When does a baby start to turn head down
Symptoms of Baby Turning Head Down
Your baby kicks, squirms, and flips all day (and night!). But what exactly are they doing in there?
Well, toward the end of your pregnancy, your baby will likely get into a head-down position so that they can begin their descent into the birth canal. The exact timing of when your baby hits this position is individual. And some babies prefer other positions, like breech (head up) or transverse (side lying).
Regardless, some signs can serve as clues about how baby’s relaxing in there. Here’s more about when your baby will move head down, what the options are if they stay head up or in another position, and what to feel for when trying to determine your baby’s position at home.
Related: What Sleeping Position Will Help Turn My Breech Baby?
Most babies tend to shimmy their way into a cephalic (head-first) presentation before birth.
Fast fact
At 28 weeks, around 25 percent of babies are breech (head up), but this number jumps down to just 3 or 4 percent at term.
Your baby may move all over the place in the first and second trimesters. Their position may change wildly early on in the third trimester as well.
However, if you’re between 32 and 36 weeks, you may notice your baby staying put in a head-down position. Your uterus grows to accommodate their size — but there’s only so much room. As time passes, your baby gets bigger and starts to run out of space to move into different positions.
Related: The Third Trimester of Pregnancy: Concerns and Tips
Being head down is just half of the equation when it comes to birth. There’s also the matter of which way your baby is facing.
Why does this make a difference? It comes down to geometry. Your baby’s head must fit through the pelvis on its way into the vaginal canal for delivery. Some positions make this journey easier than others, especially considering how different parts of your baby’s skull are wider and narrower than others.
- Occiput anterior: This position is the most common.
 It means that your baby is head down with their back against your stomach and their chin tucked into their chest.
It means that your baby is head down with their back against your stomach and their chin tucked into their chest. - Occiput posterior: This position means that your baby is head down but facing the opposite direction. In this position, your baby’s back is at your back.
Anterior is the ideal position for an uncomplicated vaginal delivery. When your baby’s chin is tucked, it helps the narrowest part of their head go through the birth canal. Posterior presentation can mean a longer or potentially more difficult delivery, sometimes requiring a vacuum, forceps, or cesarean section.
If your baby is posterior even in early labor, they may still turn throughout the process as contractions move them around in the womb. Some babies completely spin to an anterior position during labor while others are born posterior.
Related: What Your Baby’s Position in the Womb Means
You may not experience any signs that your baby has flipped into a head-down position. There’s really no easy way to tell just by looking at your bump. You need to get in there and feel around. But how?
There’s really no easy way to tell just by looking at your bump. You need to get in there and feel around. But how?
Fortunately, your doctor or midwife is trained to feel for your baby’s position using what are called Leopold’s maneuvers.
With this technique, your provider will feel for what part of your baby is presenting in the pelvis, then for your baby’s back, and then for what part of your baby is in your fundus (up high, near your rib cage). They’ll also feel around for your baby’s cephalic prominence, which simply means which way your baby is facing.
With a head-down presentation:
- baby’s head would be in your pelvis
- baby’s back position would depend on whether baby is anterior/posterior, but generally baby will have either their back to your belly (anterior) or your back (posterior)
- baby’s bottom/legs would be in your fundus
All these findings can also be confirmed via ultrasound to give you the clearest picture.
But how can you figure out your baby’s position at home? Pay close attention to the shapes in your belly, as well as the different movements you feel.
Your baby may be head down if you can:
- feel their head low down in your belly
- feel their bottom or legs above your belly button
- feel larger movements — bottom or legs — higher up toward your rib cage
- feel smaller movements — hands or elbows — low down in your pelvis
- feel hiccups on the lower part of your belly, meaning that their chest is likely lower than their legs
- hear their heartbeat (using an at-home doppler or fetoscope) on the lower part of your belly, meaning that their chest is likely lower than their legs
Belly mapping
It can be difficult to read the different lumps and bumps you feel on your stomach. With practice, you may start to understand what you’re feeling. You might even try belly mapping — a process to estimate baby’s position. It was created by Gaily Tully, certified professional midwife and author of SpinningBabies.com.
To use this technique, wait until you are at least 30 weeks pregnant. You may even want to try belly mapping following a prenatal appointment so your doctor can give you some guidance on baby’s position.
You may even want to try belly mapping following a prenatal appointment so your doctor can give you some guidance on baby’s position.
Lie down in bed or on the couch. Using a washable marker or finger paint, gently mark where you feel your baby’s head (it feels like a small bowling ball). The arms and hands are likely near the head, and their tiny movements give them away.
Then feel for the back, butt, and legs, as well as larger movements. You may find it helpful to use a baby doll to play with different possible positions. You can then lightly draw or paint your baby on your stomach to help you visualize how they’re lying.
Related: Can You Give Birth with Baby in the Vertex Position?
If you’re in late pregnancy and have concerns about your baby’s positioning, ask your doctor about it at your next prenatal appointment. Chances are that your healthcare provider is making a note of your baby’s position as well.
If your baby is breech or in some other position besides head down, there are several options for delivery. Factors at play here include:
Factors at play here include:
- whether your baby stays in a certain position as you reach term
- any other pregnancy complications you might have
- when you end up going into labor naturally
Wait-and-see approach
Again, your baby’s position isn’t usually a big concern until you reach between 32 and 36 weeks in your pregnancy. Before that point, the fluid in the uterus gives your baby plenty of space to move around. As you get closer to delivery and your baby hasn’t settled head down, they start to run out of room to make the switch.
Your doctor can monitor your baby’s position at your prenatal appointments by feeling your belly for where their head, back, and buttocks are. To confirm, you may also have an ultrasound or pelvic exam.
External cephalic version (ECV)
External cephalic version (ECV) is a procedure during which your doctor tries to move your baby into a head-down position to increase the chance you’ll have a vaginal birth. This is done in a setting in which baby can be monitored and you can have an emergency cesarean section (C-section) if needed.
This is done in a setting in which baby can be monitored and you can have an emergency cesarean section (C-section) if needed.
Your provider uses their hands to manually turn the baby head down. If you’ve reached 36 weeks and your baby still isn’t head down, your doctor may suggest an ECV.
The success rate of this procedure is around 58 percent. While that’s not a super impressive statistic, ECV may be worth a try if delivering vaginally is important to you.
It’s also worth noting that some babies that are flipped return to a breech position. You can have a repeat ECV, but space runs out the closer you get to birth, so it may be more difficult the second time.
Cesarean delivery (C-section)
A C-section is another option for delivering babies who aren’t head down. It involves major surgery that you may schedule ahead of time (if you know your baby isn’t head down) or that can be performed in the event you go into labor naturally.
Around 85 percent of breech babies are born via C-section. While this surgery is routine, it involves some risks, including:
While this surgery is routine, it involves some risks, including:
- infection
- postpartum hemorrhage
- blood clots
- issues with future pregnancies, like a risk of placenta previa or uterine rupture
Vaginal birth
The American College of Obstetricians and Gynecologists explains that some women may be candidates for a vaginal birth even if their babies are breech. This possibility is determined on a case-by-case basis and involves a review of your medical history and weighing the benefits of vaginal delivery versus the risks of C-section.
If you choose to go this route, you’ll need to follow any specific guidelines set up by your hospital or birth center.
Related: Midwives Are Growing in Popularity: Here’s What You Need to Know
Your baby moves a lot throughout your pregnancy. As you get closer to your due date, they’ll likely settle into a head-down position as they get ready for birth.
If you have concerns about your baby’s position, don’t hesitate to bring them up at your next prenatal appointment. Your healthcare provider is also keeping tabs on whether baby is head down and can help guide you with options for repositioning or an alternate birth plan, if necessary. You’ve got this, mama!
Your healthcare provider is also keeping tabs on whether baby is head down and can help guide you with options for repositioning or an alternate birth plan, if necessary. You’ve got this, mama!
Symptoms of Baby Turning Head Down
Your baby kicks, squirms, and flips all day (and night!). But what exactly are they doing in there?
Well, toward the end of your pregnancy, your baby will likely get into a head-down position so that they can begin their descent into the birth canal. The exact timing of when your baby hits this position is individual. And some babies prefer other positions, like breech (head up) or transverse (side lying).
Regardless, some signs can serve as clues about how baby’s relaxing in there. Here’s more about when your baby will move head down, what the options are if they stay head up or in another position, and what to feel for when trying to determine your baby’s position at home.
Related: What Sleeping Position Will Help Turn My Breech Baby?
Most babies tend to shimmy their way into a cephalic (head-first) presentation before birth.
Fast fact
At 28 weeks, around 25 percent of babies are breech (head up), but this number jumps down to just 3 or 4 percent at term.
Your baby may move all over the place in the first and second trimesters. Their position may change wildly early on in the third trimester as well.
However, if you’re between 32 and 36 weeks, you may notice your baby staying put in a head-down position. Your uterus grows to accommodate their size — but there’s only so much room. As time passes, your baby gets bigger and starts to run out of space to move into different positions.
Related: The Third Trimester of Pregnancy: Concerns and Tips
Being head down is just half of the equation when it comes to birth. There’s also the matter of which way your baby is facing.
Why does this make a difference? It comes down to geometry. Your baby’s head must fit through the pelvis on its way into the vaginal canal for delivery. Some positions make this journey easier than others, especially considering how different parts of your baby’s skull are wider and narrower than others.
- Occiput anterior: This position is the most common. It means that your baby is head down with their back against your stomach and their chin tucked into their chest.
- Occiput posterior: This position means that your baby is head down but facing the opposite direction. In this position, your baby’s back is at your back.
Anterior is the ideal position for an uncomplicated vaginal delivery. When your baby’s chin is tucked, it helps the narrowest part of their head go through the birth canal. Posterior presentation can mean a longer or potentially more difficult delivery, sometimes requiring a vacuum, forceps, or cesarean section.
If your baby is posterior even in early labor, they may still turn throughout the process as contractions move them around in the womb. Some babies completely spin to an anterior position during labor while others are born posterior.
Related: What Your Baby’s Position in the Womb Means
You may not experience any signs that your baby has flipped into a head-down position.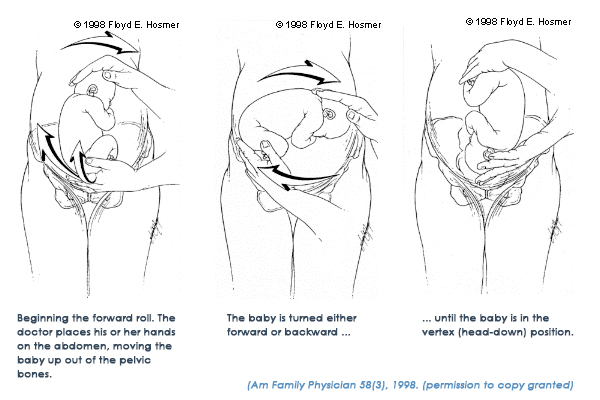 There’s really no easy way to tell just by looking at your bump. You need to get in there and feel around. But how?
There’s really no easy way to tell just by looking at your bump. You need to get in there and feel around. But how?
Fortunately, your doctor or midwife is trained to feel for your baby’s position using what are called Leopold’s maneuvers.
With this technique, your provider will feel for what part of your baby is presenting in the pelvis, then for your baby’s back, and then for what part of your baby is in your fundus (up high, near your rib cage). They’ll also feel around for your baby’s cephalic prominence, which simply means which way your baby is facing.
With a head-down presentation:
- baby’s head would be in your pelvis
- baby’s back position would depend on whether baby is anterior/posterior, but generally baby will have either their back to your belly (anterior) or your back (posterior)
- baby’s bottom/legs would be in your fundus
All these findings can also be confirmed via ultrasound to give you the clearest picture.
But how can you figure out your baby’s position at home? Pay close attention to the shapes in your belly, as well as the different movements you feel.
Your baby may be head down if you can:
- feel their head low down in your belly
- feel their bottom or legs above your belly button
- feel larger movements — bottom or legs — higher up toward your rib cage
- feel smaller movements — hands or elbows — low down in your pelvis
- feel hiccups on the lower part of your belly, meaning that their chest is likely lower than their legs
- hear their heartbeat (using an at-home doppler or fetoscope) on the lower part of your belly, meaning that their chest is likely lower than their legs
Belly mapping
It can be difficult to read the different lumps and bumps you feel on your stomach. With practice, you may start to understand what you’re feeling. You might even try belly mapping — a process to estimate baby’s position. It was created by Gaily Tully, certified professional midwife and author of SpinningBabies.com.
To use this technique, wait until you are at least 30 weeks pregnant. You may even want to try belly mapping following a prenatal appointment so your doctor can give you some guidance on baby’s position.
You may even want to try belly mapping following a prenatal appointment so your doctor can give you some guidance on baby’s position.
Lie down in bed or on the couch. Using a washable marker or finger paint, gently mark where you feel your baby’s head (it feels like a small bowling ball). The arms and hands are likely near the head, and their tiny movements give them away.
Then feel for the back, butt, and legs, as well as larger movements. You may find it helpful to use a baby doll to play with different possible positions. You can then lightly draw or paint your baby on your stomach to help you visualize how they’re lying.
Related: Can You Give Birth with Baby in the Vertex Position?
If you’re in late pregnancy and have concerns about your baby’s positioning, ask your doctor about it at your next prenatal appointment. Chances are that your healthcare provider is making a note of your baby’s position as well.
If your baby is breech or in some other position besides head down, there are several options for delivery. Factors at play here include:
Factors at play here include:
- whether your baby stays in a certain position as you reach term
- any other pregnancy complications you might have
- when you end up going into labor naturally
Wait-and-see approach
Again, your baby’s position isn’t usually a big concern until you reach between 32 and 36 weeks in your pregnancy. Before that point, the fluid in the uterus gives your baby plenty of space to move around. As you get closer to delivery and your baby hasn’t settled head down, they start to run out of room to make the switch.
Your doctor can monitor your baby’s position at your prenatal appointments by feeling your belly for where their head, back, and buttocks are. To confirm, you may also have an ultrasound or pelvic exam.
External cephalic version (ECV)
External cephalic version (ECV) is a procedure during which your doctor tries to move your baby into a head-down position to increase the chance you’ll have a vaginal birth. This is done in a setting in which baby can be monitored and you can have an emergency cesarean section (C-section) if needed.
This is done in a setting in which baby can be monitored and you can have an emergency cesarean section (C-section) if needed.
Your provider uses their hands to manually turn the baby head down. If you’ve reached 36 weeks and your baby still isn’t head down, your doctor may suggest an ECV.
The success rate of this procedure is around 58 percent. While that’s not a super impressive statistic, ECV may be worth a try if delivering vaginally is important to you.
It’s also worth noting that some babies that are flipped return to a breech position. You can have a repeat ECV, but space runs out the closer you get to birth, so it may be more difficult the second time.
Cesarean delivery (C-section)
A C-section is another option for delivering babies who aren’t head down. It involves major surgery that you may schedule ahead of time (if you know your baby isn’t head down) or that can be performed in the event you go into labor naturally.
Around 85 percent of breech babies are born via C-section. While this surgery is routine, it involves some risks, including:
While this surgery is routine, it involves some risks, including:
- infection
- postpartum hemorrhage
- blood clots
- issues with future pregnancies, like a risk of placenta previa or uterine rupture
Vaginal birth
The American College of Obstetricians and Gynecologists explains that some women may be candidates for a vaginal birth even if their babies are breech. This possibility is determined on a case-by-case basis and involves a review of your medical history and weighing the benefits of vaginal delivery versus the risks of C-section.
If you choose to go this route, you’ll need to follow any specific guidelines set up by your hospital or birth center.
Related: Midwives Are Growing in Popularity: Here’s What You Need to Know
Your baby moves a lot throughout your pregnancy. As you get closer to your due date, they’ll likely settle into a head-down position as they get ready for birth.
If you have concerns about your baby’s position, don’t hesitate to bring them up at your next prenatal appointment. Your healthcare provider is also keeping tabs on whether baby is head down and can help guide you with options for repositioning or an alternate birth plan, if necessary. You’ve got this, mama!
Your healthcare provider is also keeping tabs on whether baby is head down and can help guide you with options for repositioning or an alternate birth plan, if necessary. You’ve got this, mama!
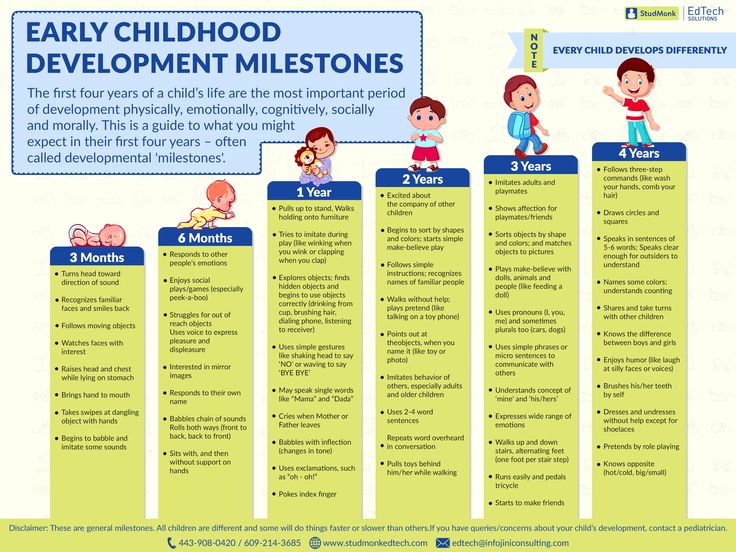
Child under 1 year old.
We would like to note that children are all different and develop in different ways. This article is intended for your reference and gives approximate norms for the degree of formation of the mental processes of your child at this age. You can check his potential in different areas of knowledge, find out in which areas of knowledge your child succeeds, and in which additional attention and time are required.
We also want to note that the sooner you begin to develop logical thinking, which is based on the child's feelings and perceptions, the higher will be the level of his cognitive activity.
1 month
What your child should be able to do:
1. Lying on the stomach on a flat surface, raise the head for a short time
2.Focus on the face
3. Respond to communication with him - stop crying, concentrate on the adult
4. In the position on the stomach, raise the head and try to hold it
5. Make sounds other than crying (e.g. gurgle)
6. Smile when you smile
7. Clench your hands into fists and bring them to your mouth
2 months
What your child should be able to do:
1. Smile in response to your smile
2. Lying on stomach, raise head 45°
3. Hold inserted toy in hand
4. Reach for objects
5. Laugh out loud; - squeal with delight
6. Turn your head towards the sound source
3 months
What your child should know:
1. In prone position, can pull up on elbows and hold elevated shoulders and head for 10 seconds
2. Liven up when communicating with adults, cooing
3. Smiling distractedly
4. Resting feet on a hard surface with support under the armpits
5.Responding to the presence of parents: trying to attract attention
6. Searching for the source of the sound with the eyes while turning the head
7 Follow moving objects and look at them for a long time
4 months
What your child should know:
1. Lying on stomach, raise head 90°
2. Raise shoulders and head while lying on back
3. Laugh out loud
4. When pulling the handles, bend your elbows and pull yourself up.
5. Say the first syllables
6. Reach for the toy, put everything in your mouth
5 months
What your child should know:
1. Keep head firmly upright
2. Roll over (to one side)
3. Pay attention to a very small object
4. "Sing" sounds, changing intonation
5. Pull up on hands, trying to sit up
6. Shift object from one hand to another
7. Pull a small object towards you and hold it in your fist
8.Babbling, pronouncing various combinations of vowels and consonants
9. Be able to hold a bottle with one or both hands
6 months
What your child should know:
1. Pronounce some vowels and consonants or combinations of them
2. Sit with support for a short time
3. Try to crawl on your stomach
4. Sit down on your own from a position on your stomach
5. Roll over from your stomach to your back
6. Respond to one's name
7. Make a variety of sounds
7 months
What your child should know:
1. Sit without support
2. Climb on all fours and crawl
3. Understand what “no” means by the tone of your voice
4. Play “coo-coo” (by 7 months and ¼ of a month)
5. Keep in each hand on an object (may hit them together)
6. Pick up a small object with thumb and forefinger
8 months
What your child should be able to do:
1.Play while sitting (may sometimes “fall over” on the side)
2. Pick up a small object from the surface with thumb and forefinger
3. Indistinctly pronounce "mom" or "dad"
4. Stand up independently, holding on to a support
5. Understand the word "no", wave bye bye, clap your hands
6. Play with objects for a long time
9 months
What your child should know:
1. Flipping thick pages of a cardboard book
2. Play ball (roll it back to you)
3. Drink from a cup without help
4. Say "dad" or "mum" clearly
5. Respond with a gesture to a short command, such as "Give it to me"
6 Move around holding on to a support
7. Sit well, lie down from a sitting position and sit down from a lying position
8. Find a toy hidden in front of him
9. Know and respond to his own name
10 months
What your child should know:
1.Standing unsupported, but not for long, walking with both hands
2. Objecting if you try to take a toy away from him
3. Sit down from a standing position
4. Imitate gestures, facial expressions, sounds
5. Use baby jargon (babble that sounds like the Child is talking in a foreign language of his own making)
6. Respond with a gesture to a short command, such as "give it to me"
7. Perform complex movements, open, close, assemble a pyramid, show parts of the body of another person
11 months
What your child should know:
1. Stand and walk independently
2. Pick up a small object from the surface with any part of the thumb and forefinger (by 10 months and 1/4 month)
3. Understand the word "don't" (but not always obey)
4. Express their desires in a way other than crying
5. Saying 3 (or more) words other than "mom" or "dad"
6. Knowing the names of many objects
12 months
What your child should know:
1.Understand the word "no"
2. Fulfill simple requests
3. Know his name
4. Walk well, sit down, stand up, stand
5. Say 10 or more words, except for "mom", "dad"
6. Play "Magpie-Crow", assemble a pyramid, build 2-3 figures from blocks
7. Actively draw scribbles with a pencil or crayons
8. Recognize objects in the picture
9. Bite, chew solid food
10. Use a spoon and cup
11. Be independent
Breech presentation - how to turn the baby
Vatagina Maria Alexandrovna
Obstetrician-gynecologist
Lapino-1 Clinical Hospital "Mother and Child"
Do not worry and worry if a child under 36 weeks is "ass forward": this is completely normal and the crumbs still have time to roll over. By the way, it happens that the baby turns upside down and immediately before the birth, and even in the birth itself
Try to get the baby to turn into the desired position. Tell everything in detail: why he should turn around, what it will give both mother and child in childbirth. You can talk out loud, or you can talk to yourself, the main thing is to talk to the baby about it all the time
You can talk out loud, or you can talk to yourself, the main thing is to talk to the baby about it all the time
In the water, the mother’s body relaxes, which means that the muscles of the uterus relax, its volume increases somewhat, and as a result, the child has a little more space “for maneuvers ".
Talk to him
There is always a connection between a child and a mother. And mother is the first person whom the baby believes and obeys. Therefore, try to persuade the baby to turn into the desired position. Tell everything in detail: why he should turn around, what it will give both mother and child in childbirth. You can talk out loud, or you can talk to yourself, the main thing is to talk to your baby about it all the time. Be gentle and at the same time persistent. Be sure to connect the future dad to the conversation, children obey men even more. When you persuade the baby, additionally stroke the stomach, as if instructing the child how to turn around. Great option: dad talks and strokes his stomach with you.
Great option: dad talks and strokes his stomach with you.
Imagine
Visualization - a way in which a person imagines the picture he wants. So the expectant mother just needs to imagine the baby in the right position. If you don't know what it looks like or you just can't imagine a baby in your belly - find a beautiful photo from a magazine, book, Internet. Some kind of anatomical accuracy is not important here, just a pleasant and understandable picture is enough: the baby lies upside down inside the mother's belly. Look at the illustration more often and imagine that inside you the baby is also in the correct position. But you must not only look at someone else's photo, but imagine yourself and your child.
Lure him
Another way is to lure the baby. Children, especially small ones, are very curious, so make the baby turn around by showing him something interesting. But the baby is still in the stomach, how can he see something? We do not know exactly how the baby reacts to the world outside the mother's stomach, but it is believed that he, for example, can hear sounds. Place headphones with pleasant music in the lower abdomen, this can also encourage the child to turn towards the sound. Music should be calm, melodic and not loud so that the baby is not scared.
Place headphones with pleasant music in the lower abdomen, this can also encourage the child to turn towards the sound. Music should be calm, melodic and not loud so that the baby is not scared.
You can also turn on the flashlight and put it against the mother's stomach in the place where the baby's head is, and then, while talking, slowly move the flashlight to the side and down, dragging the baby along with you.
Swim and relax
Swimming also helps your baby get into head presentation. In the water, the mother’s body relaxes, which means that the muscles of the uterus also relax, its volume increases somewhat, and as a result, the child has a little more space “for maneuvers”. But swimming should be pleasant for mom, if a woman is afraid of water or she is not warm enough, then there will be no relaxation. Therefore, you must want to swim, plus the water must be at a comfortable temperature.
Do the exercises
There are very simple exercises , that will help the baby to fit correctly. But first, check with your doctor if you can do such exercises. Gymnastics to turn the baby into head presentation is not carried out if there is gestosis, the threat of termination of pregnancy, a scar on the uterus after a previous cesarean section, placenta previa.
But first, check with your doctor if you can do such exercises. Gymnastics to turn the baby into head presentation is not carried out if there is gestosis, the threat of termination of pregnancy, a scar on the uterus after a previous cesarean section, placenta previa.
Turns. Lying on the couch, turn from side to side 3-4 times in 10 minutes. Perform 3 times a day. The turn usually occurs within the first week.
Force of attraction. Lie on your back with a large pillow under your lower back and a small one under your head. Bend your knees, placing your feet on the floor. Lie like this for 10 minutes.
Knee-elbow position. Get on your knees and elbows, at this time the pelvis is located above the head. Stay in this position for 15 minutes several times a day.
Consult a specialist
If exercises and psychological methods do not work, there is another way – prophylactic external rotation performed by an experienced obstetrician-gynecologist in the maternity hospital. First, the mother is injected with drugs that relax the uterus, then the doctor tries to turn the child with certain hand movements, acting on his head and pelvis through the belly of the expectant mother. All this takes place under the control of ultrasound, and usually a woman does not experience any discomfort during this manipulation.
First, the mother is injected with drugs that relax the uterus, then the doctor tries to turn the child with certain hand movements, acting on his head and pelvis through the belly of the expectant mother. All this takes place under the control of ultrasound, and usually a woman does not experience any discomfort during this manipulation.
True, external rotation is now rarely performed: firstly, not all obstetricians and gynecologists can do it, and not all doctors believe that it is needed; secondly, not every woman is psychologically tuned in to him, and, besides, there are not always indications for him.
Psychological methods may seem questionable, but they often help. And if you add gymnastics and swimming, then the likelihood that the baby will turn into the correct position only increases. So if you don’t want to do a cesarean section with a breech presentation or give birth “ass first”, then you should try all the methods that are suitable and allowed for you.