Head sutures in babies
Facts about Craniosynostosis | CDC
Craniosynostosis is a birth defect in which the bones in a baby’s skull join together too early. This happens before the baby’s brain is fully formed. As the baby’s brain grows, the skull can become more misshapen.
Click here to view a larger image
Click here to view a larger image
What is Craniosynostosis?
Craniosynostosis is a birth defect in which the bones in a baby’s skull join together too early. This happens before the baby’s brain is fully formed. As the baby’s brain grows, the skull can become more misshapen. The spaces between a typical baby’s skull bones are filled with flexible material and called sutures. These sutures allow the skull to grow as the baby’s brain grows. Around two years of age, a child’s skull bones begin to join together because the sutures become bone. When this occurs, the suture is said to “close.” In a baby with craniosynostosis, one or more of the sutures closes too early. This can limit or slow the growth of the baby’s brain.
When a suture closes and the skull bones join together too soon, the baby’s head will stop growing in only that part of the skull. In the other parts of the skull where the sutures have not joined together, the baby’s head will continue to grow. When that happens, the skull will have an abnormal shape, although the brain inside the skull has grown to its usual size. Sometimes, though, more than one suture closes too early. In these instances, the brain might not have enough room to grow to its usual size. This can lead to a build-up of pressure inside the skull.
Types of Craniosynostosis
The types of craniosynostosis depend on what sutures join together early.
- Sagittal synostosis– The sagittal suture runs along the top of the head, from the baby’s soft spot near the front of the head to the back of the head. When this suture closes too early, the baby’s head will grow long and narrow (scaphocephaly).
 It is the most common type of craniosynostosis.
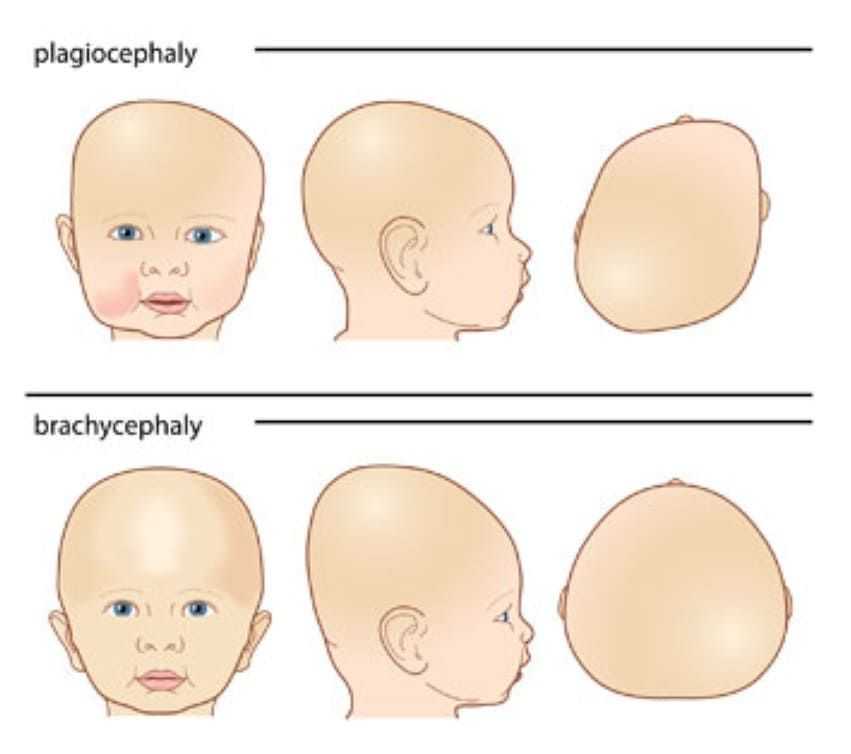
It is the most common type of craniosynostosis. - Coronal synostosis – The right and left coronal sutures run from each ear to the sagittal suture at the top of the head. When one of these sutures closes too early, the baby may have a flattened forehead on the side of the skull that closed early (anterior plagiocephaly). The baby’s eye socket on that side might also be raised up and his or her nose could be pulled toward that side. This is the second most common type of craniosynostosis.
- Bicoronal synostosis – This type of craniosynostosis occurs when the coronal sutures on both sides of the baby’s head close too early. In this case, the baby’s head will grow broad and short (brachycephaly).
- Lambdoid synostosis – The lambdoid suture runs along the backside of the head. If this suture closes too early, the baby’s head may be flattened on the back side (posterior plagiocephaly). This is one of the rarest types of craniosynostosis.
- Metopic synostosis – The metopic suture runs from the baby’s nose to the sagittal suture at the top of the head. If this suture closes too early, the top of the baby’s head shape may look triangular, meaning narrow in the front and broad in the back (trigonocephaly). This is one of the rarest types of craniosynostosis.
Other Problems
Many of the problems a baby can have depend on:
- Which sutures closed early
- When the sutures closed (was it before or after birth and at what age)
- Whether or not the brain has room to grow
Sometimes, if the condition is not treated, the build-up of pressure in the baby’s skull can lead to problems, such as blindness, seizures, or brain damage.
How Many Babies are Born with Craniosynostosis?
Researchers estimate that about 1 in every 2,500 babies is born with craniosynostosis in the United States.1
Causes and Risk Factors
The causes of craniosynostosis in most infants are unknown.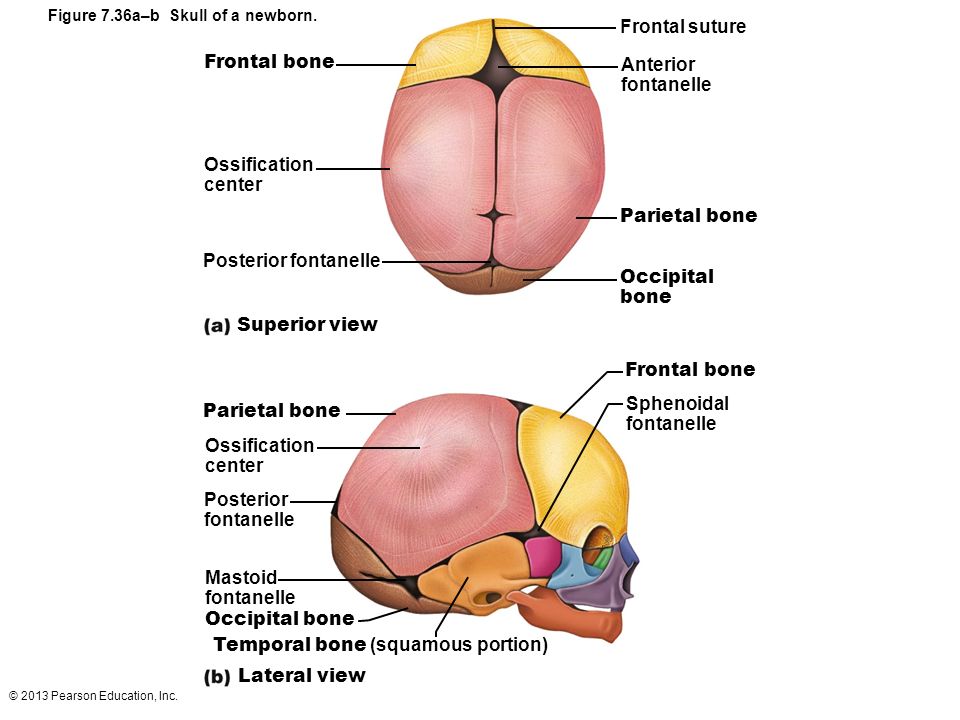 Some babies have a craniosynostosis because of changes in their genes. In some cases, craniosynostosis occurs because of an abnormality in a single gene, which can cause a genetic syndrome. However, in most cases, craniosynostosis is thought to be caused by a combination of genes and other factors, such as things the mother comes in contact with in her environment, or what the mother eats or drinks, or certain medications she uses during pregnancy.
Some babies have a craniosynostosis because of changes in their genes. In some cases, craniosynostosis occurs because of an abnormality in a single gene, which can cause a genetic syndrome. However, in most cases, craniosynostosis is thought to be caused by a combination of genes and other factors, such as things the mother comes in contact with in her environment, or what the mother eats or drinks, or certain medications she uses during pregnancy.
CDC, like the many families of children with birth defects, wants to find out what causes these conditions. Understanding the factors that are more common among babies with a birth defect will help us learn more about the causes. CDC funds the Centers for Birth Defects Research and Prevention, which collaborate on large studies such as the National Birth Defects Prevention Study (NBDPS; births 1997-2011), to understand the causes of and risks for birth defects, such as craniosynostosis.
Recently, CDC reported on important findings from research studies about some factors that increase the chance of having a baby with craniosynostosis:
- Maternal thyroid disease ― Women with thyroid disease or who are treated for thyroid disease while they are pregnant have a higher chance of having an infant with craniosynostosis, compared to women who don’t have thyroid disease.
 2
2 - Certain medications ― Women who report using clomiphene citrate (a fertility medication) just before or early in pregnancy are more likely to have a baby with craniosynostosis, compared to women who didn’t take this medicine.3
CDC continues to study birth defects, such as craniosynostosis, and how to prevent them. If you are pregnant or thinking about becoming pregnant, talk with your doctor about ways to increase your chances of having a healthy baby.
Diagnosis
Craniosynostosis usually is diagnosed soon after a baby is born. Sometimes, it is diagnosed later in life.
Usually, the first sign of craniosynostosis is an abnormally shaped skull. Other signs may include:
- No “soft spot” on the baby’s skull
- A raised firm edge where the sutures closed early
- Slow growth or no growth in the baby’s head size over time
Doctors can identify craniosynostosis during a physical exam. A doctor will feel the baby’s head for hard edges along the sutures and unusual soft spots. The doctor also will look for any problems with the shape of the baby’s face. If he or she suspects the baby might have craniosynostosis, the doctor usually requests one or more tests to help confirm the diagnosis. For example, a special x-ray test, such as a CT or CAT scan, can show the details of the skull and brain, whether certain sutures are closed, and how the brain is growing.
The doctor also will look for any problems with the shape of the baby’s face. If he or she suspects the baby might have craniosynostosis, the doctor usually requests one or more tests to help confirm the diagnosis. For example, a special x-ray test, such as a CT or CAT scan, can show the details of the skull and brain, whether certain sutures are closed, and how the brain is growing.
Treatments
Many types of craniosynostosis require surgery. The surgical procedure is meant to relieve pressure on the brain, correct the craniosynostosis, and allow the brain to grow properly. When needed, a surgical procedure is usually performed during the first year of life. But, the timing of surgery depends on which sutures are closed and whether the baby has one of the genetic syndromes that can cause craniosynostosis.
Babies with very mild craniosynostosis might not need surgery. As the baby gets older and grows hair, the shape of the skull can become less noticeable. Sometimes, special medical helmets can be used to help mold the baby’s skull into a more regular shape.
Each baby born with craniosynostosis is different, and the condition can range from mild to severe. Most babies with craniosynostosis are otherwise healthy. Some children, however, have developmental delays or intellectual disabilities, because either the craniosynostosis has kept the baby’s brain from growing and working normally, or because the baby has a genetic syndrome that caused both craniosynostosis and problems with how the brain works. A baby with craniosynostosis will need to see a healthcare provider regularly to make sure that the brain and skull are developing properly. Babies with craniosynostosis can often benefit from early intervention services to help with any developmental delays or intellectual problems. Some children with craniosynostosis may have issues with self-esteem if they are concerned with visible differences between themselves and other children. Parent-to-parent support groups also can be useful for new families of babies with birth defects of the head and face, including craniosynostosis.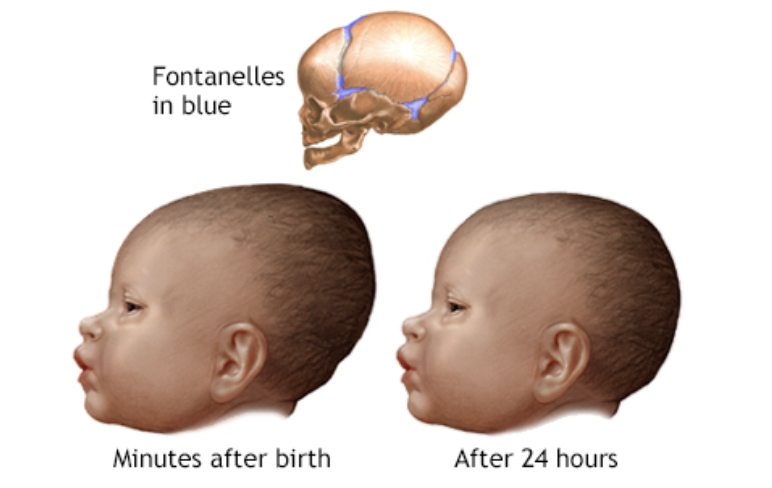
Other Resources
The views of these organizations are their own and do not reflect the official position of CDC.
- Children’s Craniofacial Association (CCA)
CCA addresses the medical, financial, psychosocial, emotional, and educational concerns relating to craniofacial conditions. - The National Craniofacial Association (FACES)
FACES is dedicated to assisting children and adults who have craniofacial disorders resulting from disease, accident, or birth.
References
- Boulet SL, Rasmussen SA, Honein MA. A population-based study of craniosynostosis in metropolitan Atlanta, 1989-2003. Am J Med Genet Part A. 2008;146A:984–991.
- Rasmussen SA, Yazdy MM, Carmichael SL, Jamieson DJ, Canfield MA, Honein MA. Maternal thyroid disease as a risk factor for craniosynostosis. Obstet Gynecol. 2007;110:369-377.
- Reefhuis J, Honein MA, Schieve LA, Rasmussen SA, and the National Birth Defects Prevention Study. Use of clomiphene citrate and birth defects, National Birth Defects Prevention Study, 1997–2005.
 Hum Reprod. 2011;26:451–457.
Hum Reprod. 2011;26:451–457.
The images are in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider (Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities) be credited and notified in any public or private usage of this image.
The images are in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider (Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities) be credited and notified in any public or private usage of this image.
Cranial sutures Information | Mount Sinai
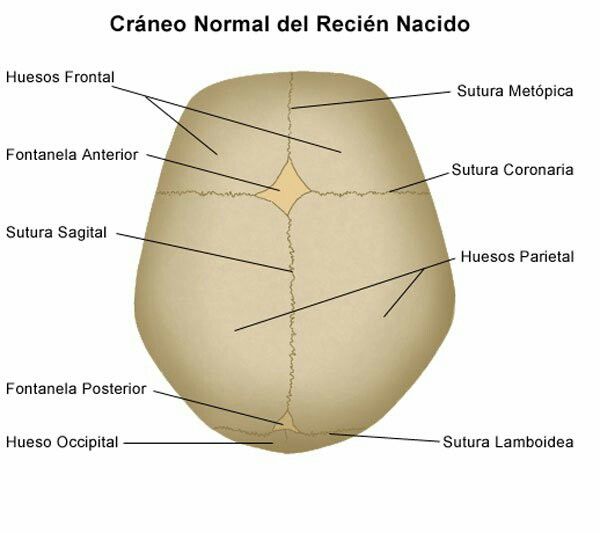
Fontanelles; Sutures - cranial
Cranial sutures are fibrous bands of tissue that connect the bones of the skull.
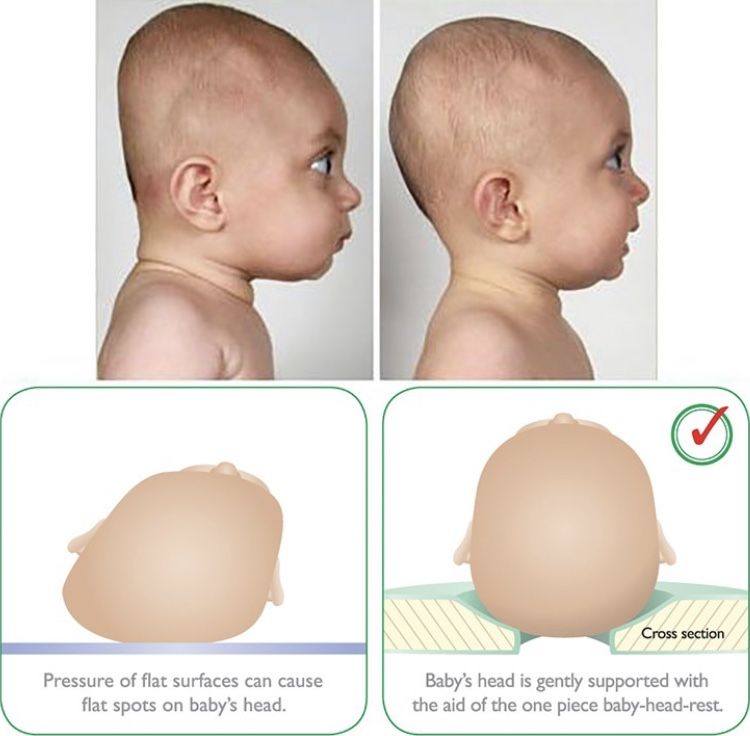
The sutures or anatomical lines where the bony plates of the skull join together can be easily felt in the newborn infant.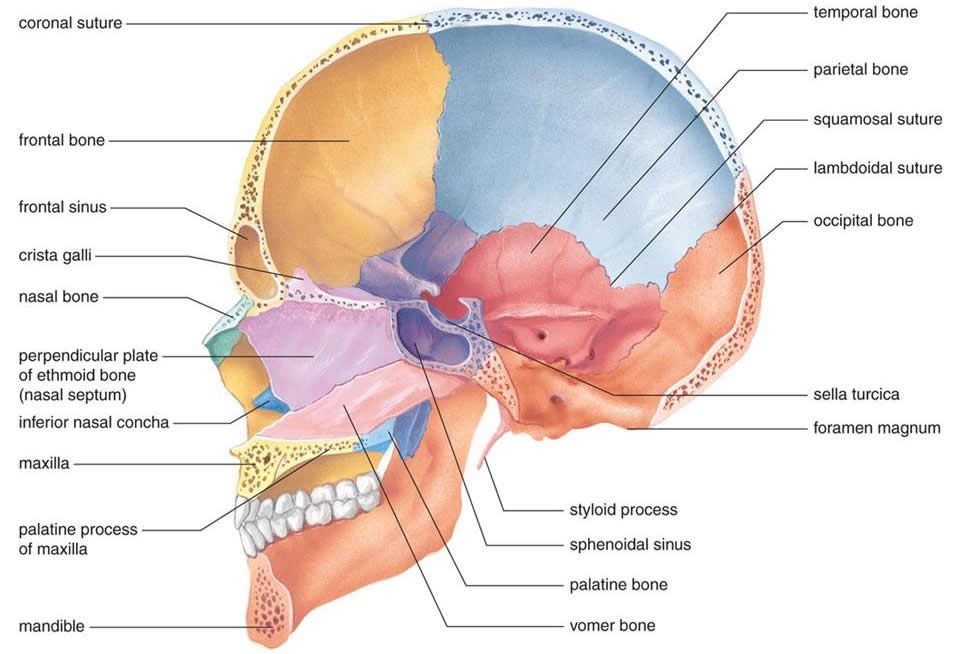 The diamond shaped space on the top of the skull and the smaller space further to the back are often referred to as the soft spot in young infants.
The diamond shaped space on the top of the skull and the smaller space further to the back are often referred to as the soft spot in young infants.
Fontanelles are the soft spots on an infant's head where the bony plates that make up the skull have not yet come together. It is normal for infants to have these soft spots, which can be seen and felt on the top and back of the head. Fontanelles that are abnormally large may indicate a medical condition.
Information
An infant's skull is made up of 6 separate cranial (skull) bones:
- Frontal bone
- Occipital bone
- Two parietal bones
- Two temporal bones
These bones are held together by strong, fibrous, elastic tissues called sutures.
The spaces between the bones that remain open in babies and young children are called fontanelles. Sometimes, they are called soft spots. These spaces are a part of normal development.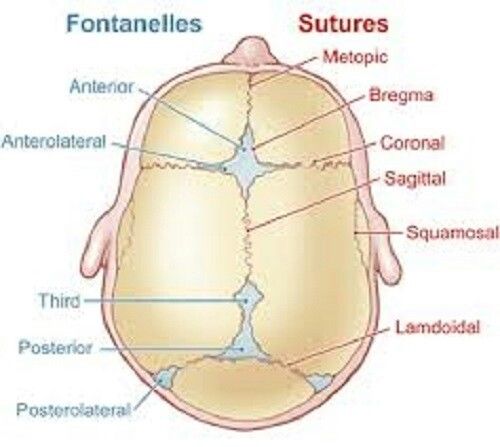 The cranial bones remain separate for about 12 to 18 months. They then grow together as part of normal growth. They stay connected throughout adulthood.
The cranial bones remain separate for about 12 to 18 months. They then grow together as part of normal growth. They stay connected throughout adulthood.
Two fontanelles usually are present on a newborn's skull:
- On the top of the middle head, just forward of center (anterior fontanelle)
- In the back of the middle of the head (posterior fontanelle)
The posterior fontanelle usually closes by age 1 or 2 months. It may already be closed at birth.
The anterior fontanelle usually closes sometime between 9 months and 18 months.
The sutures and fontanelles are needed for the infant's brain growth and development. During childbirth, the flexibility of the sutures allows the bones to overlap so the baby's head can pass through the birth canal without pressing on and damaging their brain.
During infancy and childhood, the sutures are flexible. This allows the brain to grow quickly and protects the brain from minor impacts to the head (such as when the infant is learning to hold his head up, roll over, and sit up).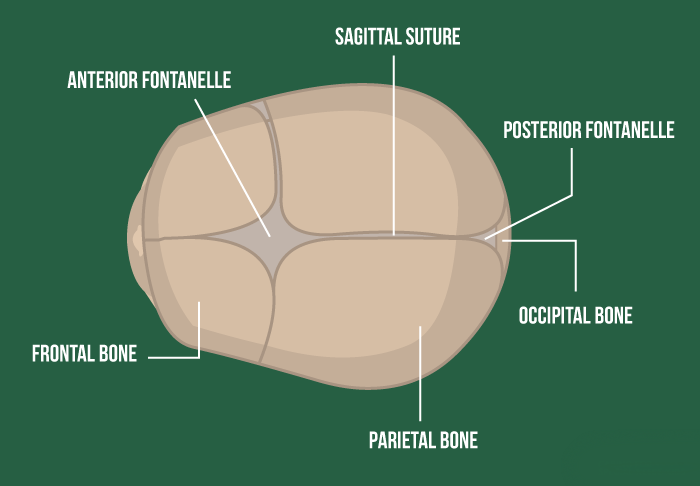 Without flexible sutures and fontanelles, the child's brain could not grow enough. The child would develop brain damage.
Without flexible sutures and fontanelles, the child's brain could not grow enough. The child would develop brain damage.
Feeling the cranial sutures and fontanelles is one way that health care providers follow the child's growth and development. They are able to assess the pressure inside the brain by feeling the tension of the fontanelles. The fontanelles should feel flat and firm. Bulging fontanelles may be a sign of increased pressure within the brain. In this case, providers may need to use imaging techniques to see the brain structure, such as CT scan or MRI scan. Surgery may be needed to relieve the increased pressure.
Sunken, depressed fontanelles are sometimes a sign of dehydration.
Goyal NK. The newborn infant. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 113.
Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 113.
Varma R, Williams SD. Neurology. In: Zitelli BJ, McIntire SC, Nowalk AJ, eds. Zitelli and Davis' Atlas of Pediatric Physical Diagnosis. 7th ed. Philadelphia, PA: Elsevier; 2018:chap 16.
Last reviewed on: 2/2/2021
Reviewed by: Neil K. Kaneshiro, MD, MHA, Clinical Professor of Pediatrics, University of Washington School of Medicine, Seattle, WA. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
Departments
- Main
- Subject of the Ministry of Health of the Russian Federation
- News
- About the hospital
- Information about the CSTO
- Wards
- Center for Specialized Surgical Care
- Uroandrology department
- Surgery
- Maxillofacial Surgery
- Traumatology and Orthopedics
- ENT (otorhinolaryngology department)
- Neurosurgical Department
- Operating unit
- Anesthesiology and Intensive Care Center
- Intensive Care Unit nine0003 Department of dialysis and efferent methods of therapy
- Anesthesiology-Intensive Care Unit
- Center for Specialized Surgical Care
- Center for specialized ophthalmological care
- Ophthalmological hospital for round-the-clock stay nine0003 Ophthalmic Day Hospital
- Outpatient appointment with an ophthalmologist
- Retinopathy of Prematurity Room (RetCam)
- Laser ophthalmology cabinet nine0007
- Auxiliary medical and diagnostic units
- Physiotherapy department
- Department of functional diagnostics
- Department of ultrasound diagnostics nine0003 Laboratory Technology Center
- Department of Radiology
- Endoscopy Department
- Hyperbaric Oxygen Room nine0003 Transfusiology room
- Department of Pediatric Oncology and Hematology
- Pediatric oncology and hematology day hospital with chemotherapy
- Department of Medical Rehabilitation
- Medical Rehabilitation Day Hospital
- General information nine0003 Doctors of department
- General information
- Interesting facts about the "Armenian disease"
- Photo gallery nine0003 Pediatric department
- Pulmonology department
- Photo gallery
- Doctors of the department
- General information
- Photo gallery
- Doctors of the department
- General information
- Photo gallery
- Doctors of the department
- General information
- Photo gallery
- Doctors of the department
- General information
- List of doctors nine0003 Price list
- Consultative Diagnostic Polyclinic
- Department of visiting advisory medical and preventive care
- General Information
- Photo gallery
- Doctors of the department
- General information nine0003 Photo gallery
Working hours of the organization and reception
Documents
- Anti-corruption
- Medical license
- Supplement to the license to carry out medical activities
- State registration certificate nine0003 Internal regulations
Manual.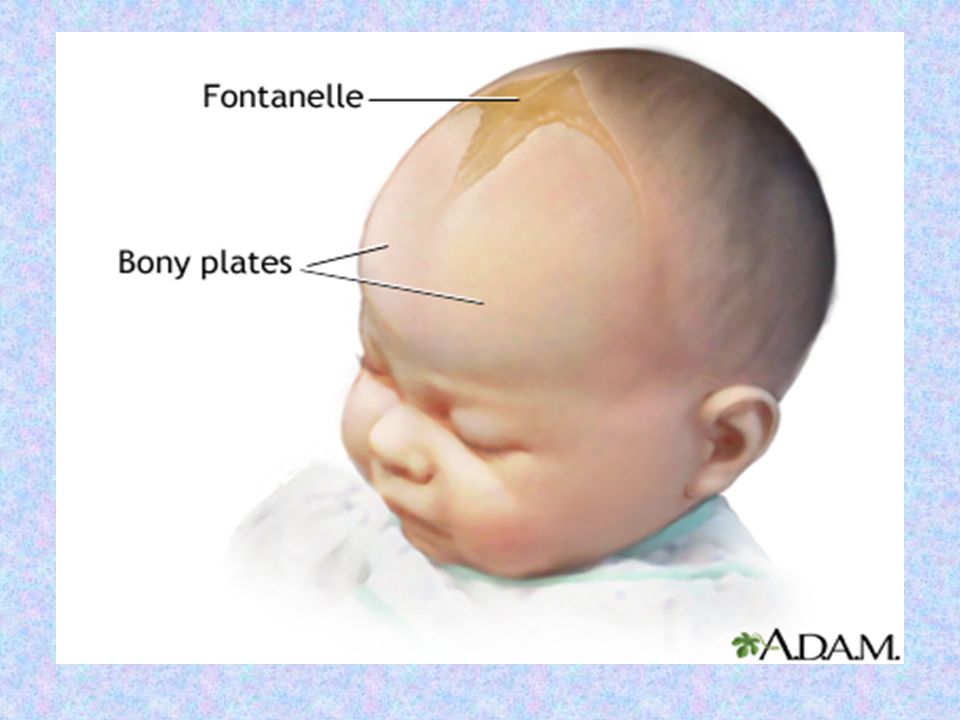 Employees
Employees
Rules and terms of hospitalization
Conditions for the provision of medical care
List of services
Indicators of accessibility and quality of medical care
Insurance companies
Supervisory and control bodies
Documents
- CMO List
- Work schedule of doctors of polyclinic
- On the possibility of families receiving a monthly payment in connection with the birth (adoption) of the first child
- List of types of MP provided free of charge
- Vital and Essential Drug List nine0003 Rights and obligations of citizens of the Russian Federation
- Instructions for making an appointment
- Appointment for a free appointment
- Appointment for a paid appointment (tel.
 300-80-39)
300-80-39) - If there are problems with writing
- Reviews and appeals
- Procedure for receiving and considering appeals
- Read reviews or appeals nine0003 Send feedback or appeal
- Manual
- Chief freelance specialists MH RO
- Pediatric uroandrology department nine0003 Surgical Department
- Photo
Photo gallery
- News
- Branches
- Video
- 2015
- 2016 nine0003 2017
Fontanelle of a newborn
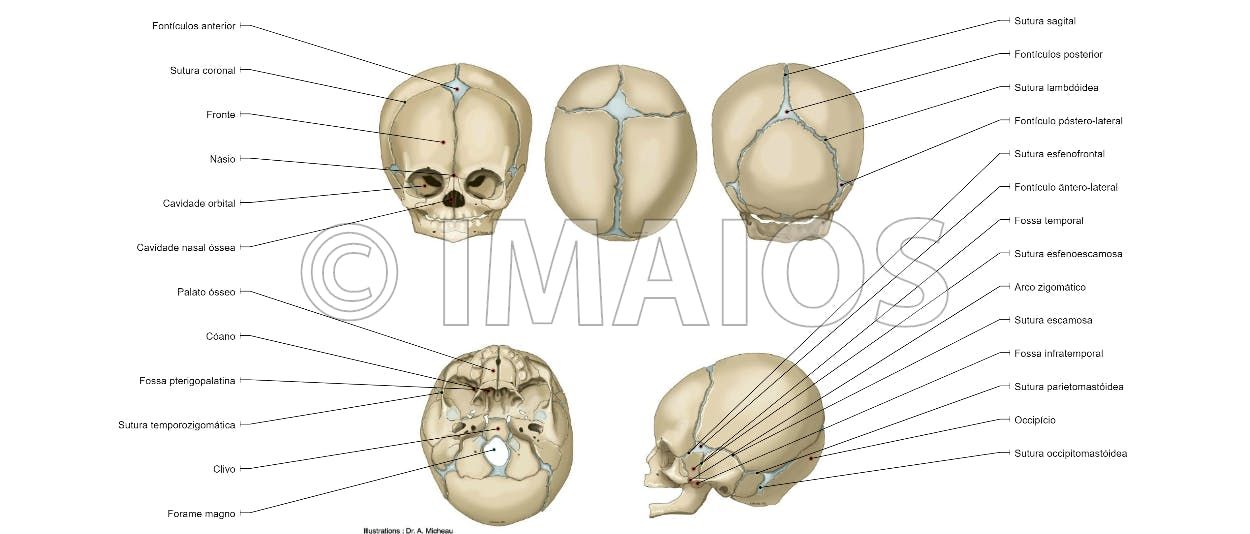
Fontanelles are non-ossified areas between the bones of the skull.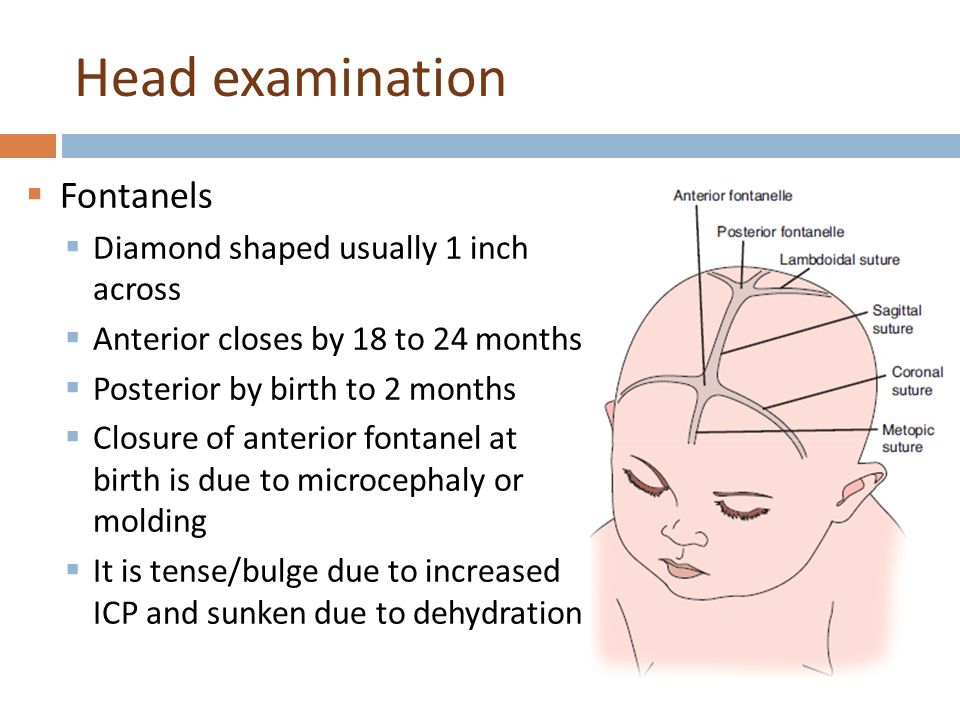 By the time of birth, the baby has 6 fontanelles:
By the time of birth, the baby has 6 fontanelles:
- front (large) - has a diamond shape, its size is from 0.6 to 3.6 cm (average 2.1)
- back (small) - its dimensions are about 0.5 cm
- paired lateral: wedge and mastoid
The size of the fontanelles is determined by a large number of factors: gestational age, hereditary predisposition, metabolic state, the presence of diseases, and other components. nine0197
What are fontanelles for?
They allow the movement of the bones of the skull and the reshaping of the head for safe passage through the birth canal.
Mothers who have given birth naturally remember what a strange head shape the baby had after birth, and how it became normal after 3-5 days.
Nature designed it so that the bones of the skull during childbirth would not damage the brain, and the baby would not get stuck in the birth canal at birth. nine0197
What about skull growth?
It may be surprising, but the brain does not grow behind the bones of the skull, but the cranium increases due to the active growth of the brain.