What is being induced
Labor induction - Mayo Clinic
Overview
Labor induction — also known as inducing labor — is prompting the uterus to contract during pregnancy before labor begins on its own for a vaginal birth.
A health care provider might recommend inducing labor for various reasons, primarily when there's concern for the mother's or baby's health. An important factor in predicting whether an induction will succeed is how soft and expanded the cervix is (cervical ripening). The gestational age of the baby as confirmed by early, regular ultrasounds also is important.
If a health care provider recommends labor induction, it's typically because the benefits outweigh the risks. If you're pregnant, understanding why and how labor induction is done can help you prepare.
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Book: Mayo Clinic Guide to a Healthy Pregnancy
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Why it's done
To determine if labor induction is necessary, a health care provider will likely evaluate several factors. These include the mother's health and the status of the cervix. They also include the baby's health, gestational age, weight, size and position in the uterus. Reasons to induce labor include:
- Nearing 1 to 2 weeks beyond the due date without labor starting (postterm pregnancy).
- When labor doesn't begin after the water breaks (prelabor rupture of membranes).
- An infection in the uterus (chorioamnionitis).
- When the baby's estimated weight is less than the 10th percentile for gestational age (fetal growth restriction).
- When there's not enough amniotic fluid surrounding the baby (oligohydramnios).
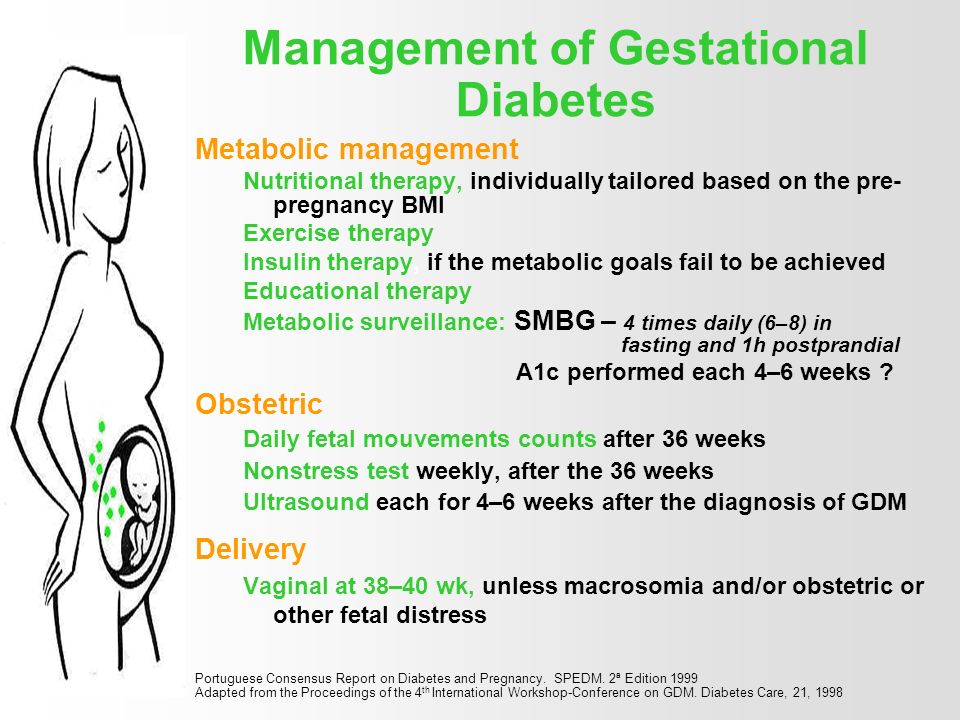
- Possibly when diabetes develops during pregnancy (gestational diabetes), or diabetes exists before pregnancy.
- Developing high blood pressure in combination with signs of damage to another organ system (preeclampsia) during pregnancy. Or having high blood pressure before pregnancy, developing it before 20 weeks of pregnancy (chronic high blood pressure) or developing the condition after 20 weeks of pregnancy (gestational hypertension).
- When the placenta peels away from the inner wall of the uterus before delivery — either partially or completely (placental abruption).
- Having certain medical conditions. These include heart, lung or kidney disease and obesity.
Elective labor induction is the starting of labor for convenience when there's no medical need. It can be useful for women who live far from the hospital or birthing center or who have a history of fast deliveries.
A scheduled induction might help avoid delivery without help. In such cases, a health care provider will confirm that the baby's gestational age is at least 39 weeks or older before induction to reduce the risk of health problems for the baby.
As a result of recent studies, women with low-risk pregnancies are being offered labor induction at 39 to 40 weeks. Research shows that inducing labor at this time reduces several risks, including having a stillbirth, having a large baby and developing high blood pressure as the pregnancy goes on. It's important that women and their providers share in decisions to induce labor at 39 to 40 weeks.
It's important that women and their providers share in decisions to induce labor at 39 to 40 weeks.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health. Click here for an email preview.
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Risks
Uterine incisions used during C-sections
Uterine incisions used during C-sections
A C-section includes an abdominal incision and a uterine incision. After the abdominal incision, the health care provider will make an incision in the uterus. Low transverse incisions are the most common (top left).
Labor induction carries various risks, including:
- Failed induction. An induction might be considered failed if the methods used don't result in a vaginal delivery after 24 or more hours. In such cases, a C-section might be necessary.
- Low fetal heart rate. The medications used to induce labor — oxytocin or a prostaglandin — might cause the uterus to contract too much, which can lessen the baby's oxygen supply and lower the baby's heart rate.
- Infection. Some methods of labor induction, such as rupturing the membranes, might increase the risk of infection for both mother and baby. The longer the time between membrane rupture and labor, the higher the risk of an infection.
-
Uterine rupture. This is a rare but serious complication in which the uterus tears along the scar line from a prior C-section or major uterine surgery. Rarely, uterine rupture can also occur in women who have not had previous uterine surgery.
An emergency C-section is needed to prevent life-threatening complications. The uterus might need to be removed.
- Bleeding after delivery. Labor induction increases the risk that the uterine muscles won't properly contract after giving birth, which can lead to serious bleeding after delivery.
Labor induction isn't for everyone. It might not be an option if:
- You've had a C-section with a classical incision or major uterine surgery
- The placenta is blocking the cervix (placenta previa)
- Your baby is lying buttocks first (breech) or sideways (transverse lie)
- You have an active genital herpes infection
- The umbilical cord slips into the vagina before delivery (umbilical cord prolapse)
If you have had a C-section and have labor induced, your health care provider is likely to avoid certain medications to reduce the risk of uterine rupture.
How you prepare
Labor induction is typically done in a hospital or birthing center. That's because mother and baby can be monitored there, and labor and delivery services are readily available.
What you can expect
During the procedure
There are various ways of inducing labor. Depending on the circumstances, the health care provider might use one of the following ways or a combination of them. The provider might:
-
Ripen the cervix. Sometimes prostaglandins, versions of chemicals the body naturally produces, are placed inside the vagina or taken by mouth to thin or soften (ripen) the cervix. After prostaglandin use, the contractions and the baby's heart rate are monitored.
In other cases, a small tube (catheter) with an inflatable balloon on the end is inserted into the cervix. Filling the balloon with saline and resting it against the inside of the cervix helps ripen the cervix.
- Sweep the membranes of the amniotic sac.
 With this technique, also known as stripping the membranes, the health care provider sweeps a gloved finger over the covering of the amniotic sac near the fetus. This separates the sac from the cervix and the lower uterine wall, which might help start labor.
With this technique, also known as stripping the membranes, the health care provider sweeps a gloved finger over the covering of the amniotic sac near the fetus. This separates the sac from the cervix and the lower uterine wall, which might help start labor. -
Rupture the amniotic sac. With this technique, also known as an amniotomy, the health care provider makes a small opening in the amniotic sac. The hole causes the water to break, which might help labor go forward.
An amniotomy is done only if the cervix is partially dilated and thinned, and the baby's head is deep in the pelvis. The baby's heart rate is monitored before and after the procedure.
- Inject a medication into a vein. In the hospital, a health care provider might inject a version of oxytocin (Pitocin) — a hormone that causes the uterus to contract — into a vein. Oxytocin is more effective at speeding up labor that has already begun than it is as at cervical ripening.
 The provider monitors contractions and the baby's heart rate.
The provider monitors contractions and the baby's heart rate.
How long it takes for labor to start depends on how ripe the cervix is when the induction starts, the induction techniques used and how the body responds to them. It can take minutes to hours.
After the procedure
In most cases, labor induction leads to a vaginal birth. A failed induction, one in which the procedure doesn't lead to a vaginal birth, might require another induction or a C-section.
By Mayo Clinic Staff
Related
Products & Services
I’m Being Induced! What Should I Expect?
Home / Community / News Releases / Maternity / I’m Being Induced! What Should I Expect?
Posted on
The goal of any healthcare practitioner is to carry all pregnancies to term, or 39 weeks. This means that generally speaking, labor shouldn’t be induced electively before that time—however, certain situations can come up when your body’s natural processes need a little nudge in the right direction.
Being induced simply means that your labor contractions are started using medications or other methods because they aren’t starting naturally. There are a series of steps your doctor will follow to try to induce your labor, and most women don’t have to go through all of them!
Reasons Your Doctor Might Induce LaborYour baby is overdue.
If it’s time for your baby to make their debut, but there are no signs of action from your body, your doctor might induce labor around the 42-week mark.
You’re experiencing complications.
Conditions like preeclampsia, diabetes or gestational diabetes, issues with your placenta, or problems with your amniotic fluid make it risky to keep carrying your pregnancy. Your doctor may choose to induce your labor as soon as it’s safe to reduce the effects of these risks.
Broken water, but no contractions.
If your water has broken, but your contractions don’t start on their own within 24 hours, your doctor might need to get them started for you.
You live far from the hospital.
If you live far away from your hospital, your doctor might choose to induce labor to minimize the risk of not making it in time. On average, second-time moms experience much shorter labor than they did during their first time—so if your first baby came very quickly, your doctor might decide to induce your second to make sure you’re at the hospital when you need to be. This is known as an elective induction because it’s planned ahead of time and occurs no earlier than 39 weeks.
How Does It Work?As mentioned above, there are a series of steps your doctor will go through to induce your labor. It’s fairly rare that a doctor has to go through every step to jumpstart your labor, but it is possible.
The first thing your doctor will try is ripening your cervix. Typically in natural labor, your cervix will open up, soften, and thin out in preparation for your baby. Your doctor might have to move things alone themselves, and they’ll do this by applying a topical form of the hormone prostaglandin to your cervix. After a few hours, labor could be well on its way—if it isn’t, your doctor will continue down the chain of steps toward successfully inducing your labor.
After a few hours, labor could be well on its way—if it isn’t, your doctor will continue down the chain of steps toward successfully inducing your labor.
If your amniotic sac is still intact, meaning your water hasn’t broken, your doctor may get things started by swiping their finger across the fine membranes that connect it—the goal here isn’t to break your water, although that’s a possibility. Your doctor’s goal is to encourage your uterus to release prostaglandin as you would naturally if your labor was starting. This should cause your cervix to soften, and your contractions to start. This is called “membrane stripping.”
If your cervix has started dilating, but your water hasn’t broken yet, your doctor might break it artificially. They’ll do this with an instrument that looks like a long crochet hook with a sharp tip—but don’t worry, while it might not be the most comfortable experience, it shouldn’t be painful.
If nothing your doctor tries is bringing on regular contractions, they will slowly start to give you Pitocin via IV. Pitocin is a synthetic form of the naturally occurring hormone oxytocin and should induce contractions. Contractions typically start about 30 minutes after you’ve been given the medication, and they’re usually stronger, more regular, and more frequent than natural labor contractions. If you’d like an epidural, you should ask your doctor about getting that started while the Pitocin is being administered, so that it’s ready to go once your labor starts.
Pitocin is a synthetic form of the naturally occurring hormone oxytocin and should induce contractions. Contractions typically start about 30 minutes after you’ve been given the medication, and they’re usually stronger, more regular, and more frequent than natural labor contractions. If you’d like an epidural, you should ask your doctor about getting that started while the Pitocin is being administered, so that it’s ready to go once your labor starts.
There are exceptions to every rule when it comes to pregnancy and the human body, which means that there are certain situations where labor shouldn’t be induced—in these situations, your doctor will recommend a c-section instead. Here are a few reasons you might have a c-section instead of being induced:
- If there’s a need for immediate delivery, i.e. there’s no time to waste
- If there’s any doubt at all that your baby can fit through your pelvis
- If you’ve had a c-section before, and now you’re attempting a vaginal birth
- If the placenta is near or covering your cervix
- If there’s a prolapsed cord, i.
 e. it has slipped down into the vagina before the baby’s head
e. it has slipped down into the vagina before the baby’s head - If you’re experiencing a genital herpes outbreak
- If you’re carrying multiple babies
- If your baby is breech
Keep in mind that your doctor’s goal is to minimize interventions as best they can, and will only induce your labor or recommend a c-section if they decide it’s necessary.
Looking for more pregnancy advice? Visit our website today.
Chapter 19. Conductors and dielectrics in an electric field
The school physics course has a section on the electrical properties of conductors and dielectrics and their behavior in an external electric field. The necessary minimum knowledge on this issue includes an understanding of the phenomenon of electrostatic induction and its mechanisms in conductors and dielectrics, as well as the ability to find charges induced in conductors and dielectrics in the simplest situations. Let's briefly consider these questions.
Atoms are composed of charged particles (electrons and protons). Therefore, any body contains a huge amount of charges. The number of protons and the number of electrons in an uncharged body is the same, a charged body contains different numbers of protons and electrons.
Therefore, any body contains a huge amount of charges. The number of protons and the number of electrons in an uncharged body is the same, a charged body contains different numbers of protons and electrons.
Depending on whether the charges inside the body are free or bound, all substances are divided into conductors, dielectrics (or insulators) and semiconductors. In conductors, electric charges can move freely, and therefore such bodies conduct electric current. Conductors include all metals in which the charge carriers are valence electrons (free electrons) that have “torn off” atoms, as well as electrolyte solutions (acids, alkalis and salts), in which positive and negative ions move.
In dielectrics, all charges are “attached” to atoms at rest and cannot move. Therefore, dielectrics do not conduct electricity. Dielectrics, for example, include: gases, plastics, ebonite, rubber, distilled water.
Substances that are intermediate in their conductivity between conductors and dielectrics are called semiconductors. Typical semiconductors are crystalline germanium and silicon. There are free charge carriers in semiconductors, but they are few. One should not, however, think that semiconductors are simply "bad" conductors or "bad" insulators. The intermediate conductivity of semiconductors leads to many of their unusual properties that distinguish semiconductors from both conductors and dielectrics. These properties are associated with many applications of semiconductors in engineering.
Typical semiconductors are crystalline germanium and silicon. There are free charge carriers in semiconductors, but they are few. One should not, however, think that semiconductors are simply "bad" conductors or "bad" insulators. The intermediate conductivity of semiconductors leads to many of their unusual properties that distinguish semiconductors from both conductors and dielectrics. These properties are associated with many applications of semiconductors in engineering.
When a conductor is placed in an electric field, free charge carriers move inside the conductor and regions of positive and negative charge are formed on its surface. This phenomenon of charge separation in a conductor under the action of an external electric field is called electrostatic induction or conductor polarization. As a result of polarization, the electric field in space changes and becomes equal to the sum of the external field and the field of induced charges. It can be proved that the movement of charges in the conductor will occur until the total field inside the conductor becomes zero, and on its surface - perpendicular to the surface.
This property of a conductor makes it possible to find the charges induced on its surface. To do this, you need to enter these charges as some unknown quantities, then find the field created by these charges and the total field equal to the vector sum of the external field and the field of induced charges, equate the total field inside the conductor to zero. The solution of the resulting equation will allow us to find the induced charges.
Polarization also occurs in a dielectric, but the mechanisms of this phenomenon are different. As a rule, dielectric molecules are polar, i.e. some area of the molecule is positively charged, some is negatively charged. When a dielectric is placed in an external field, the molecules turn, and their positive regions “go out” to certain parts of the dielectric surface, and their negative ones to others. As a result, regions of positive and negative charge are formed on the surface of the dielectric, but when cutting the dielectric (as opposed to cutting the conductor), the resulting parts will be uncharged. Due to the polarization of the dielectric, the field in it is weakened, but does not become equal to zero. Dielectric characteristic, which shows how many times the field is weakened in it, is called dielectric constant.
Due to the polarization of the dielectric, the field in it is weakened, but does not become equal to zero. Dielectric characteristic, which shows how many times the field is weakened in it, is called dielectric constant.
Let's consider the problems of the first part within the framework of this factual material.
In problem 19.1.1 from the list of substances listed below, the conductor of electric current is metal - lead (answer 3 ).
In problem 19.1.2 , chalk is a dielectric (answer 1 ; aluminum and iron are metals, i.e. current conductors, various salts are dissolved in tap water in such an amount that it is an excellent conductor of electric current).
As noted earlier, when a metallic body is introduced into an electric field ( task 19.1.3 ), electric charges are induced on the surface of the body, the sum of which is equal to zero. All other proposed answers are incorrect: in order to acquire an electric charge, the body needs to be given or taken away from it electrons, charges cannot be induced in the volume of the conductor - they cannot be kept there.
Interaction between a charge and an uncharged dielectric body occurs ( problem 19.1.4 ), and this interaction is attraction (answer 2 ). This interaction arises due to polarization: due to the orientation of the dielectric molecules, the part of the body surface facing the charge acquires a charge of the opposite sign, the part of the body surface far from the charge acquires a charge of the same sign (see figure).
|
|
Therefore, two forces will arise - the attraction of close sections and the repulsion of distant ones. But since the induced charges are the same in magnitude, and the Coulomb interaction decreases with increasing distance, the attraction is stronger than the repulsion, and the body will be attracted to the charge.
| As stated in the introduction to this chapter, parts of a metal body brought into an electric field and cut there ( task 19. |
 1.5 ) will be charged. Since the direction of the tension vector coincides with the direction of the force acting on the positive charge, part will be positively charged, part negatively (answer 2 ). If the body is a dielectric, then its parts will be uncharged ( task 19.1.6 - answer 1 ).
1.5 ) will be charged. Since the direction of the tension vector coincides with the direction of the force acting on the positive charge, part will be positively charged, part negatively (answer 2 ). If the body is a dielectric, then its parts will be uncharged ( task 19.1.6 - answer 1 ). | When a conducting body is introduced into an electric field ( task 19.1.7 ) all three phenomena listed as possible answers to the problem will take place. Points (1) and (3) (“the field inside the conductor is zero” and “the field on the surface is perpendicular to the surface”) were discussed in the introduction to this chapter. Let us prove that the potential is the same at all points of the body. To do this, let's take a point test charge and mentally transfer it from one point of the body to another (see the figure; the trajectory of the charge is shown by a dotted line). On the one hand, with such a motion, the field will do work , where and are the potentials of the initial and final points of the body's trajectory. |
 On the other hand, since the field strength inside the conducting body is zero, this work is zero. Therefore (the correct answer in the problem is 4 ). Similarly, in problem 19.1.8 (answer , 3 ).
On the other hand, since the field strength inside the conducting body is zero, this work is zero. Therefore (the correct answer in the problem is 4 ). Similarly, in problem 19.1.8 (answer , 3 ). After connecting with a conductor ( task 19.1.9 ) two metal bodies and the connecting conductor will be a single conducting body. Therefore, the potentials of any points of this body must be the same. Consequently, the potentials of the spheres will equalize (answer 1 ).
In problems with grounding ( problem 19.1.10 ) the following model of the Earth is considered: it is a conducting ball with dimensions much larger than the dimensions of any bodies present in the problem. Therefore, for the Earth's potential, we can use the formula (18.8), which for any charges with which we are dealing, gives a zero result. Therefore, when the body is grounded, its potential becomes equal to zero (answer 2 ).
The force of interaction of opposite electric charges when a dielectric plate is introduced between them ( task 19.2.1 ) will increase (answer 2 ). Indeed, in the field of charges on the surface of the plate, charges will be induced: closer to positive - minuses, closer to negative - pluses (see figure). As a result, for each point, along with the same force of attraction to another charge (and it, of course, does not change, because the principle of superposition says that all charges interact independently), two additional forces will act. This will be the force of attraction to charges of the same sign and repulsion from charges of the opposite sign. And since the charges of the opposite sign are closer, the force of attraction will be greater. The appearance of an additional force directed towards the plate will be perceived as an increase in the force of attraction.
As noted above (problem 19.1.7), the potential of the electric field at all points of the conducting body is the same. Therefore, we can introduce the concept of the potential of a conducting body, which is defined as the potential of the electric field at any point of this body. Therefore, for the potential of a metal ball from of problem 19.2.2 we have , where , is the charge of the ball, is its radius. The field potential of the ball at a distance of two radii from its surface and, therefore, three radii from the center of the ball is , i.e. one third of the ball's potential. From here we find B (answer 2 ).
Therefore, we can introduce the concept of the potential of a conducting body, which is defined as the potential of the electric field at any point of this body. Therefore, for the potential of a metal ball from of problem 19.2.2 we have , where , is the charge of the ball, is its radius. The field potential of the ball at a distance of two radii from its surface and, therefore, three radii from the center of the ball is , i.e. one third of the ball's potential. From here we find B (answer 2 ).
The potential of each drop of mercury ( task 19.2.3 ) is , where , is the charge of the drop, is its radius. After merging, the charge of the large drop is , and the radius is , where is the number of drops (the latter follows from the fact that the volume of the large drop is equal to the sum of the volumes of the drops). From here we find the potential of a large drop
|
|
(answer 2 ).
Since after joining the balls will be a single metal body ( task 19.2.4 ), then the charge will be divided between them so that the potentials of the balls will be the same. Therefore, for the charges of the balls and the condition
|
|
From here we find (the answer is 4 ).
According to the principle of superposition, the potential of each point is the sum of the potential created at this point by all charges. Therefore, the potentials of both the internal and external spheres ( task 19.2.5 ) are created by the charges of the inner and outer spheres. And since the potential at any point inside the sphere is determined by its radius of the sphere (see (18.8)), we get
|
|
Similarly, we find the potential of the outer sphere
|
|
From here we find
|
|
(answer 3 ).
To find the potential difference between two conductors, you need to mentally transfer the test charge from one of them to the other, find the work done by the electric field in this case, divide the work by the value of the test charge. In problem 19.2.6 there will be a uniform field with intensity between the plates. Therefore, the work of the field on the test charge when it moves from one plate to another is . On the other hand, the work of the field is related to the potential difference in the following way. From here we find the potential difference of the plates
|
|
(answer 3 ).
Since the field strength between two parallel plates charged with the same charge is equal to zero (see problem 18.2.8), when the test charge is transferred from one plate to another, the field does not do work. Therefore, the potential difference between such plates in problem 19.2.7 is equal to zero (answer 4 ).
B problem 19.2.8 charges will be distributed only over the outer surface of the hollow ball (if all the charge or some part of it was on the inner surface, then there would be an electric field in the volume of the conductor, which should not be). And since the charge located on the surface of the sphere creates a field only outside this sphere, the intensity will be different from zero only in region 3. Therefore, the correct answer in the problem is 4 .
In problem 19.2.9 charges are induced both on the outer and inner surfaces of the hollow ball, and their sum is equal to zero. The resulting field will be created by the central charge and induced charges, which, in fact, are uniformly charged spheres. And since the field of the sphere is equal to zero inside this sphere, the total field in the cavity (in region 1) is equal to the field of a point charge, i.e. not equal to zero. Inside the metallic body (in area 2) the field is equal to zero, as well as inside any conductor. Outside the ball, the fields of induced charges compensate each other, so the total field is equal to the field of a point charge, i.e. not equal to zero. So the correct answer for this problem is 9.0021 2 .
Outside the ball, the fields of induced charges compensate each other, so the total field is equal to the field of a point charge, i.e. not equal to zero. So the correct answer for this problem is 9.0021 2 .
In problem 19.2.10 on the outer and inner surfaces of the spherical shell such charges will be induced that the total field (external plus the field of induced charges) inside the shell will be equal to zero. Let the charge - be induced on the inner surface, then the charge will be induced on the outer surface. The field inside the shell (in region 2) will be created only by a point charge and charges of the inner surface (the charge of the outer surface, due to its sphericity, does not create an electric field in this region). On the other hand, this field is zero. Hence we conclude that the charge of the inner surface of the shell is opposite in sign to the central point charge and is equal to it in magnitude. Therefore, the charge of the outer surface of the shell to the central charge (answer 1 ).
Phosphate modified CpG oligonucleotides induce maturation of human myeloid dendritic cells in vitro | Ostanin
1. Alyamkina E.A., Leplina O.Yu., Sakhno L.V., Chernykh E.R., Ostanin A.A., Efremov Ya.R., Shilov A.G., Orishchenko K.E., Likhacheva A.S., Dolgova E.V., Nikolin V.P., Popova N.A., Zagrebelniy S.N., Bogachev S.S., Shurdov M.A. Effect of double-stranded DNA on maturation of dendritic cells in vitro. cell. Immunol. 2010;266(1): 46-51. DOI 10.1016/j.cellimm.2010.08.011.
2. Banchereau J., Briere F., Caux C., Davoust J., Lebecque S., Liu Y.J., Palendran B., Palucka K. Immunobiology of dendritic cells. Annu. Rev. Immunol. 2000;18:767-811. DOI 10.1146/annurev.immunol.18.1.767.
3. Bauer S., Kirschning C.J., Hacker H., Redecke V., Hausmann S., Akira S., Wagner H., Lipfordet G.B. Human TLR9 confers responsiveness to bacterial DNA via species-specific CpG motif recognition. Proc. Natl. Acad. sci. USA. 2001;98(16):9237-9242. DOI 10.1073/pnas.161293498.
4. Behboudi S., Chao D., Klenerman P., Austyn J. The effects of DNA containing CpG motif on dendritic cells. Immunology. 2000;99(3): 361-366. DOI 10.1046/j.1365-2567.2000.00979.x.
5. Cehim G., Chies J.A.B. In vitro generation of human monocyte-derived dendritic cells methodological aspects in a comprehensive review. an. Acad. Bras. Cienc. 2019;91:e20190310. DOI 10.1590/0001-3765201920190310.
6. Chelobanov B.P., Burakova E.A., Prokhorova D.V., Fokina A.A., Stetsenko D.A. New oligodeoxynucleotide derivatives containing N-(methanesulfonyl)-phosphoramidate (mesyl phosphoramidate) internucleotide group. Russ. J. Bioorg. Chem. 2017;43(6):664-668. DOI 10.1134/S1068162017060024.
7. Dyakonova V.A., Dambaeva S.V., Pinegin B.V., Khaitov R.M. Study of interaction between the polyoxidonium immunomodulator and the human immune system cells. Inter. Immunopharm. 2004;4(13): 1615-1623. DOI 10.1016/j.intimp.2004.07.015.
8. Hoene V., Peiser M., Wanner R. Human monocyte-derived dendritic cells express TLR9 and react directly to the CpG-A oligonucleotide D19. J. Leuk. Biol. 2006;80(6):1328-1336. DOI 10.1189/jlb.0106011.
9. Iwasaki A., Medzhitov R. Toll-like receptor control of the adaptive immune responses. Nat. Immunol. 2004;5(10):987-995. DOI 10.1038/ni1112.
10. Jounai N., Kobiyama K., Takeshita F., Ishii K.J. Recognition of damage-associated molecular patterns related to nucleic acids during inflammation and vaccination. front. cell. Infect. microbiol. 2013; 2:168. DOI 10.3389/fcimb.2012.00168.
11. Kabanov V.A. From synthetic polyelectrolytes to polymer-subunit vaccines. Pure Apple. Chem. 2004;76(9):1659-1677. DOI 10.1351/pac200476091659.
12. Kawasaki T., Kawai T. Toll-like receptor signaling pathways. front. Immunol. 2014. DOI 10.3389/fimmu.2014.00461.
13. Krug A., Towarowski A., Britsch S., Rothenfusser S., Hornung V., Bals V., Giese T., Engelmann H., Endres S., Krieg A.M., Hartmann G. Toll-like receptor expression reveals CpG DNA as a unique microbial stimulus for plasmacytoid dendritic cells which synergizes with CD40 ligand to induce high amounts of IL-12. Eur. J. Immunol. 2001;31(10):3026-3037. DOI 10.1002/1521-4141(2001010)31:10<3026::aid-immu3026>3.0.co;2-h.
14. Levy R., Reagan P.M., Friedberg J.W., Bartlett N.L., Gordon L.I., Leung A., Peterkin J., Xing B., Coffman R., Janssen R., Candia A., Khodadoust M., Frank M.J. , Long S.R., Czerwinski D.K., Chu M. SD-101, a novel class C CpG-oligodeoxynucleotide (ODN) toll-like receptor 9(TLR9) agonist, given with low dose radiation for untreated low grade B-cell lymphoma: interim results of a phase 1/2 trial. Blood. 2016;128(22):2974. DOI 10.1182/blood.V128.22.2974.2974.
15. Li T., Wu J., Zhu S., Zang G., Li S., Lv X., Yue W., Qiao Y., Cui J., Shao Y., Zhang J., Liu Y .-J., Chen J. A novel C type CpG oligodeoxynucleotide exhibits immunostimulatory activity in vitro and enhances antitumor effect in vivo. front. Pharmacol. 2020;11:8. DOI 10.3389/fphar.2020.00008.
16. Marshall J.D., Fearon K.L., Higgins D., Hessel E.M., Kanzler H., Abbate C., Yee P., Gregorio J., Cruz T. D., Lizcano J.O., Zolotorev A., McClure H.M., Brasky K.M., Murthy K.K. , Coffman R.L., Nest G.V. Superior activity of the type C class of ISS in vitro and in vivo across multiple species. DNA Cell Biol. 2005;24(2):63-72. DOI 10.1089/dna.2005.24.63. 17. Miroshnichenko S.K., Patutina O.A., Burakova E.A., Chelobanov B.P., Fokina A.A., Vlassov V.V., Altman S., Zenkova M.A., Stetsenko D.A. Mesyl phosphoramidate antisense oligonucleotides as an alternative to phosphorothioates with improved biochemical and biological properties. Proc. Natl. Acad. sci. USA. 2019;116(4): 1229-1234. DOI 10.1073/pnas.1813376116.
18. Orishchenko K.E., Ryzhikova S.L., Druzhinina Y.G., Ryabicheva T.G., Varaksin N.A., Alyamkina E.A., Dolgova E.V., Rogachev V.A., Proskurina A.S., Nikolin V.P., Popova N.A., Strunov A.A., A. Cherny.Oplina E.V. E.R., Sidorov S.V., Mayorov V.I., Bogachev S.S., Shurdov M.A. Effect of human double-stranded DNA preparation on the production of cytokines by dendritic cells and peripheral blood cells from relatively healthy donors. Cancer Ther. 2013;8:191-205.
19. Polovinkina V.S., Markov E.Yu. Structure and immune adjuvant properties of CpG-DNA. Meditsinskaya Immunologiya = Medical Immunology (Russia). 2010;12(6):469-476. DOI 10.15789/1563-0625-2010-6-469-476. (in Russian)
20. Powell B.S., Andrianov A.K., Fusco P.C. Polyionic vaccine adjuvants: another look at aluminum salts and polyelectrolytes. Clin. Exp. Vaccine Res. 2015;4(1):23-45. DOI 10.7774/cevr.2015.4.1.23. Rothenfusser S., Tuma E., Endres S., Hartmann G. Plasmacytoid dendritic cells: the key to CpG. Hum. Immunol. 2002;63(12):1111-1119. DOI 10.1016/s0198-8859(02)00749-8.
21. Scheiermann J., Klinman D.M. Clinical evaluation of CpG oligonucleotides as adjuvants for vaccines targeting infectious diseases and cancer. Vaccine. 2014;32(48):6377-6389. DOI 10.1016/j.vaccine.2014.06.065.
22. Shirota H., Klinman D.M. Recent progress concerning CpG DNA and its use as a vaccine adjuvant. Expert Rev. Vaccines. 2014;13(2):299-312. DOI 10.