Cervix contractions during pregnancy
Contractions and signs of labor
Learning the signs of labor before your due date can help you feel ready for your baby’s birth.
Signs of labor include strong and regular contractions, pain in your belly and lower back, a bloody mucus discharge and your water breaking.
If you think you’re in labor, call your health care provider.
Not all contractions mean you're in true labor. Learning the difference between true and false labor can help you know when it’s the real thing.
What is labor?
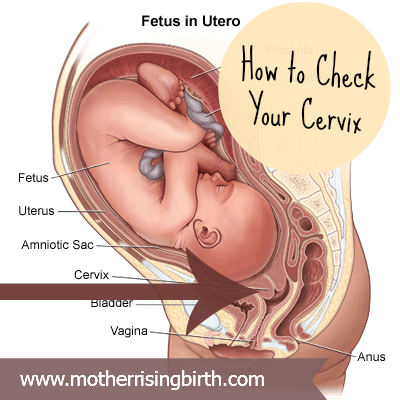
Labor (also called childbirth) is the process of your baby leaving the uterus (womb). You’re in labor when you have regular contractions that cause your cervix to change. Contractions are when the muscles of your uterus get tight and then relax. Contractions help push your baby out of your uterus. Your cervix is the opening to the uterus that sits at the top of the vagina. When labor starts, your cervix dilates (opens up).
As you get closer to your due date, learning the signs of labor can help you feel ready for labor and birth. If you have any signs of labor, call your health care provider.
What are the signs of labor?
You know you’re in true labor when:
- You have strong and regular contractions. A contraction is when the muscles of your uterus tighten up like a fist and then relax. Contractions help push your baby out. When you’re in true labor, your contractions last about 30 to 70 seconds and come about 5 to 10 minutes apart. They’re so strong that you can’t walk or talk during them. They get stronger and closer together over time.
- You feel pain in your belly and lower back. This pain doesn't go away when you move or change positions.
- You have an increase in vaginal discharge that can be clear, pink or slightly bloody (brownish or reddish). This is called bloody show. It can happen a few days before labor or at the beginning of labor.
 If you have bright red bleeding or if the bleeding is heavy, tell your provider right away.
If you have bright red bleeding or if the bleeding is heavy, tell your provider right away. - Your water breaks. Your baby has been growing in amniotic fluid (the bag of waters) in your uterus. When the bag of waters breaks, you may feel a big rush of water. Or you may feel just a trickle.
If you think you’re in labor, call your health care provider, no matter what time of day or night. Your provider can tell you if it’s time to head for the hospital. To see for sure that you’re in labor, your health care provider measures your cervix.
What are signs that you may be close to starting labor?
You may be close to starting labor if:
- Your baby drops or moves lower into your pelvis. This is called lightening. It means that your baby is getting ready to move into position for birth. It can happen a few weeks or even just a few hours before your labor begins.
- You have an increase in vaginal discharge that’s clear, pink or slightly bloody.
 This is called show or bloody show. It can happen a few days before labor starts or at the beginning of labor.
This is called show or bloody show. It can happen a few days before labor starts or at the beginning of labor. - At a prenatal checkup, your health care provider tells you that your cervix has begun to efface (thin) and dilate (open). Before labor, your cervix is about 3.5 to 4 centimeters long. When it’s fully dilated (open) for labor, it’s 10 centimeters. Once labor starts, contractions help open your cervix.
- You have the nesting instinct. This is when you want to get things organized in your home to get ready for your baby. You may want to do things like cook meals or get the baby’s clothes and room ready. Doing these things is fine as long as you’re careful not to overdo it. You need your energy for labor and birth.
If you have any of these signs, you may start labor soon. Learn the signs of labor so you know when to call your provider.
What are false labor and Braxton-Hicks contractions?
Not all contractions mean you’re in labor. You may have contractions on and off before true labor starts. These contractions are called false labor or Braxton-Hicks contractions. They soften and thin the cervix to help your body get ready for labor and birth. You may feel them in the weeks right before your due date. Learning the differences between true labor contractions and false labor contractions can help you know when you’re really in labor.
You may have contractions on and off before true labor starts. These contractions are called false labor or Braxton-Hicks contractions. They soften and thin the cervix to help your body get ready for labor and birth. You may feel them in the weeks right before your due date. Learning the differences between true labor contractions and false labor contractions can help you know when you’re really in labor.
It can be hard to tell the difference between true labor and false labor. When you first feel contractions, time them. Write down how much time it takes from the start of one contraction to the start of the next. Make a note of how strong the contractions feel. Keep a record of your contractions for 1 hour. Walk or move around to see if the contractions stop when you change positions.
What is preterm labor?
Preterm labor is labor that begins too early, before 37 weeks of pregnancy. Premature babies (born before 37 weeks of pregnancy) can have health problems at birth and later in life.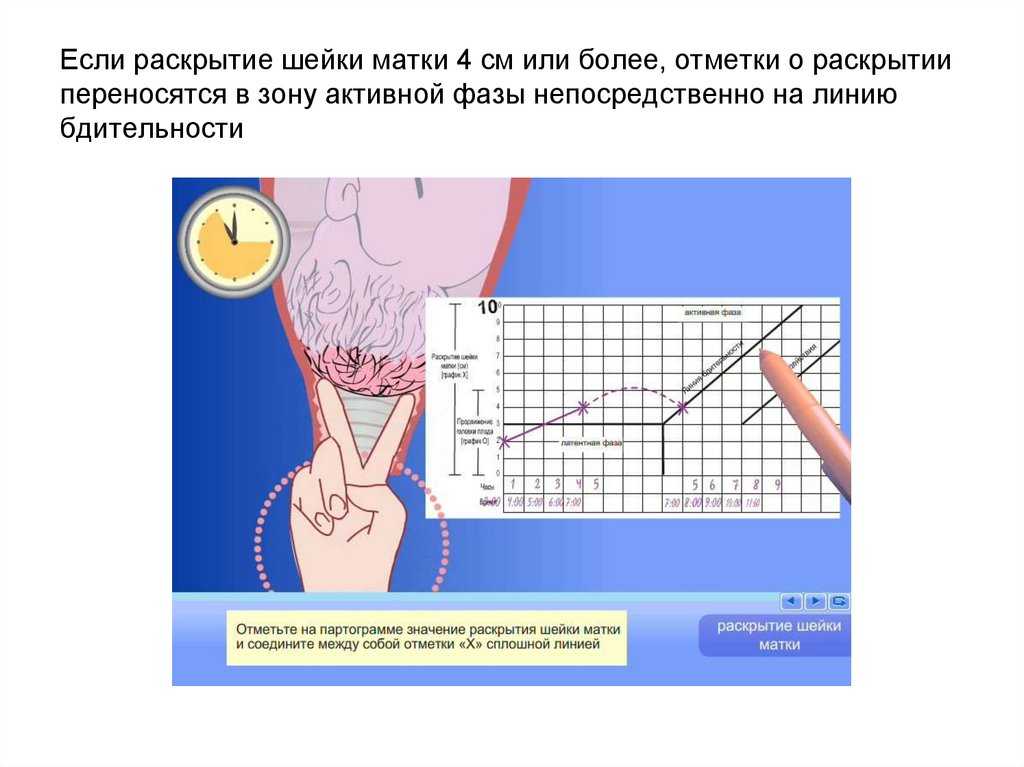 If you’re not to 37 weeks of pregnancy and you have signs or symptoms of preterm labor, call your provider. Getting help quickly is the best thing you can do. Learn about risk factors for preterm labor and what you can do to help reduce your risk.
If you’re not to 37 weeks of pregnancy and you have signs or symptoms of preterm labor, call your provider. Getting help quickly is the best thing you can do. Learn about risk factors for preterm labor and what you can do to help reduce your risk.
What are stages of labor?
Stages of labor include the whole process of labor, from your first contractions (stage 1) to pushing (stage 2) to delivery of the placenta (stage 3) after your baby is born. Learning about the stages of labor can help you know what to expect during labor and birth.
Last reviewed: December, 2018
Signs of Labor (Cervical Effacement) During Pregnancy
Written by WebMD Editorial Contributors
In this Article
- What Are the Signs of Labor?
- What's the Difference Between True Labor and False Labor?
- Time Your Contractions
- Try to Relax
- When Should I Call My Health Care Provider or Go to the Hospital?
What Are the Signs of Labor?
Labor is another word for your body’s natural process of childbirth. It starts with your first steady contractions and goes through the delivery of both your baby and placenta.
It starts with your first steady contractions and goes through the delivery of both your baby and placenta.
Some women have very distinct signs of labor, while others don’t. No one knows what causes labor to start or when it will start, but several hormonal and physical changes help indicate the beginning of labor.
Lightening during labor
The process of your baby settling or lowering into your pelvis just before labor is called lightening. It’s also referred to as the baby “dropping.”
- Lightening can happen a few weeks or a few hours before labor.
- Because the uterus rests on the bladder more after lightening, you may feel the need to urinate more often.
- But the extra room in your upper abdomen may make it easier to breathe and relieve heartburn.
Passing of the mucus plug
The mucus plug accumulates at the cervix during pregnancy. When the cervix begins to open wider, the mucus is discharged into the vagina.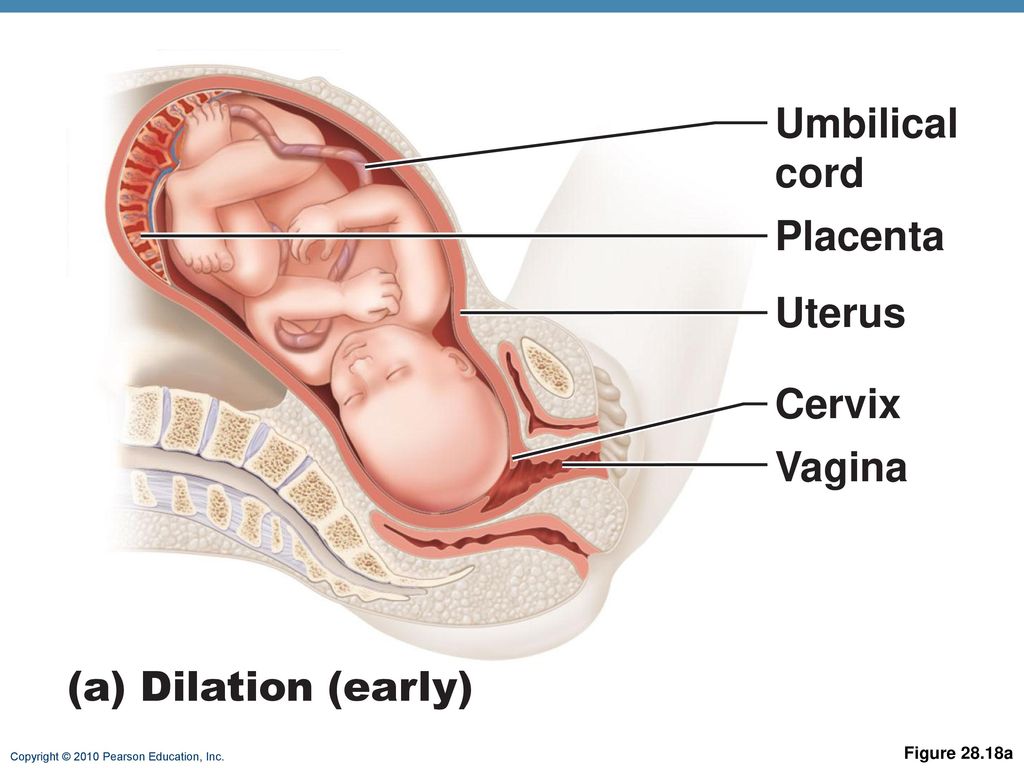 It may be clear, pink, or slightly bloody. This is also known as “show” or “bloody show.” Labor may begin soon after the mucus plug is discharged or one to two weeks later.
It may be clear, pink, or slightly bloody. This is also known as “show” or “bloody show.” Labor may begin soon after the mucus plug is discharged or one to two weeks later.
Labor contractions
Contractions are the tightening of the muscles of the uterus. During contractions, the abdomen becomes hard. Between contractions, the uterus relaxes and the abdomen becomes soft. The way a contraction feels is different for each woman, and it may feel different from one pregnancy to the next.
- Labor contractions usually cause discomfort or a dull ache in your back and lower abdomen, along with pressure in the pelvis.
- Contractions move in a wave-like motion from the top of the uterus to the bottom.
- Some women describe contractions as strong menstrual cramps.
- Unlike false labor contractions or Braxton Hicks contractions, true labor contractions don’t stop when you change your position or relax.
- Although they may be uncomfortable, you’ll be able to relax in between contractions.
Diarrhea
You may notice your poops are loose or watery. This may mean you are within a day or two of labor beginning.
Weight loss
While you’re pregnant, it may seem like you’re never going to stop gaining weight. But many women actually lose a few pounds in the days leading up to labor.
Nesting instinct
Some women find themselves with an urge to get ready shortly before their baby’s arrival. That’s known as the nesting instinct.
- You may have a sudden burst of energy after weeks of feeling more and more tired.
- You may feel like shopping, cooking, or cleaning the house.
- Be careful not to overdo it. Childbirth will take a lot of energy.
Activity of the baby
Your baby may move less as you get closer to the start of labor, but let your doctor know.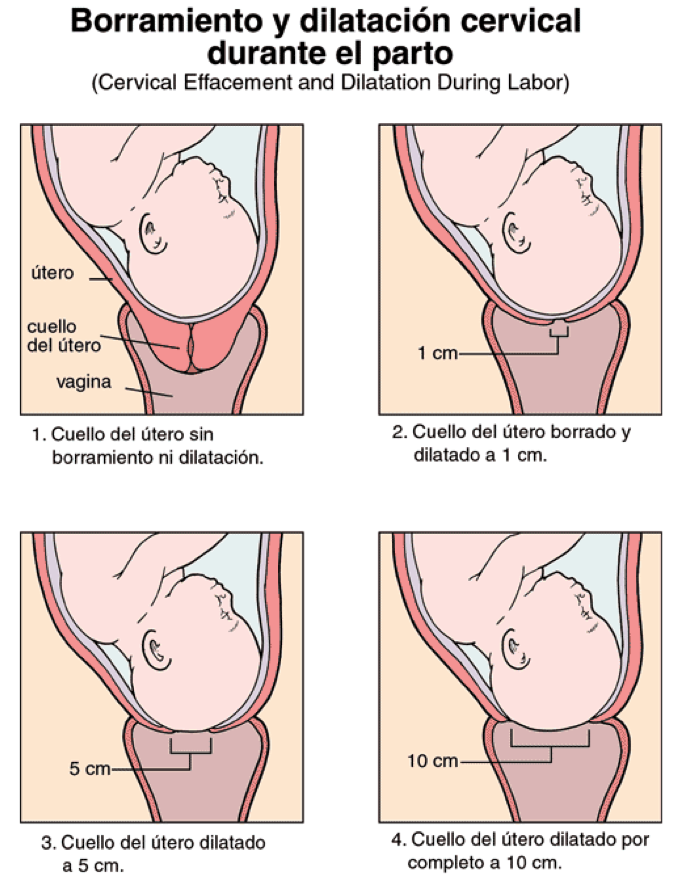 It can sometimes be a sign of a problem.
It can sometimes be a sign of a problem.
Cramps and back pain
It may be hard to recognize a contraction, especially with your first baby. Many women have what feels like menstrual cramps in the lower abdomen. They may stay the same or they may come and go. You might also have pain in your lower back that either stays or comes and goes.
Looser joints
If you find yourself “waddling” as your pregnancy winds down, that’s just your body getting ready for the job ahead. A hormone called relaxin loosens up the ligaments around your pelvis to make it easier for the baby to pass through.
Water breaking
The rupture of the amniotic membrane (the fluid-filled sac that surrounds the baby during pregnancy) may happen before you get to the hospital.
- It may feel either like a sudden gush of fluid or a trickle of fluid that leaks steadily.
- The fluid is usually odorless and may look clear or straw-colored.
- If your "water breaks," write down the time this happens, how much fluid is released, and what the fluid looks like, then let your health care provider know. They’ll advise you what to do next.
- Not all women have their water break when they’re in labor. Many times the doctor will rupture the amniotic membrane in the hospital.
Effacement
During labor, your cervix gets shorter and thins out in order to stretch and open around your baby's head. The shortening and thinning of the cervix is called effacement. Your health care provider will be able to tell you if there are changes to the cervix during a pelvic exam.
Effacement is measured in percentages from 0% to 100%. If there are no changes to the cervix, it is described as 0% effaced. When the cervix is half the normal thickness, it is 50% effaced. When the cervix is completely thinned out, it is 100% effaced.
Dilation
The stretching and opening of your cervix is called dilation and is measured in centimeters, with complete dilation being at 10 centimeters.
Effacement and dilation are a direct result of effective uterine contractions. Progress in labor is measured by how much the cervix has opened and thinned to allow your baby to pass through the vagina.
What's the Difference Between True Labor and False Labor?
Before "true" labor begins, you may have "false" labor pains, also known as Braxton Hicks contractions. These irregular uterine contractions are perfectly normal and may start to occur in your second trimester, although more commonly in your third trimester of pregnancy. They are your body's way of getting ready for the "real thing."
What do Braxton Hicks contractions feel like?
Braxton Hicks contractions can be described as a tightening in the abdomen that comes and goes. These contractions do not get closer together, do not increase with walking, do not increase in duration, and do not feel stronger over time as they do when you are in true labor.
How do I know when I am in true labor?
To figure out if the contractions you are feeling are the real thing, ask yourself the following questions.
| Contraction Characteristics | False Labor | True Labor |
| How often do the contractions occur? | Contractions are often irregular and do not get closer together. | Contractions come at regular intervals and last about 30-70 seconds. As time progresses, they get closer together. |
| Do they change with movement? | Contractions may stop when you walk or rest, or may even stop if you change positions. | Contractions continue despite movement or changing positions. |
| How strong are they? | Contractions are usually weak and do not get much stronger. Or they may be strong at first and then get weaker. | Contractions steadily increase in strength. |
| Where do you feel the pain? | Contractions are usually only felt in the front of the abdomen or pelvic region. | Contractions usually start in the lower back and move to the front of the abdomen. |
Time Your Contractions
When you think you are in true labor, start timing your contractions. To do this, write down the time each contraction starts and stops or have someone do it for you. The time between contractions includes the length or duration of the contraction and the minutes in between the contractions (called the interval).
Mild contractions generally begin 15 to 20 minutes apart and last 60 to 90 seconds. The contractions become more regular until they are less than 5 minutes apart. Active labor (the time you should come into the hospital) is usually characterized by strong contractions that last 45 to 60 seconds and occur 3 to 4 minutes apart.
The contractions become more regular until they are less than 5 minutes apart. Active labor (the time you should come into the hospital) is usually characterized by strong contractions that last 45 to 60 seconds and occur 3 to 4 minutes apart.
Try to Relax
It’s best to go through the first stage of labor (called the Latent Phase) in the comfort of your home. Here are some tips to help you manage:
- Distract yourself -- take a walk, watch a movie.
- Soak in a warm tub or take a warm shower. But, ask your health care provider if you can take a tub bath if your water has broken.
- Rest. Try to sleep or take a nap if it is in the evening. You need to store up your energy for active labor.
When Should I Call My Health Care Provider or Go to the Hospital?
When you suspect you are in true labor, call your health care provider. Also, call:
- If you think your water has broken.
- If you’re bleeding (more than spotting).

- If the baby seems to be moving less than normal.
- When your contractions are very uncomfortable and have been coming every 5 minutes for an hour.
- If you have any of the signs of labor, but you haven’t reached your 37th week of pregnancy. You may be going into labor before your baby is ready and will need medical help right away.
Your health care provider will give you specific guidelines about when you should get ready to come to the hospital.
ICI correction during pregnancy at St. Mary's Women's Health Clinic in Vladivostok
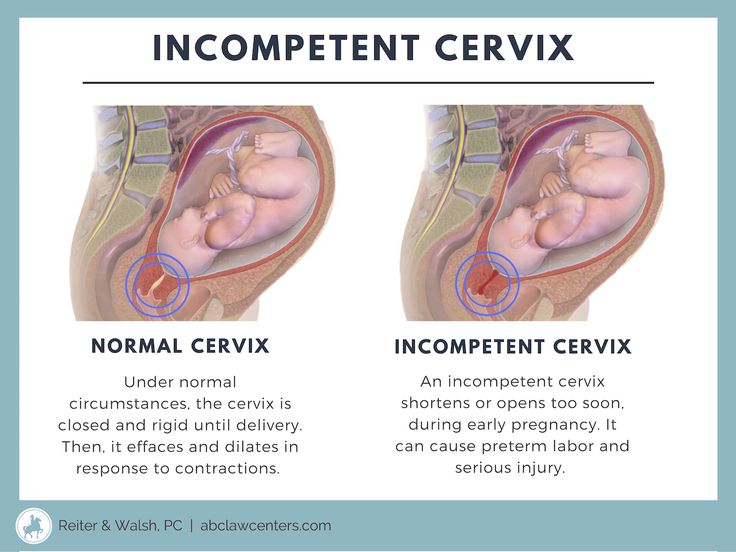
Isthmic-cervical insufficiency (abbreviated as ICI) is failure (insufficiency) of the isthmus and cervix. They are shortened, softened and slightly opened. This state during pregnancy is dangerous by spontaneous miscarriage.
When pregnancy is proceeding normally, the muscles of the cervix are in tone. This muscle ring holds the fetus, prevents it from leaving uterus ahead of schedule. As the term grows pregnancy, the size and weight of the fetus increase, the volume of amniotic water. In parallel, the load on the cervix also increases. At isthmic-cervical insufficiency, the muscles of the uterus are not able to cope with the growing workload.
This muscle ring holds the fetus, prevents it from leaving uterus ahead of schedule. As the term grows pregnancy, the size and weight of the fetus increase, the volume of amniotic water. In parallel, the load on the cervix also increases. At isthmic-cervical insufficiency, the muscles of the uterus are not able to cope with the growing workload.
With ICI, the fetus descends. The membranes of the fetal bladder bulge into cervical canal, they become infected, and they are opened. it threatened with premature birth.
Most often, ICI correction is necessary for multiple pregnancies.
What are the symptoms of isthmic-cervical insufficiency?
The symptoms of ICI are usually very mild.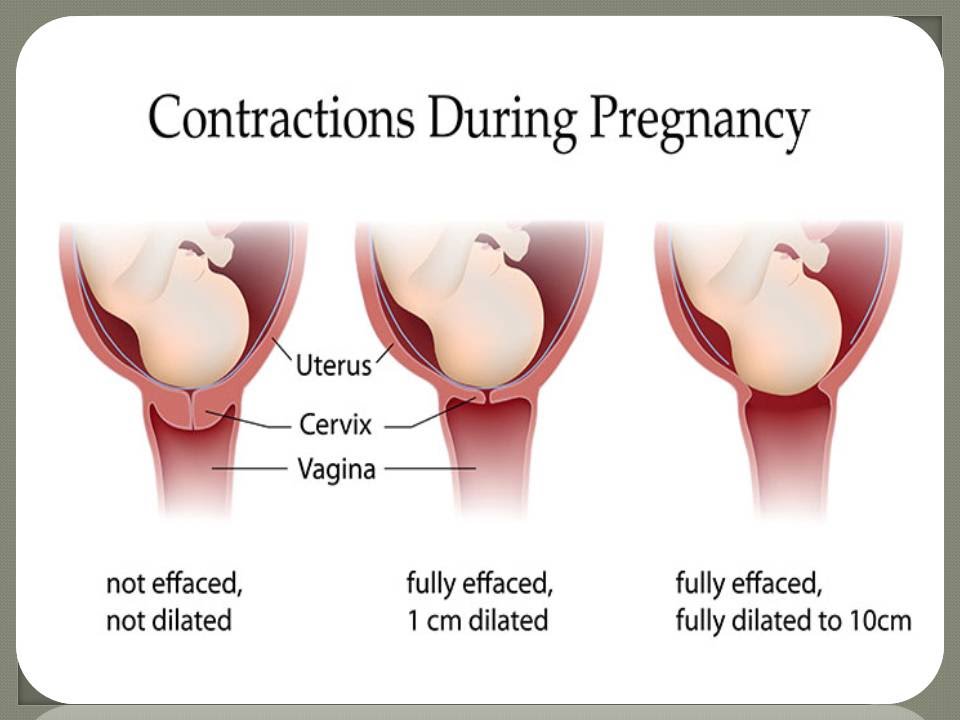 After all, pathology occurs due to the opening of the cervix - a condition in which there is no noticeable bleeding, no noticeable pain.
After all, pathology occurs due to the opening of the cervix - a condition in which there is no noticeable bleeding, no noticeable pain.
A pregnant woman may experience the following symptoms:
- feeling of heaviness in the lower abdomen;
- frequent urination;
- profuse vaginal discharge of a mucous nature.
If such manifestations occur, they should be reported immediately. obstetrician-gynecologist.
Treatment of cervical insufficiency
Timely diagnosis, medical and protective regimen, correct management of pregnancy, as well as positive psychological mood will help bring the pregnancy to a normal term and give birth healthy child.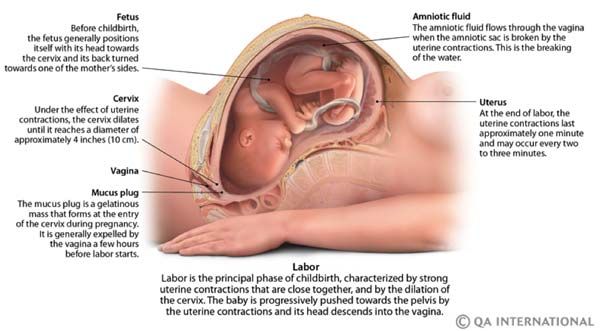
There are different ways to correct CCI:
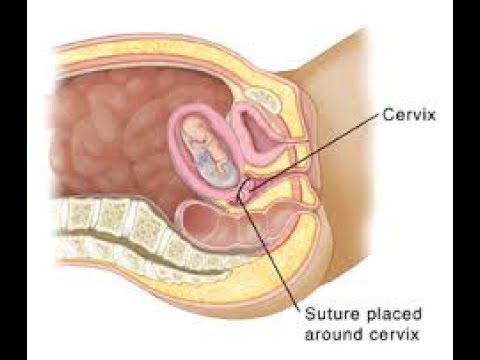
- Suturing the cervix.
- Use of obstetric pessaries.
- Combination of the above two methods.
Surgical treatment of CCI
The essence of surgical correction of CI is quite simple. The stitches placed on the cervix, help to strengthen it, prevent further disclosure. As a result, she is again able to cope with the growing load. Usually sutures are placed at 13-17 weeks of gestation, but for each woman it is individual. The timing of surgical correction is determined by the time occurrence of CI and its clinical manifestations.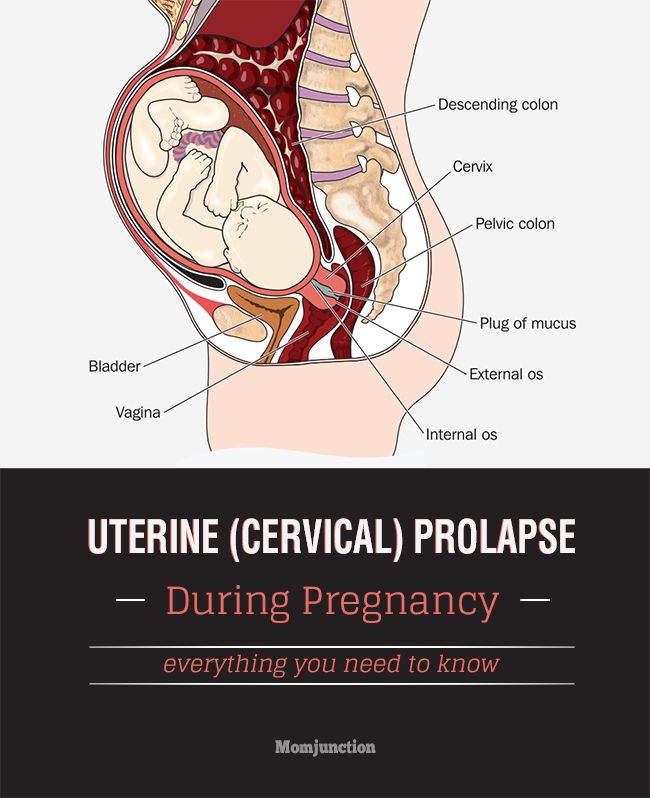
Surgical treatment is carried out in a hospital, under intravenous anesthesia. Medicines that are applied, absolutely safe for the fetus. Once on the neck the uterus is sutured, the doctor prescribes drugs that reduce the tone uterus.
Use of obstetric pessaries
An obstetrician-gynecologist can install an obstetric pessary on an outpatient basis, for This does not require hospitalization. Usually in practice obstetric pessaries are installed no earlier than 20-22 weeks of pregnancy. At earlier dates, doctors prefer to apply on the cervix seams.
Indications for suture removal and pessary removal:
- Gestational gestational age 37-38 weeks: if delivery occurs before this period, they will be considered premature and the stitches will be removed and/or removal of the pessary during delivery.
- If an emergency delivery is needed.
- If the amniotic fluid has broken.
- If a woman goes into labor.
If you experience the symptoms described on this page, contact doctor. Timely treatment will help prevent interruption pregnancy and provide optimal conditions for the development of your future baby.
We will be happy to answer
+7 (423) 233-90-55 +7 (423) 244-00-00 [email protected]
Changes in the cervix during pregnancy
Pregnancy is always pleasant, but sometimes not planned. And not all women have time to prepare for it, to be fully examined before its onset. And the detection of diseases of the cervix already during pregnancy can be an unpleasant discovery.
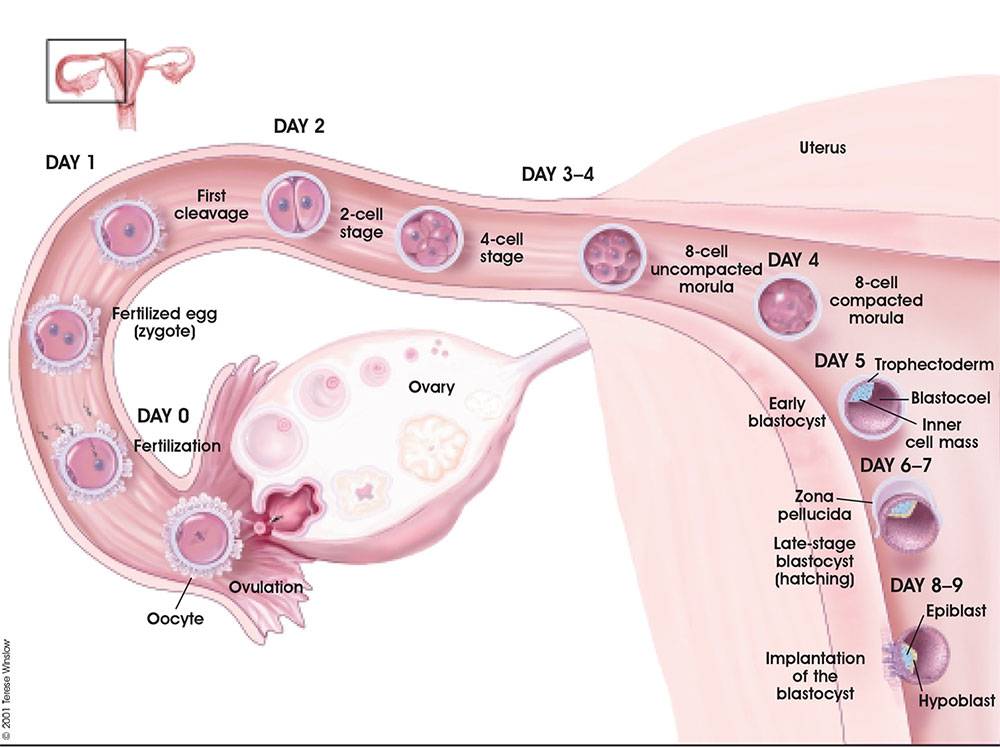
The cervix is the lower segment of the uterus in the form of a cylinder or cone. In the center is the cervical canal, one end of which opens into the uterine cavity, and the other into the vagina. On average, the length of the cervix is 3–4 cm, the diameter is about 2.5 cm, and the cervical canal is closed. The cervix has two parts: lower and upper. The lower part is called the vaginal, because it protrudes into the vaginal cavity, and the upper part is supravaginal, because it is located above the vagina. The cervix is connected to the vagina through the vaginal fornices. There is an anterior arch - short, posterior - deeper and two lateral ones. Inside the cervix passes the cervical canal, which opens into the uterine cavity with an internal pharynx, and is clogged with mucus from the side of the vagina. Mucus is normally impervious to infections and microbes, or to spermatozoa. But in the middle of the menstrual cycle, the mucus thins and becomes permeable to sperm.
In the center is the cervical canal, one end of which opens into the uterine cavity, and the other into the vagina. On average, the length of the cervix is 3–4 cm, the diameter is about 2.5 cm, and the cervical canal is closed. The cervix has two parts: lower and upper. The lower part is called the vaginal, because it protrudes into the vaginal cavity, and the upper part is supravaginal, because it is located above the vagina. The cervix is connected to the vagina through the vaginal fornices. There is an anterior arch - short, posterior - deeper and two lateral ones. Inside the cervix passes the cervical canal, which opens into the uterine cavity with an internal pharynx, and is clogged with mucus from the side of the vagina. Mucus is normally impervious to infections and microbes, or to spermatozoa. But in the middle of the menstrual cycle, the mucus thins and becomes permeable to sperm.
Outside, the surface of the cervix has a pinkish tint, it is smooth and shiny, durable, and from the inside it is bright pink, velvety and loose.
The cervix during pregnancy is an important organ, both in anatomical and functional terms. It must be remembered that it promotes the process of fertilization, prevents infection from entering the uterine cavity and appendages, helps to "endure" the baby and participates in childbirth. That is why regular monitoring of the condition of the cervix during pregnancy is simply necessary.
During pregnancy, a number of physiological changes occur in this organ. For example, a short time after fertilization, its color changes: it becomes cyanotic. The reason for this is the extensive vascular network and its blood supply. Due to the action of estriol and progesterone, the tissue of the cervix becomes soft. During pregnancy, the cervical glands expand and become more branched.
Screening examination of the cervix during pregnancy includes: cytological examination, smears for flora and detection of infections. Cytological examination is often the first key step in the examination of the cervix, since it allows to detect very early pathological changes that occur at the cellular level, including in the absence of visible changes in the cervical epithelium.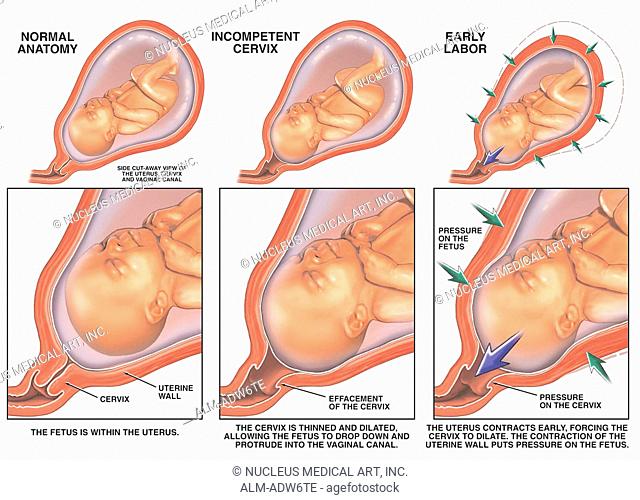 The examination is carried out to identify the pathology of the cervix and the selection of pregnant women who need a more in-depth examination and appropriate treatment in the postpartum period. When conducting a screening examination, in addition to a doctor's examination, a colposcopy may be recommended. As you know, the cervix is covered with two types of epithelium: squamous stratified from the side of the vagina and single-layer cylindrical from the side of the cervical canal. Epithelial cells are constantly desquamated and end up in the lumen of the cervical canal and in the vagina. Their structural characteristics make it possible, when examined under a microscope, to distinguish healthy cells from atypical ones, including cancerous ones.
The examination is carried out to identify the pathology of the cervix and the selection of pregnant women who need a more in-depth examination and appropriate treatment in the postpartum period. When conducting a screening examination, in addition to a doctor's examination, a colposcopy may be recommended. As you know, the cervix is covered with two types of epithelium: squamous stratified from the side of the vagina and single-layer cylindrical from the side of the cervical canal. Epithelial cells are constantly desquamated and end up in the lumen of the cervical canal and in the vagina. Their structural characteristics make it possible, when examined under a microscope, to distinguish healthy cells from atypical ones, including cancerous ones.
During pregnancy, in addition to physiological changes in the cervix, some borderline and pathological processes may occur.
Under the influence of hormonal changes that occur in a woman's body during the menstrual cycle, cyclic changes also occur in the cells of the epithelium of the cervical canal. During the period of ovulation, the secretion of mucus by the glands of the cervical canal increases, and its qualitative characteristics change. With injuries or inflammatory lesions, sometimes the glands of the cervix can become clogged, a secret accumulates in them and cysts form - Naboth follicles or Naboth gland cysts that have been asymptomatic for many years. Small cysts do not require any treatment. And pregnancy, as a rule, is not affected. Only large cysts that strongly deform the cervix and continue to grow may require opening and evacuation of the contents. However, this is very rare and usually requires monitoring during pregnancy.
During the period of ovulation, the secretion of mucus by the glands of the cervical canal increases, and its qualitative characteristics change. With injuries or inflammatory lesions, sometimes the glands of the cervix can become clogged, a secret accumulates in them and cysts form - Naboth follicles or Naboth gland cysts that have been asymptomatic for many years. Small cysts do not require any treatment. And pregnancy, as a rule, is not affected. Only large cysts that strongly deform the cervix and continue to grow may require opening and evacuation of the contents. However, this is very rare and usually requires monitoring during pregnancy.
Quite often, in pregnant women, during a mirror examination of the vaginal part, polyps cervix. The occurrence of polyps is most often associated with a chronic inflammatory process. As a result, a focal proliferation of the mucosa is formed, sometimes with the involvement of muscle tissue and the formation of a pedicle.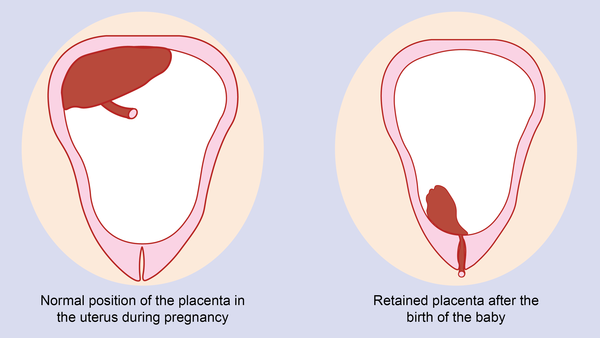 They are mostly asymptomatic. Sometimes they are a source of blood discharge from the genital tract, more often of contact origin (after sexual intercourse or defecation). The size of the polyp is different - from millet grain rarely to the size of a walnut, their shape also varies. Polyps are single and multiple, their stalk is located either at the edge of the external pharynx, or goes deep into the cervical canal. Sometimes during pregnancy there is an increase in the size of the polyp, in some cases quite fast. Rarely, polyps first appear during pregnancy. The presence of a polyp is always a potential threat of miscarriage, primarily because it creates favorable conditions for ascending infection. Therefore, as a rule, more frequent monitoring of the cervix follows. The tendency to trauma, bleeding, the presence of signs of tissue necrosis and decay, as well as questionable secretions require special attention and control. Treatment of cervical polyps is only surgical and during pregnancy, in most cases, treatment is postponed until the postpartum period, since even large polyps do not interfere with childbirth.
They are mostly asymptomatic. Sometimes they are a source of blood discharge from the genital tract, more often of contact origin (after sexual intercourse or defecation). The size of the polyp is different - from millet grain rarely to the size of a walnut, their shape also varies. Polyps are single and multiple, their stalk is located either at the edge of the external pharynx, or goes deep into the cervical canal. Sometimes during pregnancy there is an increase in the size of the polyp, in some cases quite fast. Rarely, polyps first appear during pregnancy. The presence of a polyp is always a potential threat of miscarriage, primarily because it creates favorable conditions for ascending infection. Therefore, as a rule, more frequent monitoring of the cervix follows. The tendency to trauma, bleeding, the presence of signs of tissue necrosis and decay, as well as questionable secretions require special attention and control. Treatment of cervical polyps is only surgical and during pregnancy, in most cases, treatment is postponed until the postpartum period, since even large polyps do not interfere with childbirth.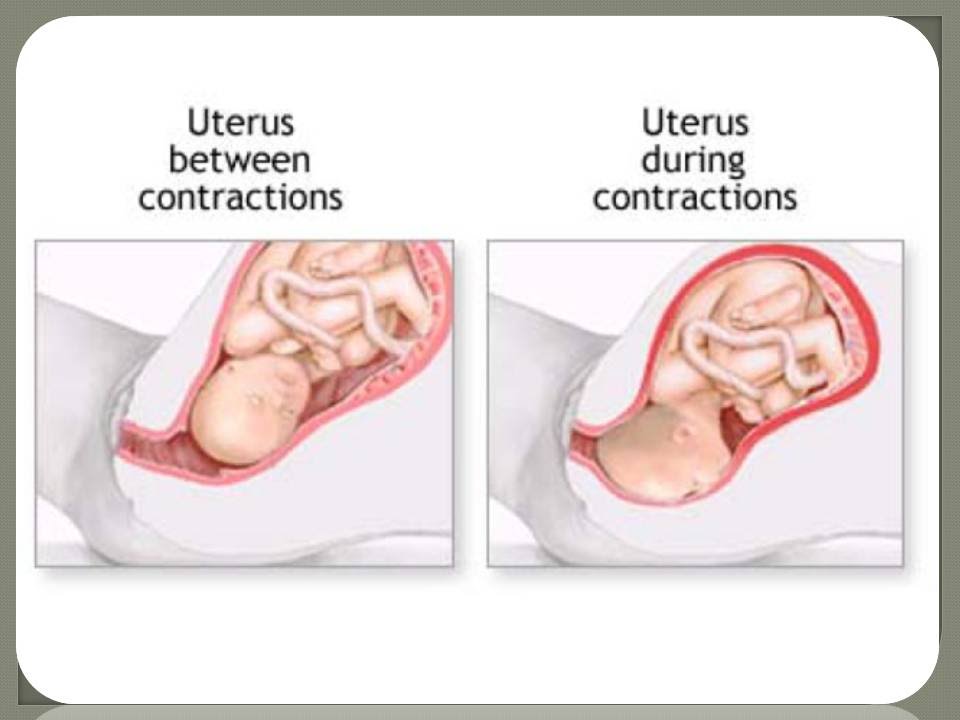
The most common pathology of the cervix in women is erosion . Erosion is a defect in the mucous membrane. True erosion is not very common. The most common pseudo-erosion (ectopia) is a pathological lesion of the cervical mucosa, in which the usual flat stratified epithelium of the outer part of the cervix is replaced by cylindrical cells from the cervical canal. Often this happens as a result of mechanical action: with frequent and rough sexual intercourse, desquamation of the stratified squamous epithelium occurs. Erosion is a multifactorial disease. The reasons may be:
- genital infections, vaginal dysbacteriosis and inflammatory diseases of the female genital area;
- is an early onset of sexual activity and frequent change of sexual partners. The mucous membrane of the female genital organs finally matures by the age of 20-23. If an infection interferes with this delicate process, erosion is practically unavoidable;
- is an injury to the cervix.
 The main cause of such injuries is, of course, childbirth and abortion;
The main cause of such injuries is, of course, childbirth and abortion; - hormonal disorders;
- , cervical pathology may also occur with a decrease in the protective functions of immunity.
The presence of erosion does not affect pregnancy in any way, as well as pregnancy on erosion. Treatment during pregnancy consists in the use of general and local anti-inflammatory drugs for inflammatory diseases of the vagina and cervix. And in most cases, just dynamic observation is enough. Surgical treatment is not carried out throughout the entire pregnancy, since the excess of risks and benefits is significant, and after treatment during childbirth, there may be problems with opening the cervix.
Almost all women with various diseases of the cervix safely bear and happily give birth to beautiful babies!
Attention! Prices for services in different clinics may vary. To clarify the current cost, select a clinic
Clinical Hospital of IDKClinic "Mother and Child" Entuziastov Samara
All directionsSpecialist consultations (adults)Specialist consultations (children's)Laboratory of molecular geneticsGeneral clinical examinationsProcedural roomOther gynecological operationsTelemedicine for adultsTherapeutic examinationsUltrasound examinations for adults
01.