How much pain in giving birth
Worried about the pain of labor and delivery? It’s not as bad as you think!
CHICAGO – Few things are more daunting for first-time moms than the prospect of childbirth. They wonder: Will my baby be OK? What will labor and delivery be like? How painful will it be, and can I handle it? Moms who have been there offer the low-down on labor and delivery and their message is comforting. Yes, childbirth is painful. But it’s manageable. In fact, nearly half of first-time moms (46 percent) said the pain they experienced with their first child was better than they expected, according to a nationwide survey commissioned by the American Society of Anesthesiologists (ASA) in honor of Mother’s Day.
The survey findings suggest that being proactive in managing pain with your physician anesthesiologist is important, whether laboring moms demand an epidural right away, choose other medical pain management methods, use complementary techniques only or opt for a combination. Nine out of 10 women said pain management was effective, no matter what method they chose. (Click here to download infographic)
But the survey also revealed that many first-time moms held some false beliefs about labor pain management before they experienced childbirth:
• 74 percent thought you couldn’t have an epidural after a certain time in labor (you can have one up until the baby’s head begins emerging, known as crowning)
• 44 percent feared pain at the epidural injection site would last for a prolonged time
• 26 percent believed an epidural slows labor
• Most concerning, 20 percent believed only one pain management option could be provided during labor and 16 percent thought about it but didn’t know
Expectant mothers should work with their health care providers, including their physician anesthesiologist, to discuss what pain management methods may work best for them. They should talk to their physicians to find out who will administer their anesthesia if they decide to have pain medication during labor. Anesthesia care should be led by a physician anesthesiologist, a medical doctor specializing in anesthesia, pain and critical care medicine, who will work with all of the mother’s physicians to develop and administer her pain management plan.
Anesthesia care should be led by a physician anesthesiologist, a medical doctor specializing in anesthesia, pain and critical care medicine, who will work with all of the mother’s physicians to develop and administer her pain management plan.
“First-time mothers need to know that a wide variety of options exist to manage pain, from epidural to massage, nitrous oxide to breathing techniques and that it’s acceptable to change methods or use a combination during nearly every stage of labor,” said ASA President James D. Grant, M.D., M.B.A., FASA. “But it’s also important to be flexible, since it may be necessary to change pain management methods based on the labor process itself.”
When it hurt most and what it was like
While slightly more than half said having contractions was the most painful aspect of delivery, about one in five noted pushing or post-delivery was most painful. Moms 18 to 39 were more likely to say post-delivery pain was the most painful aspect than those 40 and older. The most common description of the level of pain experienced was extreme menstrual cramps (45 percent), while 16 percent said it was like bad back pain and 15 percent compared it to a broken bone.
The most common description of the level of pain experienced was extreme menstrual cramps (45 percent), while 16 percent said it was like bad back pain and 15 percent compared it to a broken bone.
Health and safety are top of mind
It’s no surprise that when choosing a pain relief option, nearly all mothers (99 percent) said the health and safety of themselves and the baby was an important factor in their decision. Not far behind was making sure the pain relief option didn’t delay the labor process (86 percent) as well as being able to enjoy the labor and delivery experience (84 percent). But the importance of other factors diverged depending on the pain method chosen. Having no pain during labor was very or somewhat important to women who chose medical methods (epidural, medication delivered through an IV or injection, spinal block or nitrous oxide) only (79 percent) compared to women who opted for complementary methods (breathing, water birth, massage, visualization or hypnosis) only (37 percent).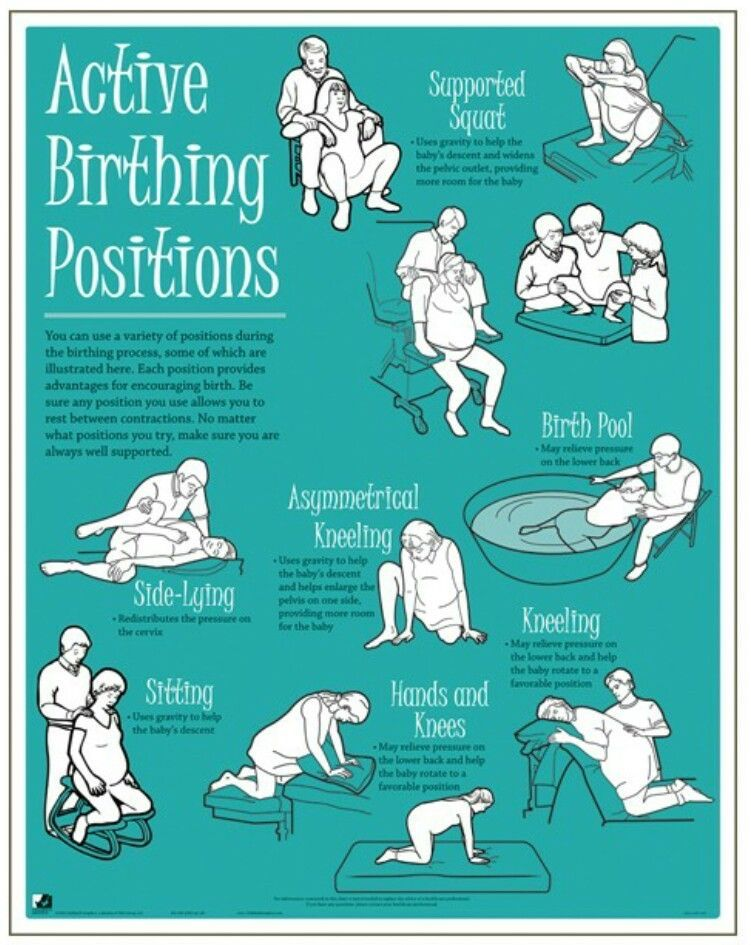 Being able to move around during labor was important to 90 percent of moms who only had complementary methods, while just 60 percent of moms who had medical methods only agreed.
Being able to move around during labor was important to 90 percent of moms who only had complementary methods, while just 60 percent of moms who had medical methods only agreed.
So, what pain management did they choose?
While the epidural reigned supreme as the most common option, chosen by 73 percent, 40 percent of women used complementary methods. Additionally, pain management during labor and delivery may not be “one size fits all,” with 31 percent having used both medical and complementary methods. More than half used medical methods only and 9 percent chose complementary methods only. Sixty-five percent of women who had medical options only said they were very effective in managing pain, while 39 percent who had complementary methods only said they were very effective.
And while nitrous oxide has received a lot of attention recently, the survey results suggest it’s rarely used. Only 2 percent of moms had nitrous oxide, and none 40 and older or who lived in the Midwest used it to manage labor pain. Before childbirth, slightly more than 1 in 10 thought nitrous oxide relieved pain and 63 percent didn’t think about it at all. “This suggests that despite the buzz, nitrous oxide may not be widely available yet, or that mothers aren’t convinced it would be very helpful,” said Dr. Grant.
Before childbirth, slightly more than 1 in 10 thought nitrous oxide relieved pain and 63 percent didn’t think about it at all. “This suggests that despite the buzz, nitrous oxide may not be widely available yet, or that mothers aren’t convinced it would be very helpful,” said Dr. Grant.
In the future
If they were to give birth again, most moms would choose the pain management method, whether medical and/or complementary, they originally chose during their first childbirth, with the majority (60 percent) opting again for an epidural to manage their pain.
Women were split on the pain management advice they would give to first-time prospective moms – 21 percent would recommend getting an epidural as fast as possible, while 20 percent say try complementary methods first and if they don’t work, try other options. However, 43 percent of mothers agree that choosing one’s pain management method is a personal decision and you need to opt for those that work best for you.
“Every woman’s pain during labor is different and talking with your health care provider and physician anesthesiologist can help you decide which pain management method will give you the best labor and delivery experience,” said Dr. Grant. “Women may choose to use none, some or more than one pain management method depending on how labor progresses."
The 10-question ORC International CARAVAN® Omnibus Survey was conducted online April 3-11 among 912 mothers (18 years or older) of children ages 0-8, whose first child was born either via vaginal childbirth or Cesarean section (C-section) after the onset of labor. Ultimately, 73 percent had a vaginal childbirth.
For more information about pain management during labor and delivery and the importance of seeing a physician anesthesiologist, visit asahq.org/labor.
The American Society of Anesthesiologists
Founded in 1905, the American Society of Anesthesiologists (ASA) is an educational, research and scientific society with more than 52,000 members organized to raise and maintain the standards of the medical practice of anesthesiology. ASA is committed to ensuring that physician anesthesiologists evaluate and supervise the medical care of patients before, during, and after surgery to provide the highest quality and safest care that every patient deserves.
ASA is committed to ensuring that physician anesthesiologists evaluate and supervise the medical care of patients before, during, and after surgery to provide the highest quality and safest care that every patient deserves.
For more information on the field of anesthesiology, visit the American Society of Anesthesiologists online at asahq.org. To learn more about the role physician anesthesiologists play in ensuring patient safety, visit asahq.org/WhenSecondsCount. Like ASA on Facebook; follow ASALifeline on Twitter.
# # #
How Painful Is Childbirth, Really?
Moaning, screaming, and cursing. These are some of the pleasant sounds commonly associated with childbirth.
You’ve likely seen birth graphically depicted on television, or if you’re pregnant, all of your family and friends may have decided to share their harrowing birth stories with you. If you’re like most women, this has led to a lot of fear about the amount of pain you’ll face during labor.
Is this really the truth about birth though? How much pain will you actually experience? Can you do anything to diminish that pain? While birth is different for everyone, we’ve got the information, tips, and tricks to help you feel prepared for the pain of childbirth.
Every person’s experience with birth will be different. Pain is subjective and can vary greatly. This means that you may have a very different pain experience from even your mother or sister.
It’s important to remember that the pain of childbirth is a manageable one, and both medicated and more holistic pain relief measures like visualization and massage are available.
Despite what you may have seen on YouTube or elsewhere, there’s no reliable unit to measure pain. Back in the 1940s, researchers tried to employ a device known as the dolorimeter, which used the heat from a light source, to establish levels of pain.
However, this measurement fell out of favor with growing evidence that pain isn’t solely dependent on an isolated physical sensation. Rather, it’s affected by a person’s fears, mood, memories, and personality, as well as factors like the duration and overall experience of the pain source.
Rather, it’s affected by a person’s fears, mood, memories, and personality, as well as factors like the duration and overall experience of the pain source.
Your healthcare provider will likely ask you to track and quantify your pain by rating it on a scale. They may discuss the intensity of the pain and your feelings about your ability to work through or manage it. This information will help them determine the appropriate pain relief options with you.
Pain is not necessarily consistent during the labor process, and you’ll probably experience breaks from it between contractions or while pushing. Although, you may notice though that it increases after your water breaks or as labor picks up, and that some elements of the pain are temporary while others continue for a period of time after giving birth.
When you think about the pain of childbirth, just remember that it’s purposeful, anticipated, intermittent, and a necessary part of your baby coming into this world!
You can expect to experience a variety of sensations during the end of your pregnancy and labor.
During pregnancy, you may experience Braxton-Hicks contractions, which are usually irregular and inconsistent. They tend to be felt in the abdominal area and make the belly feel tight, causing discomfort more than pain.
One thing that sets these contractions apart from labor contractions is that they don’t become more consistent, stronger, and longer. (If you would like to reduce the discomfort of Braxton Hicks, you can try drinking some more water, changing position, or resting on your left side.)
Early labor
In the early stages of labor, contractions will increase in intensity and frequency as they fall into a steady pattern.
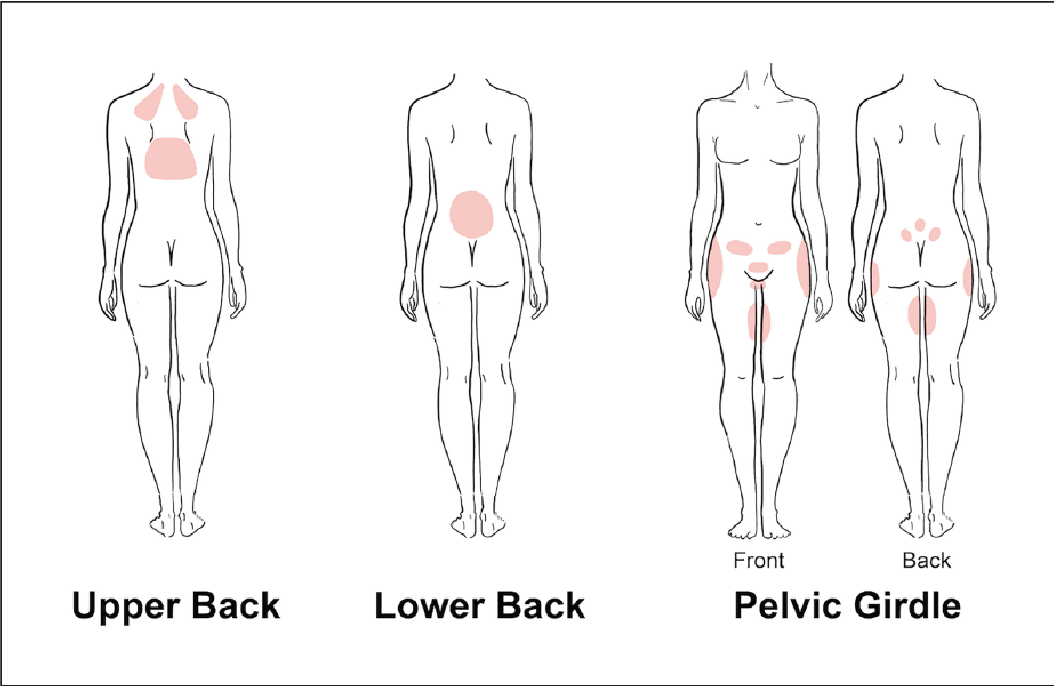
Early labor contractions will usually cause the abdomen to feel tight to the touch. You may also experience a dull backache, feelings of pressure in the abdomen and pelvis, and sensations similar to those of intense menstrual cramping.
When contractions begin, they may only be 30 to 45 seconds in length with several minutes of rest in between.
Active labor
As labor progresses, contractions may feel like they are wrapping around your body from the back to the front. You may also begin to notice cramping and discomfort in your legs as the contractions become more frequent and last closer to 1 minute in length.
When you’re approximately 8 centimeters dilated, you may have 30 seconds to 1 to 2 minutes between contractions as you prepare to enter the pushing stage of labor. During this time it’s not uncommon to feel lightheaded, nauseous, and have hot flashes or chills.
Pushing
When you are fully dilated (around 10 cm) and it’s time to push, you may feel an intense pressure that feels like you need to poop. You can relax a little knowing that your body is just telling you that it’s ready for you to help push out your baby.
During this period, you’ll typically be instructed to push with the peaks of your contractions. Because you’re pushing with the contractions, many women find these contractions less painful than the contractions helping them to dilate.
Other parts of the experience may also cause discomfort or pain, including an episiotomy or vaginal tearing. You may also feel muscle pain or fatigue from pushing or experience uncomfortable side effects from medications used during labor.
If you’re feeling nervous about giving birth, there are things you can do before and during labor to decrease your pain (and increase your chance of having a positive birthing experience!).
Before giving birth
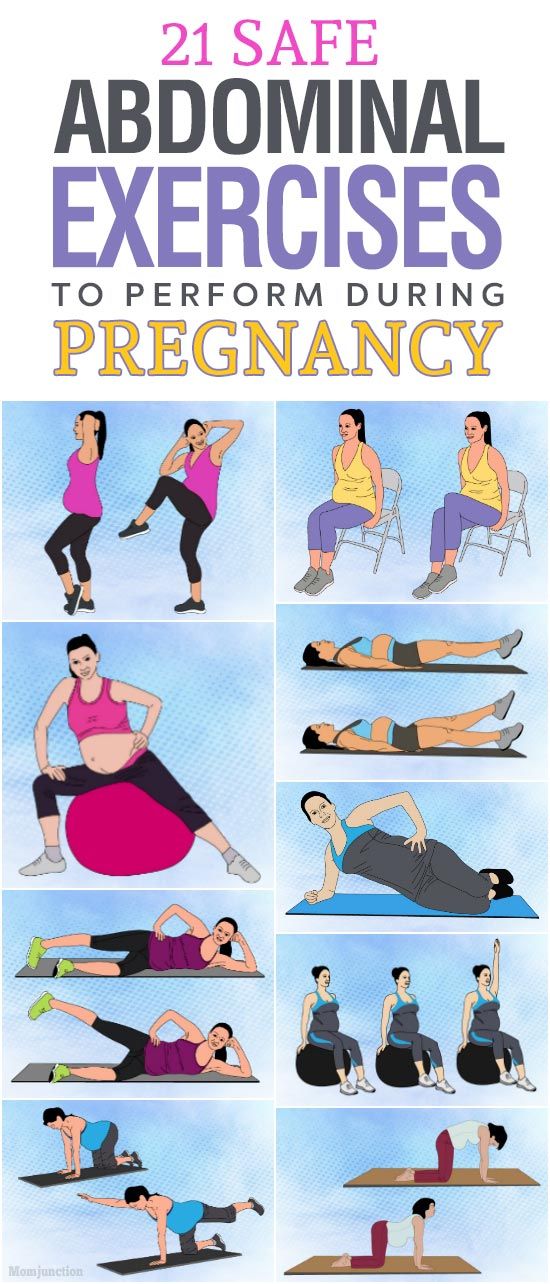
Exercise frequently
While you may need to modify your normal exercise plan, it’s worth continuing to exercise during pregnancy. Regular exercise during pregnancy not only helps control your blood pressure, mood, and weight but also can help keep your body in shape for the work of labor.
Take a birth preparation class
Knowing what’s ahead can help you relax and feel more comfortable during labor. Most birth preparation classes include instruction on comfort measures during labor, so you and your partner can get ideas and practice before the big event.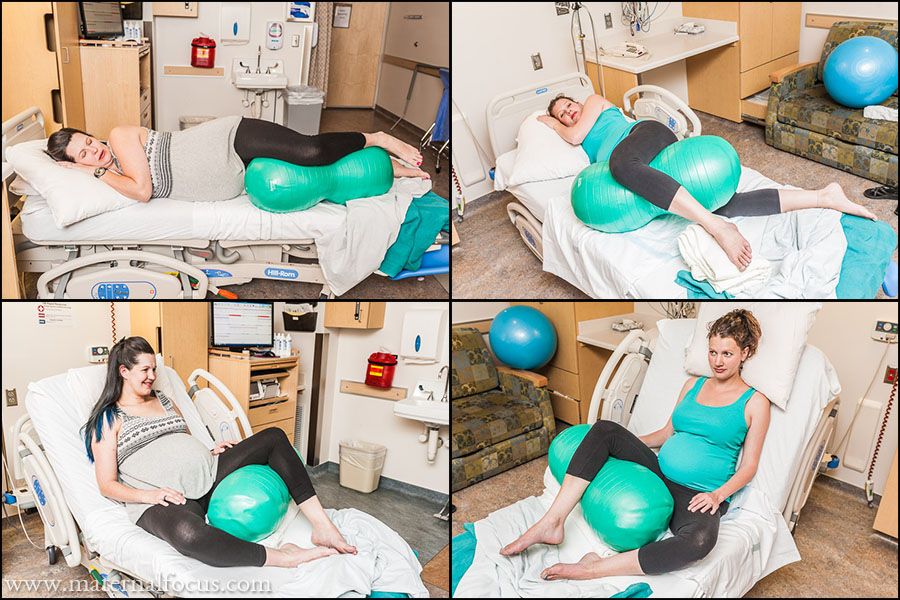 (While you’re at it, you may also want to sign up for a baby care or breastfeeding class!)
(While you’re at it, you may also want to sign up for a baby care or breastfeeding class!)
Eat well and take your prenatal vitamins
It’s important to put the right nutrients in your body to help your baby grow properly and give yourself energy for labor.
Consider optimal fetal positioning
It’s easier to birth your baby when they’re in an optimal position. If your baby is breech or transverse, you may want to consider actions that will encourage them to shift their position… before you go into labor!
During labor
Pain relief during labor is a personal choice. You can try any combination of the following methods.
Breathing techniques
Whether you choose to follow a particular breathing routine during labor or just need to do some low vocalizations to help you through the more intense contractions, focusing on your breathing can help you manage the pain.
Water
Even if you don’t want to give birth in water, spending some time in a shower or bath can help relieve the pain of childbirth.![]()
Being in water has been found to be particularly effective in the first stage of labor. It can help relieve both pain and anxiety. If you have access to a moveable showerhead, aiming warm water directly onto the lower back may feel especially pleasant.
Massage and counterpressure
Many different types of massage can help manage pain during labor. Foot, hand, back, and shoulder rubs may all appeal to you. One study from 2010 found that a 15-minute massage each hour during labor helped alleviate pain and was even associated with shorter labor.
Additionally, perineal massage can help protect and prepare the perineum for the stretching involved in birthing a baby.
In addition to massage, many women enjoy pressure being strategically placed on parts of their body to help counteract the discomforts they may be feeling.
Music
Music can lower stress and blood pressure. It can also improve your mood! But can it really help with pain during labor? Yes — a large meta-analysis found that music interventions helped alleviate pain and anxiety during labor.
Visualization or hypnosis
Guided imagery, hypnotic tracks, and other visuals can all help relax a mother in labor and relieve pain.
Movement
Walking, rocking on a birthing ball, or even slow dancing with your partner can help labor progress and relieve some of the discomforts you may be feeling.
Experimenting with different positions, including sitting, standing, or squatting, may also help reduce pain. One study found squatting offered the most pain reduction, but you can experiment with what feels best for you.
A doula
Research shows that having a doula present at your birth can lead to a better birth outcome. A doula can help with positioning/counterpressure, offer suggestions for comfort measures, advocate for your choices, and help answer your questions throughout the laboring process.
Not sure where to find a doula? Start here.
A TENS unit
Many people have found some pain relief during labor by stimulating their lower back with a transcutaneous electrical nerve stimulation (TENS) unit.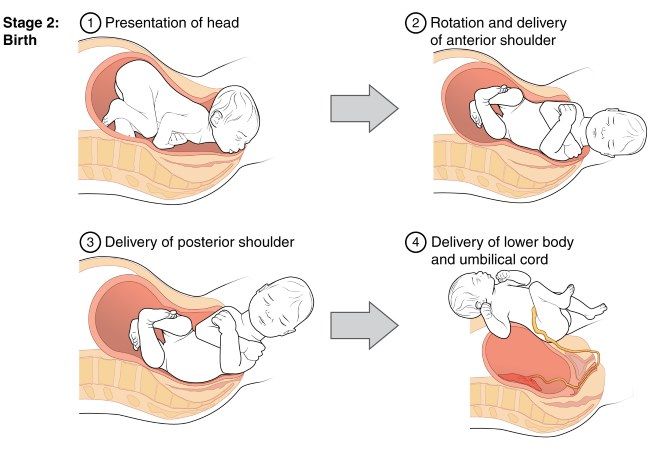 (Some hospitals even have TENS devices that you can borrow during labor!)
(Some hospitals even have TENS devices that you can borrow during labor!)
Aromatherapy
If you’re feeling nauseous or anxious, peppermint, lavender, or some citrus essential oils may provide some relief during labor.
IV narcotics
Intravenous (IV) narcotics offer some of the pain relief of an epidural for a more limited time. As in the case of an epidural, nausea, headaches, drowsiness, and the transmission of medication to the baby are potential risks.
For a woman seeking a brief reprieve from the intensity of birth, an IV narcotic can be a very appealing pain relief option.
Nitrous oxide
While you may have seen it during dental visits, in the United States nitrous oxide is less commonly used as a pain relief option during childbirth. It’s a fast-acting option for pain and anxiety relief that doesn’t stay in the system as long as narcotics.
Nitrous oxide has been used for over a century and is generally considered safe for the mother and baby. While it’s used regularly in some locations around the world, you’ll need to check with your provider as to whether it’s available where you’re delivering.
While it’s used regularly in some locations around the world, you’ll need to check with your provider as to whether it’s available where you’re delivering.
Epidural
The most common pain medication for birthing mothers in the United States, an epidural can relieve the pain a mother is feeling within 10 to 20 minutes. Most hospitals provide epidural analgesia, and if your pain is beyond a manageble level, you can request one.
The vast majority of women who receive an epidural feel pressure and not pain from that point on in their labor. (Many women can even sleep while laboring once the epidural has been placed.)
There’s some risk that an epidural will result in a specific type of headache, pushing may be more difficult, your lower half may remain numb for a period of time after giving birth, or you may react to the medication used in the epidural. Still, many women find that the pain relief an epidural offers outweighs these risks.
There’s no way to know exactly what childbirth will be like for you. Even if you have given birth before, each experience is different. Taking steps to prepare beforehand and using comfort measures during labor can reduce the pain of childbirth.
There’s no reason to be fearful about giving birth. While it’s called labor for a reason, millions of babies are born each year. You’re not alone! Your care provider can work with you to ensure that you have the medication and holistic pain reduction measures you need to handle your contractions.
Labor Pain: You can handle it!
For many expectant mothers, the pain that may be in childbirth is a real "sore topic". Wander from mouth to mouth "horror stories" of grandmothers and girlfriends. Meanwhile, these sensations are fundamentally different from pain during injuries, diseases and other unpleasant incidents. It is not enough to say that childbirth is a pleasant event, it is a holiday, it is a sacrament. And contractions and attempts are the way to the holiday. Just to make the holiday a success - you have to work hard. "Work", "work" is the period of contractions in English and French. Thinking of them as a difficult path to the joy of meeting a baby is the first step to not hurting. And the joyful acceptance of contractions is almost one hundred percent painkiller. But this is already a feat of maternal love. nine0003
Childbirth is not painful or scary,
because there are many simple and natural pain relief methods. In our age, many means have been invented to facilitate any work, in any way. And in such a primordial human business as obstetrics, there are dozens of such methods, both ancient and modern.
Remember that there will be no task beyond your strength! There will be a job that suits you.
All people are different - and from everything that will be described here, you will definitely choose something of your own. You should think, try and take with you on the road what is useful for you. We will only make a reservation that only natural childbirth can be effectively anesthetized by natural methods, that is, those that are not "caused" artificially and go without medical interventions. Then, believe me, looking back immediately after giving birth, you will say: it was wonderful! But when will I give birth next time ...
Relaxation
The more relaxed you are during the contraction, the easier it will be for you to “work through” it, the better the cervix will open, releasing the baby. And this is the meaning of your work. Actually, your body will do the work, you just need to help yourself and your baby in the right way ... Everyone has their own way to relax: focusing on a visual or auditory image, breathing, posture, sound.
Concentration
From practice it is known that focusing on something helps to relax during a fight. You must choose for yourself individually what will be close to you. Some prefer to focus on what is happening inside: they imagine how the cervix opens, how the baby's head moves forward. nine0003
Visual images are closer to others: they imagine themselves in some beautiful and pleasant place (on the seashore, in the mountains) or imagine a fight in the form of an obstacle that must be overcome (for example, in the form of a big wave). Sometimes it is convenient for a woman to focus her eyes on a certain object or follow a line with her eyes in the course of a fight.
There are people who find it easier to focus on a sound, whether produced by themselves or heard from outside. It can be music, the voice of a husband or a midwife, the sound of the sea or rain. Sometimes it's easier to focus on the tactile sensation: massages, firm pressure, and even hugs can help distract and relax. You can focus on a short prayer, verse, phrase, as well as on a certain rhythmic movement - which is closer to whom. nine0003
Breathing and sound
Instinctively holding one's breath and straining is a natural human response to a disturbing stimulus. We will do the opposite - breathe evenly and calmly. And surprisingly, the irritant will bother us less!
- Long exhalation. A deep, calm breath in through the nose and a long, calm (not forced!) exhalation through the mouth. To make the exhalation longer, you can fold your “lips into a tube”, as if blowing on a flame.
- Intermittent exhalation. A deep, calm breath in and a long, interrupted exhalation that sounds like "poo-poo-poo-poo ...". nine0030
- "Engine". You shortly inhale and exhale, while the sounds are similar to how a steam locomotive puffs.
- "Dog breath". Frequent short breathing: this is how a dog breathes in the heat. This breathing helps to prevent pushing too early or to hold it back (preventing ruptures).
Sounds. It is much easier for many to “sound” in a fight than to remain silent. This is by no means a cry, but lingering sounds of different heights on the exhalation. From the outside it looks like a primitive song. You need to choose the height of the sound for yourself individually. nine0003
Movement and various postures
Movement. Usually, immobility and the supine position are the least comfortable during contractions. Hence the main advice: find your posture and move! In addition to anesthesia, the movement contributes to the correct insertion of the baby's head at the exit from the small pelvis. Between contractions, you can walk around, and if the contractions are weak and rare, then you need to walk quite quickly - this gives mild stimulation. Movements resembling the rotation of a hoop around the waist or an oriental dance work wonderfully. nine0003
The following positions are good during contractions:
- Standing posture, leaning forward. This position is very convenient if you walk during contractions. You stop where the fight caught you and, leaning on a table or wall, "work through" the fight.
- "Pose of a cat" or position on all fours. Remember how old Hank carried the Chief of the Redskins on his back when they played Indians. The pose is convenient in the active phase of contractions, when it is no longer possible to walk. nine0029 "Child's Pose" is similar to the previous one, the difference is that the arms are bent at the elbows and the head is low. Your baby is in the same position in the womb. Pillows can be placed on the sides for comfort.
- Side lying position. Also good for contractions and relaxation. For convenience, the upper leg, bent at the knee, can be placed on a large pillow.
- Hanging position. Sometimes, during contractions, it is comfortable for mommy to hang: on the sports complex or in a squatting position, leaning on her husband supporting her from behind. The meaning of the hanging position is to relax the lower body, which softens the sensations. In addition, the force of gravity helps the child move from the inside out. nine0030
Stroking, massage, pressure
Most women enjoy being touched during contractions. The sacrum is the area where the nerves leading to the uterus come from. If you look closely at the lower back, you will see a rhombus, which is formed by the muscles of the back and buttocks. Often, stroking from top to bottom, or vigorous rubbing at points on the sides of the rhombus, significantly changes the sensations. For some, just applying firm pressure to the area helps. A woman can do a massage with her own hands only at the initial stage of childbirth, in the future it sometimes has to be done by her husband or someone who helps in childbirth. nine0003
Heat and cold
- Hot compress. Try to apply a hot compress from a towel folded several times to the sacrum area during a contraction. You can add a few drops of lavender essential oil to the water.
- Heating pad. This is dry heat on the sacrum. Very convenient electric heating pad with adjustable heat. Sometimes a mother is pleased when heat is applied not to the sacrum, but to the stomach, groin or perineum.
- Ice. All people are different: in rare cases, not heat, but ice should be applied to the sacrum (sliced frozen vegetables usually act as ice - they easily take the shape of the body). However, at the same time, the mother as a whole should be warm. nine0030
Water
Water has a wonderful analgesic and relaxing effect.
- Warm shower. Once you are comfortable and relaxed, direct the shower jet to where you feel most comfortable. The shower gives local warmth and light massage.
- Pool. Contractions are greatly facilitated by immersion in water. It is enough just to sit comfortably in the pool or bath, relaxing well. If the contractions are very strong - some mothers dive under the water and find that this is an excellent pain reliever. If you add 5-6 drops of verbena essential oil diluted in milk or yogurt to the water, the analgesic effect will increase, and the air around the mother will be filled with a delicate and wonderful aroma (be careful if the mother is prone to allergies!). nine0030
Aromatic oils
Verbena and lavender oils have already been mentioned above, which are used for water procedures. They also work great as a relaxing and analgesic, if you rub a drop in your palms and inhale the vapors, as well as if you use an aroma lamp. Allergy sufferers should test with a very small amount of oil and observe their reaction.
Homeopathy
This is the science that says that the symptoms are the language of the human body, in which he speaks what specific remedy he needs in a given situation. Therefore, according to a vivid picture of symptoms, even a person who is superficially familiar with homeopathy can successfully prescribe a harmless and very effective medicine. Here are the "pictures" (look closely!). nine0003
- Caulophyllum 30. Sharply painful contractions that occur in the lower abdomen. Despite this, the midwife or doctor says that the cervix does not dilate. Mom feels tired, trembling, thirsty.
- Cimicifuga 30. Also, during contractions, sharply painful sensations in the lower part of the abdomen, they "jump" from place to place. He talks a lot and rather randomly, "jumps". Mom is full of fears and forebodings (in fact, often such women have a difficult past experience of pregnancy and childbirth, failures in married life). Her deepest feeling is "I can't!". nine0030
- Gelsemin 30.
Feeling of trembling and tiredness, eyes literally closing. Trembling in the fight. The cervix does not open. Internal tension, bad forebodings.
- Coffea 30. Contractions seem unbearable. Sharp emotional arousal, as if drinking coffee.
- Hamomilla 30. Contractions seem unbearable. Extremely sensitive and misbehaving. Screaming, cursing and bickering. Sensation of heat, flushed face. nine0029 Pulsatilla 30. The main indications for this remedy are tearfulness, self-doubt, need for comfort and support. Does not tolerate stuffiness. The contractions are sluggish and weak in this remedy. Its use will avoid harsh drug stimulation leading to painful contractions.
- Arnika 30. Mom doesn't want to be touched: she claims that she's all right and sends everyone away. Feeling of muscle weakness and soreness. In childbirth relieves fatigue, prevents bleeding. After childbirth - accelerates recovery. nine0030
These drugs are freely sold in homeopathic pharmacies.
How to use the medicine: Take 3 grains and observe your reaction. If there are changes for the better, it is not necessary to repeat the reception while the improvement lasts. Take again if symptoms return. Choose another medicine if there is no effect. It is reasonable to visit a homeopathic doctor at the end of pregnancy, who, after talking with you individually, will select such medicines for childbirth that will be useful for you, and will also prescribe prophylactic agents to make childbirth easier. nine0003
Listen to your body
Take it on faith: you know how to give birth (this has been encoded in the genes of every cell of your body since ancient times) and you know exactly what you and your baby need to make childbirth easier and better. You just need to understand your own body language. The famous Canadian midwife Gloria Lemay finds it useful to look at childbirth as a excretory process, like other excretory processes: coughing, stool, crying. “They don’t need a mind - they require a different state. Each person is able to carry out his excretory processes without special instructions from his neighbors ...,” she writes.
But all people are different. Many give birth on their own, many need help (even in finding themselves). If you are not one of those who know with their inner instinct what to do, take courses for expectant mothers. If you are not one of those who finds the strength to give birth completely on their own, find good helpers.
Traditional midwives know many other ways to make childbirth easier. Moreover, experience allows them to see what is best for you. Find such assistants who, having all the necessary professional knowledge and experience, would have the wisdom to respect your opinion, follow the nature of your body and not interfere with natural processes unless absolutely necessary. nine0003
Veronika Maslova, family doctor, homeopath
Why the memory of the pain experienced does not leave us
- Claudia Hammond
- BBC Future
9000
Sign up for our Satter ”: it will help you to find out the context” in events.
Image copyright Thinkstock
If people weren't able to forget the pain they once experienced, women would never decide to have a second child. At least that's what the popular myth says. However, in reality, as the correspondent found out BBC Future , painful memories don't always fade.
Talk to any woman who has just had a baby and she will almost certainly say, describing the pain of childbirth, "Again? Never in my life!" A friend of mine begged me to dissuade her from such a step if she even hinted at a second child in the future. And what? It's only been a few years, and here you are: it's time for her to give birth...
The usual explanation is that women simply forget the pain they experienced during childbirth, as the brain edits memories. From an evolutionary point of view, it would be wise to forget the pain of childbearing if the memory of it would restrain the desire of people to reproduce. Unfortunately, things are not so simple. nine0003
Unfortunately, things are not so simple. nine0003
With regard to childbirth in particular, a review of studies conducted up to 2000 suggests that women do not completely forget the pain of labor pains, as well as the intensity of the pain they had to experience. However, this is a difficult topic to study. There is a scale that allows people to assess the severity of pain, but since labor can last for many hours, it is not very clear at what stage of contractions or labor itself the study participants concentrated their attention. Even the pain of each uterine contraction can vary in severity, so assessing the pain experienced during the entire process is unlikely to ever be an easy task. nine0003
(Similar articles in the "Journal" section)
However, there are still some things that can be done, such as examining whether a particular woman's memories of pain have changed over time. Swedish experts conducted a survey of 2428 women and compared their memories of pain experienced two months and one year after childbirth.
The data obtained showed that most women do not forget their feelings: memories of the experience of childbirth in 60% of women remained the same, both after two and after 12 months. In fact, only a third of mothers at 12 months had forgotten how painful it was for them to remember childbirth two months after birth. With 18% of the women surveyed, something exactly the opposite happened - they not only did not forget the intensity of the pain experienced, but, on the contrary, in their memory, childbirth became more painful 12 months later. nine0003
Rewrite the past
Skip the Podcast and continue reading.
Podcast
What was that?
We quickly, simply and clearly explain what happened, why it's important and what's next.
episodes
The End of the Story Podcast
Five years have passed and the scientists again polled the same group of women. By this time, indeed, the memory of pain in some of them had become dull. About half said the pain was less severe than they thought two months after giving birth. However, those who most negatively assessed the experienced experience of childbirth two months after the event, memories of pain did not leave. However, this is not necessarily a bad thing. In the course of some studies, it turned out that women who remember the pain experienced during childbirth perceive this event as their own achievement that remains with them forever. "If I can handle the pain during contractions, I can handle anything." nine0003
By this time, indeed, the memory of pain in some of them had become dull. About half said the pain was less severe than they thought two months after giving birth. However, those who most negatively assessed the experienced experience of childbirth two months after the event, memories of pain did not leave. However, this is not necessarily a bad thing. In the course of some studies, it turned out that women who remember the pain experienced during childbirth perceive this event as their own achievement that remains with them forever. "If I can handle the pain during contractions, I can handle anything." nine0003
At the same time, the very fact that the memory of pain does not change over time can be surprising. As the results of several decades of psychological research show, whenever we remember something, we reconstruct the events of the past in a slightly different way.
Image copyright, Thinkstock
Image caption,The pain a woman experiences during childbirth is hard to measure
Our memory is not a collection of digital discs of videotape that will play back the events of the past every time we see them exactly as they were in reality. Instead, the context of the original memory is changed. We talk about this or that event, each time reproducing it from memory in a slightly different way than before. nine0003
Instead, the context of the original memory is changed. We talk about this or that event, each time reproducing it from memory in a slightly different way than before. nine0003
Pain during childbirth has a purpose. If the birth went well, this positive outcome in itself should dull the memory of suffering. But something else is also clear: for some mothers, even the happy event of having a baby does not alleviate the painful memories of the childbearing process.
So, if the intensity of this kind of "positive" pain is not necessarily forgotten, how about negative experiences?
Sometimes it is important that we experience pain and remember what caused it. Such a memory ensures our safety and avoids the repetition of painful troubles. If you cut yourself painfully while opening a tin, you'll be more careful the next time you cook dinner. Or if, like me, you decide to test whether the metal rim around the hearth really gets very hot, and touch it with four fingers, you probably won't repeat this experiment.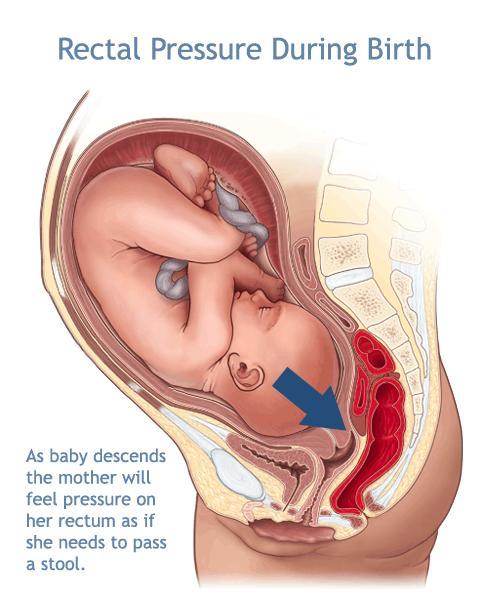 Alas, I was 30 years old, not five. Not surprisingly, people who suffer from disorders that prevent them from feeling pain often get burned or otherwise injure themselves. So forget about the pain is not necessary. nine0003
Alas, I was 30 years old, not five. Not surprisingly, people who suffer from disorders that prevent them from feeling pain often get burned or otherwise injure themselves. So forget about the pain is not necessary. nine0003
Forgetting about pain is sometimes useful, although chronic pain is often associated with diseases such as diabetes. The key to regulating this kind of pain and getting rid of it at the molecular level is provided by some new discoveries.
Even when you just walk through the gate where you once cut your leg, or open the door where you once pinched your finger, you will close your eyes at the memory of these incidents. In 2006, researchers at the Arizona State University College of Medicine made the claim that this was due to the function of the PKM-zeta (PKM-ζ) molecule. This molecule (also called the memory molecule in the popular science literature) strengthens the connections between neurons in the brain when we learn something new.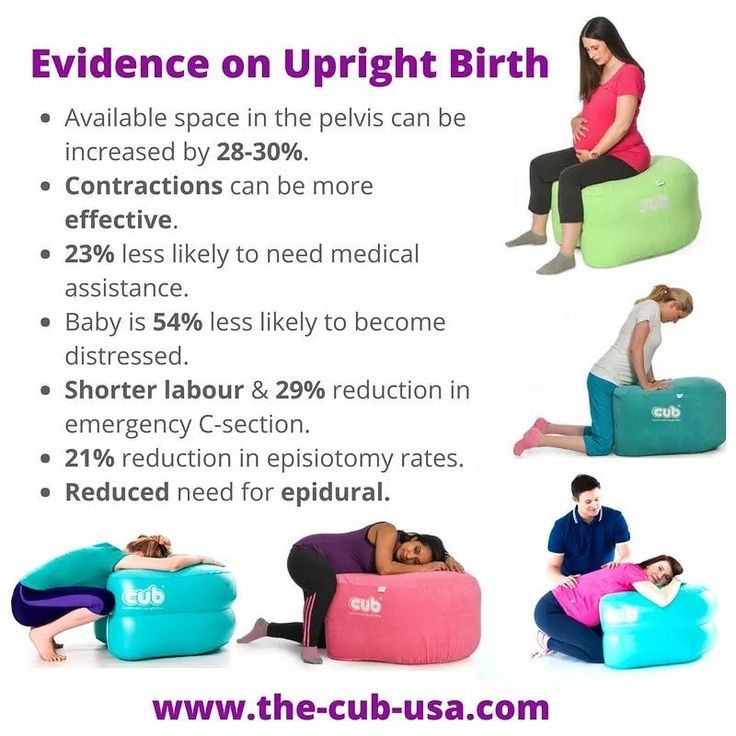 It also creates physical sensitivity after experienced pain. nine0003
It also creates physical sensitivity after experienced pain. nine0003
Image copyright Thinkstock
Image captionEven if memories of pain can be erased, what will it do?
Experiments on mice have shown that if you block a certain molecule in the spine of experimental animals, you can thereby erase their additional susceptibility to pain. However, later other scientists called the results of the described experiment into question and proved that mice born with the PCM-zeta molecule could still feel pain.
What about uncomfortable or traumatic pain associated with certain medical procedures? For example, when colonoscopy (bowel probing) is performed using conscious sedation, patients are sometimes given a drug called medazolam, which reduces the urge to defecate and contributes to the inability to form memories after the onset of the disease. Patients may wince or writhe in discomfort during this procedure, but it is hoped that at the end of the colonoscopy they will not feel pain and discomfort. nine0003
nine0003
Underlying sensations
Some people question the ethics of this approach, as well as its consequences. In an article published last year, Andrew Davidson, an anesthesiologist at the Royal Victorian Children's Hospital in Australia, warns that while drugs like midazolam make it harder to form conscious memories, they can't affect implicit, unconscious memories. These memories affect us, although we cannot consciously recall them. Just like we automatically button up our shirts or arrive at the bus stop in a familiar way, without thinking about when and how we formed the memories of these actions. nine0003
Worryingly, as Davidson suggests, even if you forget about the colonoscopy, you "will feel strange discomfort at the sight of a garden hose." Wouldn't it be more ethical to warn the patient in advance that this could happen?
It has even been suggested that, in order to prevent the psychological trauma that can result from such a rare occurrence as waking up a patient during an operation under general anesthesia, he should be given midazolam as soon as the anesthesiologist notices that he is awake, in order to prevent the formation of a memory of this incident.