At what age can you get pregnant
What’s Ideal and What Are the Risks?
Childbearing Age: What’s Ideal and What Are the Risks?Medically reviewed by Holly Ernst, PA-C — By Stephanie Watson on June 6, 2018
What’s the childbearing age?
Technically, women can get pregnant and bear children from puberty when they start getting their menstrual period to menopause when they stop getting it. The average woman’s reproductive years are between ages 12 and 51.
Your fertility naturally declines as you get older, which could make it harder for you to conceive. And starting a family later in life could pose greater risks for pregnancy complications.
Experts say the best time to get pregnant is between your late 20s and early 30s. This age range is associated with the best outcomes for both you and your baby. One study pinpointed the ideal age to give birth to a first child as 30.5.
Your age is just one factor that should go into your decision to get pregnant. You also need to consider your emotional and financial readiness to start a family. That timing is unique for each woman.
How does age affect fertility?
Women are born with all the eggs they’ll ever have — about 2 million of them. Your number of eggs gradually falls over the years.
By age 37, you’ll have about 25,000 eggs left. By age 51, you’ll only have 1,000 eggs left. That might still sound like a lot of eggs, but the quality of your eggs also goes down as you age.
Your risk for developing conditions that can negatively impact fertility, like endometriosis and tubal disease, also increases as you get older.
Because of these factors, your fertility begins to gradually decline at around age 32. Starting between 35 and 37, fertility begins to drop more quickly.
Your chance of getting pregnant decreases as you get older. After three months of trying, your odds of conceiving in during your next cycle are:
- 18 percent at age 25
- 16 percent at age 30
- 12 percent at age 35
- 7 percent at age 40
Other factors may reduce your chances of getting pregnant, including:
- smoking
- cancer treatments such as radiation and chemotherapy
- pelvic infection
What are the benefits of getting pregnant at certain ages?
Women in the United States are waiting longer than ever to get pregnant. The average age of first-time moms is nearly 27, according to the Centers for Disease Control and Prevention. Birth rates have risen among women in their 30s and dropped among those in their 20s.
The average age of first-time moms is nearly 27, according to the Centers for Disease Control and Prevention. Birth rates have risen among women in their 30s and dropped among those in their 20s.
Benefits of delaying starting a family
Waiting to start a family can have some benefits. You’ll have more time to save up money, establish your relationship, and become more financially secure for your child.
Age can also bring wisdom and patience. And there’s some evidence that children born to older parents achieve higher levels of education.
Holding off on pregnancy might have advantages for you, as well. A 2012 study suggested that women who gave birth to their last or only child at age 40 or older had a lower risk for uterine cancer.
Benefits of having children at a younger age
Being a younger mother is more beneficial to your baby’s health. Your odds of conceiving are increased in your late 20s or early 30s. Getting pregnant during this time also reduces your chances of having a pregnancy complication.
Risks of getting pregnant at age 35 and older
Starting at age 35, these pregnancy risks become more common:
- gestational diabetes
- high blood pressure
- preeclampsia
- placenta previa
- miscarriage
- premature birth
- stillbirth
- need for a cesarean delivery
- heavy bleeding after delivery
- infant low birth weight
- chromosomal abnormalities such as Down syndrome
When should you see a doctor for fertility questions?
Fertility issues are very common. More than 12 percent of women have difficulties getting pregnant. If you haven’t been able to get pregnant, a fertility specialist can do tests to see why you’re not conceiving and offer treatments to improve your odds of a pregnancy.
See a fertility specialist if:
- You’re age 35 or younger and you’ve been trying to get pregnant for a year.
- You’re over age 35 and you’ve been trying for more than 6 months.

- You’re over age 40 and you’d like to start a family.
The fertility treatment your doctor recommends depends on factors like the cause of your fertility issues, your age, and your preferences. Options include:
- fertility drugs to stimulate ovulation
- surgery to fix a uterine condition, such as endometriosis, fibroids, or blocked fallopian tubes
- intrauterine insemination, where sperm is placed directly into your uterus during ovulation
- in vitro fertilization, where sperm and egg are placed together in a lab until they form an embryo, which is then implanted into your uterus
- zygote intrafallopian transfer and gamete intrafallopian transfer, where the sperm and egg or a fertilized egg is placed into your fallopian tube
Tips for conception
If you’re ready to start trying for a baby, here are a few things you can do to help make parenthood a reality:
- Get to a healthy weight. An ideal body mass index is between 19 and 24.
 Being overweight or underweight can affect your ability to ovulate.
Being overweight or underweight can affect your ability to ovulate. - Quit smoking. Smoking can damage your egg supply and make you more likely to miscarry if you do get pregnant.
- Watch your diet. Eating a high-fat diet can contribute to weight gain and disrupt your reproductive cycle.
- Limit caffeine and alcohol. Research has linked excess amounts of caffeine (more than two or three cups of coffee daily) with miscarriage. Frequent alcohol use can prolong the time it takes you to get pregnant and is harmful to fetal development.
You can increase your chances of having a healthy baby by following these tips:
- Treat any conditions that could make pregnancy risky, including diabetes and high blood pressure.
- See your obstetrician for a preconception visit to make sure you’re healthy enough to get pregnant. Then, keep up with all of your scheduled pregnancy visits. Seeing you regularly will let your doctor monitor your and your baby’s health and address any problems that arise.
- Take good care of your body. Don’t smoke or drink alcohol, follow a healthy eating plan, exercise often, and get enough sleep.
The takeaway
You’ll have the best odds of getting pregnant and having a healthy baby if you start trying in your 20s or 30s, but that scenario isn’t right for every woman. When deciding to start a family, you also need to consider whether you’re:
- in a solid relationship or have the support system to have a child on your own
- ready to temporarily put your career on hold
- financially secure enough to support a child
If you have any concerns about your ability to get pregnant, see your gynecologist or visit a fertility specialist.
Last medically reviewed on June 6, 2018
- Parenthood
- Pregnancy
How we reviewed this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
- Age and fertility. (n.d.).
pregnancy.sogc.org/fertility-and-reproduction/age-and-fertility - Alcohol and fertility. (n.d.).
yourfertility.org.au/for-women/alcohol-and-fertility/ - Barclay K. (2016). Advanced maternal age and offspring outcomes: Reproductive aging and counterbalancing period trends. DOI:
10.1111/j.1728-4457.2016.00105.x - Births and natality. (2017).
cdc.gov/nchs/fastats/births.htm - Births in the United States, 2016. (2017).
cdc.gov/nchs/products/databriefs/db287.htm - Dietl A, et al. (2015). Pregnancy and obstetrical outcomes in women over 40 years of age. DOI:
10.1055/s-0035-1546109 - Female age-related fertility decline. (2014).
acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Gynecologic-Practice/Female-Age-Related-Fertility-Decline - Having a baby after age 35.
 (2017).
(2017).
acog.org/Patients/FAQs/Having-a-Baby-After-Age-35 - Infertility. (2016).
cdc.gov/nchs/fastats/infertility.htm - Lyngsø J, et al. (2017). Association between coffee or caffeine consumption and fecundity and fertility: A systematic review and dose-response meta-analysis. DOI:
10.2147/CLEP.S146496 - Mayo Clinic Staff. (2018). Infertility.
mayoclinic.org/diseases-conditions/infertility/diagnosis-treatment/drc-20354322 - Menopause 101: A primer for the perimenopausal. (n.d.).
menopause.org/for-women/menopauseflashes/menopause-symptoms-and-treatments/menopause-101-a-primer-for-the-perimenopausal - Mirowsky J. (2002). Parenthood and health: The pivotal and optimal age at first birth. DOI:
10.1353/sof.2002.0055 - Periods. (2016).
nhs.uk/conditions/periods - Setiawan VW, et al. (2012). Age at last birth in relation to risk of endometrial cancer: pooled analysis in the epidemiology of endometrial cancer consortium.
 DOI:
DOI:
10.1093/aje/kws129 - Sozou PD. (2012). Time to pregnancy: A computational method for using the duration of non-conception for predicting conception. DOI:
10.1371/journal.pone.0046544 - When to see a fertility specialist. (n.d.).
fertility.womenandinfants.org/services/see-fertility-specialist
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
Share this article
Medically reviewed by Holly Ernst, PA-C — By Stephanie Watson on June 6, 2018
Read this next
How Long Does It Take to Get Pregnant?
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
Getting pregnant can take longer than expected. Many couples also struggle with infertility. Learn how long it typically takes to conceive after sex…
READ MORE
Gifts for a Friend Going Through IVF
Medically reviewed by Karen Gill, M.
 D.
D.In vitro fertilization is a tough journey. Let your friend know you’re there for them. Here are our top picks of gifts that anyone going through IVF…
READ MORE
How Much of Infertility Is Genetic?
From health conditions to hormonal imbalances, it can seem that there are so many possible causes of infertility. Find out whether genetics play a…
READ MORE
How Fertility Treatment May Affect Your Mental Health
Medically reviewed by Joslyn Jelinek, LCSW
Infertility can affect your mental health. We explore the impact of infertility on your mental health and ways to feel better.
READ MORE
What’s the Infertility Journey Like for Non-Carrying Partners?
Fertility treatments take a toll on nonpregnant partners, too. We discuss their journey and provide expert advice on finding support.

READ MORE
What to Know in Your 20s, 30s, and 40s
Age and Fertility: What to Know in Your 20s, 30s, and 40sMedically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT — By Stephanie Watson on September 19, 2018
Overview
Thanks to contraception and the widespread availability of reproductive technologies, couples today have more control over when they want to begin their family than in the past.
Waiting to start a family is possible, although it can make it a little harder to get pregnant.
Fertility naturally declines with age, and having a baby later in life can increase the risk for pregnancy complications.
That said, there’s no “best age” to get pregnant. The decision to start a family should be based on many factors — including your age and your readiness to be a parent.
Just because you’re over 30 or 40 doesn’t mean you can’t have a healthy baby.
Read on to learn more about getting pregnant in each stage of your life.
In your 20s
Women are most fertile and have the best chance of getting pregnant in their 20s.
This is the time when you have the highest number of good quality eggs available and your pregnancy risks are lowest.
At age 25, your odds of conceiving after 3 months of trying are just under 20 percent.
In your 30s
Fertility gradually begins to decline at around age 32. After age 35, that decline speeds up.
Women are born with all the eggs they’ll ever have — about 1 million of them. The number of eggs gradually drops over time.
At age 37, it’s estimated that you’ll have around 25,000 eggs left.
By age 35, your odds of conceiving after 3 months of trying are about 12 percent.
The risk for miscarriage and genetic abnormalities also begins to rise after age 35. You might face more complications in your pregnancy or during delivery having a baby later in life.
Due to this, your doctor might recommend additional screening and testing for you and your baby.
In your 40s
There’s a steep decline in a woman’s ability to get pregnant naturally in her 40s. At age 40, your odds of conceiving after 3 months of trying are around 7 percent.
Over time, the quantity and quality of your eggs decline. Older eggs can have more chromosome problems, which increases the odds of having a baby with a birth defect.
Most women in their 40s can still have a healthy pregnancy and baby, but the risks increase significantly during this time. These risks include:
- C-section delivery
- premature birth
- low birth weight
- birth defects
- stillbirth
Medical conditions, like diabetes and high blood pressure, are more common in women after age 35. These can lead to pregnancy complications like gestational diabetes and preeclampsia.
After age 40, your doctor may do extra testing and monitoring to look for possible complications.
Fertility options
If you’re over 35 and you’ve been trying to get pregnant for more than 6 months, you might be dealing with fertility issues. Your doctor or a fertility specialist can help determine why you aren’t pregnant yet and recommend next steps for trying to conceive.
Your doctor or a fertility specialist can help determine why you aren’t pregnant yet and recommend next steps for trying to conceive.
Assisted reproductive technologies (ART) can help you conceive, but they can’t entirely make up for age-related declines in your fertility.
Doctors treat fertility issues in women with drugs that stimulate egg production, and techniques like in vitro fertilization (IVF).
But the odds of achieving a successful pregnancy with these methods do get lower as you age.
Another option is to use a healthy donor egg. The egg is fertilized with your partner’s sperm and then transferred to your uterus.
Freezing your eggs
If you’re not quite ready to have a family but know that you’ll want one in the future, you might want to consider freezing your eggs during your peak reproductive years.
First, you’ll take hormones to stimulate egg production. Then the eggs will be retrieved and frozen. They can stay frozen for several years.
When you’re ready to use them, the eggs will be thawed and injected with a sperm to be fertilized. The resulting embryos will then be implanted in your uterus.
Freezing your eggs won’t guarantee a pregnancy. Conceiving — even with younger eggs — is more difficult once you’re in your late 30s and 40s. But it can ensure that healthy eggs are available to you when you’re ready.
Male fertility
A man’s fertility also declines with age. But this process happens later, usually starting around age 40.
After that age, men have a lower semen volume and sperm count. The sperm they do have don’t swim as well.
Sperm cells of an older man are also more likely to have genetic abnormalities than those of a younger man.
The older a man is, the longer it will take him to get his partner pregnant. And his partner is at greater risk for a miscarriage, regardless of her age.
This doesn’t mean that a man can’t father children in his 40s and beyond. But it might be a little more difficult than it was earlier in his life.
Benefits of having children later | Benefits
In addition to giving you time to explore your career and relationship, waiting to get pregnant has other benefits to both you and your baby.
A 2016 study found that older mothers are more patient and tend to yell and punish their children less. Their children also have fewer social, emotional, and behavioral problems in elementary school.
Research has also found that children born to older mothers are generally healthier and end up better educated than their peers who were born to younger mothers.
Waiting to get pregnant might even help you live longer. Another 2016 study found that the odds of living to 90 were much higher in women who delayed having children.
There’s no proof that delaying childbearing directly causes any of these effects. It’s possible that other factors in older mothers besides their age might have played a role. But these findings suggest there are some advantages to waiting.
When to get help
If you’ve been trying to get pregnant but aren’t having any luck, it’s time to see a fertility specialist.
Here’s when to see a doctor:
- within a year of trying if you’re under age 35
- within 6 months if you’re over age 35
Couples with known genetic diseases or those who’ve had multiple miscarriages should also check in with their doctor or a fertility specialist.
Takeaway
The passing years can make it more challenging to get pregnant. Yet it’s still possible to have a healthy baby when you’re in your 30s or 40s.
Ultimately, the perfect time to get pregnant is when it feels right to you. It’s not unreasonable to wait until you feel more confident in your career and finances to start building your family.
If you do choose to wait, you might want to check in with your doctor or a fertility specialist to make sure no health issues will stand in your way once you’re ready.
Last medically reviewed on September 19, 2018
- Parenthood
- Pregnancy
How we reviewed this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
- Age and fertility. (2017).
betterhealth.vic.gov.au/health/conditionsandtreatments/age-and-fertility - Age and fertility. (n.d.).
pregnancy.sogc.org/fertility-and-reproduction/age-and-fertility/ - Barclay K, et al. (2016). Advanced maternal age and offspring outcomes: Reproductive aging and counterbalancing period trends. DOI:
doi.org/10.1111/j.1728-4457.2016.00105.x - Belloc S, et al. (2014). How to overcome male infertility after 40: Influence of paternal age on fertility. DOI:
ncbi.nlm.nih.gov/pubmed/24680129 - Cohen WR. (2014). Does maternal age affect pregnancy outcome? DOI:
doi.org/10.1111/1471-0528.12563 - Female reproductive system. (2012).
my.clevelandclinic.org/health/articles/9118-female-reproductive-system - Pregnancy after age 35.
 (2016).
(2016).
marchofdimes.org/complications/pregnancy-after-age-35.aspx - Shadyab AH, et al. (2016). Maternal age at childbirth and parity as predictors of longevity among women in the United States: The Women’s Health Initiative.
ajph.aphapublications.org/doi/abs/10.2105/AJPH.2016.303503 - Sozou PD, et al. (2012). Time to pregnancy: A computational method for using the duration of non-conception for predicting conception. DOI:
doi.org/10.1371/journal.pone.0046544 - Thinking about fertility treatment. (2016).
marchofdimes.org/pregnancy/thinking-about-fertility-treatment.aspx - Trillingsgaard T, et al. (2016). Associations between older maternal age, use of sanctions, and children’s socio-economic development through 7, 11, and 15 years. DOI:
doi.org/10.1080/17405629.2016.1266248
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
Current Version
Sep 19, 2018
Written By
Stephanie Watson
Edited By
Nizam Khan (TechSpace)
Medically Reviewed By
Debra Rose Wilson, PhD, MSN, RN, IBCLC, AHN-BC, CHT
Share this article
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT — By Stephanie Watson on September 19, 2018
Read this next
5 Common Signs of Infertility in Men and Women
Medically reviewed by Nicole Galan, RN
Many couples experience problems with infertility when trying to conceive. Here are the common symptoms of infertility.
READ MORE
Fertility Drugs: Treatment Options for Women and Men
Medically reviewed by Alan Carter, Pharm.D.
Fertility treatments can be confusing — what are they and what do they do? Here’s a list of fertility drugs to help you decide if one’s a good option…
READ MORE
What Medicines Can I Take While Pregnant?
Medically reviewed by Dena Westphalen, Pharm.
 D.
D.If you’re wondering what medicines are safe during pregnancy, you’re not alone. It’s important to talk to your doctor and be cautious, as some…
READ MORE
The Best 7 At-Home Fertility Tests of 2022
Medically reviewed by Amanda Kallen, MD
At-home fertility tests are a great option for people wanting an answer about their fertility as soon as possible. Read on for the best at-home…
READ MORE
What to Expect from the Egg Freezing Process
For various reasons, many people are choosing to delay pregnancy, yet still want to preserve fertility. Here's what to expect from the egg freezing…
READ MORE
Early pregnancy and childbirth in adolescence
For all questions, please contact:
Kiev (Poznyaki)
st. A. Akhmatova 31
+38(096) 683-06-18
+38(063) 217-14-64
Sign up for a consultation
General information.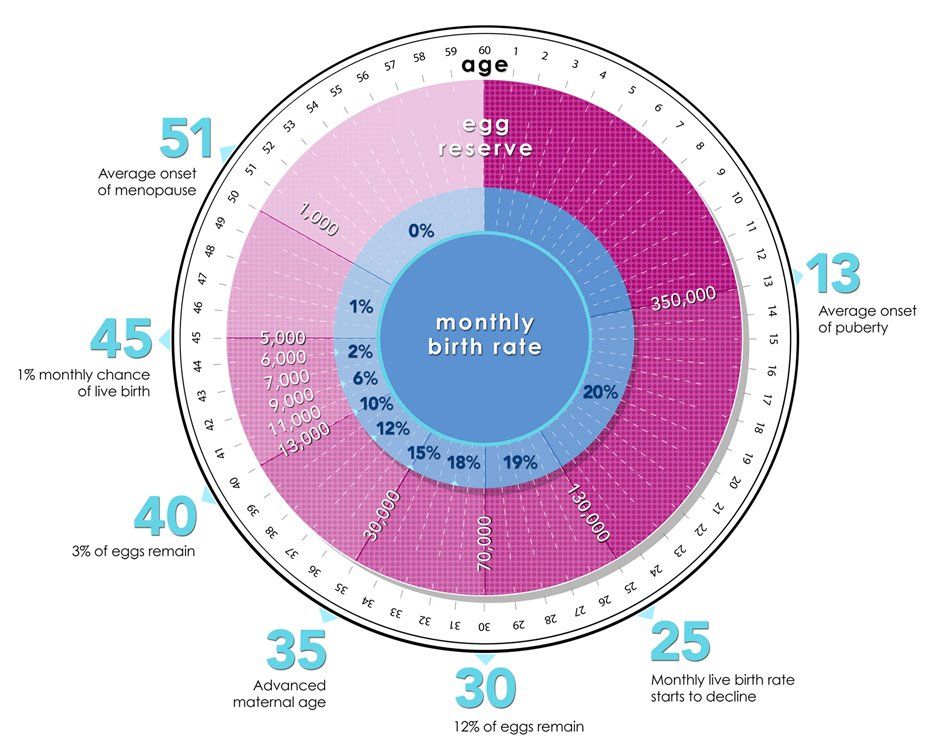 In medical practice, there are episodes when young pregnant women need obstetric care (a primipara is called young if she gave birth before the age of 18). Her pregnancy proceeds, undoubtedly, in unusual conditions associated with the immaturity of adaptive mechanisms.
In medical practice, there are episodes when young pregnant women need obstetric care (a primipara is called young if she gave birth before the age of 18). Her pregnancy proceeds, undoubtedly, in unusual conditions associated with the immaturity of adaptive mechanisms.
The heavy burden on the immature, immature body due to pregnancy is a serious test.
Pregnancy in girls under 8 years of age becomes possible in case of accelerated puberty. At the age of 9 to 16 years, pregnancy can occur even in cases where the dynamics of puberty is not ahead of the norm.
Classification of pregnancy. A distinction is made between pregnancy that occurred before puberty (violent ovulation occurs long before puberty) and pregnancy in a woman who has already entered puberty. In these two groups, the features of the course of pregnancy and childbirth and, of course, the tactics of their management differ significantly. In particular, during pregnancy and childbirth during puberty, there are fewer complications than at a younger age.
In addition, cases of pregnancy that occur in girls without signs of precocious puberty (on the one hand) and those who have them (on the other) are to be distinguished. With premature puberty, pregnancy often occurs with its true variant than with pathological (on the basis of a tumor, etc.).
The effect of pregnancy on a girl's body. There is no doubt that pregnancy, if it occurs at a young age, accelerates the processes of somatic and puberty. The secretion of estrogen and progesterone is not inferior to that of adult pregnant women.
Changes in the bone pelvis are especially evident, which during pregnancy in 13-15-year-olds can reach the size characteristic of 16-18 years old. However, the outer conjugate increases more slowly than the other outer dimensions. Of the young primiparous, 10.7% of births proceed in the presence of an anatomically narrowed pelvis; at the same time, to a greater extent than in adult women, hydrophilicity and elasticity of the ligamentous apparatus, symphysis and cartilaginous zones are expressed. All this provides some flexibility of the bone ring.
All this provides some flexibility of the bone ring.
We have to observe how in a girl without pronounced secondary sexual characteristics before pregnancy, they appear even if the pregnancy was terminated at an early date.
As for the mental reactions of young pregnant women, according to our observations, they correspond to age, but do not outstrip it. Psychopathies and psychoses are rare, mostly with rape (reactive psychosis). A number of character traits revealed in this group are explained by the shortcomings of education. So, after polling 79underage pregnant women, they stated the predominance of their independent character, a tendency to experiment, impracticality, poverty of the emotional world, bad manners.
Features of the course of pregnancy in adolescence. Pregnancy proceeds, as a rule, favorably. Its duration is 38 ± 0.9 weeks, i.e., slightly less than in adult women. Prematurity is 3%. Overlapping is almost not observed. Multiple pregnancy in young is less common (1: 100) than in older age groups.
Early toxicosis was diagnosed by us in isolated cases. Complication of pregnancy by late toxicosis is observed, according to our data, in 0.5%, which is 20 times less than usual. In the literature, there are completely different figures for the frequency of late toxicosis: 46-65.29%.
According to the opinion of the cited authors, pregnancy at a young age is generally complicated by 40-70%. This is significantly different from our data (no more than 5%), as well as from the opinion of W. Stockel, M. Shash and L. Kovacs (1967). Such a significant difference in the nature of the course of pregnancy is undoubtedly due to different tactics of management, in particular, regular medical supervision adopted in the IMMI clinic throughout pregnancy and carefully observed preventive hospitalization.
Diagnosis of early pregnancy. Diagnosis of pregnancy at a young age is based on the identification of the same supposed, probable and undoubted signs as in adult women, however, the diagnosis is often established with a delay, that is, with the appearance of precisely reliable signs.
The main obstacle to correct and timely diagnosis is the young pregnant woman herself, who, due to a number of circumstances, either does not suspect pregnancy or hides the appearance of dubious (subjective) signs of pregnancy. Sometimes a person whom the girl especially trusts learns about pregnancy for the first time: a school teacher, a pioneer leader, etc.
Often, the first diagnosis of pregnancy is made by the district pediatrician during examination and palpation of the abdomen.
Diagnostic errors in establishing pregnancy at a young age are a fairly common phenomenon. Even at the stage of acquaintance with the anamnesis, the assurances of the relatives accompanying the girl that "pregnancy is impossible here" lead to a medical error.
The integrity of the hymen or the absence of its integrity is not of decisive diagnostic value. Characteristically, in the first trimester of pregnancy, there is insufficient softening of the uterus, some lag in its size from the timing of the delay in menstruation, and a moderate severity of a group of probable signs based on ascertaining softening of the isthmus.
In addition to the generally accepted clinical diagnostic methods, one should not forget about the existence of such additional methods as the determination of placental lactogen, chorionic gonadotropin, abdominal radiography, ultrasound diagnostics, phono- and electrocardiography of the fetus.
In the process of differential diagnosis, it becomes necessary to distinguish pregnancy from the following diseases: anomalies in the development of the uterus, kidney prolapse, tumors of the small pelvis or abdominal cavity, obesity (often accompanied by amenorrhea), primary ectopic pregnancy (often in the right fallopian tube).
Pregnancy management. The very fact of establishing a pregnancy diagnosis imposes additional responsibility on the doctor for the fate of a young mother and her child. First of all, we have to resolve the issue of the possibility of carrying pregnancy and giving birth with minimal damage to health. The decision must be strictly individual. The age of the girl and the gestational age are decisive. Stereotypical decisions aimed at, say, unconditional termination of pregnancy can be harmful, as there are situations, especially in the second trimester, in which the risk associated with termination outweighs the health damage from the burden of pregnancy and childbirth.
The age of the girl and the gestational age are decisive. Stereotypical decisions aimed at, say, unconditional termination of pregnancy can be harmful, as there are situations, especially in the second trimester, in which the risk associated with termination outweighs the health damage from the burden of pregnancy and childbirth.
In healthy girls of 15-17 years of age in the first trimester, a positive decision on the issue of leaving the pregnancy is preferable, because pregnancy and childbirth are usually successful. At the same time, the risk of complications associated with induced abortion at a young age is greater than in adult women. In the presence of serious illnesses or the occurrence of complications that threaten health, an abortion is undertaken according to the relevant indications.
If a schoolgirl has a full term pregnancy, then school attendance is undesirable for ethical and pedagogical reasons. In addition, the study load adversely affects the formation of gestational dominance and can be an etiological moment in the development of late toxicosis of pregnant women. We must not forget that the need for frequent hospitalization also does not favor the continuation of studies.
We must not forget that the need for frequent hospitalization also does not favor the continuation of studies.
The girl is registered in the antenatal clinic and periodically (at least 3 times during pregnancy) goes to the antenatal department, where an in-depth monitoring of her health and the development of the fetus is carried out. Preventive or curative measures are taken as needed; in particular, foci of latent infection are eliminated and the vagina is sanitized. Particular attention in the hospital is given to physio-psycho-prophylactic preparation for childbirth, since this is difficult to implement in the antenatal clinic.
Given that at a young age, childbirth occurs 1-2 weeks earlier than in adult women, the last admission to the hospital should be made no later than 36-37 weeks of pregnancy. During this time, the next examination is carried out, preparations for childbirth are carried out and a plan for their maintenance is drawn up.
The course of childbirth. The course and outcomes of childbirth significantly depend on the girl's belonging to a certain age group. If at the age of 14 and younger the percentage of severe complications is high (15), then in the group of 15-17 years the percentage of complications decreases sharply (1-2).
The course and outcomes of childbirth significantly depend on the girl's belonging to a certain age group. If at the age of 14 and younger the percentage of severe complications is high (15), then in the group of 15-17 years the percentage of complications decreases sharply (1-2).
In parturient women under 14 years of age, the following structure of the main complications in childbirth can be outlined:
a) clinical discrepancy between the fetal head and the mother's pelvis,
b) weakness of labor activity,
c) injuries of the birth canal,
d) hypotonic bleeding (listed in descending order).
At the same time, in women in labor 15-17 years old, the structure of complications is somewhat different:
a) rapid delivery,
b) primary weakness of labor,
c) rupture of the cervix and perineum,
d) hypotonic bleeding.
Thus, most of the complications owe their genesis to a violation of the contractility of the uterus, due to both the immaturity of the regulatory links and the inferiority of the executive tissues (myometrium).
Birth management. Delivery of young pregnant women should be carried out in highly qualified institutions, preferably those with specialists with relevant experience and round-the-clock anesthesia and pediatric services. The doctor and midwife require a special approach to the young woman in labor, dictated by the need to reckon with the unusual position, emotional lability, low threshold of pain sensitivity and the constant threat of complications for the mother and fetus.
In the first stage of labor, in parallel with careful monitoring of the dynamics of structural changes in the cervix (external methods are preferred, for example, the Rogovin method), it is necessary to prescribe antispasmodic agents, thereby reducing pain.
The use of anesthesia is based on a sufficient choice of means. The widespread use of painkillers is not justified in cases where there is a high possibility of a clinical discrepancy between the fetal head and the mother's pelvis. For the same reasons, the appointment of strong uterine stimulants is contraindicated.
Surgical interventions among young women in labor are undertaken no more often than usual in clinical practice: perineotomy - in 12%, obstetric forceps - in 1%, caesarean section - in 0.5%. Vacuum extraction of the fetus is not used at all. Those authors who point to a high incidence of late toxicosis in young pregnant women, naturally, give a high percentage of operative delivery (17-22%).
In pregnant women under the age of 14 years (especially younger than 12), it is more likely than at an older age to tend to delivery by caesarean section in a planned manner at term 39-40 weeks. The determining circumstances are the size of the pelvis, the nature of the presentation, the estimated weight of the fetus and the state of health of the girl. 1-3 hours before the production of caesarean section, the fetal bladder is opened. This achieves gradual emptying of the uterus and, consequently, the prevention of hypotonic bleeding and lochiometers.
If the doctor has a hope for a spontaneous completion of labor, then at first he conducts labor conservatively; in the future, the appearance of complications makes it necessary to proceed with operative delivery. With modern anesthesia, a caesarean section poses no greater risk for a pregnant woman under 14 years of age than, for example, delivery per vias naturales or a fetus-destroying operation. In addition, during the abdominal surgery, it is possible to revise the pelvic organs, in particular, to assess the condition of the ovaries.
With modern anesthesia, a caesarean section poses no greater risk for a pregnant woman under 14 years of age than, for example, delivery per vias naturales or a fetus-destroying operation. In addition, during the abdominal surgery, it is possible to revise the pelvic organs, in particular, to assess the condition of the ovaries.
Transfer to the postpartum department after spontaneous delivery and examination of the soft birth canal is usually carried out not after 2-4 hours, but after 10-12 hours due to fear of not noticing the onset of hypotonic bleeding.
In the postpartum period, the issue of breastfeeding is solved in different ways, depending on the plans of the guardians, the adoptive parents of the child. In relation to women in childbirth under the age of 14 and older who refuse children, measures are taken to stop lactation. Subsequently, a visit by a girl to the same group of students, obviously, cannot be considered justified from a pedagogical point of view.
Thus, pregnancy imposes additional requirements on all organs and systems of a young pregnant woman, which, due to age characteristics, are in a state of functional stress. Our experience convinces us that careful monitoring of such pregnant women in a antenatal clinic and especially a hospital, timely and targeted correction of the observed deviations, as well as careful management of childbirth naturally reduce the number of complications.
Until what age can you get pregnant - the likelihood of conception, infertility
What do you know about your reproductive health? It turns out that there is a big difference between what most people say about this and the actual biological facts. This conclusion was made by researchers from the Reproductive Medicine Associates of New Jersey (RMANJ) after a survey of 1,000 Americans aged 18 to 40 years, conducted in March 2016.
Thus, 57% of respondents said that a woman's "biological clock" "stops" at the age of 44. This is partly true: only some 44-year-old women can become pregnant naturally. But in fact, fertility declines over the course of 20 years, almost throughout adulthood, especially after 35 years.
This is partly true: only some 44-year-old women can become pregnant naturally. But in fact, fertility declines over the course of 20 years, almost throughout adulthood, especially after 35 years.
If before the age of 31, three-quarters of women can become pregnant within a year, after 35 years, only half. At 44, this figure drops to 1-5%, and only in 2% of cases the child will receive completely normal chromosomes from the mother.
"Biological clock" that stops "ticking" is not quite a correct comparison, but, indeed, the fact is that the chances of pregnancy in women after 40 years of age are greatly reduced.
Other similar surveys have been conducted in the past. For example, researchers at the Royal College of Obstetricians and Gynaecologists in the UK asked 1,000 young men and women aged 16 to 24 about fertility. More than 80% of respondents claimed that female reproductive function begins to decline only after the age of 35, which, as we have already noted, is actually not the case: the decline begins much earlier, it just increases strongly by the age of 35. Among young people, 25% said that female fertility decreases only after the age of 40; among girls, 16% gave a similar answer.
Among young people, 25% said that female fertility decreases only after the age of 40; among girls, 16% gave a similar answer.
Another 2016 survey by the Fertility Centers of Illinois found that among women aged 25-45 who had never given birth, less than half (48%) understood that the chances of having a child decreased with age, the risk increased abortion and chromosomal abnormalities.
If we turn to the results of earlier studies, we will see that over the past few years, people's opinion about the effect of age on the state of reproductive function has changed little.
In 2011, experts from the biopharmaceutical company EMD Serono assessed the fertility knowledge of 1,010 women aged 25 to 35 who had never planned or become pregnant before. Many of them wanted to have a child after 30, and 73% of those surveyed rated their chances as higher than is the case in reality. At the age of 35-44, every fourth woman experiences problems with conception, while up to 30 years - only every tenth.
Researchers from EMD Serono noted that only a third of the respondents correctly identified age as an important factor influencing fertility. Many hoped that as soon as they want to have a baby, it will happen in the first month with a probability of 10-40%. In fact, this figure is only 10%.
In addition, the respondents strongly overestimated the possibilities of in vitro fertilization. They said that after IVF, pregnancy will occur with a probability of 50-59%, although in reality the effectiveness of the method ranges from 20 to 29%. Many respondents did not know that the “age” of the egg also plays an important role. 54% of women were confident that IVF would help them get pregnant, regardless of the age at which their eggs were retrieved.
Where do women get such erroneous knowledge about their reproductive health? How many discuss these issues with gynecologists? It turns out that not all.
In the RMANJ survey, only 26% of women said they had talked to their gynecologists about the effect of age on fertility. Nearly half (42%) of the women who experienced infertility reported that gynecologists had never talked to them about fertility.
Nearly half (42%) of the women who experienced infertility reported that gynecologists had never talked to them about fertility.
Researchers at EMD Serono got similar results. 52% of women did not have conversations with gynecologists about their plans for pregnancy in the future, 78% - about age as a factor affecting fertility, 89-96% - about infertility treatment methods.
And this is not because women themselves do not want such conversations. In a survey by the Illinois Fertility Center, 89% of respondents agreed that gynecologists should talk to patients about reproductive health and infertility, 52% of women 35 and older said they would change their pregnancy plans if they knew that with age, the chances on its offensive are reduced.
Why don't gynecologists talk about this with their patients?
Experts note that doctors often simply do not have time, but this is not the only reason. The topic of fertility and infertility is highly stigmatized. Many doctors are uncomfortable discussing this with their patients. And the woman herself often cannot ask the right questions, because she does not have the necessary information.
Many doctors are uncomfortable discussing this with their patients. And the woman herself often cannot ask the right questions, because she does not have the necessary information.
Some modern experts believe that fertility issues should be discussed with girls starting in high school. For example, the chairman of the British Fertility Society (British Fertility Society) Adam Balen openly advocates the concept of "choice, not chance." He notes:
Our goal is for sex education courses to cover not only contraception and protection against sexually transmitted diseases, but also fertility, planning the optimal time to start a family. We want young people to make informed choices about pregnancy planning.
Many topics related to fertility and infertility are taboo in today's society. For example, the topic of “freezing” eggs is a procedure that gives a woman the opportunity to preserve her germ cells while she is young in order to increase the chances of pregnancy and the birth of a healthy child in the future.