Feet first birth
Causes, Complications, Turning & Delivery
Overview
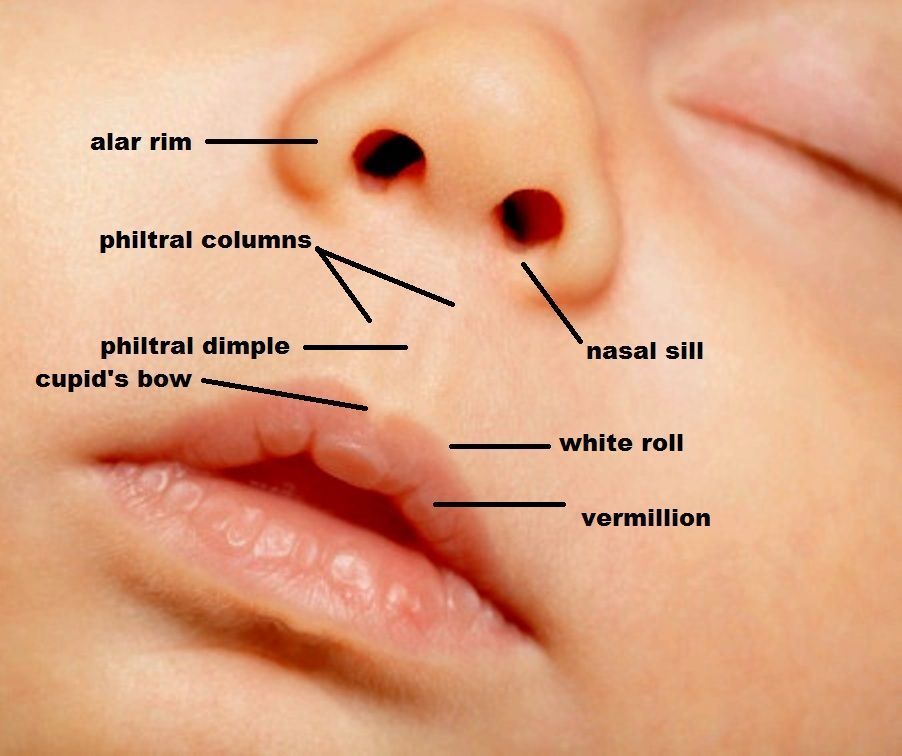
Types of breech positions during pregnancy.What is a breech baby?
A breech baby, or breech birth, is when your baby’s feet or buttocks are positioned to come out of your vagina first. Your baby’s head is up closest to your chest and its bottom is closest to your vagina. Most babies will naturally move so their head is positioned to come out of the vagina first during birth. Breech is common in early pregnancy and most babies will move to a head-first position by 36 weeks of pregnancy. This head-first position is called vertex presentation and is the safest position for birth.
How common is a breech baby?
There is a small chance that your baby will not move into a head-first position before 37 weeks of pregnancy. Breech babies account for about 3% to 4% of all full-term pregnancies.
What are the types of breech position a baby can be in?
There are several fetal positions your baby may present in. Ideally, your baby is positioned head-down, facing your back, with their chin tucked to their chest.
Breech babies can be in a few different positions:
- Frank breech: The baby’s buttocks are aimed at the vaginal canal with its legs sticking straight up in front of their body and the feet near their head.
- Complete breech: The baby’s buttocks are pointing downward and both the hips and the knees are flexed (folded under themselves).
- Footling breech: One or both of the baby’s feet point downward and will deliver before the rest of their body.
- Transverse lie: This is a form of breech presentation where your baby is positioned horizontally across your uterus instead of vertically. This would make their shoulder enter the vagina first.
How does a breech baby affect pregnancy?
Your pregnancy is usually not affected. Most breech babies are born healthy, although there is a slightly elevated risk for certain birth defects. Your baby’s movements may feel a little different. You will feel your baby’s kicks lower in your belly. You may feel a hard lump closer to your ribs. This is your baby’s head.
Your baby’s movements may feel a little different. You will feel your baby’s kicks lower in your belly. You may feel a hard lump closer to your ribs. This is your baby’s head.
If you planned a vaginal delivery, a breech baby could change these plans. When your baby is breech, a vaginal delivery can be complicated and dangerous. Your healthcare provider may feel comfortable attempting a vaginal breech delivery, but in most cases, they will recommend a Cesarean birth (C-section).
How does a breech baby affect delivery?
If your baby presents in a breech position after 36 weeks of pregnancy, your birthing plan will likely change. It's usually unsafe for a breech baby to be born vaginally due to risks of injury. In most cases, a planned C-section is the safest way to deliver your baby. Some healthcare providers may be comfortable with a vaginal breech birth. In some cases, turning your baby to a head-down position while they are still inside your uterus is an option. Your baby is then born head first.
Symptoms and Causes
How can you tell if your baby is breech?
You may be able to tell if your baby is breech, especially if you have had past pregnancies where your baby was head-first. The places where you feel lumps and kicks might indicate that your baby is breech. Let your healthcare provider know where you feel movement. They will feel your belly or do an ultrasound to confirm that your baby is breech.
What causes a baby to be breech?
It’s not always known why a baby is breech. Some factors that may contribute to this position are:
- You are expecting multiples (twins or more). This makes it harder for each baby to get into the right position.
- There is too much or too little amniotic fluid.
- The uterus is not normal in shape or has abnormal growths such as fibroids. Most of the time, the uterus is shaped like an upside-down pear. If it's shaped differently, there might not be enough room for a full-grown baby to move into position.

- The placenta covers all or part of the cervix (a condition called placenta previa).
- The baby is preterm. This means they are less than 37 weeks gestation and may not have turned to a head-first position.
- Your baby has a birth defect that causes them to not turn head-down.
Diagnosis and Tests
How is a breech baby diagnosed?
Your healthcare provider may be able to tell which way your baby is facing by placing their hands at certain places on your abdomen. By feeling where the baby’s head, back and buttocks are, it’s usually possible to find out what part of the baby is positioned to come out of the vagina first. An ultrasound may be used to confirm the baby’s position.
When is a breech baby diagnosed?
Almost all babies are breech at some point. As your pregnancy progresses, your baby will naturally move to a head-down position — probably between 32 and 36 weeks. Your healthcare provider will feel your belly and determine where your baby is positioned. This will happen during most of your appointments in the third trimester. After 37 weeks, a breech baby usually does not turn on their own. Your healthcare provider will discuss delivery options with you.
This will happen during most of your appointments in the third trimester. After 37 weeks, a breech baby usually does not turn on their own. Your healthcare provider will discuss delivery options with you.
Management and Treatment
What are the options for treating a breech baby?
If your baby is breech at 37 weeks of pregnancy, your healthcare provider may:
- Try turning your baby in your uterus into the head-first position.
- Plan a C-section birth.
- Plan a vaginal breech birth.
What are some complications of having a breech baby?
The complications of having a breech baby usually do not occur until it's time to deliver. Some breech babies can be safely delivered through the vagina.
The risks of attempting a vaginal breech birth are:
- Injuries to your baby’s legs or arms such as dislocated or broken bones.
- Umbilical cord problems. The umbilical cord can be flattened or twisted during delivery. This can cause nerve or brain damage due to a lack of oxygen.

Will my doctor try to flip my baby if it's breech?
If your baby is breech, your healthcare provider may consider turning your baby so that you can have a vaginal delivery. In some cases, trying to turn your baby may not be safe or the risks outweigh the benefits.
Flipping your baby may not be safe if you have any of the following:
- Bleeding from your vagina.
- Placenta previa. This is when your placenta covers all or part of your cervix.
- A nonreactive nonstress test.
- An abnormally small baby.
- Low level of amniotic fluid.
- Low or high fetal heart rate.
- Premature rupture of the membranes.
- Twins or multiples.
The most common method used to turn a breech baby is called external cephalic version (ECV). It's performed by your healthcare provider around 37 weeks of pregnancy. This procedure is performed in the hospital just in case an emergency occurs. It involves placing hands on your abdomen and applying firm pressure to turn your baby to a head-down position while your baby is still in your uterus. It is about 65% effective and carries some risks.
It is about 65% effective and carries some risks.
What are the risks of turning my breech baby?
The risks of ECV include the following:
- Premature labor.
- Premature rupture of the amniotic sac.
- Blood loss for either you or your baby.
- Emergency C-section.
- Your baby might turn back to the breech position.
Although the risk of having these complications is small, some healthcare providers prefer not to try to flip a breech baby.
Will my breech baby flip on their own?
Most babies will flip to a head-down position before they reach full term (37 weeks). If your baby is still in a breech position at this time, your healthcare provider will determine if you can deliver vaginally or if you will need a C-section.
How can I flip my baby if it's breech?
Some women will try at-home methods to flip their baby to a head-first position. They may help, but there is no scientific evidence that they work.
- Bridge position: Lie on the floor with your legs bent and your feet flat on the ground. Raise your hips and pelvis into a bridge position. Hold this position for 10 or 15 minutes several times a day.
- Child’s pose: Rest in the child’s pose for 10 to 15 minutes. It can help relax your pelvic muscles and uterus. You can also rock back and forth on your hands and knees or make circles with your pelvis to promote activity.
- Music: Place headphones or a speaker at the bottom of your uterus to encourage your baby to turn.
- Temperature: Try placing something cold at the top of your stomach where your baby’s head is. Then, place something warm at the bottom of your stomach.
A chiropractic technique, called the Webster technique, can also help your uterus relax. Some providers even recommend acupuncture. Both of these techniques need to be done by a professional that your healthcare provider has recommended.
Prevention
How can I reduce my risk of having a breech baby?
There is nothing you can do to prevent your baby from being in a breech position. If your baby is in a breech position, it’s not because you did anything wrong.
Outlook / Prognosis
Can you deliver vaginally with a baby breech?
It's possible to deliver a breech baby vaginally. It can be more dangerous for the baby and the risk of injury is much higher. If the umbilical cord is compressed during birth, the baby could be deprived of oxygen and this could harm their brain and nerves. The cord could also slip around the baby’s neck or arms, causing injury. Healthcare providers have various levels of comfort with vaginal deliveries of breech babies. Talk to your provider about the risks and benefits of different types of birth for a breech baby.
Living With
When should I see my healthcare provider?
Contact your healthcare provider if you experience any of the following symptoms during pregnancy:
- Severe cramping or contractions.

- Vaginal bleeding.
What questions should I ask my doctor?
Learning your baby is breech may give you concerns about your delivery. It’s completely natural to have questions. Some questions to ask your doctor can include:
- How can I tell if my baby is breech?
- Is my baby OK?
- What are the benefits and risks of turning my baby?
- What are my options for delivery if my baby remains in the breech position?
- What are the health risks to my baby and me if they are born breech?
Frequently Asked Questions
Do birth defects cause breech position?
Birth defects are slightly more common in breech babies. It might be the reason that the baby didn’t move to the head-down position. Most babies who are breech at delivery are born without any health complications.
Will I need a C-section if my baby is breech?
Most of the time, a C-section is the safest way to deliver a breech baby. Your risks of developing complications are much higher if you try to deliver a breech baby through the vagina. However, some healthcare providers may feel comfortable performing a vaginal breech birth.
However, some healthcare providers may feel comfortable performing a vaginal breech birth.
How does labor start if your baby is breech?
Having a breech baby doesn’t change some of the first signs of labor like contractions or rupturing of your membranes. In most cases, your healthcare provider will recommend a planned C-section. If your delivery is planned, you may not have any labor symptoms.
If you are in labor and go to the hospital for delivery, your provider will confirm your baby’s position a final time. Your provider could attempt a vaginal delivery, but it's more likely they will proceed with a C-section to be safe.
A note from Cleveland Clinic
Having a breech baby can be unexpected and change the vision you had for childbirth. Talk to your healthcare provider about what to expect during a breech delivery. They can help you understand the risks and benefits of a breech birth so that you and your baby are kept safe.
What happens if your baby is breech?
Babies often twist and turn during pregnancy, but most will have moved into the head-down (also known as head-first) position by the time labour begins. However, that does not always happen, and a baby may be:
However, that does not always happen, and a baby may be:
- bottom first or feet first (breech position)
- lying sideways (transverse position)
Bottom first or feet first (breech baby)
If your baby is lying bottom or feet first, they are in the breech position. If they're still breech at around 36 weeks' gestation, the obstetrician and midwife will discuss your options for a safe delivery.
Turning a breech baby
If your baby is in a breech position at 36 weeks, you'll usually be offered an external cephalic version (ECV). This is when a healthcare professional, such as an obstetrician, tries to turn the baby into a head-down position by applying pressure on your abdomen. It's a safe procedure, although it can be a bit uncomfortable. Around 50% of breech babies can be turned using ECV, allowing a vaginal birth.
Giving birth to a breech baby
If an ECV does not work, you'll need to discuss your options for a vaginal birth or caesarean section with your midwife and obstetrician.
If you plan a caesarean and then go into labour before the operation, your obstetrician will assess whether it's safe to proceed with the caesarean delivery. If the baby is close to being born, it may be safer for you to have a vaginal breech birth.
The Royal College of Obstetricians and Gynaecologists (RCOG) website has more information on what to expect if your baby is still breech at the end of pregnancy.
The RCOG advises against a vaginal breech delivery if:
- your baby's feet are below its bottom – known as a "footling breech"
- your baby is larger or smaller than average – your healthcare team will discuss this with you
- your baby is in a certain position – for example, their neck is very tilted back, which can make delivery of the head more difficult
- you have a low-lying placenta (placenta praevia)
- you have pre-eclampsia
Lying sideways (transverse baby)
If your baby is lying sideways across the womb, they are in the transverse position. Although many babies lie sideways early on in pregnancy, most turn themselves into the head-down position by the final trimester.
Although many babies lie sideways early on in pregnancy, most turn themselves into the head-down position by the final trimester.
Giving birth to a transverse baby
Depending on how many weeks pregnant you are when your baby is in a transverse position, you may be admitted to hospital. This is because of the very small risk of the umbilical cord coming out of your womb before your baby is born (cord prolapse). If this happens, it's a medical emergency and the baby must be delivered very quickly.
Sometimes, it's possible to manually turn the baby to a head-down position, and you may be offered this.
But, if your baby is still in the transverse position when you approach your due date or by the time labour begins, you'll most likely be advised to have a caesarean section.
Video: My baby is breech. What help will I get?
In this video, a midwife describes what a breech position is and what can be done if your baby is breech.
Media last reviewed: 3 February 2023
Media review due: 3 February 2026
Page last reviewed: 12 November 2020
Next review due: 12 November 2023
Harbingers - childbirth is coming soon!
Wrestler Maria Vladimirovna
Obstetrician-gynecologist
MD GROUP Clinical Hospital, Mother and Child Clinic Savelovskaya
False contractions
They may appear after the 38th week of pregnancy. False contractions are similar to Braxton-Hicks contractions, which a woman could already feel starting from the second trimester of pregnancy (the uterus seems to stiffen for a few seconds - a couple of minutes, then the tension in it subsides). False contractions train the uterus before childbirth, they are irregular and painless, the intervals between them are not reduced. Real labor pains, on the contrary, are regular, their strength gradually increases, they become longer and more painful, and the intervals between them are reduced. That's when you can already say that the birth began for real. In the meantime, false contractions are going on, it is not necessary to go to the maternity hospital - you can easily survive them at home.
That's when you can already say that the birth began for real. In the meantime, false contractions are going on, it is not necessary to go to the maternity hospital - you can easily survive them at home.
Abdominal prolapse
Approximately two to three weeks before birth, the baby, in preparation for birth, presses the presenting part (usually the head) against the lower part of the uterus and pulls it down. As a result, the uterus moves lower into the pelvic region, its upper part ceases to put pressure on the internal organs of the chest and abdominal cavity. In the people it is called - the stomach dropped. As soon as the stomach drops, the expectant mother notices that it has become easier for her to breathe, but, on the contrary, it becomes more difficult to sit and walk. Heartburn and belching also disappear (after all, the uterus no longer presses on the diaphragm and stomach). But, having dropped down, the uterus begins to put pressure on the bladder - naturally, urination becomes more frequent.
For some, uterine prolapse causes a feeling of heaviness in the lower abdomen and even slight pain in the area of the inguinal ligaments. These sensations arise due to the fact that the child's head, moving down, irritates the nerve endings of the pelvic organs.
During the second and subsequent births, the belly drops later - right before the birth. It happens that this harbinger of childbirth is not at all.
Removal of the mucous plug
This is one of the main and obvious harbingers of childbirth. During pregnancy, the glands in the cervix produce a secret (it looks like a thick jelly and forms the so-called cork), which prevents various microorganisms from entering the uterine cavity. Before childbirth, under the influence of estrogens, the cervix softens, the cervical canal opens slightly and the cork can come out - the woman will see that there are mucus clots on the linen that look like jelly. Cork can be of different colors - white, transparent, yellowish-brown or pink-red. Often it is stained with blood - this is completely normal and may indicate that childbirth will occur within the next day. The mucus plug can come out all at once (at once) or come out piecemeal throughout the day.
Often it is stained with blood - this is completely normal and may indicate that childbirth will occur within the next day. The mucus plug can come out all at once (at once) or come out piecemeal throughout the day.
Weight loss
Approximately two weeks before delivery, weight loss may occur, usually by 0.5–2 kg. This happens because excess fluid is removed from the body and swelling decreases. If earlier during pregnancy, under the influence of the hormone progesterone, fluid in the body of a pregnant woman accumulated, now, before childbirth, the effect of progesterone decreases, but other female sex hormones - estrogens - begin to work hard, they remove excess fluid from the body of the expectant mother.
In addition, the expectant mother often notices that at the end of pregnancy it became easier for her to put on rings, gloves, shoes - this means that swelling on the hands and feet has decreased.
Change of stool
Right before childbirth, hormones often act on the intestines - they relax its muscles, as a result, stool disorder begins. Sometimes such frequent (up to 2-3 times a day) and even loose stools are mistaken for an intestinal infection. But if there is no nausea, vomiting, discoloration and smell of feces, or any other symptoms of intoxication, you should not worry: this is one of the harbingers of the upcoming birth.
Sometimes such frequent (up to 2-3 times a day) and even loose stools are mistaken for an intestinal infection. But if there is no nausea, vomiting, discoloration and smell of feces, or any other symptoms of intoxication, you should not worry: this is one of the harbingers of the upcoming birth.
And on the eve of childbirth, you often don't feel like eating at all. All this is also the preparation of the body for natural childbirth.
Mood changes
Many women experience mood changes a few days before giving birth. The expectant mother gets tired quickly, she wants to have more rest, sleep, even some kind of apathy appears. This state is quite understandable - you need to gather strength to prepare for childbirth. Often, just before giving birth, a woman wants to retire, looking for a secluded place where you can hide and focus on yourself and your experiences.
What should I do if there are any signs of childbirth? Usually you don’t need to do anything, because the harbingers are completely natural, they just say that the body is rebuilding and preparing for the birth of a child. Therefore, you should not worry and go to the hospital as soon as, for example, training contractions have begun or the mucous plug has come off. We must wait for real labor pains or outpouring of water.
Therefore, you should not worry and go to the hospital as soon as, for example, training contractions have begun or the mucous plug has come off. We must wait for real labor pains or outpouring of water.
Make an appointment
to the doctor - Borets Maria Vladimirovna
By clicking on the send button, I consent to the processing of personal data
01/26/2018
IVF failures: embryological stage
Wrestler Maria Vladimirovna
Harbingers of childbirth. How do you know when it's time to go to the hospital?
January 10, 2017
Alekseeva Inna
Obstetrician-gynecologist, Doctor of the highest category
Subscribe to our Instagram! Useful information about pregnancy and childbirth from leading obstetricians and gynecologists in Moscow and foreign experts: https://www.instagram.com/roddompravda/
Tips and opinions from leading child professionals: https://www. instagram.com/emc.child/
instagram.com/emc.child/
Every pregnant woman with excitement and joy awaits the upcoming birth. The closer the cherished date, the more attentively the expectant mother listens to the changes taking place in her body and in the behavior of the baby. Of course, the expectant mother wants to know by what signs it is possible to understand that childbirth is just around the corner.
It is customary to call the harbingers of childbirth external, really tangible changes in the body, which are direct preparation for the onset of labor. The tissues of the birth canal - the cervix, vagina, vulva, perineum - become quite elastic, extensible, but at the same time - very strong and resistant to tearing. The cervix is located in the center of the vaginal vault, shortens by almost half its normal length and softens significantly. The cervical canal - the lumen of the cervix connecting the uterine cavity with the vagina - opens slightly, as a result, the diameter of the cervical canal is approximately 2-2. 5 cm. Of course, such a significant "perestroika" takes more than one day.
5 cm. Of course, such a significant "perestroika" takes more than one day.
Female sex hormones are responsible for preparing for childbirth. During the nine months of pregnancy, progesterone "reigns" in the body of the expectant mother. It ensures the normal tone of the uterus (relaxed state of the muscles), the production of cervical mucus - a mucous plug in the cervix that protects the fetus from infection. The amount of progesterone during pregnancy largely determines the normal development and growth of the fetus, the necessary concentration of nutrients and oxygen in the mother's blood, as well as their timely and uninterrupted delivery to the baby.
Shortly before childbirth, the production of progesterone decreases markedly, it is replaced by estrogens - female sex hormones. The increase in estrogen in the blood is caused by the need to prepare the body for the upcoming birth. It is these hormones that are responsible for the elasticity and patency of the birth canal. The rate of cervical dilatation in the first stage of labor depends on them. In the second period, when the cervix is fully opened and the fetus passes through the birth canal, it is also very important how elastic and extensible the walls of the vagina are - this will largely determine the duration of the straining period. Finally, the onset of labor itself depends on the level of estrogen: contractions occur as a result of a nerve impulse that is caused by a certain level (“peak”) of estrogen accumulation.
The rate of cervical dilatation in the first stage of labor depends on them. In the second period, when the cervix is fully opened and the fetus passes through the birth canal, it is also very important how elastic and extensible the walls of the vagina are - this will largely determine the duration of the straining period. Finally, the onset of labor itself depends on the level of estrogen: contractions occur as a result of a nerve impulse that is caused by a certain level (“peak”) of estrogen accumulation.
These changes are normal and do not require an unscheduled visit to the doctor or hospitalization. Harbingers of childbirth are manifestations of a planned restructuring in the body of a future mother, the “finishing touches” of preparation for the upcoming joyful event.
The absence of clearly perceptible changes on the eve of the expected date of birth is also not a pathology. Not all expectant mothers note those changes in well-being that are commonly called harbingers. However, this does not mean that there is no preparation. In some cases, the “final preparations” go unnoticed by the pregnant woman. Therefore, do not worry or urgently contact a specialist.
However, this does not mean that there is no preparation. In some cases, the “final preparations” go unnoticed by the pregnant woman. Therefore, do not worry or urgently contact a specialist.
The appearance of any of the "harbingers" indicates the likelihood of the development of regular labor activity over the next two hours - two weeks. None of the sensations described gives a 100% guarantee that a woman will become a mother within the next 24 hours. Hormonal changes before childbirth begin approximately two weeks before the expected birth. Theoretically, during these two weeks, at any time, a pregnant woman can notice certain changes in her state of health. Consequently, the absence of labor activity an hour, a day, or even a week after the first noted changes is not a pathology and does not require special medical advice.
- Scarlet discharge from the genital tract in any amount.
- Severe abdominal pain.
- Increased blood pressure (above 130/80 mmHg).

- An increase in body temperature to 37.5 ° C and above.
- Increased heart rate (more than 100 beats per minute).
- Severe headache, vomiting, blurred vision.
- Significant increase in edema.
- Absence, sharp decrease, sharp increase in fetal movements.
- Suspicion of amniotic fluid leakage.
Weight loss . Shortly before the expected date of delivery, the expectant mother may notice some “weight loss”. Weight loss during this period is associated with the removal of excess fluid from the body, that is, a general decrease in edema. The more pronounced the fluid retention during pregnancy, the more mass the pregnant woman will “lose” on the eve of childbirth. During pregnancy, water is retained in the body of all expectant mothers to a greater or lesser extent. The reason is progesterone - a hormone whose main function is to support the processes of pregnancy. Before childbirth, progesterone is replaced by estrogen. It is estrogen that removes excess fluid from the body. The first results are visible on the hands, feet and legs. Depending on the severity of edema, weight loss before childbirth varies from 0.5 to 2.5 kg.
Before childbirth, progesterone is replaced by estrogen. It is estrogen that removes excess fluid from the body. The first results are visible on the hands, feet and legs. Depending on the severity of edema, weight loss before childbirth varies from 0.5 to 2.5 kg.
Change of stool. Increased frequency and change in the consistency of physiological functions on the eve of childbirth is also associated with an increase in estrogen levels and the removal of fluid from the body of the expectant mother. Similar changes in the body of a non-pregnant woman are observed during menstruation. The chair can become more frequent up to 2-3 times a day, at the same time there may be some liquefaction of the feces. More frequent urge to defecate, a sharp change in the color and smell of feces, combined with nausea and vomiting, is a reason for consulting a doctor - food poisoning can be masked under such "harbingers".
Fundal prolapse. Shortly before delivery, the baby presses the presenting part (most often the head) against the lower segment of the uterus and pulls it down, pressing against the entrance to the small pelvis. The fetus "groups", taking the most advantageous position for itself at the time of the onset of contractions. As a result of such "preparations" from the side of the fetus, the uterus "sags", and its upper part - the bottom - ceases to exert pressure on the internal organs. After lowering the bottom of the uterus, the pregnant woman has no shortness of breath (it becomes easier to breathe, there is a feeling of a full breath). If in the last month the expectant mother had belching, heartburn, a feeling of heaviness in the stomach after eating, these phenomena disappear when the bottom of the uterus descends. However, lowering down to the pelvic area, the uterus will put more pressure on the internal organs located there. The pelvic organs, in particular, include the bladder. It is located directly in front of the uterus, in its lower part.
Shortly before delivery, the baby presses the presenting part (most often the head) against the lower segment of the uterus and pulls it down, pressing against the entrance to the small pelvis. The fetus "groups", taking the most advantageous position for itself at the time of the onset of contractions. As a result of such "preparations" from the side of the fetus, the uterus "sags", and its upper part - the bottom - ceases to exert pressure on the internal organs. After lowering the bottom of the uterus, the pregnant woman has no shortness of breath (it becomes easier to breathe, there is a feeling of a full breath). If in the last month the expectant mother had belching, heartburn, a feeling of heaviness in the stomach after eating, these phenomena disappear when the bottom of the uterus descends. However, lowering down to the pelvic area, the uterus will put more pressure on the internal organs located there. The pelvic organs, in particular, include the bladder. It is located directly in front of the uterus, in its lower part. Behind the uterus, at a distance of several centimeters, there is an ampulla of the rectum - the output section of the intestine. It is not difficult to guess what the result of pressure on the bladder and rectum will be: the urge to go to the toilet before childbirth can become noticeably more frequent.
Behind the uterus, at a distance of several centimeters, there is an ampulla of the rectum - the output section of the intestine. It is not difficult to guess what the result of pressure on the bladder and rectum will be: the urge to go to the toilet before childbirth can become noticeably more frequent.
Isolation of the mucous plug. During pregnancy, the glands of the mucous membrane of the cervical canal (the lumen of the cervix) secrete a special secret. It is a thick, sticky, jelly-like mass that forms a kind of cork. The mucous plug completely fills the cervical canal, preventing the penetration of bacterial flora from the vagina into the uterine cavity. Thus, cervical mucus, or the mucous plug of the cervix, protects the fetus from ascending infection. Before childbirth, when the cervix begins to soften under the influence of estrogen, the cervical canal opens slightly and the cervical mucus contained in it can be released. In this case, the expectant mother may find small clots of yellowish-brownish mucus, transparent, jelly-like, odorless. The mucous plug can stand out at once or depart in parts during the day. In the latter case, slight discomfort is sometimes noted in the form of "sipping" in the lower abdomen, reminiscent of sensations before or during menstruation. However, most often, the release of the mucous plug is not accompanied by tangible changes in the well-being of the expectant mother. After the discharge of the mucous plug, it is not recommended to visit the pool, swim in the reservoirs and in the bath. When immersed in water, it fills the vagina; thus, in the absence of a mucous plug, the risk of infection of the fetus and membranes through the ajar cervix increases.
The mucous plug can stand out at once or depart in parts during the day. In the latter case, slight discomfort is sometimes noted in the form of "sipping" in the lower abdomen, reminiscent of sensations before or during menstruation. However, most often, the release of the mucous plug is not accompanied by tangible changes in the well-being of the expectant mother. After the discharge of the mucous plug, it is not recommended to visit the pool, swim in the reservoirs and in the bath. When immersed in water, it fills the vagina; thus, in the absence of a mucous plug, the risk of infection of the fetus and membranes through the ajar cervix increases.
Training contractions. Training or false contractions are called such contractions that appear shortly before childbirth and are not actually labor activity, since they do not lead to the opening of the cervix. A contraction is essentially a single contraction of the uterine wall; this contraction usually lasts a few seconds. At the time of the contraction, the expectant mother feels a gradually increasing and then gradually decreasing tension in the abdomen. If at this moment you put your hand on your stomach, you can notice that the stomach becomes very hard, but after the contraction it completely relaxes and becomes soft again. In addition to involuntary tension of the uterus, other changes in the well-being of the expectant mother during false contractions are usually not noted. It is not difficult to distinguish training fights from real ones. In most cases, false contractions are weak, painless, irregular or alternating at a significant interval (30 minutes or more). Labor pains, on the contrary, are distinguished by regularity and a gradual increase in intensity. Unlike false contractions, real contractions lead to a visible result - the opening of the cervix. In doubtful cases, a simple obstetric examination will be enough to make an accurate diagnosis. In other cases, training contractions, like all harbingers of childbirth, do not require a visit to a doctor or hospitalization.
At the time of the contraction, the expectant mother feels a gradually increasing and then gradually decreasing tension in the abdomen. If at this moment you put your hand on your stomach, you can notice that the stomach becomes very hard, but after the contraction it completely relaxes and becomes soft again. In addition to involuntary tension of the uterus, other changes in the well-being of the expectant mother during false contractions are usually not noted. It is not difficult to distinguish training fights from real ones. In most cases, false contractions are weak, painless, irregular or alternating at a significant interval (30 minutes or more). Labor pains, on the contrary, are distinguished by regularity and a gradual increase in intensity. Unlike false contractions, real contractions lead to a visible result - the opening of the cervix. In doubtful cases, a simple obstetric examination will be enough to make an accurate diagnosis. In other cases, training contractions, like all harbingers of childbirth, do not require a visit to a doctor or hospitalization. False contractions may recur for several hours and then stop. Most often, they disturb a pregnant woman in the evening and morning hours for several days.
False contractions may recur for several hours and then stop. Most often, they disturb a pregnant woman in the evening and morning hours for several days.
Discomfort. In the last weeks before giving birth, many pregnant women report discomfort in the lower abdomen and in the area of the sacrum (the area slightly below the waist). Such changes in
the well-being of the expectant mother is caused by sprain of the pelvic ligaments and increased blood flow to the pelvic organs. Usually these minor sensations, described as a feeling of "light languor" in the lower abdomen, are comparable to similar phenomena in the period before or during menstruation. Discomfort, like training contractions, more often disturbs the expectant mother in the morning and evening hours. The level of discomfort is minimal, it should not worry the expectant mother and does not require medical intervention.
All harbingers of childbirth can appear during the last two weeks before childbirth, their presence, as well as their absence, is the norm and does not require a visit to a doctor.