Signs of special needs newborn
Risk Factors and Early Warning Signs
Knowing the early warning signs and risk factors for childhood disabilities and delays is key to getting the early help your child may need. Early intervention is proven to be effective in helping children with special needs – either to overcome delays or help set them up for future success.
Children develop at different rates and in different ways. These variances may be related to factors like health, personality, temperament, and/or experiences. Since the first five years of development are so critical, the sooner a concern is identified, the sooner your child can benefit from specialized services to support growth and development.
If you ever have any concerns about your child’s development, or if something just seems a little off, don’t hesitate to reach out to your pediatrician – even if no issues were identified at your child’s last appointment. And be sure to communicate your concerns with your child’s caregiver – whether it’s a family member, a nanny, or a child care program.
Most developmental disabilities are thought to be caused by a mix of factors. Some of these factors may include:
Prematurity or low birth weight.
Prenatal or environmental exposure to drugs, alcohol, or tobacco.
Poor nutrition (lack of nutritious foods, vitamins, proteins, or iron in diet, etc.) or difficulty eating.
Exposure to high levels of environmental toxins by the mother or child (such as lead).
Infections in the mother during pregnancy or baby early in life.
Trauma and stress.
Trauma, Stress, and Special Needs
Children may face stressful, negative life experiences that actually affect how their brains develop. Adverse Childhood Experiences (ACEs) refer to specific, emotionally traumatic life events. These can include early medical complications or delays leading to medical procedures, extended hospital stays, living with pain, discrimination, and more. Researchers have found that the more ACEs experienced by a child, the more likely that child may face medical and mental health issues throughout life. In other words, trauma and stress in a child’s life can lead to medical and mental health conditions. Stress has also been found to change the shape and size of an individual’s brain and the connections between the brain cells. Stress affects development, behavior, lives and learning. In other words, experiencing stress at an early age, especially numerous negative life events, can have a negative impact on a child’s development.
Researchers have found that the more ACEs experienced by a child, the more likely that child may face medical and mental health issues throughout life. In other words, trauma and stress in a child’s life can lead to medical and mental health conditions. Stress has also been found to change the shape and size of an individual’s brain and the connections between the brain cells. Stress affects development, behavior, lives and learning. In other words, experiencing stress at an early age, especially numerous negative life events, can have a negative impact on a child’s development.
Signs of Development Delays
Children with special needs can have differences in the way they develop and act. As your child grows, watch for these early signs:
Up to 6 months
Doesn’t coo or smile
Doesn’t react to loud noises or turn to follow sounds and voices
Has difficulty holding head up by age three months
Has difficulty following objects or people with their eyes
Arms or legs are stiff, or posture is floppy or limp
6 months to 1 year
Has trouble figuring out simple things like finding an object after seeing it be hidden
Has problems responding when being called from across the room, even when it involves something interesting
Has difficulty sitting, standing up, reaching for objects, or picking up objects, and doesn’t play games like peek-a-boo
Hasn’t started to say simple words like “mama” or “dada" by age one
Repeats behavior that could hurt, like self-biting or banging the head
Check out the Milestones page for more information.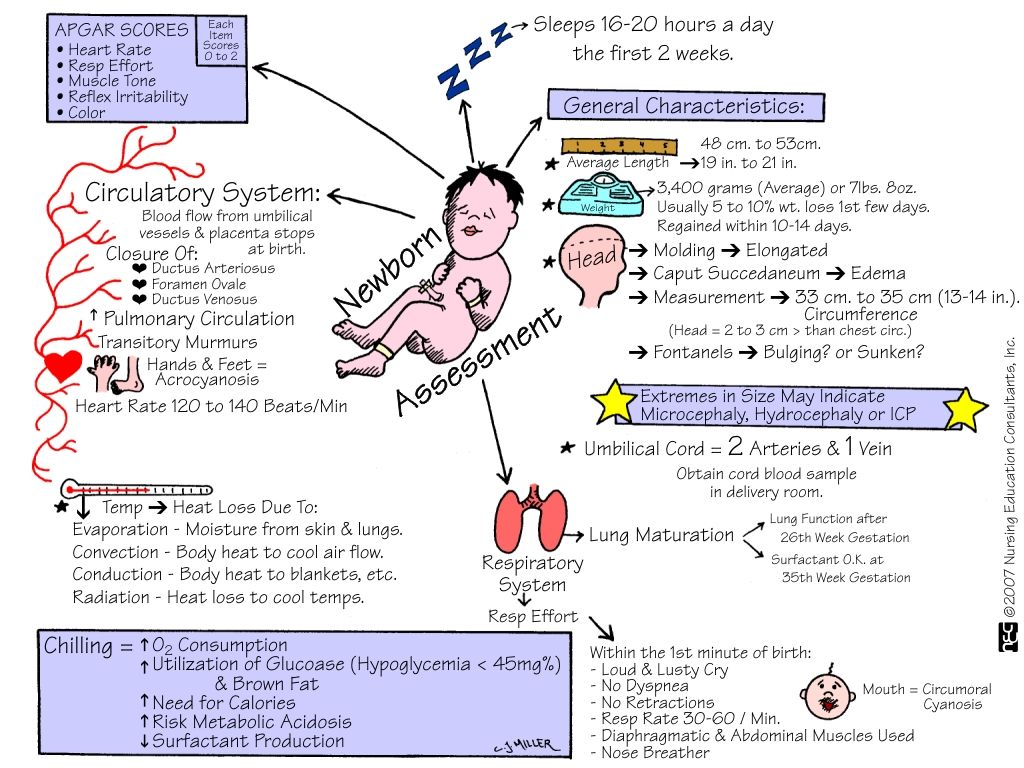
QUICK TIP: Did you know that your child's brain is at its most flexible from birth to age five, making it a prime window for learning? That's why it's so important to get your child the help and resources needed if there is a suspected or diagnosed disability. Earlier intervention can result in better outcomes for your child. Don't wait – ask your child’s pediatrician about any concerns you have and options for help.
7 Early Signs That Your Child Has Special Needs
In the United States, approximately 12.8 percent of children age 18 and younger have special needs. This includes conditions like autism, Asperger’s, and down syndrome.
For children with special needs, the sooner they can be diagnosed by a medical professional, the easier it is for them to get the treatment they need to feel their best and enjoy a high quality of life. Listed below are 7 of the most common signs of special needs that parents ought to watch for.
- Missing Developmental Milestones
One of the earliest warning signs that a child has special needs is missing development milestones. There are specific actions and behaviors that children should be able to practice when they reach certain ages.
There are specific actions and behaviors that children should be able to practice when they reach certain ages.
For example, at 2 months, a baby should be starting to smile at others or following things with their eyes. At 1 year, they should be able to play simple games (such as peek-a-boo) and pull themselves up to a standing position.
If a child is missing several developmental milestones, that can be an indicator that they have a disability and need to see a doctor.
- Difficulty Focusing and Controlling Impulses
All children have trouble focusing or practicing impulse control from time to time. However, if a child seems to never be able to focus or is extremely hyperactive in a wide range of settings, there’s a chance that they have Attention-Deficit Hyperactive Disorder (or ADHD).
Children who ADHD may have a hard time keeping up in school because they’re more easily distracted or have trouble sitting still. With proper accommodations, though, they can perform on par with, if not ahead of, their peers.
- Difficulty Making Eye Contact and Responsiveness
Most children start making eye contact at a young age (around 6-8 weeks). Their visual perception and communication also become more advanced around 16 weeks.
If a child is having trouble making eye contact after they’ve passed this point, this could be an indicator that they’re dealing with Autism Spectrum Disorder (ASD) or another disability.
Children with autism tend to struggle to make eye contact, and they may also show a lack of responsiveness to others. For example, they may not smile, speak, or respond to their name.
Autism Spectrum Disorders range greatly in severity, and it’s important to work with a team of doctors and therapists to provide your child with adequate support, especially if their symptoms fall on the more severe end.
- Difficulty Speaking
Children with Autism Spectrum Disorder often have trouble speaking. They may not start speaking at the same time as their peers, for example, or they may not speak at all.
They may not start speaking at the same time as their peers, for example, or they may not speak at all.
Difficulty speaking can also be an indicator of various phonemic awareness-based learning disabilities. These disabilities can be seen in very young children who have trouble pronouncing words, rhyming, or handling other language skills that kids their age are capable of.
Children who have a family history of reading or writing challenges should also be closely monitored when they reach preschool or kindergarten age. They may be more likely to struggle with these issues and will need extra support.
- Difficulty Reading and Spelling
As they get older and start attending school, some children may have a difficult time reading, pronouncing words, and spelling words correctly. In some cases, this can be a sign of dyslexia, a disability that affects a person’s ability to consistently link written words and letters with the sounds they make.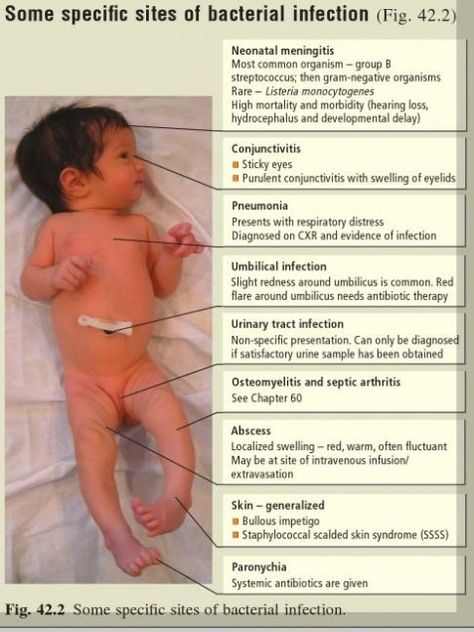
Dyslexia does not affect a person’s intelligence, but it can make reading very challenging. It may be characterized by late talking, being slow to learn new words, and a delay in learning how to read.
- Difficulty Understanding Lessons or Retaining Information
Some children struggle with learning disabilities. This, in turn, makes it hard for them to understand school lessons or retain information as it’s relayed to them.
Some signs that a child is dealing with a learning disability include not being able to recognize letters, not being interested in reading or writing, not understand instructions, or having difficulty holding and writing with a pencil. This challenges may also be accompanied by difficulty sitting still or staying focused.
- Poor Muscle, Speech, and Vision Control
Cerebral palsy is a brain disorder that affects coordination, movement, and posture. It often is not diagnosed until a child is age 2 or older.
One of the most common warning signs of cerebral palsy is missing key developmental milestones like sitting up, holding up one’s head, and crawling. Difficulties with speaking and vision are common, too.
How to Support a Child with Special Needs
Do any of these warnings signs stand out to you? Do you suspect your child has special needs? If so, it’s important to consult their pediatrician right away.
If your child is diagnosed with autism, dyslexia, cerebral palsy, or any other type of disability, their pediatrician can refer you to other professionals who can help them (and you) manage their condition and overcome many of the challenges they’re facing. This list includes speech therapists, occupational therapists, and physical therapists, as well as private tutors and in-home caregivers.
As a parent to a child with special needs, it’s also important to advocate for your child when they start attending school. Learn all you can about their condition and encourage their teachers to have a look at various resources as well. This ensures everyone is on the same page and makes it easier to create a game plan to give your child the support and attention they need.
This ensures everyone is on the same page and makes it easier to create a game plan to give your child the support and attention they need.
Do You Suspect You Have a Special Needs Child?
Children with special needs often can and do lead healthy, happy, and productive lives. The key is getting them the support they need sooner rather than later.
If, after reading through the signs listed above, you suspect your child has special needs, reach out to a healthcare professional right away. They can perform the proper tests and refer you to other professionals for a more complete diagnosis.
In the meantime, if you want to learn more about caring for and supporting a child with special needs, check out the Children’s Health section of our site today.
Sitemap
State autonomous professional
educational institution
Republic of Bashkortostan
"Salavat Medical College"
453261 Republic of Bashkortostan
Salavat, st. Furmanova, 4
Furmanova, 4
Phone/fax: (3476)-38-78-83
e-mail: [email protected]
- College information
- Basic information
- Structure and governing bodies of the college
- Documents
- Education
- Educational standards and requirements
- Manual. Teaching staff
- Logistics and equipment of the educational process
- Scholarships and other financial support
- Paid educational services
- Financial and business activities
- Vacancies for reception (transfer)
- Personal data processing
- Anti-corruption
- Legal framework for combating extremism and terrorism
- Vacancies
- Information security
- Olympics
- Mentoring
- Available environment
- International cooperation
- Applicant
- Applicant
- Control figures for the reception of citizens
- Admission Rules
- Regulations on Individual Achievements
- Local regulations
- List of specialties
- Document acceptance schedule
- Terms of admission under contracts for the provision of paid educational services
- Information on the need for applicants to undergo a mandatory preliminary medical examination (examination)
- Exemplary entrance tests
- Features of conducting entrance examinations for the disabled and persons with disabilities
- Information about the possibility of filing documents by mail
- Submission of documents by e-mail
- List and deadlines for submission of documents
- Information on the availability of a hostel and the number of places in hostels allocated for nonresident applicants
- Enrollment Orders
- Number of applications submitted
- Filing and hearing appeals
- College Application
- Appeal of citizens on admission issues
- Targeted training
- Consent to the processing of personal data
- Entrance examinations
- Rating of applicants
- student
- Fundamentals
- Regulations
- Culture and sports
- Dormitory
- Student Council
- Life safety
- Teaching materials
- Employment of graduates
- Graduate Accreditation
- Page of educational psychologist
- Student Union
- Scholarship of the Head of the Republic of Bashkortostan
- teacher
- Reference information
- Educational and methodical work
- Additional education
- Republican information and training pedagogical seminars
- Contacts
- Hotline
- Feedback
- Contacts of controlling organizations
This page does not exist.
|
Need for communication: congenital or acquired?
As you know, L.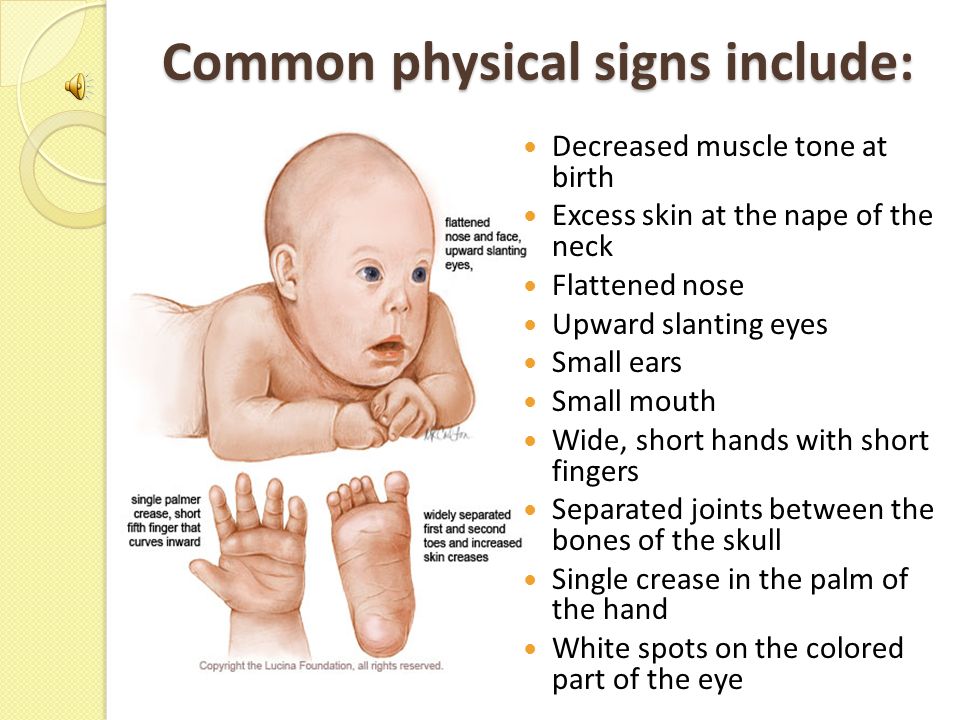 S. Vygotsky called the infant the most social being, since the satisfaction of all his needs is carried out by another person. “From here it is clear,” writes L.S. Vygotsky, “why any need of an infant, whatever this need may be, gradually, in the process of development, becomes for him a need for another person, for contact with a person, for communication with him” 1.
S. Vygotsky called the infant the most social being, since the satisfaction of all his needs is carried out by another person. “From here it is clear,” writes L.S. Vygotsky, “why any need of an infant, whatever this need may be, gradually, in the process of development, becomes for him a need for another person, for contact with a person, for communication with him” 1.
Analyzing the social situation of an infant's development, L.S. Vygotsky comes to the conclusion that, starting from the first days of life, the objective conditions for the development of a child create the necessary prerequisites for the emergence of a need for communication, which is social both in its content and in origin. This need is the basis and driving force of all further mental development of the child 2. L.S. Vygotsky believed that the need for communication is formed in vivo on the basis of primary biological needs - for food, warmth, movement, etc.
Developing the views of L.S. Vygotsky about the lifetime formation of the child's need for communication, L. I. Bozhovich believed that primary biological needs cannot be considered the basis for the development of this need, and put forward a number of arguments in defense of this statement. First, if the need for communication were built only on the basis of biological needs, it could not be considered truly social during this period, since most animals have the same need for maternal care and dependence on the mother. Secondly, it remains unclear how the need for a mother, as a creature that satisfies the biological needs of the child, develops into a social need for communication 3.
I. Bozhovich believed that primary biological needs cannot be considered the basis for the development of this need, and put forward a number of arguments in defense of this statement. First, if the need for communication were built only on the basis of biological needs, it could not be considered truly social during this period, since most animals have the same need for maternal care and dependence on the mother. Secondly, it remains unclear how the need for a mother, as a creature that satisfies the biological needs of the child, develops into a social need for communication 3.
In addition, says L.I. Bozhovich, “the question arises whether the need for communication, so understood, can be the leading factor in the mental development of the child. Indeed, in this case, if communication is built around the cleanliness of the child, his feeding, etc., then the true development of specifically human forms of the psyche will very soon come to a standstill. It is also difficult to imagine the possibility that these instinctive needs could develop into the highest spiritual needs of a person” 4.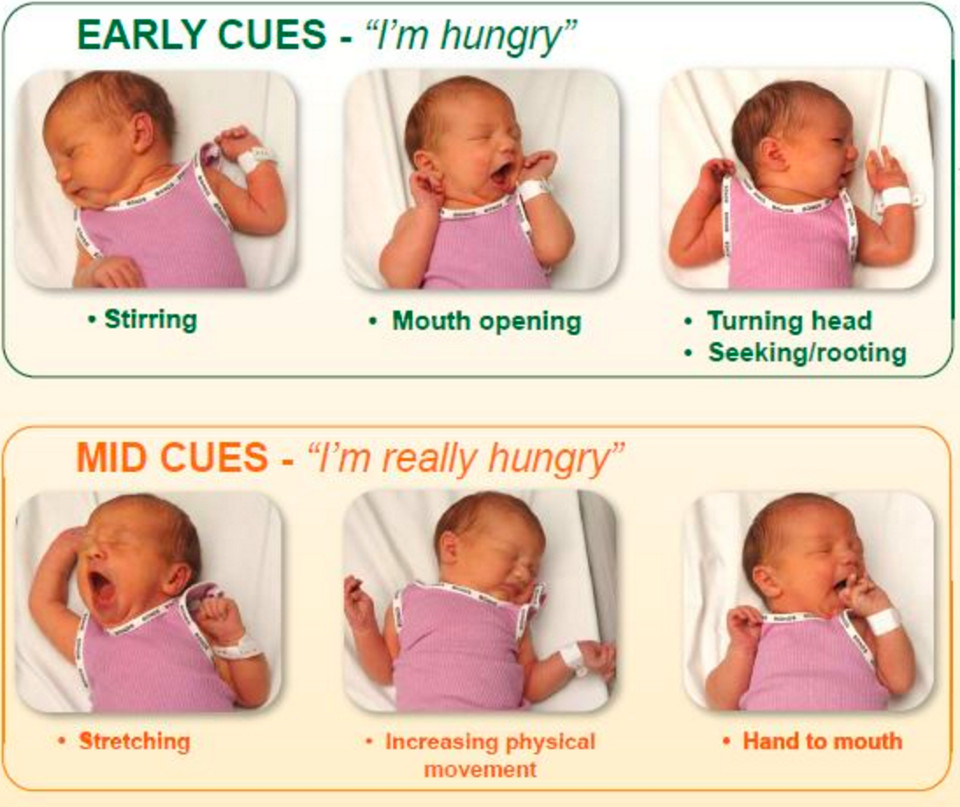 As a result, L.I. Bozovic puts forward a hypothesis about the existence of another primary need, which is basic for the need for communication. Such a need, from her point of view, is the need for new experiences, observed approximately at the 3-5th week of a child's life.
As a result, L.I. Bozovic puts forward a hypothesis about the existence of another primary need, which is basic for the need for communication. Such a need, from her point of view, is the need for new experiences, observed approximately at the 3-5th week of a child's life.
Although very little was known about this need in the 1970s, some of its main characteristics testified to its uniqueness and special significance for mental development. Thus, it was shown that the need for new impressions is most clearly manifested in visual concentration during the transition of children from the neonatal period to infancy and changes all their behavior and the nature of emotional experiences (N.L. Figurin, R.Ya Lekhtman-Abramovich and others. ). Let us consider this transition associated with the emergence of the need for new impressions in more detail.
The generally accepted point of view was that in the neonatal period a child does not have even the most elementary images and ideas about the world around him, and his mental life can be defined as an alloy of undifferentiated emotionally colored sensations caused by organic needs and their satisfaction. At the same time, the inability to perceive objects of the outside world deprives newborns of purposeful activity (W. Stern, K. Buhler, K. Koffka).
At the same time, the inability to perceive objects of the outside world deprives newborns of purposeful activity (W. Stern, K. Buhler, K. Koffka).
It was assumed that such content of the mental life of newborns is determined by the level of maturity of their nervous system and the situation of development, i.e. total dependence on the adult caring for the child. “In essence,” writes L.I. Bozhovich, “newborn is only a transitional stage from intrauterine to extrauterine existence, a period during which the newborn continues to develop according to the type of fetus” 5.
By the end of the first month of life, when the neonatal period ends, the child is separated from the mother not only physically, but also mentally, it is believed that during this period he has an “individual mental life” (L.S. Vygotsky). The transition to an individual mental life is physiologically connected with a certain level of development of the visual analyzer, and psychologically with the development of a new need for impressions of the external world.
During the transition to the period of infancy, active wakefulness appears in the child's behavior, which is filled with the perception of stimuli from the outside world and is accompanied by a joyful emotional state. The main thing is that along with the need for new impressions, purposeful cognitive activity is born, the search for new impressions from the objects of the outside world.
What is the qualitative difference between the need for new impressions and other biological needs?
First of all, it is associated not with negative, but with positive emotions, therefore, marks "the desire to achieve, and not the desire to get rid of something that interferes with the normal existence of the body" 6. In addition, unlike other organic needs , the need for new experiences is, as it were, insatiable. And, finally, the need for new impressions has a promising character, it is progressive by its very nature, as it is associated with the development of the human brain, due to the active cognitive activity of the subject.
L.I. Bozovic considers the need for impressions as the basis for the development of social needs. Developing and becoming more complex, this primary need stimulates the child's diverse and multifaceted research activity and, already on its basis, a cognitive need, "which pushes the child to enter the environment wider and deeper and master it" 7.
The child cannot be without the help of adults develop new forms of cognitive activity and satisfy their need for new, more complex information about the world around them. Therefore, in order to satisfy the cognitive need, the child needs other people, and, consequently, the development of social forms of communication between the child and the adult takes place. At the same time, L.I. Bozhovich notes that the need for communication, which arises on the basis of the need for new impressions and is initially inseparable from it, later acquires an independent meaning for the child and makes its own path of development.
Thus, in accordance with the views of L. I. Bozovic, the primary force that stimulates the mental development of a child is the need for new experiences. It is involved in the formation of complex functional systems of the brain, then it is transformed into a cognitive need, which becomes the basis for the development of needs for communication and movement. The need for communication then develops on the basis of cooperation between an adult and a child, their joint activities, games, and various types of children's productive activities. And the need for movement becomes a need for mastery, assimilation of a system of skills and abilities 8.
I. Bozovic, the primary force that stimulates the mental development of a child is the need for new experiences. It is involved in the formation of complex functional systems of the brain, then it is transformed into a cognitive need, which becomes the basis for the development of needs for communication and movement. The need for communication then develops on the basis of cooperation between an adult and a child, their joint activities, games, and various types of children's productive activities. And the need for movement becomes a need for mastery, assimilation of a system of skills and abilities 8.
M.I. also contributed to the understanding of the sources of the need for communication. Lisin in his concept of the genesis of communication in ontogenesis. M.I. Lisina agreed that the need for communication is based on other needs, but is not limited to them. First, the organic needs of the child are among the sources of the need for communication. Being helpless and not being able to satisfy independently the need for food, warmth, etc. , the baby signals uncomfortable conditions; his cries, movements, facial expressions objectively become signals for adults caring for him. Secondly, the source of the need for communication is the need for new experiences. From the point of view of satisfying this need, the other person turns out to be the most informative object in the world around the baby 9.
, the baby signals uncomfortable conditions; his cries, movements, facial expressions objectively become signals for adults caring for him. Secondly, the source of the need for communication is the need for new experiences. From the point of view of satisfying this need, the other person turns out to be the most informative object in the world around the baby 9.
However, according to M.I. Lisina, crucial for the emergence of the actual need for communication is related to the child of an adult, his position regarding the child. The fact is that an adult from the very beginning treats the child as a subject, a person and behaves with him as a communication partner, endowing his actions with a sense and meaning in advance, which they do not yet have. Such behavior of an adult, setting, as it were, a “zone of proximal development” (in the words of L.S. Vygotsky), actualizes the child’s perception of an adult not only as a passive object of the external world, but also as an actively acting subject, and also provides the child with the opportunity to discover subjective, personal qualities and in yourself.
Communication does not occur immediately after birth, it develops gradually and is observed in infants at the beginning of the second month of life under adequate educational conditions. M.I. Lisina singled out the criteria for the formation of a need for communication: 1) the child's attention and interest in an adult, reflecting his focus on adult cognition; 2) emotional manifestations of the child in relation to the adult, expressing his assessment of the adult; 3) initiative actions of the child aimed at attracting the attention of an adult, for example, demonstrating their skills and abilities; 4) the emergence of a child's sensitivity to the attitude of an adult 10.
The neonatal period acts as a preparatory stage, during which the child learns to single out an adult, to focus attention on him, which is the first sign of emerging communication. The appearance of a response smile to the influence of an adult marks the transition to the next stage: to the appearance of the first situational-personal form of communication and the formation of the first leading activity - directly emotional communication 11. During the first 4-6 weeks of life, the infant gradually masters various means to establish contact with at the end of the second month, he himself begins to influence others, encouraging them to communicate. The main form of a child's behavior at this age is the "animation complex", which includes motor animation, a smile, and vocalizations of pleasure. An adult reinforces the initiative of the child, responding with a smile and an affectionate conversation to his calls, emotional communication is established between them - an exchange of positive expressions. At the same time, the infant uses all the expressive-mimic means available to him to attract and hold the attention of an adult.
During the first 4-6 weeks of life, the infant gradually masters various means to establish contact with at the end of the second month, he himself begins to influence others, encouraging them to communicate. The main form of a child's behavior at this age is the "animation complex", which includes motor animation, a smile, and vocalizations of pleasure. An adult reinforces the initiative of the child, responding with a smile and an affectionate conversation to his calls, emotional communication is established between them - an exchange of positive expressions. At the same time, the infant uses all the expressive-mimic means available to him to attract and hold the attention of an adult.
In the conditions of a family, children already at the 2nd month of life are not limited only to the reciprocal manifestation of love for an adult, but also show their own initiative. Thus, the components that make up the “revitalization complex” ensure that the child successfully separates an adult from the environment (freezing), performs mimic (smile) and specific vocal (humming) communication with him, as well as actively attracts an adult to communication (movements of limbs and bodies).
The main content of the need for communication at this stage is the need for the benevolent attention of an adult, whom the child perceives as a subject, a communication partner.
Direct-emotional communication with an adult in the first six months of life acts as the leading activity of the child. 12. Direct-emotional communication forms other types of activity: cognitive activity, objective actions. In the process of communication, the development of emotional, cognitive processes takes place, the formation of an affective connection with a close adult, the fundamental principles of the personality and self-awareness of the child begin to take shape. . L.S. Vygotsky assumed that communication develops on the basis of adult satisfaction of the biological needs of the child. L.I. Bozovic put forward a hypothesis about the need for new experiences as a basis for the development of social communication. M.I. Lisina combined these points of view and considered two sources for the development of the need for communication - organic needs and the need for new impressions.
Foreign psychology is dominated by the idea that a child is a social being from birth. Therefore, the main content of a child's development in early childhood is considered to be the formation and natural change of his social and emotional relationships with other people, primarily with his mother. At the same time, the inseparability of the cognitive, social and emotional development of the child is emphasized.
Currently, there are many facts that testify to the social competence of an infant already from the neonatal period. This is data on the presence of special abilities of visual and auditory perception, facial expressions, intermodal synthesis and imitation that are important for communication, as well as on the social signals sent by the child and his ability to participate in social interaction.
Features of the infant's visual perception. Babies begin to react to people from the first days of life. Already in the first hours after birth, newborns prefer the face of a person, located at a distance of twenty centimeters, to other stimuli; it is at this distance that the mother's face is when she holds the child in her arms during feeding. Infants are hypothesized to have an innate “face” schema 14. This is supported by evidence that newborns prefer to look at stimuli that look like a human face rather than drawings with jumbled facial parts, and also follow a moving face with more interest than behind another moving object 15.
Infants are hypothesized to have an innate “face” schema 14. This is supported by evidence that newborns prefer to look at stimuli that look like a human face rather than drawings with jumbled facial parts, and also follow a moving face with more interest than behind another moving object 15.
Human face sensitivity allows babies to recognize their mother's face very early. During the first hours after birth, there is a sensitive period when the newborn is awake and able to capture the individual features of the mother's face. In a study by J. Walton and T. Bauer in 1991, it was shown that already 7 hours after birth, babies prefer to look at a color image of their mother on a computer screen, and not at the face of a stranger with hair of the same color. The preference was not for any particular attribute, but for the person as such 16.
In Carpenter's experiments in 1974, two-week-old newborns were shown images of the faces of their mother and a stranger. Infants clearly preferred to look at a familiar face and often completely turned away from an unfamiliar image. Newborns of 5 days of age were supported in a sitting position in front of a large white screen in which two slots were made at a distance of 12 cm from the midline on each side. The child's mother and a woman unknown to him, similar in color and length of hair to her, sat behind the screen so that their heads were visible through the slits. The demonstration of faces lasted 20 seconds. The results showed that babies preferred to look at their own mother's face 18.
Newborns of 5 days of age were supported in a sitting position in front of a large white screen in which two slots were made at a distance of 12 cm from the midline on each side. The child's mother and a woman unknown to him, similar in color and length of hair to her, sat behind the screen so that their heads were visible through the slits. The demonstration of faces lasted 20 seconds. The results showed that babies preferred to look at their own mother's face 18.
When perceiving a person, not only the face attracts the child's attention. At the age of 3 months, babies are able to recognize the schematic image of a walking person. In experiments three and five month old children observed the movement of 11 points of light on the screen, depicting a walking person in one case, and randomly moving points in the other. Children saw the difference between these two configurations, preferring to look at a moving person 19.
It is shown that infants view a human face and inanimate objects differently. Looking at the face, they utter more sounds, begin to move their arms and legs, clench and unclench their fists, make smooth movements 20.
Looking at the face, they utter more sounds, begin to move their arms and legs, clench and unclench their fists, make smooth movements 20.
Infants are able to distinguish facial expressions of adults. In experiments with the presentation of photographs first with one and then with another facial expression in terms of the oculomotor system and habituation, it was found that newborns are able to distinguish between expressions of happiness, sadness, surprise, and at a later age they distinguish between slides with an expression of joy, anger and a neutral expression. faces. In this case, infants are better at distinguishing positive facial expressions than negative or neutral ones 21.
Peculiarities of baby's auditory perception. Babies show not only visual but also auditory preferences. Apparently, there is an innate ability to distinguish between speech and non-speech sounds. Children clearly prefer the human voice to sounds of the same pitch and loudness, and they distinguish coherent speech from a set of meaningless syllables.
Newborns are able to distinguish their mother's voice from the voices of other women. This may be based on the memorization of the mother's voice by the child even in the period of intrauterine development. Decasper and Phifer in their study 19The 1980s put this assumption to the test. During the last third of the pregnancy, the mothers read the same story aloud. On the first day of life, the newborn was allowed to listen through headphones to a recording of the same story performed by the mother and a stranger. During listening, the infants sucked on the pacifier, and it turned out that the sucking rhythm synchronized with the speech of the mother faster than with the speech of a stranger, which indicates a prenatal formation of a preference for the mother's voice.
Infants prefer female voices to male voices (one octave lower on average). Perhaps that is why adults and children usually speak to the infant in a higher voice, as if they "know" about his preferences. The infant has an innate coordination between sight and hearing, which helps to recognize different people and, above all, to recognize the mother.
E. Spelke's experiments showed that a few months after birth, babies can recognize the voices of their mother and father. The infants were given a tape recording of the voice of one of the parents through a loudspeaker that was placed exactly between the father and the mother. The parents sat without speaking and did not move their lips. Already 3-month-old babies looked at their mother when they heard their mother's voice and at their father if his voice sounded. This allows us to conclude that three-month-old infants are able to form certain ideas about the voice and appearance of those who care for them.
Ability to imitate. Jean Piaget believed that babies cannot imitate the actions of another person until they reach the age of 6 months. However, in the well-known experiments of E. Meltzoff and M. Moore in 1977, it was found that newborns at the age of two to three weeks are able to imitate many facial movements of adults, such as sticking out the tongue, opening and closing the mouth, protruding lips. E. Wiener's research, conducted in 1986, confirmed these data and showed that newborns are able to imitate facial movements as early as seven days of age. In addition, they can also imitate finger movements, provided that they have been able to observe how adults perform such movements.
E. Wiener's research, conducted in 1986, confirmed these data and showed that newborns are able to imitate facial movements as early as seven days of age. In addition, they can also imitate finger movements, provided that they have been able to observe how adults perform such movements.
Imitation in newborns is seen as another example of intermodal interaction, where infants match facial or hand movements observed in an adult with their own. Imitation in an infant serves to establish contact with parents.
Social cues in the infant's behavioral repertoire. Babies change their facial expressions already in the first weeks of life, and many parents interpret this as joy, anger, surprise, fear, sadness or interest maturity, and the movements of the facial muscles are combined into recognizable configurations that have the value of social signals. One study videotaped infants playing with their mothers and unfamiliar adults. When viewing slides and videos, mothers could categorize the baby's facial expressions as similar to universal adult facial expressions. Thus, it has been shown that facial expressions of an infant as early as 2-4 months old can be easily recognized and classified using the same categories as for identifying adult facial expressions. Parents are guided by the expression on the face of the child, interacting with him.
Thus, it has been shown that facial expressions of an infant as early as 2-4 months old can be easily recognized and classified using the same categories as for identifying adult facial expressions. Parents are guided by the expression on the face of the child, interacting with him.
An infant's cry is also seen as an important social signal. It is shown that crying is as unique a characteristic of an infant as fingerprints, and enables the mother to recognize her child already on the second day after birth. In addition, crying is not uniform and can convey different messages about the infant's condition, which the mother learns to recognize. Crying causes not only a reaction of empathy and a desire to help, show care, but also a feeling of emotional discomfort, prompts an adult nearby to eliminate the causes that caused it 24.
Among the infant's social signals that regulate interaction, there are two groups: signals of attracting attention and initiating interaction, and signals of avoiding or wanting to stop interactions. In addition, "light" and "explicit" signals of both groups are distinguished. In the first month of life, signals of the newborn's readiness for interaction (a "light" invitation) are revival on the face, opening the arms with slightly bent fingers, raising the head and reducing body movements, and freezing. Clear signals are vocalizations, a smile, a look into the eyes, cyclic movements of the arms and legs. The signals of the desire to interrupt the interaction in the first month of life are considered lip tightening, a grimace on the face, a frown in the eyes, blinking or closing the eyes, looking away, accompanied by increased sucking movements, whimpering, hiccups, clenching hands, bringing hands to the head (neck, face ), stretching arms and legs, increased movement of the legs. Obvious signals of the child's desire to interrupt the interaction are a whining face, whimpering, crying, coughing, looking away, head turning, pushing away, closed postures 25.
In addition, "light" and "explicit" signals of both groups are distinguished. In the first month of life, signals of the newborn's readiness for interaction (a "light" invitation) are revival on the face, opening the arms with slightly bent fingers, raising the head and reducing body movements, and freezing. Clear signals are vocalizations, a smile, a look into the eyes, cyclic movements of the arms and legs. The signals of the desire to interrupt the interaction in the first month of life are considered lip tightening, a grimace on the face, a frown in the eyes, blinking or closing the eyes, looking away, accompanied by increased sucking movements, whimpering, hiccups, clenching hands, bringing hands to the head (neck, face ), stretching arms and legs, increased movement of the legs. Obvious signals of the child's desire to interrupt the interaction are a whining face, whimpering, crying, coughing, looking away, head turning, pushing away, closed postures 25.
Ability for social interaction. In the 1970s, the use of video recording and frame-by-frame analysis of video materials allowed psychologists to conclude that a child has innate abilities for social interaction, establishing a connection with his mother.
In the 1970s, the use of video recording and frame-by-frame analysis of video materials allowed psychologists to conclude that a child has innate abilities for social interaction, establishing a connection with his mother.
Mutual adjustment can already be observed in the feeding situation. During feeding, an infant has been found to suckle at the breast in bursts lasting 8 to 10 seconds, interrupted by pauses of 2 to 5 seconds. At the same time, from the point of view of the transfer of breath and rest, there is no need for these pauses. Most mothers, regardless of the nature of feeding (breastfeeding or bottle feeding), during pauses, pat the baby, stimulating him to continue sucking, although he begins to suck without any action from the mother. Since no physiological reasons for pauses have been identified, it has been suggested that they are necessary to establish the first dialogue between the infant and the mother, which looks like an alternation between the baby suckling, pauses and tactile stimulation from the mother 26.
Katherine Garvey in 1977 studied the synchronization of mother and 4-month-old infants during stereotyped play and found that the child participates in play by looking at the mother. He alternately looks at an adult showing him a “goat” or making “patties”, then looks away, and then again directs his gaze to the adult’s face, thereby helping to establish the pace and rhythm of the interaction. After 4 months, infants regulate interaction not only with a look, but also with a gesture.
In the studies of D.L. Stern (1977) showed that the movements of a mother and a 3-month-old baby during interaction are a very precise harmonious combination of mutual approaches and removals, resembling a kind of "waltz". The study of how the mother and child look at each other during the interaction made it possible to identify such an organization of their actions that can be compared with the exchange of replicas of adult communication partners. It is based on the alternation of the roles of the actor and the observer, the sequential switching on and off of activity 27. To describe the positive interaction in the dyad, research uses such descriptive characteristics as reciprocity, synchronicity, elusive ballet, attunement to each other 28.
To describe the positive interaction in the dyad, research uses such descriptive characteristics as reciprocity, synchronicity, elusive ballet, attunement to each other 28.
In the study of mother-infant interaction, special attention is paid to the study of intersubjectivity. Under experimental conditions, the behavior of five infants aged from one week to six months was filmed in two situations: when the mother was next to the child and when the mother was absent, and a bright toy lay in front of the child. According to the results of the experiments, it turned out that the behavior of infants in response to the presence of the mother and the behavior in response to an inanimate object differ significantly. The infant produces, as it were, two modes of spontaneous activity, two different "interests" in living and inanimate objects. The greatest differences were recorded in facial expressions, vocal responses, and hand position during the perception of the mother and the toy already from the first weeks of life. In addition, characteristic changes in the movement of the fingers, tongue, and lips during the perception of the mother's speech were revealed, which had never been observed in response to the presentation of a toy. The facts obtained indicate that already in the first weeks of life, infants are capable of perceiving people and inanimate objects as completely different..
In addition, characteristic changes in the movement of the fingers, tongue, and lips during the perception of the mother's speech were revealed, which had never been observed in response to the presentation of a toy. The facts obtained indicate that already in the first weeks of life, infants are capable of perceiving people and inanimate objects as completely different..
K. Trevarten suggested that already two-month-old infants in interaction with an adult in some way feel their ability to act, have a sense of subjectivity. But even more surprising is that they have an idea of the relationship between their own behavior and the behavior of another person, a partner in interaction. Trevarten called this primary intersubjectivity, an innate form of adjustment that provides the infant with the ability to interact with other people 30.
Over the next few months, cognitive development and interpersonal experiences lead the infant to increase his ability to understand the desires and behaviors of others. Around the age of 8-9 months, secondary intersubjectivity is formed - an understanding that there are other people in the world, and objects of the outside world can be the focus of joint activities of a child and an adult. It is assumed that during this period the child shows interest in what other people know about the surrounding objects and how they know how to act with them 31.
Around the age of 8-9 months, secondary intersubjectivity is formed - an understanding that there are other people in the world, and objects of the outside world can be the focus of joint activities of a child and an adult. It is assumed that during this period the child shows interest in what other people know about the surrounding objects and how they know how to act with them 31.
Another line of research developed with the discovery of “mirror neurons” in the 1990s by Rizzolatti and Arbib. or another action, but also when she sees how this action is performed by others. These neurons were called mirror neurons and were soon found in the human cerebral cortex, and not only in the motor area. Mirror systems exist in almost all parts of the human brain, and they are activated, including when anticipating an action, when remembering emotions, when empathizing with the emotions of another person, etc. Mirror neurons are the natural basis that provides social behavior, helps to understand the intentions, actions of another person, to show empathy 33.