Pregnancy bladder infections
Urinary Tract Infection During Pregnancy: Symptoms & Prevention
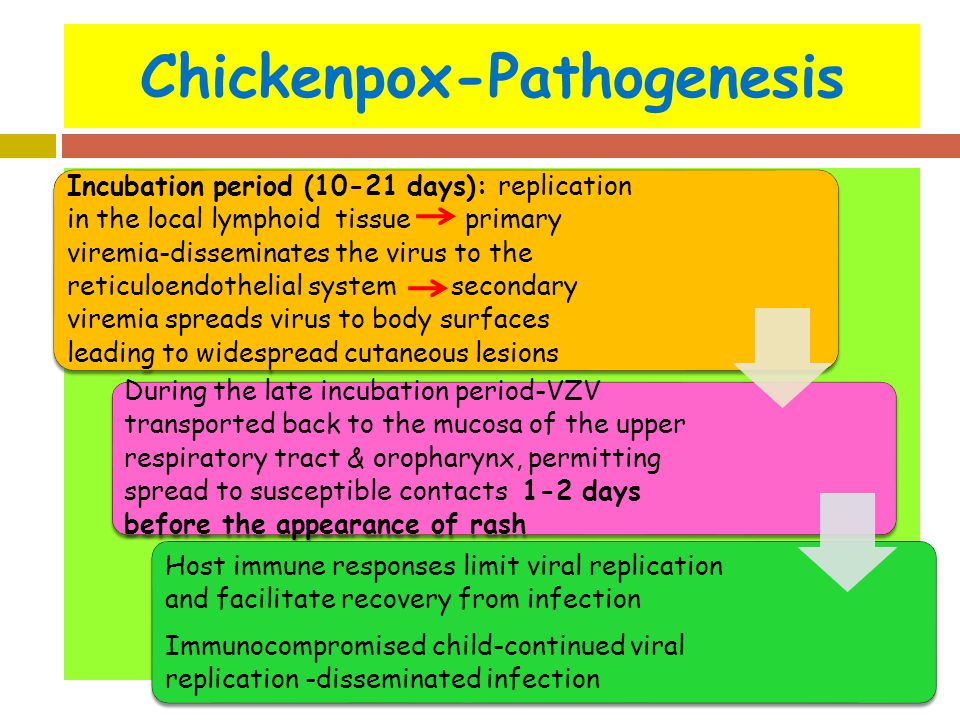
A urinary tract infection (UTI), also called bladder infection, is a bacterial inflammation in the urinary tract. Pregnant women are at increased risk for UTIs starting in week 6 through week 24 because of changes in the urinary tract. The uterus sits directly on top of the bladder. As the uterus grows, its increased weight can block the drainage of urine from the bladder, causing a urinary tract infection during pregnancy.
What are the signs and symptoms of UTIs?
If you have a urinary tract infection, you may experience one or more of the following symptoms:
- Pain or burning (discomfort) when urinating
- The need to urinate more often than usual
- A feeling of urgency when you urinate
- Blood or mucus in the urine
- Cramps or pain in the lower abdomen
- Pain during sexual intercourse
- Chills, fever, sweats, leaking of urine (incontinence)
- Waking up from sleep to urinate
- Change in the amount of urine, either more or less
- Urine that looks cloudy, smells foul or unusually strong
- Pain, pressure, or tenderness in the area of the bladder
- When bacteria spreads to the kidneys you may experience back pain, chills, fever, nausea, and vomiting.
How will a UTI affect my baby?
If the UTI goes untreated, it may lead to a kidney infection. Kidney infections may cause early labor and low birth weight. If your doctor treats a urinary tract infection early and properly, the UTI will not cause harm to your baby.
How do I know if I have a UTI?
A urinalysis and a urine culture can detect a urinary tract infection throughout pregnancy.
What treatment options are available?
UTIs can be safely treated with antibiotics during pregnancy. Urinary tract infections are most commonly treated by antibiotics. Doctors usually prescribe a 3-7 day course of antibiotics that is safe for you and the baby. Call your doctor if you have fever, chills, lower stomach pains, nausea, vomiting, contractions, or if after taking medicine for three days, you still have a burning feeling when you urinate.
How can I prevent a bladder infection?
You may do everything right and still experience a urinary tract infection during pregnancy, but you can reduce the likelihood by doing the following:
- Drink 6-8 glasses of water each day and unsweetened cranberry juice regularly.

- Eliminate refined foods, fruit juices, caffeine, alcohol, and sugar.
- Take Vitamin C (250 to 500 mg), Beta-carotene (25,000 to 50,000 IU per day) and Zinc (30-50 mg per day) to help fight infection.
- Develop a habit of urinating as soon as the need is felt and empty your bladder completely when you urinate.
- Urinate before and after intercourse.
- Avoid intercourse while you are being treated for a UTI.
- After urinating, blot dry (do not rub), and keep your genital area clean. Make sure you wipe from the front toward the back.
- Avoid using strong soaps, douches, antiseptic creams, feminine hygiene sprays, and powders.
- Change underwear and pantyhose every day.
- Avoid wearing tight-fitting pants.
- Wear all-cotton or cotton-crotch underwear and pantyhose.
- Don’t soak in the bathtub longer than 30 minutes or more than twice a day.
Want to Know More?
- 7 Common Discomforts of Pregnancy
- How Your Body Changes During Pregnancy
- Pregnancy Nutrition
- Exercise During Pregnancy
Compiled using information from the following sources:
1. American Academy of Family Physicians
American Academy of Family Physicians
https://www.aafp.org/
2. William’s Obstetrics Twenty-Second Ed. Cunningham, F. Gary, et al, Ch. 48.
Urinary Tract Infections (UTI) During Pregnancy
Written by WebMD Editorial Contributors
Medically Reviewed by Nivin Todd, MD on September 04, 2022
In this Article
- UTI Symptoms
- Why Are UTIs More Common During Pregnancy?
- UTI Diagnosis
- UTI Treatment During Pregnancy
- UTI Complications During Pregnancy
- UTI Prevention
A urinary tract infection (UTI) is an infection of some part of your body's urinary system, which includes your:
- Kidneys
- Ureters (tubes that carries urine from your kidneys to your bladder)
- Bladder
- Urethra (a short tube that carries urine from your bladder to outside your body)
Bacteria cause most UTIs. Anyone can get one, but they're most common in women, and they can be extra concerning if you're pregnant.
If you think you might have a UTI, tell your doctor. With proper care, you and your baby should be fine.
Usually, these infections are in the bladder and urethra. But sometimes they can lead to kidney infections. If they do, UTIs may lead to preterm labor (giving birth too early) and low birth weight.
UTI Symptoms
If you have a UTI, you may have:
- An urgent need to pee, or peeing more often
- Trouble with peeing
- A burning sensation or cramps in your lower back or lower belly
- A burning feeling when you pee
- Urine that looks cloudy or has an odor
- Blood in your pee, which can turn it red, bright pink, or cola-colored
If you have a kidney infection, you may have:
- Fever
- Nausea
- Vomiting
- Upper back pain, often on just one side
If you have symptoms of a kidney infection, see your doctor right away. Without treatment, the infection can spread into your bloodstream and cause life-threatening conditions.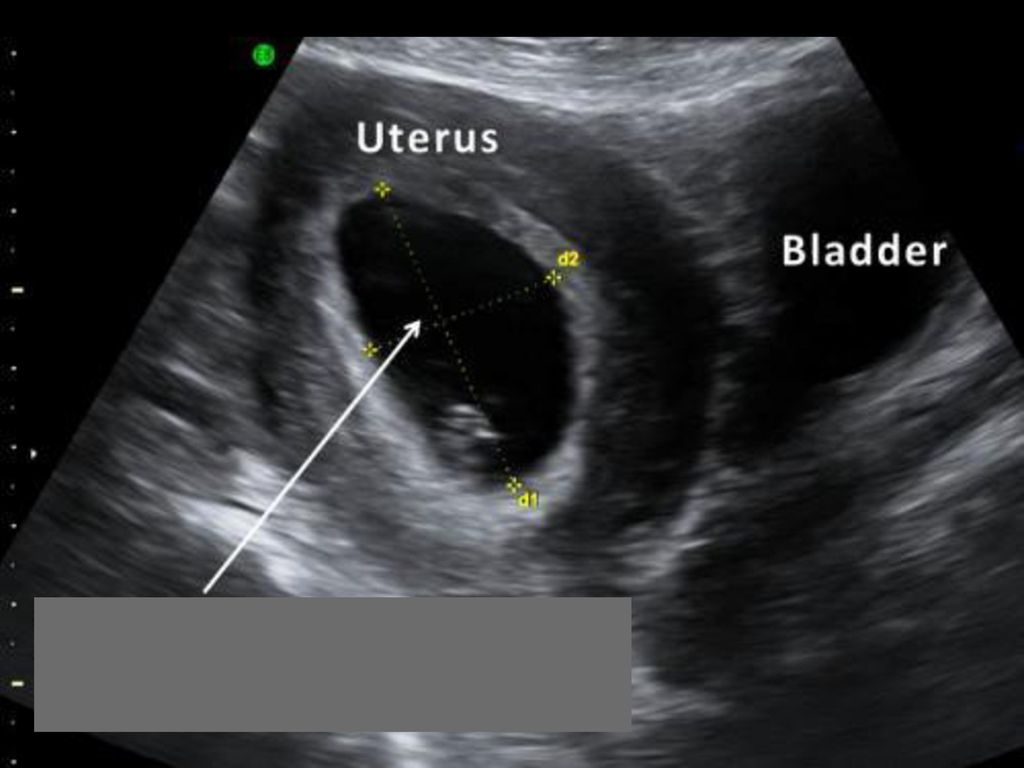
Why Are UTIs More Common During Pregnancy?
Hormones are one reason. In pregnancy, they cause changes in the urinary tract, and that makes women more likely to get infections. Changes in hormones can also lead to vesicoureteral reflux, a condition in which your pee flows back up from your bladder to your kidneys. This can cause UTIs.
When you’re pregnant, your pee has more sugar, protein, and hormones in it. These changes also put you at higher risk for a UTI.
Because you’re pregnant, your growing uterus presses on your bladder. That makes it hard for you to let out all the urine in your bladder. Leftover urine can be a source of infection.
Other causes of UTIs include:
Escherichia coli and other bacteria from your poop. E. Coli is the most common cause of UTIs and can move from your rectum to your urethra if you don’t wipe from front to back.
Sexual activity. Fingers, your partner’s penis, or devices can move bacteria near your vagina into your urethra.
Group B streptococcus. Many women have this bacteria in their colon and vagina. It can cause UTIs and women can pass it to their newborns. Your doctor will test you for this bacteria around weeks 36 to 37 of pregnancy. If you’re positive for group B strep, your doctor will give you IV antibiotics during labor.
UTI Diagnosis
You’ll take a urine test. Your doctor will test it for bacteria and red and white blood cells. A urine culture may also be checked. It shows what kind of bacteria are in the urine.
UTI Treatment During Pregnancy
You’ll take antibiotics for 3 to 7 days or as your doctor recommends. If your infection makes you feel uncomfortable, your doctor will probably start your treatment before you get your urine test results.
Your symptoms should go away in 3 days. Take all of your medication on schedule anyway. Don’t stop it early, even if your symptoms fade.
Many common antibiotics -- amoxicillin, erythromycin, and penicillin, for example -- are considered safe for pregnant women.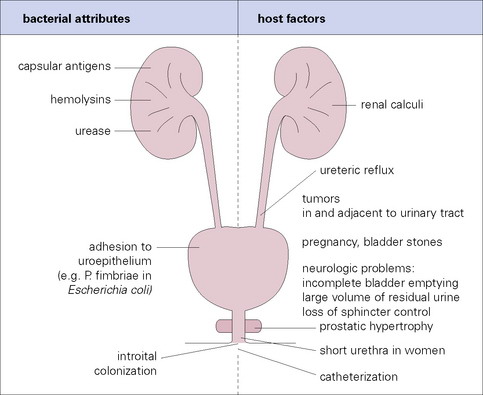 Your doctor wouldn’t prescribe others, such as ciprofloxacin (Cipro), sulfamethoxazole, tetracycline, or trimethoprim (Primsol, Proloprim, Trimpex), that can affect your baby’s development.
Your doctor wouldn’t prescribe others, such as ciprofloxacin (Cipro), sulfamethoxazole, tetracycline, or trimethoprim (Primsol, Proloprim, Trimpex), that can affect your baby’s development.
UTI Complications During Pregnancy
Pyelonephritis is a UTI that affects the kidneys. If you’re pregnant it can cause:
- Preterm labor
- Severe infection
- Adult respiratory distress syndrome
- Anemia
- Long-term infection
UTI Prevention
To try to avoid getting a UTI:
- Drink at least eight glasses of water a day.
- Wipe yourself from front to back when you go to the bathroom.
- Empty your bladder shortly before and after sex.
- If you need a lubricant when you have sex, choose a water-based one.
- Don't douche.
- Avoid strong feminine deodorants or soaps that cause irritation.
- Wash your genital area with warm water before sex.
- Wear cotton underwear.
- Take showers instead of baths.
- Don’t wear pants that are too tight.
- Pee often.
- Avoid alcohol, citrus juices, spicy food, and caffeinated drinks, which can irritate your bladder.
Women's Health Guide
- Screening & Tests
- Diet & Exercise
- Rest & Relaxation
- Reproductive Health
- Head to Toe
Urinary tract infections vs pregnancy: treatment and prevention
Summary. Urinary tract infections are one of the most common complications in pregnant women, which can lead to serious consequences not only for the expectant mother, but also for the child. When managing pregnant women with diseases of the urinary system, it is extremely important to choose the right and, most importantly, safe therapeutic tactics. What drugs are safe during pregnancy? What obstetric and therapeutic tactics are most effective for kidney diseases in pregnant women? What diagnostic methods are best used for asymptomatic bacteriuria, acute cystitis and pyelonephritis? Professor 9 spoke about this in her speech0003 Olga Grishchenko , Head of the Department of Perinatology, Obstetrics and Gynecology of the Kharkov Medical Academy of Postgraduate Education during the training workshop for gynecologists "Actual Guidelines of Gynecology, Reproductology, Obstetrics", held on March 29, 2019 in Kharkov.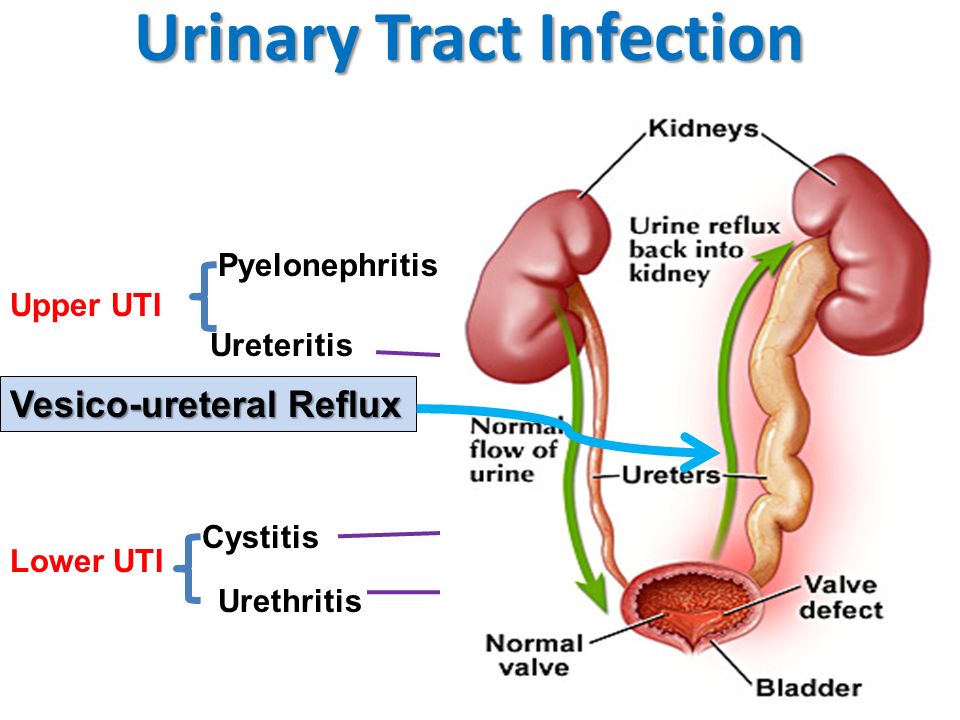 The event was organized by the MedExpert Group of Companies together with the National Medical University named after A.A. Bogomolets and National Medical Academy of Postgraduate Education named after P.L. Shupyk.
The event was organized by the MedExpert Group of Companies together with the National Medical University named after A.A. Bogomolets and National Medical Academy of Postgraduate Education named after P.L. Shupyk.
Urgency of the problem
Urinary tract infections (UTIs) are the most common bacterial infections in outpatient practice, they take the 2nd place, second only to respiratory tract infections. According to statistics, 50% of women in the world have an episode of UTI at least once in their lives, of which 25–40% experience a relapse of the disease within 6–12 months. Every year, about 10% of women develop acute cystitis, and pyelonephritis remains the leading cause of hospitalization during pregnancy for non-obstetric indications.
In the presence of UTI in pregnant women, the risk of preterm labor and rupture of amniotic fluid, chorioamnionitis increases, premature or functionally immature children are born, and the level of perinatal mortality increases.
In the structure of UTI, asymptomatic bacteriuria is observed in 4-9.5% of pregnant women, acute pyelonephritis - in 12-25%, chronic pyelonephritis - in 33%, glomerulonephritis, urolithiasis - in 0.1-0.2%.
Risk factors and pregnancy
As a rule, infections, self-medication or improper treatment, asymptomatic bacteriuria, frequent UTIs in combination with inflammatory diseases (colpitis), lifestyle and nutrition can affect the occurrence of pathology of the urinary system.
Pregnant women have an increased risk of diseases of the urogenital tract. A high level of progesterone leads to the development of hypotension, hypokinesia, dyskinesia of the ureters and pyelocaliceal system. In turn, the uterus compresses the ureter, high intra-abdominal pressure occurs, especially in primiparas. During pregnancy, the renal pelvis enlarges, the growing uterus squeezes the ureter more and more, the outflow of urine from the kidneys becomes difficult, the urine stagnates, bacteria multiply in it, and inflammation easily occurs.
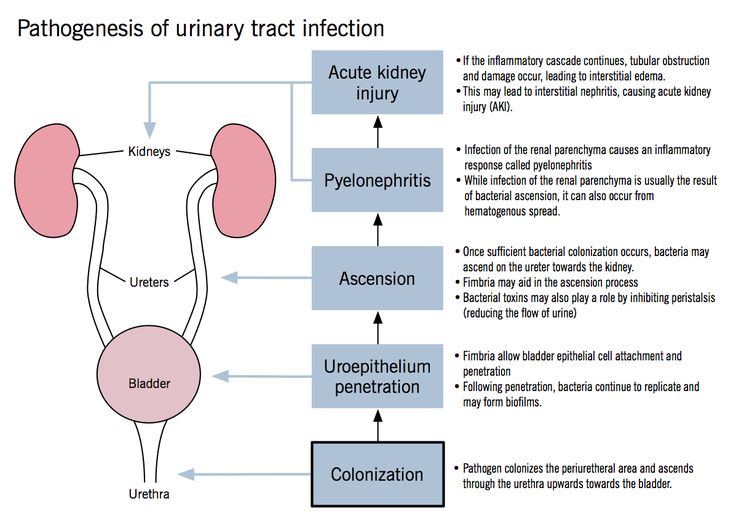
Infectious agents can enter the bladder by ascending (with inflammatory diseases of the urethra), descending (most often with tuberculous kidney damage), hematogenous (if there is a purulent focus in other parts of the body) and lymphogenic (with diseases of the genital organs) by.
Classification of UTIs in pregnant women
UTIs in pregnant women include asymptomatic bacteriuria, lower urinary tract infections (acute and recurrent cystitis) and upper urinary tract infections (acute pyelonephritis, chronic pyelonephritis in remission, exacerbation, latent course).
Cystitis in pregnancy: course, diagnosis
Cystitis is an inflammation of the bladder wall, one of the most common urological diseases, as a rule, its cause is an infection. Symptoms of cystitis in women are manifested in the form of frequent urination, cramps and pain when urinating, pulling sensations in the lower abdomen, weakness, fatigue, irritability, blood in the urine, cloudy urine, pus or yellow spots on the underwear.
Normally, urination is not accompanied by pain. In women, painful urination can be caused by diseases of the bladder, urethra, or vagina. So, pain in the bladder, as a rule, is felt in the area of the womb, it can increase during urination or, conversely, decrease when the bladder is empty. Urethral pain associated with urination is felt by the patient directly in the urethra and is usually aggravated by urination. Urine entering the vaginal opening can cause pain if it is inflamed. Inflammation of the urethra is most often characterized by a bacterial nature and requires additional examination and treatment.
Primary diagnosis of cystitis involves an examination by specialized specialists (urologist, nephrologist, gynecologist), as well as taking an anamnesis and establishing possible causes of the disease (hypothermia, unprotected intercourse, taking medications, the presence of concomitant diseases).
Laboratory tests include a urinalysis for Nechiporenko cultures (helps identify the pathogen), a general urinalysis (allows you to identify erythrocytes, leukocytes, protein in the urine; the urine itself may be cloudy with an admixture of blood or pus), a general blood test (allows you to identify a picture inflammatory process, it is possible to increase the erythrocyte sedimentation rate (ESR), leukocytosis). Among instrumental methods, ultrasound examination (ultrasound) of the bladder, ureteroscopy and cystoscopy (in case of violation of the passage of urine) are used.
Among instrumental methods, ultrasound examination (ultrasound) of the bladder, ureteroscopy and cystoscopy (in case of violation of the passage of urine) are used.
Asymptomatic bacteriuria during pregnancy
Asymptomatic bacteriuria during pregnancy is dangerous for both mother and fetus, against its background, 25% of women develop acute pyelonephritis. According to the World Health Organization, about 8% of women report asymptomatic bacteriuria, 15-57% of women with untreated asymptomatic bacteriuria develop symptoms of a UTI (acute cystitis or pyelonephritis). Therapy of this disease during pregnancy reduces the risk of developing acute UTIs, preterm birth, and low birth weight.
Diagnosis of asymptomatic bacteriuria can be established by detecting 10 5 CFU/ml of one bacterial strain or 10 2 CFU/ml of uropathogen Escherichia coli field of view in the absence of clinical manifestations of UTI.
It should be remembered that the risk of this pathology is most real from the 9th to the 17th week of pregnancy. The only reliable method for diagnosing asymptomatic bacteriuria is the method of urine culture.
The only reliable method for diagnosing asymptomatic bacteriuria is the method of urine culture.
In accordance with Ukrainian and international guidelines for asymptomatic bacteriuria, oral antibiotic therapy with a single dose of fosfomycin trometamol is recommended.
Pyelonephritis: diagnosis
Pyelonephritis is an infectious and inflammatory disease of the kidneys of bacterial etiology with a primary and predominant lesion of the interstitium and tubular apparatus. The incidence of pyelonephritis during pregnancy reaches 33%, mortality - 3.5%, maternal mortality from kidney disease in the structure of extragenital pathology is 8-10%, the incidence of gestational pyelonephritis is 11.5%.
Primary pyelonephritis in pregnant women is difficult to treat, may be accompanied by fever, chills, nausea, vomiting, pain in the lumbar region, the appearance of pyuria, bacteriuria. As a rule, the right kidney is affected more often than the left one, with expansion of the pelvicalyceal system (according to ultrasound).
In acute pyelonephritis, the mandatory research methods are a general urinalysis (in 2 portions) 1 time in 7 days, a Nechiporenko urinalysis, a general and biochemical blood test, a bacteriological urinalysis, ultrasound of the kidneys and bladder, daily proteinuria, a biochemical blood test , blood pressure monitoring, urologist consultation. Additional research methods - computed tomography without contrast or excretory urogram, nuclear magnetic resonance imaging - are carried out exclusively for strict, sometimes vital, indications.
It should be remembered that dysuria in primary acute cystitis with a body temperature of 38 ° C and chills may indicate acute ascending pyelonephritis. A sharp dysuric syndrome is characteristic of the associated cystitis during exacerbation of chronic pyelonephritis. Urinary syndrome (proteinuria, leukocyturia, hematuria, etc.) may periodically disappear with a unilateral process and ureter occlusion; therefore, serial urine tests are necessary. The degree of leukocyturia does not always correspond to the severity of the inflammatory process. A single urine culture gives at least 20% false positive results. Bacteriuria appears and can be detected 2 days earlier than pyuria.
The degree of leukocyturia does not always correspond to the severity of the inflammatory process. A single urine culture gives at least 20% false positive results. Bacteriuria appears and can be detected 2 days earlier than pyuria.
Choice of drugs for the treatment of pregnant women with UTIs
There are certain requirements for antibiotics for the treatment of UTIs in pregnant women. In particular, they must be effective against most pathogenic pathogens, have the ability to create a high concentration in organs - foci of infection, have a long half-life sufficient to maintain a high concentration of the antibiotic in the blood, not have toxic and allergic effects, be well tolerated by patients, be harmless to mother and fetus.
It has been shown that for the treatment of pregnant women with acute cystitis, asymptomatic bacteriuria, acute pyelonephritis, it is advisable to use antibacterial uroseptics. In particular, fosfomycin trometamol has a bactericidal effect associated with blocking the bacterial enzyme involved in the synthesis of the cell wall, as well as an anti-adhesive effect (destroys the fimbria of Escherichia coli, preventing it from fixing on the wall of the urothelium and promoting leaching from the urinary tract). After a single dose of the drug, the therapeutic concentration is observed for 48 hours (this is enough to sterilize urine and recover).
After a single dose of the drug, the therapeutic concentration is observed for 48 hours (this is enough to sterilize urine and recover).
An alternative to antibiotics are phytoneering preparations with anti-adhesive and antibacterial activity, as well as anti-inflammatory, antispasmodic, nephroprotective properties.
Organization of care for pregnant women with UTI and prevention
Delivery of pregnant women with UTI (without obstetric pathology) is carried out through the natural birth canal, taking into account the obstetric situation.
There are degrees of risk of pyelonephritis:
- I degree - uncomplicated pyelonephritis that occurred during pregnancy;
- II degree - chronic uncomplicated pyelonephritis, noted before pregnancy;
- III degree - pyelonephritis with hypertension, azotemia, pyelonephritis of a single kidney.
They must be taken into account when managing pregnant women. So, at I-II degree of risk, pregnancy can be prolonged, but at III degree (creatinine> 265 μmol / l, glomerular filtration rate < 30 ml / min), pregnancy should be terminated.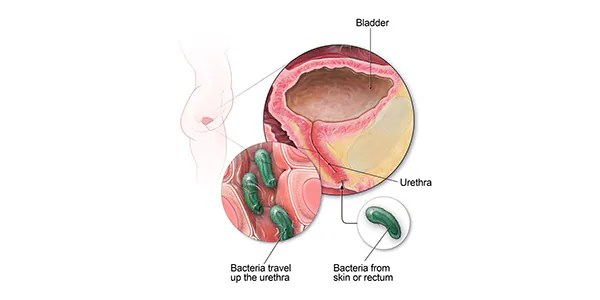
Prevention of UTIs in pregnant women should include sanitation of the vagina in case of violation of its microflora and other sources of infection (teeth, pharynx, etc.), normalization of bowel function, optimal water regime.
Subscribe to our Telegram channel, Viber community, Instagram, Facebook page, and Twitter to be the first to receive the latest and most relevant news from the world of medicine.
Marina Kolesnik,
photo of the author
Site map
|
|