Excess milk in breast
Too Much Milk and Oversupply
While it’s good to have plenty of milk, some mothers produce more milk than their babies need. This is commonly called oversupply and can be very challenging.
Some babies cope very well with a generous milk supply; however, some babies, whilst appearing to thrive, will be unhappy and uncomfortable. Oversupply can also make nursing uncomfortable for the mother and increase the risk of mastitis.
Symptoms
How does oversupply happen?
A note about foremilk and hindmilk
How your milk supply is established
What can I do to remedy symptoms of oversupply?
Reducing your milk supply
Coping with leaking
As milk flow slows
Adjusting to the new normality
Symptoms
The main symptoms of oversupply for a baby are:
- Very large weight gain (as much as 400g/14oz per week), moving upwards through centile lines
- Explosive green, frothy poos
- Struggling to control milk flow
- Pain and excessive wind or ‘gas’
You may also notice the following:
- Choking, coughing, spluttering at the breast
- Fussing, arching and pulling on and off the breast
- Clamping down or biting (to slow the flow of milk)
- Frequent spitting up
- Always appearing ravenous and unsatisfied despite large weight gain
- Unwillingness to nurse to sleep or find the breast a restful and calming place
- Breast refusal
- Faltering weight gain (due to breast refusal)
- Lots of wet and dirty nappies
- General ‘colicky’ behaviour
A mother with oversupply may have the following symptoms:
- Breasts that are rarely soft or comfortable
- A forceful or ‘over-active’ letdown
- A painful letdown
- Profuse leaking
- Painful nipples (from baby clamping and pulling on and off)
- Recurring blocked ducts and/or mastitis (see here for more info)
- Distress about your breasts not providing the calming place for your baby you had expected
Some of these symptoms may have other causes and they may also fall within the normal range, so it is important to rule things out before taking steps to reduce your milk supply, as this can have longer term consequences.
It is also important to consider all, and not just any one, of the symptoms and to consider them in context; for example, an occasional green poo does not indicate oversupply, and it is not uncommon for newborns to be gassy and have ‘colicky’ symptoms. Allergies, reflux and other problems can also present similar symptoms.
How does oversupply happen?
Some mothers naturally produce large quantities of milk and occasionally there are medical reasons for an over-abundant milk supply. In addition, we tend to produce more milk with each baby. Oversupply can also occur as a result of breastfeeding management, for example, if a baby’s feeds are scheduled or if a mother is told to feed from each breast for a certain amount of time.
You may be given conflicting information about foremilk and hindmilk and how long a feed ‘should’ last, or you may be encouraged to express milk to stay ahead of demand. Sometimes these ‘rules’ interfere with the regulation process. Milk production is best regulated by your baby’s appetite.
When you breastfeed responsively, following your baby’s cues (and your body) rather than a schedule, milk production adapts to their needs. Occasionally, an ineffective latch can contribute to oversupply, as a baby might feed very frequently to get the volume they need; however, more typically, this tends to reduce milk supply over time.
A note about foremilk and hindmilk
There is a common misconception that the breasts make two different kinds of milk – thirst-quenching, lower-fat foremilk and fat-rich hindmilk – and that one is inferior to the other; this is not the case! All breastmilk is good; however, typically, the fat content increases during the feed, as the fat globules stick to the ducts and tend to be drawn down towards the end of a feed.
You may be encouraged to feed on one side for a certain length of time in order to ‘get to the hindmilk’; however, it is not the length of a feed that is important, it is the length of time between feeds. Why? The length of a feed doesn’t determine its fat content; some babies get everything they need in 5 minutes! Fat content is determined by the fullness of the breast. If there is a long gap between feeds and the breast is full, the baby may get a large quantity of lower-fat milk before much of the fat starts getting pulled down. The same may be true if a mother naturally produces very large quantities of milk. In the absence of fat-rich milk, the lower-fat milk moves through the gut faster than it can be digested, leading to fermentation and signs of lactose overload, such as green, frothy stools, ‘gas’ and pain.
If there is a long gap between feeds and the breast is full, the baby may get a large quantity of lower-fat milk before much of the fat starts getting pulled down. The same may be true if a mother naturally produces very large quantities of milk. In the absence of fat-rich milk, the lower-fat milk moves through the gut faster than it can be digested, leading to fermentation and signs of lactose overload, such as green, frothy stools, ‘gas’ and pain.
What is most important to a baby’s weight gain is the total volume of milk every 24 hours. When your baby is feeding effectively and you allow them to determine the length and frequency of breastfeeds, they will also get the right balance.
You can find more about the fat content of milk here
How your milk supply is established
Before you baby is born, milk production is hormonally driven. After birth and the delivery of the placenta, milk production is regulated on a supply and demand system; the more milk your baby removes, the more milk you are likely to make. How quickly or slowly milk is made depends on the fullness of the breast. When the breast is less full, milk is made more rapidly. When the breast is full, milk production slows down.
How quickly or slowly milk is made depends on the fullness of the breast. When the breast is less full, milk is made more rapidly. When the breast is full, milk production slows down.
Typically, milk supply takes 6-8 weeks, and sometimes up to 12 weeks, to regulate. Nature can be overly generous at first and it can take time for your supply to settle down to what your baby actually needs. It is not unusual in the early weeks to feel as if you have too much milk and it is not unusual to have periods when the breasts feel engorged. Feeding frequently and removing milk from the breasts is essential to resolving engorgement; it won’t make the engorgement worse or result in too much milk.
Periods of increased nursing due to development changes and growth spurts can also cause fluctuations in supply. Many mothers find there are changes to their babies’ nursing patterns during holidays and family get-togethers, or during periods of stress. Milk supply is very adaptable; if you follow your baby and your body, rather than the clock or a schedule, your supply will most likely regulate itself at these times.
What can I do to remedy symptoms of oversupply?
In the first instance, you might like to consider adjusting positioning and attachment to help your baby manage a fast letdown, feeding responsively (‘on demand’) and/or offering more frequent feeds, and using breast massage.
Managing a Fast letdown
When your baby suckles at the breast, a neurohormonal reflex causes milk to release. This is known as the Milk Ejection Reflex (MER) or, more commonly, letdown. In the early weeks, it is not uncommon for this to occur just by thinking about or hearing your baby!
When the milk ‘lets down’, it is not unusual for it to spray out, and sometimes with a degree of force. Whilst some babies aren’t bothered by this fast flow, others are upset and distressed by it. They may gulp and cough and pull on and off the breast, as they struggle to coordinate sucking, swallowing and breathing. A fast letdown can be a symptom of oversupply; however, it is possible to have a fast letdown with an average milk production.
Unless your baby is showing other signs of oversupply (explosive green poo, pain and large weight gain), then it might be worth reviewing and experimenting with the following:
- Ensure that your baby is deeply attached at the breast – it is easier for a baby to manage a fast flow if they are deeply latched. An LLL Leader can help you adjust positioning and attachment.
- Adjust your body – make use of gravity by feeding in a ‘laidback’ (reclined) position. Some mothers find it helps to feed in an upright position or side-lying so that the excess milk can easily dribble out. Breastfeeding in a position where your baby’s head is higher than your breast, so that you are not leaning over, can help your baby to manage the flow.
- Allow your baby to come off the breast when he needs to catch his breath. Keep your supporting hand down near your baby’s shoulders and neck to avoid pushing on the back of his head. Have a muslin to hand to catch the spray.
- Let the flow subside by taking your baby off the breast, catching the spray in a muslin and then bringing him back to the breast.
 Your baby will have an easier time nursing when the flow slows. Some mothers hand express a little to slow the flow before bringing the baby to the breast; however, if this is done frequently, it may exacerbate oversupply. If your breast is very full and engorged, you might try reverse pressure softening to move fluids away from the nipple area, which can help your baby to latch more deeply. You can read more about this here
Your baby will have an easier time nursing when the flow slows. Some mothers hand express a little to slow the flow before bringing the baby to the breast; however, if this is done frequently, it may exacerbate oversupply. If your breast is very full and engorged, you might try reverse pressure softening to move fluids away from the nipple area, which can help your baby to latch more deeply. You can read more about this here - Feed frequently so that the spray doesn’t have quite so much volume and force behind it.
- Try breastfeeding before your baby is really hungry or while they are slightly sleepy – if your baby is relaxed she may nurse more gently, be more coordinated and receive a slower flow of milk.
Responsive feeding
How do you know how often or how long to feed your baby for? Let your baby tell you! We all have different milk storage capacities and this may determine how frequently your baby feeds and whether they feed from one side or two.
A good approach is to let your baby take as much milk as they want from the first breast. If they come off looking satisfied and your breast feels soft and comfortable, then offer the second breast; they may or may not take it. If your baby isn’t satisfied and wants to nurse again after a short period of time and the first breast still feels full, offer the first breast again, then offer the second breast.
Sometimes babies will only take one breast and sometimes two (or three or four!). Most babies will take both breasts, at least some of the time. Babies are very good at letting us know how often they want to feed and, if in doubt, it is always fine to offer.
Breast massage
You could also do what is sometimes called the ‘breast milkshake’. This term was coined by American lactation consultant Christina Smillie and involves gently massaging each side for half a minute or so before feeding and then using a combination of massage and breast compressions during a feed to help dislodge some of the fat. Massage during a feed can also help to prevent blocked ducts or areas of engorgement.
Massage during a feed can also help to prevent blocked ducts or areas of engorgement.
Sufficient fat-rich milk leads to the production of cholecystokinin (CKK) at high enough levels to give a feeling of satiety. Without enough fat-rich milk, a baby acts hungry even though he has a full stomach; he feels uncomfortable and windy because of his overfull stomach so may want to nurse even more, for comfort as well as food, creating a vicious cycle.
You can find information about breast compressions below
Reducing your milk supply
If your baby is gaining more weight than average and you and your baby are happy, then you don’t need to change anything. If you or your baby are suffering from some of the above symptoms, you have ruled out other causes and changes to breastfeeding management do not help, then you may want to consider taking steps to gradually slow milk production.
Consult an LLL Leader before using these approaches. This is especially important if your baby is under one month old, or you are experiencing other problems such as sore nipples or mastitis.
Monitor your baby’s weight gain to ensure it doesn’t drop below expected levels (at least 20-30g a day, on average, during the first three or four months) and keep a close eye on nappy output.
One side per feed
Limit your baby to one breast per feed. If your baby wants to come to the breast again for comfort or connection before the next full feeding, stay on the first breast. When a mother has a generous milk storage capacity, her baby may only need to feed on one side and this approach may help to calm things down. Should the unused breast feel uncomfortably full before the next feed, then express to comfort only. This will help avoid developing blocked ducts or mastitis and may also make milk flow more manageable for your baby. Avoid excessive pumping, as it can make things worse.
Block feeding
Block feeding involves feeding on the same side for set periods of time, e.g. for two or three hours (or longer depending on the severity of your oversupply). If your baby wants to feed again within that timeframe, offer the same side. Again, If the other breast feels uncomfortably full before the next feed, then express to comfort only. As a starting point, you might like to:
If your baby wants to feed again within that timeframe, offer the same side. Again, If the other breast feels uncomfortably full before the next feed, then express to comfort only. As a starting point, you might like to:
- Limit your baby to one breast for about two hours, allowing him to nurse as often and as long as he likes, but only on that one side.
- Continue in this way, switching breasts every two hours. If your baby is asleep, switch breasts when he wakes.
It is important not to have a rigid approach to block feeding; it is much more a matter of reading your breasts and your baby than the clock. By doing this, you will find the time interval that works best for you and your baby, by slowing production at the same time as ensuring that your baby is fed.
It is possible to experience oversupply in just one breast, in which case you could nurse for longer periods on the unaffected side. Watch for blocked ducts and sore areas on your breast. If you’ve been expressing regularly, reduce this gradually to avoid further problems.
If you’ve been expressing regularly, reduce this gradually to avoid further problems.
By sticking to one side per feed or for set intervals of time, the unused breast will be fuller. A full breast makes milk more slowly and, therefore, you will gradually reduce your supply.
Full drainage and block feeding method
For more severe oversupply – for example, if you are suffering from recurrent blocked ducts or mastitis and your breasts never feel soft and comfortable, even after a breastfeed – you will need to keep your breasts well-drained while you take steps to reduce milk production.
You could try the following, in consultation with an infant feeding specialist, in addition to block feeding:
- Express from both sides thoroughly to “empty” your breasts as fully as possible.
- After expressing, immediately offer both “empty” breasts to your baby.
- Next, limit your baby to one breast changing sides every two or three hours (as per block feeding above).

Some mothers will need to use this approach only once. However, if your breasts feel uncomfortably full you may need to repeat it, increasing the interval between each pumping, before your breasts completely readjust.
Herbs
Some mothers have had success using herbal preparations, such as sage, parsley and peppermint, or homeopathic remedies to slow milk production. Prescribed and over-the-counter medications (such as pseudoephedrine) can also be used in this way. When using herbs or medications, it is important to consult with someone knowledgeable in their use and with your healthcare provider.
If you still have problems
After 4-7 days, your breasts may be more comfortable. If your baby still has trouble coping with the supply of milk, and/or has other symptoms and you are not experiencing uncomfortable engorgement, you can increase the block of time you keep your baby to one breast. It’s important to build up the time you limit your baby to one breast very gradually – an extra hour or two at a time – so you experience comfortable fullness while avoiding blocked ducts and mastitis.
Some women with extreme oversupply have gone as long as six or more hours before switching breasts to adjust milk production. Rarely, a hormonal imbalance may cause overproduction of milk. A visit to your doctor may be helpful if the suggestions offered here aren’t enough.
Block feeding should be a temporary measure. Typically, it is suggested that it is done for no more than one week and only when babies are gaining double (or more) the average weight. Once supply has settled, you can return to a more normal feeding pattern, following and trusting your baby and your body.
Coping with Leaking
Breast pads inside your bra will provide some protection from leaks. Avoid plastic backed pads, as these can trap wetness next to the skin and cause soreness.
If you feel the tingling of your milk beginning to flow, pressing hard on your nipples and areolas for several seconds may prevent leaking. This can be done quite unobtrusively by crossing your arms tightly across your chest and pressing firmly on your nipples with the palms of your hands for a few seconds before releasing. If it doesn’t work first time, try again for a little longer, but bear in mind that if your breasts feel full, this may be a sign to take the time to nurse your baby.
If it doesn’t work first time, try again for a little longer, but bear in mind that if your breasts feel full, this may be a sign to take the time to nurse your baby.
As milk flow slows
Babies used to an abundant milk flow can become fussy at the breast when milk flow slows. They may also have become used to having a more shallow latch, as they have not had to work as hard to get milk. Ensuring your baby has a good, comfortable latch can help them remove milk effectively. You can use breast compressions to increase milk flow and encourage your baby to keep feeding actively. Breast compressions can also help to release more of the fat-rich milk:
- Support your breast with one hand – thumb on one side, fingers on the other.
- Wait while your baby breastfeeds actively, his jaw moving all the way to his ear. When he stops swallowing, compress your breast firmly. Hold it squeezed until he stops nursing actively and then release your hand.
- Rotate your hand around your breast and repeat step 2 on different areas of the breast as needed.
 Go gently – this should not hurt.
Go gently – this should not hurt.
Adjusting to the new normality
Always monitor your baby’s wet and dirty nappies, weight gain and overall well-being while following these strategies. Your baby’s weight gain may slow, especially if he has been comfort nursing to cope with the discomfort of lactose overload. A healthy baby will nurse to get the calories he needs – so follow his cues. A growth chart will indicate how he is doing (see Further Reading). Monitor weight over a period of several weeks to see a trend. If your baby has been gaining excessive amounts because of oversupply you may see ‘catch-down’ growth. Your baby will gain weight steadily, but may gradually drop against the percentile lines as your milk production adjusts. His weight should then settle into following a new percentile line on the chart.
Crossing more than one percentile line may be a sign you need to stop reducing your milk supply. Most mothers with oversupply usually find it easy to increase milk production by switching breasts more often if their babies’ weight gain drops too low or when their babies have a growth spurt.
As things get more manageable, your breasts will feel softer and more comfortable and leaking will be reduced. Soft comfortable breasts between feeds during the early weeks are normal and a sign that your milk production is in tune with your baby’s needs. As your baby grows, gradual baby-led weaning can help avoid problems caused by sudden changes in feeding pattern and missed feeds. These strategies really can make a difference to both you and your baby if you have an overabundance of milk. You may also find it helpful to meet with other mothers at your local LLL group where you can exchange practical tips on nursing and mothering.
Written by Charlotte Allam, Karen Butler, Sue Upstone and mothers of La Leche League GB
Kimberly Seals Allers’ photos on this site are used under a creative commons license of Black Breastfeeding 360° http://mochamanual.com/bb/
Further Reading
Mastitis
Engorged Breasts – Avoiding & Treating
Hand Expression of Breastmilk
Is My Baby Getting Enough Milk
Comfortable Breastfeeding
Rhythms & Routines
The Unhappy Breastfed Baby
Allergies and Intolerances
Fat Content of Breastmilk – FAQs
Positioning and Attachment
Other websites
UK–WHO Growth Charts: www. rcpch.ac.uk/growthcharts
rcpch.ac.uk/growthcharts
Gastro-oesophageal Reflux: https://abm.me.uk/wp-content/uploads/ABM-reflux-breastfeeding-baby.pdf
Oversupply of Breast Milk: https://breastfeeding.support/oversupply-breast-milk/
Block Feeding Dos and Don’ts: http://www.nancymohrbacher.com/articles/2013/10/9/block-feeding-dos-donts.html?rq=oversupply
Foremilk and Hindmilk: http://www.nancymohrbacher.com/articles/2010/6/27/worries-about-foremilk-and-hindmilk.html
Books
The Womanly Art Of Breastfeeding. LLLI, London: Pinter & Martin, 2010
LLLGB kindle edition of Positioning & Attachment
References
ABM Clinical Protocol #4: Mastitis. Breastfeeding Medicine 2014; 3(3): 177-180.
Livingstone, V. The maternal hyperlactation syndrome. Medicine North America 1997; 20(2): 42-46.
Smillie, C. Campbell, S. & Iwinski, S. Hyperlactation: how left-brained rules for breastfeeding can wreak havoc with a natural process. Newborn Infant Nurs Rev 2005; 5: 49-58.
Van Veldhuizen-Staas, CGA. Overabundant milk supply: an alternate way to intervene by full drainage and block feeding. Int Breastfeed J 2007; 2(11) available online at: www.internationalbreastfeedingjournal.com/content/2/1/11
Wilson-Clay, B. Consultants’ Corner—Milk oversupply. Journal of Human Lactation 2006;22(2): 218-220.
Copyright LLLGB 2021
Oversupply of breastmilk | Pregnancy Birth and Baby
beginning of content4-minute read
Listen
A mother’s milk supply usually adjusts to her baby’s needs after about 4 weeks of breastfeeding. Some mothers continue to make more milk than the baby requires, and this is known as ‘oversupply’.
Oversupply can make breastfeeding difficult for both mother and baby.
What are the causes of oversupply?
Breastmilk oversupply that continues after the first 4 weeks or so can have many causes. Feeding patterns may cause the oversupply, such as:
Feeding patterns may cause the oversupply, such as:
- feeding the baby on a set schedule rather than according to need
- pumping too much before a feed to make the breast soft and easier for the baby to latch onto
- the baby preferring to feed mainly from 1 breast
Other causes of oversupply include:
- an excess of the milk production-stimulating hormone prolactin in your blood (hyperprolactinemia)
- a congenital predisposition
How breastmilk oversupply affects your baby
Your baby may be unsettled or distressed during and after feeding, and it can be hard to know whether they are still hungry or are getting too much milk too fast. Your baby may:
- choke and splutter at the breast due to the high rate of milk flow
- have trouble latching onto the breast
- feed for only short periods of time leading to ‘lactose overload’
- have a lot of urine (more than 10 wees a day) or diarrhoea with green, frothy poos and nappy rash
- have excessive wind, causing unsettled, colicky behaviour
- bring up a lot of milk after breastfeeding
- put on weight quickly
How breastmilk oversupply affects you
Oversupply can also cause problems for you.
You might feel your breasts refill very quickly after feeding your baby. They might feel lumpy and tight after breastfeeding. You might also leak more than usual or have an explosive milk-ejection reflex, which makes it difficult to feed in public, and can cause difficulties for your baby at the beginning of feeding.
You could develop blocked milk ducts or mastitis and breast abscesses.
Oversupply can make breastfeeding a less pleasurable experience for you or your baby. Some mothers think about early weaning if oversupply is not diagnosed and managed well.
How is breastmilk oversupply diagnosed?
It is essential to have a health professional such as a lactation consultant, breastfeeding counsellor, doctor or child health nurse watch your baby breastfeed to diagnose true oversupply. It can easily be confused with breast engorgement or a fast ‘let-down’ reflex.
For help with the diagnosis and treatment of oversupply, contact a health professional, such as a lactation consultant, breastfeeding counsellor, or child health nurse, or call Pregnancy Birth and Baby on 1800 882 436.
How is breastmilk oversupply treated?
The aim of treatment is to reduce your milk production. This is best done while you are being supported by a lactation consultant, breastfeeding counsellor, or child health nurse.
‘Block feeding’ is a method that can help reduce milk supply in just a few days:
- Choose a time frame, usually from 3 to 4 hours, and feed your baby from only 1 breast during that time.
- Then change to the other breast for the same time period.
- Continue this pattern for a few days.
- You might need to hand express a small amount from the unused breast to relieve pressure or discomfort, but don’t empty it — the residual milk in the unused breast triggers the reduction in milk production.
Block feeding ensures that 1 breast always contains residual milk. This will trigger both breasts to reduce milk production, and should gradually resolve oversupply of milk. How long it takes depends on your situation.
Block feeding will also help to reduce the amount of thinner foremilk consumed by your baby. As your baby gets to drink more of the creamy hindmilk, you’ll see your baby’s stools get thicker. This tells you that you are on the way.
As your baby gets to drink more of the creamy hindmilk, you’ll see your baby’s stools get thicker. This tells you that you are on the way.
If your milk supply does not respond to block feeding, talk to your doctor.
The Australian Breastfeeding Association website has more tips about managing oversupply.
Sources:
Australian Breastfeeding Association (Too much milk), Australian Breastfeeding Association (Lactose overload in babies), Raising Children Network (Oversupply of breastmilk and engorgement), King Edward Memorial Hospital Obstetrics & Gynaecology (Clinical Practice Guideline: Breastfeeding challenges: oversupply/hyperlactation), Breastfeeding USA (Oversupply: Symptoms, causes, and what to do if you have too much milk))Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: January 2021
Back To Top
Related pages
- Breastfeeding your baby
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Some features, tools or interaction may not work correctly.
Too much milk? Reduced lactation
Sometimes you may feel like you are producing too much milk, especially in the first weeks of breastfeeding. After reading our article, you will find out if you really have too much milk, and what can be done to reduce it.
Share this information
Breast milk is very healthy, so it's good to have a lot of it, right? However, this is not always the case. Babies can sometimes have a hard time coping with the rapid rush of milk that usually accompanies excess lactation. And mothers who have too much milk often experience discomfort due to the constant leakage of milk and often suffer from mastitis.
Fortunately, there are a number of ways to help in this situation. But before you use them, answer two important questions:
Do I really have too much milk?
Some of the symptoms of over-lactation (listed below) may occur for very different reasons. You should not try to reduce the production of breast milk, if you are not sure that it is the overabundance of it that is the main problem. Otherwise, this can lead to the fact that your baby will produce less milk than your baby needs, especially in the critical first month when production is just being established.
You should not try to reduce the production of breast milk, if you are not sure that it is the overabundance of it that is the main problem. Otherwise, this can lead to the fact that your baby will produce less milk than your baby needs, especially in the critical first month when production is just being established.
Is being overweight a problem for me or my baby?
If you are sure that you have an excess of milk, but this does not cause problems for you and your baby, you do not need to do anything. In most cases, everything returns to normal within the first few months. As the baby grows, he will learn to better cope with the rapid flow of milk and will feed with pleasure.
Leakage is not always a sign of too much milk
During the first four to six weeks of your baby's birth, the level of prolactin, the hormone responsible for milk production, will rise each time the breast is emptied. In these first weeks, the breast learns to produce milk in the amount that the baby needs, depending on the time of day. Therefore, excessive leakage, rapid filling of the breast, and even splashing of milk during a rush are the norm. 1
Therefore, excessive leakage, rapid filling of the breast, and even splashing of milk during a rush are the norm. 1
At the same time, your baby is learning to suck and swallow milk, so you shouldn't be surprised if he suddenly coughs or chokes when he suckles.
After about four to six weeks, the spikes in prolactin levels will begin to fade and milk production will become more balanced, adjusting to your baby's needs on a supply and demand basis. 2 However, given the many hormonal changes that occur in the body of a young mother, such a restructuring may take some time. In some mothers, milk production is established quickly, in others a little longer.
Behavior of the child, which may indicate an excess of milk
When overproduced, milk is usually released very quickly, especially during the first flush. As a result, the baby may cough or choke at the beginning of a feed, push back, or hold the breast loose in the mouth. The baby may pull away from the chest, frightened by a quick rush, and then cry because he hasn’t eaten. He can swallow milk in large volumes and with a lot of air, and after that he will spit up a lot. Try to be as careful as possible when you help him burp - sudden movements combined with a full tummy can cause the baby to vomit and scare him even more.
He can swallow milk in large volumes and with a lot of air, and after that he will spit up a lot. Try to be as careful as possible when you help him burp - sudden movements combined with a full tummy can cause the baby to vomit and scare him even more.
At the start of a feed, milk is relatively low in fat and consists mainly of lactose (sugar) and proteins. As the breast is fed and emptied, the fat content constantly increases. In the case of excess milk production, your baby may feel full before he completely empties his breast. This means that he will get a lot of lactose-rich milk, but not enough fat-rich milk that comes towards the end of a feed. Excess lactose instead of a balanced diet can make digestion difficult and cause hard, frothy, and greenish stools.
Oddly enough, in such a situation, the baby may constantly want to eat and behave restlessly between feedings. Despite the high calorie content, the low fat content of milk prevents it from being fully satiated. It is the fat contained in food that gives us a feeling of satiety. What happens if you eat a few dozen rice crackers or a slice of cheese with a cookie instead? You will fill up on cheese faster, as it is more saturated with fats.
It is the fat contained in food that gives us a feeling of satiety. What happens if you eat a few dozen rice crackers or a slice of cheese with a cookie instead? You will fill up on cheese faster, as it is more saturated with fats.
However, all these symptoms can be caused by completely different problems, such as reflux, allergies, or even vice versa, insufficient milk production. An excess of breast milk can indeed cause these symptoms, but only if they are accompanied by excessive weight gain. Children usually dial around 900 g per month, but in the case of an excess of milk, they can gain much more, often almost twice as much. 1 If you feel like you are having too much milk but your baby is gaining weight normally, contact your lactation consultant or your healthcare provider.
Symptoms that may indicate an excess of milk in mothers
Mothers with an excess of breast milk often experience swelling and tightness in the breast, which constantly seems full. 3 As already noted, the leakage of breast milk in the first six weeks does not indicate its excess. However, if this continues at every feeding and after this period, it may be that the problem is in the overabundance.
3 As already noted, the leakage of breast milk in the first six weeks does not indicate its excess. However, if this continues at every feeding and after this period, it may be that the problem is in the overabundance.
A baby cannot always empty a full breast, so when there is an excess of breast milk, blockage of the milk ducts or periodic bouts of mastitis often occur. However, these problems can also be caused by other reasons.
How to reduce milk production
If you have found that you have too much breastmilk and this is causing you concern, here are a few simple things that can help. For some mothers, they are enough.
- Try feeding in a relaxed position. Reclining or lying down feeding will allow the baby to better control the process. In this position, the baby sets the rhythm of feeding himself and can always raise his head to take a break if the milk is released too quickly. Don't forget to put a towel over to soak up spilled milk.

- Release pressure. If full breasts make you uncomfortable, try expressing some milk by hand or with a breast pump, but try to express as little milk as possible. Every time you empty your breast, you send a signal to her to produce even more milk. Therefore, pumping provides short-term relief, but with prolonged use, it can only aggravate the situation. If you need to express and store milk to feed your baby when you are not around, it is best to address the problem of excess production first.
- Try bra pads. If you have milk leaks, put special pads or pads in your bra to collect milk* to keep your underwear dry. If your milk leakage is moderate and already decreasing, or your breasts leak slightly during pregnancy, ultra-thin disposable pads will help you feel confident in any life situation.
- Avoid teas and lactation supplements. If you have been drinking teas, eating special biscuits, or taking supplements to improve breast milk production, this should be stopped now to resolve the problem.

"Breast Watch" to reduce milk production
If all the above methods fail, you can try a technique called "Breast Watch", which allows you to better control milk production. However, before trying this method, check with a lactation consultant or healthcare provider.
On breastfeeding, you feed your baby on demand, but only on one breast for four hours. The second breast during this time is strongly filled. Since breast milk contains what is known as a "feedback lactation inhibitor", due to overfullness, the body sends a signal to that breast to slow down milk production. This is a natural way to protect the breast from endless filling.
This technique must be applied for 24 hours, changing breasts every four hours. If the milk does not become less, try increasing the duration of the "watch" to six hours.
Complete emptying and “breast duty” technique
If after another day there is still a lot of milk produced,
you can try another version of this technique, which is recommended in cases of extreme overabundance. It is called "complete emptying and duty of the breast." 3
It is called "complete emptying and duty of the breast." 3
In this method, both breasts must be completely emptied in the morning with an electric breast pump and breastfeeding should be started immediately. The flow of milk will be weaker and allow the baby to eat calmly. In addition, he will get more fat-rich milk, which comes at the end of feeding, which means he will feel more full.
After that, you can continue the "breast watch" for four hours, as described above. If that doesn't help, try increasing the interval to six, eight, or twelve hours the next day, depending on the extent of the problem. Before using this technique, be sure to consult with your doctor.
You may not need to completely empty your breasts after the first use of this technique, but some mothers have to do this once or twice. Improvement usually occurs within the first two days or a little later, but in no case should "breast watch" be used for more than five days.
Literature
1 Morbacher N.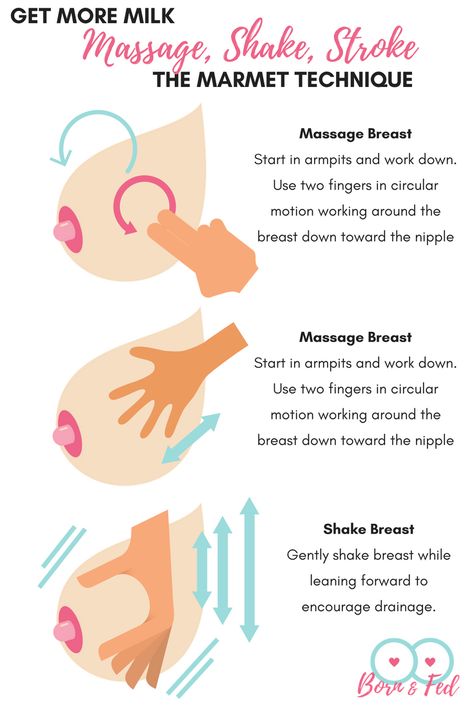 Breastfeeding answers made simple. Amarillo TX , USA : Hale Publishing ; 2010. - Morbacher N., "Simple answers to questions about breastfeeding." Amarillo, Texas, USA: Publishing Hale 0106 et al . Blood and milk prolactin and the rate of milk synthesis in women. Exp Physiol. 1996;81(6):1007-1020. - Cox D.B. et al., Effects of blood and milk prolactin on milk production in women. Exp Physiol. 1996;81(6):1007-1020.
Breastfeeding answers made simple. Amarillo TX , USA : Hale Publishing ; 2010. - Morbacher N., "Simple answers to questions about breastfeeding." Amarillo, Texas, USA: Publishing Hale 0106 et al . Blood and milk prolactin and the rate of milk synthesis in women. Exp Physiol. 1996;81(6):1007-1020. - Cox D.B. et al., Effects of blood and milk prolactin on milk production in women. Exp Physiol. 1996;81(6):1007-1020.
3 van Veldhuizen-Staas CG. Overabundant milk supply: an alternative way to intervene by full drainage and block feeding. Int Breastfeed J . 2007;2(1):11. - van Velhusen-Staas SJ, "Milk Overabundance: An Alternative Countermeasure by Total Drying and Blocking of Feeds." Int Brestfeed J (International Journal of Breastfeeding). 2007;2(1):11.
2007;2(1):11.
Read instructions before use. Consult a specialist about possible contraindications.
* RC № FZZ 2010/07352 dated 19.07.2010
Breast milk production | Baby's needs
Did you know that the amount of breast milk adapts to your baby's needs? In this article, you will learn amazing facts about breast milk production in the first days, weeks and months.
Share this information
Your body is capable of producing breast milk for your baby at every stage of development. Understanding how milk production “turns on”, what happens to milk when you feed your baby, and why production adjusts to his needs as he grows, will help you start this amazing process in the right way.
Day one: milk production at birth
The baby is usually ready to breastfeed from birth. When he grabs the breast and begins to suck rhythmically, the milk-producing cells “turn on” and the formation of the first breast milk, colostrum, starts. 1 Try to feed your baby as much as possible in the first hour of his life, and then as soon as he shows interest in feeding. This will help lay the foundation for good milk production later on. 2
1 Try to feed your baby as much as possible in the first hour of his life, and then as soon as he shows interest in feeding. This will help lay the foundation for good milk production later on. 2
The first days: the arrival of milk
At this stage, your body's level of progesterone,
pregnancy hormone, which begins to fall after the placenta comes out, is reduced, and the hormones responsible for milk production - prolactin, insulin and hydrocortisone - are included in the work. These hormones will help start milk production. 3 Approximately on the third day of the baby's life, milk will begin to come in, and you will feel that the breast is full and has become noticeably firmer. 1
First month: shaping milk production
During the first weeks, your body will be especially sensitive to the amount of milk produced as it learns to produce the right amount. Prolactin levels increase dramatically each time you empty your breasts, thereby helping shape the lactation process. It also contributes to the maturation of your milk in terms of composition. At this stage, transitional milk is produced and the amount continues to grow. 3.4
It also contributes to the maturation of your milk in terms of composition. At this stage, transitional milk is produced and the amount continues to grow. 3.4
For good long-term milk production, it is very important that you are close to your baby during the first few weeks. The more often you breastfeed, the more milk will be produced. This process resembles the law of supply and demand. Each time after emptying the breast, whether it is feeding the baby or pumping, even more milk will be produced.
Remember that it is normal for newborns to eat frequently, perhaps even every 45 minutes, and this does not mean that they are not getting enough milk. Frequent feedings help shape milk production, so feed your baby on demand, not on a schedule.
“In the first few weeks you may feel like you don’t have enough milk because your baby will be feeding all the time, but that’s okay,” says UK mom-of-two Jo, “We tend to think that the baby wants to eat every few hours, but that is not necessarily the case. "
"
Don't forget that babies also breastfeed for comfort. Breastfeeding helps them calm down and adjust to their new life outside the womb. In addition, feeding helps to establish a connection between you.
Stable milk production in the first month
If you follow your baby's needs and feed him as often and for as long as he wants, milk production should adjust. 5
Some mothers try to increase the period between feedings so that the breasts can produce more milk during this time, but this should not be done, as this may have the opposite effect. 2
If you are unable to breastfeed directly for the first two weeks, express your milk to build and maintain your milk supply during this critical period and beyond.
Did you know that feeding your baby extra formula unnecessarily can reduce your milk production? The chest will not receive a signal to increase production, because it will not be emptied. In addition, if the baby sleeps longer after formula, he may miss his usual next feeding time.
This is a kind of “supplementing trap”. After three to four days of formula supplementation, during which the breasts have emptied less, the body will receive a signal that breastfeeding has stopped, and the amount of milk produced will begin to decrease. As a result, the baby will remain hungry and will need additional formula supplementation. And so on in a circle ... As a result, this will lead to really low milk production, and the baby will eat mainly the mixture.
Breast milk production after six weeks
After a month of breastfeeding, post-feeding bursts of prolactin secretion begin to decrease, milk matures, and the body gets used to producing as much milk as your baby needs. In fact, the chest begins to work "on autopilot." 4 You may also notice at this time that your breasts are softer and your milk flow has stopped.
At this stage, women often have fears of "losing milk".
However, this only means that milk production has been established and now fully meets the needs of the child. It is noteworthy that although the baby continues to grow, he will consume approximately the same amount of milk both at six weeks and at six months. You may notice that the baby began to suckle the breast longer, but less often. On some days he may eat a little less than usual - his appetite changes in the same way as an adult.
It is noteworthy that although the baby continues to grow, he will consume approximately the same amount of milk both at six weeks and at six months. You may notice that the baby began to suckle the breast longer, but less often. On some days he may eat a little less than usual - his appetite changes in the same way as an adult.
Now your body will produce exactly the amount of milk,
as much as your baby needs. Therefore, the more milk the baby drinks (or you express), the more milk will be produced.
How does this happen? The reason for this is thought to be the so-called "feedback lactation inhibitor" that controls milk production. The more milk in the breast, 2 the higher the inhibitor level, so a full breast produces less milk than one that has been emptied.
What is the rate of milk production?
Mothers often worry about their milk supply and think about how to increase it. However, if the baby is healthy and growing well, problems usually do not arise.
“I was worried that my newborn daughter was not getting enough milk as she was feeding very quickly and always from one breast even though I offered both,” says Marjorie, mother of two in the UK, “But when I pumped from using a breast pump, I was surprised at how much milk I produced, and calmed down. I just had to keep feeding her little and often.”
Keep in mind, however, that not all mothers are able to express a lot of milk right away. You can also try hand expressing milk and see if there is a change in breast fullness.
If you're worried about your milk supply, read our tips for symptoms of too little or too much milk.
Literature
1 Pang WW, Hartmann PE. Initiation of human lactation: secretory differentiation and secretory activation. J9 Mammary Gland Biol Neoplasia . 2007;12(4):211-221. - Pang, W.W., Hartmann, P.I., "Lactation initiation in the lactating mother: secretory differentiation and secretory activation. " G Mammary Gland Biol Neoplasia. 2007;12(4):211-221.
" G Mammary Gland Biol Neoplasia. 2007;12(4):211-221.
2 Kent JC et al. Principles for maintaining or increasing breast milk production. J Obstet Gynecol Neonatal Nurs . 2012;41(1):114-121. - Kent J.S. et al., "Principles for Maintaining and Increasing Milk Production". G Obstet Ginecol Neoneutal Nurs. 2012;41(1):114-121.
3 Ostrom KM. A review of the hormone prolactin during lactation. Prog Food Nutr Sci . 1990;14(1):1-43. - Ostrom KM, "Review of the role of the hormone prolactin during lactation." Prog Food Nutr Sai. 1990;14(1):1-43.
4 Cox DB et al. Blood and milk prolactin and the rate of milk synthesis in women. Exp Physiol. 1996;81(6):1007-1020. - Cox D.B. et al., Effects of blood and milk prolactin on milk production in women.