Signs urinary tract infection toddlers
Urinary tract infection (UTI) in children
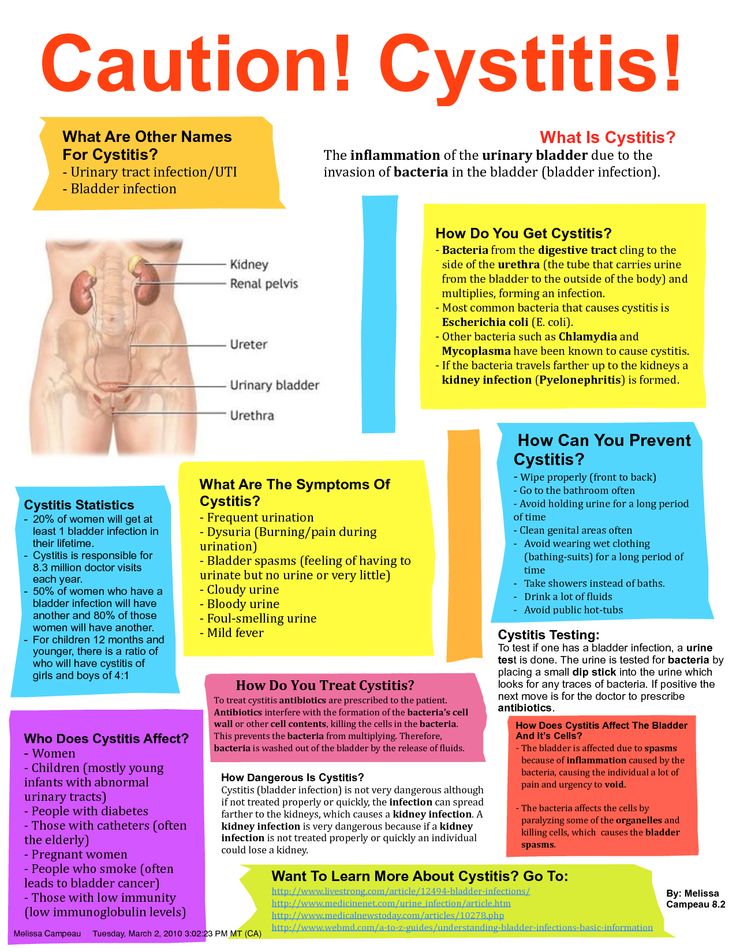
Urinary tract infections (UTIs) in children are fairly common, but not usually serious. They can be effectively treated with antibiotics.
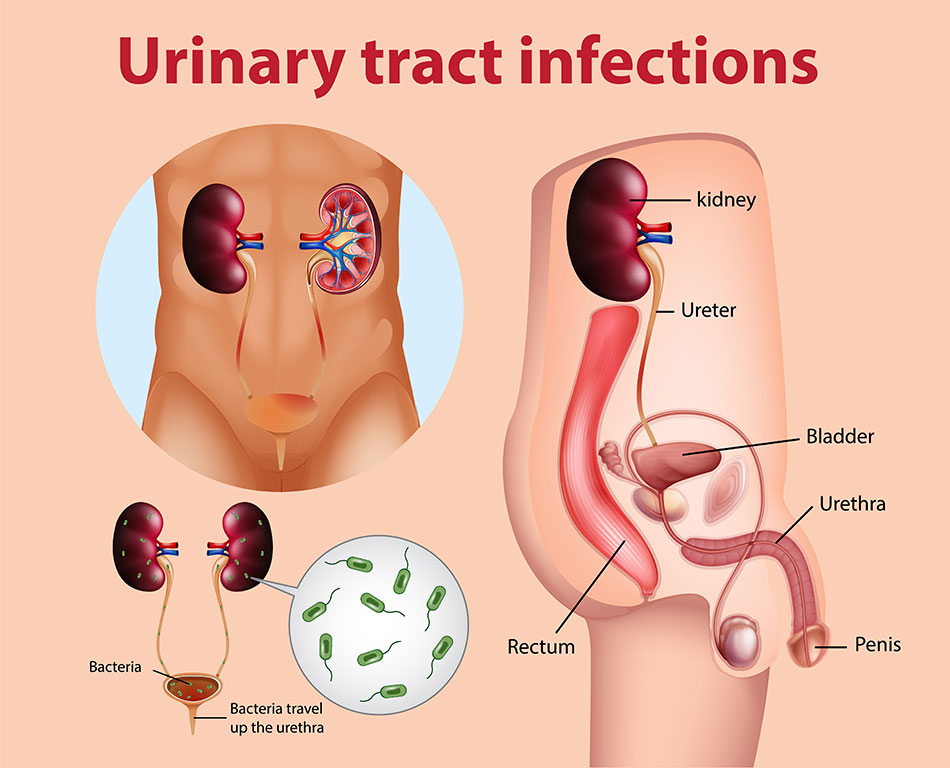
A UTI may be classed as either:
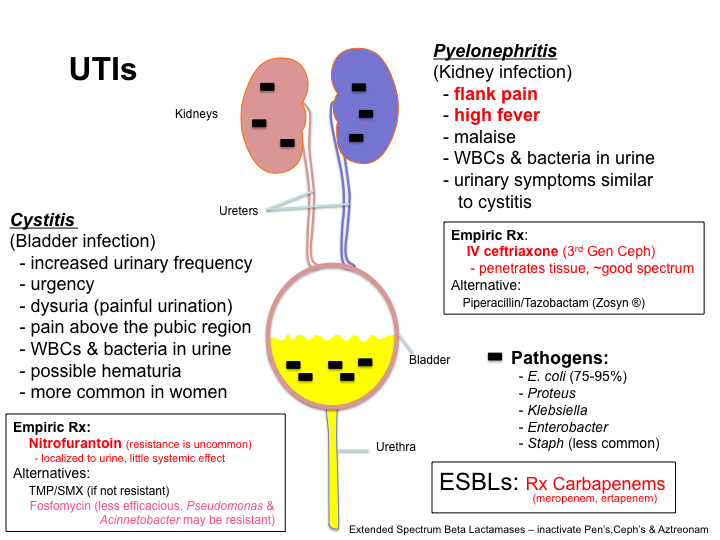
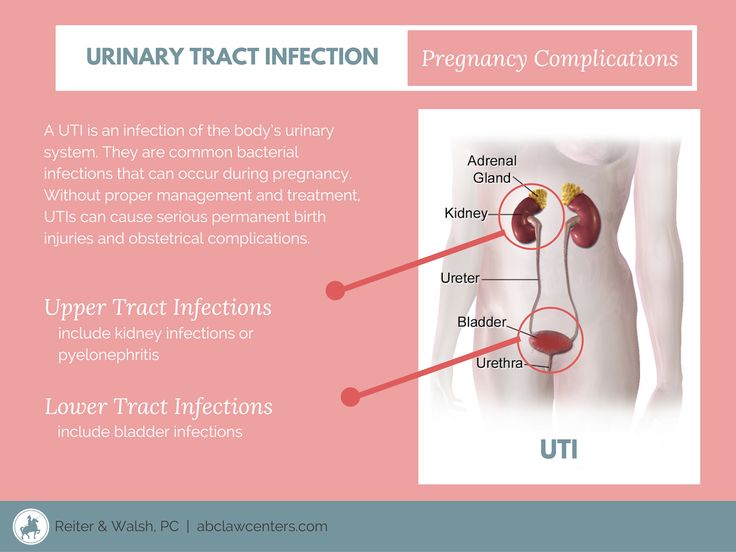
- an upper UTI – if it's a kidney infection or an infection of the ureters, the tubes connecting the kidneys to the bladder
- a lower UTI – if it's a bladder infection (cystitis) or an infection of the urethra, the tube that carries urine from the bladder out of the body
When to seek medical advice
If you think your child is unwell and could have a UTI, contact your GP as soon as possible.
Although UTIs aren't normally a serious type of infection, they should be diagnosed and treated quickly to reduce the risk of complications.
Symptoms of a UTI in children
It can be difficult to tell whether your child has a UTI, as the symptoms can be vague and young children can't easily communicate how they feel.
General signs that may suggest your child is unwell include:
- a high temperature (fever)
- vomiting
- tiredness and lack of energy (lethargy)
- irritability
- poor feeding
- not gaining weight properly
- in very young children, yellowing of the skin and whites of the eyes (jaundice)
More specific signs that your child may have a UTI include:
- pain or a burning sensation when peeing
- needing to pee frequently
- deliberately holding in their pee
- a change in their normal toilet habits, such as wetting themselves or wetting the bed
- pain in their tummy (abdomen), side or lower back
- unpleasant-smelling pee
- blood in their pee
- cloudy pee
Diagnosing UTIs in children
In most cases, your GP can diagnose a UTI by asking about your child's symptoms, examining them, and arranging for a sample of their pee to be tested.
Treatment usually begins soon after a urine sample has been taken, and your child won't need any further tests.
In a few circumstances, further tests may be needed in hospital to check for abnormalities. Your GP may refer you straight to hospital if your child is very young.
Read more about diagnosing UTIs in children
Causes of UTIs in children
Most UTIs in children are caused by bacteria from the digestive system entering the urethra.
There are many ways this can happen, including:
- when a child wipes their bottom and soiled toilet paper comes into contact with their genitals – this is more of a problem for girls than boys because girls' bottoms are much nearer the urethra
- babies getting small particles of poo in their urethra when they soil their nappies – particularly if they squirm a lot when being changed
There's often no obvious reason why some children develop UTIs and others don't.
However, some children may be more vulnerable to UTIs because of a problem with emptying their bladder, such as:
- constipation – this can sometimes cause part of the large intestine to swell, which can put pressure on the bladder and prevent it emptying normally
- dysfunctional elimination syndrome – a relatively common childhood condition where a child "holds on" to their pee, even though they have the urge to pee
- vesicoureteral reflux – an uncommon condition where urine leaks back up from the bladder into the ureters and kidneys; this occurs as a result of a problem with the valves in the ureters where they enter the bladder
Treating UTIs in children
Most childhood UTIs clear up within 24 to 48 hours of treatment with antibiotics and won't cause any long-term problems.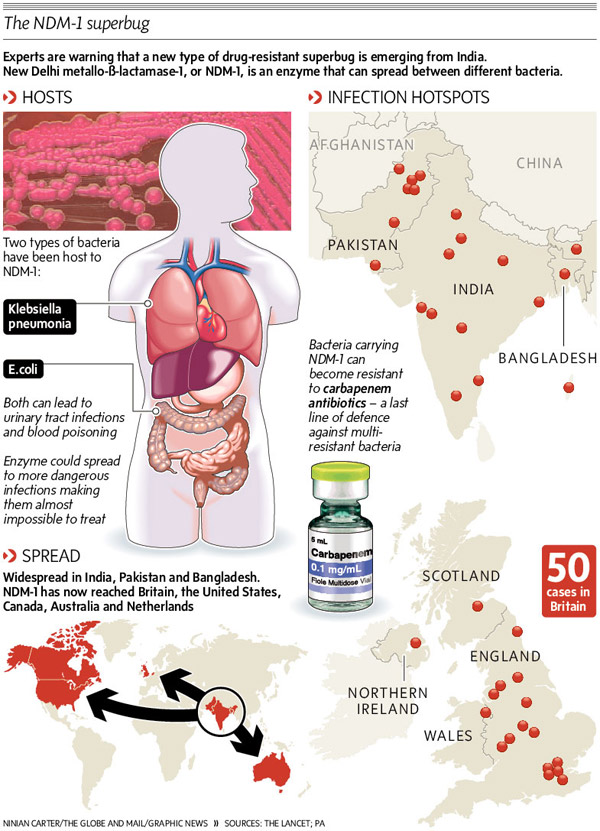
In many cases, treatment involves your child taking a course of antibiotic tablets at home.
As a precaution, babies under three months old and children with more severe symptoms are usually admitted to hospital for a few days to receive antibiotics directly into a vein (intravenous antibiotics).
Read more about treating UTIs in children
Preventing UTIs in children
It isn't possible to prevent all childhood UTIs, but there are some things you can do to reduce the risk of your child getting one.
The following advice may help:
- if possible, exclusively breastfeed your baby for the first six months after they're born – this can help improve your baby's immune system and reduce their risk of constipation
- encourage girls to wipe their bottom from front to back – this helps to minimise the chances of bacteria entering the urethra
- make sure your child is well hydrated and goes to the toilet regularly – not urinating regularly and "holding in" urine can make it easier for bacteria to infect the urinary tract
- avoid nylon and other types of synthetic underwear – these can help promote the growth of bacteria; loose-fitting cotton underwear should be worn instead
- avoid using scented soaps or bubble baths – these can increase your child's risk of developing a UTI
- take steps to reduce your child's risk of constipation – make sure they drink enough to keep their urine pale and clear during the day, and speak to your GP about medications that can help if constipation is a persistent problem
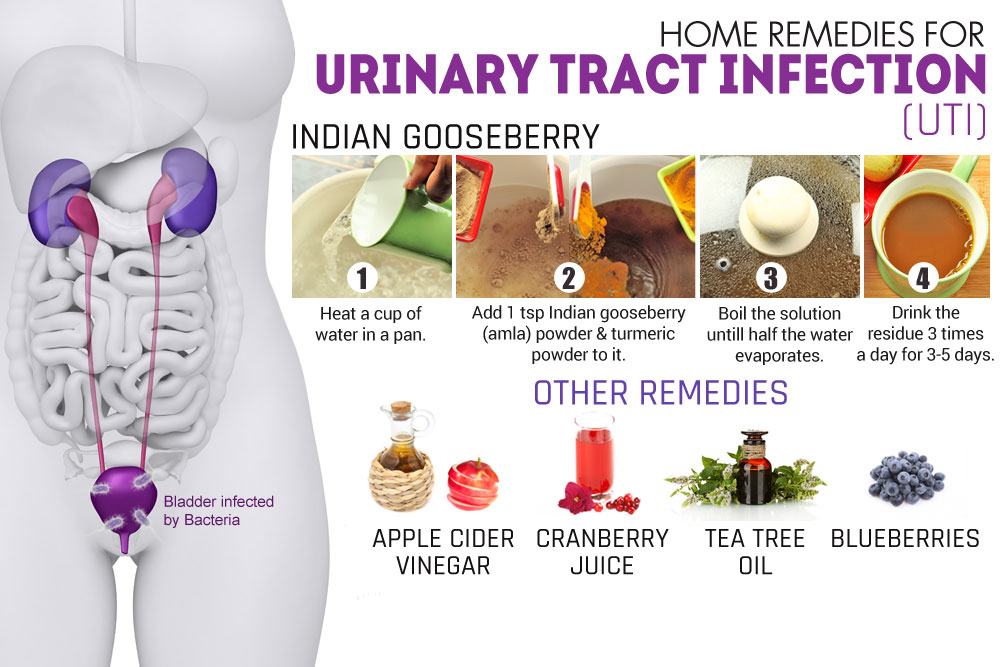
Some people feel that drinking cranberry juice or taking cranberry supplements can help reduce their risk of UTIs.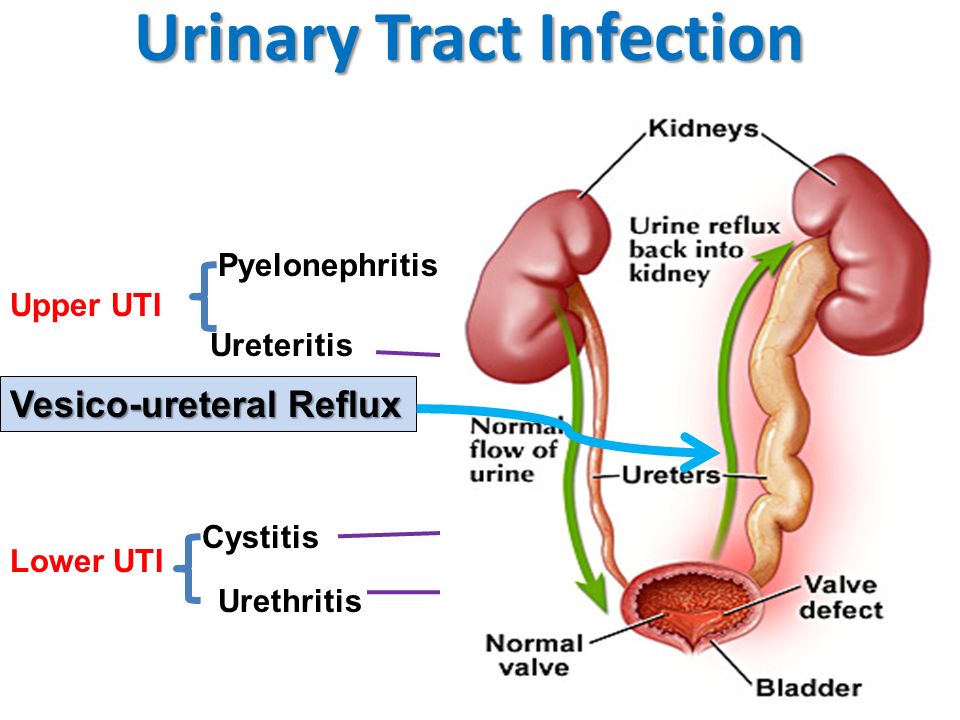
However, recent high-quality research into these claims found little evidence to suggest cranberries have a significant impact on your chances of developing a UTI.
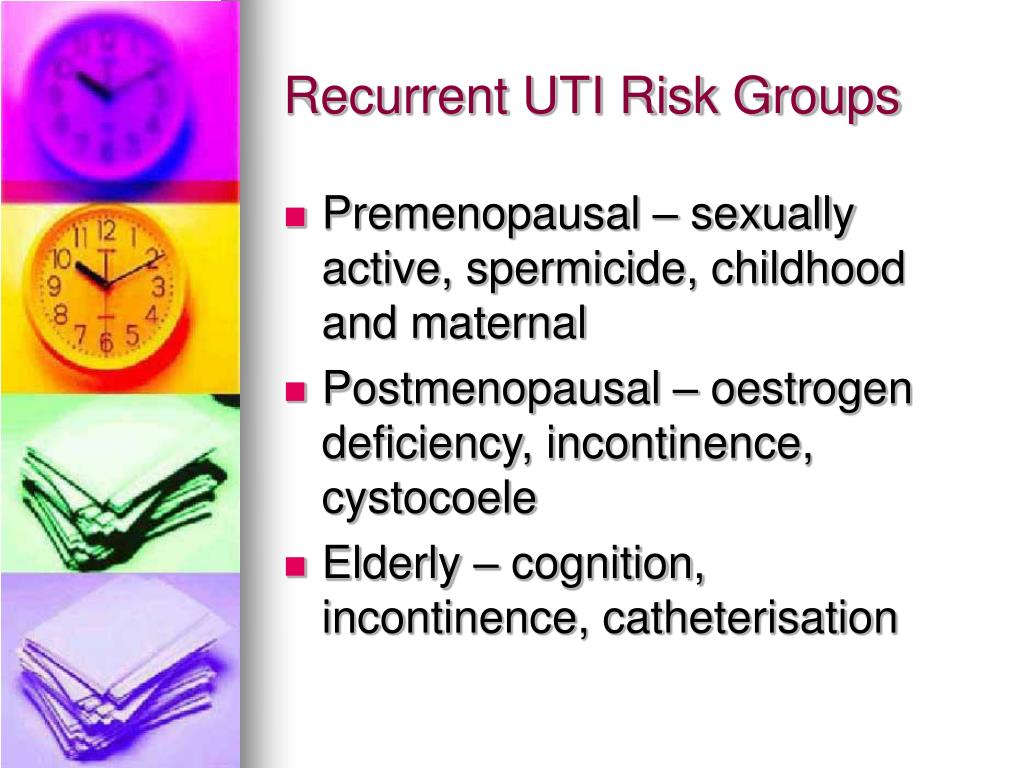
Recurrent UTIs in children
A small number of children have recurring UTIs. If your child's had a UTI before, it's important that both of you watch for the return of any associated symptoms.
Tell your GP about any symptoms as soon as possible so a diagnosis can be confirmed and treatment can begin.
If your child has a problem that increases their risk of UTIs, such as faulty valves that allow urine to flow the wrong way, they may be prescribed low-dose antibiotics as a long-term measure to prevent further infections.
Urinary Tract Infections (UTIs) (for Parents)
Urinary tract infections (UTIs) are common in kids. They happen when bacteria (germs) get into the bladder or kidneys.
A baby with a UTI may have a fever, throw up, or be fussy. Older kids may have a fever, have pain when peeing, need to pee a lot, or have lower belly pain.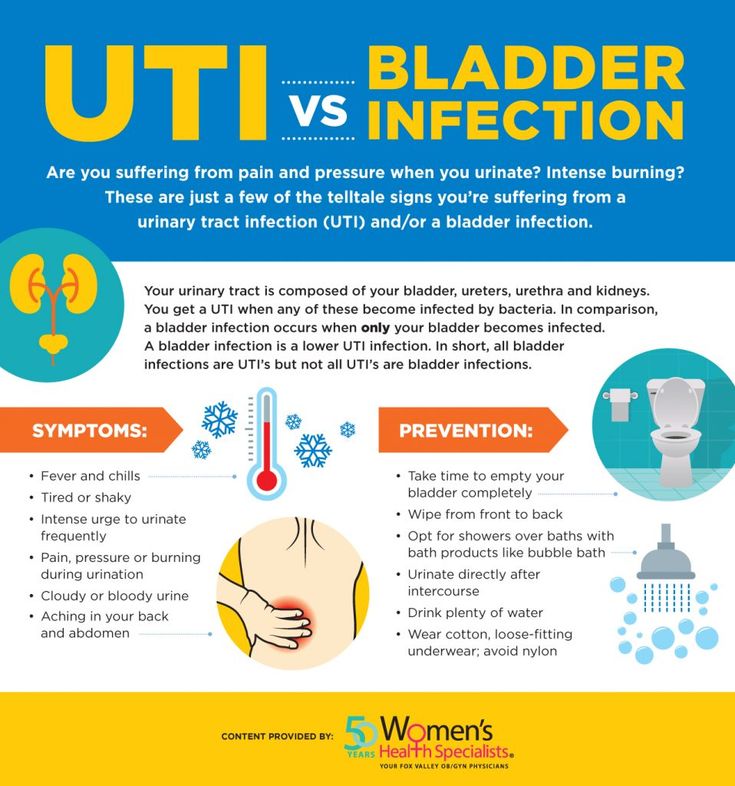
Kids with UTIs need to see a doctor. These infections won't get better on their own. UTIs are easy to treat and usually clear up in a week or so.
Taking antibiotics kills the germs and helps kids get well again. To be sure antibiotics work, you must give all the prescribed doses — even when your child starts feeling better.
What Are the Signs & Symptoms of a UTI?
Most UTIs happen in the lower part of the urinary tract — the urethra and bladder. This type of UTI is called cystitis. A child with cystitis may have:
- pain, burning, or a stinging sensation when peeing
- an increased urge or more frequent need to pee (though only a very small amount of pee may be passed)
- fever
- waking up at night a lot to go to the bathroom
- wetting problems, even though the child is potty trained
- belly pain in the area of the bladder (generally below the belly button)
- foul-smelling pee that may look cloudy or contain blood
An infection that travels up the ureters to the kidneys is called pyelonephritis (pie-low-nih-FRY-tis) and is usually more serious. It causes many of these same symptoms, but the child often looks sicker and is more likely to have a fever (sometimes with shaking chills), pain in the side or back, severe tiredness, or vomiting.
It causes many of these same symptoms, but the child often looks sicker and is more likely to have a fever (sometimes with shaking chills), pain in the side or back, severe tiredness, or vomiting.
What Causes UTIs?
UTIs are much more common in girls because a girl's urethra is shorter and closer to the anus (where poop comes out). Uncircumcised boys younger than 1 year also have a slightly higher risk for a UTI.
Other risk factors for a UTI include:
- a problem in the urinary tract (for example, a malformed kidney or a blockage somewhere along the tract of normal urine flow)
- an abnormal backward flow (reflux) of urine from the bladder up the ureters and toward the kidneys. This is known as vesicoureteral reflux (VUR), and many kids with a UTI are found to have it.
- poor toilet and hygiene habits
- family history of UTIs
UTIs are easy to treat, but it's important to catch them early. Undiagnosed or untreated UTIs can lead to kidney damage.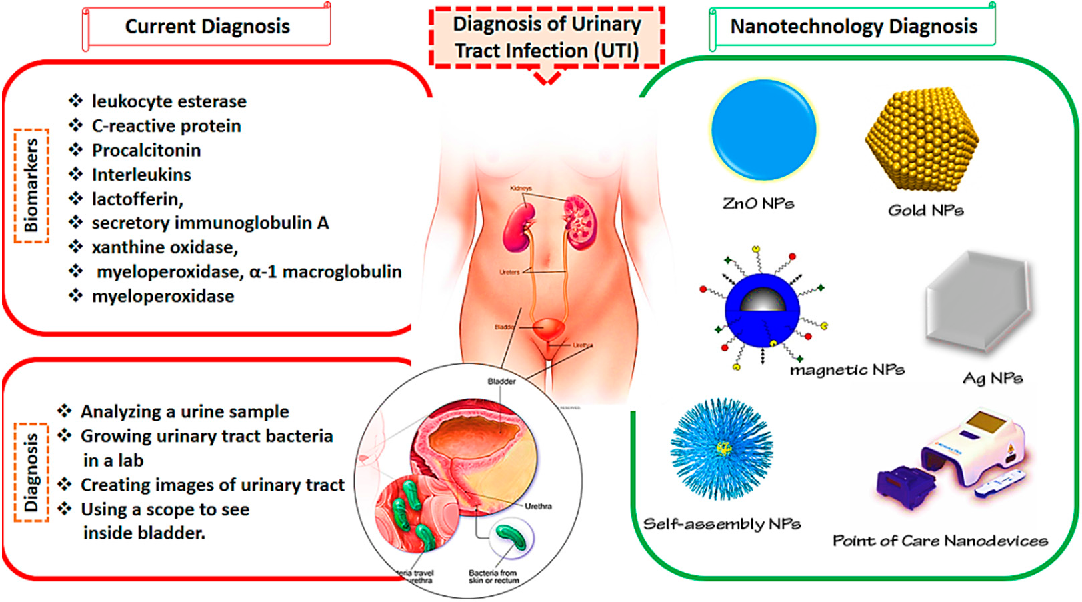
How Are UTIs Diagnosed?
To diagnose a UTI, health care providers ask questions about what's going on, do an exam, and take a sample of pee for testing.
How a sample is taken depends on a child's age. Older kids might simply need to pee into a sterile cup. For younger children in diapers, a catheter is usually preferred. This is when a thin tube is inserted into the urethra up to the bladder to get a "clean" urine sample.
The sample may be used for a urinalysis (a test that microscopically checks the urine for germs or pus) or a urine culture (which attempts to grow and identify bacteria in a laboratory). Knowing what bacteria are causing the infection can help your doctor choose the best treatment.
How Are UTIs Treated?
UTIs are treated with antibiotics. After several days of antibiotics, your doctor may repeat the urine tests to be sure that the infection is gone. It's important to make sure of this because an incompletely treated UTI can come back or spread.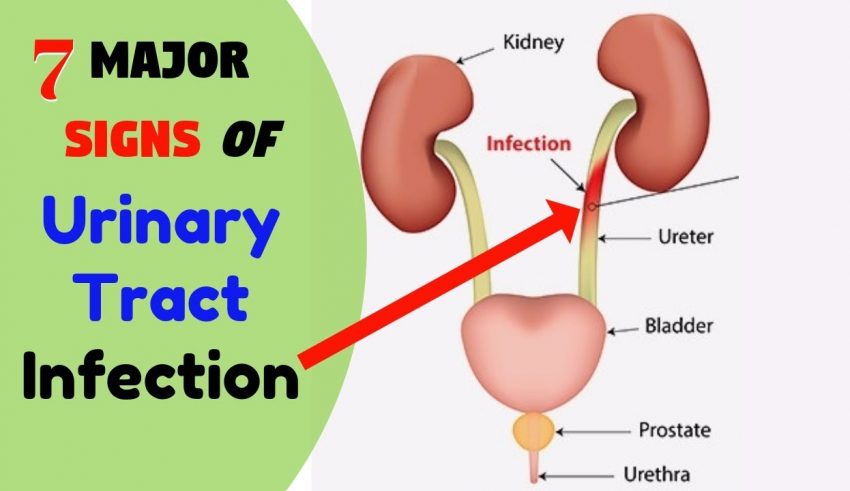
If a child has severe pain when peeing, the doctor may also prescribe medicine that numbs the lining of the urinary tract. (This medicine temporarily causes the pee to turn orange.)
Give prescribed antibiotics on schedule for as many days as your doctor directs. Keep track of your child's trips to the bathroom, and ask your child about symptoms like pain or burning during peeing. These symptoms should improve within 2 to 3 days after antibiotics are started.
Encourage your child to drink plenty of fluids, but skip drinks that containe caffeine (which can irritate the bladder), such as soda and iced tea.
Most UTIs are cured within a week with treatment.
Treatment for More Severe UTIs
Kids with a more severe infection may need treatment in a hospital so they can get antibiotics by injection or IV (intravenously, given into a vein right into the bloodstream).
This might happen if:
- the child has high fever or looks very ill, or a kidney infection is likely
- the child is younger than 6 months old
- bacteria from the infected urinary tract may have spread to the blood
- the child is dehydrated or is vomiting and cannot take any fluids or medicine by mouth
Kids with VUR will be watched closely by the doctor. VUR might be treated with medicines or, less commonly, surgery. Most kids outgrow mild forms of VUR, but some can develop kidney damage or kidney failure later in life.
VUR might be treated with medicines or, less commonly, surgery. Most kids outgrow mild forms of VUR, but some can develop kidney damage or kidney failure later in life.
Can UTIs Be Prevented?
These tips can help prevent UTIs:
- In infants and toddlers, change diapers often to help prevent the spread of bacteria that cause UTIs. When kids are potty trained, it's important to teach them good hygiene. Girls should know to wipe from front to rear — not rear to front — to prevent germs from spreading from the anus to the urethra.
- School-age girls should avoid bubble baths and strong soaps that might cause irritation. They also should wear cotton underwear instead of nylon because it's less likely to encourage bacterial growth.
- All kids should be taught not to "hold it" when they have to go. Pee that stays in the bladder gives bacteria a good place to grow.
- Kids should drink plenty of fluids but avoid those with caffeine.
When Should I Call the Doctor?
Call the doctor right away if your child has an unexplained fever with shaking chills, especially if there's also back pain or any type of pain when peeing.
Also call if your child has any of these:
- bad-smelling, bloody, or discolored pee
- low back pain or belly pain (especially below the belly button)
- a fever of over 101°F (38.3°C) in children or 100.4°F (38°C) rectally in infants
Call the doctor if your infant has a fever, feeds poorly, vomits repeatedly, or seems unusually irritable.
Urinary tract infection in children. What is urinary tract infection in children?
IMPORTANT
The information in this section should not be used for self-diagnosis or self-treatment. In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests. For diagnosis and proper treatment, you should contact your doctor.
Urinary tract infection in children is a group of microbial-inflammatory diseases of the urinary system organs: kidneys, ureters, bladder, urethra. Depending on the location of the inflammation, urinary tract infection in children can be manifested by dysuric disorders, pain in the bladder or lower back, leukocyturia and bacteriuria, and temperature reaction.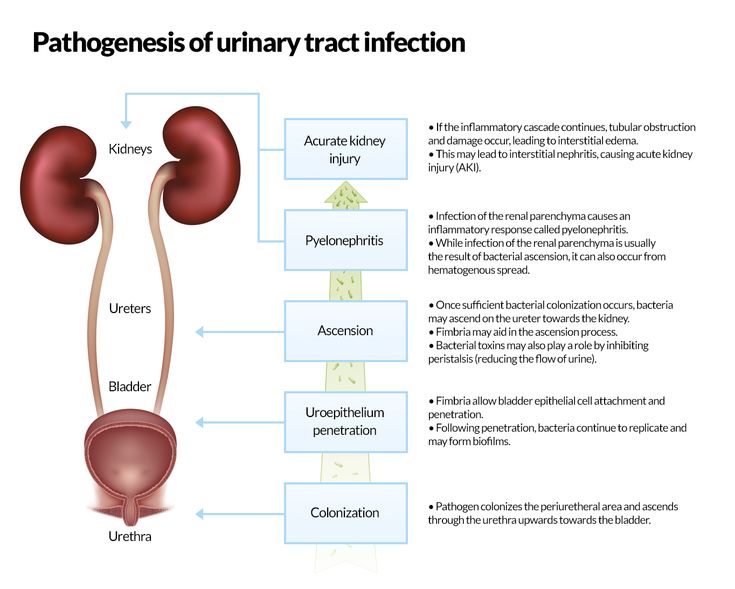 Examination of children with suspected urinary tract infection includes urinalysis (general, bacterial culture), ultrasound of the urinary system, cystoureterography, excretory urography, cystoscopy. The basis for the treatment of urinary tract infections in children is the appointment of antimicrobial drugs, uroantiseptics.
Examination of children with suspected urinary tract infection includes urinalysis (general, bacterial culture), ultrasound of the urinary system, cystoureterography, excretory urography, cystoscopy. The basis for the treatment of urinary tract infections in children is the appointment of antimicrobial drugs, uroantiseptics.
- Causes of urinary tract infection in children
- Classification
- Symptoms in children
- Diagnostics
- Treatment of urinary tract infection in children
- Prognosis and prevention
- Prices for treatment
General
Urinary tract infection in children is a general concept that refers to inflammatory processes in various parts of the urinary tract: infections of the upper urinary tract (pyelitis, pyelonephritis, ureteritis) and lower urinary tract (cystitis, urethritis). Urinary tract infections are extremely common in childhood - by age 5, 1-2% of boys and 8% of girls have had at least one episode of the disease.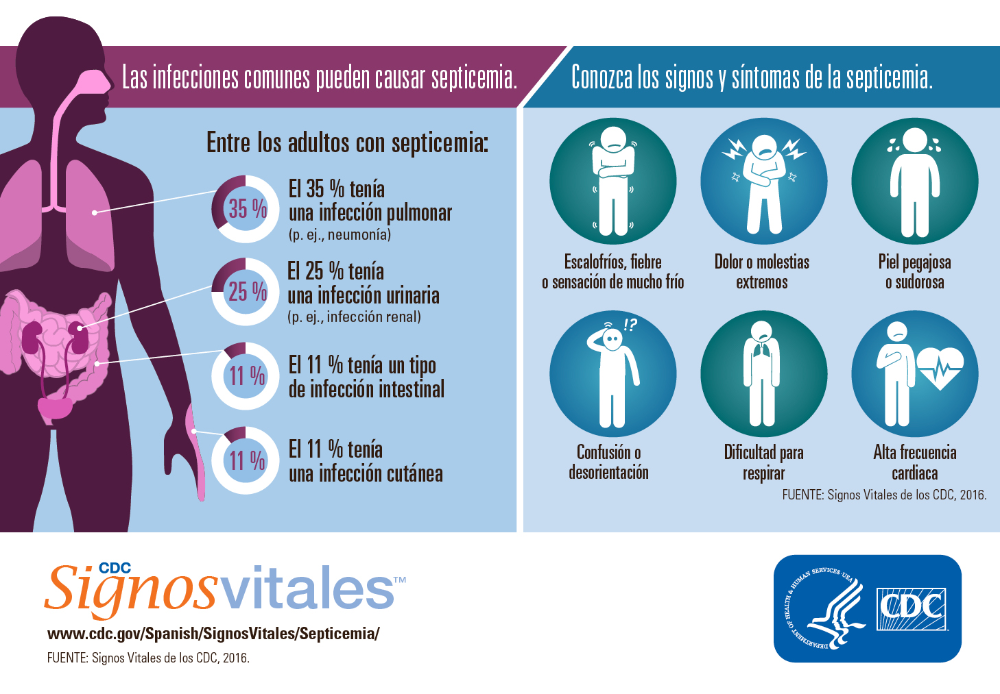 The prevalence of urinary tract infections depends on age and gender: for example, among newborns and infants, boys are more likely to get sick, and girls between the ages of 2 and 15 years. Most often in the practice of pediatric urology and pediatrics one has to deal with cystitis, pyelonephritis and asymptomatic bacteriuria.
The prevalence of urinary tract infections depends on age and gender: for example, among newborns and infants, boys are more likely to get sick, and girls between the ages of 2 and 15 years. Most often in the practice of pediatric urology and pediatrics one has to deal with cystitis, pyelonephritis and asymptomatic bacteriuria.
urinary tract infection in children
Causes of urinary tract infection in children
The spectrum of microbial flora that causes urinary tract infections in children depends on the sex and age of the child, the conditions of infection, the state of intestinal microbiocenosis and general immunity. In general, among bacterial pathogens, enterobacteria are in the lead, primarily E. coli (50-90%). In other cases, Klebsiella, Proteus, Enterococci, Pseudomonas aeruginosa, Staphylococci, Streptococci, etc. are sown. Acute urinary tract infections in children are usually caused by one type of microorganism, however, with frequent relapses and malformations of the urinary system, microbial associations are often detected.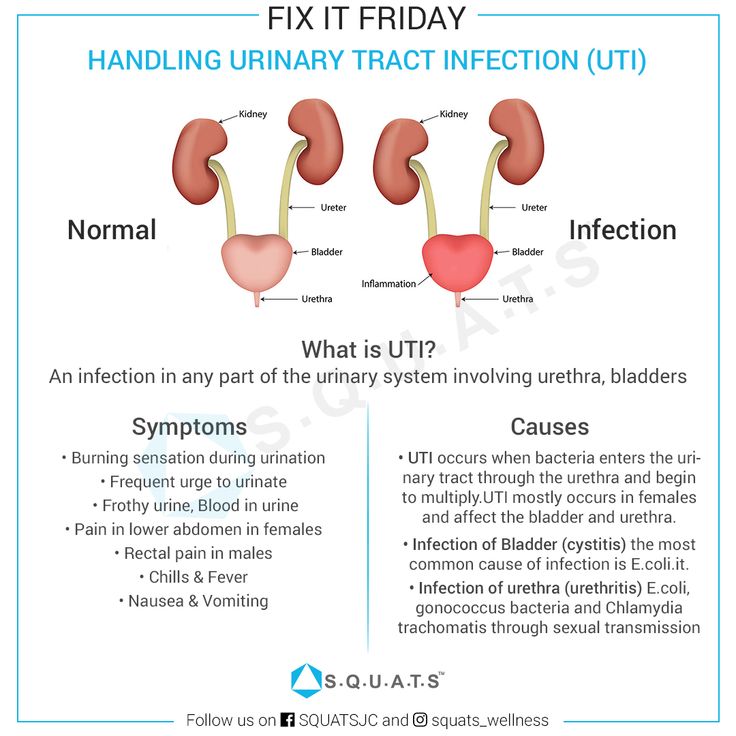
Urinary tract infections in children can be associated with urogenital chlamydia, mycoplasmosis and ureaplasmosis and combined with vulvitis, vulvovaginitis, balanoposthitis. Fungal infections of the urinary tract often occur in debilitated children: premature, suffering from malnutrition, immunodeficiency states, anemia. There is an assumption that a viral infection (infection with Coxsackie, influenza, adenoviruses, herpes simplex virus types I and II, cytomegalovirus) is a factor contributing to the layering of a bacterial infection.
Conditions accompanied by impaired urodynamics predispose to the development of urinary tract infection in children: neurogenic bladder, urolithiasis, bladder diverticula, vesicoureteral reflux, pyelectasis, hydronephrosis, polycystic kidney disease, kidney dystopia, ureterocele, phimosis in boys, synechia of the labia in girls. Often, urinary tract infections in children develop against the background of gastrointestinal diseases - dysbacteriosis, constipation, colitis, intestinal infections, etc.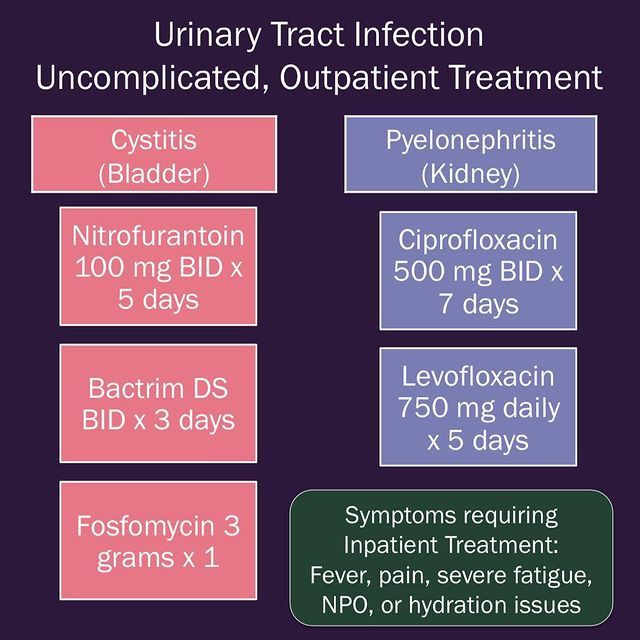 Metabolic disorders (dysmetabolic nephropathy in children, glucosuria, etc.) can be a risk factor.
Metabolic disorders (dysmetabolic nephropathy in children, glucosuria, etc.) can be a risk factor.
The introduction of infection into the urinary tract can occur with insufficient hygiene of the external genitalia, improper washing technique of the child, lymphogenous and hematogenous routes, during medical manipulations (bladder catheterization). Boys who have undergone circumcision suffer from urinary tract infections 4-10 times less often than uncircumcised boys.
Classification
According to the localization of the inflammatory process, infections of the upper urinary tract are distinguished - the kidneys (pyelonephritis, pyelitis), ureters (ureteritis) and the lower sections - the bladder (cystitis) and urethra (urethritis).
According to the period of the disease, urinary tract infections in children are divided into the first episode (debut) and relapse. The course of recurrent urinary tract infection in children may be maintained by unresolved infection, persistence of the pathogen, or reinfection.
According to the severity of clinical symptoms, mild and severe urinary tract infections in children are distinguished. In a mild course, the temperature reaction is moderate, dehydration is insignificant, the child complies with the treatment regimen. Severe urinary tract infection in children is accompanied by high fever, persistent vomiting, severe dehydration, sepsis.
Symptoms in children
Clinical manifestations of urinary tract infection in a child depend on the localization of the microbial-inflammatory process, the period and severity of the disease. Consider the signs of the most common urinary tract infections in children - pyelonephritis, cystitis and asymptomatic bacteriuria.
Pyelonephritis in children occurs with febrile temperature (38-38.5 ° C), chills, symptoms of intoxication (lethargy, pallor of the skin, loss of appetite, headache). At the height of intoxication, frequent regurgitation, vomiting, diarrhea, neurotoxicosis, and meningeal symptoms may develop. The child is concerned about pain in the lumbar region or abdomen; effervescence symptom is positive. At an early age, infections of the upper urinary tract in children can be hidden under the guise of pylorospasm, dyspeptic disorders, acute abdomen, intestinal syndrome, etc.; in older children - flu-like syndrome.
The child is concerned about pain in the lumbar region or abdomen; effervescence symptom is positive. At an early age, infections of the upper urinary tract in children can be hidden under the guise of pylorospasm, dyspeptic disorders, acute abdomen, intestinal syndrome, etc.; in older children - flu-like syndrome.
Cystitis in children is manifested primarily by dysuric disorders - frequent and painful urination in small portions. In this case, complete simultaneous emptying of the bladder is not achieved, episodes of urinary incontinence are possible. In infants, cystitis is often accompanied by stranguria (urinary retention). The presence of dysuria in children of the first year of life can be indicated by anxiety or crying associated with urination, intermittent and weak urine stream. Cystitis is characterized by pain and tension in the suprapubic region; the temperature in cystitis is normal or subfebrile.
Asymptomatic bacteriuria is more common in girls. This form of urinary tract infection in children is not accompanied by any subjective clinical signs, but is detected only during laboratory examination. Sometimes parents pay attention to the turbidity of the child's urine and the bad smell emanating from it.
This form of urinary tract infection in children is not accompanied by any subjective clinical signs, but is detected only during laboratory examination. Sometimes parents pay attention to the turbidity of the child's urine and the bad smell emanating from it.
Diagnostics
Assessment of the severity of urinary tract infections in children requires an integrated approach and the participation of a number of specialists - a pediatrician, pediatric urologist, pediatric nephrologist, pediatric gynecologist.
Urinary tract infections in children may be suspected if leukocyturia, bacteriuria, proteinuria, and sometimes hematuria are detected in a general urine test. For a more detailed diagnosis, a urine test according to Nechiporenko, Zimnitsky's test is shown. Blood changes are characterized by neutrophilic leukocytosis, elevated ESR; with pyelonephritis - a high level of acute phase proteins (CRP, alpha globulins).
The basis for the diagnosis of urinary tract infections in children is a bacteriological culture of urine with the release of the pathogen, an assessment of the degree of bacteriuria and sensitivity to antibiotics. In some cases, a urine test for chlamydia, ureaplasma, mycoplasma is required by cultural, cytological, serological (ELISA) methods, PCR.
In some cases, a urine test for chlamydia, ureaplasma, mycoplasma is required by cultural, cytological, serological (ELISA) methods, PCR.
Children with a urinary tract infection must undergo an ultrasound examination of the urinary system (ultrasound of the kidneys, ultrasound of the vessels of the kidneys, ultrasound of the bladder). X-ray contrast studies of the urinary tract (excretory urography, voiding cystography, urethrography) are indicated only for repeated episodes of urinary tract infections in children and only in the remission phase. To study the state of the renal parenchyma, static or dynamic scintigraphy of the kidneys is performed.
Endoscopy methods in children (ureteroscopy, cystoscopy) are used to detect urethritis, cystitis, anomalies of the urethra and bladder. In order to study urodynamics, uroflowmetry and cystometry are performed.
Treatment of urinary tract infection in children
The main place in the treatment of urinary tract infections in children belongs to antibiotic therapy. Until a bacteriological diagnosis is established, initial antibiotic therapy is given on an empirical basis. Currently, in the treatment of urinary tract infections in children, preference is given to inhibitor-protected penicillins (amoxicillin), aminoglycosides (amikacin), cephalosporins (cefotaxime, ceftriaxone), carbapenems (meropenem, imipenem), uroantiseptics (nitrofurantoin, furazidin). The duration of the course of antimicrobial therapy should be 7-14 days. After completion of the course of treatment, a repeated laboratory examination of the child is carried out.
Until a bacteriological diagnosis is established, initial antibiotic therapy is given on an empirical basis. Currently, in the treatment of urinary tract infections in children, preference is given to inhibitor-protected penicillins (amoxicillin), aminoglycosides (amikacin), cephalosporins (cefotaxime, ceftriaxone), carbapenems (meropenem, imipenem), uroantiseptics (nitrofurantoin, furazidin). The duration of the course of antimicrobial therapy should be 7-14 days. After completion of the course of treatment, a repeated laboratory examination of the child is carried out.
It is recommended to take NSAIDs (ibuprofen), desensitizing agents (clemastine, loratadine), antioxidants (vitamin E, etc.), herbal medicine. Asymptomatic bacteriuria usually does not require treatment; sometimes uroseptics are prescribed in these cases.
When an acute urinary tract infection subsides, children are shown physiotherapy: microwave, UHF, electrophoresis, paraffin and ozocerite applications, mud therapy, pine baths.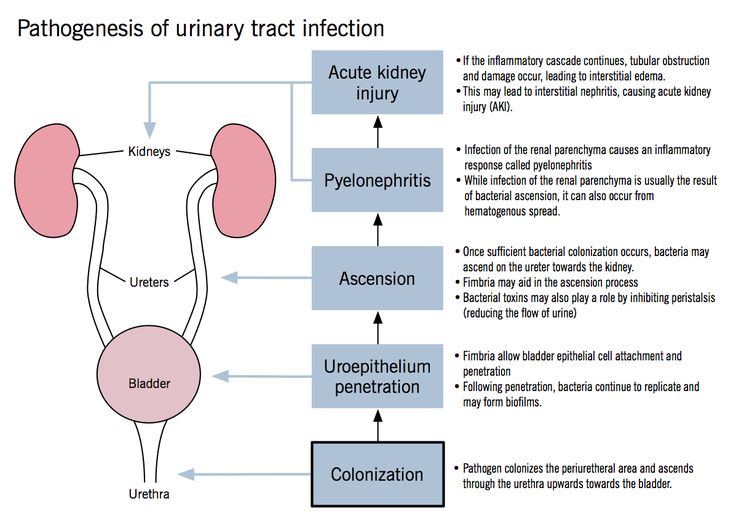
Prognosis and prevention
Advanced urinary tract infections in children can lead to irreversible damage to the renal parenchyma, kidney shrinkage, hypertension, and sepsis. Recurrences of urinary tract infections occur in 15-30% of cases, so children at risk are given anti-relapse prophylaxis with antibiotics or uroantiseptics. The child should be under the supervision of a pediatrician and a nephrologist. Vaccination of children is carried out during periods of clinical and laboratory remission.
Primary prevention of urinary tract infection in children should include the inculcation of proper hygiene skills, the rehabilitation of chronic foci of infection, and the elimination of risk factors.
Sources
- In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests. For diagnosis and proper treatment, you should contact your doctor.
Urinary tract infection in children
Urinary tract infection is the presence of a clinically significant number of bacteria in the urinary tract in a patient with clinical manifestations of infection [2]. This definition is given to us by foreign colleagues. In domestic recommendations, the definition is somewhat simpler, and this, in our opinion, creates some confusion in the heads of doctors, and, as a result, parents.
A urinary tract infection is a growth of bacteria in the urinary tract.
A little later I will explain why the difference in definitions is so important.
Urinary tract infection occurs at different ages with different frequency. It is customary to say that in children under 3 months the average frequency is about 7.2%, while in girls it is about 7.5%, and in boys it is 2.3% with circumcised foreskin and 20.1% without circumcision. At the age of over 3 months, such striking differences are no longer found, and the frequency of occurrence is 4.
 5–6.5%. And it remains approximately the same throughout the entire period of childhood, while in girls the frequency of occurrence is approximately 4 times higher than in boys [1].
5–6.5%. And it remains approximately the same throughout the entire period of childhood, while in girls the frequency of occurrence is approximately 4 times higher than in boys [1]. Why is a urinary tract infection dangerous?
First of all, the fact that as a result of the course of the infectious process, the death of some parts of the renal tissue may occur, as a result of which scars will form. This is called nephrosclerosis. It is bad because the scar, unlike the renal tissue, which is called the parenchyma, does not perform the functions of the kidney, that is, the renal function decreases. As a result, chronic kidney disease develops, or, as it was previously called, chronic renal failure.
Also, until we started discussing the causes and other things associated with UTIs in children, I want to note that the division of urinary tract infections in children into the usual cystitis, pyelonephritis at an early age is extremely difficult, in connection with this, it is customary to use a broad term UTI for children under two years of age.
Causes
The causes of any infection are infectious agents. There are several of them: bacteria, viruses, fungi, protozoa . In the case of urinary tract infections in children, the most common cause is bacteria . Urinary tract infections of viral etiology are extremely rare in children, usually they are children older than two years and it manifests itself most often as cystitis, fungal infections are always associated with immunodeficiencies, and therefore are also quite rare [3,2].
About bacteria: the leader in this matter is E. coli. Its share in the structure of the incidence of urinary infections accounts for about 80%. Of course, both Klebsiela and Proteus and various types of Staphylococci are capable of causing UTI and even cause it, but their proportion is not very large. Moreover, if we focus on the global evidence base, it is urinary tract infections caused by Escherichia coli that most often lead to the formation of nephrosclerosis [1,3,4].
Pathogenesis
A terrible word, this will probably be the most difficult to read section of this article, but without understanding it, it will be quite difficult to understand the logic of diagnosis and treatment. We will try to make it as accessible as possible.
A huge amount of research tells us that bacteria enter the urinary tract from below. In medicine, this is called the ascending pathway of penetration, but this is not particularly important. From below, this is not from the floor, as one might think, but from the skin of the perineum and the mucous membrane of the genital organs. However, this does not mean at all that it is urgent to wash the child with antibacterial soap.
- First, antibacterial soap was invented to wash the surgeon's hands before surgery.
- Secondly, in principle, washing the perineum with soap is not very good, bacteria will be there anyway, because their home is there.
Bacteria adapt - this is important.
In order for bacteria, like any organism, to survive, they have all sorts of useful devices. For example, small legs (drank), with which they can attach to the mucous membrane, or a capsule that protects the cell wall from an aggressive environment. All these things, bacteria acquire in the process of evolution and interaction with various environments. In addition, we ourselves actively help them in this matter, for example, when they use antibacterial drugs uncontrollably and incorrectly. [6, 7, 8]
After the bacteria have entered the urethra, they diligently begin to climb higher, and here our body has something to oppose to them.
-
The mucous membrane begins to actively produce mucus . The more bacteria, the more active. Mucus - firstly, it makes the attachment of bacteria not so strong. Try to hang on a dry horizontal bar yourself and hang on a horizontal bar that has been lathered with soap. The difference will be very obvious.
 In addition, when mucus is produced, the blood flow increases, and with the blood flow, a huge amount of very useful for protection comes to this place, including leukocytes and other substances that are so “favorite” by mothers, which, after getting into place, come to grips with the intruder. [1,6].
In addition, when mucus is produced, the blood flow increases, and with the blood flow, a huge amount of very useful for protection comes to this place, including leukocytes and other substances that are so “favorite” by mothers, which, after getting into place, come to grips with the intruder. [1,6]. -
The next defense mechanism is urine itself (just try to take it out of context and start using it, I will come in terrible dreams for the rest of my life).
-
The third protective factor that helps the body fight infection is urinary tract epithelium . It updates very quickly. And if the inflammatory process flows
The main protective properties of urine include the fact that it flows and this current washes away bacteria that do not cling very tightly to the wall due to mucus.
The second equally important property of urine is that it is acidic, and most bacteria do not really like an acidic environment, and if they do not die immediately in it, then at least they stop multiplying.
It is on this fact that the idea of taking cranberry-based drugs or products for prevention is based.
 The only problem is that the body is a little more complicated than a pot of soup, but more on that later.
The only problem is that the body is a little more complicated than a pot of soup, but more on that later.
So why does an infection still occur?
Mucus is released, urination has become more frequent, urine is acidic in itself, but this does not save if there are too many bacteria.
No matter how cool the 3 musketeers are, but there are only three of them, if the guardsmen have a numerical advantage, the musketeers cannot cope.
When is there a lot of bacteria?
-
When the path to be taken by bacteria is short (the female urethra is only 8–9cm, and men's - 20-25)
-
When a child cannot control a bowel movement (for example, in a diaper)
-
When there is an obstruction to the outflow of urine (hydronephrosis, vesicoureteral reflux, posterior urethral valve, bladder dysfunction, chronic constipation)
Usually these are the most common reasons that bacteria still break into the urinary tract.
After they have broken through, they begin to actively share, and here the help of doctors is needed.
It seems that we figured out the pathogenesis, drove on. I hope those who read carefully will be a little less afraid of a urine test with 3 leukocytes.
Clinical picture
Symptoms of UTIs in children differ depending on the age of the child [1].
It is customary to talk about signs of infection in a child younger than two years old.
Why are the manifestations different?
Most likely this is due to the fact that it is extremely difficult for a child under 2 years old to complain, and we are forced to focus on objective indicators of the disease.
Objective symptoms of UTI in a child under 2 years of age, most often only one - an increase in body temperature above 38.5 degrees Celsius, without other signs of infection. Namely, the pediatrician examines and ascertains the absence of cough, redness of the throat, runny nose and other signs of respiratory infections.
There are no other manifestations of urinary tract infection at this age!
What about our favorite urine test. Urine analysis is of clinical importance only if there is a guarantee of a sterile set of this very urine. Recommendations say that the guarantee of a clean collection is collection with a sterile urinary catheter or suprapubic puncture of the bladder. And one and the other way is only suitable for a doctor. That is, the urine collected by the mother in a jar to assess the presence of a urinary tract infection is not suitable. [1,2,4,5].
In children older than two years, additional symptoms of a urinary tract infection may appear, such as: frequent urination, pain when urinating, pain in the lumbar region or above the pubis.
But, here it is also very important that all this should be the same against the background of an increase in temperature above 38.5 degrees. Urinary tract infection in healthy children always occurs with fever.
No other is given. [9, 5] All parents whose children were diagnosed with chronic pyelonephritis by urinalysis, in the absence of clinical symptoms - congratulations. You most likely do not have any chronic pyelonephritis.
Separately, I would like to note such a moment as the smell of urine. There is a discrepancy between our recommendations and foreign ones. Foreigners say that the smell of urine is not a diagnostic symptom of urinary tract infection in children and at the same time refer to a number of clinical studies in which parents, using a questionnaire, noted that the smell was different from the usual one, and doctors, not knowing about the questionnaire, diagnosed UTIs. As a result, most studies have not found a clear statistically significant relationship between urine odor and UTI in children [1].
Our guidelines state that foul-smelling urine is a clinical criterion for urinary tract infection, without reference to anything [4]. This is how we write recommendations, nothing can be done about it.
Although, it should be noted that this is also not the main feature, so let's forgive our creators this discrepancy.
Why, in my opinion, the smell of urine has no clinical significance? Because the smell changes depending on a bunch of different factors that cannot be objectively taken into account.
Given the very minor manifestations of urinary tract infections in children, there are very few diagnostic methods, not because there are few methods, but because more is simply not needed. To diagnose a urinary tract infection in children, an examination by a pediatrician is sufficient. If the child can collect an average portion of urine, then a urine test will also help.
Also, if a urinary tract infection is suspected, ultrasound of the kidneys and bladder is performed in order to assess the condition of these same organs [2].
The main examinations begin after a urinary tract infection, as we need to exclude what is called in medical language - a complicated urinary tract infection.
Namely, anomalies in the development of the urinary tract.
Here again we run into differences, this time between the recommendations of pediatricians and the recommendations of urologists. The American Academy of Pediatrics considers that a single episode of urinary tract infection is not a reason to conduct an examination [1]. The American Association of Urology (there are no separate pediatric urologists and this is reasonable) does not agree with this idea, because there is about a 40% chance of missing vesicoureteral reflux and other pathologies that do not manifest themselves.
The European Association of Pediatric Urology also disagrees with the idea of no examination for a single urinary tract infection. As a result, until a consensus was reached in the following way: if the child had a urinary tract infection and, according to ultrasound, he does not have signs of expansion of the pyelocaliceal system of the kidneys, then you can not examine, but control the ultrasound of the kidneys and bladder.
If the child had a urinary tract infection more than 1 time, even without changes according to ultrasound, a complete urological examination is indicated [10].
Here, it is important to remember that the infection must be confirmed clinically. That is, there should be a clinical picture if we are talking about children under 2 years old. If the child is older than two years, then there should be a clinical picture, analysis and urine culture.
And the second point, which is no less important for children older than two years. If they have a urinary tract infection, it is imperative to indicate the location of the infection. This is where the well-known come on stage: cystitis and pyelonephritis.
How to treat?
Given the fact that we are talking about an infection, that is, about the presence of bacteria, we treat it with antibacterial drugs. The doctor at the appointment will tell you about the dosage, duration, etc., but there is no other method of treating the infection.
If someone says: you have a urinary tract infection - drink vitamins, dietary supplements, herbal remedies - this has nothing to do with treatment. In order to cure the infection, you need to kill the bacteria in the urinary tract.
Where, then, are all the different preparations for prophylaxis?
They are for prevention. But prevention is the measures we take to prevent re-infection. It is usually done after treatment, when we have proven clear test results and understand that there are no bacteria in the urinary tract.
What methods are available to prevent UTIs in children?
Given the fact that there are natural functions of the body that protect us from the penetration of bacteria into the urinary tract, prevention should begin influencing these very functions:
-
Drinking regimen - there is no norm for fluid intake. Here it is important to dance from the characteristics of the body, someone needs a little more, someone a little less, however, when a girl of 7-8 years old comes to the reception, fills out a urination diary and we understand that she drinks 400-500 milliliters of fluid per day - it is still very small.
A child under 3 years old usually drinks 200-900 ml. liquids. A child over 3 years of age usually drinks more than 1 liter. It is important to take into account all the liquid, and water and juice and tea and compote. That is, if a child drinks a cup of tea and 1 glass of water 4 times a day, most likely he does not have a deficit in fluid intake. Here our task is rather to offer a drink, since children tend to forget about it when they are busy with something interesting. -
An integral part of the drinking regime - urination . Just as a child can forget to drink, go to the toilet, he too can forget or delay. It is important to remind the child of this. On average, this must be done 1 time in 2-2.5 hours.
-
Control of vaginal microflora in girls . Yes, unfortunately, even in little girls, often recurrent urinary tract infections occur due to problems in the vagina or problems associated with the vulva. An examination by a gynecologist is very important, since often the symptoms attributed to cystitis are not related to it.
-
Control of stool regularity . A constipated child is the number 1 candidate for a urinary tract infection. It is important to consume a sufficient amount of fiber, to monitor the regularity of the stool. If you can’t solve problems with the stool on your own, you need to contact a pediatrician or gastroenterologist.
-
Antibiotic prophylaxis - a situation where a child is prescribed to take uroseptic drugs for a long time. Yes, there is such a method. Yes, it's in the instructions. But antibiotics do not cure the cause. If the infection recurs, there is a reason. The antibiotic treats the infection. The cause remains, which means that after the antibiotic is discontinued, it is likely to reappear.
Bladder infusions and instillations, physical therapy do not appear in the recommendations and decent studies, since there is no data on their effectiveness.
Currently, bacteriophage preparations are being actively studied and used for the prevention of urinary tract infections, including in children.
According to currently available data, these methods show good efficiency, but research is ongoing.
Terminals
As a conclusion, I would like to say that urinary tract infection is a rather wide problem for a number of reasons:
- Firstly, outpatient doctors have obvious difficulties in understanding the criteria for making this diagnosis and the tactics of examination and treatment of such children.
- Secondly, the cheapness and availability of basic urinalysis results in a huge stream of children with "bad" urinalysis who are prescribed therapy with the sole purpose of curing the analysis.
- Thirdly, at the same time, there is a fairly large number of children with recurrent cystitis, the diagnosis and treatment of which is carried out without taking into account any recommendations, using "author's" treatment regimens, which is unacceptable in medicine in general, and especially in pediatric practice. The inefficiency of such methods significantly increases the duration of the disease, reduces the quality of life of children and parents, in addition, economically, these methods can be very costly for the family budget.