Missed period pcos
Polycystic Ovary Syndrome (PCOS) | Johns Hopkins Medicine
Polycystic ovary syndrome (PCOS) is a condition in which the ovaries produce an abnormal amount of androgens, male sex hormones that are usually present in women in small amounts. The name polycystic ovary syndrome describes the numerous small cysts (fluid-filled sacs) that form in the ovaries. However, some women with this disorder do not have cysts, while some women without the disorder do develop cysts.
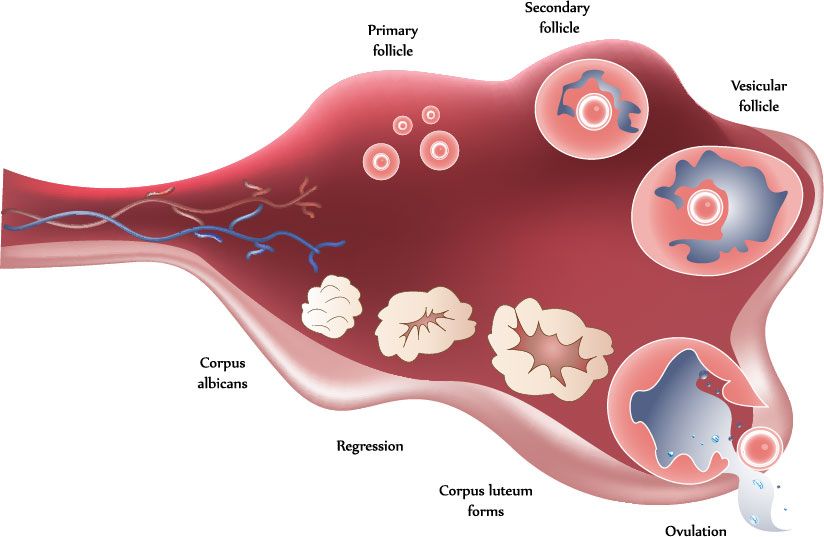
Ovulation occurs when a mature egg is released from an ovary. This happens so it can be fertilized by a male sperm. If the egg is not fertilized, it is sent out of the body during your period.
In some cases, a woman doesn’t make enough of the hormones needed to ovulate. When ovulation doesn’t happen, the ovaries can develop many small cysts. These cysts make hormones called androgens. Women with PCOS often have high levels of androgens. This can cause more problems with a woman’s menstrual cycle. And it can cause many of the symptoms of PCOS.
Treatment for PCOS is often done with medication. This can’t cure PCOS, but it helps reduce symptoms and prevent some health problems.
What causes PCOS?
The exact cause of PCOS is not clear. Many women with PCOS have insulin resistance. This means the body can't use insulin well. Insulin levels build up in the body and may cause higher androgen levels. Obesity can also increase insulin levels and make PCOS symptoms worse.
PCOS may also run in families. It's common for sisters or a mother and daughter to have PCOS.
What are the risks for PCOS?
You may be more likely to have PCOS if your mother or sister has it. You may also be more likely to have it if you have insulin resistance or are obese.
What are the symptoms of PCOS?
The symptoms of PCOS may include:
-
Missed periods, irregular periods, or very light periods
-
Ovaries that are large or have many cysts
-
Excess body hair, including the chest, stomach, and back (hirsutism)
-
Weight gain, especially around the belly (abdomen)
-
Acne or oily skin
-
Male-pattern baldness or thinning hair
-
Infertility
-
Small pieces of excess skin on the neck or armpits (skin tags)
-
Dark or thick skin patches on the back of the neck, in the armpits, and under the breasts
How is PCOS diagnosed?
Your health care provider will ask about your medical history and your symptoms. You will also have a physical exam. This will likely include a pelvic exam. This exam checks the health of your reproductive organs, both inside and outside your body.
You will also have a physical exam. This will likely include a pelvic exam. This exam checks the health of your reproductive organs, both inside and outside your body.
Some of the symptoms of PCOS are like those caused by other health problems. Because of this, you may also have tests such as:
-
Ultrasound. This test uses sound waves and a computer to create images of blood vessels, tissues, and organs. This test is used to look at the size of the ovaries and see if they have cysts. The test can also look at the thickness of the lining of the uterus (endometrium).
-
Blood tests. These look for high levels of androgens and other hormones. Your health care provider may also check your blood glucose levels. And you may have your cholesterol and triglyceride levels checked.
How is PCOS treated?
Treatment for PCOS depends on a number of factors. These may include your age, how severe your symptoms are, and your overall health. The type of treatment may also depend on whether you want to become pregnant in the future.
The type of treatment may also depend on whether you want to become pregnant in the future.
If you do plan to become pregnant, your treatment may include:
-
A change in diet and activity. A healthy diet and more physical activity can help you lose weight and reduce your symptoms. They can also help your body use insulin more efficiently, lower blood glucose levels, and may help you ovulate.
-
Medications to cause ovulation. Medications can help the ovaries to release eggs normally. These medications also have certain risks. They can increase the chance for a multiple birth (twins or more). And they can cause ovarian hyperstimulation. This is when the ovaries release too many hormones. It can cause symptoms such as abdominal bloating and pelvic pain.
If you do not plan to become pregnant, your treatment may include:
-
Birth control pills. These help to control menstrual cycles, lower androgen levels, and reduce acne.

-
Diabetes medication. This is often used to lower insulin resistance in PCOS. It may also help reduce androgen levels, slow hair growth, and help you ovulate more regularly.
-
A change in diet and activity. A healthy diet and more physical activity can help you lose weight and reduce your symptoms. They can also help your body use insulin more efficiently, lower blood glucose levels, and may help you ovulate.
-
Medications to treat other symptoms. Some medications can help reduce hair growth or acne.
What are the complications of PCOS?
Women with PCOS are more likely to develop certain serious health problems. These include type 2 diabetes, high blood pressure, problems with the heart and blood vessels, and uterine cancer. Women with PCOS often have problems with their ability to get pregnant (fertility).
Living with PCOS
Some women struggle with the physical symptoms of PCOS, such as weight gain, hair growth, and acne. Cosmetic treatments, such as electrolysis and laser hair removal, may help you feel better about your appearance. Talk with your health care provider about the best ways to treat the symptoms that bother you.
Cosmetic treatments, such as electrolysis and laser hair removal, may help you feel better about your appearance. Talk with your health care provider about the best ways to treat the symptoms that bother you.
When should I seek medical care?
If you have missed or irregular periods, excess hair growth, acne, and weight gain, call your doctor for an evaluation.
Key points
-
PCOS is a very common hormone problem for women of childbearing age.
-
Women with PCOS may not ovulate, have high levels of androgens, and have many small cysts on the ovaries.
-
PCOS can cause missed or irregular menstrual periods, excess hair growth, acne, infertility, and weight gain.
-
Women with PCOS may be at higher risk for type 2 diabetes, high blood pressure, heart problems, and endometrial cancer.
-
The types of treatment for PCOS may depend on whether or not a woman plans to become pregnant.
 Women who plan to become pregnant in the future may take different kinds of medications.
Women who plan to become pregnant in the future may take different kinds of medications.
Next steps
Tips to help you get the most from a visit to your health care provider:
-
Before your visit, write down questions you want answered.
-
Bring someone with you to help you ask questions and remember what your provider tells you.
-
At the visit, write down the names of new medicines, treatments, or tests, and any new instructions your provider gives you.
-
If you have a follow-up appointment, write down the date, time, and purpose for that visit.
-
Know how you can contact your provider if you have questions.
Park Avenue Women's Center: OB-GYNs
Is Your Period Delayed Every Month? You Might Have PCOS: Park Avenue Women's Center: OB-GYNsPolycystic ovary syndrome (PCOS) is a common condition among women of childbearing years, affecting about 1 in 10, or about 10 million women worldwide. Hormonal imbalance is the main culprit of this syndrome, but environmental and genetics can also play a role.
Hormonal imbalance is the main culprit of this syndrome, but environmental and genetics can also play a role.
A common symptom of PCOS is missed or irregular periods. While some women may relish the idea of not getting their period every month, they won’t like the symptoms. PCOS can lead to pelvic pain, headaches, and infertility. So if you suspect you have PCOS, you should see your OB/GYN.
While there is no cure for PCOS, there are many treatments to help you minimize or eliminate the symptoms.
What is PCOS and what causes it?
The exact cause of PCOS is unknown. But some factors that are thought to contribute or play a role in the condition are an excess of androgen, a male hormone, and excess insulin, which can lead to excess androgen.
When your body has too much androgen, it can affect your regular monthly cycle. This hormonal imbalance prevents the egg from developing or releasing properly. As a result, women with PCOS often miss their periods or have delayed or irregular periods.
PCOS can affect all women, usually between the ages of 15 and 44, but women who are obese and women who have a close relative with PCOS are at higher risk for developing this syndrome.
In addition to missed or delayed periods, other common symptoms include:
- Acne
- Thinning hair or hair loss on the scalp
- Weight gain or difficulty losing weight
- Skin tags
- Skin discoloration
- An increase in facial and body hair, also called hirsutism
- Sleep issues
- Infertility
PCOS is the most common cause of infertility. About 70-80% of women with PCOS experience fertility issues. Fortunately, it’s also very treatable.
PCOS diagnosis and treatment
There is no single blood test or other types of tests that provide a positive diagnosis for PCOS. Instead, the providers at Park Avenue Women’s Center conduct a series of tests to rule out other conditions and identify markers for PCOS. These tests can include:
- A physical exam
- A pelvic exam
- A pelvic ultrasound
- Blood tests to check your hormone levels and maybe cholesterol levels
If other conditions have been ruled out and you have at least two of the following symptoms, your provider will discuss PCOS treatment options with you:
- Irregular periods
- High levels of androgen, as noted in blood tests or by symptoms such as excessive hair growth or acne
- Small fluid-filled sacs, or follicles, on one or both ovaries
Treatment options can include lifestyle changes, medications, or both. Lifestyle changes include losing weight, watching your diet, and exercising more regularly. Medication options include anti-androgen medicines, hormonal birth control pills, or a hormonal birth control device such as an IUD.
Lifestyle changes include losing weight, watching your diet, and exercising more regularly. Medication options include anti-androgen medicines, hormonal birth control pills, or a hormonal birth control device such as an IUD.
For women who want to get pregnant, birth control pills are obviously not an option. Treatment options for women with PCOS who want to have a baby, include:
- Clomid, a medicine that helps you ovulate
- In vitro fertilization
- Surgery to help restore ovulation
For more information about diagnosis and treatment of PCOS, call us at Park Avenue Women’s Center, located on Manhattan’s Upper East Side in the Yorkville neighborhood. You can also book an appointment online through this website.
You Might Also Enjoy...
Tips for Choosing the Best Birth Control for Your Body
The good news about birth control is that you have many options to choose from.
 The bad news is that with all the options, it can be difficult to choose the right one. Read our guide about the choices you have and learn which one may be best for you.
The bad news is that with all the options, it can be difficult to choose the right one. Read our guide about the choices you have and learn which one may be best for you. What are the Risk Factors for Postpartum Depression?
Having a baby should be a happy event. Unfortunately, not all new mothers feel joy. Postpartum depression can produce feelings of sadness and an inability to bond with your baby. Learn the risk factors for postpartum depression and how to treat it.
Postpartum Depression
Having a baby should be a happy event. Unfortunately, not all new mothers feel joy. Postpartum depression can produce feelings of sadness and an inability to bond with your baby. Learn the risk factors for postpartum depression and how to treat it.
Polycystic ovary syndrome
Burlakova Elena Vladimirovna
Pediatrician
Clinic "Mother and Child" Kuntsevo,
The criteria for the diagnosis of PCOS are:
- no ovulation (anovulation),
- hyperandrogenism,
- the presence of polycystic disease (multifollicular ovaries) with an increase in the volume of the ovaries according to ultrasound.
The diagnosis can be made if two of these three manifestations are present.
As a rule, the examination of a woman begins with an ultrasound examination of the pelvic organs. Often, if the conclusion indicates the presence of "multifollicular ovaries" (MFO), on this basis, the diagnosis of PCOS is erroneously established. The term "multifollicular ovaries" is simply a description of the ultrasound pattern, which reflects the presence of a large number of antral follicles in the ovaries.
Such a conclusion, of course, is one of the criteria for PCOS, but, I remind you that not one symptom, but two, is required for a diagnosis. The presence of MFN by ultrasound performed at the beginning of the menstrual cycle does not make it possible to judge from the presence or absence of ovulation in a woman's menstrual cycles. The detection of a large number of follicles in the ovaries and by ultrasound is the norm for young women! With preserved ovulation, the absence of menstrual irregularities, this treatment does not require and does not prevent pregnancy!
To diagnose anovulation, it is necessary to perform ultrasonic folliculometry (FM), preferably within 2-3 menstrual cycles. Moreover, when performing FM, you need to decide on the period until which it makes sense to wait for the appearance of the dominant follicle. This is where mistakes often happen. The fact is that most women have a menstrual cycle of 28-30 days, while ovulation occurs on days 14-16 of the cycle.
Moreover, when performing FM, you need to decide on the period until which it makes sense to wait for the appearance of the dominant follicle. This is where mistakes often happen. The fact is that most women have a menstrual cycle of 28-30 days, while ovulation occurs on days 14-16 of the cycle.
But, if this is the case for the majority, should it be so for everyone? No. The normal length of a menstrual cycle is 21 to 42 days. This means that with a 21 day cycle, ovulation occurs on days 7–8 of the cycle, but with a 42 day cycle? On the 20th day? No. With a cycle duration of 42 days, ovulation should occur on days 26-30 of the cycle. Thus, when folliculometry is stopped on the 14th-16th day of the cycle due to the absence of a dominant follicle, an erroneous conclusion is made about anovulation. Although, with a regular, but long (32–42 days) menstrual cycle, ovulatory function can be preserved. Such a delusion is very dangerous, because it entails the start of stimulation therapy in women who are planning a pregnancy, although, in fact, they do not need it. Conversely, women who are not currently planning a pregnancy get the wrong impression that there is no need for contraception, which leads to unwanted pregnancies and, as a result, to abortion.
Conversely, women who are not currently planning a pregnancy get the wrong impression that there is no need for contraception, which leads to unwanted pregnancies and, as a result, to abortion.
The next symptom of PCOS is hyperandrogenism, which is an increase in the content of male hormones (androgens). This is a sufficient general statement. Characteristic of PCOS is an increase in testosterone, which is produced in excess in the ovaries. This can lead to appearances such as excessive hair growth on the skin of the abdomen, thighs and even the face (this is called hirsutism), as well as increased activity of the skin sebaceous glands, which is manifested by oily skin and a tendency to acne. But testosterone is not the only androgen in the body.
In addition, other male hormones are present in the body: androstenedione, DEHA, 17-OH progesterone, etc., which are produced mainly by the adrenal glands. Their determination is necessary during the examination in case of suspicion of PCOS, the presence of manifestations of hyperandrogenism, anovulation, but is not a sign of PCOS, since they are produced not in the ovary, but in the adrenal glands. So the determination of DHEA is necessary to exclude formations of the adrenal glands that produce hormones (hormone-producing tumors), the determination of 17-OH progesterone is performed to diagnose such a congenital disease as VDKN (formerly called adrenogenital syndrome - AGS), which can also lead to cycle disorders and anovulation, but, however, is not synonymous with PCOS and requires different treatment. With HCHD, there is at least a three-fold increase in the level of 17-OH progesterone, while a slight increase of 1-2 ng / ml or nmol / ml is neither a sign of HCHD nor PCOS, and, as a rule, is asymptomatic and does not require treatment.
So the determination of DHEA is necessary to exclude formations of the adrenal glands that produce hormones (hormone-producing tumors), the determination of 17-OH progesterone is performed to diagnose such a congenital disease as VDKN (formerly called adrenogenital syndrome - AGS), which can also lead to cycle disorders and anovulation, but, however, is not synonymous with PCOS and requires different treatment. With HCHD, there is at least a three-fold increase in the level of 17-OH progesterone, while a slight increase of 1-2 ng / ml or nmol / ml is neither a sign of HCHD nor PCOS, and, as a rule, is asymptomatic and does not require treatment.
Often, hormonal disorders in PCOS are accompanied by impaired insulin function (insulin resistance) and/or its excessive production (hyperinsulinemia). This leads to the fact that PCOS is accompanied by a complex of symptoms called metabolic syndrome (MS) and is manifested by obesity, hypertension, high cholesterol, and impaired glucose uptake.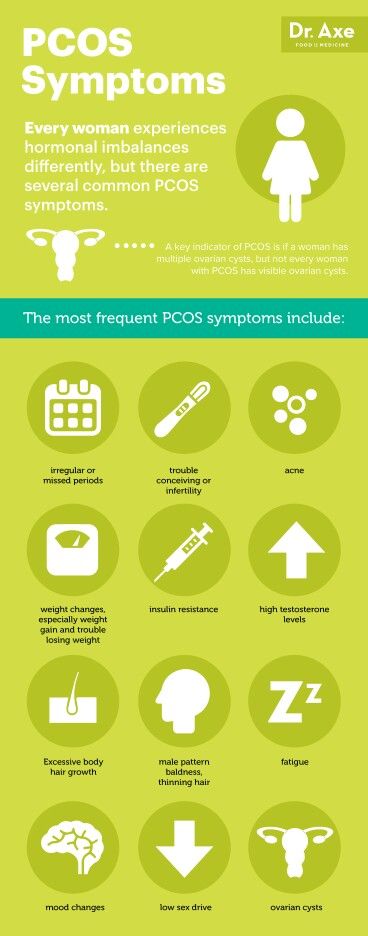 This manifestation of PCOS is dangerous with very serious consequences: if left untreated, type 2 diabetes mellitus, coronary heart disease, etc. develop over time, which is the main cause of death along with cancer. Insulin resistance, of course, requires medical correction with special drugs, but a woman herself can help the drugs work more efficiently. How? Weight loss, proper nutrition and regular physical activity. Agree, it is available to everyone.
This manifestation of PCOS is dangerous with very serious consequences: if left untreated, type 2 diabetes mellitus, coronary heart disease, etc. develop over time, which is the main cause of death along with cancer. Insulin resistance, of course, requires medical correction with special drugs, but a woman herself can help the drugs work more efficiently. How? Weight loss, proper nutrition and regular physical activity. Agree, it is available to everyone.
It's time to move on to treating PCOS.
Speaking about the treatment of this disease, it is important to answer the question: is a woman planning a pregnancy at the moment or not? So, if pregnancy is not planned in the near future, then combined oral contraceptives (COCs) are the best suited to normalize the cycle, prevent and treat endometrial hyperplasia, dysfunctional bleeding, and cosmetic problems. These drugs are quite effective, inexpensive and easy to take, which allows you to solve these problems.
On the topic "COC - to drink or not to drink?" many copies have been broken, but there is still no tool more effective, safer and easier to use.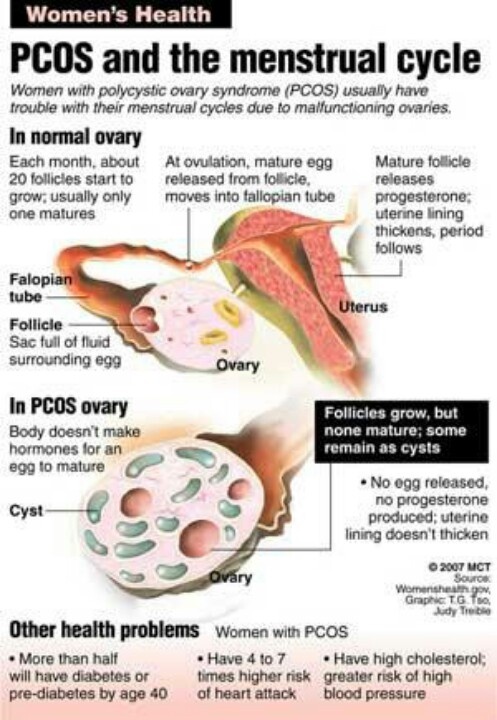 Like any other drug, COCs have both contraindications and side effects, so these drugs should be prescribed by a doctor who has experience working with them, after identifying possible contraindications to taking, for example, a tendency to thrombosis. There are a lot of drugs from this group on the market now, and their tolerance can be quite different. But I am convinced that among the existing variety it is possible to choose the right drug, it just does not always happen the first time, even if the appointment is made by a very experienced doctor. Unfortunately, in the medical literature, there is no unequivocal answer to the question of how long it is safe to take COCs. Based on my own experience, I can say that on average this is up to 5 years. I emphasize that this is an average value - in each individual case, this issue should be resolved individually.
Like any other drug, COCs have both contraindications and side effects, so these drugs should be prescribed by a doctor who has experience working with them, after identifying possible contraindications to taking, for example, a tendency to thrombosis. There are a lot of drugs from this group on the market now, and their tolerance can be quite different. But I am convinced that among the existing variety it is possible to choose the right drug, it just does not always happen the first time, even if the appointment is made by a very experienced doctor. Unfortunately, in the medical literature, there is no unequivocal answer to the question of how long it is safe to take COCs. Based on my own experience, I can say that on average this is up to 5 years. I emphasize that this is an average value - in each individual case, this issue should be resolved individually.
If a woman diagnosed with PCOS is planning a pregnancy, she needs to contact a reproductive specialist in a specialized clinic. Since for the onset of pregnancy it is necessary not only to make the menstrual cycle regular, but to establish the ovulatory function of the ovary, since without the release of the egg from the ovary, that is, ovulation, pregnancy is impossible. In such cases, ovulation induction is performed (stimulation of ovulation, stimulation of ovarian function) with the use of special preparations.
Since for the onset of pregnancy it is necessary not only to make the menstrual cycle regular, but to establish the ovulatory function of the ovary, since without the release of the egg from the ovary, that is, ovulation, pregnancy is impossible. In such cases, ovulation induction is performed (stimulation of ovulation, stimulation of ovarian function) with the use of special preparations.
It is good if ovulation is stimulated by a reproductive specialist who knows ultrasound and can independently monitor the growth of follicles and prescribe appropriate drugs. Before using ovulation induction, it is necessary to perform a study of the patency of the fallopian tubes and a diagnosis of the state of the sperm in the husband/partner (spermogram, MAP test, strict morphology according to the Kruger criteria) and other examinations that are mandatory when planning a pregnancy. Since, unfortunately, the lack of ovulation may not be the only reason for the lack of a desired pregnancy.
Often, a replacement for ovulation stimulation is the appointment of progesterone preparations from days 16 to 25 of the cycle. However, this is not at all the case. The appointment of these drugs will help to even out the cycle, make it 28 days, may be an alternative to COCs for the prevention and treatment of endometrial hyperplasia, but will not help the onset of pregnancy. On the contrary, it's more likely to get in the way. The fact is that under the influence of these drugs, changes occur in the endometrium that are characteristic of the second phase of the cycle, that is, after ovulation has occurred, which allows you to get a menstrual-like reaction, but their effect does not extend to the ovary, does not allow you to establish ovulation. But, in the event that ovulation suddenly decides to occur (this happens, including with PCOS once a year or once every several years), then taking these drugs can desynchronize the development of the embryo and the preparation of the endometrium, and this is one of the necessary conditions for pregnancy .
Previously, to normalize the cycle and restore ovulation, the method of ovarian cauterization (“notches”, resection of the ovaries) was used, which was performed during laparoscopy. For a long time, this was almost the only means of restoring the functioning of the ovaries in the absence of special drugs, the wide availability of ultrasound and qualified reproductologists. But now this method is not the method of choice, since among its consequences there is often premature ovarian exhaustion, that is, the irreversible disappearance of the follicular apparatus.
These are very difficult situations when young women begin menopausal manifestations, and there are no own eggs left, and pregnancy planning becomes possible only with the use of donor oocytes. In addition, I want to note that ovarian biopsy during laparoscopy is also not a modern criterion for the diagnosis of PCOS and you will not find indications of its need in any modern manual on operative gynecology. Since, unfortunately, even a slight damage to the ovarian tissue can lead to irreversible consequences.
Since, unfortunately, even a slight damage to the ovarian tissue can lead to irreversible consequences.
In conclusion, I want to say that although PCOS is a common pathology that leads to serious consequences, in the modern world there are many means to cope with it and realize the reproductive function. Take care of your health, contact qualified specialists and be happy!
Make an appointment
to the doctor - Burlakova Elena Vladimirovna
Clinic "Mother and Child" Kuntsevo
Children's emergency care
By clicking on the send button, I consent to the processing of personal data
Polycystic ovary syndrome - symptoms, causes, features, diagnosis and treatment in medical centers "K + 31
Causes of polycystic ovary syndrome
PCOS is a dyshormonal disease that leads to the formation of a dense membrane around the ovaries that prevents the release of an egg (ovulation) . For the first time, the clinical picture of this pathology was described by Stein and Leventhal in the last century. For this reason, PCOS is also called Stein-Leventhal syndrome.
For this reason, PCOS is also called Stein-Leventhal syndrome.
The mechanisms by which PCOS develops are not fully understood. At present, the role of hereditary factors in its occurrence has been proven. With PCOS, the conversion of male sex hormones into female sex hormones is disrupted in the ovaries. As a result, an excess of androgens appears in the blood, the maturation of follicles in the ovaries stops, many cysts form, and their albuginea thickens.
These disorders are based on increased activity of insulin during puberty, the effect of which on the ovaries is mediated through the main regulatory center - the pituitary gland and its hormones: follicle-stimulating (FSH) and luteinizing (LH).
How does polycystic ovary syndrome manifest itself?
Violation of the production of sex hormones in the ovaries leads to a decrease in estrogen levels. As a result, menstruation becomes rare until their complete disappearance. In some cases, on the contrary, uterine bleeding is noted due to the formed hyperplastic process of the endometrium.
An excess of androgens in the body leads to the development of hirsutism (excessive growth of hair on the body and face). At the same time, there may even be baldness or hair loss with bald patches on the sides of the forehead and on the top of the head. Many women develop acne, seborrhea, the skin becomes oily. One of the main reasons for patients with PCOS to see a doctor is infertility due to the lack of ovulation.
A characteristic symptom of polycystic ovaries is male-type obesity, in which the bulk of adipose tissue is deposited in the lower abdomen and in the abdominal cavity. As a result of a rapid increase in body weight against the background of hormonal imbalance, stretch marks appear on the skin of the abdomen, hips, buttocks - striae.
Patients with PCOS often experience:
- depression,
- decreased libido,
- irritability,
- nervousness,
- aggressiveness,
- often drowsiness,
- lethargy,
- "head fog" complaints.

With this pathology, there is a dysfunction not only of the ovaries, but also of other organs: the hypothalamus, pituitary gland, adrenal glands, thyroid gland. Therefore, the clinical picture and the severity of manifestations are very diverse.
Absence of ovulation
Any woman may suspect that she has polycystic ovaries. As we said, with PCOS, a dense capsule forms around the ovary, which prevents ovulation. Its absence can be registered using the basal temperature (BT) chart, which is recommended for a patient with infertility to be measured within 3-6 months. With PCOS, the BBT schedule will be monotonous without a characteristic ovulatory peak in the middle of the cycle throughout the entire observation period.
You can also detect anovulation with home tests, which are carried out starting from the 17th day before the expected period. With PCOS, all tests will be negative. The absence of ovulation according to BT and tests for several months requires further examination, first of all, ultrasound.
What will the ultrasound show?
Ultrasound can detect the following signs of PCOS:
- bilateral ovarian enlargement 2–3 times;
- many small cysts (more than 10) on the periphery of the ovaries, which look like a "pearl necklace", an accumulation of whitish bubbles or "fruit seeds";
- capsule thickened to 5 mm or more;
- reduction in the size of the uterus.
Ultrasound is highly informative for PCOS. However, the data of this method alone is not enough to establish a diagnosis. A laboratory study of the patient's blood is necessary.
Hormonal disorders
An important step in the examination of patients with suspected PCOS is the study of the hormonal profile, which is carried out on the 2nd-4th day of the menstrual cycle. With this pathology in the serum, there is an increase in the level of LH, testosterone, dehydroepiandrosterone (DHEA), estradiol deficiency.
It is also common for patients with PCOS to have decreased thyroid function.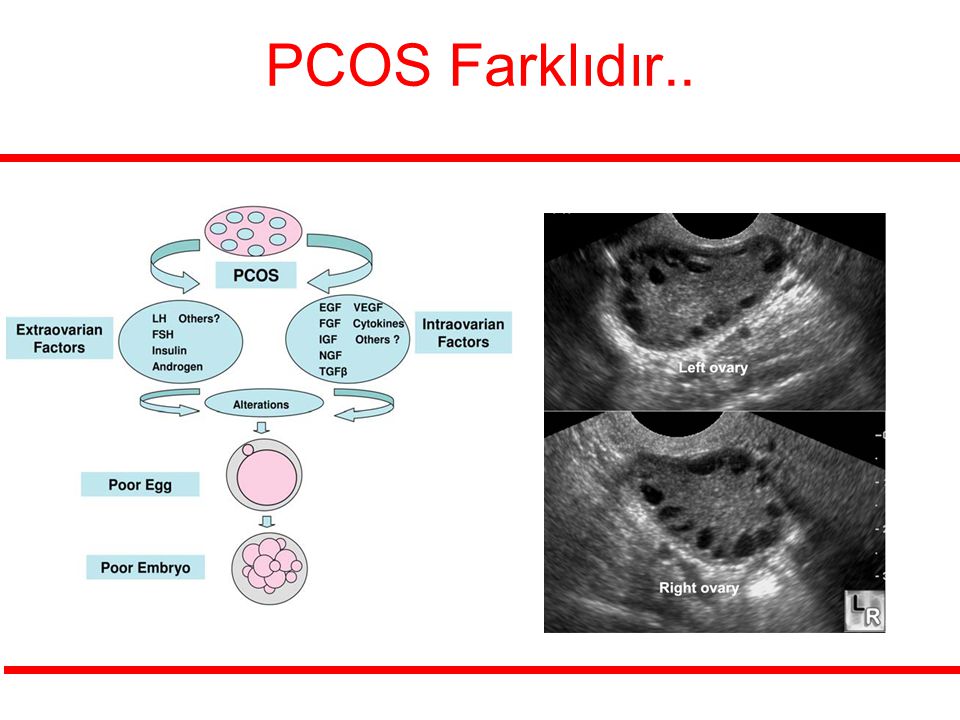 Therefore, the concentrations of thyroid-stimulating hormone (TSH), thyroxine (T4) and prolactin should be additionally assessed, which can be changed.
Therefore, the concentrations of thyroid-stimulating hormone (TSH), thyroxine (T4) and prolactin should be additionally assessed, which can be changed.
An anti-Müllerian hormone (AMH) test plays an important role in the detection of PCOS. Normally, its level is 1-2.5 ng / ml. With polycystic it increases.
How to distinguish between PCOS and adrenal pathology?
Often, PCOS has to be distinguished from adrenogenital syndrome (AGS) - a hereditary pathology of the adrenal glands, which also increases the content of male sex hormones. But with PCOS, unlike AGS, they are synthesized in the ovaries, and not in the adrenal glands.
To establish the diagnosis, tests with glucocorticoids (prednisolone, dexamethasone, cortisone) are carried out, the deficiency of which is present in adrenogenital syndrome and absent in PCOS. In the pathology of the adrenal glands, after the introduction of the missing glucocorticoid, the levels of androgens, their intermediate products and metabolites (DHEA, 17-OK, 17-OP) are normalized. With PCOS, this effect is absent.
With PCOS, this effect is absent.
Currently, to establish the diagnosis of AHS, genotyping of the 21-hydroxylase gene mutation (CYP21A2) is performed, which makes it possible to detect a deficiency of this enzyme, which is the cause of congenital adrenal pathology.
Run diagnostics
Assessing glucose tolerance
A distinctive feature of PCOS is insulin resistance - a violation of insulin susceptibility by tissues. A similar condition occurs in type 2 diabetes.
For this reason, patients with PCOS have a glucose tolerance test.
With PCOS, there is often a change in the lipid spectrum of the blood with a predominance of atherogenic components: cholesterol, triglycerides, low and very low density lipoproteins (LDL and VLDL).
Normalizing carbohydrate metabolism
Women with PCOS and overweight are advised to change their lifestyle and diet. It is necessary to follow a diet (eating enough pure protein, vegetables, limiting carbohydrates), doing fitness and sports.
Given the decrease in tissue sensitivity to insulin, as in type 2 diabetes mellitus, gynecologists-endocrinologists of the gynecology department of the K + 31 Clinic in PCOS prescribe metformin (MF), which increases the susceptibility of cells to insulin. Against the background of taking the drug, carbohydrate metabolism is normalized, the number of male sex hormones in the blood decreases, and ovarian function is restored.
We stimulate ovulation
An important step in the treatment of PCOS is the normalization of the menstrual cycle. For this purpose, combined oral contraceptives (COCs) are used, which include antiandrogens that block the effects of male sex hormones. Taking COCs prevents further progression of the disease. After the withdrawal of hormones, the patient ovulates and there is a chance to become pregnant.
If at the end of the COC course the ovarian function has not returned to normal, and the woman is interested in pregnancy, it is necessary to induce (stimulate) ovulation with special hormonal preparations (clostilbegyt). The scheme is selected by the doctor. Usually, treatment is started with a low dose and, in the absence of a result, it is increased.
The scheme is selected by the doctor. Usually, treatment is started with a low dose and, in the absence of a result, it is increased.
Also, in order to correct hyperandrogenism, cyproterone acetate (androkur) and spironolactone (veroshpiron), which have an antiandrogenic effect, are additionally used. Against the background of their intake, the greasiness of the skin decreases, acne disappears, and hair growth improves.
Surgical treatment of polycystic ovary syndrome (PCOS)
If ovulation still does not occur despite 3-6 months of hormone therapy, surgery is performed. When choosing an access, preference is given to laparoscopy. During the operation, either small incisions (wedge resection) or holes (cauterization) are made in the dense shell of the ovaries, through which the egg can leave the ovary and be fertilized. After the intervention, the menstrual cycle becomes ovulatory. This effect lasts up to a year, during which a woman can become pregnant.
Treatment of PCOS takes a long time - from 3 to 12 months.












