the-odds babies are part of a population which is larger now than at any time in history: young adults who are survivors of extreme prematurity. For the first time, researchers can start to understand the long-term consequences of being born so early. Results are pouring out of cohort studies that have been tracking kids since birth, providing data on possible long-term outcomes; other studies are trialling ways to minimize the consequences for health.
These data can help parents make difficult decisions about whether to keep fighting for a baby’s survival. Although many extremely premature infants grow up to lead healthy lives, disability is still a major concern, particularly cognitive deficits and cerebral palsy.
Researchers are working on novel interventions to boost survival and reduce disability in extremely premature newborns. Several compounds aimed at improving lung, brain and eye function are in clinical trials, and researchers are exploring parent-support programmes, too.
Several compounds aimed at improving lung, brain and eye function are in clinical trials, and researchers are exploring parent-support programmes, too.
Researchers are also investigating ways to help adults who were born extremely prematurely to cope with some of the long-term health impacts they might face: trialling exercise regimes to minimize the newly identified risk of cardiovascular disease, for example.
“We are really at the stage of seeing this cohort becoming older,” says neonatologist Jeanie Cheong at the Royal Women’s Hospital in Melbourne, Australia. Cheong is the director of the Victorian Infant Collaborative Study (VICS), which has been following survivors for four decades. “This is an exciting time for us to really make a difference to their health.”
The late twentieth century brought huge changes to neonatal medicine. Lex Doyle, a paediatrician and previous director of VICS, recalls that when he started caring for preterm infants in 1975, very few survived if they were born at under 1,000 grams — a birthweight that corresponds to about 28 weeks’ gestation. The introduction of ventilators, in the 1970s in Australia, helped, but also caused lung injuries, says Doyle, now associate director of research at the Royal Women’s Hospital. In the following decades, doctors began to give corticosteroids to mothers due to deliver early, to help mature the baby’s lungs just before birth. But the biggest difference to survival came in the early 1990s, with surfactant treatment.
The introduction of ventilators, in the 1970s in Australia, helped, but also caused lung injuries, says Doyle, now associate director of research at the Royal Women’s Hospital. In the following decades, doctors began to give corticosteroids to mothers due to deliver early, to help mature the baby’s lungs just before birth. But the biggest difference to survival came in the early 1990s, with surfactant treatment.
“I remember when it arrived,” says Anne Monique Nuyt, a neonatologist at Sainte-Justine and one of Girard-Bock’s advisers. “It was a miracle.” Risk of death for premature infants dropped to 60–73% of what it was before1,2.
Marcelle Girard looks in at baby Camille, born weighing just 920 grams (2 pounds).Credit: Camille Girard-Bock
Today, many hospitals regularly treat, and often save, babies born as early as 22–24 weeks. Survival rates vary depending on location and the kinds of interventions a hospital is able to provide. In the United Kingdom, for example, among babies who are alive at birth and receiving care, 35% born at 22 weeks survive, 38% at 23 weeks, and 60% at 24 weeks3.
For babies who survive, the earlier they are born, the higher the risk of complications or ongoing disability (see ‘The effects of being early’). There is a long list of potential problems — including asthma, anxiety, autism spectrum disorder, cerebral palsy, epilepsy and cognitive impairment — and about one-third of children born extremely prematurely have one condition on the list, says Mike O’Shea, a neonatologist at the University of North Carolina School of Medicine in Chapel Hill, who co-runs a study tracking children born between 2002 and 2004. In this cohort, another one-third have multiple disabilities, he says, and the rest have none.
“Preterm birth should be thought of as a chronic condition that requires long-term follow-up,” says Casey Crump, a family physician and epidemiologist at the Icahn School of Medicine at Mount Sinai in New York, who notes that when these babies become older children or adults, they don’t usually get special medical attention. “Doctors are not used to seeing them, but they increasingly will. ”
”
What should doctors expect? For a report in the Journal of the American Medical Association last year4, Crump and his colleagues scraped data from the Swedish birth registry. They looked at more than 2.5 million people born from 1973 to 1997, and checked their records for health issues up until the end of 2015.
Source: Ref. 4
Of the 5,391 people born extremely preterm, 78% had at least one condition that manifested in adolescence or early adulthood, such as a psychiatric disorder, compared with 37% of those born full-term. When the researchers looked at predictors of early mortality, such as heart disease, 68% of people born extremely prematurely had at least one such predictor, compared with 18% for full-term births — although these data include people born before surfactant and corticosteroid use were widespread, so it’s unclear if these data reflect outcomes for babies born today. Researchers have found similar trends in a UK cohort study of extremely premature births. In results published earlier this year5, the EPICure study team, led by neonatologist Neil Marlow at University College London, found that 60% of 19-year-olds who were extremely premature were impaired in at least one neuropsychological area, often cognition.
In results published earlier this year5, the EPICure study team, led by neonatologist Neil Marlow at University College London, found that 60% of 19-year-olds who were extremely premature were impaired in at least one neuropsychological area, often cognition.
Such disabilities can impact education as well as quality of life. Craig Garfield, a paediatrician at the Northwestern University Feinberg School of Medicine and the Lurie Children’s Hospital of Chicago, Illinois, addressed a basic question about the first formal year of schooling in the United States: “Is your kid ready for kindergarten, or not?”
To answer it, Garfield and his colleagues analysed standardized test scores and teacher assessments on children born in Florida between 1992 and 2002. Of those born at 23 or 24 weeks, 65% were considered ready to start kindergarten at the standard age, 5–6 years old, with the age adjusted to take into account their earlier birth. In comparison, 85.3% of children born full term were kindergarten-ready6.
Despite their tricky start, by the time they reach adolescence, many people born prematurely have a positive outlook. In a 2006 paper7, researchers studying individuals born weighing 1,000 grams or less compared these young adults’ perceptions of their own quality of life with those of peers of normal birthweight — and, to their surprise, found that the scores were comparable. Conversely, a 2018 study8 found that children born at less than 28 weeks did report having a significantly lower quality of life. The children, who did not have major disabilities, scored themselves 6 points lower, out of 100, than a reference population.
As Marlow spent time with his participants and their families, his worries about severe neurological issues diminished. Even when such issues are present, they don’t greatly limit most children and young adults. “They want to know that they are going to live a long life, a happy life,” he says. Most are on track to do so. “The truth is, if you survive at 22 weeks, the majority of survivors do not have a severe, life-limiting disability. ”
”
A nurse uses electroencephalography (EEG) to carry out a check of brain development on a baby born at 25 weeks.Credit: BSIP/Universal Images Group via Getty
BreathlessBut scientists have only just begun to follow people born extremely prematurely into adulthood and then middle age and beyond, where health issues may yet lurk. “I’d like scientists to focus on improving the long-term outcomes as much as the short-term outcomes,” says Tala Alsadik, a 16-year-old high-school student in Jeddah, Saudi Arabia.
When Alsadik’s mother was 25 weeks pregnant and her waters broke, doctors went so far as to hand funeral paperwork to the family before consenting to perform a caesarean section. As a newborn, Alsadik spent three months in the neonatal-intensive-care unit (NICU) with kidney failure, sepsis and respiratory distress.
The complications didn’t end when she went home. The consequences of her prematurity are on display every time she speaks, her voice high and breathy because the ventilator she was put on damaged her vocal cords. When she was 15, her navel unexpectedly began leaking yellow discharge, and she required surgery. It turned out to be caused by materials leftover from when she received nutrients through a navel tube.
When she was 15, her navel unexpectedly began leaking yellow discharge, and she required surgery. It turned out to be caused by materials leftover from when she received nutrients through a navel tube.
The brain, interrupted
That certainly wasn’t something her physicians knew to check for. In fact, doctors don’t often ask if an adolescent or adult patient was born prematurely — but doing so can be revealing.
Charlotte Bolton is a respiratory physician at the University of Nottingham, UK, where she specializes in patients with chronic obstructive pulmonary disease (COPD). People coming into her practice tend to be in their 40s or older, often current or former smokers. But in around 2008, she began to notice a new type of patient being referred to her owing to breathlessness and COPD-like symptoms: 20-something non-smokers.
Quizzing them, Bolton discovered that many had been born before 32 weeks. For more insight, she got in touch with Marlow, who had also become concerned about lung function as the EPICure participants aged. Alterations in lung function are a key predictor of cardiovascular disease, the leading cause of death around the world. Clinicians already knew that after extremely premature birth, the lungs often don’t grow to full size. Ventilators, high oxygen levels, inflammation and infection can further damage the immature lungs, leading to low lung function and long-term breathing problems, as Bolton, Marlow and their colleagues showed in a study of 11-year-olds9.
Alterations in lung function are a key predictor of cardiovascular disease, the leading cause of death around the world. Clinicians already knew that after extremely premature birth, the lungs often don’t grow to full size. Ventilators, high oxygen levels, inflammation and infection can further damage the immature lungs, leading to low lung function and long-term breathing problems, as Bolton, Marlow and their colleagues showed in a study of 11-year-olds9.
Treatments for premature babies have improved in recent decades, but survival rates vary by age and country.Credit: Mohammed Hamoud/Getty
VICS research backs up the cardiovascular concerns: researchers have observed diminished airflow in 8-year-olds, worsening as they aged10, as well as high blood pressure in young adults11. “We really haven’t found the reason yet,” says Cheong. “That opens up a whole new research area.”
At Sainte-Justine, researchers have also noticed that young adults who were born at 28 weeks or less are at nearly three times the usual risk of having high blood pressure12. The researchers figured they would try medications to control it. But their patient advisory board members had other ideas — they wanted to try lifestyle interventions first.
The researchers figured they would try medications to control it. But their patient advisory board members had other ideas — they wanted to try lifestyle interventions first.
The scientists were pessimistic as they began a pilot study of a 14-week exercise programme. They thought that the cardiovascular risk factors would be unchangeable. Preliminary results indicate that they were wrong; the young adults are improving with exercise.
Girard-Bock says the data motivate her to eat healthily and stay active. “I’ve been given the chance to stay alive,” she says. “I need to be careful.”
From the startFor babies born prematurely, the first weeks and months of life are still the most treacherous. Dozens of clinical trials are in progress for prematurity and associated complications, some testing different nutritional formulas or improving parental support, and others targeting specific issues that lead to disability later on: underdeveloped lungs, brain bleeds and altered eye development.
For instance, researchers hoping to protect babies’ lungs gave a growth factor called IGF-1 — which the fetus usually gets from its mother during the first two trimesters of pregnancy — to premature babies in a phase II clinical trial reported13 in 2016. Rates of a chronic lung condition that often affects premature babies halved, and babies were somewhat less likely to have a severe brain haemorrhage in their earliest months.
Could baby’s first bacteria take root before birth?
Another concern is visual impairment. Retina development halts prematurely when babies born early begin breathing oxygen. Later it restarts, but preterm babies might then make too much of a growth factor called VEGF, causing over-proliferation of blood vessels in the eye, a disorder known as retinopathy. In a phase III trial announced in 2018, researchers successfully treated 80% of these retinopathy cases with a VEGF-blocking drug called ranibizumab14, and in 2019 the drug was approved in the European Union for use in premature babies.
Some common drugs might also be of use: paracetamol (acetaminophen), for example, lowers levels of biomolecules called prostaglandins, and this seems to encourage a key fetal vein in the lungs to close, preventing fluid from entering the lungs15.
But among the most promising treatment programmes, some neonatologists say, are social interventions to help families after they leave the hospital. For parents, it can be nerve-racking to go it alone after depending on a team of specialists for months, and lack of parental confidence has been linked to parental depression and difficulties with behaviour and social development in their growing children.
At Women & Infants Hospital of Rhode Island in Providence, Betty Vohr is director of the Neonatal Follow-Up Program. There, families are placed in private rooms, instead of sharing a large bay as happens in many NICUs. Once they are ready to leave, a programme called Transition Home Plus helps them to prepare and provides assistance such as regular check-ins by phone and in person in the first few days at home, and a 24/7 helpline. For mothers with postnatal depression, the hospital offers care from psychologists and specialist nurses.
For mothers with postnatal depression, the hospital offers care from psychologists and specialist nurses.
The results have been significant, says Vohr. The single-family rooms resulted in higher milk production by mothers: 30% more at four weeks than for families in more open spaces. At 2 years old, children from the single-family rooms scored higher on cognitive and language tests16. After Transition Home Plus began, babies discharged from the NICU had lower health-care costs and fewer hospital visits — issues that are of great concern for premature infants17. Other NICUs are developing similar programmes, Vohr says.
With these types of novel intervention, and the long-term data that continue to pour out of studies, doctors can make better predictions than ever before about how extremely premature infants will fare. Although these individuals face complications, many will thrive.
Alsadik, for one, intends to be a success story. Despite her difficult start in life, she does well academically, and plans to become a neonatologist. “I, also, want to improve the long-term outcomes of premature birth for other people.”
“I, also, want to improve the long-term outcomes of premature birth for other people.”
Premature birth - Symptoms and causes
Overview
A premature birth is a birth that takes place more than three weeks before the baby's estimated due date. In other words, a premature birth is one that occurs before the start of the 37th week of pregnancy.
Premature babies, especially those born very early, often have complicated medical problems. Typically, complications of prematurity vary. But the earlier your baby is born, the higher the risk of complications.
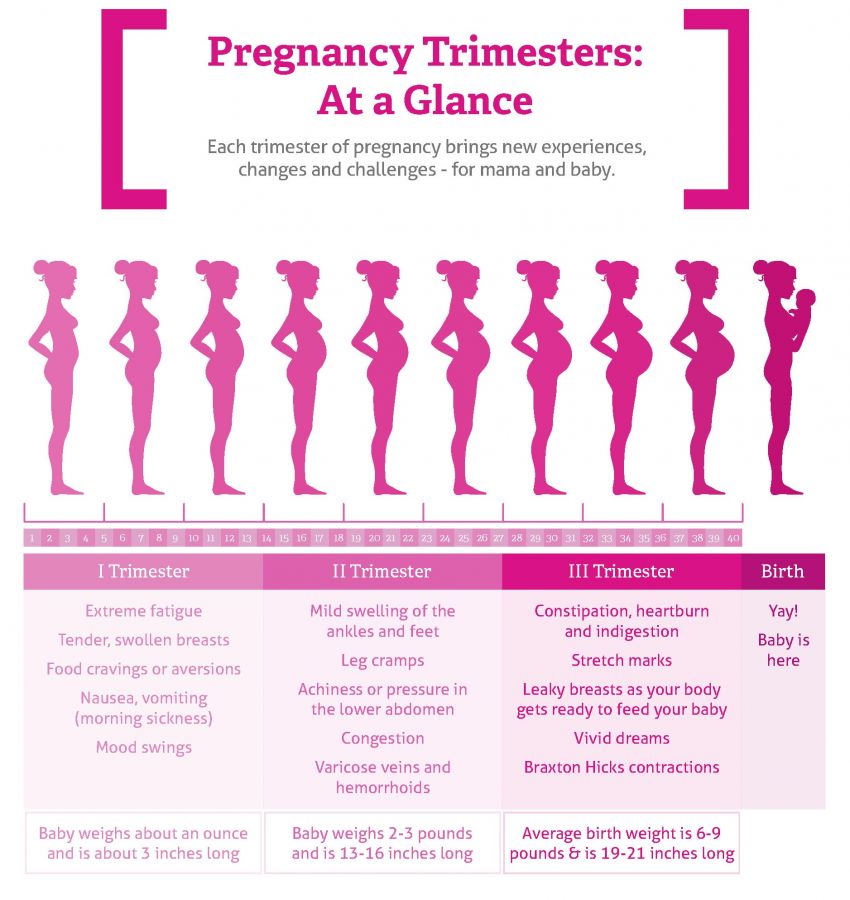
Depending on how early a baby is born, he or she may be:
- Late preterm, born between 34 and 36 completed weeks of pregnancy
- Moderately preterm, born between 32 and 34 weeks of pregnancy
- Very preterm, born at less than 32 weeks of pregnancy
- Extremely preterm, born at or before 25 weeks of pregnancy
Most premature births occur in the late preterm stage.
Products & Services
- Book: Mayo Clinic Guide to a Healthy Pregnancy
- Book: Mayo Clinic Guide to Your Baby's First Years
Symptoms
Your baby may have very mild symptoms of premature birth, or may have more-obvious complications.
Some signs of prematurity include the following:
- Small size, with a disproportionately large head
- Sharper looking, less rounded features than a full-term baby's features, due to a lack of fat stores
- Fine hair (lanugo) covering much of the body
- Low body temperature, especially immediately after birth in the delivery room, due to a lack of stored body fat
- Labored breathing or respiratory distress
- Lack of reflexes for sucking and swallowing, leading to feeding difficulties
The following tables show the median birth weight, length and head circumference of premature babies at different gestational ages for each sex.
| Weight, length and head circumference by gestational age for boys | |||
|---|---|---|---|
| Gestational age | Weight | Length | Head circumference |
| 40 weeks | 7 lbs. , 15 oz. , 15 oz.(3.6 kg) | 20 in. (51 cm) | 13.8 in. (35 cm) |
| 35 weeks | 5 lbs., 8 oz. (2.5 kg) | 18.1 in. (46 cm) | 12.6 in. (32 cm) |
| 32 weeks | 3 lbs., 15.5 oz. (1.8 kg) | 16.5 in. (42 cm) | 11.6 in. (29.5 cm) |
| 28 weeks | 2 lbs., 6.8 oz. (1.1 kg) | 14.4 in. (36.5 cm) | 10.2 in. (26 cm) |
| 24 weeks | 1 lb., 6.9 oz. (0.65 kg) | 12.2 in. (31 cm) | 8.7 in. (22 cm) |
| Weight, length and head circumference by gestational age for girls | |||
|---|---|---|---|
| Gestational age | Weight | Length | Head circumference |
| 40 weeks | 7 lbs. , 7.9 oz. , 7.9 oz.(3.4 kg) | 20 in. (51 cm) | 13.8 in. (35 cm) |
| 35 weeks | 5 lbs., 4.7 oz. (2.4 kg) | 17.7 in. (45 cm) | 12.4 in. (31.5 cm) |
| 32 weeks | 3 lbs., 12 oz. (1.7 kg) | 16.5 in. (42 cm) | 11.4 in. (29 cm) |
| 28 weeks | 2 lbs., 3.3 oz. (1.0 kg) | 14.1 in. (36 cm) | 9.8 in. (25 cm) |
| 24 weeks | 1 lb., 5.2 oz. (0.60 kg) | 12.6 in. (32 cm) | 8.3 in. (21 cm) |
Special care
If you deliver a preterm baby, your baby will likely need a longer hospital stay in a special nursery unit at the hospital. Depending on how much care your baby requires, he or she may be admitted to an intermediate care nursery or the neonatal intensive care unit (NICU).![]() Doctors and a specialized team with training in taking care of preterm babies will be available to help care for your baby. Don't hesitate to ask questions.
Doctors and a specialized team with training in taking care of preterm babies will be available to help care for your baby. Don't hesitate to ask questions.
Your baby may need extra help feeding, and adapting immediately after delivery. Your health care team can help you understand what is needed and what your baby's care plan will be.
Request an Appointment at Mayo Clinic
Risk factors
Often, the specific cause of premature birth isn't clear. However, there are known risk factors of premature delivery, including:
- Having a previous premature birth
- Pregnancy with twins, triplets or other multiples
- An interval of less than six months between pregnancies
- Conceiving through in vitro fertilization
- Problems with the uterus, cervix or placenta
- Smoking cigarettes or using illicit drugs
- Some infections, particularly of the amniotic fluid and lower genital tract
- Some chronic conditions, such as high blood pressure and diabetes
- Being underweight or overweight before pregnancy
- Stressful life events, such as the death of a loved one or domestic violence
- Multiple miscarriages or abortions
- Physical injury or trauma
For unknown reasons, black women are more likely to experience premature birth than are women of other races. But premature birth can happen to anyone. In fact, many women who have a premature birth have no known risk factors.
But premature birth can happen to anyone. In fact, many women who have a premature birth have no known risk factors.
Complications
While not all premature babies experience complications, being born too early can cause short-term and long-term health problems. Generally, the earlier a baby is born, the higher the risk of complications. Birth weight plays an important role, too.
Some problems may be apparent at birth, while others may not develop until later.
Short-term complications
In the first weeks, the complications of premature birth may include:
-
Breathing problems. A premature baby may have trouble breathing due to an immature respiratory system. If the baby's lungs lack surfactant — a substance that allows the lungs to expand — he or she may develop respiratory distress syndrome because the lungs can't expand and contract normally.
Premature babies may also develop a lung disorder known as bronchopulmonary dysplasia.
 In addition, some preterm babies may experience prolonged pauses in their breathing, known as apnea.
In addition, some preterm babies may experience prolonged pauses in their breathing, known as apnea. - Heart problems. The most common heart problems premature babies experience are patent ductus arteriosus (PDA) and low blood pressure (hypotension). PDA is a persistent opening between the aorta and pulmonary artery. While this heart defect often closes on its own, left untreated it can lead to a heart murmur, heart failure as well as other complications. Low blood pressure may require adjustments in intravenous fluids, medicines and sometimes blood transfusions.
- Brain problems. The earlier a baby is born, the greater the risk of bleeding in the brain, known as an intraventricular hemorrhage. Most hemorrhages are mild and resolve with little short-term impact. But some babies may have larger brain bleeding that causes permanent brain injury.
-
Temperature control problems.
 Premature babies can lose body heat rapidly. They don't have the stored body fat of a full-term infant, and they can't generate enough heat to counteract what's lost through the surface of their bodies. If body temperature dips too low, an abnormally low core body temperature (hypothermia) can result.
Premature babies can lose body heat rapidly. They don't have the stored body fat of a full-term infant, and they can't generate enough heat to counteract what's lost through the surface of their bodies. If body temperature dips too low, an abnormally low core body temperature (hypothermia) can result.Hypothermia in a premature baby can lead to breathing problems and low blood sugar levels. In addition, a premature infant may use up all of the energy gained from feedings just to stay warm. That's why smaller premature infants require additional heat from a warmer or an incubator until they're larger and able to maintain body temperature without assistance.
- Gastrointestinal problems. Premature infants are more likely to have immature gastrointestinal systems, resulting in complications such as necrotizing enterocolitis (NEC). This potentially serious condition, in which the cells lining the bowel wall are injured, can occur in premature babies after they start feeding.
 Premature babies who receive only breast milk have a much lower risk of developing NEC.
Premature babies who receive only breast milk have a much lower risk of developing NEC. -
Blood problems. Premature babies are at risk of blood problems such as anemia and newborn jaundice. Anemia is a common condition in which the body doesn't have enough red blood cells. While all newborns experience a slow drop in red blood cell count during the first months of life, the decrease may be greater in premature babies.
Newborn jaundice is a yellow discoloration in a baby's skin and eyes that occurs because the baby's blood contains excess bilirubin, a yellow-colored substance, from the liver or red blood cells. While there are many causes of jaundice, it is more common in preterm babies.
- Metabolism problems. Premature babies often have problems with their metabolism. Some premature babies may develop an abnormally low level of blood sugar (hypoglycemia). This can happen because premature infants typically have smaller stores of stored glucose than do full-term babies.
 Premature babies also have more difficulty converting their stored glucose into more-usable, active forms of glucose.
Premature babies also have more difficulty converting their stored glucose into more-usable, active forms of glucose. - Immune system problems. An underdeveloped immune system, common in premature babies, can lead to a higher risk of infection. Infection in a premature baby can quickly spread to the bloodstream, causing sepsis, an infection that spreads to the bloodstream.
Long-term complications
In the long term, premature birth may lead to the following complications:
- Cerebral palsy. Cerebral palsy is a disorder of movement, muscle tone or posture that can be caused by infection, inadequate blood flow or injury to a newborn's developing brain either early during pregnancy or while the baby is still young and immature.
- Impaired learning. Premature babies are more likely to lag behind their full-term counterparts on various developmental milestones. Upon school age, a child who was born prematurely might be more likely to have learning disabilities.

- Vision problems. Premature infants may develop retinopathy of prematurity, a disease that occurs when blood vessels swell and overgrow in the light-sensitive layer of nerves at the back of the eye (retina). Sometimes the abnormal retinal vessels gradually scar the retina, pulling it out of position. When the retina is pulled away from the back of the eye, it's called retinal detachment, a condition that, if undetected, can impair vision and cause blindness.
- Hearing problems. Premature babies are at increased risk of some degree of hearing loss. All babies will have their hearing checked before going home.
- Dental problems. Premature infants who have been critically ill are at increased risk of developing dental problems, such as delayed tooth eruption, tooth discoloration and improperly aligned teeth.
- Behavioral and psychological problems. Children who experienced premature birth may be more likely than full-term infants to have certain behavioral or psychological problems, as well as developmental delays.

- Chronic health issues. Premature babies are more likely to have chronic health issues — some of which may require hospital care — than are full-term infants. Infections, asthma and feeding problems are more likely to develop or persist. Premature infants are also at increased risk of sudden infant death syndrome (SIDS).
Prevention
Although the exact cause of preterm birth is often unknown, there are some things that can be done to help women — especially those who have an increased risk — to reduce their risk of preterm birth, including:
- Progesterone supplements. Women who have a history of preterm birth, a short cervix or both factors may be able to reduce the risk of preterm birth with progesterone supplementation.
-
Cervical cerclage. This is a surgical procedure performed during pregnancy in women with a short cervix, or a history of cervical shortening that resulted in a preterm birth.

During this procedure, the cervix is stitched closed with strong sutures that may provide extra support to the uterus. The sutures are removed when it's time to deliver the baby. Ask your doctor if you need to avoid vigorous activity during the remainder of your pregnancy.
By Mayo Clinic Staff
Related
Associated Procedures
Products & Services
Premature baby: development by month
Nursing methods for premature newborns are developing rapidly these days. It happens that babies are born with a weight of 500 grams. How do doctors assess their condition? What indicators of development should be guided by in order to understand whether everything is normal for the baby?
In the official language
Russia switched to the medical birth criteria approved by the World Health Organization in 2012. They are determined by the presence of the following signs in a newborn: breathing, heartbeat, pulsation of the umbilical cord, or voluntary muscle movements.
According to these parameters, a premature newborn is an infant weighing over 500 grams, over 25 centimeters tall, born at the 22nd week of pregnancy. Every year, 5-10% of such children are born from the total number of newborns around the world.
Today there are all conditions for nursing "early" children.
Early help
A 500g baby is not just very small. In such babies, the organs and systems are immature, the immune system does not work at full strength, so the body of prematurely born children is very vulnerable and susceptible to the effects of various adverse factors. What does not harm the health of full-term babies may affect a child with extremely low body weight.
Children weighing 1000-1499 g and less than 1000 g are most at risk of developing various diseases. Moreover, the shorter the gestation period, the higher the risk that the baby may have several problems at once.
The sooner doctors can identify possible pathologies and disorders, the sooner it will be possible to start adequate treatment, facilitate the adaptation of the baby to the air environment and provide him with the most favorable opportunities for development./imgs/2019/04/01/08/3032738/a717beab6b02a9e8c34b77202d653d88bc9ce4bd.png)
Three ages of premature baby
Usually a person's age is calculated from the moment of his birth. But for each premature baby, doctors determine three ages at once.
Chronological
This indicator is familiar to everyone. It is counted from the moment the child is born. If the baby was born on December 1, then on January 1 he will be 1 month old.
Gestational
This is the age that is equal to the number of completed weeks of pregnancy at the time of delivery. It is counted in weeks and days. For example, a child was born on January 1 at 25 weeks and 5 days. In this case, his age is 25 weeks, rounding up does not occur.
Adjusted
This is the child's age minus the "missing" weeks. It is considered relative to 40 weeks.
Corrected age = chronological age - (40 weeks - gestational age)
For example, the child's chronological age is 4 months (i.e. 16 weeks). The baby was born at the 28th week of gestation, that is, 12 weeks earlier (term delivery = 40 weeks). Corrected age of the child: 16-12 = 4 weeks (or 1 month).
Corrected age of the child: 16-12 = 4 weeks (or 1 month).
This means that if a full-term baby usually starts crawling around the age of 9months, then for a child born 3 months premature, it is permissible to start crawling at the age of up to 12 months. This is by no means considered a pathology. In addition, if a premature baby was sick after birth and, for example, was connected to a ventilator, this period will affect its development. In this case, such a baby will learn everything a little later.
The most commonly used skill scale for preterm infants, adjusted for age.
Peculiarities of psychomotor development
Each child is individual, and one should not compare different children with each other. It is quite natural that a baby born at 34 weeks is more likely to catch up with his full-term peers than a baby born at 27 weeks. What indicators do doctors focus on? What should parents pay attention to?
Pediatrician Natalya Maykova tells about what scientists know today.
- The child develops gradually and progressively.
- In premature babies, skills are formed in approximately the same sequence as in full-term babies, but adjusted for corrected age.
- The individual characteristics of a child's development are related to his gestational age (the gestational age at which he was born) and his condition at the time of birth. That is, the more problems the baby experienced in the first months of his life, the longer it will take him to acquire new skills.
- For an adequate assessment of the pace and level of development of the baby, dynamic monthly monitoring of the child is necessary.
Monthly development
There is an approximate list of skills and abilities that can be expected from a premature baby in the first 18 months of his life. However, it is worth remembering that one should focus not on the chronological age, but on the corrected one.
Of course, conditional standards cannot be applied to absolutely all premature babies, but they can serve as a guideline for both doctors and parents.
Only prematurely born children, as a rule, need special conditions and constant medical supervision. Often these babies are fed through a food tube and supported by their breathing through artificial oxygen supply.
2 months of corrected age
The baby holds his head well, his first coos, smiles appear. The child begins to listen, recognize native people and rejoice when communicating with them.
4 months
The child lies confidently on his tummy, raises his head, looks around. He watches over objects and people. Some babies are already well rolled over on their stomach and back.
6 months
The child learns several skills at once: he learns to sit, crawl, stand on all fours. Babble appears in the baby’s speech when he repeats the same simple syllables: “ma-ma-ma”, “yes-yes-yes”, etc. He enthusiastically plays with toys and various objects. He is interested in those that are out of his reach, and tries to crawl up to them or reach out to them.
9 months
Baby crawls everywhere, gets up, reaches for objects, plays with them. More and more new syllables appear in his "lexicon", he tries to imitate new sounds. At this time, the child begins to understand the word "no" well.
12 months
By the age of one, children, as a rule, are already completely catching up with their peers who were born on time, both physically and psycho-emotionally. They already know a lot: they take their first steps, walk holding on to walls and furniture, bend down and pick up objects from the floor. The speech of a one-year-old child is actively developing: the baby consciously pronounces new words, enters into communication, answering the questions posed. He likes to communicate with the help of gestures: he waves his hand, shakes his head, nods. During this period, the child begins to get upset at the moments of the absence of a close adult nearby.
15 months
The child's vocabulary grows quickly. He can, upon request, point his finger at objects, animals, body parts. The coordination of movements improves, the gait becomes confident, the child knows how to squat. The kid's games with simple educational toys (cubes, pyramid) become conscious. He learns to sort objects, to solve simple puzzles.
He can, upon request, point his finger at objects, animals, body parts. The coordination of movements improves, the gait becomes confident, the child knows how to squat. The kid's games with simple educational toys (cubes, pyramid) become conscious. He learns to sort objects, to solve simple puzzles.
18 months
At this age, the child can confidently use a spoon and drink from a cup. He knows how to go up and down the stairs, tries to dress and undress on his own. The child communicates emotionally, uses more and more words in speech.
Specialists: a pediatrician and a neurologist can help parents evaluate the harmonious development of the baby. Doctors will notice “weak points” in the development of the child in time and help develop a plan for his further observation and, if necessary, treatment, which includes not only drugs, but also massage, physiotherapy exercises, kinesitherapy and other modern methods.
It is important to remember that the development of a premature baby largely depends on the care and responsible attitude of parents to the recommendations of doctors.
Photo: Collection/iStock
Answering important questions about preterm babies — CSM Zdravica
Every year, thousands of premature babies are born in Novosibirsk, weighing no more than one kilogram. After being discharged from the hospital, such "early" babies need special care and qualified supervision by a pediatrician.
For many years, small patients with extremely low body weight have been successfully observed in Zdravitsa. Over the past 5 years, 9 people have come out here and put on their feet23 babies.
Nadezhda Georgievna Vasilchenko, Head of the Department of Pediatrics at Zdravitsa, spoke about the special conditions created for babies in this clinic and how mothers and fathers can help the development of a premature baby at home.
When should a baby be born to be called premature?
Up to 38 weeks, 37 weeks is the upper limit of the estimate, the lower is 24 weeks. Extremely low body weight is considered to be a child weighing up to one kilogram, and very low - from one to one and a half kilograms at birth.
How is such a child different from a baby who was born at term?
This is a small child who does not keep heat very well or does not keep heat at all, whose lung tissue has not fully matured, and he cannot breathe on his own, he needs oxygen support, warming, these children are nursed in an incubator where oxygen can be given in different ways: mask, artificial lung ventilation. This is a child who can give edematous syndrome, especially if there is an element of hypothermia, these children are usually small, they cannot swallow themselves, so they are often fed through a tube.
Until what time are such children in the incubator? Are they discharged at 41 weeks?
No, when they gain about 2 kg of weight, keep warm, start sucking and swallowing themselves, it's all individual. If everything goes well, and he is just premature, then he is discharged in 2-3 months.
What problems can premature babies have that parents will have to face?
The most common is bronchopulmonary dysplasia, that is, underdevelopment of the lungs, as there is not enough surfactant, this is a substance that prevents the lungs from sticking together, and because of this, the lung cannot fully open. Also dysbiosis, since colonization of the intestine is not the same as in a full-term baby. Anemia is a lack of iron / hemoglobin, since the child receives the main amount in the 3rd trimester of pregnancy, and this child was born before that time. Almost every premature baby suffers from this condition. Reduced immunity as the microbiota cannot fully develop. Due to immaturity, retinopathy of the newborn develops, or such children are at risk for retinopathy, so they are observed by ophthalmologists according to a special schedule, they are removed from the register when the gestational age approaches 40 weeks, by which time the fundus is formed. (Retinopathy is a lesion of the retina of the eyeball of any origin. The main cause is vascular disorders that lead to a disorder in the blood supply to the retina).
Also dysbiosis, since colonization of the intestine is not the same as in a full-term baby. Anemia is a lack of iron / hemoglobin, since the child receives the main amount in the 3rd trimester of pregnancy, and this child was born before that time. Almost every premature baby suffers from this condition. Reduced immunity as the microbiota cannot fully develop. Due to immaturity, retinopathy of the newborn develops, or such children are at risk for retinopathy, so they are observed by ophthalmologists according to a special schedule, they are removed from the register when the gestational age approaches 40 weeks, by which time the fundus is formed. (Retinopathy is a lesion of the retina of the eyeball of any origin. The main cause is vascular disorders that lead to a disorder in the blood supply to the retina).
Is prematurity a sentence? Will the child always get sick?
No, this is the state at the time of birth. Yes, these children will be with developmental disabilities, but they always have a head start. When we evaluate the psychomotor development of a child, we focus on his post-conceptual age, that is, he was born prematurely and should be like a child of 2 months of age, although his passport age is already 6 months.
When we evaluate the psychomotor development of a child, we focus on his post-conceptual age, that is, he was born prematurely and should be like a child of 2 months of age, although his passport age is already 6 months.
Over time, these kids are trimmed, everything is very individual. As a rule, by the age of 1.5 it is no longer possible to distinguish such a child from a full-term one. And those children who were born at 35-36 weeks, they can no longer be distinguished from an ordinary baby even in a year. We are now talking about the backlog of children who were born at a very early stage with very low or extremely low body weight.
How susceptible are these children to infections?
In different ways, sometimes such children are cared for in very comfortable conditions and, for example, if there are no older children in the family, then they may not get sick at all, but we are talking about the first year of life. If we take an older age, then these children need special supervision, so it all depends on what such a child is fed, breast milk is very important for strong immunity. Yes, these children will be at risk, this does not mean that they will get sick.
Yes, these children will be at risk, this does not mean that they will get sick.
How to properly feed premature babies? Are the timing of complementary foods shifting? What are the children fed in the couveuse?
As a rule, for such children, the ideal option is breastfeeding or native, native is formula, breast milk and formula. Such feeding is important, because we populate the flora of the child and his intestines begin to work and perform their function in nutrition, the intake of nutrients and the formation of immunity. For feeding premature babies, there are special mixtures that belong to the PRE group. These are mixtures for small premature babies with a higher concentration of proteins and fats, due to which children gain well in weight and equalize with the weight gain of full-term babies. The time of transfer to a regular formula is individual for each child; at each examination by a pediatrician, the doctor must calculate the amount of food. In the introduction of complementary foods, we focus on the post-conceptual age, for example, a child is 8 months old, a full-term baby at this age would already receive 3 meals of complementary foods, and in premature babies, we only introduce the first complementary foods, focusing on how ready the child is for its use.
Can they be vaccinated?
These children must be vaccinated, as their immunity is weaker. Usually they begin to vaccinate them in the hospital, and then, if there are no contraindications and the child is healthy, then they are vaccinated according to an individual vaccination schedule.
How are premature babies observed in Zdravitsa? What should mom do after being discharged from the hospital and what kind of help will she get here?
We have several programs for monitoring premature babies, depending on birth weight. Supervision programs include all necessary services for a child of this age. Of course, these children are special and they have their own individual observation schedule, which includes all the necessary specialists. The attending physician and the head of the department will monitor the well-being and development of the baby. Moreover, it can be both receptions at home and calling a specialist at home. Mandatory consultations of specialized children's specialists - an ophthalmologist, neurologist, cardiologist, surgeon, otorhinolaryngologist, orthopedist, pulmonologist, dentist, immunologist. Random people do not work in our children's department, our team consists of only highly qualified specialists with in-depth knowledge and extensive and successful practical experience. 14 pediatricians of our clinic completed a refresher course in gastroenterology, and all pediatricians, without exception, learned baby massage with a specialist. Now, at the reception, they can show parents a number of basic massage movements, exercises and exercise therapy techniques.
Random people do not work in our children's department, our team consists of only highly qualified specialists with in-depth knowledge and extensive and successful practical experience. 14 pediatricians of our clinic completed a refresher course in gastroenterology, and all pediatricians, without exception, learned baby massage with a specialist. Now, at the reception, they can show parents a number of basic massage movements, exercises and exercise therapy techniques.
Can a mother, while the child is still in the hospital, ask for help so that the doctor is always in touch with her?
Of course, it can, but in this case it is better not to buy the program yet, but just come to me for a consultation and then keep in touch. Or use the online consultation service. You need to understand that the doctor cannot influence the stages of observation and management of the child in the hospital, cannot influence his treatment. But a doctor can support a mother, advise on breastfeeding, prepare for the baby at home, prevent the risk of allergies, hypothermia, give advice on how to equip a nursery, and so on.
Is there a time in your history when you saw a premature baby and then he made some progress?
Yes, there are such stories, there was a case when a child was born with a weight of 600 grams, spent a long time in a children's hospital, during the examination it turned out that almost all body systems were involved in the pathological process she herself was scared how the child would get out of this state. But the parents believed in him, invested a lot of time and effort, there were various consultations of doctors and various interventions, as a result, at 1.5 years old, the child walked, was very active at the reception, rolled cars, looked at toys, tried to communicate, and not with the help of gestures that he had long mastered, but with the help of words, and this communication was conscious. Therefore, a very small premature baby is not always a sentence.
How can parents know if their child is developing normally?
It is necessary to be monitored regularly, in the first six months it is 2 times a month, then every month to go through all the narrow specialists, and if one of the doctors suspects that something has gone wrong, then it is necessary to intervene in a timely manner and not postpone treatment indefinitely.