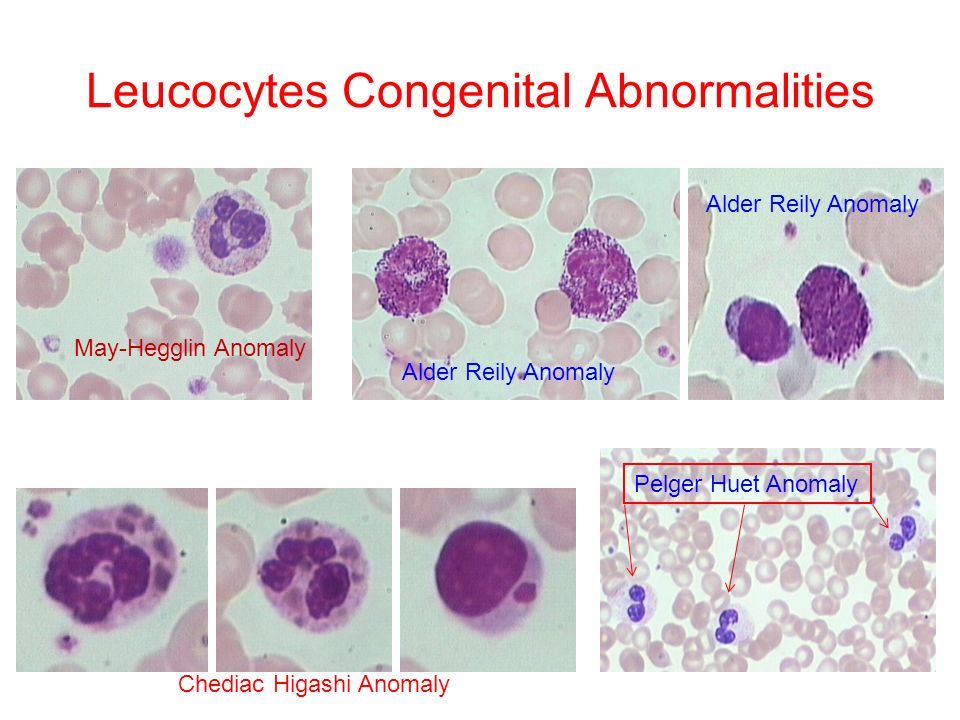
Congenital abnormalities list
1.4 Congenital Anomalies - Definitions
- Chapter 1: Surveillance of Congenital Anomalies
- 1.1 Introduction
- 1.2 The Purpose of Congenital Anomalies Surveillance
- 1.3 Types of Surveillance Programmes
- 1.4 Congenital Anomalies - Definitions
Congenital anomalies comprise a wide range of abnormalities of body structure or function that are present at birth and are of prenatal origin. For efficiency and practicality, the focus is commonly on major structural anomalies. These are defined as structural changes that have significant medical, social or cosmetic consequences for the affected individual, and typically require medical intervention. Examples include cleft lip and spina bifida.
Major structural anomalies are the conditions that account for most of the deaths, morbidity and disability related to congenital anomalies (see Box 1.1 for a list of selected external and internal major congenital anomalies). In contrast, minor congenital anomalies, although more prevalent among the population, are structural changes that pose no significant health problem in the neonatal period and tend to have limited social or cosmetic consequences for the affected individual. Examples include single palmar crease and clinodactyly.
| External | Internal |
|
|
| Chromosomal | |
| Trisomy 21 (Down syndrome) | |
Major anomalies are sometimes associated with minor anomalies, which might be objective (e. g. preauricular tags) or more subjective (e.g. low-set ears). Box 1.2 represents selected external minor congenital anomalies frequently captured by different surveillance systems, but only when associated with any of the major anomalies under surveillance. For a more detailed listing of minor anomalies, please refer to Appendix B. Often, surveillance systems will collect information on specific syndromes that are multiple anomalies pathogenetically related due to a single cause – for example, genetic or environmental causes that are known to cause birth defects. Certain syndromes caused by infectious diseases are of special interest in many low- and middle-income countries . For a detailed listing of selected syndromes of infectious origin that are of public health significance, please refer to Appendix B.
g. preauricular tags) or more subjective (e.g. low-set ears). Box 1.2 represents selected external minor congenital anomalies frequently captured by different surveillance systems, but only when associated with any of the major anomalies under surveillance. For a more detailed listing of minor anomalies, please refer to Appendix B. Often, surveillance systems will collect information on specific syndromes that are multiple anomalies pathogenetically related due to a single cause – for example, genetic or environmental causes that are known to cause birth defects. Certain syndromes caused by infectious diseases are of special interest in many low- and middle-income countries . For a detailed listing of selected syndromes of infectious origin that are of public health significance, please refer to Appendix B.
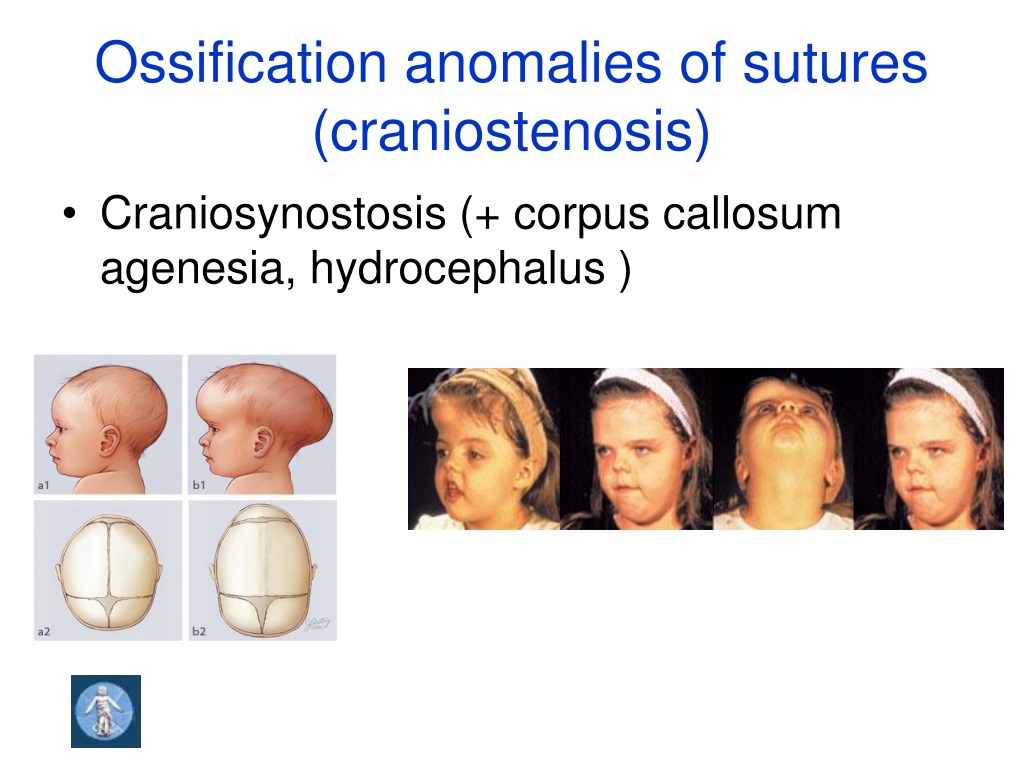
When establishing a new congenital anomalies surveillance programme, the initial anomalies that are included can be limited to structural anomalies that are readily identifiable and easily recognized on physical examination at birth or shortly after birth. The list may vary, depending on the capacity and resources of the health-care system and surveillance programme, but typically includes major external congenital anomalies. Examples include:
The list may vary, depending on the capacity and resources of the health-care system and surveillance programme, but typically includes major external congenital anomalies. Examples include:
- orofacial clefts,
- neural tube defects, and
- limb deficiencies.
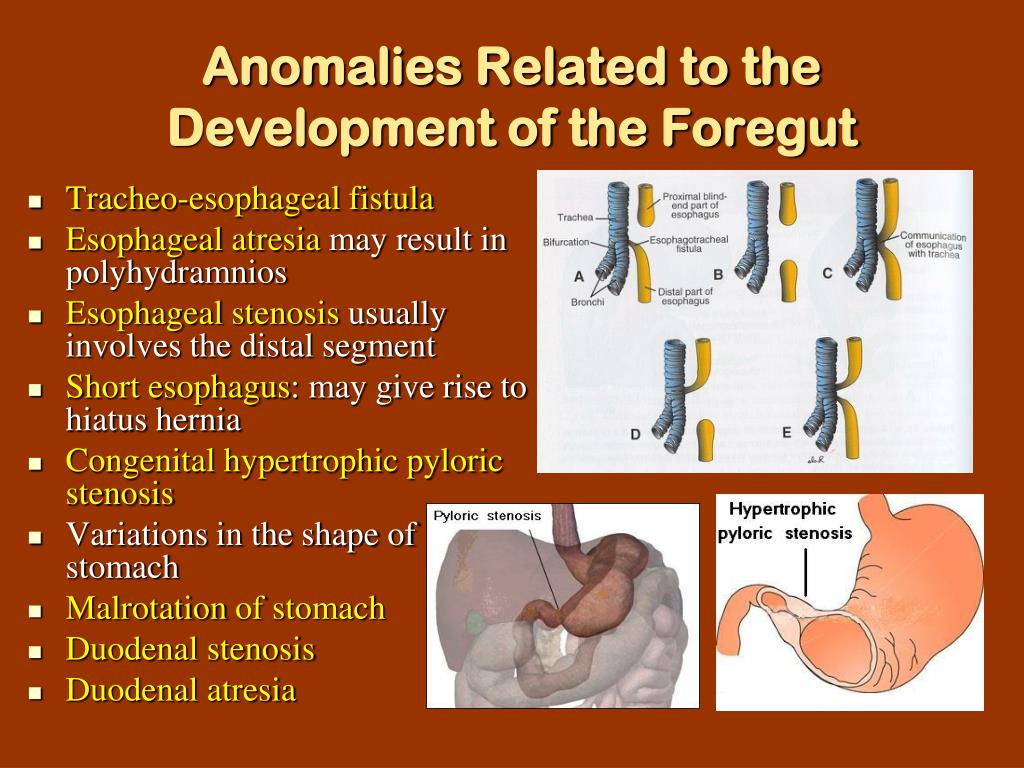
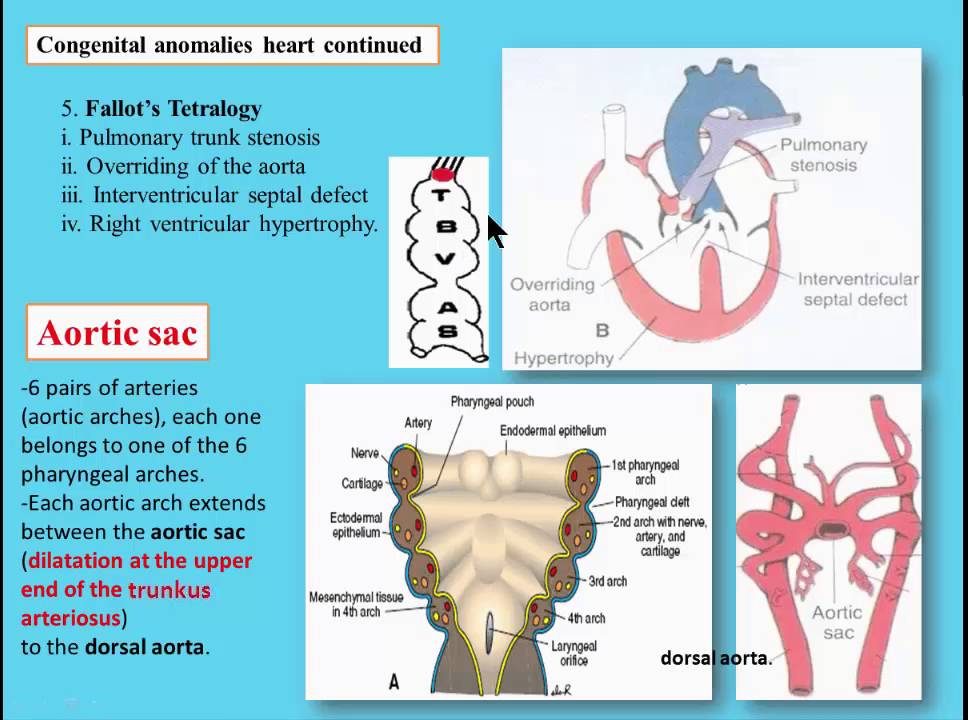
In contrast, detecting the vast majority of internal structural anomalies (e.g. congenital heart defects, intestinal malrotation and unilateral kidney agenesis) requires imaging techniques or other specialized procedures that may not be available consistently. In some cases, internal anomalies have external manifestations that allow the observer to suspect a particular diagnosis, as is the case with the urethral obstruction sequence. Similar to collecting information on internal defects, collecting information on syndromes often requires gathering data from multiple sources such as laboratory, imaging or genetic testing. Therefore, collecting surveillance data on internal defects and syndromes is typically not recommended when first starting a surveillance programme.
Classification by developmental mechanism or clinical presentation can be important in surveillance, because the same congenital anomaly can have different etiologies. Futhermore, the distinction may be important both clinically and in etiological studies. Please refer to Appendix C for more information about the causes of congenital anomalies and their classification according to developmental mechanism and clinical presentation.
| Box 1.2. Selected external minor congenital anomalies | |
|---|---|
| Absent nails Accessory tragus Anterior anus (ectopic anus) Auricular tag or pit Bifid uvula or cleft uvula Branchial tag or pit Camptodactyly Cup ear Cutis aplasia (if large, this is a major anomaly) Ear lobe crease Ear lobe notch Ear pit or tag Extra nipples (supernumerary nipples) Facial asymmetry Hydrocele Hypoplastic fingernails Hypoplastic toenails Iris coloboma | Lop ear Micrognathia Natal teeth Overlapping digits Plagiocephaly Polydactyly type B tag, involves hand and foot Preauricular appendage, tag or lobule Redundant neck folds Rocker-bottom feet Single crease, fifth finger Single transverse palmar crease Single umbilical artery Small penis (unless documented as micropenis) Syndactyly involving second and third toes Tongue-tie (ankyloglossia) Umbilical hernia Undescended testicle Webbed neck (pterygium colli) |
2. Planning Activities and Tools
Planning Activities and Tools
Congenital anomalies
Congenital anomalies- All topics »
- A
- B
- C
- D
- E
- F
- G
- H
- I
- J
- K
- L
- M
- N
- O
- P
- Q
- R
- S
- T
- U
- V
- W
- X
- Y
- Z
- Resources »
- Fact sheets
- Facts in pictures
- Multimedia
- Publications
- Questions & answers
- Tools and toolkits
- Popular »
- Air pollution
- Coronavirus disease (COVID-19)
- Hepatitis
- Monkeypox
- All countries »
- A
- B
- C
- D
- E
- F
- G
- H
- I
- J
- K
- L
- M
- N
- O
- P
- Q
- R
- S
- T
- U
- V
- W
- X
- Y
- Z
- Regions »
- Africa
- Americas
- South-East Asia
- Europe
- Eastern Mediterranean
- Western Pacific
- WHO in countries »
- Statistics
- Cooperation strategies
- Ukraine emergency
- All news »
- News releases
- Statements
- Campaigns
- Commentaries
- Events
- Feature stories
- Speeches
- Spotlights
- Newsletters
- Photo library
- Media distribution list
- Headlines »
- Focus on »
- Afghanistan crisis
- COVID-19 pandemic
- Northern Ethiopia crisis
- Syria crisis
- Ukraine emergency
- Monkeypox outbreak
- Greater Horn of Africa crisis
- Latest »
- Disease Outbreak News
- Travel advice
- Situation reports
- Weekly Epidemiological Record
- WHO in emergencies »
- Surveillance
- Research
- Funding
- Partners
- Operations
- Independent Oversight and Advisory Committee
- WHO's Health Emergency Appeal 2023
- Data at WHO »
- Global Health Estimates
- Health SDGs
- Mortality Database
- Data collections
- Dashboards »
- COVID-19 Dashboard
- Triple Billion Dashboard
- Health Inequality Monitor
- Highlights »
- Global Health Observatory
- SCORE
- Insights and visualizations
- Data collection tools
- Reports »
- World Health Statistics 2022
- COVID excess deaths
- DDI IN FOCUS: 2022
- About WHO »
- People
- Teams
- Structure
- Partnerships and collaboration
- Collaborating centres
- Networks, committees and advisory groups
- Transformation
- Our Work »
- General Programme of Work
- WHO Academy
- Activities
- Initiatives
- Funding »
- Investment case
- WHO Foundation
- Accountability »
- Audit
- Programme Budget
- Financial statements
- Programme Budget Portal
- Results Report
- Governance »
- World Health Assembly
- Executive Board
- Election of Director-General
- Governing Bodies website
- Member States Portal
- Home/
- Health topics/
- Congenital anomalies
UNICEF/Noorani
Newborn baby in Timor-Leste
© Credits
Fact sheets
Questions and answers
Guidelines
Databases and tools
Resolutions and decisions
Technical work
- Newborn Health Unit
- Maternal, Newborn, Child and Adolescent Health and Ageing
- Nutrition and Food Safety
- Sensory Functions, Disability and Rehabilitation
- Sexual and Reproductive Health
Our work
News
All →Publications
All →A wide range of causes of congenital anomalies means that a portfolio of prevention approaches is needed including prevention of sexually transmitted infections,. ..
..
Congenital anomalies, also known as birth defects, are structural or functional abnormalities, including metabolic disorders, that are present from birth....
Survive and thrive: transforming care for every small and sick newborn maps out a pathway towards 2030. It is built upon epidemiology, historical trends,...
Feature stories
Related health topics
Congenital genetic anomalies
Home / Congenital genetic anomalies
Genetic are diseases that occur due to defects in genes, chromosomal abnormalities. Every healthy person has 6-8 damaged genes, but they do not disrupt cell functions and do not lead to disease, because they are recessive (non-manifested). If a person inherits two similar abnormal genes from his mother and father, he becomes ill. The probability of such a coincidence is extremely small, but it increases dramatically if the parents are relatives (that is, they have a similar genotype).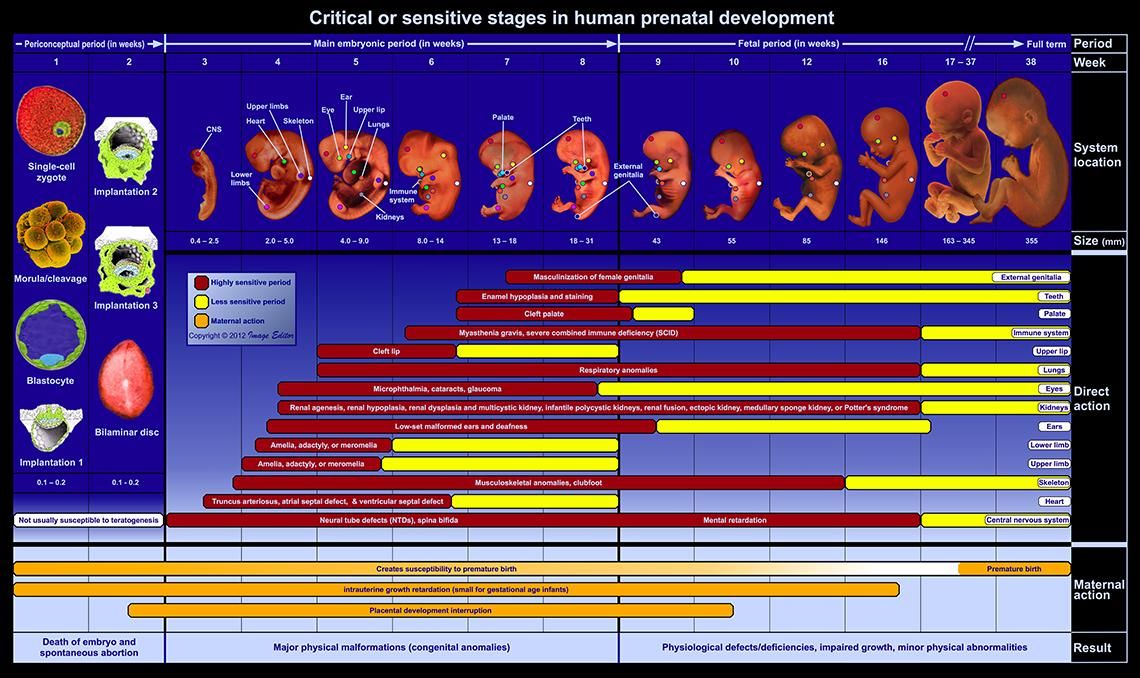 For this reason, the frequency of genetic abnormalities is high in closed populations.
For this reason, the frequency of genetic abnormalities is high in closed populations.
Each gene in the human body is responsible for the production of a specific protein. Due to the manifestation of a damaged gene, the synthesis of an abnormal protein begins, which leads to cell dysfunction and developmental defects.
A doctor can establish the risk of a possible genetic anomaly by asking you about the diseases of relatives “up to the third knee”, both on your part and on the part of your husband.
Currently, the problem of congenital malformations is relevant in many branches of medicine. According to long-term observation, more than 5.5% of children with congenital malformations are born in the world, mortality among newborns from congenital malformations is about 30% (up to 270 thousand children die annually under the age of 28 days of life). In the structure of perinatal mortality, congenital malformations in full-term children occupy the first place. About 10% of conceptions in the human population are accompanied by congenital anomalies in the development of the fetus. Approximately 0.5% of cases are chromosomal diseases, 0.7% are molecular pathologies, 1.8% are hereditary polygenic diseases, and about 7% are hereditary predispositions.
Approximately 0.5% of cases are chromosomal diseases, 0.7% are molecular pathologies, 1.8% are hereditary polygenic diseases, and about 7% are hereditary predispositions.
The viability of children with combined congenital malformations is increasingly considered as the main criterion in assessing the state of health. Despite the progress made in improving the quality of modern surgical care and intensive care for young children, the results of treatment, unfortunately, are not always encouraging.
When analyzing a diagnostic study of a detected birth defect in a newborn, a neonatologist must highlight the type of this pathology, its causes, belonging to a particular syndrome, and how often this defect is accompanied by other congenital diseases.
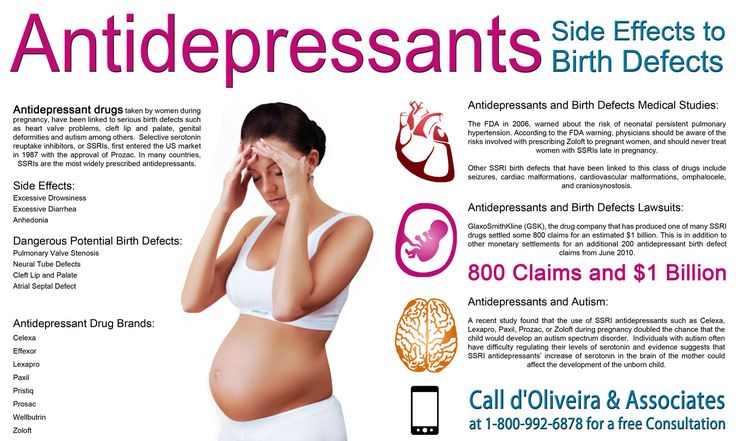
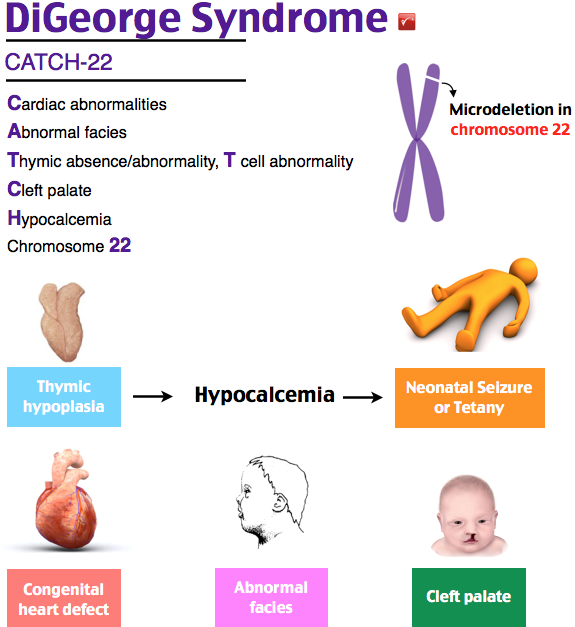
Congenital anomalies in the development of a child can be hereditary (due to gene mutations and chromosomal pathologies), teratogenic (acquired during pregnancy) and multifactorial (a combination of the first two factors). Of the various hereditary defects, a fairly common chromosomal disease should be distinguished - Down syndrome , in which the characteristic appearance of the child indicates his physical and mental retardation. Endocrine and hormonal pathologies of a pregnant woman, injuries during childbearing, oligohydramnios, viral diseases (rubella, influenza), intoxication of the body with chemicals, the intake of antidepressants, antibiotics, anticonvulsants by the expectant mother lead to deviations in the intrauterine development of the fetus. And sometimes the true causes of congenital anomalies are not possible for embryologists, geneticists and neonatologists to establish at all.
Of the various hereditary defects, a fairly common chromosomal disease should be distinguished - Down syndrome , in which the characteristic appearance of the child indicates his physical and mental retardation. Endocrine and hormonal pathologies of a pregnant woman, injuries during childbearing, oligohydramnios, viral diseases (rubella, influenza), intoxication of the body with chemicals, the intake of antidepressants, antibiotics, anticonvulsants by the expectant mother lead to deviations in the intrauterine development of the fetus. And sometimes the true causes of congenital anomalies are not possible for embryologists, geneticists and neonatologists to establish at all.
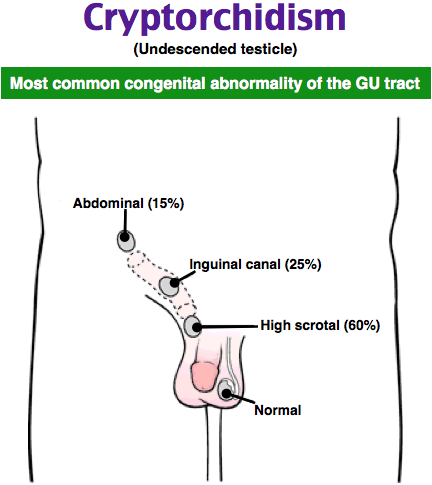
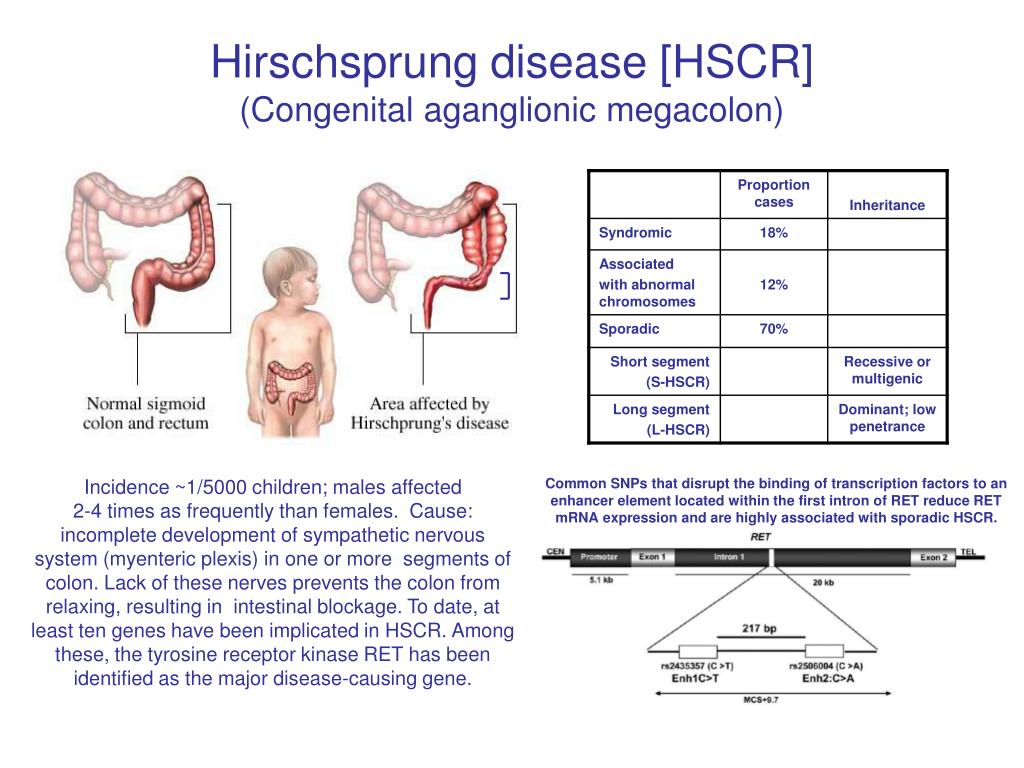
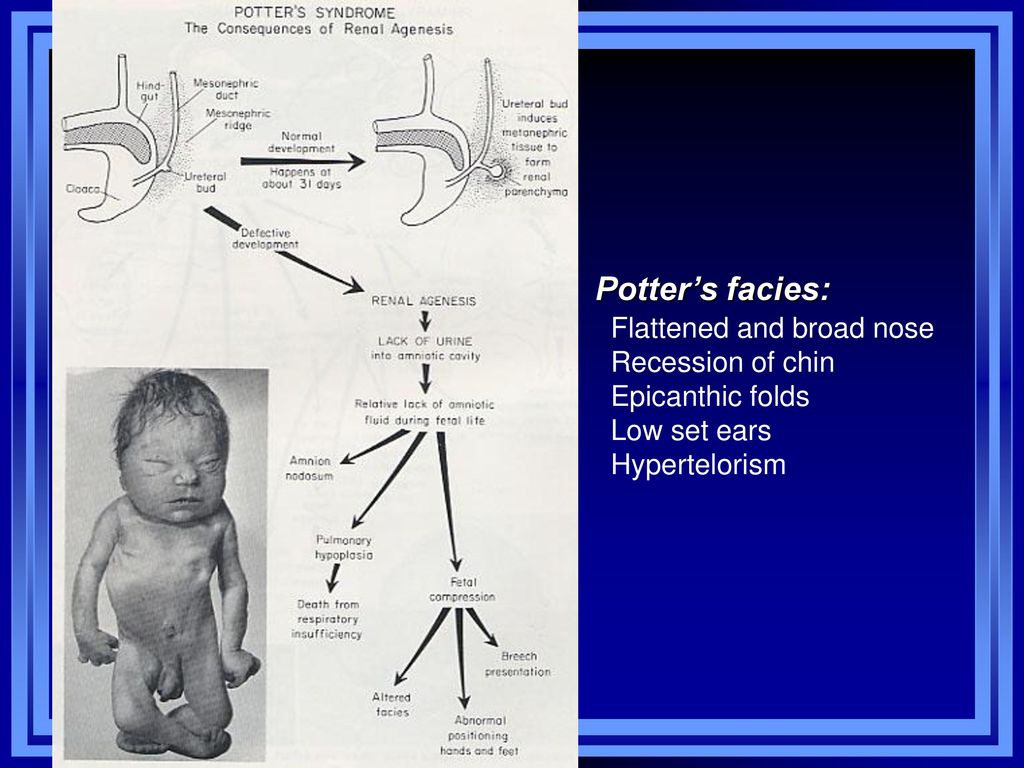
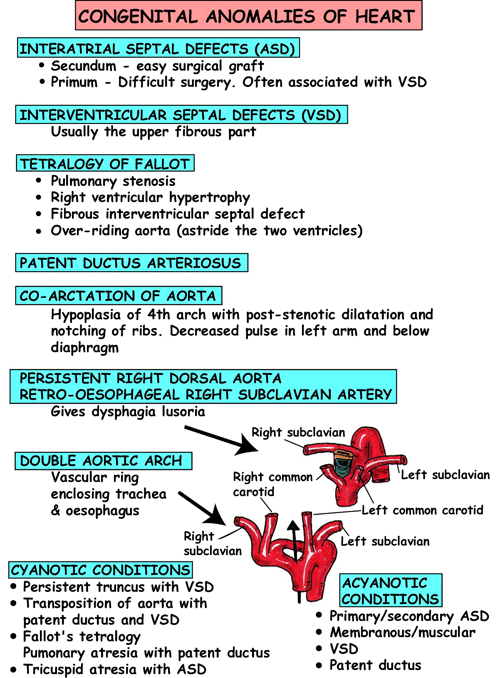
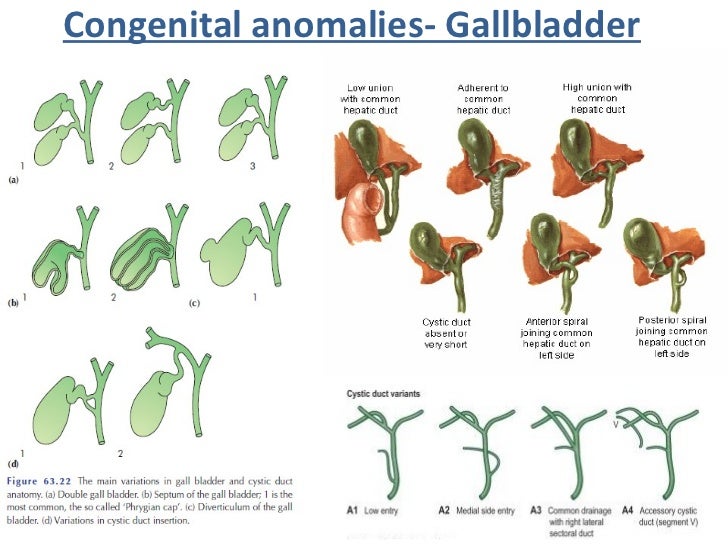
There are a great many pathological deviations in the development of children, since absolutely any organ of a child can undergo an abnormal anatomical structure or a degenerative-dystrophic condition. A common anomaly is congenital heart disease, accompanied by defects in the interventricular and interatrial septum, stenosis (narrowing) of the aortic valve, which lead to a change in intracardiac hemodynamics. Renal congenital pathologies are also common: fusion, absence of one kidney ( agenesis ), or the appearance of a third. There are known cases of abnormal elongation and thickening of the large intestine ( Hirschsprung's disease ), the occurrence of diaphragmatic hernia, the absence of testicles in the scrotum ( cryptorchidism ).
Renal congenital pathologies are also common: fusion, absence of one kidney ( agenesis ), or the appearance of a third. There are known cases of abnormal elongation and thickening of the large intestine ( Hirschsprung's disease ), the occurrence of diaphragmatic hernia, the absence of testicles in the scrotum ( cryptorchidism ).
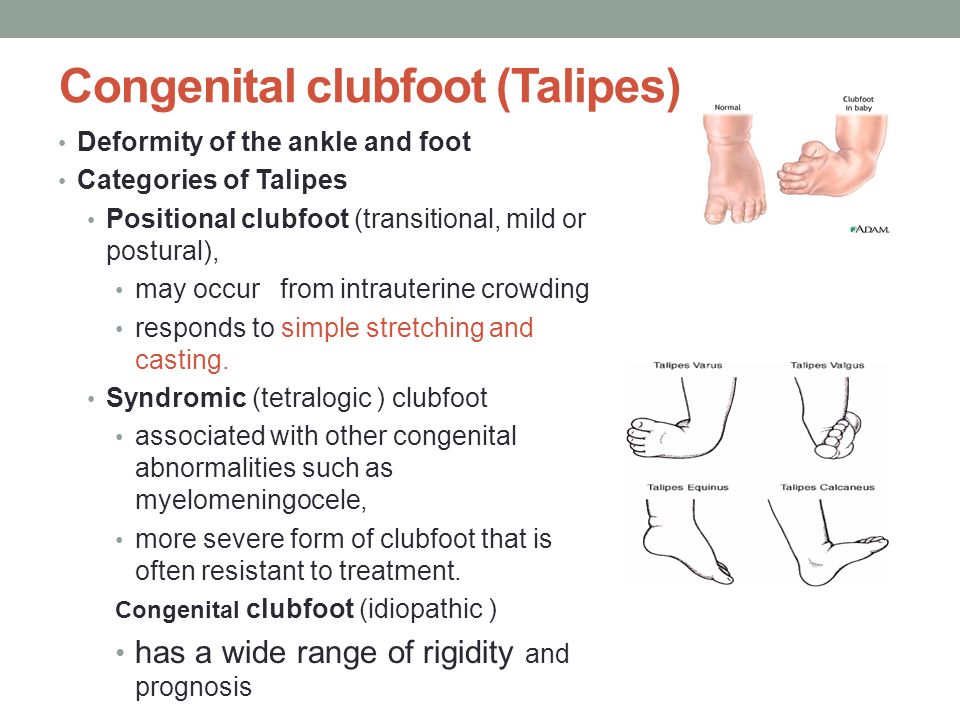
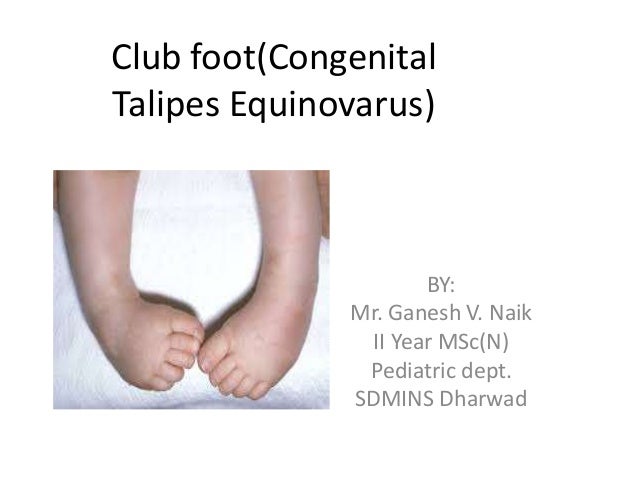
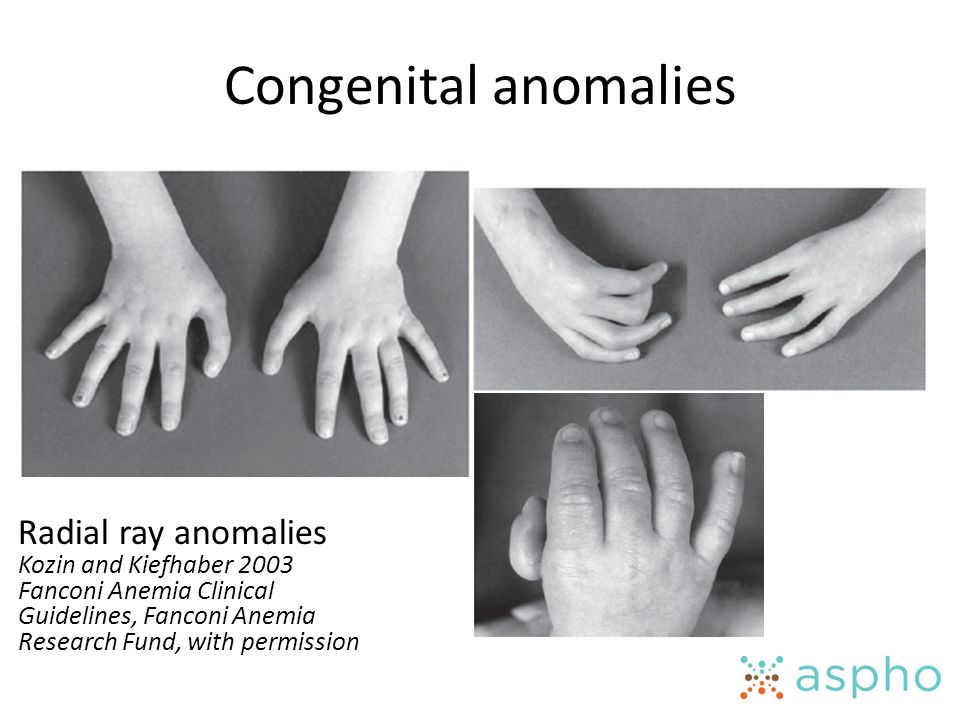
Of course, the external manifestations of childhood malformations look very unsightly. A child can be born with deformed or abnormally short upper and lower limbs ( clubfoot, lameness ), congenital dislocation of the hip, cleft lip, cleft palate, protruding chest, pathological bends of the spine. Often, melanin pigment is completely absent in the skin ( albinism ), so the child is contraindicated in sun exposure. Sometimes there is an increased number ( polydactyly ) of fingers and toes or their fusion ( syndactyly ), absence of an anal opening ( atresia ), reduction in the size of the skull ( microcephaly ), drooping of the upper eyelid ( itosis ) .
It should be noted that the numerous list of congenital malformations includes such diseases as a violation of the blood clotting factor ( hemophilia ), color blindness ( color blindness ), spina bifida ( spina bifida ). Many of these pathologies are treatable, some of them lead to lifelong disability, but, unfortunately, there are defects in which the child is not viable. These include complete absence of lungs or kidneys, skin ( acrania ), or cerebral hemispheres (anencephaly ).
Congenital malformations in children can develop immediately after fertilization, occur in the first weeks of pregnancy, or at later stages of bearing a child. In this regard, pregnancy planning and prenatal diagnosis (medical genetic counseling), which involves a comprehensive examination of the health status of both spouses, are of great importance. This is especially true of persons in whose families people with abnormal deviations were previously born. Of course, today medicine has reached unprecedented heights, but it is better not to tempt fate and take care of the health of the unborn child long before pregnancy.
Of course, today medicine has reached unprecedented heights, but it is better not to tempt fate and take care of the health of the unborn child long before pregnancy.
Each gene in the human body is responsible for the production of a specific protein. Due to the manifestation of a damaged gene, the synthesis of an abnormal protein begins, which leads to cell dysfunction and developmental defects.
The doctor can determine the risk of a possible genetic anomaly by asking you about the diseases of relatives “up to the third generation”, both on your side and on the side of your husband.
Turner syndrome is a disorder affecting girls characterized by the partial or total absence of one or two X chromosomes. The disease occurs in one in 3,000 girls. Girls with this disease are usually very small and their ovaries do not function.
Trisomy X syndrome is a condition in which a girl is born with three X chromosomes. This disease occurs in an average of one in 1000 girls. The X-trisomy syndrome is characterized by a slight mental retardation and, in some cases, infertility.
This disease occurs in an average of one in 1000 girls. The X-trisomy syndrome is characterized by a slight mental retardation and, in some cases, infertility.
Klinefelter syndrome is a disorder in which a boy has one extra chromosome. The disease occurs in one boy out of 700. Patients with Klinefelter's syndrome, as a rule, are tall, there are no noticeable external developmental anomalies (after puberty, facial hair growth is difficult and the mammary glands are somewhat enlarged). Intellect in patients is usually normal, but speech disorders are common. Men with Klinefelter syndrome are usually infertile.
Cystic fibrosis is a genetic disease in which the functions of many glands are impaired. Cystic fibrosis only affects Caucasians. Approximately one in 20 white people has one damaged gene that, if manifested, can cause cystic fibrosis. The disease occurs when a person receives two of these genes (from the father and from the mother). In Russia, cystic fibrosis, according to various sources, occurs in one newborn out of 3500-5400, in the USA - in one out of 2500. With this disease, the gene responsible for the production of a protein that regulates the movement of sodium and chlorine through cell membranes is damaged. There is dehydration and an increase in the viscosity of the secretion of the glands. As a result, a thick secret blocks their activity. In patients with cystic fibrosis, protein and fat are poorly absorbed, as a result, growth and weight gain are greatly slowed down. Modern methods of treatment (taking enzymes, vitamins and a special diet) allow half of the patients with cystic fibrosis to live more than 28 years.
In Russia, cystic fibrosis, according to various sources, occurs in one newborn out of 3500-5400, in the USA - in one out of 2500. With this disease, the gene responsible for the production of a protein that regulates the movement of sodium and chlorine through cell membranes is damaged. There is dehydration and an increase in the viscosity of the secretion of the glands. As a result, a thick secret blocks their activity. In patients with cystic fibrosis, protein and fat are poorly absorbed, as a result, growth and weight gain are greatly slowed down. Modern methods of treatment (taking enzymes, vitamins and a special diet) allow half of the patients with cystic fibrosis to live more than 28 years.
Hemophilia is a genetic disease characterized by increased bleeding due to a deficiency of one of the blood coagulation factors. The disease is inherited through the female line, while it affects the vast majority of boys (an average of one in 8500). Hemophilia occurs when the genes responsible for the activity of blood clotting factors are damaged. With hemophilia, frequent hemorrhages in the joints and muscles are observed, which can ultimately lead to their significant deformation (that is, to a person's disability). People with hemophilia should avoid situations that could lead to bleeding. Patients with hemophilia should not take drugs that reduce blood clotting (for example, aspirin, heparin, and some painkillers). To prevent or stop bleeding, the patient is given a plasma concentrate containing a large amount of the missing clotting factor.
With hemophilia, frequent hemorrhages in the joints and muscles are observed, which can ultimately lead to their significant deformation (that is, to a person's disability). People with hemophilia should avoid situations that could lead to bleeding. Patients with hemophilia should not take drugs that reduce blood clotting (for example, aspirin, heparin, and some painkillers). To prevent or stop bleeding, the patient is given a plasma concentrate containing a large amount of the missing clotting factor.
Tay Sachs disease is a genetic disease characterized by the accumulation of phytanic acid (a product of the breakdown of fats) in tissues. The disease occurs mainly among Ashkenazi Jews and Canadians of French origin (in one newborn in 3600). Children with Tay-Sachs disease are retarded from an early age, then they become paralyzed and blind. As a rule, patients live up to 3-4 years. There are no treatments for this disease.
It is believed that the probability of having a baby with a congenital or hereditary pathology, the so-called population or general statistical risk, is approximately 3-5% for each pregnant woman. \n \n \n \nCongenital malformations are also referred to as congenital malformations, congenital disorders, or congenital deformities. Congenital malformations can be defined as structural or functional abnormalities (eg, metabolic disorders) that appear in utero and may be identified before birth, during birth, or later in life. \n \n \nApproximately 50% of all malformations cannot be attributed to any specific cause, but some causes or risk factors are known. \n \n \nAlthough low income may be an indirect determinant, malformations are more likely to occur in families and countries with insufficient resources. It is estimated that approximately 94% of severe malformations occur in middle- and low-income countries, where women often do not have access to sufficient and good enough food and may be exposed to some agent or factor, such as infection or alcohol, that provokes or enhances deviations from the norm in prenatal development. \n \n \nIncest (consanguinity) increases the incidence of rare genetic birth defects and almost doubles the risk of neonatal and infant mortality, mental retardation and severe birth defects in children born to first cousins . Some ethnic groups, such as Ashkenazi Jews and Finns, have a relatively high prevalence of rare genetic mutations that lead to an increased risk of malformations.\n \n \n \nMaternal infections such as syphilis or measles are a common cause of birth defects in low- and middle-income countries. \n \n \nDeficiencies in iodine, folate, obesity, or conditions such as diabetes mellitus are associated with some malformations. \n \n \nMaternal exposure to certain pesticides and other chemicals, as well as certain drugs, alcohol, tobacco, psychoactive substances, or radiation during pregnancy may increase the risk of developing the fetus or a newborn baby with birth defects. Working or living near or close to landfills, smelters or mines can also be a risk factor, especially if the mother is exposed to other environmental risk factors or malnutrition. \n \n \nPregnancy and conception preventive health care, and prenatal care, reduce the incidence of some birth defects. Primary prevention of malformations includes the following measures: \n \n \n \nPre-conception (pre-conception) and near conception (peri-conception) health care includes basic reproductive health care as well as medical genetic screening and counseling. Screening can be carried out during the three periods listed below. \n \n \n \nIn countries with adequate health services, structural congenital malformations can be corrected with pediatric surgery and provide timely treatment for children with functional problems such as thalassemia (inherited by recessive blood disease), sickle cell disorders, and congenital hypothyroidism. \n \n \nIn 2010, the World Health Assembly published a report on birth defects. The report outlines the main components of establishing national programs for the prevention and care of birth defects before and after birth. The report also recommends priority actions for the international community to help establish and strengthen such national programs. \n \nThe Global Strategy for Women's and Children's Health, announced in September 2010 by the United Nations in collaboration with government leaders and other organizations such as WHO and UNICEF, plays a critical role in implementing efficient and cost-effective action to promote newborn and child health.\n \n \nWHO is also working with the National Center for Birth and Developmental Disorders, part of the US Centers for Disease Control and Prevention (CDC), and other partners to develop a global policy to fortify foods with salt folic acid at the country level. In addition, WHO is working with partners to provide the necessary technical expertise to conduct surveillance of neural tube defects, monitor efforts to fortify foods with folic acid salts, and strengthen laboratory capacity to assess risks for birth defects prevented by folic acid salts. \n \nThe International Clearing House for Surveillance and Research on Birth Defects is a voluntary, non-profit, international organization in official relations with WHO. \n \nThe WHO Departments of Reproductive Health and Research and Nutrition for Health and Development, in collaboration with the International Clearing House for Surveillance and Research on Birth Defects and the CDC National Center for Birth Defects and Development, organize annual seminars on surveillance and prevention of birth defects and preterm birth. The WHO Department of HIV/AIDS is collaborating with these partners to strengthen surveillance for malformations among women receiving antiretroviral drugs during pregnancy as an integral part of the monitoring and evaluation of national HIV programs. \n \nThe GAVI Alliance, partnered with WHO, is helping developing countries to increase the control and elimination of rubella and congenital rubella syndrome through immunization. \n \nWHO is developing normative tools, including guidelines and a global plan of action to strengthen health care and rehabilitation services in support of the implementation of the Convention on the Rights of Persons with Disabilities. Similarly, WHO is helping countries integrate health care and rehabilitation services into general primary health care, supporting the development of community-based rehabilitation programs and strengthening specialized rehabilitation centers and their links with community-based rehabilitation centers. \n \n \nThe WHO Department of Public Health and Environment works across a range of activities and develops interventions to address the environmental and social determinants of child development. These include: child-only vulnerability to indoor and outdoor air pollution, water pollution, lack of basic hygiene, toxic compounds, heavy metals, waste components and radiation exposure; mixed impact of factors related to the social environment, professional activities and nutrition, as well as the living conditions of children (home, school). \n ","datePublished":"2022-02-28T22:52:00.0000000+00:00","image":"https://cdn.who.int/media/images/default -source/imported/preterm-birth-mother-jpg.jpg?sfvrsn=c5c1adf1_0","publisher":{"@type":"Organization","name":"World Health Organization: WHO","logo": {"@type":"ImageObject","url":"https://www.who.int/Images/SchemaOrg/schemaOrgLogo.jpg","width":250,"height":60}},"dateModified ":"2022-02-28T22:52:00.0000000+00:00","mainEntityOfPage":"https://www.who.int/ru/news-room/fact-sheets/detail/congenital-anomalies", "@context":"http://schema.org","@type":"Article"}; Malformations and preterm birth are major causes of childhood death, chronic disease and disability in many countries. In 2010, the World Health Assembly adopted a resolution calling on all Member States to promote primary prevention and health promotion for children with developmental disabilities through: Congenital malformations are also referred to as congenital malformations, congenital disorders or congenital deformities. Congenital malformations can be defined as structural or functional abnormalities (eg, metabolic disorders) that appear in utero and may be identified before birth, during birth, or later in life. Approximately 50% of all malformations cannot be attributed to any specific cause, but some causes or risk factors are known. While low income may be an indirect determinant, malformations are more likely to occur in under-resourced families and countries. It is estimated that approximately 94% of severe malformations occur in middle- and low-income countries, where women often do not have access to sufficient and good enough food and may be exposed to some agent or factor, such as infection or alcohol, that provokes or enhances deviations from the norm in prenatal development. Incest (consanguinity) increases the prevalence of rare genetic birth defects and almost doubles the risk of neonatal and infant mortality, mental retardation and severe birth defects in children born to first cousins. Some ethnic groups, such as Ashkenazi Jews and Finns, have a relatively high prevalence of rare genetic mutations that lead to an increased risk of malformations. Maternal infections such as syphilis or measles are a common cause of birth defects in low- and middle-income countries. Deficiency of iodine, folic acid salts, obesity, or conditions such as diabetes mellitus are associated with some malformations. For example, folic acid deficiency increases the risk of having a baby with a neural tube defect. Maternal exposure to certain pesticides and other chemicals, as well as certain drugs, alcohol, tobacco, psychoactive substances, or radiation during pregnancy may increase the risk of birth defects in the fetus or newborn. Working or living near or close to landfills, smelters or mines can also be a risk factor, especially if the mother is exposed to other environmental risk factors or malnutrition. Preventive health care during pregnancy and conception, as well as antenatal care, reduce the incidence of some birth defects. Primary prevention of malformations includes the following measures: Medical care before conception (in the preconception period) and around the time of conception (in the periconceptional period) includes basic reproductive health care, as well as medical genetic screening and counseling. Screening can be carried out during the three periods listed below. In countries with adequate health services, structural birth defects can be corrected with pediatric surgery and timely treatment can be provided for children with functional problems such as thalassemia (a recessive blood disorder), sickle cell disorders, and congenital hypothyroidism. In 2010, the World Health Assembly published a report on birth defects. The report outlines the main components of establishing national programs for the prevention and care of birth defects before and after birth. The report also recommends priority actions for the international community to help establish and strengthen such national programs. The Global Strategy for Women's and Children's Health, launched in September 2010 by the United Nations in collaboration with government leaders and other organizations such as WHO and UNICEF, plays a critical role in achieving effective and cost-effective action to improve newborn health and children. WHO is also working with the National Center for Birth and Developmental Disorders, part of the US Centers for Disease Control and Prevention (CDC), and other partners to develop a global policy for folic acid fortification at the country level. In addition, WHO is working with partners to provide the necessary technical expertise to conduct surveillance of neural tube defects, monitor efforts to fortify foods with folic acid salts, and strengthen laboratory capacity to assess risks for birth defects prevented by folic acid salts. The International Clearing House for Surveillance and Research on Birth Defects is a voluntary, non-profit international organization in official relations with WHO. This organization collects surveillance data on birth defects and research programs around the world to study and prevent birth defects and mitigate their effects. The WHO Departments of Reproductive Health and Research and Nutrition for Health and Development, in collaboration with the International Clearing House for Surveillance and Research on Birth Defects and the CDC National Center for Birth Defects and Development, organize annual workshops on surveillance and prevention of birth defects and premature birth. The WHO Department of HIV/AIDS is collaborating with these partners to strengthen surveillance for malformations among women receiving antiretroviral drugs during pregnancy as an integral part of the monitoring and evaluation of national HIV programs. The GAVI Alliance, with WHO among its partners, is helping developing countries to accelerate the control and elimination of rubella and congenital rubella syndrome through immunization. WHO is developing normative tools, including guidelines and a global action plan to strengthen health care and rehabilitation services in support of the implementation of the Convention on the Rights of Persons with Disabilities. Similarly, WHO is helping countries integrate health care and rehabilitation services into general primary health care, supporting the development of community-based rehabilitation programs and strengthening specialized rehabilitation centers and their links with community-based rehabilitation centers. The WHO Department of Public Health and Environment works across a range of activities and develops interventions to address the environmental and social determinants of child development. These include: child-only vulnerability to indoor and outdoor air pollution, water pollution, lack of basic hygiene, toxic compounds, heavy metals, waste components and radiation exposure; mixed impact of factors related to the social environment, professional activities and nutrition, as well as the living conditions of children (home, school). In rare cases, the probability of the birth of a child with a genetic disease can be predicted and the pathology can be diagnosed already in the period of intrauterine development of the child. Certain congenital malformations and diseases are established using laboratory biochemical, cytogenetic and molecular genetic methods even in the fetus, since some diseases are detected during a complex of prenatal (prenatal) diagnostic methods.
In rare cases, the probability of the birth of a child with a genetic disease can be predicted and the pathology can be diagnosed already in the period of intrauterine development of the child. Certain congenital malformations and diseases are established using laboratory biochemical, cytogenetic and molecular genetic methods even in the fetus, since some diseases are detected during a complex of prenatal (prenatal) diagnostic methods.
\n
Definition
Causes and risk factors
Socio-economic factors
 Moreover, motherhood in adulthood increases the risk of chromosomal abnormalities, including Down's syndrome, while motherhood at a young age increases the risk of certain congenital malformations.
Moreover, motherhood in adulthood increases the risk of chromosomal abnormalities, including Down's syndrome, while motherhood at a young age increases the risk of certain congenital malformations. Genetic factors
Infections
Maternal nutrition
 For example, folic acid deficiency increases the risk of having a baby with a neural tube defect. In addition, increased intake of vitamin A may affect the normal development of the embryo or fetus.
For example, folic acid deficiency increases the risk of having a baby with a neural tube defect. In addition, increased intake of vitamin A may affect the normal development of the embryo or fetus. Environmental factors
Prevention
\n
 This disease can be prevented by vaccinating children. Rubella vaccine may also be given to women who are not immune to the disease at least one month before pregnancy.
This disease can be prevented by vaccinating children. Rubella vaccine may also be given to women who are not immune to the disease at least one month before pregnancy. Identification
\n
 In some countries, all newborns are screened for thyroid and adrenal abnormalities before being discharged from the maternity ward.
In some countries, all newborns are screened for thyroid and adrenal abnormalities before being discharged from the maternity ward. Treatment and care
WHO activities
 This organization collects surveillance data on birth defects and research programs around the world to study and prevent birth defects and mitigate their effects.
This organization collects surveillance data on birth defects and research programs around the world to study and prevent birth defects and mitigate their effects. 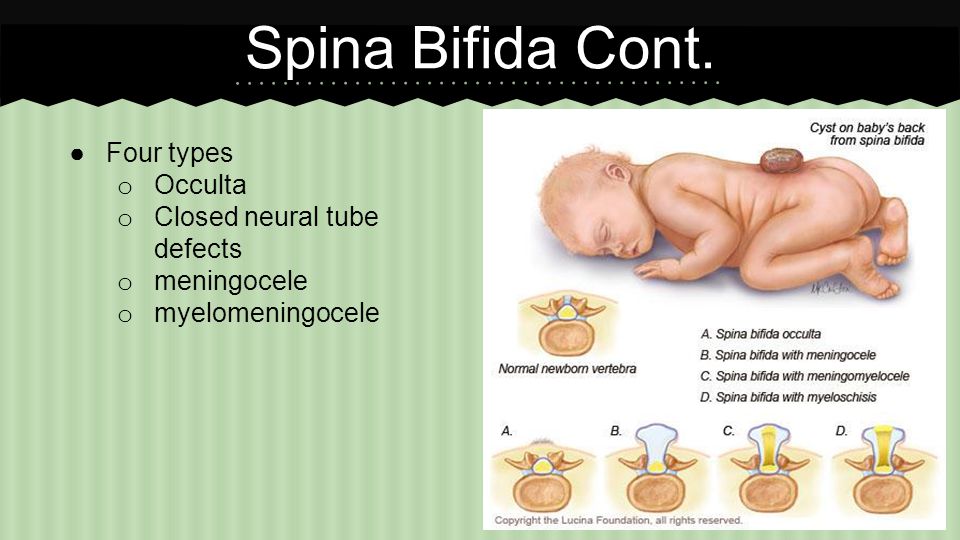
United Nations Convention on the Rights of Persons with Disabilities
Key Facts
Definition
Causes and risk factors
Socio-economic factors
 Moreover, motherhood in adulthood increases the risk of chromosomal abnormalities, including Down's syndrome, while motherhood at a young age increases the risk of certain congenital malformations.
Moreover, motherhood in adulthood increases the risk of chromosomal abnormalities, including Down's syndrome, while motherhood at a young age increases the risk of certain congenital malformations. Genetic factors
Infections
Maternal nutrition
 In addition, increased intake of vitamin A may affect the normal development of the embryo or fetus.
In addition, increased intake of vitamin A may affect the normal development of the embryo or fetus. Environmental factors
Prophylaxis
 This disease can be prevented by vaccinating children. Rubella vaccine may also be given to women who are not immune to the disease at least one month before pregnancy.
This disease can be prevented by vaccinating children. Rubella vaccine may also be given to women who are not immune to the disease at least one month before pregnancy. Identification
 During this period, screening of young and mature mothers, as well as screening for the use of alcohol, tobacco and other psychoactive substances, can be carried out. Ultrasound can be used to detect Down's syndrome during the first trimester of pregnancy and severe fetal malformations during the second trimester. Additional tests and amniocentesis help detect neural tube defects and chromosomal abnormalities during the first and second trimesters of pregnancy.
During this period, screening of young and mature mothers, as well as screening for the use of alcohol, tobacco and other psychoactive substances, can be carried out. Ultrasound can be used to detect Down's syndrome during the first trimester of pregnancy and severe fetal malformations during the second trimester. Additional tests and amniocentesis help detect neural tube defects and chromosomal abnormalities during the first and second trimesters of pregnancy. Treatment and medical care
WHO activities

UN Convention on the Rights of Persons with Disabilities