How to help an addicted child
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders. This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
SAMHSA Behavioral Health Treatment Services Locator
HomeWelcome to the Behavioral Health Treatment Services Locator, a confidential and anonymous source of information for persons seeking treatment facilities in the United States or U.S. Territories for substance use/addiction and/or mental health problems.
PLEASE NOTE: Your personal information and the search criteria you enter into the Locator is secure and anonymous. SAMHSA does not collect or maintain any information you provide.
Please enter a valid location.
please type your address
-
FindTreatment.
 gov
gov Millions of Americans have a substance use disorder. Find a treatment facility near you.
-
988 Suicide & Crisis Lifeline
Call or text 988
Free and confidential support for people in distress, 24/7.
-
National Helpline
1-800-662-HELP (4357)
Treatment referral and information, 24/7.

-
Disaster Distress Helpline
1-800-985-5990
Immediate crisis counseling related to disasters, 24/7.
- Overview
- Locator OverviewLocator Overview
- Locator OverviewLocator Overview
- Finding Treatment
- Find Facilities for VeteransFind Facilities for Veterans
- Find Facilities for VeteransFind Facilities for Veterans
- Facility Directors
- Register a New FacilityRegister a New Facility
- Register a New FacilityRegister a New Facility
- Other Locator Functionalities
- Download Search ResultsDownload Search Results
- Use Google MapsUse Google Maps
- Print Search ResultsPrint Search Results
- Use Google MapsUse Google Maps
- Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
 Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). - Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). Find programs providing methadone for the treatment of opioid addiction (heroin or pain relievers).
The Locator is authorized by the 21st Century Cures Act (Public Law 114-255, Section 9006; 42 U.S.C. 290bb-36d). SAMHSA endeavors to keep the Locator current. All information in the Locator is updated annually from facility responses to SAMHSA’s National Substance Use and Mental Health Services Survey (N-SUMHSS). New facilities that have completed an abbreviated survey and met all the qualifications are added monthly. Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Regional operator of the state bank for children left without parental care in the Sverdlovsk region
Dependent teenager and codependent parent: features of interaction in a couple
Author - Elizaveta Pavlova, a practicing psychologist. Source - http://psyholog-in-web.ru
co-dependent". I will describe here for memory what I remember about that training.
To begin with, I don't think it's necessary to explain that if an addict is found in a family, then you have to look for a co-dependent somewhere next to him? It seemed to me that this was common knowledge, but no: to one colleague, recounting the results of the seminar, I stated for a long time that it was necessary to work with the family as with a system. And it will not be possible to get the addict out of the problem alone - it is necessary to help his relatives and relatives.
And it will not be possible to get the addict out of the problem alone - it is necessary to help his relatives and relatives.
The psychological center where I was for teenagers, so they talked mainly about addicted teenagers, but many approaches are applicable to adult addicts as well.
In general, a dependent child/codependent parent couple comes to see a psychologist. The parent, by the time of the meeting with the psychologist, is already fairly chewed up by guilt, the experience of “I am a bad mother / father” and has tried a lot of approaches in ridding the other of addiction. And also already quite far advanced in hiding the dependence of the child on others and doing as much as possible for him. The behavior of the codependent (i.e., adult) in this couple is characterized by:
- A propensity to rescue (with all the ensuing consequences, see "Karpman's Triangle"): "Without me, he will be lost"
- Focusing solely on the addict, his addiction, his needs and interests, and forgetting his own interests and needs (in general, codependence is a great opportunity to forget about your own unresolved problems and instead try to cure, save and make others happy).
 Therefore, a co-dependent with a light heart spits on his goals and interests, and his whole life revolves around: “Did the child use / did not use today? How to stop drinking? How to save him???
Therefore, a co-dependent with a light heart spits on his goals and interests, and his whole life revolves around: “Did the child use / did not use today? How to stop drinking? How to save him??? - Tendency to control the addict, even in small things (especially in small things), harassment and accusations (“You missed the test again! What were you thinking, you are ruining your life!”
- Isolation : codependents are very ashamed of their own family problems, hide them from others - well, they think they do - and try to distance themselves from other people who are not included in the vicious system of addiction / codependency. They are very ashamed to ask for help, and make contact with a psychologist only as a last resort, often driven by external circumstances (school, law enforcement agencies).
The addicted teenager in this couple, most likely, didn’t choose to go to a psychologist at all, he didn’t need it for a hundred years, he was driven by the combined efforts of the school, the police and his parents. An addict who has finally reached a psychologist has been using, most likely, for a very long time, and a variety of methods have already been applied to him. These methods did not work, now you need to go here,
An addict who has finally reached a psychologist has been using, most likely, for a very long time, and a variety of methods have already been applied to him. These methods did not work, now you need to go here, check in to say: “And the psychologist didn’t help me!” . The addict at this stage is already well acquainted with the withdrawal syndrome (“withdrawal”, panic attacks, emotional discomfort), repeatedly gave “vows” (“From tomorrow - never again!”), Most often, there is anosognosia (i.e., denial of the problem, denial of the disease).
Most likely, the young addict has already committed antisocial actions in order to acquire the substance on which the addiction has arisen (I repeat, in our country, only a few reach a psychologist at an early stage of addiction, most likely, the problem is already running) - he stole, deceived, extorted, robbed and etc. In the behavior of the addict, pronounced physiological reactions to the abolition of use are noticeable: arousal, sweating, excitement. Interest in other activities besides the use and obtaining of the substance is reduced or completely absent.
Interest in other activities besides the use and obtaining of the substance is reduced or completely absent.
What are the two participants in the couple who turned to the psychologist expecting (explicitly or implicitly)?
The parent (codependent) brings certain expectations into contact with the psychologist:
- "Fix it for me" , i.e., do something so that, as if by magic, the child stops using. Yes, no more changes are needed, in our family there are no special problems. Well, only this one uses, and everything else is fine - not without difficulties, but, in general, everything is fine. A child is an object that needs to be remade at the request of adults in the direction that the parent considers correct.
- The child's addiction is presented as a private, local problem . That is, the idea that the problem of addiction is a SYSTEMIC one, and that everything needs to change, and changing relationships in the family is also necessary for recovery, the codependent parent accepts with surprise, and often with hostility.
 “Everything is fine with us, you are treating HIM, and leave us alone.”
“Everything is fine with us, you are treating HIM, and leave us alone.” - Parent eats wine , great guilt and shame that the family looks dysfunctional in the eyes of others. Accordingly, in the best traditions of "Doctor House", the parent tries to hide some of the problematic situations, not to tell, and even to "keep face" in front of the psychologist. The parent is in pain, and he demands from the psychologist: “Tell me that I am a good parent, the problem is something else!” (most often - in a "really intolerable, trashy child"). It is hard for a parent to endure shame and guilt, he strives to push them either habitually - on a child, school, bad company, or in a new way, on a “non-professional psychologist”.
- The parent is angry, very angry, offended and exhausted . In many of his actions in relation to the child, in addition to the obvious care and concern, there is also pain, rage, anger, and aggression. Naturally, for their manifestation in the address of their own child, the parent again feels guilty.
 The knot is tightened.
The knot is tightened. - The parent's resources at the stage of contacting a psychologist are already, usually, at the end of : the option "We can handle it ourselves, without any psychotic" did not work anymore. So the parent comes to the psychologist exhausted, humiliated, exhausted and angry. And joyfully offers: "SAVE MY CHILD!". Well, that is, he wants to shift the obligation to “save” an addicted teenager to the professional shoulders of a psychologist.
And many insufficiently developed psychologists fall for this, and joyfully begin to "save".
A teenager (addicted), most often, goes to a psychologist:
- To endure what they are forced to do - again these crazy adults have come up with something, you have to wait, be patient, and then you can again live “normally” (“normal” for an addict implicitly implies use).
- With an implicit desire to provoke a parent and / or a psychologist into such behavior against which one can look good.
 Therefore, the child will not make contact, will show aggression and unwillingness to cooperate: “Make me, well, make me! Oh, you are! Are you forcing me??? Then I won’t communicate with you, such bastards!” – leaves, slams the door and starts “normal life” again (using first to relax and calm down).
Therefore, the child will not make contact, will show aggression and unwillingness to cooperate: “Make me, well, make me! Oh, you are! Are you forcing me??? Then I won’t communicate with you, such bastards!” – leaves, slams the door and starts “normal life” again (using first to relax and calm down). - "Tell the ancestors to leave me behind!" is, oddly enough, a rather sensible thought, which parents are prevented from accepting by a tangle of emotions from anxiety, guilt, fear and aggression. But, again, initially the teenager himself does not want to change anything in family relationships and in his behavior, and this “leave me alone” means that he just wants to get the opportunity to “just live normally” (see the previous paragraphs - i.e. , calmly, without interference from time to time to use).
Separately, during the training, it was noted that for a teenager, the main difficulty in getting rid of addiction is that the consequences of using it are not obvious for him. The consequences do not come immediately, as in an adult who begins to seriously use: a teenager does not lose his job, does not remain without money, does not lose his circle of familiar acquaintances, his life does not collapse before his eyes. Did you get expelled from school/college? Think! The problem of lack of education will “shoot” in years, and now he has more time to use - there is no need to learn how to walk!
The consequences do not come immediately, as in an adult who begins to seriously use: a teenager does not lose his job, does not remain without money, does not lose his circle of familiar acquaintances, his life does not collapse before his eyes. Did you get expelled from school/college? Think! The problem of lack of education will “shoot” in years, and now he has more time to use - there is no need to learn how to walk!
Therefore, a psychologist usually builds work with a family where a teenager is addicted on interaction with a parent. But, since the family is a single system, along with a change in one of its elements, it is possible to achieve changes in the behavior of the dependent too.
The co-dependent parent habitually balances “helplessness/omnipotence” on the swing: from “Without me, my child will be lost!” (i.e., I am omnipotent and the life of another completely depends on me) the parent tumbles into “I can’t do anything with him!” (i.e., here he wants to use - and uses; and no matter how you control him, but finds ways, an infection).
The position of the “almighty” is offered to the psychologist as well: “You will cure him!”. When it turns out that the psychologist is not able to heal by the laying on of hands, the parent with anguish decides the usual: “He can’t do anything ...”. Awareness of one's own capabilities comes to a co-dependent parent very, very slowly. And in the course of a long and difficult work with a psychologist.
It's not sugar or honey for an addict either: on the one hand, you want to stop using it, but on the other, it's TERRIBLE. So you first need to establish contact and build a support system in difficult situations, so as not to look for oblivion and comfort in use, as a teenager is already used to.
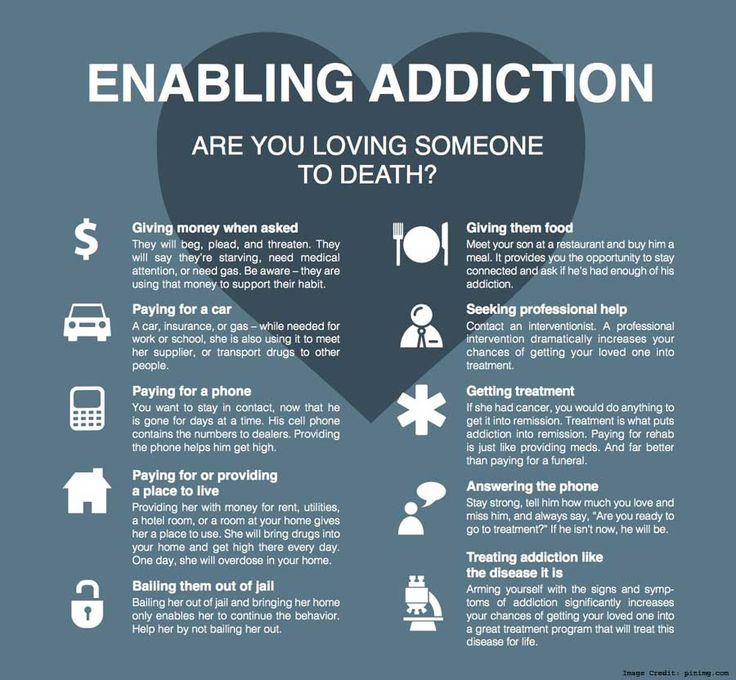
Well, meanwhile, the codependent parent is tormented by three fears:
- Fear of physical destruction and death (of himself or another): “He will be expelled from school if I don’t solve problems for him!” "He will die in the street if I don't help him," etc.
 Ironically, it is beneficial for the addict to be allowed to face the real problem that the addiction leads to. Well, they will kick you out, well, sleep on the street once - painfully, but not fatally. If the use does not lead to any real problems, and “mom will decide everything,” then why stop using? It's nice! And here, as the addiction worsens, the problems can become much more serious, by an order of magnitude!
Ironically, it is beneficial for the addict to be allowed to face the real problem that the addiction leads to. Well, they will kick you out, well, sleep on the street once - painfully, but not fatally. If the use does not lead to any real problems, and “mom will decide everything,” then why stop using? It's nice! And here, as the addiction worsens, the problems can become much more serious, by an order of magnitude! - Fear of destruction of relationships : codependent is afraid that the dependent child will be very offended and break off the relationship. (About the shame, guilt and fear of judgment by others that whip up a codependent adult, have I already mentioned? Well, so the excruciating horror of what they say: “Well, what kind of mother are you?” Makes an adult drag a successful teenager and endure much more of him than normal family relationships can handle).
- Fear of shame, condemnation . The codependent is terribly afraid of public condemnation.
 Shame and guilt are his Achilles heel. To hide the actual state of affairs both from oneself and from others - the co-dependent has learned masterfully. But the teenager's addiction progresses, and his antics become more and more serious, rude and outrageous. Hiding and covering up a child's actions is becoming increasingly difficult. A confrontation with shame is inevitable, and it will prove to be extremely painful. Yes, an adult codependent in this situation behaves in the worst way for himself - instead of admitting a problem and turning to others for help, a person hides it, tries to hide it, pretend that "everything is fine" - until absolutely everyone and it will not become clear to everyone that the situation is already completely abnormal.
Shame and guilt are his Achilles heel. To hide the actual state of affairs both from oneself and from others - the co-dependent has learned masterfully. But the teenager's addiction progresses, and his antics become more and more serious, rude and outrageous. Hiding and covering up a child's actions is becoming increasingly difficult. A confrontation with shame is inevitable, and it will prove to be extremely painful. Yes, an adult codependent in this situation behaves in the worst way for himself - instead of admitting a problem and turning to others for help, a person hides it, tries to hide it, pretend that "everything is fine" - until absolutely everyone and it will not become clear to everyone that the situation is already completely abnormal.
If you support an adult co-dependent and help him cope with his fears (to the heap - both with shame and guilt), then the prospects for healing the family become brighter.
Material taken from the site: http://detivokrug. ru/spetsialistam/150-vy-rabotaete-s-prijomnoj-semjoj-s-osobym-rebjonkom/sistema-raboty-s-semjej/590-zavisimyj-podrostok-i- sozavisimyj-parentel-osobennosti-vzaimodejstviya-v-pare
ru/spetsialistam/150-vy-rabotaete-s-prijomnoj-semjoj-s-osobym-rebjonkom/sistema-raboty-s-semjej/590-zavisimyj-podrostok-i- sozavisimyj-parentel-osobennosti-vzaimodejstviya-v-pare
How to protect a child from alcohol and drugs?
09/03/2018 Dependent behavior
Dependent behavior, to one degree or another, is the essence of human life.
And it doesn't have to be addiction to psychoactive substances. The same eating habits, musical preferences, choice of partners cannot do without elements of dependence.
The only question is when craving becomes pathological. By and large, dependent behavior is a kind of attempt to escape from reality, going into an altered mental state. The main thing is that it provides security (at least imaginary) and emotional comfort.
Dependency criteria:
• a person begins to ignore previously significant events for him;
• old relationships and connections break up, the immediate environment is replaced;
• misunderstanding or even hostility on the part of people significant to the dependent person;
• secrecy, irritability, sharply aggressive reaction to criticism;
• Feelings of guilt or anxiety about your addiction;
• unsuccessful attempts to get rid of an addiction to a psychoactive substance.
Start with yourself
It is known that neither alcoholism nor drug addiction is inherited. Only predisposition is transmitted. However, this fact must be taken into account. So, children from drinking families are 7 times more likely to develop alcoholism than those from families where they practically do not drink.
But even the presence of a predisposition does not mean at all that the disease will definitely develop: it all depends on the influence of the family and the social environment surrounding the child. The behavior of the expectant mother during pregnancy is of great importance. The use of any psychoactive substances in any doses negatively affects the child. This is a proven and indisputable fact.
What causes your children to become addicted to alcohol and drugs, and what to do about it.
The only question is whether these will be congenital deformities, a congenital disease, or changes in the biochemistry of the brain that will change the psyche of the unborn child. In heroin addicts, children are born with a formed drug addiction, and already 4 hours after birth, a real “withdrawal” can begin in a baby. But seemingly “harmless” smoking during pregnancy also affects the future behavior of children and their health.
In heroin addicts, children are born with a formed drug addiction, and already 4 hours after birth, a real “withdrawal” can begin in a baby. But seemingly “harmless” smoking during pregnancy also affects the future behavior of children and their health.
The risk of becoming a drug addict for a teenage girl is 5 times greater if her mother smoked more than 10 cigarettes a day during pregnancy. Among young men whose mothers smoked during pregnancy, bouts of inappropriate behavior are 4 times higher than among young men whose mothers did not smoke.
The mother's mental trauma, excessive stress during pregnancy, and even unwanted pregnancy increase the risk of developing addictive behavior in a child.
The behavior of the expectant mother during pregnancy is of great importance. Thus, the prevention of alcoholism and drug addiction in a child begins long before his birth and even conception.
Be an example
Psychologists have long noticed: in what mental state the mother is, the child is in such a state, especially under the age of 2 years. This is very important, because the child copies both the range of mental reactions and their intensity from their parents.
This is very important, because the child copies both the range of mental reactions and their intensity from their parents.
Suppose a mother is a kindergarten teacher and is accustomed to "high" speech, excessive gestures, exaggerated expressions of feelings, and sometimes to a commanding tone. In a child of such a mother, if she does not make a “correction for home”, with a high degree of probability, subtle tint emotions will practically not be formed, and the threshold of mental reactions will be artificially high. And in adolescence, he may well begin to compensate for these violations with cigarettes, alcohol or drugs.
If a mother is alienated from her child, the mother-child system may not form at all. And then the mental reactions of the child will develop with a lag, emotionally depleted. It will be difficult for him to build interpersonal relationships in the future, he withdraws into himself. And the teenager will also try to cope with these problems with the help of psychoactive substances.
At the same time, it is important to remember the balance of rewards and punishments in education. Thus, the child trains to experience troubles, albeit minor ones. Having grown up in an atmosphere of excessive "love", a person will not be able to "take a hit" and will look for a surrogate for that very atmosphere, including among drugs.
Pick up key
Kindergarten and school, where the processes of social adaptation of the child take place, are also a risk zone. The first class is especially difficult in this sense. For children who are used to perceiving the world through bodily sensations (touch, run, toss, turn in their hands, play), sitting still at a desk for 30-45 minutes is real torture.
They are actually deprived of the main channel for receiving information. Hence the difficulties in mastering the material, conflicts with the teacher and classmates. And after all, there are up to 30 percent of such children in the first grade. In another group of children, the degree of assimilation of the material depends on the impression it makes, on the intonations and emotions that the teacher “gave out” during the lesson.
In another group of children, the degree of assimilation of the material depends on the impression it makes, on the intonations and emotions that the teacher “gave out” during the lesson.
It is difficult for such students to perceive clearly systematized information (for example, mathematics), they consider it dry and boring. And they also experience "emotional starvation", but for a different reason.
Kindergarten and school, where the processes of social adaptation of the child take place, are also a risk zone. The first class is especially difficult in this sense. If a teenager strives to "be like everyone else", there is a high risk that he will try the drug.
What should parents do?
Do not discourage when children begin to try many circles and sections, without lingering for a long time in any of them. This is fine. Thus, they try on various types of activities, gain experience in getting pleasure, satisfaction from creativity or self-realization. The more such experience a child has, the less risk that he will seek surrogate pleasure in psychoactive substances.
The more such experience a child has, the less risk that he will seek surrogate pleasure in psychoactive substances.
Narcological dispensaries
The nearest drug dispensary that will help you get rid of addiction can be found in our database.
At school, from about 9–10 years old, a child’s group behavior is also formed. It is formed according to different principles - yard, interests, music, sports, etc. Sooner or later, a psychoactive substance may accidentally get into the group. And if a teenager strives to "be like everyone else", if the status in the group is above everything else for him, he will definitely try it.
Fortunately, groups rarely start trying heroin right away, most often it is psychostimulants or marijuana.
Do not keep the child in an information vacuum - he will fill it in from other sources. And it is not a fact that they will be reliable and adequate.
Inform
The child should learn about drugs from you. Although a teenager can be much more impressed by a conversation with a relative closer in age - an older sibling or cousin, your sisters or brothers.
Although a teenager can be much more impressed by a conversation with a relative closer in age - an older sibling or cousin, your sisters or brothers.
Explain that "soft" drugs do not exist, they are just a "jump airfield" for switching to more "heavy" ones. That the mental dependence that develops when smoking marijuana "does not let go" in the same way as the physical dependence on alcohol. And that sometimes just one shot of heroin is enough to form a lifelong and persistent drug addiction.
Show him anti-drug websites, let him read real stories of drug addicts, look at photos of possible consequences. A great impression on teenagers is usually made by Darren Aranofsky's feature film Requiem for a Dream, and there are enough documentaries on this topic.
Parental commandments
1. Do not try to make a copy of your child, he will be himself, even if you actively oppose this.
2. Do not demand gratitude from the child only for the fact that you gave him life. In due time, he will give life to your grandchildren and by this he will repay his debt with a vengeance.
In due time, he will give life to your grandchildren and by this he will repay his debt with a vengeance.
3. Do not take out your anger and resentment on your child for failures in work or personal life. All the evil that you poured out on the child will return to you, often in a hypertrophied form.
4. Take your child's problems seriously, even if they seem funny to you. He has less life experience, help him, share your knowledge.
5. Never humiliate a child. Remember that he is the same person as everyone else, he also has self-esteem.
6. Love a child just for the sake of it, and not because he is talented, handsome or smart.
7. Never do to someone else's child what you would not do to your own.
You can get information on any questions related to the use of alcohol by calling the Healthy Russia telephone information service. The hotline operates at 8-800-200-0-200. Calls to it are free from all regions of Russia.