How to prepare child for sleep study
Tips for your Child's Sleep Study
/in News, Uncategorized /by Sharon GoldmanBy Amanda Jones RPSGT- A Sleep Technician Mommy
An in-lab sleep study can be stressful for the adult patient. But bringing your child in for a sleep study can be nerve-wracking for the both of you. Our Sleep Technician Manager (and mommy of 2) is here to help give you some tips for your child’s sleep study and what to expect.
Pediatric Sleep Study Tips
- To best prepare your child, keep napping to a minimum on the day of the study. Keeping your child from napping may help them fall asleep easier in the lab. Of course, it may be difficult to prevent your child from falling asleep, but do your best to minimize napping the day of the study.
- You and your child will be greeted by a friendly, experienced licensed sleep technologist. You both will be shown to your private room for the night. Our rooms have a queen size bed, TV, and an overstuffed recliner for your comfort.
- The sleep technologist will go over any questions you may have prior to starting the study. Your child will be asked to sit in a computer chair while the wires are applied. The hook up can take up to 30 minutes, so if your child has an iPad, book, or toy they like, feel free to bring it!
- During the hook up, the sleep tech will politely explain why the wires are being applied. This, in turn, will make your child feel more comfortable. As an example: For some younger children, some techs will say the wires will test for superpowers! This set-up includes the following equipment:
- A bandage-like sensor that measures your child’s oxygen will be placed on the toe or finger
- Small plastic prongs at the nose will measure your child’s exhaled air
- Elastic or cloth belts will be placed on your child’s chest and stomach, usually over their pajamas
- Stick-on electrodes will be placed on your child’s face and chest to measure eye movements, heart rate, and muscle tone during sleep.
- A few additional electrodes are applied with a washable paste on your child’s scalp to measure stages of sleep
- We do recommend and ask that the parent sleep in the recliner and not in the bed with the child. This is so we get a clear recording of your child’s movements and sleep patterns. If the parent were to sleep in the bed with a child and simply just change positions, it could cause the child to wake up or make it look like the child was moving their leg.
- We understand that this can be stressful and at times scary for your little one, and they may need your comfort while laying in bed. This is OK. We only ask that once the child is asleep, you exit the bed quietly and move to the recliner to sleep.
- If your child has any comfort items (blanket, stuffed animal, etc.), we recommend and welcome them to come to the sleep over as well!
- If your child likes to have a bedtime snack or a specific nighttime drink (ex: milk), make sure to bring those as well.
 The lab does have a refrigerator, a water cooler with hot and cold water and a microwave, if needed.
The lab does have a refrigerator, a water cooler with hot and cold water and a microwave, if needed. - No need to worry if your child is a restless sleeper. The sleep technologist will be monitoring your child and the leads throughout the night. They might have to come into the room a few times to adjust or reattach wires that come loose.
- If your child has a hard time tolerating the study, don’t worry. The sleep technologist is experienced working with children and will work hard to get the proper data for the doctors. The doctors are great and are equipped to read the data collected, even if its not perfect.
- If your child has bed-wetting accidents at night, that is not a problem! Kindly let the tech know so they can lay down extra protection.
- The wires are pain-free to attach, as well as remove. We have adhesive remover on hand for an easy removal in the morning with little irritation! There will be some paste residue on the face and head once the wires are removed.
 This residue is water soluble and will wash out with warm water. Using conditioner can help make the paste removal easier, as well as micellar water or rubbing alcohol.
This residue is water soluble and will wash out with warm water. Using conditioner can help make the paste removal easier, as well as micellar water or rubbing alcohol.
Pediatric Sleep Disorders
Up to 50% of children will experience a sleep problem. Early identification of sleep problems may prevent negative consequences, such as daytime sleepiness, irritability, behavioral problems, learning difficulties, motor vehicle crashes in teenagers, and poor academic performance.
Our goal at Comprehensive Sleep Care Center is to make you and your child’s experience as comfortable and beneficial as possible.
Tags: childhood sleep disorders, Children and sleep, kids sleep study tips, Pediatric Sleep Disorders, pediatric sleep study, Pediatric Sleep Study Tips, Sleep Study, Sleep Study FAQ, sleep study for children, sleep study for kids, Sleeping issues with children, Tips for kids sleep studyShare this entry
 com/wp-content/uploads/2019/08/941871_10200847474085584_1363427941_n.jpg 612 612 Sharon Goldman https://comprehensivesleepcare.com/wp-content/uploads/2017/05/CSC.png Sharon Goldman2020-08-12 10:46:092022-07-07 15:45:37Tips for Your Child's Sleep Study
com/wp-content/uploads/2019/08/941871_10200847474085584_1363427941_n.jpg 612 612 Sharon Goldman https://comprehensivesleepcare.com/wp-content/uploads/2017/05/CSC.png Sharon Goldman2020-08-12 10:46:092022-07-07 15:45:37Tips for Your Child's Sleep Study COMPREHENSIVE SLEEP CARE CENTER
We offer quality sleep diagnostics and affordable pricing for people like you. Contact us today to say hello to sleep again.
9 SLEEP CARE CENTERS IN DC AREA
Alexandria, Arlington, Bethesda, Chantilly, Dumfries, Germantown, Lansdowne, Manassas, Woodbridge
Corporate Office Hours
Monday-Friday 8:00 am to 5:30 pm
Sleep Center open 7 nights a week
Phone: (703) 729 3420
Fax: (703) 729 3422
[email protected]
©2022 Comprehensive Sleep Care Centers in DC area
Kids, Sleep and COVID-19 Breast Cancer and Sleep Apnea
» How to Prepare Your Child for His Sleep Study.

25-30 percent of children suffer from some form of sleep disturbance such as sleep apnea, narcolepsy, sleepwalking, bed wetting or night terrors. 2-3 percent of children have sleep apnea. While many childhood sleep issues are not cause for concern, a disturbance that reduces your child’s quality or quantity of sleep on a regular basis can lead to more serious problems including:
– Accidents and injuries
– Behavior problems
– Mood problems
– Memory, concentration, and learning problems
– Performance problems
– Slower reaction times
With the increased importance medical and public health officials are placing on quality sleep, more doctors are recommending that their child patients undergo a sleep study to diagnose or rule out a sleep disorder.
In a previous post, we described the most common sleep disorders affecting children, along with their symptoms. In this post, we explain what you and your child should expect if your doctor recommends a sleep study.
A sleep study can appear to be a complicated procedure, especially when the patient is a child. However, the process is actually quite simple. Technicians will explain the process, in great detail, to both the child and his guardian who will stay in the room for the entire sleep study (overnight). The child can bring his own pillow, blanket, stuffed animal or comfort toy.
- Child and guardian arrive at the sleep center. You may arrive in your pajamas or change at the sleep center. The child must wear a separate top and bottom.
- Child and guardian get acquainted with the technologist and the sleep study room.
- The technologist explains what will happen during the sleep study.
- When it’s time to go to bed, the technologist places sensors on the child’s head that attach to the head with a gentle adhesive. These sensors are the electrodes that will be monitoring brain waves during sleep (see the child in the picture at the top of this post).
- An electrode is placed on the child’s finger and stretchy belts around their abdomen to track breathing during sleep.

- Child and guardian go to sleep for the night. The guardian will usually sleep in a separate bed, cot or air mattress in the same room.
- While the child and guardian are sleeping, the technologist stays up all night and monitors the child’s sleep through a video camera. They also monitor heart rate, breathing and brain activity.
- During the night, the technologist may quietly enter the into the sleep study room to adjust an electrode that may have fallen off.
- In the morning, the technologists carefully removes the electrodes and sleeping belt from the child. Once everything is removed, the child and guardian are free to go!
- A few days following the sleep study, a sleep doctor will look at the information collected during the study to report on how the child slept.
- The report will be sent to the child’s physician to review the findings and discuss next steps.
Following the sleep study, there are treatment options available for children. If the sleep study reveals that the child an airway obstruction causing sleep apnea, treatments include breathing support (CPAP therapy) during sleep or surgery to remove the tonsils and adenoids. If the sleep study shows that the child’s sleep is disturbed by a psychological or behavioral problem, pediatric behavioral psychologists can assist the child in finding specific behavioral techniques to help children develop better sleeping patterns.
If the sleep study reveals that the child an airway obstruction causing sleep apnea, treatments include breathing support (CPAP therapy) during sleep or surgery to remove the tonsils and adenoids. If the sleep study shows that the child’s sleep is disturbed by a psychological or behavioral problem, pediatric behavioral psychologists can assist the child in finding specific behavioral techniques to help children develop better sleeping patterns.
We perform sleep studies at each of our sleep centers (click here to see our locations across Southern California) 7 nights a week, for children over one year old. If your child’s doctor has recommended a sleep study, learn more about having your sleep study with us.
Request a sleep study
If you are a healthcare provider looking for information about referring your pediatric patients for sleep studies, visit our online resource library. It’s full of tools and guides including CPT and ICD10 codes and guides to understanding sleep study reports and insurance coverage.
Resources Library
Other posts you may find interesting:
- Sleepy Students Perform Worse in School
- Sleep Disorders Affecting Children; Does Your Child Need a Sleep Study?
- What Causes Sleep Apnea in Children?
- Chasing Away Midnight Monsters: How to Handle Nightmares
- Toddlers and Sleep- Skipping Naps Decreases Joy, Interest and Understanding
- Why Do Kids Like Jahi McMath Need Surgery to Remove their Tonsils for Sleep Apnea?
- Doctors: “Start School Later, Give Students Time to Sleep”
Sources:
http://www.childrenshospital.org/conditions-and-treatments/conditions/sleep-studies/overview
http://my.clevelandclinic.org/services/neurological_institute/sleep-disorders-center/disorders-conditions/pediatric-sleep-disorders
http://www.webmd.com/sleep-disorders/guide/children-sleep-problems
Editor’s Note: This post was originally published in January 2014 and has been edited and updated for accuracy and comprehensiveness.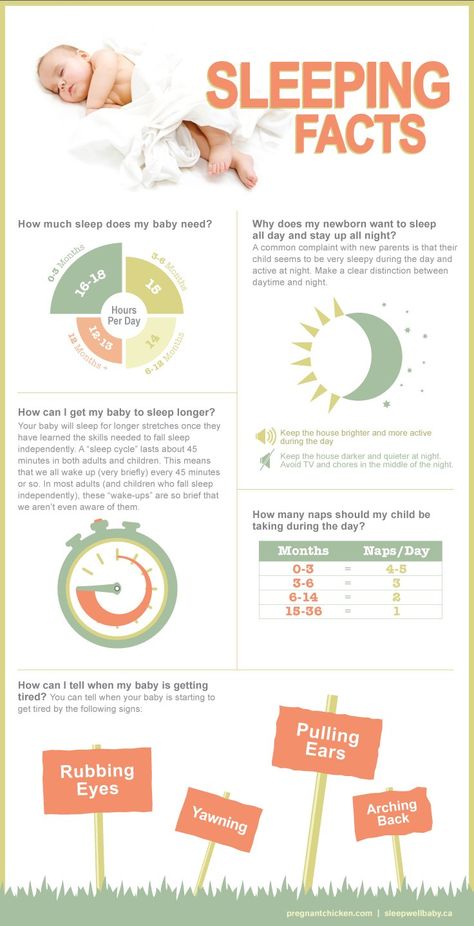
Julia Rodriguez
Julia joined Advanced Sleep Medicine Services, Inc. in 2011 with a background in sales, marketing and customer service. She is currently the vice president of marketing and operations and enjoys the opportunity to educate and interact with those looking to improve their health through better sleep.
The Kim West Method - The Kim West Self-Sleep Method, description
The method that the Sleep Baby team uses in their work was developed by the leading specialist in children's sleep Kim West The Sleep Lady ™ and is called The Sleep Lady Shuffle. This is a soft approach to sleep education, which provides for a comprehensive adjustment of the sleep and wakefulness regimen, sleep hygiene conditions, as well as the adjustment of associations for sleep, takes into account everyday and emotional aspects that are of great importance at an early age. The Kim West technique has been successfully used in many countries of the world for almost 20 years and has proven its safety and effectiveness.
Kim West is the official partner and curator of the Sleep, Baby project in Russia.
In this article, we will talk in detail about K. West's approach to teaching sleep and why we chose him to work with Russian-speaking mothers.
Who is Kim West?
Kim West or Lady Sleep (The Sleep Lady TM) is a world-famous specialist in the behavioral problems of children's sleep, the author of the Slow Withdrawal Method (The Sleep Lady Shuffle TM), which has been successfully used all over the world for more than 20 years.
Kim West is author of three best-selling parenting books translated into several languages, author of the Gentle Sleep Coach http://gentlesleepcoach.com, founder of the International Children's Sleep Association www.IACSC.com.
Kim West is the founder of the Gentle Sleep Coach School. Already more than 150 certified consultants around the world carry the title of GSC, among them all members of the team of sleep consultants for children Sleep, Baby.
Kim West has helped thousands of families around the world improve their babies' sleep. Kim developed the Slow Withdrawal Technique and described it in detail in her book Good Night, Sweet Dreams, which became a bestseller.
Research on the effectiveness of the
Scientific study on the effectiveness of the Slow Withdrawal method is scheduled for early 2019. A research team of scientists (Wendy Middlemiss, PhD, Sarah Blunden, PhD, Macall Gordon, M.A.) plans to compare 2 groups of parents of children aged 6 months, where one group will use the Ferber method, and the other group will use the Kim West method (or the Slow Method). distance). It is hypothesized that in the group of parents using the Slow Withdrawal technique, there will be a higher percentage of % of consecutive actions of parents and the number of cases of bringing the technique to completion.
Description of the technique
The Kim West or The Shuffle TM technique was created over 20 years ago based on a huge request from parents related to children's sleep. In response to this request at that time, doctors suggested 2 ways:
In response to this request at that time, doctors suggested 2 ways:
1) wait until the child outgrows sleep problems
2) use the Cry It Out technique (CIO or “cry before falling asleep”), which was actively promoted by Dr. Mark Weissbluth.
But neither of these two ways solved the problem of sleepless parents by 100%. Moreover, the CIO Method raised concerns about the psychological and physiological safety of a child learning to fall asleep on his own with this approach. And not all parents decided on the use of CIO.
K. West has done a great deal of work on the physiology and psychology of children's sleep. Based on this knowledge and extensive experience with behavioral correction, and as an alternative to the CIO method, a soft technique for teaching independent sleep was created, which is called the Slow Withdrawal Method.
Kim's approach is based on gently and consistently teaching the child to fall asleep on his own. The technique is implemented through a gradual reduction in helping the child fall asleep, when the parent minimizes his direct participation in this process.
The technique is carried out in the presence of a parent (the baby is not left alone in the crib / room) and with maximum help to the child when learning to fall asleep.
Soft Withdrawal Technique:
- Can be applied to healthy children over 6 months old
- Parents do not intervene where the child can cope on his own, and help where he cannot yet!
- Mom or dad stay in the room with the baby until he falls asleep
- Adults gradually reduce their assistance until the child has mastered the skill. The pace of change is individual.
- You can teach your child to fall asleep on their own both in a separate bed and while sleeping together.
VIDEO LESSON
How to Teach Falling Asleep on Your Own?
More
Scheme of application
PREPARATION
The Slow Withdrawal Method is complex and requires a mandatory preparation step. Important things to do before starting the technique:
- Get your sleep conditions in order. It has been proven that the quality of sleep conditions directly affect the quality of sleep.
- Find a comfortable sleep and wake schedule. An overworked child will not be able to quickly relax and fall asleep due to the action of the “stress hormone” cortisol. That is why the comfortable mode of sleep and wakefulness directly affects the rate of falling asleep and the continuity of sleep. Check if the baby has enough sleep, make sure that the baby does not overwork.
- Find a window to sleep. "Window to sleep" - the beginning of the production of the "sleep hormone" melatonin and the ideal time to go to sleep. Watch your baby and write down signs of fatigue.
- Remove all negative associations for falling asleep. Sleep associations - all those actions that help the baby fall asleep.
 For example, motion sickness and feeding. If the baby, waking up between sleep cycles, cannot reproduce his associations for falling asleep on his own, he will call his parents for help, and sleep will become intermittent.
For example, motion sickness and feeding. If the baby, waking up between sleep cycles, cannot reproduce his associations for falling asleep on his own, he will call his parents for help, and sleep will become intermittent.
- Get the green light from your pediatrician. It is important to get confirmation from your pediatrician that poor sleep is not related to medical problems. All health issues should be addressed by a doctor!
- Choose a realistic start date: 2-3 weeks of sleep in one place. To form the right sleep habits, it is important to let the baby get used to the conditions in which he falls asleep and leave them unchanged, at least for the period of learning and consolidating the habit.
- Enlist the support of your loved ones. A tired mom will find it difficult to stick to the rules. If there is no support from relatives, it is important at least to restore strength and sleep for the mother herself.
Otherwise, she will not have the resource to change. And the emotional state of the mother will certainly affect the children's sleep.
APPLICATION OF THE PROCEDURE
Begin the procedure with a night's sleep. At night, the “sleep hormone” melatonin will help you fall asleep. Prepare the child for sleep, perform rituals, put the child in the crib “ready for sleep”, but not sleeping. It is important that the baby understands that he was put in the crib. Stay close and comfort your child. Don't leave the room. The next day, start applying the technique for daytime sleep. Every three days, move your chair further away from the crib until you're out the door.
HOW SOON WILL THE CHILD RESPONSE TO THE APPLICATION OF THE METHOD
It is difficult to answer this question unambiguously, because each family and each child has their own characteristics. For some children, 3 days is enough to master the skill of falling asleep on their own, for someone it stretches for 4 weeks. The methodology that we use cannot be universal, because every family and every child has its own characteristics.
The methodology that we use cannot be universal, because every family and every child has its own characteristics.
The effect of applying the technique depends on several factors:
- realistic expectations and goals for the sleep training program
- features and temperament of the child
- parents, their attitude, patience and consistency in performing all the necessary actions.
How and why we adapted the Kim West approach in Russia
Kim West is one of the gentlest approaches to sleep training. Its author is an American, and, of course, working according to this methodology, we adapted it to Russian conditions and found a response from many families.
It is necessary to understand that children's sleep does not "live" by itself, but is an organic part of life, the relationship between parents and children. Therefore, the way babies are put to bed varies greatly in different cultures, just like, say, the age and method of complementary foods, the start time of going to kindergarten, attitudes towards illness, mom's going to work, and so on. Particularly different is what is considered “normal”, what is welcomed and what is condemned.
Particularly different is what is considered “normal”, what is welcomed and what is condemned.
In our video lessons, we take into account the cultural characteristics of Russian-speaking mothers, analyzing the experience of our team of family and perinatal psychologists, sleep consultants.
KIM WEST (The Sleep Lady) and Ksenia Antipova (SPE, Kid)
9000
We understand that at an early age to form a very important thing, very importantly, very importantly, very importantly form a very important thing. while mother and child. We know how to achieve this and practice an integrated and systematic approach.
Sleep Specialists, Baby take into account all the causes that affect your baby's poor sleep:
- health,
- organization of sleep and wakefulness,
- family atmosphere,
- mother-child relationship
- and, of course, the mood and well-being of the mother herself.

In the process of improving sleep, we offer mothers to find their own comfortable solutions, listen to their desires and needs of the baby, and calmly deal with current difficulties.
In addition, we always encourage the involvement of the closest circle, those relatives and friends on whom mom can rely on in work, we are looking for affordable ways to recuperate. Indeed, the quality of care for the baby, and hence the quality of his sleep, fully depends on her rest and positive attitude.
In the lessons we warn about all possible risks, give complete information about the options for actions in case of medical problems and work only within the framework of our professional competence.
Self-Falling Sleep Training0003
BABY'S SLEEP AND DREAMS • EVO Medical Center
How does a newborn's brain work during rest? What does the child dream about?
What happens in a dream?
While young mother and father “forgot when they slept for the last time”, the very source of parents' insomnia is sleeping a lot and soundly. The first week after birth, the baby sleeps about 16 hours a day, at the age of one year - about 13 hours. What happens at this time in the charming head of a son or daughter? Does the baby see magical dreams? Does he have nightmares? Or is it just that the child “turns off” and gains strength to wake up, leaving only the biochemical processes in the body to work?
The sleep of adults - still not known and not fully understood, the sleep of an infant - leaves even more questions. One of the key milestones in the scientific knowledge of sleep is the discovery of its phases. Phase "rapid sleep" (REM - rapid eye movement, that is, the phase of rapid eye movement) was discovered in 1953 by an American neurophysiologist, a pioneer in the scientific study of sleep, Professor Nathaniel Kleitman (University of Chicago, USA), by the way, a native of Chisinau, and his student Eugene Acerinski, also a representative of a family of Jewish emigrants from the Russian Empire. It is while in the phase of "REM sleep" that a person most often sees dreams.
It is while in the phase of "REM sleep" that a person most often sees dreams.
In parallel, a team of scientists from Northwestern University (Ohio, USA) was working on a system of dream systematization that would allow analyzing their content. Professor of psychology Calvin Hall paid special attention to the problems of personality psychology, temperament and dream analysis and brought sleep into the category of systemically studied states of the body.
Further, the alternation of the phases of "REM" and "slow" sleep was discovered and it was confirmed that at least 80% of dreams are contemplated by a person in the REM phase. The concept itself "sleep" - has been transformed and refined, shifting from the narrow "viewing pictures and stories" to the side - cognitive activity in sleep. Thus, the answer to the question about sleep has now ceased to be exclusively a retelling and presentation of dreams. In addition, scientists have made sure that sleep is necessary for many processes in our body:
- memory consolidation;
- "repair" of damage in various systems and organs;
- relaxation of all muscle groups;
- metabolic processes and skin regeneration;
- hormone synthesis;
- active production of antibodies by the immune system;
- stabilization of the “hydraulics” of blood supply and lymph flow, etc.
 etc.
etc.
The baby fell asleep! And this means - ...
Starting to study children's sleep, scientists had no doubt that this state is even more important for newborns and babies than periods of their activity and wakefulness, knowledge of the world through the senses . Children in a dream not only rest, their sleep phases change approximately hourly. In the REM phase, the brain continues to work actively, thought processes do not stop. The baby shows this to mom and dad with a wandering smile, twisting arms and legs, moving fingers, moving eyeballs under closed eyelids. As many studies show, the neurons of the child's brain during this period are often more active than outside of sleep.
REM sleep allows babies to:
- process and synchronize all the information received during the wakefulness stage;
- generalize experience, archive it and keep memories;
- create new neural connections and information flows between individual parts of the brain;
- acquire skills and learn the language;
- grow and develop.

In the phase of deep sleep - the baby rests from the received loads, recovers and accumulates energy for the future exploits of a growing man.
What does the baby dream about? Different points of view.
We just have to find out - do our babies dream? If they see, are these dreams similar to ours? “Getting inside a child's head is like deciphering a kitten's thoughts” (Angela Saini, British science journalist for the Guardian). The human brain is an extremely complex substance, the methods and technologies by which doctors and scientists “look” into the adult brain are hardly applicable to children. This means: the question of children's dreams gives rise to endless intrigue, reasons for scientific discussions and concerns of parents.
What do we know? Children stay in the REM phase much longer than adults. For newborns, this phase is almost 50% and about 8 hours a day (in adults - 20-25%). Logically, children should see and dream also a lot more. Pediatrician, Professor Alan Green (Stanford University, USA) believes that the child is able to dream while still in the womb (this is confirmed by measuring the brain waves of the fetus). In utero, the fetus stays in REM sleep for about 10 hours a day.
One can only guess about the content of children's dreams.
- It is believed that a child who woke up with a smile - had a good dream, woke up in tears - at least the dream was "not very good". Many researchers pay attention to the movement of the eyes under the eyelids: the eyes move to the sides - in a dream the child sees objects that move horizontally, if the vertical movement of the eyes is noticeable - the baby looks up, climbs, climbs, and so on.
- However, the opinion that babies dream is disputed by some experts. Dream is not a primitive process, which is always accompanied by the information perceived during wakefulness from the surrounding world.
 This process requires self-awareness, symbolic thinking, that is, the ability to turn impressions into images. This position is supported by the American psychologist and authoritative child sleep researcher Diane B Fawkes, who says that "living dreams" become available to children at the age of 7-8 along with self-awareness. At the age of 4-5 years, the description of sleep by a child is a static image that does not move in space and does not show emotions. In the first years of life, a child does not see anything in a dream; in the REM phase of this age, sleep is not constructed, but the construction of neural connections occurs, the development of language skills and the assimilation of new knowledge. These processes take up maximum resources and take up the entire performance of the “computer-brain”, there is simply no space and “RAM” for dreams. A small child is able to perceive reality, but he will be able to see dreams only when he learns to visualize the surrounding reality.
This process requires self-awareness, symbolic thinking, that is, the ability to turn impressions into images. This position is supported by the American psychologist and authoritative child sleep researcher Diane B Fawkes, who says that "living dreams" become available to children at the age of 7-8 along with self-awareness. At the age of 4-5 years, the description of sleep by a child is a static image that does not move in space and does not show emotions. In the first years of life, a child does not see anything in a dream; in the REM phase of this age, sleep is not constructed, but the construction of neural connections occurs, the development of language skills and the assimilation of new knowledge. These processes take up maximum resources and take up the entire performance of the “computer-brain”, there is simply no space and “RAM” for dreams. A small child is able to perceive reality, but he will be able to see dreams only when he learns to visualize the surrounding reality. - Some experts take an intermediate position.
 For example, the director of the Center for the Study of Sleep (Children's Hospital of Philadelphia, USA), a psychophysiologist, an expert in child psychiatry and behavioral sciences, Dr. Jodi A. Mindell believes that even today, babies born into the world see dreams, it's just that these dreams are different from adults. Most likely, these dreams are silent and consist of static "pictures" and not dynamic "videos". In an infant's dream comes someone's seen face, toy, object or form that has fallen into the field of view. Terrible dreams and nightmares - do not threaten the baby. Because fear develops in a child after 2 years.
For example, the director of the Center for the Study of Sleep (Children's Hospital of Philadelphia, USA), a psychophysiologist, an expert in child psychiatry and behavioral sciences, Dr. Jodi A. Mindell believes that even today, babies born into the world see dreams, it's just that these dreams are different from adults. Most likely, these dreams are silent and consist of static "pictures" and not dynamic "videos". In an infant's dream comes someone's seen face, toy, object or form that has fallen into the field of view. Terrible dreams and nightmares - do not threaten the baby. Because fear develops in a child after 2 years. - Modern research shows that even the youngest children understand, appreciate, explore and imagine the world much better than previously thought. To a certain extent, "they are even smarter than adults" - the opinion of psychology professor Alison Gopnik in the book "What is going on in a child's head?". Experiments confirm that children even understand probabilities, expressing extreme surprise if, from a box filled with white balls, in which there are only 4 red ones, adults draw only red balls with one white one.