Mild hip dysplasia
Hip Dysplasia | Boston Children's Hospital
Listen
What is hip dysplasia?
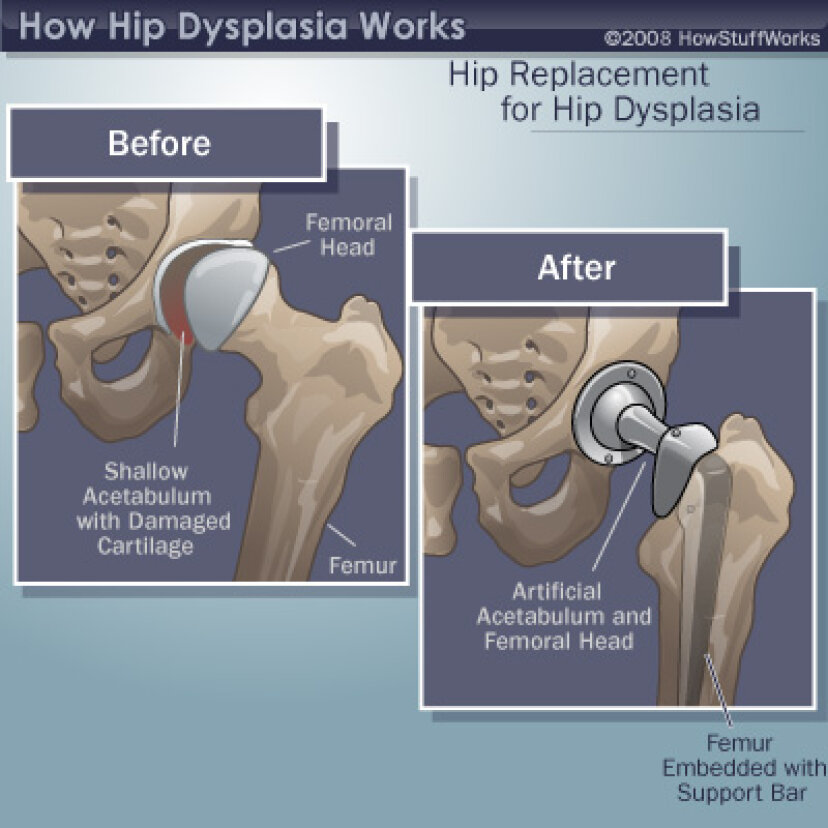
The hip is a ball-and-socket joint. Normally, the ball at the top of the thigh bone fits into the hip socket. Hip dysplasia occurs when the hip joint has not developed properly and the socket (acetabulum) is too shallow. This allows the ball (femoral head) to slip partially or completely out of the joint. Hip dysplasia ranges from a mild abnormality to a complete dislocation of the hip.
Severe cases of hip dysplasia are usually diagnosed during a routine screening within the first few months of a baby’s life. Other times, the problem may only become noticeable as a child grows and becomes more active.
Hip dysplasia is a treatable condition. However, if left untreated, it can cause irreversible damage that will cause pain and loss of function later in life. It is the leading cause of early arthritis of the hip before the age of 60. The severity of the condition and catching it late increase the risk of arthritis. Therefore, monitoring and early intervention are both important to reduce a child’s risk of pain and disability in adulthood.
Who is affected?
Hip dysplasia can affect anyone at any age. Although it is believed to develop around birth, a child with mild dysplasia may not have symptoms for years, or even decades.
- Hip dysplasia in babies is known as infant developmental dysplasia of the hip (DDH).
- When diagnosed in adolescents and young adults, it is sometimes called acetabular dysplasia.
The age at which older kids and young adults with hip dysplasia begin to notice symptoms depend on the severity of the condition and their activity level. Athletes who place a lot of load on their hips by participating in dance, hockey, football, soccer, or track and field may experience symptoms sooner.
Meet Louise
Undiagnosed hip dysplasia caused such severe knee pain, this former track star sometimes had trouble walking after competitions. With surgery behind her, and a degree in medicine in the works, she has returned to the sport she loves.
With surgery behind her, and a degree in medicine in the works, she has returned to the sport she loves.
Read her story
Girls and women are two to four times more likely than boys to have hip dysplasia. It also tends to affect first-born children and those who have a close family member with hip problems. Some people with hip dysplasia are affected in only one hip while others have it in both hips.
In boys, the condition tends to be accompanied by other hip problems. These include acetabular retroversion (when the hip socket grows too far over the head of the femur) or CAM lesions (extra bone growth on the surface of the bone that causes extra friction and joint damage).
Hip dysplasia is sometimes confused with hip impingement, which occurs when extra bone grow on the acetabulum or femoral head. The irregular shape creates friction within the joint and wears down cartilage. Some patients have both conditions, both of which cause hip pain and are easy to confuse. However, they are different issues that require different treatments.
However, they are different issues that require different treatments.
Image
Image
Generally speaking, treating hip dysplasia as early as possible can minimize joint damage and reduce the chance of early onset arthritis.
How we care for hip dysplasia
The Child and Young Adult Hip Preservation Program at Boston Children’s Hospital is at the forefront of research and innovation. We combine specialized expertise in non-surgical and surgical treatments with structured physical therapy to help children, adolescents, and young adults live healthy, active lives.
Our team has treated thousands of children with every level of complexity and severity of hip deformity. Our hip specialists have pioneered minimally invasive procedures as well as open surgical techniques to help treat patients of all ages. We perform more periacetabular osteotomy (PAO) procedures every year than any other hospital in the country and have helped hundreds of athletes return to the activities they love.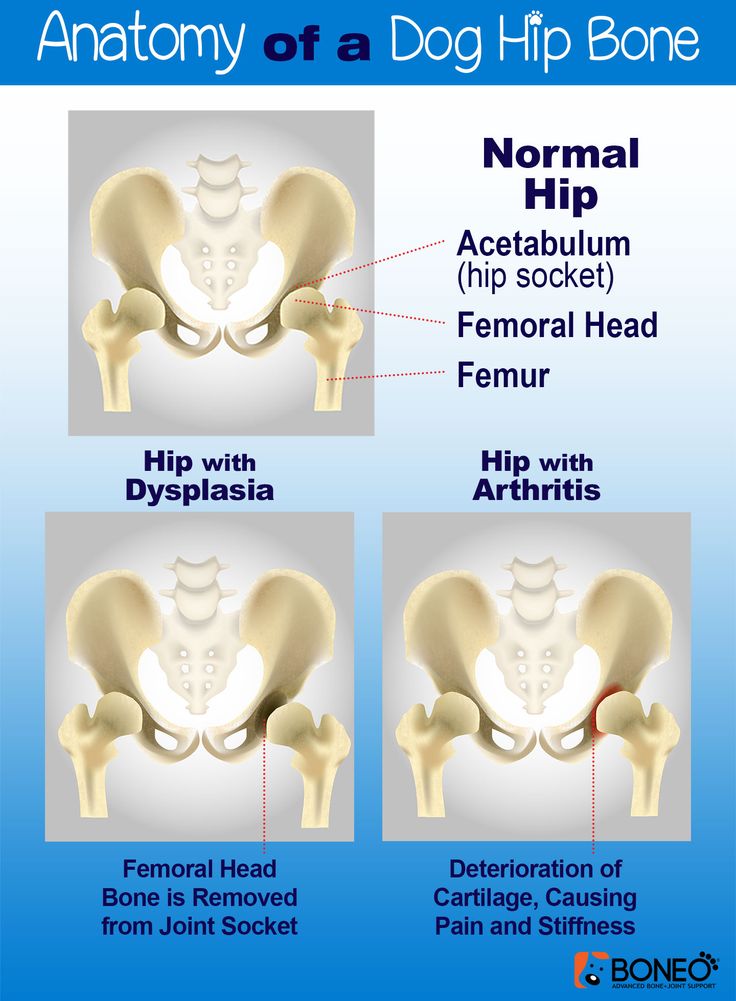
We have the experience to treat you or your child. Our goal is the same as yours: to help you get better so you can return to being healthy and pain-free.
Patient resources
Download these fact sheets to learn more about hip dysplasia and treatment options.
- fact sheet: developmental dysplasia of the hip (DDH)
- fact sheet: Pavlik harness
- fact sheet: hip dysplasia in adolescents and young adults
Hip Dysplasia | Hip Dysplasia in Adolescents
What is hip dysplasia in adolescents?
Hip dysplasia occurs when the hip socket (acetabulum) doesn't develop properly and is too shallow to cover the head of the thigh bone (femoral head) completely. Many adolescents and young adults with the condition were born with developmental dysplasia of the hip (DDH). In others, previously healthy hips did not develop properly as their bones and bodies grew.
Meet Alana and Nicole
A year and a half after hip surgery, Nicole still questioned her physical capabilities. That changed when she met Alana, another dancer who’d had the same surgery. This chance meeting became a turning point in both dancers' healing.
That changed when she met Alana, another dancer who’d had the same surgery. This chance meeting became a turning point in both dancers' healing.
Read their story
The condition ranges from a mild abnormality of the hip socket to a complete dislocation of the hip. As children become more active and demand more of their legs, the ill-fitting hip joint becomes unstable. The instability damages cartilage inside the joint that becomes increasingly painful over time.
It is important not to ignore hip pain. Hip dysplasia is a treatable condition but early diagnosis and treatment are critical to preventing irreversible damage.
What are the symptoms of hip dysplasia in adolescents and young adults?
Teens or young adults may develop a limp or have hip pain in the front of the hip or groin. For others, the first sign is knee pain. You might hear a clicking sound in your hip. As the damage progresses, you may find it more and more painful to participate in sports and other activities.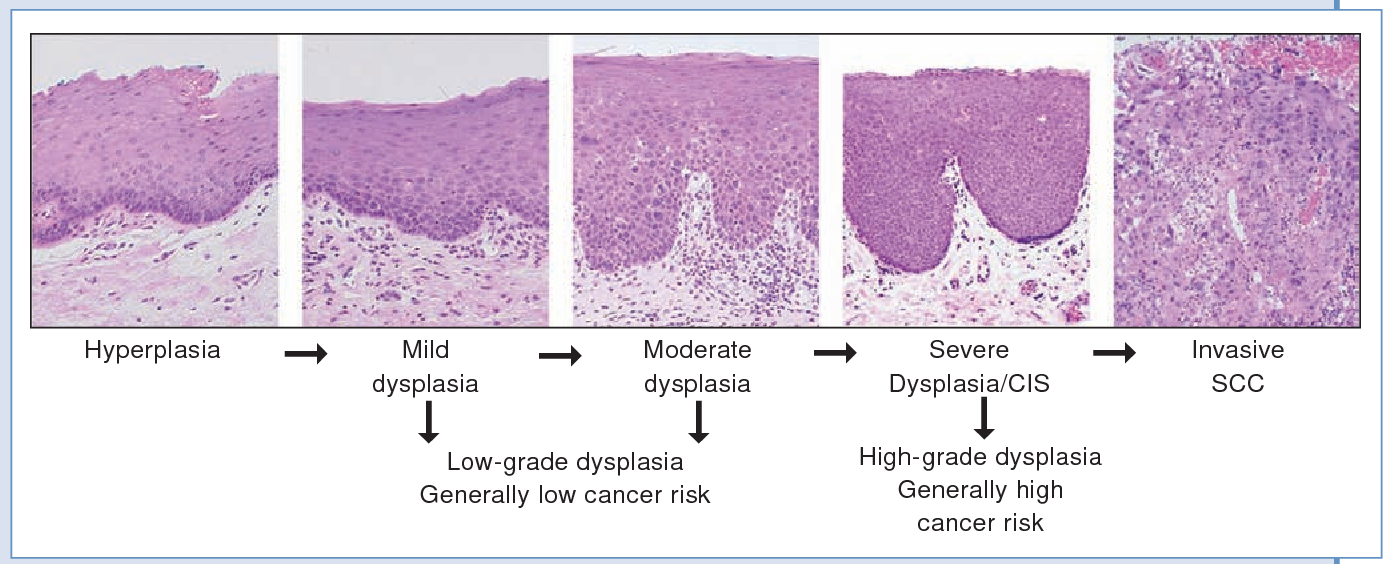 Without treatment, the pain will continue to become worse.
Without treatment, the pain will continue to become worse.
What causes hip dysplasia in adolescents and young adults?
Some teens and young adults are born with mild DDH that becomes symptomatic as they grow. However, the hip joint continues to develop throughout the teen years and sometimes does not develop properly, even if you were not born with DDH. Doctors are not sure why this happens but they do know that the condition affects girls two to four times as often as boys. People with a close relative with hip problems are also at higher risk.
Image
Image
How is hip dysplasia diagnosed in adolescents and young adults?
Doctors typically use variety of tests to determine if dysplasia is the source of hip pain in adolescents and young adults.
The first step is a thorough patient history and physical exam. The doctor will check your hip for range of motion. They may order imaging studies such as an x-ray, MRI, or CT scan to confirm the diagnosis. Ultrasound-guided diagnostic injection can help your doctor determine the location of your hip pain with greater precision.
Ultrasound-guided diagnostic injection can help your doctor determine the location of your hip pain with greater precision.
How is hip dysplasia treated in adolescents and young adults?
The goal of treatment is to restore normal hip function and eliminate pain. Your treatment will depend on the severity of your condition.
Non-surgical treatment options for adolescents and young adults
Mild to moderate cases of hip dysplasia are often treated with physical therapy and nonsteroidal anti-inflammatory drugs (NSAIDs). If you continue to be in pain after these treatments, your physician may suggest surgery.
Surgical options for adolescents and young adults
Periacetabular osteotomy (PAO) is the main surgical treatment for adolescents and young adults with hip dysplasia. PAO may serve as a lifelong treatment if performed before serious damage occurs within the joint.
The goals of PAO are to:
- reduce or eliminate pain
- maximize the function of your hip
- enable you to return to sport or other activity
Hip Dysplasia | Hip Dysplasia in Babies
What is hip dysplasia in babies?
Hip dysplasia in babies, also known as developmental dysplasia of the hip (DDH), occurs when a baby’s hip socket (acetabulum) is too shallow to cover the head of the thighbone (femoral head) to fit properly. DDH ranges in severity. Some babies have a minor looseness in one or both of their hip joints. For other babies, the ball easily comes completely out of the socket.
DDH ranges in severity. Some babies have a minor looseness in one or both of their hip joints. For other babies, the ball easily comes completely out of the socket.
Image
What are the symptoms of hip dysplasia in babies?
Many babies with DDH are diagnosed during their first few months of life.
Common symptoms of DDH in infants may include:
- The leg on the side of the affected hip may appear shorter.
- The folds in the skin of the thigh or buttocks may appear uneven.
- There may be a popping sensation with movement of the hip.
What causes hip dysplasia in babies?
The exact cause is unknown, but doctors believe several factors increase a child’s risk of hip dysplasia:
- a family history of DDH in a parent or other close relative
- gender — girls are two to four times more likely to have the condition
- first-born babies, whose fit in the uterus is tighter than in later babies
- breech position during pregnancy
- tight swaddling with legs extended
Breech position: Babies whose bottoms are below their heads while their mother is pregnant with them often end up with one or both legs extended in a partially straight position rather than folded in a fetal position. Unfortunately, this position can prevent a developing baby’s hip socket from developing properly.
Unfortunately, this position can prevent a developing baby’s hip socket from developing properly.
Tight swaddling: Wrapping a baby’s legs in a straight position may interfere with healthy development of the joint. If you swaddle your baby, you can wrap their arms and torso snugly, but be sure to leave room for their legs to bend and move.
Angela's story
Angela was 5 when her parents brought her to Boston Children’s Hospital, where she was diagnosed with hip dysplasia in both hips.
How is hip dysplasia diagnosed?
Infants in the U.S. are routinely screened for hip dysplasia. During the exam, the doctor will ask about your child’s history, including their position during pregnancy. They’ll also ask if there is any history of hip problems on either parent’s side.
The doctor will do a physical exam and order diagnostic tests to get detailed images of your child’s hip. Typical tests can include:
- Ultrasound (sonogram): Ultrasound uses high-frequency sound waves to create pictures of the femoral head (ball) and the acetabulum (socket).
 It is the preferred way to diagnose hip dysplasia in babies up to 6 months of age.
It is the preferred way to diagnose hip dysplasia in babies up to 6 months of age. - X-ray: After a child is 6 months old and bone starts to form on the head of the femur, x-rays are more reliable than ultrasounds.
How is hip dysplasia treated?
Your child’s treatment will depend on the severity of their condition. The goal of treatment is to restore normal hip function by correcting the position or structure of the joint.
Non-surgical treatment options
Observation
If your child is 3 months or younger and their hip is reasonably stable, their doctor may observe the acetabulum and femoral head as they develop. There’s a good possibility the joint will form normally on its own as your child grows.
Pavlik harness
If your child’s hip is unstable or sufficiently shallow, their doctor may recommend a Pavlik harness. The Pavlik harness is used on babies up to four months old to hold their hip in place while allowing their legs some movement. The baby usually wears the harness all day and night until their hip is stable and an ultrasound shows their hip is developing normally. Typically, this takes about eight to 12 weeks. Your child’s doctor will tell you how many hours a day your child should wear the harness. Typically, children wear the harness 24 hours a day.
The baby usually wears the harness all day and night until their hip is stable and an ultrasound shows their hip is developing normally. Typically, this takes about eight to 12 weeks. Your child’s doctor will tell you how many hours a day your child should wear the harness. Typically, children wear the harness 24 hours a day.
Image
While your child is wearing the harness, their doctor will frequently examine the hip and use imaging tests to monitor its development. After successful treatment, your child will need to continue to see the doctor regularly for the next few years to monitor the development and growth of their hip joint.
Typically, infants’ hips are successfully treated with the Pavlik harness. But some babies’ hips continue to be partially or completely dislocated. If this is the case, your child’s doctor may recommend another type of brace called an abduction brace. The abduction brace is made of lightweight material that supports your child’s hips and pelvis.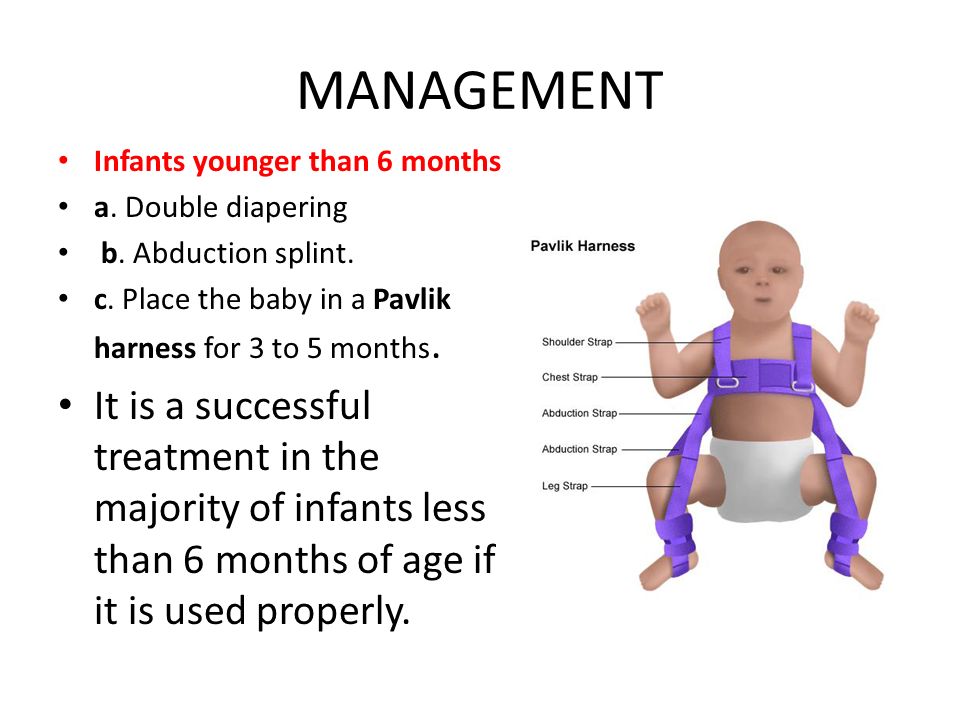 If your child’s hip becomes stable with an abduction brace, they will wear the brace for about eight to 12 weeks. If the abduction brace does not stabilize the hip, your child may need surgery.
If your child’s hip becomes stable with an abduction brace, they will wear the brace for about eight to 12 weeks. If the abduction brace does not stabilize the hip, your child may need surgery.
Image
Surgical treatment options for babies
Closed reduction
If your child’s hip continues to be partially or completely dislocated despite the use of the Pavlik harness and bracing, they may need surgery. Under anesthesia, the doctor will insert a very fine needle in the baby’s hip and inject contrast so they can clearly view the ball and the socket. This test is called an arthrogram.
The process of setting the ball back into the socket after the arthrogram is known as a closed reduction. Once the hip is set in place, technicians will put your child in a spica cast. This cast extends from slightly below the armpits to the legs and holds the hip in place. Different casts cover differing amounts of the child’s legs, based on the condition of their hips. Children typically wear a spica cast for three to six months. The cast will be changed from time to time as your baby grows.
Children typically wear a spica cast for three to six months. The cast will be changed from time to time as your baby grows.
Open reduction
If a closed reduction does not work, your child’s doctor may recommend open-reduction surgery. For this, the surgeon makes an incision and repositions the hip so it can grow and function normally. The specifics of the procedure depend on your child’s condition but it may include reshaping the hip socket, redirecting the femoral head, or repairing a dislocation. After the surgery, your child will need to wear a spica cast while they heal.
Follow-up care
Any infant treated surgically for hip dysplasia must be followed periodically by an orthopedist until they have reached physical maturity. At regular visits, their orthopedic doctor will monitor their hip to ensure it develops normally as they grow. Diagnosing and treating any new abnormality early will increase the chance your child will grow up to be active free from hip pain throughout their childhood, the teen years, and adulthood.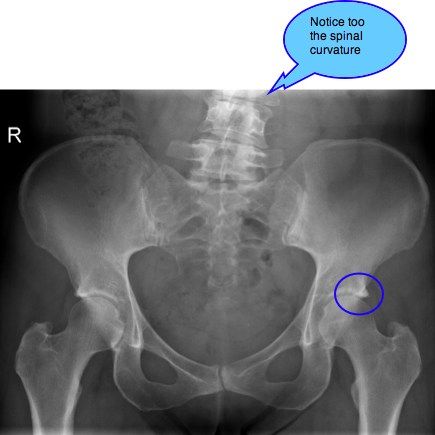
Will treatment affect my child’s ability to walk?
Depending on their age during treatment, your child may start walking later than other kids. However, after successful treatment, children typically start walking as well as other kids. By contrast, children with untreated hip dysplasia often start walking later, and many walk with a limp.
Hip Dysplasia | Programs & Services
Departments
Centers
Programs
Hip Dysplasia | Contact Us
Adolescent Hip Dysplasia - OrthoInfo
The hip is a "ball-and-socket" joint. In a normal hip, the ball at the upper end of the femur (thighbone) fits firmly into the socket, which is a curved portion of the pelvis called the acetabulum. In a young person with hip dysplasia, the hip joint has not developed normally—the acetabulum is too shallow to adequately support and cover the head of the femur. This abnormality can cause a painful hip and the early development of osteoarthritis, a condition in which the articular cartilage in the joint wears away and bone rubs against bone.
This abnormality can cause a painful hip and the early development of osteoarthritis, a condition in which the articular cartilage in the joint wears away and bone rubs against bone.
Adolescent hip dysplasia is usually the end result of developmental dysplasia of the hip (DDH), a condition that occurs at birth or in early childhood. Although infants are routinely screened for DDH, some cases remain undetected or are mild enough that they are left untreated. These patients may not show symptoms of hip dysplasia until reaching adolescence.
Treatment for adolescent hip dysplasia focuses on relieving pain while preserving the patient's natural hip joint for as long as possible. In many cases, this is achieved through surgery to restore the normal anatomy of the joint and delay or prevent the onset of painful osteoarthritis.
The hip is one of the body's largest joints. It is a "ball-and-socket" joint. The socket is formed by the acetabulum, which is a part of the large pelvis bone.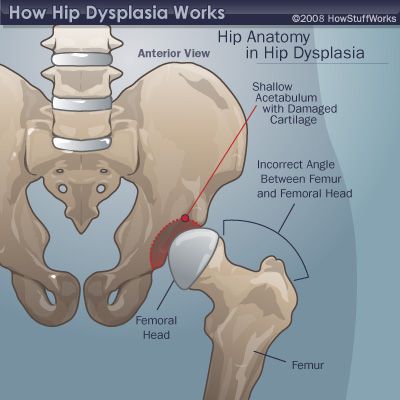 The ball is the femoral head, which is the upper end of the femur (thighbone).
The ball is the femoral head, which is the upper end of the femur (thighbone).
The hip is a "ball-and-socket" joint. In a healthy hip, the head of the femur (ball) stays firmly within the acetabulum (socket).
The bone surfaces of the ball and socket are covered with articular cartilage, a smooth, slippery substance that protects and cushions the bones and enables them to move easily.
The acetabulum is ringed by strong fibrocartilage called the labrum. The labrum forms a gasket around the socket, creating a tight seal and helping to hold the femoral head in place.
In patients with hip dysplasia, the acetabulum is shallow, meaning that the ball, or femoral head, cannot firmly fit into the socket.
As a result of this abnormality, the way that force is normally transmitted between the bone surfaces is altered. The labrum can end up bearing the forces that should normally be distributed evenly throughout the hip joint. In addition, more force is placed on a smaller surface of the hip cartilage and labrum.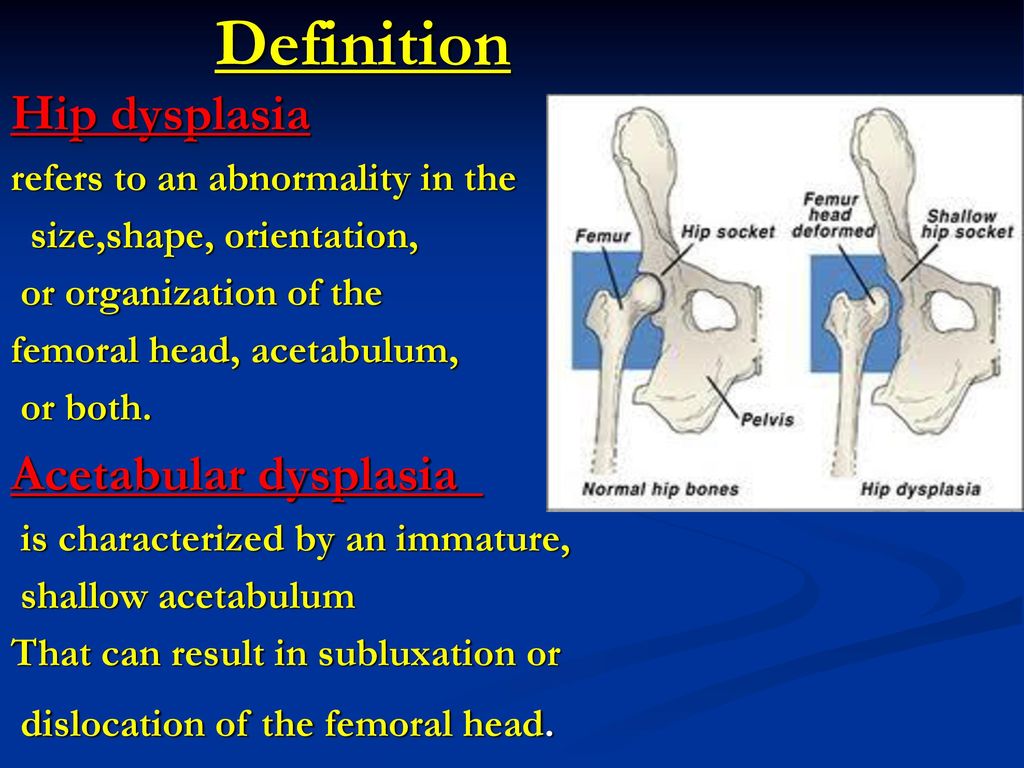 Over time, the smooth articular cartilage becomes frayed and wears away and the labrum becomes torn or damaged. These degenerative changes can progress to early osteoarthritis.
Over time, the smooth articular cartilage becomes frayed and wears away and the labrum becomes torn or damaged. These degenerative changes can progress to early osteoarthritis.
The severity of hip dysplasia can vary from patient to patient. In mild cases, the head of the femur may simply be loose in the socket. In more severe cases, there may be complete instability in the joint and/or the femoral head may be completely dislocated out of the socket.
Adolescent hip dysplasia usually results from developmental dysplasia of the hip (DDH) that is undiscovered or untreated during infancy or early childhood.
DDH can occur in families, passed on from one generation to the next. It can be present in either hip and in any individual. It usually affects the left hip and occurs more often in:
- Girls
- First-born children
- Babies born in the breech position
Hip dysplasia in younger children is not a painful condition. However, over time, pain results when the altered forces in the hip cause degenerative changes to occur in the articular cartilage and the labrum. In most cases, this pain is:
In most cases, this pain is:
- Located in the groin area, although it may sometimes be more toward the outside of the hip
- Occasional and mild initially, but may increase in frequency and intensity over time
- Worse with activity or near the end of the day
Some patients may also experience the feeling of locking, catching, or popping within the groin.
Physical ExaminationDuring the physical examination, your doctor will discuss your child's medical history and symptoms. He or she will move your child's hip in different directions to assess the range of motion and duplicate the pain or discomfort he or she is feeling.
Imaging StudiesIn most cases, adolescent hip dysplasia can be diagnosed with just a physical exam. Your doctor may order imaging studies, however, to rule out other causes for your child's pain and to help confirm the diagnosis.
- X-rays. X-rays provide images of bone, and will help your doctor assess the alignment of the acetabulum and femoral head.
 An x-ray can also show signs of arthritis.
An x-ray can also show signs of arthritis. - Computerized tomography (CT) scans. More detailed than a plain x-ray, CT scans can help your doctor determine the severity of dysplasia.
- Magnetic resonance imaging (MRI) scans. These studies can create better images of the body's soft tissues. An MRI can help your doctor find damage to the labrum and articular cartilage.
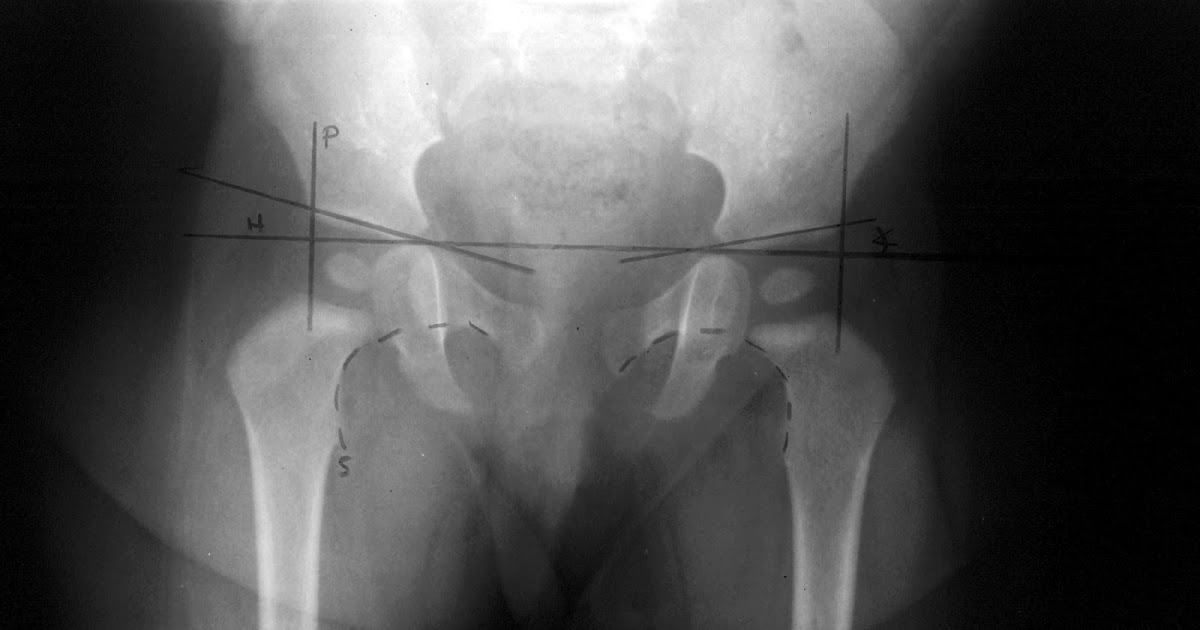
(Left) This x-ray shows two normal hips. (Right) This x-ray shows a dysplastic hip (arrow). The hip socket is shallow and there is only partial coverage of the femoral head.
To Top
Treatment for adolescent hip dysplasia focuses on delaying or preventing the onset of osteoarthritis while preserving the natural hip joint for as many years as possible.
Nonsurgical TreatmentYour doctor may recommend nonsurgical treatment if your child has mild hip dysplasia and no damage to the labrum or articular cartilage.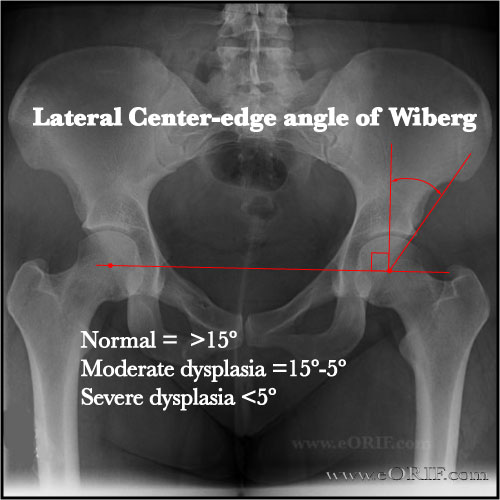 Nonsurgical treatment may also be tried initially for patients who have such extensive joint damage that the only surgical option would be a total hip replacement.
Nonsurgical treatment may also be tried initially for patients who have such extensive joint damage that the only surgical option would be a total hip replacement.
Common nonsurgical treatments for adolescent hip dysplasia include:
Observation. If your child has minimal symptoms and mild dysplasia, your doctor may recommend simply monitoring the condition to make sure it does not get worse. Your child will have follow-up visits every 6 to 12 months so that the doctor can check for any progression that may warrant treatment.
Lifestyle modification. Your doctor may also recommend that your child avoid the activities that cause the pain and discomfort. For a child who is overweight, losing weight will also help to reduce pressure on the hip joint.
Physical therapy. Specific exercises can improve the range of motion in the hip and strengthen the muscles that support the joint. This can relieve some stress on the injured labrum or cartilage.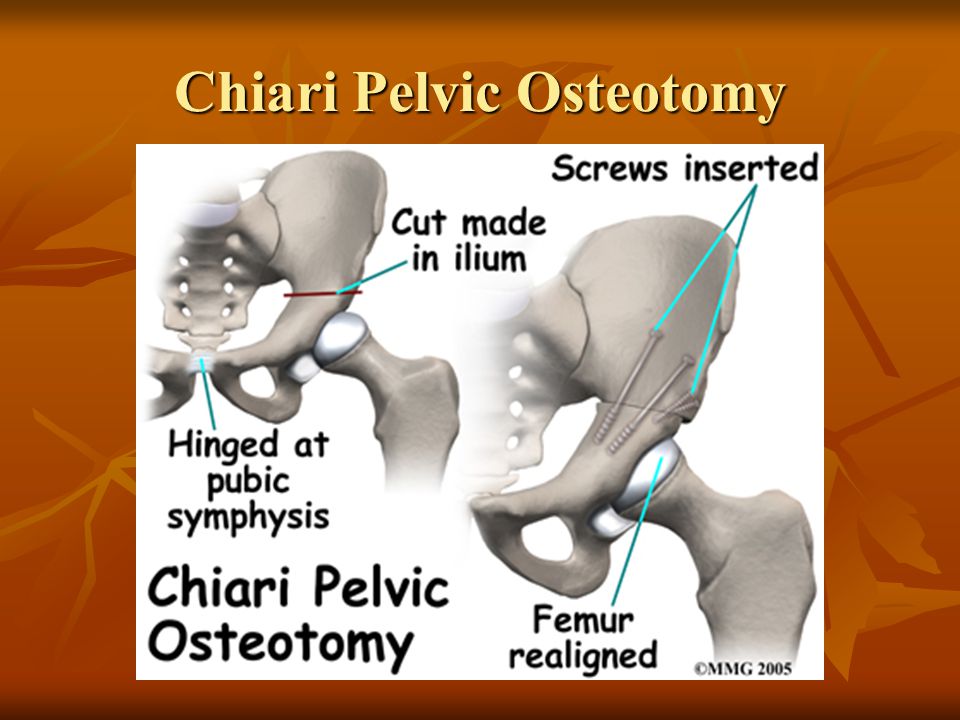
Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen and naproxen, can help relieve pain and reduce swelling in an arthritic joint. In addition, cortisone is an anti-inflammatory agent that can be injected directly into a joint. Although an injection of cortisone can provide pain relief and reduce inflammation, the effects are temporary.
Surgical TreatmentYour doctor may recommend surgery if your child is experiencing pain and has limited damage to the articular cartilage in his or her hip. The surgical procedure most commonly used to treat hip dysplasia is an osteotomy or "cutting of the bone." In an osteotomy, the doctor reshapes and reorients the acetabulum and/or femur so that the two joint surfaces are in a more normal position.
There are different types of osteotomies that can be performed to treat hip dysplasia. The specific procedure your doctor recommends will depend on a number of factors, including:
- Your child's age
- The severity of the dysplasia
- The extent of damage to the labrum
- Whether osteoarthritis is present
- The number of remaining growing years
Periacetabular osteotomy (PAO).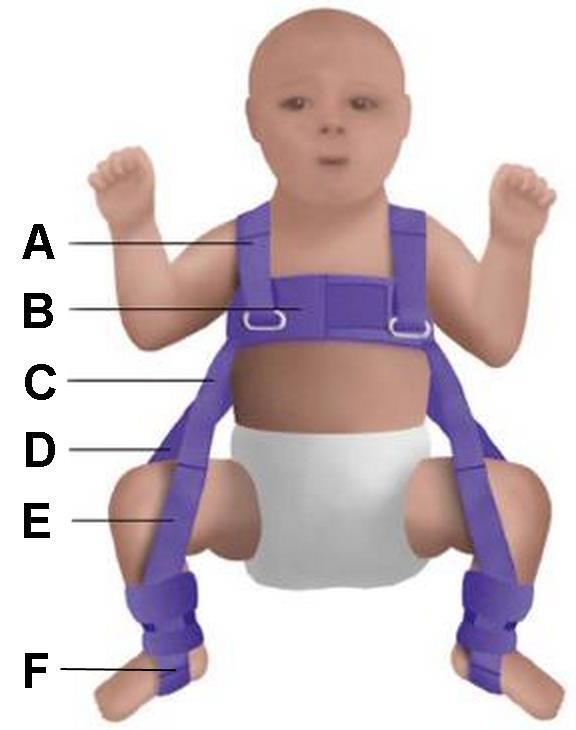 Currently, the osteotomy procedure most commonly used to treat adolescent hip dysplasia is a periacetabular osteotomy (PAO). "Periacetabular" means "around the acetabulum."
Currently, the osteotomy procedure most commonly used to treat adolescent hip dysplasia is a periacetabular osteotomy (PAO). "Periacetabular" means "around the acetabulum."
(A) In a periacetabular osteotomy, four cuts are made in the pelvic bone. (B) The doctor uses a specialized tool to manipulate the bone fragment to gain access to the acetabulum.
Reproduced with permission from Gurd, DP: Late-presenting developmental dysplasia of the hip. Orthopaedic Knowledge Online Journal 2009, Accessed April 2015.
In most cases, PAO takes from 2 to 3 hours to perform. During the surgery, the doctor makes four cuts in the pelvic bone around the hip joint to loosen the acetabulum. He or she then rotates the acetabulum, repositioning it into a more normal position over the femoral head. The doctor will use x-rays to direct the bony cuts and to ensure that the acetabulum is repositioned correctly. Once the bone is repositioned, the doctor inserts several small screws to hold it in place until it heals.
In this x-ray image, the acetabulum has been repositioned using a periacetabular osteotomy, and the bones are held in place with screws.
Arthroscopy. In conjunction with PAO, your doctor may use hip arthroscopy to repair a torn labrum. During arthroscopy, the doctor inserts a small camera, called an arthroscope, into the joint. The camera displays pictures on a television screen, and your doctor uses these images to guide miniature surgical instruments. Arthroscopic procedures may include:
- Labral refixation. In this procedure, the doctor trims the torn and frayed tissue around the acetabular rim and reattaches the torn labrum to the bone of the rim.
- Debridement. In some cases, simply removing the torn or weakened labral tissue can provide pain relief.
As with any surgical procedure, there are risks involved with PAO. Your doctor will discuss each of the risks with you and will take specific measures to help avoid potential complications.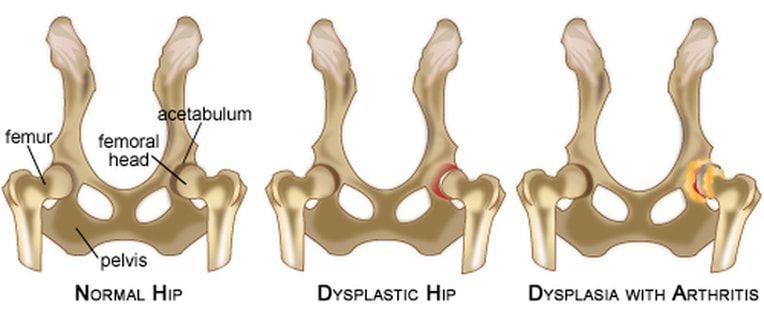
Although the risks are low, the most common complications include:
- Infection
- Blood clots
- Injuries to blood vessels and nerves
- Persistent hip pain
- Failure of the osteotomy to heal
Your child will remain in the hospital for 2 to 4 days after surgery. During this time, he or she will be monitored and given pain medication.
In most cases, full weight-bearing will not be allowed on the operated leg for 6 to 12 weeks while the bones heal in their new position. During this time, your child will need to use crutches.
About 6 weeks after surgery, your child will have a follow-up visit with the doctor. X-rays will be taken so that the doctor can see how well the PAO has healed. During your visit, the doctor will determine when it is safe to put weight on the leg and when physical therapy can begin. The physical therapist will show your child specific exercises to help maintain range of motion and restore strength and flexibility in the hip joint.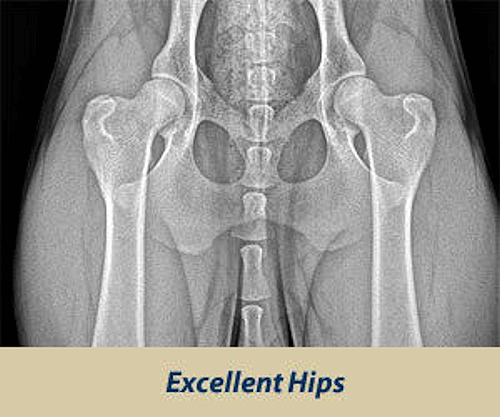
Periacetabular osteotomy is usually successful in delaying the need for an artificial hip joint and relieving pain. Whether or not a total hip replacement will be needed in the future depends on a number of factors, including the degree of osteoarthritis that was present in the joint when the PAO was performed.
To Top
Reviewed by members of
POSNA (Pediatric Orthopaedic Society of North America)
The Pediatric Orthopaedic Society of North America (POSNA) is a group of board eligible/board certified orthopaedic surgeons who have specialized training in the care of children's musculoskeletal health.
Hip dysplasia in young children
At an orthopedist's appointment in the first month of a child's life, an unpleasant detail may turn out: the baby has immaturity of the pelvic bones. Most often, at the same time, the pediatrician pronounces the words “hip dysplasia”, which instantly frighten all young parents without exception. But being scared is not the right thing to do in this situation.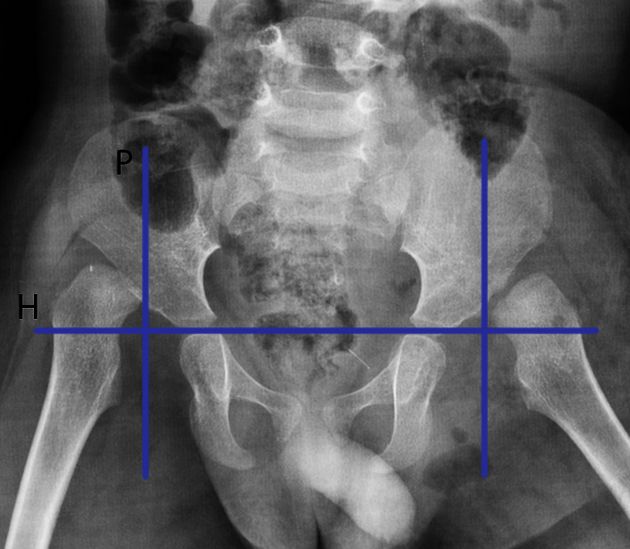 You need to be patient and strictly follow the recommendations of the attending physician. Nevertheless, all doctors will be right when they tell you that joint dysplasia, which was left without the attention of parents and doctors in the first year of a baby’s life, can form the most severe inflammatory processes in a child by the age of two or three, painful hip dislocation and in the future - lameness for life. nine0003
You need to be patient and strictly follow the recommendations of the attending physician. Nevertheless, all doctors will be right when they tell you that joint dysplasia, which was left without the attention of parents and doctors in the first year of a baby’s life, can form the most severe inflammatory processes in a child by the age of two or three, painful hip dislocation and in the future - lameness for life. nine0003
Hip dysplasia is a congenital disorder of the formation of the joint that can cause dislocation or subluxation of the femoral head. In this condition, either underdevelopment of the joint, or its increased mobility in combination with connective tissue deficiency, can be observed. Predisposing factors are unfavorable heredity, gynecological diseases of the mother and pathology of pregnancy. Hip dysplasia is 10 times more common in those children whose parents had signs of congenital hip dislocation and in those born with a breech presentation of the fetus, more often in the first birth. Often, dysplasia is detected during drug correction of pregnancy, during pregnancy complicated by toxicosis. The left hip joint is most often affected (60%), less often the right (20%) or both (20%). The relationship of morbidity with environmental problems has been noted. With untimely detection and lack of proper treatment, hip dysplasia can cause dysfunction of the lower limb and even disability. Therefore, this pathology must be identified and eliminated in the early period of the baby's life. nine0003
Often, dysplasia is detected during drug correction of pregnancy, during pregnancy complicated by toxicosis. The left hip joint is most often affected (60%), less often the right (20%) or both (20%). The relationship of morbidity with environmental problems has been noted. With untimely detection and lack of proper treatment, hip dysplasia can cause dysfunction of the lower limb and even disability. Therefore, this pathology must be identified and eliminated in the early period of the baby's life. nine0003
Hip dysplasia can present in a variety of ways. There are three main forms of dysplasia: acetabular dysplasia - acetabular dysplasia; dysplasia of the proximal femur; rotational dysplasia.
With timely detection and proper treatment, the prognosis is conditionally favorable.
Statistics say: up to 25% of newborn children have some form of hip dysplasia, in other words, they are born with subluxations. In most cases, under the constant supervision of an orthopedist, the joints “grow” on their own and return to the anatomical norm.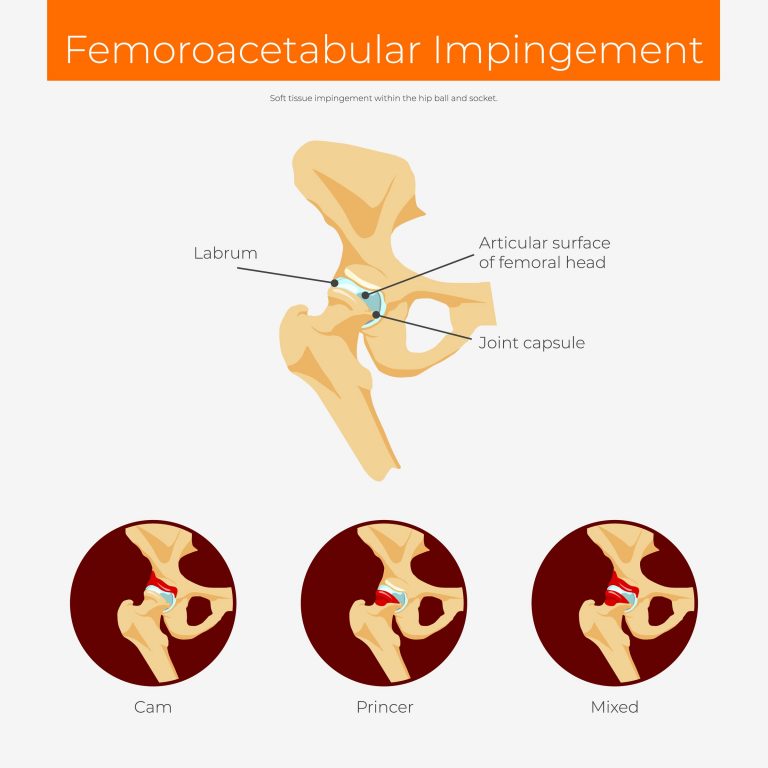 For the rest, they just need a little help. nine0003
For the rest, they just need a little help. nine0003
A preliminary diagnosis can be made even in the maternity hospital. In this case, you need to contact a pediatric orthopedist within 3 weeks, who will conduct the necessary examination and draw up a treatment regimen. In addition, to exclude this pathology, all children are examined at the age of 1-4 months. Particular attention is paid to children who are at risk. This group includes all patients with a history of maternal toxicosis during pregnancy, a large fetus, breech presentation, as well as those whose parents also suffer from dysplasia. If signs of pathology are detected, the child is sent for additional studies. nine0003
To clarify the diagnosis, methods such as radiography and ultrasonography are used. In young children, a significant part of the joint is formed by cartilage, which is not displayed on radiographs, so this method is not used until the age of 2-3 months. Ultrasound diagnostics is a good alternative to X-ray examination in children during the first months of life. This technique is practically safe and quite informative.
This technique is practically safe and quite informative.
With dysplasia, the shape, relationship and size of the structures of the hip joint change significantly. The hip joint of a newborn, even in normal conditions, is an immature biomechanical structure. If the development of the joint is disturbed, the excessively elastic ligaments and the articular capsule are not able to hold the head of the femur in the articular cavity, it shifts upward and laterally (outwards). With certain movements, the femoral head can extend beyond the acetabulum. This condition of the joint is called "subluxation". In severe hip dysplasia, the head of the femur extends completely beyond the acetabulum, a condition called hip dislocation. Hip dysplasia can manifest itself not only as a violation of the acetabulum (acetabular dysplasia), but also as an abnormal development of the proximal femur. nine0003
Hip dysplasia is suspected in the presence of shortened hip, asymmetric skin folds, limited hip abduction, and Marx-Ortolani slipping.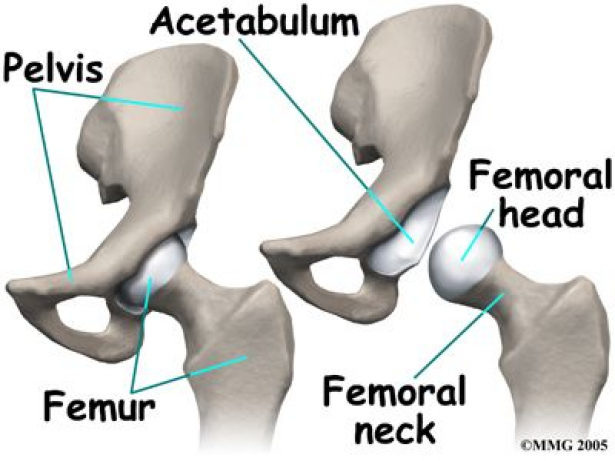 Asymmetry of the inguinal, popliteal and gluteal skin folds is usually better detected in children older than 2-3 months. During the inspection, they pay attention to the difference in the level of location, shape and depth of the folds. It should be borne in mind that the presence or absence of this symptom is not enough to make a diagnosis. With bilateral dysplasia, the folds may be symmetrical. In addition, the symptom is absent in half of the children with unilateral pathology. The asymmetry of the inguinal folds in children from birth to 2 months is of little information, since it sometimes occurs even in healthy infants. But the most important sign indicating congenital dislocation of the hip is the “click” or Marx-Ortolani symptom. Slowly abduct the hips evenly to both sides. With normal relations in the joints, both hips in the position of extreme abduction almost touch the outer surfaces of the table plane. With dislocation, the femoral head slips into the acetabulum at the moment of abduction, which is accompanied by a characteristic push - the moment when the femoral head from the dislocation position is reduced into the acetabulum.
Asymmetry of the inguinal, popliteal and gluteal skin folds is usually better detected in children older than 2-3 months. During the inspection, they pay attention to the difference in the level of location, shape and depth of the folds. It should be borne in mind that the presence or absence of this symptom is not enough to make a diagnosis. With bilateral dysplasia, the folds may be symmetrical. In addition, the symptom is absent in half of the children with unilateral pathology. The asymmetry of the inguinal folds in children from birth to 2 months is of little information, since it sometimes occurs even in healthy infants. But the most important sign indicating congenital dislocation of the hip is the “click” or Marx-Ortolani symptom. Slowly abduct the hips evenly to both sides. With normal relations in the joints, both hips in the position of extreme abduction almost touch the outer surfaces of the table plane. With dislocation, the femoral head slips into the acetabulum at the moment of abduction, which is accompanied by a characteristic push - the moment when the femoral head from the dislocation position is reduced into the acetabulum. nine0003
nine0003
Another symptom that indicates the pathology of the joint is limitation of movement. In healthy newborns, the legs are retracted to a position of 80-90 ° and freely placed on the horizontal surface of the table. When the abduction is limited to 50-60°, there is reason to suspect a congenital pathology. In a healthy child of 7-8 months, each leg is retracted by 60-70°, in a baby with congenital dislocation - by 40-50°.
The main method of preventing hip dysplasia is wide swaddling. As soon as at 19In 1971, the national health program promoted wide swaddling; already a few years later, only 0.2% of children over the age of one year suffered from this disease. Orthopedic devices that securely fix the baby's legs in a bent and divorced form. These devices include all kinds of splints (a kind of spacers between the legs), plastic corsets and even plaster retainers. The most popular fixing device is the so-called Pavlik stirrups. Moreover, Pavlik here is not a boy who was the first to try a miracle unit on himself, but a talented Czech orthopedic doctor who came up with the idea of fixing a baby’s legs with a special harness.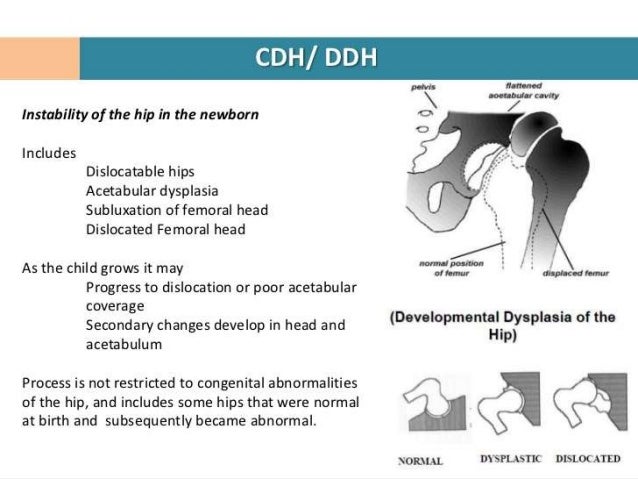 Massage and gymnastics. Your attending orthopedist will teach you specific exercises and techniques for daily massage and gymnastics, since the set of manipulations strictly depends on how the joint is under-formed. Use of carriers, slings, backpacks and car seats. But only those models that allow the baby to hold freely, legs wide apart. In the countries of Asia and Africa, where women have been carrying their babies on themselves since ancient times, tying them on their backs or on their stomachs (that is, the child spends all the time in a sitting position, with legs wide apart), there is no such phenomenon as hip dysplasia in children at all. exist. nine0003
Massage and gymnastics. Your attending orthopedist will teach you specific exercises and techniques for daily massage and gymnastics, since the set of manipulations strictly depends on how the joint is under-formed. Use of carriers, slings, backpacks and car seats. But only those models that allow the baby to hold freely, legs wide apart. In the countries of Asia and Africa, where women have been carrying their babies on themselves since ancient times, tying them on their backs or on their stomachs (that is, the child spends all the time in a sitting position, with legs wide apart), there is no such phenomenon as hip dysplasia in children at all. exist. nine0003
Treatment should begin as soon as possible. Alas, the treatment of dysplasia is not a quick matter. As a rule, it takes several months, sometimes - a year and a half. This is understandable: the hip joint cannot take the correct position and acquire reliable ligaments in a couple of days. But believe me, your efforts and patience are worth it! Of course, it’s not too pleasant to “hobble” your baby with orthopedic stirrups every day, and swaddle him with a pillow between his legs or “shackle” him in a plastic corset at night.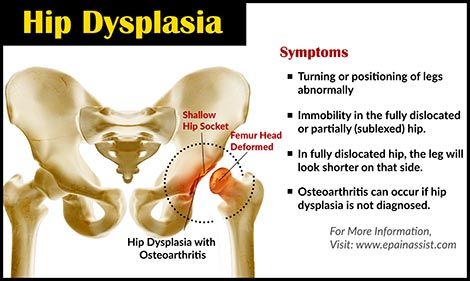 But it’s better to be a little sad before he is even a year old, so that later you can see how famously he dances at his 17-18 years old at the prom. The opposite is true: to be touched by crooked legs now and do nothing, and then reap the terrible consequences of your carelessness ... Isn't it? nine0003
But it’s better to be a little sad before he is even a year old, so that later you can see how famously he dances at his 17-18 years old at the prom. The opposite is true: to be touched by crooked legs now and do nothing, and then reap the terrible consequences of your carelessness ... Isn't it? nine0003
Radiologist of ME "3rd City Children's Clinical Clinic"
Krasovsky Vyacheslav Fedorovich
Hip Dysplasia - clinic "Family Doctor".
“Your child has hip dysplasia” - very often this phrase from the mouth of an orthopedic doctor causes a state close to emotional shock in the parents of the baby. But is everything so gloomy and scary, and what kind of pathology is this?
Dysplasia - this term means a violation of the formation of any organ or body system. In this material we will talk about hip dysplasia. nine0003
Hip dysplasia is understood as a violation of the formation of the hip joint, which captures all the elements that make up the joint: the bone and cartilage base, the ligamentous-capsular apparatus and the muscle component.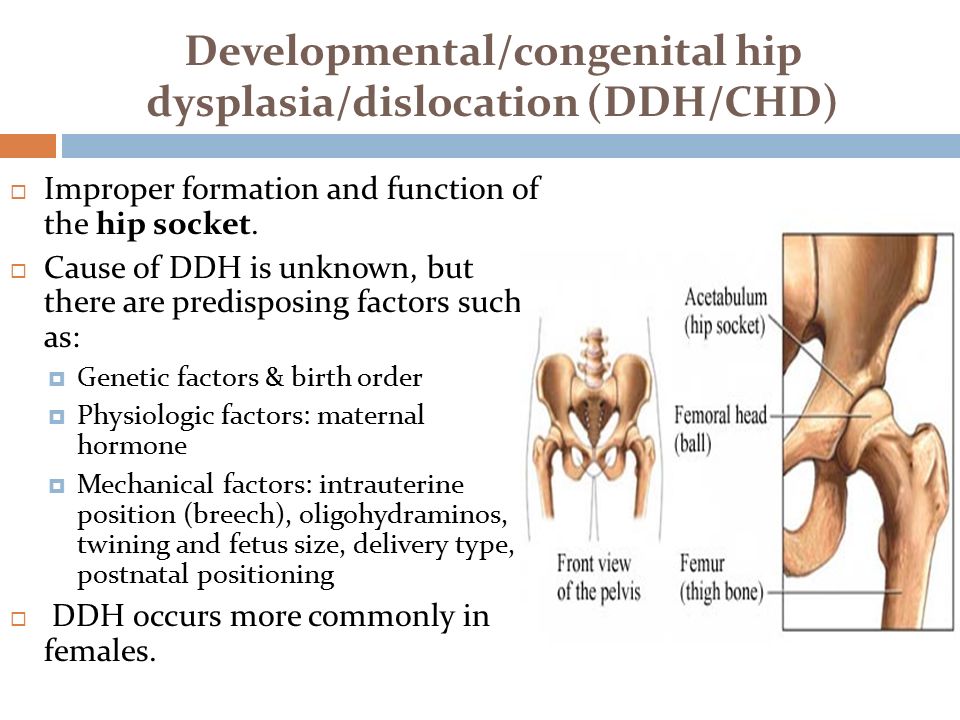 This definition is quite broad and includes the physiological immaturity of the hip joint, preluxation, subluxation and dislocation of the hip.
This definition is quite broad and includes the physiological immaturity of the hip joint, preluxation, subluxation and dislocation of the hip.
Physiological immaturity consists in the incomplete formation of the joint components without violating the congruence (correct matching) of the articular surfaces of the bones and, as a rule, requires minimal treatment or only dynamic observation, and it is this form of hip joint pathology that is mainly assigned the diagnosis of "dysplasia", although this is not entirely correct. terminologically. With pronounced immaturity of the hip joint, treatment is necessary to create favorable conditions for the proper maturation of the joint components. nine0003
Predislocation of the hip is already a pathology of the joint associated with the lack of stability of the femoral head in another component of the hip joint - the acetabulum and already requires close attention. In the absence of adequate treatment, hip predislocation can lead to the development of joint deformity (arthrosis), which leads to pain and impaired joint mobility, and can also lead to hip dislocation after the start of walking.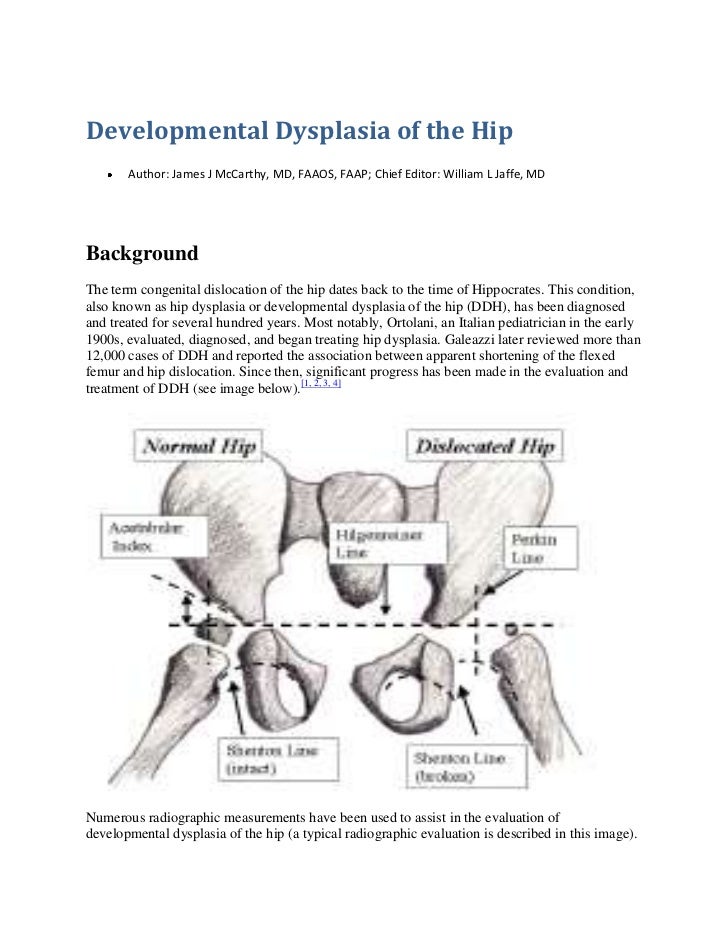
Dislocation of the hip is the most severe form of the pathology of the development of the hip joint, which consists in the almost complete discrepancy between the articular surfaces of the femoral head and the acetabulum. Such a malformation of the joint requires maximum efforts for a thorough diagnosis and active and prompt treatment. Late diagnosis or inadequate treatment leads to gross impairment of the hip joint mobility and, ultimately, leads to disability. nine0003
Now we understand why so much attention is paid to hip dysplasia by pediatricians and orthopedists. Why is it the hip joint that is most susceptible to these misfortunes?
The fact is that the hip joint, due to its anatomical and physiological characteristics, is the most loaded joint in our body, and a failure in one of its constituent components leads to dysfunction of the joint and, ultimately, to a deterioration in the quality of life of the patient. That is why the diagnosis of hip dysplasia can so often be heard from the lips of an orthopedist, although one cannot but recognize the fact of some overdiagnosis of this pathology, but given the severity of the consequences in the absence of treatment, this is still justified.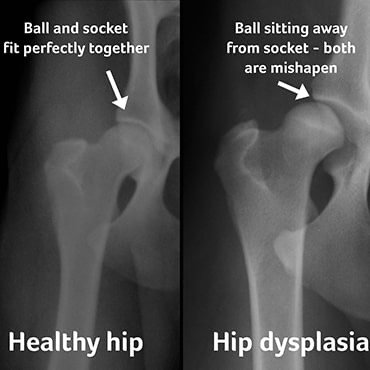 nine0003
nine0003
According to statistics, the incidence of hip dysplasia is 4-6 cases per 1000 newborns, in girls it occurs 6-7 times more often. Unilateral lesion predominates over bilateral (more often the left hip joint is affected). There is inheritance from mother to daughter. Quite a lot of factors leading to impaired intrauterine joint formation have been noted, among them are breech presentation of the fetus, narrowness of the uterus, oligohydramnios, toxic and biological (primarily viral diseases of the mother during pregnancy) factors and much more. nine0003
When and by what methods can and should hip dysplasia be diagnosed? Can a mother herself suspect the presence of hip dysplasia in a child and, if so, with what methods? The answer to this question depends on the severity of the joint injury. Let's try to answer this question by tying the timing and methods of diagnosis to the age of the baby.
When conducting ultrasound diagnostics during pregnancy, it is possible to diagnose only gross violations - subluxation and dislocation of the hip, that is, those changes in which the articular surface of the femoral head does not correspond to the surface of the acetabulum of the child's pelvis.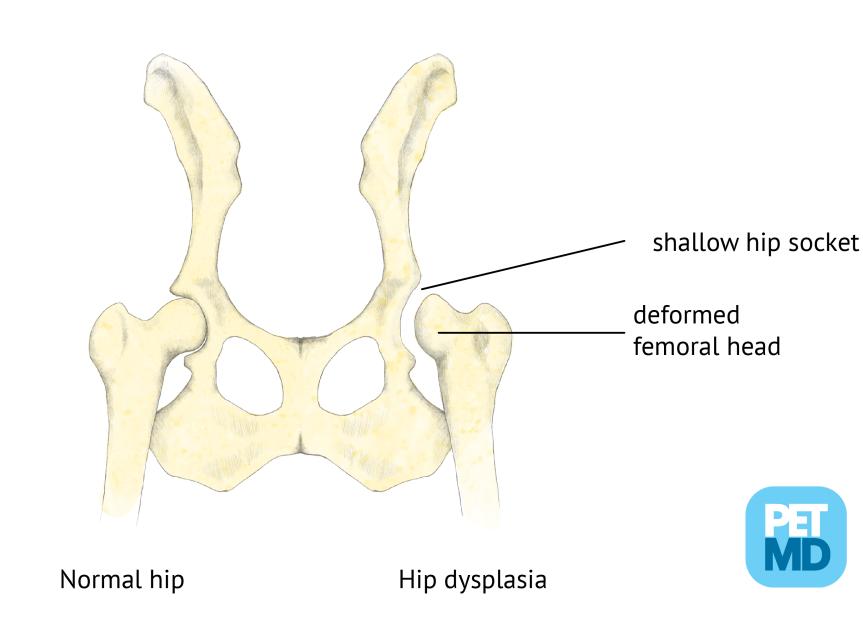 nine0003
nine0003
In the first 7-10 days of a child's life, an examination can reveal a “click symptom” or “slipping symptom” - dislocation and reduction of the hip in the joint. These symptoms are revealed in a child as follows: in the supine position, the legs are bent at the knee and hip joints at an angle of 90 degrees. The thumbs are located on the inner surface of the child's thighs, the index and middle fingers on the outer. With careful abduction and traction of the hips, the femoral head is set into the acetabulum with a characteristic click. nine0003
After the 2nd - 3rd week of a child's life, limitation of hip abduction comes to the fore in the diagnosis of hip dysplasia. To identify it, the legs of the child bent at the knee and hip joints in the supine position are bred without violence. Normally, it is possible to spread the hips to an angle of 85-90 degrees to the surface. With increased muscle tone and spasm of the muscles adducting the thigh, abduction can be limited to an angle of about 70 degrees, but such a restriction of hip abduction can also be caused by impaired joint formation.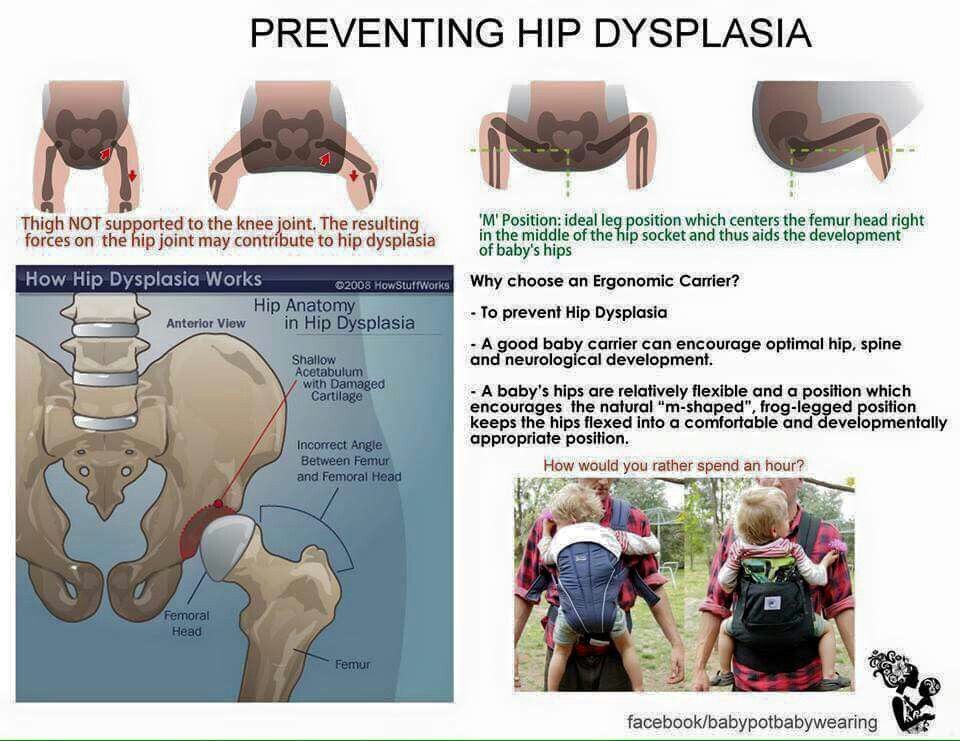 Limitation of hip abduction on one side in most cases is a sign of pathology from the hip joint. nine0003
Limitation of hip abduction on one side in most cases is a sign of pathology from the hip joint. nine0003
In favor of the pathology of the hip joint, symptoms such as shortening of one limb, turn of the foot on the side of the lesion outward from the middle position (external rotation of the foot) also speak.
The most widely known in parents (so to speak, "mommy symptom") - the asymmetry of the subgluteal folds - is not absolute and can be caused by many factors, but its importance in the diagnosis of hip dysplasia should not be underestimated, since this is the most common question that is addressed to orthopedic doctor. nine0003
To confirm the diagnosis of hip dysplasia and control the dynamics of treatment, ultrasound diagnostics are currently widely used. The positive aspects of this method of examination include painlessness, non-invasiveness, relative safety and a sharp increase in recent availability. Also, with the help of an ultrasound examination of the joint, minimal changes in the structure of the hip joint can be detected.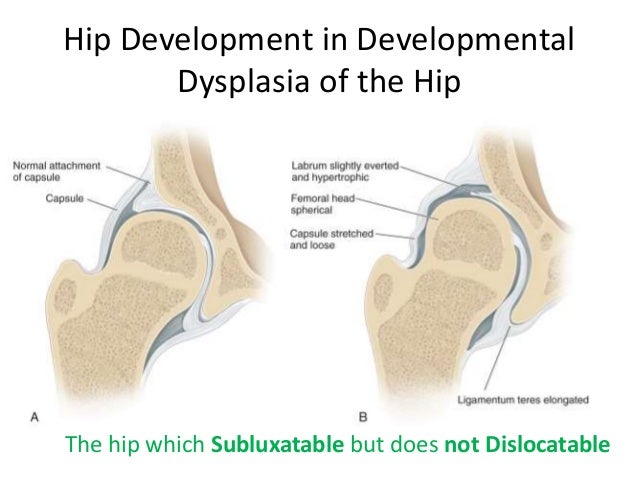 But, unfortunately, this examination method does not always give accurate results (its reliability is about 85-90%. Nevertheless, to date, ultrasound diagnostics is the main method of screening for the diagnosis of hip dysplasia.
But, unfortunately, this examination method does not always give accurate results (its reliability is about 85-90%. Nevertheless, to date, ultrasound diagnostics is the main method of screening for the diagnosis of hip dysplasia.
In the case when the clinical picture differs from the data of the ultrasound examination or in case of late diagnosis of the pathology of the hip joint, the X-ray method is used. With a correctly performed radiograph, the picture of the structure of the joint and the position of the femoral head in the joint become completely clear. But due to the rather large radiation exposure during radiography, this examination method is used as rarely as possible. nine0003
In children older than a year, the main symptom is lameness on the affected side when walking or a "duck" gait with a bilateral process. Diagnosis at this age is belated. The clinical picture in this case almost always requires confirmation by x-ray, since it is necessary to accurately determine the relative position of the joint components.
And so, the child was diagnosed with hip dysplasia, what to do next and how to help the baby? nine0003
Treatment of hip dysplasia should be started as early as possible. The goal of the treatment is to center the femoral head in the joint and create conditions for the formation of the entire acetabulum. Early, most gentle, but systematic treatment allows you to completely restore the anatomy and function of the underdeveloped hip joint.
The centering of the hip in the joint in the early stages of treatment is achieved by wide swaddling - two diapers are placed between the divorced hips of the child and fixed with a third. In severe degrees of hip dysplasia, special splints are used to center the femoral head (Pavlik's stirrups, Freik's pillow, etc.). When using these tires, parents may have questions and difficulties in caring for their baby, here are some tips to help you and your baby adjust during this period: nine0003
1. Only a baby diaper (disposable or gauze) should be under the stirrups or pillow.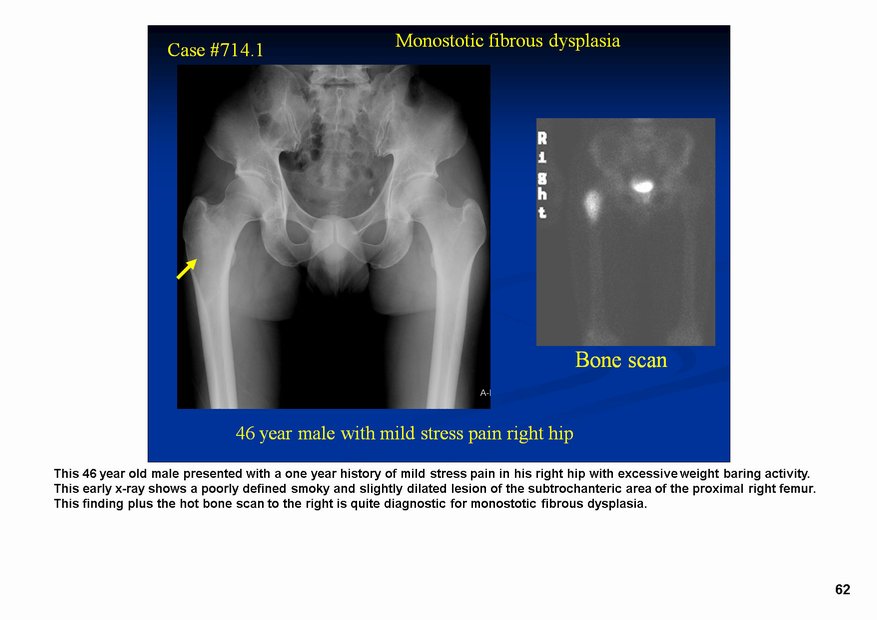 If you prefer to use gauze diapers, wear oilcloth panties that have zippers on the sides.
If you prefer to use gauze diapers, wear oilcloth panties that have zippers on the sides.
2. When changing a diaper, do not lift the child by the legs, but put your hand under the buttocks.
3. The vests can be changed without removing the stirrups: unfasten the shoulder straps from the chest strap and remove the vest over your head. nine0003
Over the tires you can wear loose pants, suits, dresses.
4. During the splint period, bathing the child is less frequent, so it is necessary to examine the skin under the straps, under the knees and around the neck 2-3 times a day to make sure there are no signs of inflammation (redness) of the skin. During this period, it is necessary to wipe the baby's skin with a soft cloth soaked in warm water. When carrying out water procedures, you can unfasten one foot part of the stirrup, but do not remove it, and keep the leg in a bent and retracted position. nine0003
5. It is also necessary to monitor the hygienic condition of the tire itself, it must always remain dry, avoid getting powders and lotions under the belts, this can cause inflammation on the baby's skin.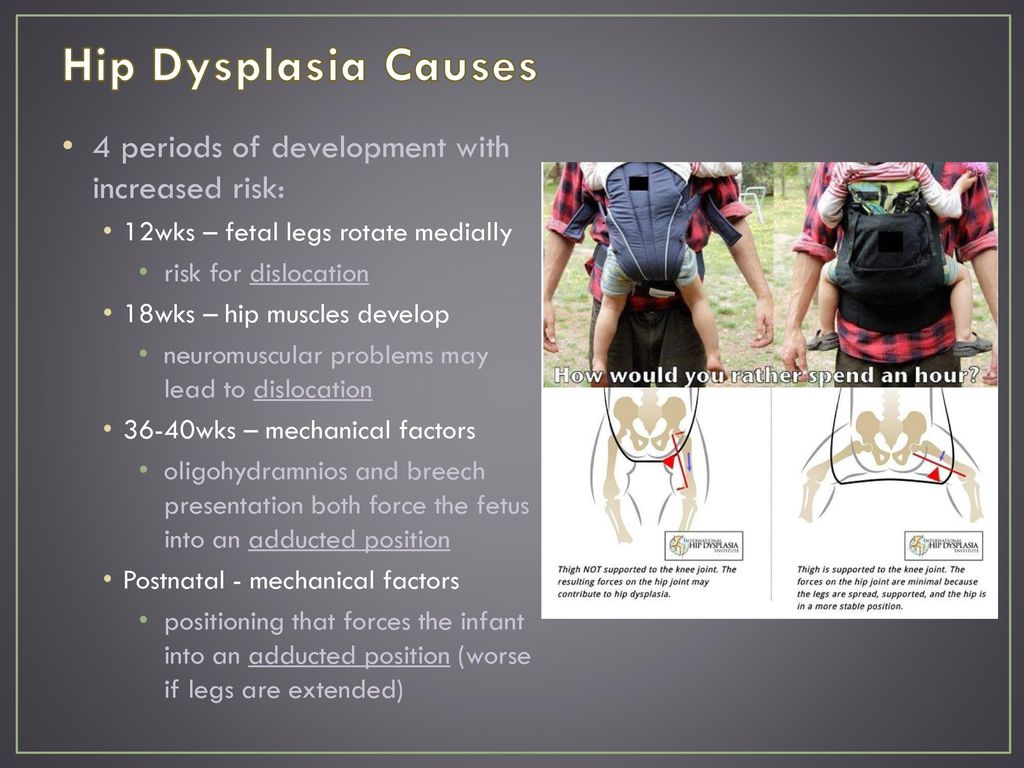
6. When feeding, be especially careful to ensure that the baby's hips do not come together.
The wearing of these devices (orthoses) is long-term - from 3 months to a year, and it is extremely important for the parents of a child who has been diagnosed with hip dysplasia to be patient and not be cowardly during the treatment period and meticulously follow the doctor's prescriptions. nine0003
After centering the femoral head, they begin massage and therapeutic exercises aimed at creating the correct ratio of the articular surfaces. We can recommend some exercises that are easy to do at home.
1. In the position of the child lying on his back, we bend the child's legs at the knee and hip joints as much as possible, and then fully straighten them.
2. In the previous starting position, we bend the child's legs at the knee and hip joints at a right angle, moderately spread the hips and, giving a moderate load along the axis of the hips, perform rotational movements with the hips. nine0003
nine0003
3. In the position of the child lying on his back, we breed the legs of the child bent at the knee and hip joints as much as possible to the surface of the table.
All exercises are performed 8-10 times 3-4 times a day.
Also during this period, physiotherapy (paraffin baths, electrophoresis with calcium and phosphorus preparations) is used to improve the nutrition of the joint components and complex orthopedic massage.
In cases of late diagnosis of hip dysplasia or in the absence of adequate treatment in the early stages, treatment is carried out by long-term staged plastering, as well as surgical treatment, but in these cases there are no standard treatment regimens and patient care tactics are developed individually. nine0003
After treatment of hip dysplasia, the child should be kept in the dispensary with an orthopedist for a long time - from 3 to 5 years until the end of growth. If necessary, control radiographs are performed once every 2 years to monitor the correct development of the joint.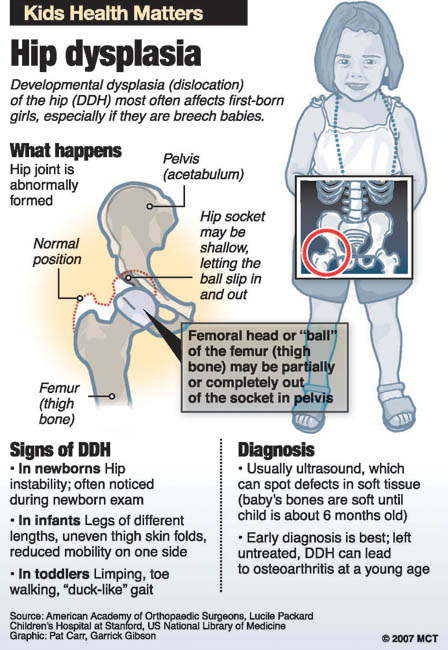 Also, restrictions on the load on the joint are often imposed. For children treated for hip dysplasia, it is desirable to visit specialized orthopedic groups in preschool institutions. nine0003
Also, restrictions on the load on the joint are often imposed. For children treated for hip dysplasia, it is desirable to visit specialized orthopedic groups in preschool institutions. nine0003
In severe degrees of hip dysplasia, functional disorders are, as a rule, lifelong in nature, even with timely and properly conducted treatment.
So what do the parents of the baby need to do in order to recognize hip dysplasia in time and, if this diagnosis was made to the child, to prevent serious complications?
First of all, it is necessary to show the child to the orthopedist in time. nine0049 The recommended terms of examination by an orthopedist are 1 month, 3 months, 6 months and 1 year.
If the orthopedist nevertheless made a diagnosis of hip dysplasia, then the effectiveness of treatment by 50 percent depends on the correct and timely fulfillment by the child's parents of the doctor's prescriptions. It is important to remember that the sooner treatment is started, the better the results and the less chance of severe complications.