Tension headaches while pregnant
What Causes Them and What You Can Do
If you’re pregnant and having headaches, you’re not alone. A medical review reports that 39 percent of pregnant and postpartum women have headaches.
Though during pregnancy you may have a different kind of headache than you usually do, most headaches during pregnancy aren’t harmful.
Headache pain during the first trimester of pregnancy may happen for different reasons than headaches in the second or third trimester. In some cases, headache pain may be a sign of other health problems during pregnancy.
Tell your doctor about any headache you have during, before, and after pregnancy. Keep a journal to record how often you have headaches and how serious the pain is. Additionally, record any other symptoms you have.
Most headaches during pregnancy are primary headaches. This means that the headache pain happens by itself. It’s not a sign or symptom of another disorder or a complication in the pregnancy. Primary headaches include:
- tension headaches
- migraine attacks
- cluster headaches
About 26 percent of headaches during pregnancy are tension headaches. Tell your doctor if you have chronic headaches or migraine during pregnancy or if you have a history of migraine.
Some women with a history of migraine get fewer migraine attacks during pregnancy. Migraine has also been linked to complications that happen later in pregnancy or after the birth of your baby.
Secondary headaches are a caused by a complication in the pregnancy, such as high blood pressure.
Headache pain may vary from one person to the next. You may have:
- dull ache
- throbbing or pulsating pain
- severe pain on one or both sides
- sharp pain behind one or both eyes
Migraine pain may also include:
- nausea
- vomiting
- seeing lines or flashes of light
- blind spots
First trimester
Tension headaches are common in the first trimester of your pregnancy. This may happen because your body is undergoing several changes at this time. These changes may trigger headache pain:
- hormonal changes
- higher blood volume
- weight changes
Common causes of headache pain during the first trimester of pregnancy also include:
- dehydration
- nausea and vomiting
- stress
- lack of sleep
- caffeine withdrawal
- poor nutrition
- low blood sugar levels
- too little physical activity
- sensitivity to light
- changes in vision
Some foods may also cause headaches. Your trigger foods may change during pregnancy. Common foods that may cause headaches in some people include:
Your trigger foods may change during pregnancy. Common foods that may cause headaches in some people include:
- dairy
- chocolate
- cheese
- yeast
- tomatoes
Second and third trimester
Headaches during your second and third trimester may have different causes. These include:
- extra weight
- posture
- too little sleep
- diet
- muscle strain and tightness
- high blood pressure
- diabetes
High blood pressure
Headaches during your second or third trimester of pregnancy may be a sign that you have high blood pressure. About 6 to 8 percent of pregnant women ages 20 to 44 in the United States have high blood pressure.
The Centers for Disease Control and Prevention (CDC) warns that this treatable condition can cause serious complications for both mother and baby. This is most common after week 20 of pregnancy.
If you’re pregnant, high blood pressure can raise the risk of:
- stroke
- preeclampsia
- eclampsia
- low oxygen flow to the baby
- preterm delivery, before 37 weeks
- placental abruption
- low baby birth weight, which is less than 5 pounds, 8 ounces
Treatment for hypertension during pregnancy
Your doctor may prescribe medication to treat your high blood pressure. You’ll also need to cut down on salt and add more fiber to your daily diet. Regular exercise is also very important to help balance your blood pressure.
You’ll also need to cut down on salt and add more fiber to your daily diet. Regular exercise is also very important to help balance your blood pressure.
Other causes of headache during pregnancy include common infections and more serious illnesses:
- sinus infection
- low blood pressure
- blood clots
- bleeding
- sickle cell anemia
- brain tumor
- aneurysm
- stroke
- heart conditions
- meningitis or encephalitis
Talk to your doctor before taking your regular headache pain medication during pregnancy. Don’t take aspirin and ibuprofen (Advil, Motrin etc.).
The CDC warns that these pain relief drugs can be harmful to your growing baby, especially if taken during the first trimester. Many women may take acetaminophen (Tylenol) during pregnancy. However, some studies suggest there may be effects from taking acetaminophen as well.
Your doctor can recommend alternative medications to treat headache during pregnancy and natural headache remedies, such as:
- drinking plenty of water
- rest
- ice pack
- heating pad
- massage
- exercise and stretching
- essential oils, such as peppermint, rosemary, and chamomile
When to see your doctorSee your doctor if you have any headache pain at all during pregnancy.
Get urgent medical attention if you have:
- fever
- nausea and vomiting
- blurred vision
- severe pain
- headache that lasts longer than a few hours
- frequent headache pain
- fainting
- seizure
Your doctor may recommend tests and scans to find out the cause of your headaches. These include:
- checking your blood pressure
- blood test
- blood sugar test
- vision test
- ultrasound of the head and neck
- heart or head scan
- checking eye health with a scope
- spine puncture
Headache pain during pregnancy is common. You may have tension headaches during your first trimester of pregnancy. This may happen because of the many changes that you’re going through in a short period.
Headache pain may happen in the second and third period of your pregnancy for other reasons. Some causes of headaches in your mid to late pregnancy may be serious.
High blood pressure is a serious cause of headache pain during pregnancy. You can have high blood pressure at any time in your pregnancy. You may not have any symptoms at all. Check your blood pressure at least once a day with a home monitor.
You can have high blood pressure at any time in your pregnancy. You may not have any symptoms at all. Check your blood pressure at least once a day with a home monitor.
Tell your doctor if you have headaches at any time in your pregnancy. Let your doctor know right away if you have a personal or family history of migraine, high blood pressure, seizures or diabetes.
Take all medications and treatment exactly as prescribed by your doctor. Follow all diet and exercise advice carefully. See your doctor for all follow-up and regular check-ups. Most causes of headaches during pregnancy are treatable or preventable with the right care.
For more pregnancy guidance and weekly tips tailored to your due date, sign up for our I’m Expecting newsletter.
Pregnancy and Headaches: When Should I Worry?
Pregnancy is a beautiful thing to be celebrated, but few people fill you in on the not-so-great symptoms that may occur during the journey. Namely, heartburn, gas, constipation and, for some pregnant mamas, headaches.
While headaches can be just another normal symptom of pregnancy, should they ever be a cause for concern?
“Headaches are common in women both in and outside of pregnancy,” said Kelley Saunders, MD, an OBGYN with Banner – University Medicine Women’s Institute. “But whether they are normal or not should always be discussed with your doctor."
Here is some insight into what causes headaches during pregnancy, some remedies to treat them and why your doctor should be kept in the loop.
Is it a headache or something else?
It isn’t always easy to tell what kind of headache you’re having, but the most common types of headaches during pregnancy are tension-type headaches, migraines and cluster headaches.
Tension headaches are the most common kind of headache in pregnant women. It can feel like someone is trying to squish your head like a watermelon. If you carry your stress in your shoulders and neck, you may be more susceptible to this kind of headache.
Migraines are a particular type of headache that occur on one side of the head. For some women, migraines can get worse the first few months and then improve in later stages of pregnancy. For others, they may experience no change, decrease or difference in their migraines.
Cluster headaches are less common but can occur during pregnancy. You’ll suddenly have severe pain around your eyes or temples usually about the same time every day.
The good news is that there are plenty of pregnancy-safe things you can do to prevent and relieve the most common pregnancy headaches.
Tips for relieving mild headaches
- Get plenty of rest. Sleep is especially hard later in your pregnancy but is so important to physical and mental health. Find yourself a comfy prenatal pillow and snuggle away.
- Drink plenty of water. Pregnant moms require more water than the average person. While you may want to avoid extra trips to the bathroom, adequate fluid intake is important for you and baby.

- Eat regular, well-balanced meals. To prevent low blood sugar, eat small meals throughout the day. Avoid sugar, like soda and candy.
- Get a prenatal massage. A full-body massage can release tension in the muscles of your neck, shoulders and back.
- Use warm compresses on head, neck and shoulders.
- Avoid triggers. Keep a journal to help identify specific triggers so you can learn what to avoid. Some common headache triggers include strong odors and nitrites or nitrates.
- Try exercise and relaxation techniques. There’s evidence that regular exercise can reduce stress and boost overall mood. Check with your doctor first before starting any new fitness routines.
- Take acetaminophen to relieve symptoms (as approved by doctor).
- Take caffeine in doses less than 200mg in a day (as approved by doctor).

If you have a history of migraines, however, your doctor may treat them differently during pregnancy. Discuss with your doctor what medications are safe to take during pregnancy.
Is my headache a cause for concern?
Sometimes. Headaches tend to be more common in the first and third trimesters, but they can occur in the second trimester as well. While there are common causes for headaches during pregnancy, it’s important to note that headaches during the second and third trimester can also be due to high blood pressure, called preeclampsia.
“Preeclampsia is a pregnancy-related condition that requires prompt evaluation and management with an obstetrician or maternal fetal medicine specialist,” Dr. Saunders said. “Elevated blood pressure prior to pregnancy puts a woman at increased risk for preeclampsia.”
When should I call my doctor?
Whether you experience headaches or not, it’s always important to discuss your pre-pregnancy history, obstetrical history and concerns with your doctor for an individualized assessment and management plan. However, if none of the above treatments resolve your mild headache or your headaches become more frequent and severe, talk to your doctor to determine the cause.
However, if none of the above treatments resolve your mild headache or your headaches become more frequent and severe, talk to your doctor to determine the cause.
“This includes new headaches that present after 20 weeks, a sudden onset of severe headaches, headaches associated with a fever, mental health changes, elevated blood pressure and vision changes,” Dr. Saunders said. “It’s important to keep an open line of communication with your physician and let them know about any changes in your health so they can rule out anything serious."
Got questions? We can help!
If a headache is keeping you up at night and your doctor isn’t available, call the Banner Nurse Now line, a free health care service that offers advice 24-hours a day, seven days a week. Call 844-259-9494.
Check out other pregnancy articles on our Banner Health blog
Pregnancy is an exciting, but also a bit scary time (especially if this is your first baby). Here are some other reads to help guide you through the trimesters and welcoming baby:
- 5 Tips for Having a Happy, Healthy Pregnancy
- Expect the Unexpected: How Your Body Changes During Pregnancy
- What To Expect In The Second Trimester
- Understanding Pulmonary Embolism Risk During Pregnancy
Women's Health Pregnancy
Join the Conversation
Migraine during pregnancy: what to do
Migraine is a benign disease, it does not affect the course of pregnancy and fetal development. However, migraine and pregnancy is a combination that requires a responsible attitude. Especially with frequent migraines (more than 2 times a week) and migraines with aura, because:
However, migraine and pregnancy is a combination that requires a responsible attitude. Especially with frequent migraines (more than 2 times a week) and migraines with aura, because:
-
medicines approved for use, few,
-
and the approach to the treatment and prevention of migraine during this period is extremely individual: it depends on the frequency, severity and duration of headache, the degree of impact on life.
Our neurologist Daria Korobkova conducted a live broadcast on the clinic's Instagram account, where she told how migraine and pregnancy are connected, why attacks become more frequent or disappear, and answered subscribers' questions. The ether was saved, see “Air recording: migraine during pregnancy and GV.
We will tell about migraine during breastfeeding separately.
The statistics of clinical observations of migraine during pregnancy looks like this:
In 60-70% of pregnant women with migraine, headache attacks become less frequent, milder, or even completely disappear in the second and third trimesters. This is due to the stabilization of estrogen levels. By the beginning of the second trimester, it rises 6 times and its fluctuations stop.
This is due to the stabilization of estrogen levels. By the beginning of the second trimester, it rises 6 times and its fluctuations stop.
In other women, migraines during pregnancy either remain unchanged or worsen. But as the duration of pregnancy increases, the proportion of such women gradually decreases:
If at the end of the first trimester the frequency and intensity of attacks persist, then it is most likely that migraine will disturb the woman throughout the entire period of pregnancy and after childbirth too.
How to manage migraine during pregnancy?
The main thing here is to learn how to control seizures and, if necessary, seek medical help.
-
Follow lifestyle advice:
-
get enough sleep;
-
drink enough fluids;
-
eat fractionally and without long breaks;
-
rest;
-
avoid stressful situations.
 This is one of the main provocateurs of migraine. Psychotherapy, relaxation and stress management are here to help you.
This is one of the main provocateurs of migraine. Psychotherapy, relaxation and stress management are here to help you.
-
Keep a headache diary. This will help you take control of migraine triggers.
Yes, these simple recommendations are sometimes enough to make seizures less frequent! Pregnancy is a special state of a woman. If in other periods of life we do not take such recommendations so seriously, then in this situation it is worth trying to change the philosophy of life and attitude towards ourselves =)
How to relieve an attack?
-
Favor non-drug methods. Sometimes, in order to relieve an attack, it is enough to eliminate an unfavorable factor:
-
dry biscuits, ginger, or applesauce may help with nausea;
-
for dehydration - diluted juice or other liquid;
-
sleep, walking or breathing exercises can also help to cope;
-
If the attacks are severe, interfere with your life, then under the supervision of a specialist, you can resort to drug therapy.

PARACETAMOL is considered the safest and can be taken throughout pregnancy.
All other drugs have nuances. For example:
-
ibuprofen can be taken in the second trimester, and in the first trimester it is better to limit, in the third trimester the drug is contraindicated for use;
-
aspirin is prohibited in the 3rd trimester and is undesirable for taking in the first two, as it can cause extremely undesirable consequences;
-
It is strictly forbidden to use ergotamine and opioid analgesics;
-
triptans are not officially approved for use during pregnancy as no controlled studies have been conducted. However, clinical observations of women around the world who took them on their own showed no adverse effects on the fetus. We discussed this issue in more detail on the air.
!Other than paracetamol, we do not recommend the use of any drug without a doctor's prescription.
When to see a doctor:
-
migraine occurred for the first time during pregnancy;
-
if migraine attacks suddenly become more frequent and stronger;
-
if the aura became longer or appeared for the first time;
-
if the headache is rapidly increasing and has an unusual character;
-
if the pressure rises during the headache.
Follow our Instagram to read the latest materials on the diagnosis and treatment of headaches!
cluster headache. Rare but painful Holidays without headaches. Real holidays Something about osteochondrosis. An excerpt from the book of Kirill Skorobogatykh.
Headache during pregnancy
Authors: A. Yu. Limanskaya, Yu.V. Davydova
Yu. Limanskaya, Yu.V. Davydova
01/19/2017
A.Yu. Limanskaya
Tension headache and migraine are the most common types of headache (30-78% and 15% respectively). According to the WHO, primary headache is in general in 10th place among all conditions leading to disability, and in women, in 5th place. In 16% of patients, episodic tension-type headache becomes chronic. The economic loss in Western Europe and North America due to headache-related disability is estimated at $17-20 billion a year. To date, there is a trend towards an increase in the incidence of headache in young people.
Yu.V. Davydova
The International Headache Society defines migraine as a unilateral, throbbing headache associated with nausea, sensitivity to light, sound, and turning of the head.
In a broader sense, this pathology can be considered as a hereditary disease in which physiological changes (whether external, such as changes in weather conditions, or internal, such as changes in sleep patterns) often cause stereotypical attacks with the migraine features defined above. Migraine occurs three times more often in women than in men, with the highest rates in women during active childbearing age, peaking at 27% at age 41 years. To date, there is no evidence that migraine itself affects fertility or the course of pregnancy, but the quality of life in pregnant women with migraine is significantly reduced.
According to some researchers, migraine and tension-type headache in pregnant women are risk factors for the development of arterial hypertension and preterm birth (F. Facchinetti et al., 2009). Pregnancy can provoke the occurrence of diseases accompanied by headache (preeclampsia, thrombosis of the cerebral arteries, compression of the brain as a result of the presence of tumors). Relevant today is the rapid diagnosis of pathology and an adequate choice of therapeutic and obstetric tactics for the treatment of headaches in pregnant women due to the great medical and social significance of the problem.
Relevant today is the rapid diagnosis of pathology and an adequate choice of therapeutic and obstetric tactics for the treatment of headaches in pregnant women due to the great medical and social significance of the problem.
Antiphospholipid syndrome (APS) is defined by the presence of antiphospholipid antibodies (APLA) associated with an increased risk of thrombosis or recurrent spontaneous abortion. The most serious complications can occur in secondary APS against the background of inflammatory systemic autoimmune diseases. Studies conducted in neurological clinics have found that it is migraine, and not headache of all types, that is significantly associated with APLA in patients with systemic autoimmune pathology. However, in patients with systemic lupus erythematosus (SLE), headache is significantly associated with positive APLA titers. Also in this group, cerebral ischemic lesions were significantly more common.
A woman may experience many health problems during pregnancy. For example, a headache during pregnancy occurs quite often, at different times of the day and for various reasons. Oddly enough, but a woman's frequent headache may be a sign of pregnancy, which she does not yet know about.
For example, a headache during pregnancy occurs quite often, at different times of the day and for various reasons. Oddly enough, but a woman's frequent headache may be a sign of pregnancy, which she does not yet know about.
More than 80% of women sooner or later complain of a headache during pregnancy. Even if a woman was absolutely healthy before pregnancy, then during the bearing of a child she gets a headache. Sometimes it becomes so strong that it is difficult to endure. Headache can occur at any time during pregnancy, but it tends to be most common during the first and third trimesters.
There are factors that can cause headaches during pregnancy.
1. Hormonal changes: the state of the nervous system depends on the woman's hormonal status, that is, on the quantity and quality of hormones produced.
2. Hypotension during pregnancy is associated with the predominance of progesterone over other hormones; the vasodilating effect of progesterone leads to a decrease in blood pressure, cerebral hypoxia and, as a result, to headache.
3. Arterial hypertension and preeclampsia cause headache as a result of generalized vasospasm and circulatory disorders in the central nervous system.
4. Nutritional factors - cold food or eating foods containing tyramine and phenylamine (nitrogen compounds that can affect blood vessels) can cause headache attacks; pregnant women who are prone to migraine headache should be careful in consuming the following foods: chocolate, nuts, yogurt, chicken liver, avocados, citrus fruits, bananas, canned and pickled foods, Japanese cuisine, tea, coffee, cola, sausages, red wine, cheese.
5. Hunger headache occurs as a result of a decrease in blood glucose levels and impaired supply of nutrients to the brain.
6. Overweight.
7. Eye strain or prolonged forced stay in the same uncomfortable position.
8. Allergic reactions.
9. Dehydration of the body.
Dehydration of the body.
10. Exacerbation of chronic diseases - spine, especially osteochondrosis, due to increased load during pregnancy, static and dynamic loads often cause headaches; neurocirculatory asthenia as a cause of vasospasm and as a consequence of the appearance of a feeling of heaviness in the head, mood lability and headache.
11. Occurrence of infectious and other diseases such as: meningitis, encephalitis, sinusitis, pyelonephritis, glomerulonephritis and certain ophthalmic pathologies; the characteristic manifestations of this headache are its intensity and the lack of effect of pain medications.
12. Stress factor. Lability of the nervous system, ups and downs in mood, excitement, psycho-emotional stress, depression - all this can cause a headache.
13. Changing weather conditions. During pregnancy, fluctuations in atmospheric pressure can lead to headaches.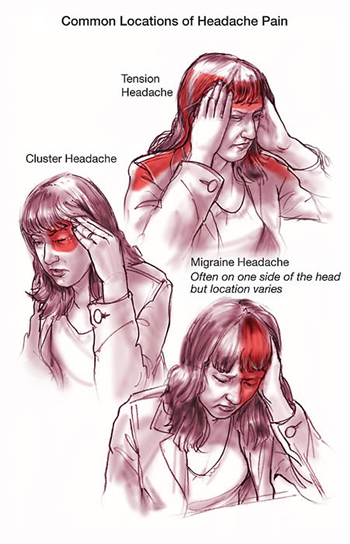
14. Physical stimuli - flickering light, noise, strong odors.
15. Weekend headache. If you sleep longer than usual during the day, the cause of headache can be, for example, venous congestion.
16. Indoor climate: too dry or warm air, a lot of tobacco smoke.
The most common form of headache during pregnancy is migraine, which is accompanied by visual impairment, gastrointestinal disorders, nausea, vomiting, photoreaction, and various vestibular disorders.
In the United States, 28 million people aged 12 and older suffer from migraine, of which 21 million are women aged 25-55. In about 25% of families, one of its members suffers from migraine.
A feature of migraine pain is known to be severe, throbbing pain, predominantly hemicrania, often preceded by aura and marked photoreaction.
It is noteworthy that about 15% of women who have never experienced migraine attacks before, experience it for the first time precisely with the onset of pregnancy. On the other hand, there are cases when during pregnancy a woman completely stops migraine attacks. In this case, this is due to changes in hormonal status and the absence of ovulation and menstruation.
On the other hand, there are cases when during pregnancy a woman completely stops migraine attacks. In this case, this is due to changes in hormonal status and the absence of ovulation and menstruation.
The occurrence of migraine in women under the influence of hormonal changes is possible throughout the entire menstrual cycle. The positive effect of pregnancy on migraine is observed in 55-90% of women during the gestation period, regardless of the type of migraine. The relief of headache symptoms during pregnancy and their possible worsening after childbirth is likely due to uniformly high and stable estrogen levels during pregnancy and their rapid decline after childbirth.
Another type of headache in pregnancy is tension headache. As a rule, it is characterized by medium intensity, unlike migraine, it often covers the entire head. The pain of tension squeezes the head like a hoop, or causes a pulling sensation; occurs mainly as a result of stress or overexertion.
- If a woman has frequent headaches before pregnancy, the risk of developing preeclampsia increases by 2.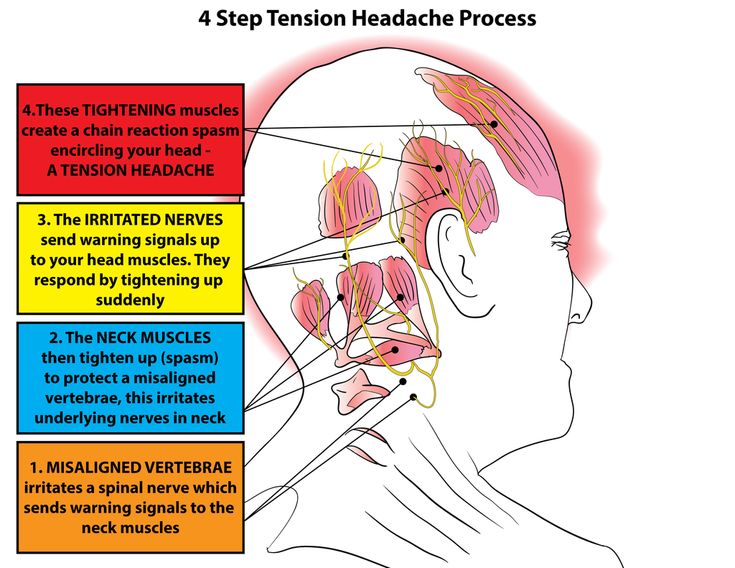 4 times
4 times
- If a woman is diagnosed with migraine before pregnancy, the risk of developing preeclampsia increases by 3.5 times migraine attacks are observed in the early stages - the risk of developing preeclampsia increases 4 times
Pregnancy headache treatment
A pregnant woman needs medical advice if:
- headache has become almost constant, and has recently changed its character;
- headache in the morning and all day;
- pain is constantly localized in a certain part of the head;
- headache is accompanied by other symptoms - impaired vision, hearing, speech, motor functions, sensitivity, etc.;
- Pain accompanies high or low blood pressure.
Doctor's prescriptions depend on the underlying cause of the headache. Sometimes several factors influence at once, so it is difficult to make an accurate diagnosis. If the headache bothers you regularly, you should contact a neurologist for a specific examination.
Primary therapy during pregnancy - non-drug (relaxation, sleep, massage). For the treatment of acute migraine attacks, paracetamol (1000 mg) is considered the drug of choice, preferably in the form of suppositories. The table shows data on the possibility of using a number of drugs for the treatment of headache during pregnancy.
The risks associated with the use of aspirin (acetylsalicylic acid) and ibuprofen are considered relatively low if the drugs are taken episodically and stopped in the last trimester.
Information on the safety of triptan treatment during pregnancy is available for only a few drugs in this group (sumatriptan, naratriptan and rizatriptan). According to information databases containing information on pregnancy outcomes in women who received these drugs, there were no facts indicating serious risks to the mother and fetus.
With some triptans (sumatriptan, zolmitriptan, naratriptan), there is currently a possibility of a slight increase in preterm birth, so triptans are acceptable in severe migraine in exceptional cases.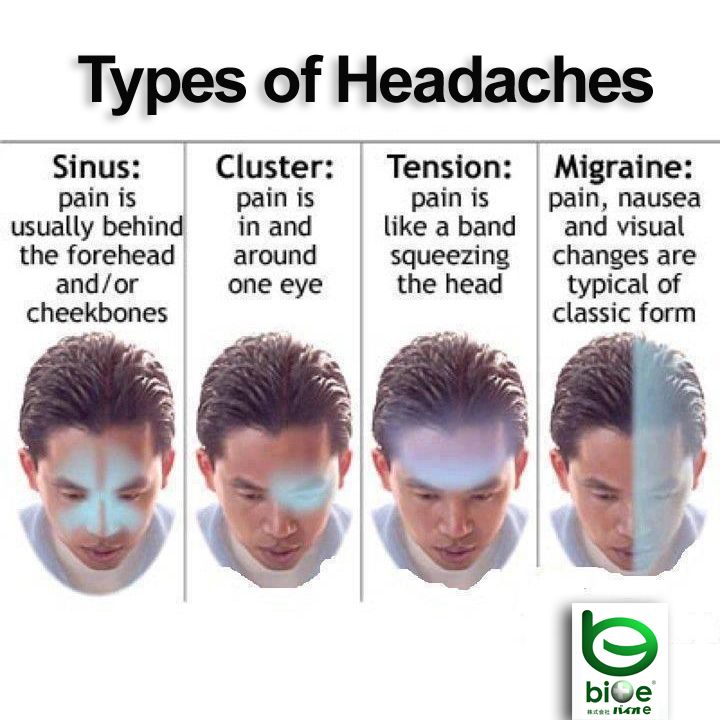 However, data on the use of triptans continues to accumulate and there is not yet sufficient evidence for the safety of the use of triptans during pregnancy.
However, data on the use of triptans continues to accumulate and there is not yet sufficient evidence for the safety of the use of triptans during pregnancy.
Dihydroergotamine and ergotamine tartrate are contraindicated in pregnant women.
Headache definitely cannot be tolerated, it must be correctly diagnosed, differentiated and treated.
The American Academy of Neurology recommends a brain scan for the following cases (MRI only is recommended during pregnancy)
- if, in the presence of a headache, a neurological deficit or any, even short-term, changes in the neurological status occurred;
- if the headache has atypical manifestations and does not fit into the strict framework of establishing a diagnosis of migraine;
- if there is a proven immunodeficiency;
- a sudden severe headache in women for the first time.
- Number:
- Thematic issue "Gynecology, Obstetrics, Reproductology" No.
 4 (24), chest 2016
4 (24), chest 2016
11/20/2022 Obstetrics/Gynecology The use of antiseptics in the treatment of vaginal infections in various etiology
Such antiseptics are an alternative to antibiotic therapy in the treatment of bacterial vaginosis due to a wide spectrum of antimicrobial activity, low toxicity and high biomass content of tissues. The Recommendations present the advantages and disadvantages of the main antiseptic products available today, which can be stasted for the treatment of vaginitis in various etiologies. ...
11/20/2022 Obstetrics/gynecology Aspects of treatment of pain syndrome in endometriosis
Pain syndrome in endometriosis is headache, for which patients go to the doctor.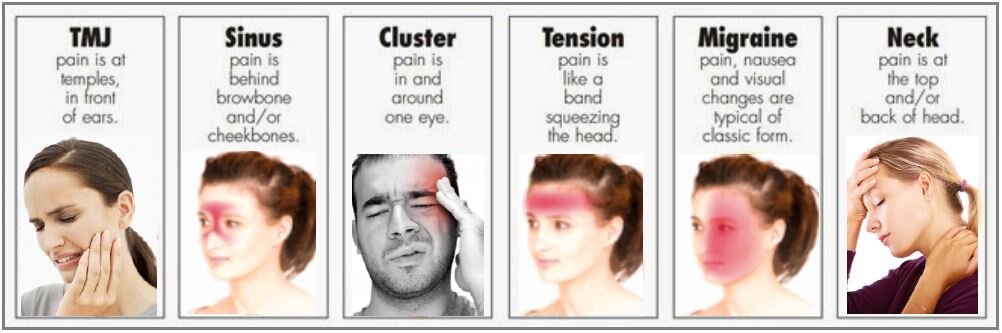 To fight with pain in case of any illness, there may be a combination of chiropractic drugs, however, non-steroidal antispasmodic preparations are most commonly used to relieve pain. ...
To fight with pain in case of any illness, there may be a combination of chiropractic drugs, however, non-steroidal antispasmodic preparations are most commonly used to relieve pain. ...
11/20/2022 Obstetrics/GynecologyAbdominal hysterectomy and post-surgical follow-up: emphasis on diseases Vidkrita abdominal hysterectomy is accompanied by a significant algogenic afferent impulse from the surgical intervention. Also, the search for effective methods to prevent post-operative pain should be relevant. In the article, the analysis of the current approached pre-juvenile (pre-operative) stoppage of non-drug effects for superior pain control. Given the literature, we can show that the total choice of paracetamol, dexketoprofen, nalbuphine, as well as ropivacaine or bupivacaine allows to implement the concept of multimodal analgesia and optimize the process of renewal after surgery.