Signs of infection miscarriage
Miscarriage | NCH Healthcare System
Overview
Miscarriage is the spontaneous loss of a pregnancy before the 20th week. About 10 to 20 percent of known pregnancies end in miscarriage. But the actual number is likely higher because many miscarriages occur very early in pregnancy — before you might even know about a pregnancy.
The term “miscarriage” might suggest that something went wrong in the carrying of the pregnancy. But this is rarely true. Most miscarriages occur because the fetus isn’t developing as expected.
Miscarriage is a relatively common experience — but that doesn’t make it any easier. Take a step toward emotional healing by understanding what can cause a miscarriage, what increases the risk and what medical care might be needed.
Symptoms
Most miscarriages occur before the 12th week of pregnancy.
Signs and symptoms of a miscarriage might include:
- Vaginal spotting or bleeding
- Pain or cramping in your abdomen or lower back
- Fluid or tissue passing from your vagina
If you have passed fetal tissue from your vagina, place it in a clean container and bring it to your health care provider’s office or the hospital for analysis.
Most women who have vaginal spotting or bleeding in the first trimester go on to have successful pregnancies.
Causes
Problems with the genes or chromosomes
Most miscarriages occur because the fetus isn’t developing as expected. About 50 percent of miscarriages are associated with extra or missing chromosomes. Most often, chromosome problems result from errors that occur by chance as the embryo divides and grows — not problems inherited from the parents.
Chromosome problems might lead to:
- Blighted ovum. Blighted ovum occurs when no embryo forms.
- Intrauterine fetal demise. In this situation, an embryo forms but stops developing and dies before any symptoms of pregnancy loss occur.
Molar pregnancy and partial molar pregnancy. With a molar pregnancy, both sets of chromosomes come from the father. A molar pregnancy is associated with abnormal growth of the placenta; there is usually no fetal development.

A partial molar pregnancy occurs when the mother’s chromosomes remain, but the father provides two sets of chromosomes. A partial molar pregnancy is usually associated with abnormalities of the placenta, and an abnormal fetus.
Molar and partial molar pregnancies are not viable pregnancies. Molar and partial molar pregnancies can sometimes be associated with cancerous changes of the placenta.
Maternal health conditions
In a few cases, a mother’s health condition might lead to miscarriage. Examples include:
- Uncontrolled diabetes
- Infections
- Hormonal problems
- Uterus or cervix problems
- Thyroid disease
What does NOT cause miscarriage
Routine activities such as these don’t provoke a miscarriage:
- Exercise, including high-intensity activities such as jogging and cycling.
- Sexual intercourse.
- Working, provided you’re not exposed to harmful chemicals or radiation. Talk with your doctor if you are concerned about work-related risks.
Risk factors
Various factors increase the risk of miscarriage, including:
- Age. Women older than age 35 have a higher risk of miscarriage than do younger women. At age 35, you have about a 20 percent risk. At age 40, the risk is about 40 percent. And at age 45, it’s about 80 percent.
- Previous miscarriages. Women who have had two or more consecutive miscarriages are at higher risk of miscarriage.
- Chronic conditions. Women who have a chronic condition, such as uncontrolled diabetes, have a higher risk of miscarriage.
- Uterine or cervical problems. Certain uterine conditions or weak cervical tissues (incompetent cervix) might increase the risk of miscarriage.
- Smoking, alcohol and illicit drugs. Women who smoke during pregnancy have a greater risk of miscarriage than do nonsmokers. Heavy alcohol use and illicit drug use also increase the risk of miscarriage.
- Weight. Being underweight or being overweight has been linked with an increased risk of miscarriage.
- Invasive prenatal tests. Some invasive prenatal genetic tests, such as chorionic villus sampling and amniocentesis, carry a slight risk of miscarriage.
Complications
Some women who miscarry develop an infection in the uterus. This is also called a septic miscarriage. Signs and symptoms of this infection include:
- Fever
- Chills
- Lower abdominal tenderness
- Foul-smelling vaginal discharge
Prevention
Often, there’s nothing you can do to prevent a miscarriage. Simply focus on taking good care of yourself and your baby:
- Seek regular prenatal care.
- Avoid known miscarriage risk factors — such as smoking, drinking alcohol and illicit drug use.
- Take a daily multivitamin.
- Limit your caffeine intake. A recent study found that drinking more than two caffeinated beverages a day appeared to be associated with a higher risk of miscarriage.
If you have a chronic condition, work with your health care team to keep it under control.
Diagnosis
Your health care provider might do a variety of tests:
- Pelvic exam. Your health care provider might check to see if your cervix has begun to dilate.
- Ultrasound. During an ultrasound, your health care provider will check for a fetal heartbeat and determine if the embryo is developing as it should be. If a diagnosis can’t be made, you might need to have another ultrasound in about a week.
- Blood tests. Your health care provider might check the level of the pregnancy hormone, human chorionic gonadotropin (HCG), in your blood and compare it to previous measurements. If the pattern of changes in your HCG level is abnormal, it could indicate a problem. Your health care provider might check to see if you’re anemic — which could happen if you’ve experienced significant bleeding — and may also check your blood type.
- Tissue tests. If you have passed tissue, it can be sent to a lab to confirm that a miscarriage has occurred — and that your symptoms aren’t related to another cause.
- Chromosomal tests. If you’ve had two or more previous miscarriages, your health care provider may order blood tests for both you and your partner to determine if your chromosomes are a factor.
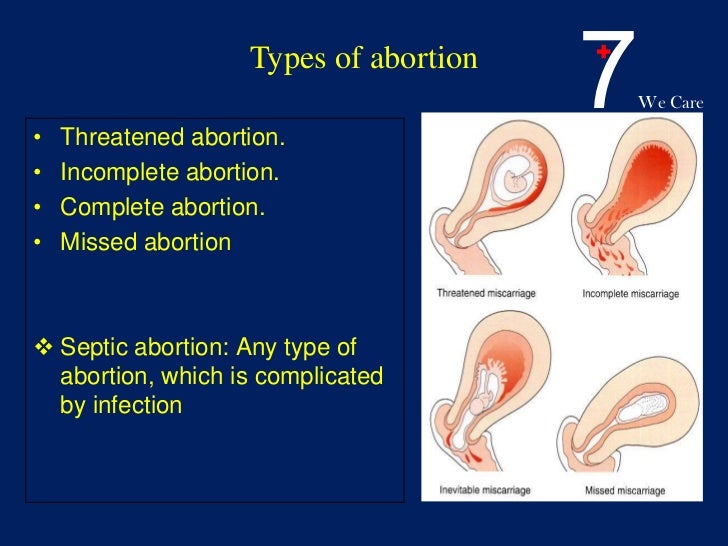
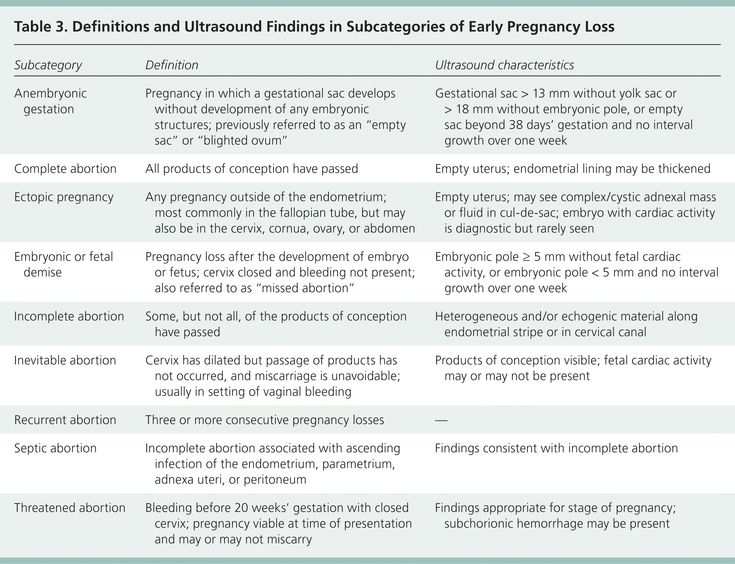
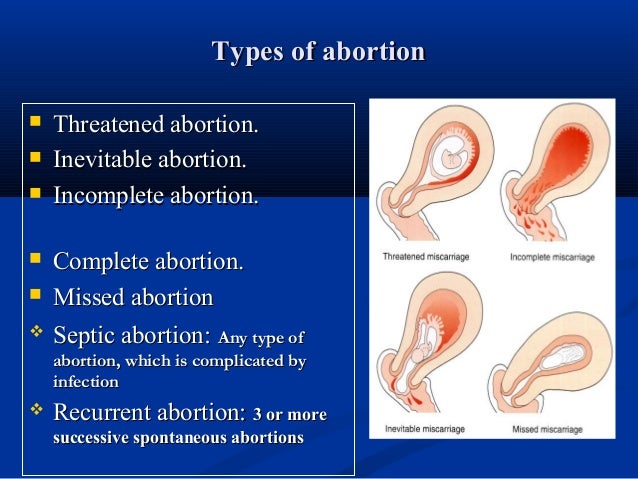
Possible diagnoses include:
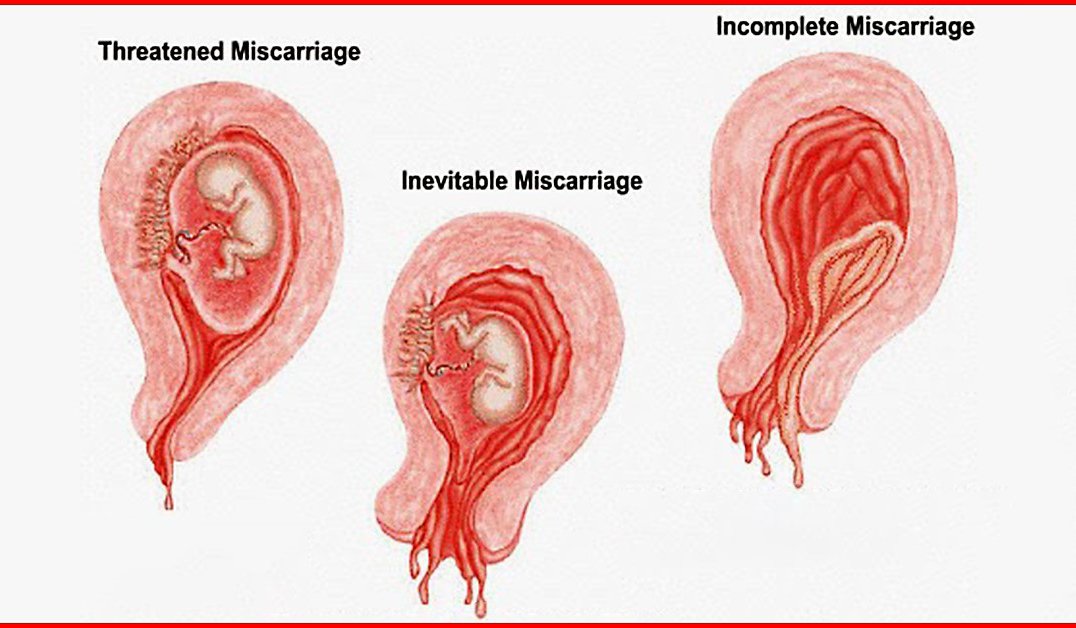
- Threatened miscarriage. If you’re bleeding but your cervix hasn’t begun to dilate, there is a threat of miscarriage. Such pregnancies often proceed without any further problems.
- Inevitable miscarriage. If you’re bleeding, cramping and your cervix is dilated, a miscarriage is considered inevitable.
- Incomplete miscarriage. If you pass fetal or placental material but some remains in your uterus, it’s considered an incomplete miscarriage.
- Missed miscarriage.
 In a missed miscarriage, the placental and embryonic tissues remain in the uterus, but the embryo has died or was never formed.
In a missed miscarriage, the placental and embryonic tissues remain in the uterus, but the embryo has died or was never formed. - Complete miscarriage. If you have passed all the pregnancy tissues, it’s considered a complete miscarriage. This is common for miscarriages occurring before 12 weeks.
- Septic miscarriage. If you develop an infection in your uterus, it’s known as a septic miscarriage. This can be a severe infection and demands immediate care.
Treatment
Threatened miscarriage
For a threatened miscarriage, your health care provider might recommend resting until the bleeding or pain subsides. Bed rest hasn’t been proved to prevent miscarriage, but it’s sometimes prescribed as a safeguard. You might be asked to avoid exercise and sex, too. Although these steps haven’t been proved to reduce the risk of miscarriage, they might improve your comfort.
In some cases, it’s also a good idea to postpone traveling — especially to areas where it would be difficult to receive prompt medical care. Ask your health care provider if it would be wise to delay any upcoming trips you’ve planned.
Ask your health care provider if it would be wise to delay any upcoming trips you’ve planned.
Miscarriage
With ultrasound, it’s now much easier to determine whether an embryo has died or was never formed. Either finding means that a miscarriage will definitely occur. In this situation, you might have several choices:
- Expectant management. If you have no signs of infection, you might choose to let the miscarriage progress naturally. Usually this happens within a couple of weeks of determining that the embryo has died. Unfortunately, it might take up to three or four weeks. This can be an emotionally difficult time. If expulsion doesn’t happen on its own, medical or surgical treatment will be needed.
- Medical treatment. If, after a diagnosis of certain pregnancy loss, you’d prefer to speed the process, medication can cause your body to expel the pregnancy tissue and placenta. The medication can be taken by mouth or by insertion in the vagina.
 Your health care provider might recommend inserting the medication vaginally to increase its effectiveness and minimize side effects such as nausea and diarrhea. For about 70 to 90 percent of women, this treatment works within 24 hours.
Your health care provider might recommend inserting the medication vaginally to increase its effectiveness and minimize side effects such as nausea and diarrhea. For about 70 to 90 percent of women, this treatment works within 24 hours. - Surgical treatment. Another option is a minor surgical procedure called suction dilation and curettage (D&C). During this procedure, your health care provider dilates your cervix and removes tissue from the inside of your uterus. Complications are rare, but they might include damage to the connective tissue of your cervix or the uterine wall. Surgical treatment is needed if you have a miscarriage accompanied by heavy bleeding or signs of an infection.
Physical recovery
In most cases, physical recovery from miscarriage takes only a few hours to a couple of days. In the meantime, call your health care provider if you experience heavy bleeding, fever or abdominal pain.
You may ovulate as soon as two weeks after a miscarriage. Expect your period to return within four to six weeks. You can start using any type of contraception immediately after a miscarriage. However, avoid having sex or putting anything in your vagina — such as a tampon — for two weeks after a miscarriage.
Expect your period to return within four to six weeks. You can start using any type of contraception immediately after a miscarriage. However, avoid having sex or putting anything in your vagina — such as a tampon — for two weeks after a miscarriage.
Future pregnancies
It’s possible to become pregnant during the menstrual cycle immediately after a miscarriage. But if you and your partner decide to attempt another pregnancy, make sure you’re physically and emotionally ready. Ask your health care provider for guidance about when you might try to conceive.
Miscarriage is usually a one-time occurrence. Most women who miscarry go on to have a healthy pregnancy after miscarriage. Less than 5 percent of women have two consecutive miscarriages, and only 1 percent have three or more consecutive miscarriages.
If you experience multiple miscarriages, generally two or three in a row, consider testing to identify any underlying causes. Such causes could include problems with the uterus, blood clotting or chromosomes. If the cause of your miscarriages can’t be identified, don’t lose hope. About 60 to 80 percent of women with unexplained repeated miscarriages go on to have healthy pregnancies.
If the cause of your miscarriages can’t be identified, don’t lose hope. About 60 to 80 percent of women with unexplained repeated miscarriages go on to have healthy pregnancies.
Coping and support
Emotional healing can take much longer than physical healing. Miscarriage can be a heart-wrenching loss that others around you might not fully understand. Your emotions might range from anger and guilt to despair. Give yourself time to grieve the loss of your pregnancy, and seek help from loved ones.
You’ll likely never forget your hopes and dreams surrounding this pregnancy, but in time acceptance might ease your pain. Talk to your health care provider if you’re feeling profound sadness or depression.
Preparing for an appointment
If you have signs or symptoms of miscarriage, contact your health care provider right away. Depending on the circumstances, you might need immediate medical care.
Here’s some information to help you get ready for your appointment, and what to expect from your health care provider.
What you can do
Before your appointment, you might want to:
- Ask about pre-appointment restrictions. In most cases you’ll be seen immediately. If that’s not the case, ask whether you should restrict your activities while you wait for your appointment.
- Find a loved one or friend who can join you for your appointment. Fear and anxiety might make it difficult to focus on what your health care provider says. Take someone along who can help remember all the information.
- Write down questions to ask your health care provider. That way, you won’t forget anything important that you want to ask, and you can make the most of your time with your health care provider.
Below are some basic questions to ask your health care provider about miscarriage:
- What are the treatment options?
- What kinds of tests do I need?
- Can I continue to do my usual activities?
- What signs or symptoms should prompt me to call you or go to the hospital?
- Do you know what caused my miscarriage?
- What are my chances for a successful future pregnancy?
In addition to the questions you’ve prepared, don’t hesitate to ask other questions during your appointment — especially if you need clarification or you don’t understand something.
What to expect from your health care provider
Your health care provider is likely to ask you a number of questions, too. For example:
- When was your last menstrual period?
- Were you using any contraceptive methods at the time you likely conceived?
- When did you first notice your signs or symptoms?
- Have your symptoms been continuous or occasional?
- Compared with your heaviest days of menstrual flow, is your bleeding more, less or about the same?
- Have you had a miscarriage before?
- Have you had any complications during a previous pregnancy?
- Do you have any other health conditions?
- Do you know your blood type?
Update Date: 10-16-2021
© 1998-2021 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use
Miscarriage: Signs, Symptoms, Diagnosis, Treatment
Series Miscarriage
Written by WebMD Editorial Contributors
What Are the Treatments for Miscarriage?
The first thing your doctor will try to do is prevent you from having a miscarriage. If the doctor thinks you’re at risk for having one, they may tell you to cut back on activity, including sex, until the signs are gone. Some recommend bed rest, although there’s no scientific evidence it’ll prevent a miscarriage. It can also raise your risk for other health issues. More often than not, there isn’t a lot your doctor can do to stop a miscarriage.
If the doctor thinks you’re at risk for having one, they may tell you to cut back on activity, including sex, until the signs are gone. Some recommend bed rest, although there’s no scientific evidence it’ll prevent a miscarriage. It can also raise your risk for other health issues. More often than not, there isn’t a lot your doctor can do to stop a miscarriage.
Treatment of a miscarriage, once it starts, depends on your symptoms. The main goal of treatment during and after a miscarriage is to prevent heavy bleeding (they’ll call it hemorrhaging) and infection.
If vaginal bleeding fills more than one super sanitary pad an hour for 2 hours, call your doctor. Heavier bleeding and cramping often indicate that a miscarriage is happening. Most of the time, your body will pass all of the pregnancy-related tissue. The earlier you are in the pregnancy, the more likely your body will complete the miscarriage on its own.
If all of the tissue didn’t come out, a condition known as an incomplete miscarriage, you may need treatment to stop the bleeding and prevent infection.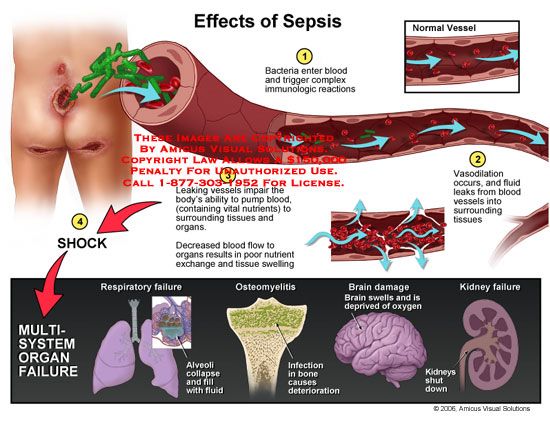 The most common procedure is a dilation and curettage (D&C), which involves widening your cervix and scraping the uterine lining, or endometrium. Sometimes the doctor uses suction along with scraping. This procedure can be uncomfortable, so you’ll probably get general anesthesia to put you to sleep if you need it. Another option is to take medication (misoprostol), which will help your body pass the tissue. Talk to your doctor to figure out what’s right for you.
The most common procedure is a dilation and curettage (D&C), which involves widening your cervix and scraping the uterine lining, or endometrium. Sometimes the doctor uses suction along with scraping. This procedure can be uncomfortable, so you’ll probably get general anesthesia to put you to sleep if you need it. Another option is to take medication (misoprostol), which will help your body pass the tissue. Talk to your doctor to figure out what’s right for you.
You may get antibiotics or other medications afterward to slow the bleeding. Let your doctor know if you have any additional vaginal bleeding. You should also find out whether you have Rh-negative blood. If you do, you’ll probably need a shot of Rh immune globulin to prevent problems in future pregnancies.
Call your doctor after a miscarriage if:
You have a fever or chills. Septic (infected) abortions are rare in cases of miscarriage, but a fever or chills could mean you have an infection.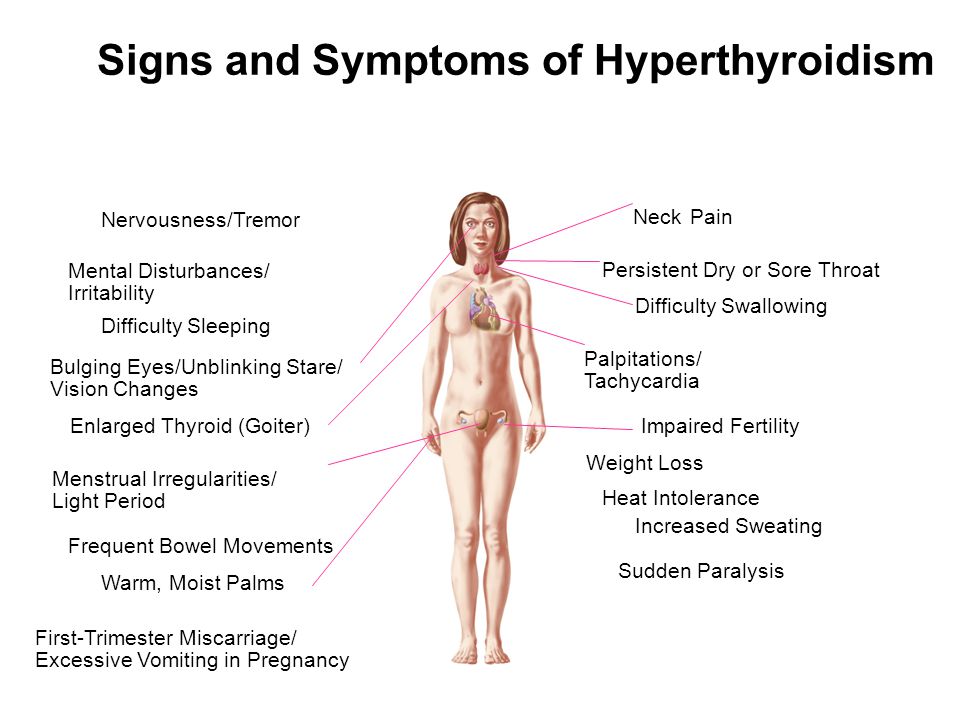 The doctor will make sure they remove any remaining pregnancy-related tissue, and you should take antibiotics to prevent serious illness.
The doctor will make sure they remove any remaining pregnancy-related tissue, and you should take antibiotics to prevent serious illness.
Tests After a Miscarriage
Most of the time, chances are good that the next pregancy after a miscarriage will be healthy. But if you have two or more miscarriages in a row, the doctor may suggest tests to find out if there’s a problem that you should treat before you try again. These could include:
Imaging tests. There may be something wrong with the structure of your uterus that’s keeping you from carrying a baby to term. The doctor can check for this with an ultrasound, an X-ray or a hysteroscopy.
Endometrial biopsy. During a hysteroscopy, your doctor may take a small piece of the lining of your uterus to look for abnormal cells.
Genetic tests.
 Chromosome problems are a common cause of miscarriages. You and your partner may get a karyotype test, which checks your chromosomes for anything unusual.
Chromosome problems are a common cause of miscarriages. You and your partner may get a karyotype test, which checks your chromosomes for anything unusual.
Blood tests. The doctor may check levels of certain hormones. Blood tests can also reveal risk factors for miscarriage, like diabetes, autoimmune disorders, and blood clotting problems.
Physical Recovery After Miscarriage
It usually doesn’t take long for your body to recover from a miscarriage. You may feel better within a few hours, or it could take a few weeks. Doctors recommend you don’t have sex or put anything in your vagina, like a tampon, for 2 weeks. That’s to lower the chances of an infection. You‘ll probably have your period again in 4-6 weeks.
Emotional Recovery After Miscarriage
It's common to feel sad after losing a pregnancy. Many couples feel the grief of losing a child. This is normal, so allow yourself time to grieve. Consider joining a support group where you can talk about your experience and feelings with others who’ve had a miscarriage.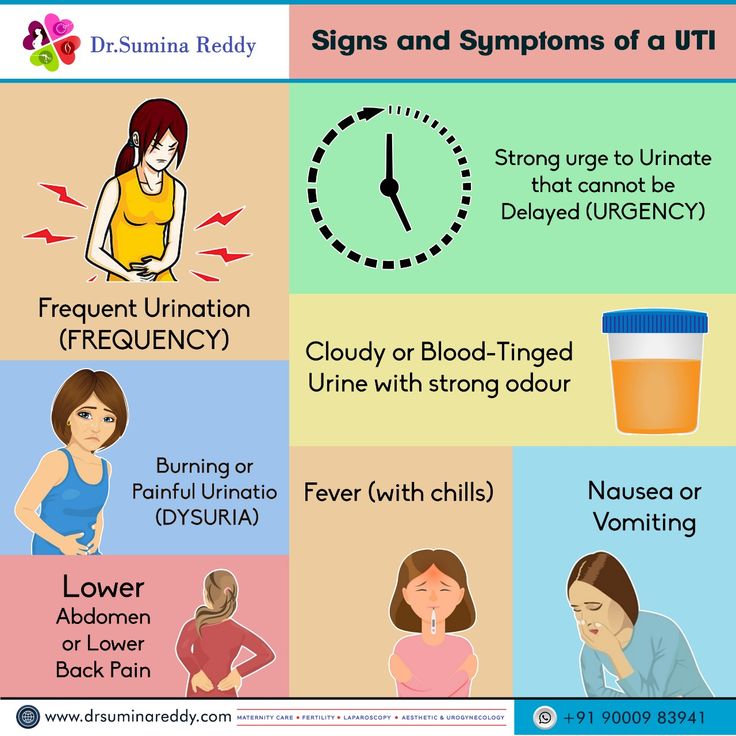 Family and friends may want to comfort you, but may feel like they don't know how. If you can, let them know that you need their support, tell them what they can do, and rely on their help.
Family and friends may want to comfort you, but may feel like they don't know how. If you can, let them know that you need their support, tell them what they can do, and rely on their help.
Miscarriage can be a physical and emotional challenge for you and your partner. It can put a high amount of stress on your relationship. You may be tempted to blame yourself or your partner for the miscarriage. Don’t. It's highly unlikely either of you did anything to cause the miscarriage or could have done anything to prevent it.
Keep in mind that there is a good chance that you will give birth to a healthy baby in the future. Only about 20% of women who have had a miscarriage have another miscarriage the next time they become pregnant.
Although it's possible to become pregnant right after a miscarriage, most experts recommend waiting until after you have had one or two normal menstrual cycles before trying to get pregnant again.
Next In Miscarriage Series:
PreventionEarly miscarriage - symptoms and how to prevent it
The term "early miscarriage" refers to a spontaneous abortion that occurs in the first 6-8 weeks of pregnancy. It can occur before 20 weeks of pregnancy for reasons related to the natural states of the fair sex. According to statistics, the logical outcome of every fifth pregnancy is a miscarriage. However, quite often a woman does not even know that she was pregnant by the time the fetus is rejected by the body. nine0003
It can occur before 20 weeks of pregnancy for reasons related to the natural states of the fair sex. According to statistics, the logical outcome of every fifth pregnancy is a miscarriage. However, quite often a woman does not even know that she was pregnant by the time the fetus is rejected by the body. nine0003
In addition, a curious pattern was revealed: more often than a natural one, a pregnancy induced artificially ends in a miscarriage. For example, in vitro fertilization, unfortunately, does not always lead to a successful pregnancy and the birth of a baby on time.
Why can an early miscarriage occur?
Here are the most common causes, each of which significantly increases the risk of miscarriage: nine0003
- the expectant mother has certain infectious diseases, as well as STDs;
- intoxication of a woman's body for various reasons, including as a result of her living in an ecologically unfavorable region;
- all kinds of metabolic disorders in the body;
- hormonal disruptions, including those caused by a malfunction of the thyroid gland;
- various neoplasms in the uterus and others, as well as the cervix, pathologies; nine0012
- maintenance by the future mother of a life far from a healthy lifestyle.
 May include drinking alcohol, smoking, taking psychotropic and narcotic drugs, as well as malnutrition;
May include drinking alcohol, smoking, taking psychotropic and narcotic drugs, as well as malnutrition; - obesity;
- immune status disorders;
- cardiac diseases;
- diabetes mellitus;
- too early for pregnancy or, conversely, the patient's overly mature age at times increases the risk of miscarriage; nine0012
- all kinds of pathologies of chromosomes and genes;
- prolonged exposure to stress or severe psycho-emotional trauma in a woman.
The timing of a miscarriage may depend, among other things, on the patient's genetic predisposition to miscarriage. Finally, often its specific cause remains unexplained to the end.
Symptoms of miscarriage
A pregnant woman should urgently seek medical help if she has the following warning signs: nine0003
- bleeding from the vagina;
- spotting discharge from the genital tract. They can have both light pink and intense red or brownish tint;
- convulsions;
- severe pain in the lumbar region;
- abdominal pain, etc.
All of the above signs can be symptoms of a miscarriage. Timely provision of qualified medical care is the key to maintaining pregnancy. nine0003
Life after miscarriage
If a woman could not bear the pregnancy - an early miscarriage crossed out all her plans - then she needs to calm down and take all measures to prevent such complications in the future. Usually obstetricians-gynecologists recommend planning a new pregnancy no earlier than six months after a miscarriage. During this time, a woman needs to be examined and find out if she has any pathology in her body that could lead to an abortion. It can be various STDs and infectious diseases. In the presence of chronic diseases that can provoke spontaneous abortion, it is necessary to throw all your efforts into their treatment. nine0003
Gynecologists of the corresponding department of our private clinic in Ryazan will help you find out what could have caused the miscarriage, as well as make recommendations on how to prepare for pregnancy. They usually include a set of physical exercises suitable for a woman, a diet rich in everything necessary for bearing a healthy baby, no stress, and measures to maintain a normal body mass index. Can't recover or get pregnant after a miscarriage? Contact "ON CLINIC in Ryazan" - here you will definitely be helped! nine0003
They usually include a set of physical exercises suitable for a woman, a diet rich in everything necessary for bearing a healthy baby, no stress, and measures to maintain a normal body mass index. Can't recover or get pregnant after a miscarriage? Contact "ON CLINIC in Ryazan" - here you will definitely be helped! nine0003
Spontaneous miscarriage and miscarriage
Over the past 10 years, the number of spontaneous miscarriages has been growing rapidly. The International Histological Classification Organization (FIGO) has declared the situation with an increase in the frequency of miscarriages an epidemic.
Spontaneous miscarriage is the termination of pregnancy before the fetus reaches a viable term (up to 22 weeks of pregnancy and fetal weight 500 g.).
Most miscarriages (about 80%) occur before 12 weeks of pregnancy. Moreover, in the early stages up to 8 weeks of pregnancy, the cause of miscarriage is chromosomal abnormalities in 50% of cases. It turns out that nature eliminates the defective product of conception. And these causes are difficult to prevent, especially in the presence of hereditary diseases. Fortunately, accidental breakdowns are much more common than genetically determined ones. Therefore, subsequent pregnancies usually end happily. nine0068 But the remaining 50% of miscarriages have completely real and avoidable causes. They can be easily identified at the stage of preparation for pregnancy by a gynecologist.
It turns out that nature eliminates the defective product of conception. And these causes are difficult to prevent, especially in the presence of hereditary diseases. Fortunately, accidental breakdowns are much more common than genetically determined ones. Therefore, subsequent pregnancies usually end happily. nine0068 But the remaining 50% of miscarriages have completely real and avoidable causes. They can be easily identified at the stage of preparation for pregnancy by a gynecologist.
What are the reasons?
- chronic diseases: inflammatory diseases of the uterus and appendages, polycystic ovary syndrome, uterine fibroids, endometriosis, malformations of the genital organs.
- infections: toxoplasmosis, listeriosis, genital tuberculosis, sexual infections - chlamydia, mycoplasma, ureaplasma, syphilis. nine0064 - antiphospholipid syndrome.
- endocrine diseases: diabetes, thyroid disease.
- metabolic disorders in the body: obesity, folic acid deficiency, iron deficiency, vitamin D deficiency.
- male factor.
Of course, these causes are identified and eliminated before the planned conception.
There are harmful factors that can affect the development of the fetus in the early stages of pregnancy and lead to miscarriage:
- alcohol consumption. nine0064 - use of caffeine (4-5 cups of coffee per day).
- smoking (more than 10 cigarettes a day).
- drug use.
- taking medications with a teratogenic effect (for example: aspirin, nise and others from this group of drugs; antifungals; antidepressants; some antibiotics and a number of other drugs).
- toxins and occupational hazards: ionizing radiation, pesticides, inhalation of anesthetic gases.
What are the signs of possible pregnancy loss? nine0069
These are complaints of pain in the lower abdomen and lower back, bloody discharge from the genital tract. It is necessary to consult a doctor to rule out an ectopic pregnancy and conduct an additional examination (hCG test, blood test for progesterone, ultrasound).
In the early stages of pregnancy, with dubious ultrasound data or suspected non-developing (missing) pregnancy, expectant management is chosen with a repeat examination by a gynecologist, ultrasound, tests after 7-10 days. If the diagnosis was made and the fact of uterine pregnancy was confirmed, with a threatened miscarriage, preservation therapy is carried out in an outpatient day hospital. A miscarriage that has begun requires hospitalization in the gynecological department. In the case of a non-developing pregnancy, an abortion is performed. nine0003
In accordance with the clinical treatment protocol approved by the Ministry of Health of the Russian Federation dated 07.06.2016. Preference is given to drug therapy aimed at terminating pregnancy with prostaglandin analogues (misoprostol) with or without prior use of an antiprogestin (mifepristone). In case of need for surgical treatment (with incomplete miscarriage with infected miscarriage), it is recommended to use aspiration curettage (with an electric vacuum source or a manual vacuum aspirator). What has a significant advantage over curettage of the uterine cavity because it is less traumatic and can be performed on an outpatient basis. nine0003
What has a significant advantage over curettage of the uterine cavity because it is less traumatic and can be performed on an outpatient basis. nine0003
All women who have had a miscarriage need treatment to prevent complications and prevent recurrent miscarriages. Why is rehabilitation therapy necessary?
According to the decision of the XVIII World Congress of Obstetricians and Gynecologists , the diagnosis of chronic endometritis should be made to absolutely all women who have had an undeveloped pregnancy. Two out of three miscarriages according to Professor V.E. Radzinsky are caused by this disease. When examining the material from the uterine cavity, infectious pathogens were isolated: ureaplasmas, mycoplasmas, streptococci, staphylococci, Escherichia coli, viruses (herpes, HPV). Therefore, it is very important to carry out treatment immediately after the termination of pregnancy. nine0064 If time is lost, it is necessary to carry out additional diagnostics: a biopsy of the endometrium with a histological examination and a study for infections, including tuberculosis. Then, taking into account the results obtained, symptomatic anti-inflammatory therapy is carried out (immunomodulators, antibacterial drugs, physiotherapy, gynecological massage, mud therapy). In parallel, an examination is prescribed to identify other causes of miscarriage (male factor, chronic maternal diseases, genital infections, antiphospholipid syndrome). nine0064 In the medical center "Mifra-Med" at the level of modern requirements of medicine, all the possibilities for a complete adequate examination have been created: all types of tests, ultrasound, hysteroscopy, aspiration biopsy, consultations of narrow specialists (endocrinologist, therapist, neurologist, urologist). Our gynecologists of the highest category Melko O.N., Novitskaya E.L., Tikhonova T.N. and urologist of the highest category Kanaev S.A. have sufficient experience in the rehabilitation and preparation of couples for the next pregnancy with a successful outcome. Treatment is carried out in a day hospital with the use of drugs, physiotherapy, gynecological massage, prostate massage.
Then, taking into account the results obtained, symptomatic anti-inflammatory therapy is carried out (immunomodulators, antibacterial drugs, physiotherapy, gynecological massage, mud therapy). In parallel, an examination is prescribed to identify other causes of miscarriage (male factor, chronic maternal diseases, genital infections, antiphospholipid syndrome). nine0064 In the medical center "Mifra-Med" at the level of modern requirements of medicine, all the possibilities for a complete adequate examination have been created: all types of tests, ultrasound, hysteroscopy, aspiration biopsy, consultations of narrow specialists (endocrinologist, therapist, neurologist, urologist). Our gynecologists of the highest category Melko O.N., Novitskaya E.L., Tikhonova T.N. and urologist of the highest category Kanaev S.A. have sufficient experience in the rehabilitation and preparation of couples for the next pregnancy with a successful outcome. Treatment is carried out in a day hospital with the use of drugs, physiotherapy, gynecological massage, prostate massage.