H v s test
How is the high vaginal swab used to investigate vaginal discharge in primary care and how do GPs’ expectations of the test match the tests performed by their microbiology services?
Article Text
Article menu
- Article
Text - Article
info - Citation
Tools - Share
- Rapid Responses
- Article
metrics - Alerts
Primary care
How is the high vaginal swab used to investigate vaginal discharge in primary care and how do GPs’ expectations of the test match the tests performed by their microbiology services?
- H Noble1,
- C Estcourt1,2,
- C Ison3,
- P Goold1,
- L Tite1,
- Y H Carter4
- 1Infection and Immunity, Barts and the London NHS Trust, London, UK
- 2Institute of Cell and Molecular Science, Barts and the London NHS Trust, Queen Mary’s School of Medicine and Dentistry, London, UK
- 3Department of Infectious Diseases and Microbiology, Imperial College School of Medicine, London, UK
- 4Department of General Practice and Primary Care, Barts and the London NHS Trust, Queen Mary’s School of Medicine and Dentistry, London, UK
- Correspondence to:
Dr C S Estcourt
Ambrose King Centre, Royal London Hospital, London E1 1BB, UK; Claudia.
estcourtbartsandthelondon.nhs.uk
Abstract
Objectives: To describe the management of vaginal discharge in general practice, with particular regard to the use of the high vaginal swab (HVS), and to compare GPs’ expectations of this test with the processing and reporting undertaken by different laboratories.
Methods: A postal questionnaire survey of 2146 GPs in the North Thames area and postal questionnaire study of the 22 laboratories serving the same GPs were carried out. GPs were asked how they would manage a young woman with vaginal discharge and what information they would like on an HVS report. Laboratories were asked how they would process and report on the HVS sample from the same patient.
Results: Response rate was 26%. 72% of GPs would take an HVS and 62% would refer on to a genitourinary medicine (GUM) clinic. 45% would offer empirical therapy and 47% of these would treat for candida initially. 75% of GPs routinely request “M,C&S” on HVS samples but 55% only want to be informed about specific pathogens. Routine processing of HVS samples varies widely between laboratories and 86% only report specific pathogens. 78% of GPs would like to be offered a suggested diagnosis on HVS reports, and 74% would like a suggested treatment. 43% of laboratories ever provide a diagnosis, and 14% provide a suggested treatment.
Routine processing of HVS samples varies widely between laboratories and 86% only report specific pathogens. 78% of GPs would like to be offered a suggested diagnosis on HVS reports, and 74% would like a suggested treatment. 43% of laboratories ever provide a diagnosis, and 14% provide a suggested treatment.
Conclusions: GPs frequently manage vaginal discharge and most of them utilise the HVS. GPs’ expectations of the test are not well matched to laboratory processing or reporting of the samples.
- vaginal discharge
- vaginal swab
- primary care
- COCP, combined oral contraceptive pill
- GUM, genitourinary medicine
- GPs, general practitioners
- HVS, high vaginal swab
- M,C&S, microscopy, culture, and sensitivity
- PHLS, Public Health Laboratory Service
- SOP, standard operating procedure
- STIs, sexually transmitted infections
http://dx.doi.org/10.1136/sti.2003.007781
Statistics from Altmetric.
 com
comRequest Permissions
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
- vaginal discharge
- vaginal swab
- primary care
- COCP, combined oral contraceptive pill
- GUM, genitourinary medicine
- GPs, general practitioners
- HVS, high vaginal swab
- M,C&S, microscopy, culture, and sensitivity
- PHLS, Public Health Laboratory Service
- SOP, standard operating procedure
- STIs, sexually transmitted infections
The National Strategy for Sexual Health and HIV, launched in England in 2002, advocates a much greater role for general practitioners (GPs) in the management of sexually transmitted infections (STIs) in the community.1 Unlike clinicians in specialist settings, GPs may not have ready access to a wide range of diagnostic tests including immediate microscopy. This may lead to differences in how conditions are investigated in general practice and specialist clinics.
This may lead to differences in how conditions are investigated in general practice and specialist clinics.
Vaginal discharge is a common presentation in general practice, potentially indicating the presence of STIs. What little is known about GPs’ investigation and management of vaginal discharge2,3 suggests that GPs commonly rely on the high vaginal swab (HVS)—an investigation rarely used by specialists.4,5 Despite this there is little information on what GPs expect from HVS, or whether they are satisfied with the reports they receive. Processing HVS samples accounts for a considerable proportion of the workload of most microbiology laboratories. Although Public Health Laboratory Service (PHLS) laboratories have a standard operating procedure (SOP)6 for HVS samples there are no universally accepted guidelines on how to process HVS samples, and this appears to be reflected by variability in processing and reporting between laboratories. 4 In addition, it is not clear whether GPs are receiving the information they want from HVS reports.
4 In addition, it is not clear whether GPs are receiving the information they want from HVS reports.
In this study we describe the management of vaginal discharge in general practice and compare GPs’ expectations of the HVS with the processing and reporting undertaken by laboratories.
METHODS
This study involved two postal questionnaire surveys: (i) a four page questionnaire to GPs in the North Thames area of the United Kingdom (a demographically mixed urban and suburban area close to and including central London). The questionnaire requested tick box and free text responses to demographic questions and investigation and management questions stemming from the case of a 20 year old woman on the combined oral contraceptive pill (COCP) who complained of vaginal discharge with a new sexual partner. (ii) A three page questionnaire to lead consultant microbiologists at the hospitals identified by the GPs as those to which they send their samples. This questionnaire requested tick box and free text responses, and focused on those tests which the laboratories would undertake on an HVS sample from the same patient both routinely and given clinical information. A questionnaire was sent to the first two out of every three GPs in an alphabetised list of those currently registered in 13 health authorities of north London. GP responses were anonymised. A single mailing was used for GP questionnaires. GPs were asked to pass the questionnaire to the practice nurse if he/she saw most of the women presenting with vaginal discharge. Microbiologists were sent a second questionnaire if no response was received to the first, and in some cases contacted by telephone.
A questionnaire was sent to the first two out of every three GPs in an alphabetised list of those currently registered in 13 health authorities of north London. GP responses were anonymised. A single mailing was used for GP questionnaires. GPs were asked to pass the questionnaire to the practice nurse if he/she saw most of the women presenting with vaginal discharge. Microbiologists were sent a second questionnaire if no response was received to the first, and in some cases contacted by telephone.
The GP questionnaire was revised in line with comments from a pilot study of 10 GPs outside the geographical area of study.
Ethical approval was obtained from the Northern and Yorkshire Multicentre Research ethics committee.
Data were recorded and analysed in an Access database.
RESULTS
Demographics
In all 2146 GPs were identified and completed responses were received from 553 (25.8%). Characteristics of responding GPs are shown in table 1.
Table 1
Characteristics of responding GPs
Seventy two per cent of GPs reported that women with vaginal discharge sometimes present directly to the practice nurse.
Completed responses were received from 14 (63.6%) of the 22 laboratories which were sent questionnaires.
Clinical management
GPs’ management of a young woman with symptoms and a new sexual partner is summarised in table 2. The case presented was as follows: “Laura, 20 years old, attends your surgery complaining of 2 weeks of increased vaginal discharge. She has a new male sexual partner and is taking the combined oral contraceptive pill.”
Table 2
Clinical management of the theoretical case
Of the 397 GPs who would take an HVS 298 (53.9%) would also routinely test for Chlamydia trachomatis and 71 (17.9%) would not (missing 27, 6.8%). Of those requesting C trachomatis routinely, 280 (94.0%) would use material from an additional endocervical swab, 18 (6.0%) would request C trachomatis on the HVS and one GP (0.3%) would test for C trachomatis on a urine sample.
Requesting, testing, and reporting of HVS samples
GPs were asked about how they request tests. When performing an HVS, 412 (75%) GPs would write “M,C&S” (microscopy, culture, and sensitivity) on the request form, with or without additional requests for culture of specific organisms. Four per cent (20) of GPs would not write “M,C&S” but would request culture for at least one of Candida spp, Trichomonas, Gardnerella, or anaerobes. Three per cent (14) of GPs would request culture for Neisseria gonorrhoeae on the HVS material.
When performing an HVS, 412 (75%) GPs would write “M,C&S” (microscopy, culture, and sensitivity) on the request form, with or without additional requests for culture of specific organisms. Four per cent (20) of GPs would not write “M,C&S” but would request culture for at least one of Candida spp, Trichomonas, Gardnerella, or anaerobes. Three per cent (14) of GPs would request culture for Neisseria gonorrhoeae on the HVS material.
Although there are no universal standards, as a point of reference, the PHLS SOP6 recommends an HVS sample from this patient be Gram stained for bacterial vaginosis (BV) and cultured for Trichomonas and yeasts. Eleven (79%) laboratories would perform microscopy and/or culture for candida, 13 (93%) would perform wet smear, six (43%) would culture for Trichomonas, and 10 (71%) would perform microscopy for clue cells. One laboratory (7%) routinely performs “full culture” on all HVS samples. Full culture varies between laboratories but usually includes aerobic and anaerobic culture. Other laboratories perform full culture on the basis of further clinical information—for example, presence of abdominal pain or postpartum state, or initial microscopy findings, but such criteria differ between laboratories (data not shown).
Other laboratories perform full culture on the basis of further clinical information—for example, presence of abdominal pain or postpartum state, or initial microscopy findings, but such criteria differ between laboratories (data not shown).
Most (303, 54.8%) GPs preferred to be informed about specific pathogens only and their respective sensitivities rather than all micro-organisms found, and 12 (85.6%) laboratories report in this way. One hundred and thirty GPs (23.5%) wanted to be informed about all micro-organisms isolated (as reported by two (14.3%) laboratories) and 120 GPs (21.7%) expressed no preference.
Four hundred and thirty (77.8%) GPs would like the HVS report to include a suggested diagnosis (1.3% wouldn’t, 116 (20.1%) missing) but only six laboratories (42.9%) ever provide this. Laboratories commented that they only provide a diagnosis on the basis of clinical information given by the GP, and several stated that they think it is inappropriate to give a clinical diagnosis on the basis of microbiological findings. Seventy four per cent (409) of GPs would like a suggested treatment to be included on the HVS report (4.3% would not, 120 (21.7%) missing) but only two laboratories (14%) provide this.
Seventy four per cent (409) of GPs would like a suggested treatment to be included on the HVS report (4.3% would not, 120 (21.7%) missing) but only two laboratories (14%) provide this.
DISCUSSION
Our study confirms that vaginal discharge is a common presentation in general practice. Almost half of our sample is seeing 1–5 women per week with vaginal discharge, and one third of our sample of GPs are prepared themselves to manage a young woman at risk of STIs, without reference to specialist services. Almost three quarters of GPs surveyed would take an HVS.
Encouragingly, GPs are screening for STIs and over half would test appropriately for C trachomatis.
Just under half of the GPs offered empirical therapy, and most commonly treated for candidiasis first line. However, bacterial vaginosis is at least as common a cause of vaginal discharge as candidiasis.7–9
GPs wanted as much information as possible from an HVS report, including direction from their laboratory with regards to diagnosis and treatment. Most laboratories do not provide this, and some expressed the opinion that this is outside their role.
Most laboratories do not provide this, and some expressed the opinion that this is outside their role.
We have shown that there is wide variation in the processing of HVS samples by microbiology laboratories in north London, and it is reasonable to assume that this is the case throughout the United Kingdom. In view of the workload that HVS samples represent to microbiology laboratories and the potential increase in samples received as GPs increase their involvement in sexual health1 a national guideline on processing HVS samples is likely to be beneficial.
Despite a disappointing GP response rate, we are able to report data from over 500 GPs. Selection bias is likely given that female GPs are over-represented in our sample,10 single handed GPs are under-represented (YH Carter, personal communication), and GPs who see fewer women with vaginal discharge were less likely to respond. Almost three quarters of GPs felt that women with vaginal discharge might present directly to their practice nurses but we only had one returned questionnaire clearly completed by a practice nurse. Further work is needed to look at how practice nurses manage women presenting with vaginal discharge. As with all questionnaire surveys our study is likely to include reporting bias.
Further work is needed to look at how practice nurses manage women presenting with vaginal discharge. As with all questionnaire surveys our study is likely to include reporting bias.
GPs in the United Kingdom are facing ever increasing clinical and administration pressures. The emphasis of the National Strategy for Sexual Health and HIV1 in widening access to sexual health care by increased provision in primary care settings is likely to be a considerable challenge to GPs who, while welcoming increased sexual health education, would have limited time in which to access it.
The HVS remains the mainstay of GPs’ management of vaginal discharge. Three quarters of GPs request non-specific processing (“M,C&S”) whereas most would prefer specific and directive reports, including suggested further investigation and treatment. Almost two thirds of GPs would do an additional C trachomatis test but in the specialist setting all such women would be tested for C trachomatis. GPs would appear to be receptive to guidance on STIs (C trachomatis) screening included on HVS reports.
GPs would appear to be receptive to guidance on STIs (C trachomatis) screening included on HVS reports.
CONCLUSIONS
Although many GPs are appropriately managing young “at risk” women with vaginal discharge our study highlights the potential for laboratory GP liaison in terms of HVS processing and reporting, which could greatly and cheaply assist GPs’ decision making when faced with a woman with vaginal discharge.
Key messages-
The HVS is the mainstay of investigation of vaginal discharge in general practice.
-
Processing of HVS samples varies widely between laboratories.
-
Inclusion of more advice on patient management on laboratory reports would be welcomed by GPs and could be a cheap and effective way of improving patient care.
Acknowledgments
We thank all the GPs and microbiologists who replied to our survey and helped with our pilot study. Invaluable IT support was provided by Peter Sutcliffe and Kevin Jones. Dr N Webber and Robin Ramphul assisted with the mail merge and data entry.
Invaluable IT support was provided by Peter Sutcliffe and Kevin Jones. Dr N Webber and Robin Ramphul assisted with the mail merge and data entry.
CONTRIBUTORS CE, HN, CI, YHC, and PG conceived and designed the study; HN, CE, LT, and PG helped with data collection and interpretation; CE, CI, and YHC supervised the study; HN wrote the draft of the manuscript; and HN, CE, CI, PG, and YHC reviewed the manuscript.
REFERENCES
- ↵
Department of Health. The national strategy for sexual health and HIV. Implementation action plan. www.doh.gov.uk/sexualhealthandhiv/index.htm (accessed 19 Dec 2002).
- ↵
Opaneye AA. Genital thrush in women: the attitudes and practice patterns of general practitioners in Teesside and north Yorkshire. J R Soc Health2999;119:163–5.
- ↵
O’Dowd TC, Parker S, Kelly A. Women’s experiences of general practitioner management of their vaginal symptoms.
 Br J Gen Pract1996;46:415–18.
Br J Gen Pract1996;46:415–18. - ↵
Jungmann E, Durrant K, Johnson A, et al. High vaginal swabs in general practice: laboratory results. 7th Conference of the Federation of Infectious Disease Societies, 29 Nov–1 Dec 2000:92.
- ↵
Dykhuizen RS, Harvey G, Gould IM. The high vaginal swab in general practice: clinical correlates of possible pathogens. Fam Pract1995;12:155–8.
- ↵
Public Health Laboratory Service. Investigation of genital tract and associated specimens. PHLS standard operating procedure. London: Public Health Laboratory Service Board, 2001.
- ↵
Murtagh J. Vaginal discharge. Aust Fam Phys1991;20:207–13.
-
Gilly PA. Vaginal discharge–its causes and cures.
 Postgrad Med1986;80:231–7.
Postgrad Med1986;80:231–7. - ↵
Wathne B, Holst E, Hovelius B, et al. Vaginal discharge–comparison of clinical, laboratory and microbiological findings. Acta Obstet Gynecol Scand1994;73:802–8.
- ↵
Department of Health. Statistics for general medical practitioners in England: 1991–2001. London: DoH, 2002.
Footnotes
Linked Articles
Read the full text or download the PDF:
Subscribe
Log in using your username and password
For personal accounts OR managers of institutional accounts
Username *
Password *
Forgot your log in details?Register a new account?
Forgot your user name or password?
6 Reasons Women need it
Women’s reproductive health is often neglected and not given the educational awareness and attention it deserves. In particular, the vagina is an essential part of the female body. It helps females get pregnant; it produces all kinds of bodily fluids and can heal itself when all the right conditions are in place. But when infections of the vagina, such as bacterial vaginosis or trichomoniasis, occur, it is detrimental to women’s health, which can eventually lead to serious health issues like urinary tract infections, cervical cancer, e.t.c. If not detected early and treated on time.
It helps females get pregnant; it produces all kinds of bodily fluids and can heal itself when all the right conditions are in place. But when infections of the vagina, such as bacterial vaginosis or trichomoniasis, occur, it is detrimental to women’s health, which can eventually lead to serious health issues like urinary tract infections, cervical cancer, e.t.c. If not detected early and treated on time.
Fortunately, there are many ways women can improve their health and protect themselves from various diseases and conditions that may harm them, especially vaginal health.
One test that is crucial for women’s health is the High Vaginal Swab Test (HVS). The test detects infections in the vagina and cervix. It is a simple test done in a doctor’s office or clinic.
There are several reasons every woman should have an HVS test at least once a year. Keep reading to learn more about the Six reasons women need a High Vaginal Swab Test to improve their health!
Need an affordable full-body screening test?
Save money and ensure sound health today.
High vaginal swab tests are an essential part of women’s health care. They can help detect infections that can cause serious health problems, such as pelvic inflammatory disease, infertility, and cancer.
The Startling Truth About Breast Cancer
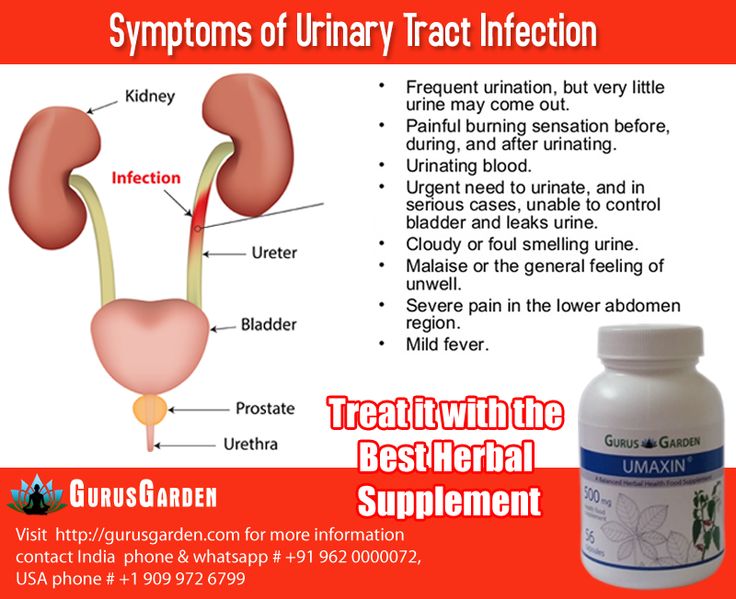
What are the symptoms of a vagina infection?Vaginal infections are a common problem. They can be hard to diagnose. To help you get your bearings and find the treatment, we have compiled a list of some of the most common symptoms of a vaginal infection.
- Nausea
- Fever
- Pain during sexual intercourse
- A discharge that is thick and yellow-green
- Signs of inflammation, such as pain during sex or after sex
- Pain while urinating
If you think you may have an infection, you should see a doctor for a proper diagnosis and treatment.
Everything You Need To Know About Cervical Screening And Pap Smear
Six (6) Important reasons for women to get this test done?- The test can help identify the cause of infertility in women.
- It can also identify whether a woman has an infection.
- The high vaginal swab test is efficient in detecting cancerous cells and preventing them from spreading to other body parts.
- The HVS test detects STDs such as HPV, chlamydia, trichomoniasis, and gonorrhea.
- A high vaginal swab test can also help detect the cause of abnormal vaginal bleeding in women who have never been diagnosed with any disease or infection.
- It is also valuable during pregnancy and postpartum because it helps to check for an infection such as Candidiasis, Group B streptococcus (GBS), or Gardnerella.
10 Things every Pregnant Woman With Diabetes should know
What are the risks associated with not getting a high vaginal swab test?Several risks are associated. The first is that you could miss an infection present in your vagina. It can worsen the infection and spread to other parts of your body. Not getting an HVS test can make it more difficult to diagnose other vaginal diseases, like bacterial vaginosis or trichomoniasis. Finally, not getting a high vaginal swab test means you cannot get the proper treatment.
Finally, not getting a high vaginal swab test means you cannot get the proper treatment.
A woman who is sexually active and has new or multiple sexual partners may also benefit from this test. Women should take a vagina swab test annually.
In conclusion, determining a woman’s reproductive health depends on taking a Vagina swab test. If a woman ignores her vaginal health, she could damage vital organs or get infected with all kinds of STDs, leading to even more danger and irreparable damage to her reproductive health. It is necessary to have regular testing done because infections are often treatable before permanent damage occurs. Need a private screening test? Click here to get started.
6 Quick Tests to Secure The Baby’s Health During Pregnancy
Frequently Asked Questions about High Vaginal Swab TestWhat is a high vaginal swab test used to diagnose?A high vaginal swab test is a diagnostic tool that helps to determine the cause of abnormal vaginal bleeding.
Doctors conduct tests for bacterial vaginosis (BV), trichomoniasis, and yeast infections.
Can the HVS test detect STDs?Yes, the HVS test can detect STDs. It is a simple blood test that checks for antibodies against specific pathogens. If an STD is present, it will reflect this in the results.
Abuser Test - Poster Daily
We have prepared a test with typical life situations that can serve as markers of abusive behavior in a relationship. Go through it and find out if you are doing everything right.
If your partner changes passwords on all social networks, how would you react?
I don't even know about it, I never follow such things
I’ll ask why it was needed, but it’s unlikely that he/she is hiding something from me
I will ask you to give me new passwords - I feel calmer when I know with whom I communicate and what my partner (s) is doing
Next!
You are about to introduce your partner to your parents. But her / his clothes for the meeting seem unsuitable to you. You:
But her / his clothes for the meeting seem unsuitable to you. You:
I'll make you change clothes. I know better how to make a good impression on my parents
I will reasonably ask you to change clothes. If I receive a refusal, of course, I will not be happy, but I will not mind
I don't think appearance will play any role. The main thing is that she/he should be comfortable
Next!
Your partner wants to discuss relationship problems. How would you react to this conversation?
I don't mind. If something does not suit her / him, let her speak out
I don't like these showdowns, they always turn into brainwashing
I think we have some work to do. It's good that we came to this conversation
It's good that we came to this conversation
Next!
You are discussing how you will spend the upcoming weekend, and your partner(s) desires do not match yours. Who will have the last word?
We will find a compromise, and if not, it is not necessary to spend the weekend together. Let's go where we want, separately
Usually I always take matters into my own hands and decide what we will do. And the partner (s) agrees with me
We will argue, give arguments and choose one thing
Next!
When can you raise your voice to your partner(s)?
I find this unacceptable. And if sometimes I break down, then I immediately apologize
I can only raise my voice if my partner provokes a quarrel with his behavior or words
It happens that I scream during quarrels, because otherwise I can’t get through to her / him
Next!
Beloved does not answer calls and messages for a long time, but you know that she/he has important things to do. Sound the alarm?
Sound the alarm?
No, he/she warned me that he/she might be late. I'll calmly go about my business
I'll wait some more time and start to worry, you never know what happened
Yes. And, in fact, it doesn’t take long to write a short message that everything is fine with her / him!
Next!
Do you ever say, "If you don't [do something necessary], then you don't love me"?
No, I think that these are manipulations that do not lead to anything good
Maybe sometimes and rather as a joke
Yes, and I don't think it's manipulation. Doing everything for a loved one is normal
Next!
Have you ever shared with someone a small and, in your opinion, not very important secret of a partner (s)?
No. All secrets will forever remain with me
All secrets will forever remain with me
He used to tell (s) to both friends close to us with a partner (s), and we all laughed together. Nothing criminal
Yes, I told a close friend of mine. But I know for sure that he won't tell anyone, you don't have to worry
Next!
Your partner is doing something that you think is hurting him (poor diet, bad habits, spending too much time on the computer, etc.). What will you do?
I will save her / him - who, if not a loved one, can help
Talk to her/him and share my concern for her/his well-being
There is nothing to discuss here. If our relationship is important to a person, he will change for me
Next!
Do you say to your partner such affectionate and joking words as "my favorite silly", "my fool", "who is this chubby piglet?" etc.
No, I don't remember such a thing
Yes, it happens, I speak from the heart and not from evil
I almost always say this and I don’t consider it something bad - such an address, on the contrary, shows my love
Next!
Repeat the test
Series Pregnancy test watch online for free all series in a row in good HD 1080 / 720 quality
Obstetrician-gynecologist Natalia Bakhmetyeva talks to the patient Nefedova lying under a dropper: the dynamics worsened, let's discuss the options, I called the urologist. Nefedova: if he removes my second kidney, it will make some sense. Bakhmetyeva: it's risky to wait, I suggest delivery at 31 weeks. Nefedova refuses: Kolmogorov said that I could hold out for another 3-4 weeks, I want to give birth to a healthy child. I knew what I was getting into - the only kidney, chronic pyelonephritis. I decided everything - I want to convey. Did Kolmogorov guide you from the very beginning of your pregnancy? Yes, I chose the best doctor. When he sent me to you, he said that I could decide for myself if there were options. And they are.
I knew what I was getting into - the only kidney, chronic pyelonephritis. I decided everything - I want to convey. Did Kolmogorov guide you from the very beginning of your pregnancy? Yes, I chose the best doctor. When he sent me to you, he said that I could decide for myself if there were options. And they are.
Bakhmetyeva unsuccessfully tries to get through to Kolmogorov. Bakhmetyeva approaches the head physician of the clinic, Ilya Yakovlevich, and says that Nefedov needs to be operated on urgently. What about Kolmogorov? Not available. The head physician says that with such urgency, Bakhmetyeva, instead of pulling him, could take the initiative into her own hands. At this moment, Bakhmeteva is summoned to Nefedova. The patient has stopped breathing. The resuscitator does her intubation and chest compressions. Nefedova is taken to the operating room. But, despite all the efforts of Bakhmetyeva and her colleagues, the patient dies on the operating table. The child is saved.
Bakhmetyeva drives up to the RAMS building. She leaves Kolmogorov a message on the answering machine: come down, I'm downstairs. But then she sees Kolmogorov leaving the building. Bakhmetyeva tells him: if you are interested, Yuri Alekseevich, then Nefedova Nadezhda Grigorievna died during the operation. Kolmogorov told her that at 46 years old with one kidney, you can give birth to a hero and a genius on the 40th week. Yura, I called you a hundred times... Kolmogorov says: stop acting like a quivering student, it's time for you to make your own decisions, it's time to grow up. Understand! Leaving Natalya, Kolmogorov heads to his wife, who meets him near the car. She asks her husband: who is this? My student. Kolmogorov kisses his wife, they get into the car and drive away.
She leaves Kolmogorov a message on the answering machine: come down, I'm downstairs. But then she sees Kolmogorov leaving the building. Bakhmetyeva tells him: if you are interested, Yuri Alekseevich, then Nefedova Nadezhda Grigorievna died during the operation. Kolmogorov told her that at 46 years old with one kidney, you can give birth to a hero and a genius on the 40th week. Yura, I called you a hundred times... Kolmogorov says: stop acting like a quivering student, it's time for you to make your own decisions, it's time to grow up. Understand! Leaving Natalya, Kolmogorov heads to his wife, who meets him near the car. She asks her husband: who is this? My student. Kolmogorov kisses his wife, they get into the car and drive away.
Bakhmetyeva submits a letter of resignation of her own free will. Ilya Yakovlevich: you're not to blame, don't punish yourself. Losing a patient on the operating table is always a tragedy, but it happens. Bakhmetyeva: don't comfort me, just sign the application, I won't change my mind. Ilya Yakovlevich: But you understand that without Kolmogorov's blessing they won't let you into any shop in Moscow now. Bakhmeteva: fortunately, there are shops not only in Moscow. Having signed the application, Ilya Yakovlevich reports: a couple of weeks ago, an old acquaintance, the head doctor of a clinic in a northern city, called me, he was looking for the head of the observation - young, promising.
Ilya Yakovlevich: But you understand that without Kolmogorov's blessing they won't let you into any shop in Moscow now. Bakhmeteva: fortunately, there are shops not only in Moscow. Having signed the application, Ilya Yakovlevich reports: a couple of weeks ago, an old acquaintance, the head doctor of a clinic in a northern city, called me, he was looking for the head of the observation - young, promising.
Late in the evening, Bakhmetyeva is loading things into the trunk of her car. Kolmogorov arrives: Natasha, what's going on? Why do you need to drop everything at once - a clinic, a dissertation? Running away in the middle of the night, not answering my calls - what kind of kindergarten? Bakhmetyeva: Don't you understand? The man is dead. Kolmogorov: Yes, sometimes patients die. So what? Analyzed, saddened - we go further. Bakhmetyeva: Here I am going. Kolmogorov: to whom and what are you proving? What can you do without me? You lived with me for ten years. Yura, to live is when under one roof. So you wanted a simple philistine happiness? I know too little about him to want. But I know exactly what I don't want anymore. Thinking you have a man when you don't. Telling yourself that working around the clock and seeing you once a week is okay. Thanks for reminding me how old I am. I'm going to grow up and find out what I want.
So you wanted a simple philistine happiness? I know too little about him to want. But I know exactly what I don't want anymore. Thinking you have a man when you don't. Telling yourself that working around the clock and seeing you once a week is okay. Thanks for reminding me how old I am. I'm going to grow up and find out what I want.
Bakhmetyeva arrives in St. Petersburg.
Obstetrician-gynecologist Alla V. Kashina sleeps in her office after celebrating her anniversary with her colleagues the day before. Kashina is 50 years old. She is awakened by a phone call: another patient has been brought to the clinic. Kashina puts himself in order and goes to the emergency department. She asks: what do we have here? The waters broke forty hours ago. Kashina examines the patient, commands: a gurney! In her operblock, quickly! The husband of the woman in labor remains in the ward, he is dressed in a Hare Krishna outfit, reciting mantras.
Bakhmetyeva drives up to the clinic building where she will now work. The security guard refuses to let her into the parking lot. He refers to the instructions: your car is not on the list, I don't know you, no one warned me about you, you don't have a pass either. Bakhmetyeva says she can call the head physician. The guard declares that he has his own superiors, to whom he submits. Bakhmetyeva leaves her passport as a pledge so that they let her through.
The security guard refuses to let her into the parking lot. He refers to the instructions: your car is not on the list, I don't know you, no one warned me about you, you don't have a pass either. Bakhmetyeva says she can call the head physician. The guard declares that he has his own superiors, to whom he submits. Bakhmetyeva leaves her passport as a pledge so that they let her through.
Midwife Evgenia Efimovna Mishina, known by her colleagues as Misha, is trying to hear the heartbeat of a Hare Krishna patient's fetus using a wooden tube. A young obstetrician-gynecologist is interested in: what is there, Misha? If I can't hear it with my ear, then it doesn't exist. Kashina enters the operative block, reports: the head physician is unavailable. Mishina turns to Kashina: the fetus is dead, it is necessary to do a fruit-destroying one. Leave her uterus, you fool, because the first child, you don’t need the last one. Irritated Kashina pulls the midwife: Evgenia Efimovna, mind your own business. The offended Mishina departs. Appears anesthesiologist Alexander Anatolyevich Dontsov: well, what do we have here? Kashin: supravaginal amputation, due to prolonged anhydrous. Dontsov sighs: it means that her fate is to be childless. Kashina: I would like children, I would not give birth at home.
The offended Mishina departs. Appears anesthesiologist Alexander Anatolyevich Dontsov: well, what do we have here? Kashin: supravaginal amputation, due to prolonged anhydrous. Dontsov sighs: it means that her fate is to be childless. Kashina: I would like children, I would not give birth at home.
In the corridor, intern Pavel Samoryadov fills in the case history of a newly admitted patient. Misha is standing nearby, she grumbles: why immediately shred the table and the uterus? Previously, a dead fetus was pulled out through a certain place, and the uterus was left in place. Bakhmetyeva comes up, says hello, looks into the medical history, is horrified and runs to the operating room. Mishina: what was that now? Paul: I don't understand.
Kashina lifts the scalpel over the patient's abdomen. Bakhmetyeva bursts into the operating room, she throws the surgical instruments prepared for the operation onto the floor. Kashina is indignant: why are outsiders in the operating block? Call security! Bakhmetyeva introduces herself, says that from today she is the head of the observation department. Then she commands: the patient to the delivery room, quickly!
Then she commands: the patient to the delivery room, quickly!
Mishina helps Bakhmetyeva remove the dead fetus. Pavel faints during this procedure. Dontsov brings the intern to his senses and puts him out into the corridor.
After a successful operation, Bakhmetyeva tells Pavel to leave his sensitivity for dates in the operating room - this is an unaffordable luxury. Bakhmetyeva is called by the head physician. When she leaves, Pavel asks Dontsov: who was right - Bakhmetyev or Kashin? He says: Kashina did what she was supposed to, but Bakhmetyeva swung at more. So you are for Bakhmeteva? No, I'm for mine. Kashina and I gave birth to half a division of children together, and I never liked doctors with God's syndrome.
Kashina reprimands the head physician of the clinic, Oleg Evgenievich Samoryadov (Pasha's father): well, you gave me a present for my anniversary. Couldn't you have at least warned me ahead of time? Samoryadov: Bakhmetyeva acted boldly and professionally, and she kept the uterus, which you wanted to cut into pieces, so as not to risk it. Yeah, and now the temperature will rise, and the uterus will still have to be removed, but only a septic one. You're screwing up! Go to work and don't disturb her. I will follow.
Yeah, and now the temperature will rise, and the uterus will still have to be removed, but only a septic one. You're screwing up! Go to work and don't disturb her. I will follow.
Bakhmetyeva enters the office. Kashina, pursing her lips, is removed. Samoryadov congratulates the new head of the observatory on her military entry into office. Just keep in mind for the future: such decisions are made by the council. Bakhmetiev: which still needs to be collected, and the risk of infectious complications increases. Samoryadov: I have no doubt that you are a good doctor, but what kind of head you will be is still unknown. You need to be able to build relationships with subordinates.
After the round, Bakhmetyev scolds Pavel. Why did you blurt out the patient about placental abruption? If the next time something seems to you, be patient until the corridor, take pity on the patient. Have you read her medical history? She had eight miscarriages! She has never made it past 30 weeks. Then Bakhmetyeva switches to Sechenov: I asked you to do an ultrasound, where is it? Sechenov is silent. Bakhmeteva leaves. Pavel: Does she even know how to talk normally? Sechenov: I'm worried about something else. I brought her cards half an hour before the round. How did she manage to study everything about 12 patients? I feel, Pasha, our free life is over. Kashina will be remembered later as a good king.
Then Bakhmetyeva switches to Sechenov: I asked you to do an ultrasound, where is it? Sechenov is silent. Bakhmeteva leaves. Pavel: Does she even know how to talk normally? Sechenov: I'm worried about something else. I brought her cards half an hour before the round. How did she manage to study everything about 12 patients? I feel, Pasha, our free life is over. Kashina will be remembered later as a good king.
IVF specialist Ruslan Bazanov enters the clinic building. Head nurse Dina Rafailovna shares with him the latest gossip about the new head of the observation. Having learned her last name, Bazanov drops a cup of coffee from his hands.
A patient comes to see Bazanov, who has been trying to get pregnant for 15 years. She underwent IVF 25 times, but to no avail. Bazanov assures that there are still chances of success. He sees no reason to refuse a woman who so wants to become a mother.
At lunchtime, Bakhmetyeva is relaxing on a bench in the clinic's yard. A Hare Krishna approaches her: why didn't you save my child? Because you marinated your wife at home for two days. The Krishnaite is crying: do you also think that only obscurantists give birth at home? But after all, you can’t tear the child from the mother when he was born, the umbilical cord must not be cut, and the placenta must be buried. We wanted children so much. My wife couldn't get pregnant for two years. Then we went to India, and a miracle happened. Why didn't you save the child?
The Krishnaite is crying: do you also think that only obscurantists give birth at home? But after all, you can’t tear the child from the mother when he was born, the umbilical cord must not be cut, and the placenta must be buried. We wanted children so much. My wife couldn't get pregnant for two years. Then we went to India, and a miracle happened. Why didn't you save the child?
Neonatologist Andrei Lazarev enters the yard. He turns to the Hare Krishna: what is your name? Andrew. Listen, namesake, is your beloved woman still alive? Yes. This is the main thing. She can still give birth - also not bad. Let's go to her now, you will say that you love her. Lazarev leads the Krishnaite away.
Bakhmetyeva sees Bazanov getting out of the car that has driven up to the clinic. She recognizes her classmate, sneaks up behind him, closes her eyes with her hands: Ruslanchik-Bazanchik, a sunny boy. Bakhmetiev! Natalya hangs on Ruslan's neck. He says you haven't changed at all. And you grew up and became even more beautiful, aren't you ashamed? Bakhmetyeva asks: where is the buffet? I haven't seen food in days. Bazanov: buffet is not food. And you are still the same snob. A long-legged brown-haired woman in a medical gown comes out of the clinic building, greets Bazanov, and passes by. Bakhmetyeva: Is that sister Nicole Kidman? Bazanov: he is lying that he is the head of the laboratory. This is Olga Olshanskaya, a great clever girl. In love? But not in me. Bazanchik, well, can there really be someone who is not in love with you? You seem to be hungry, let's go eat.
Bazanov: buffet is not food. And you are still the same snob. A long-legged brown-haired woman in a medical gown comes out of the clinic building, greets Bazanov, and passes by. Bakhmetyeva: Is that sister Nicole Kidman? Bazanov: he is lying that he is the head of the laboratory. This is Olga Olshanskaya, a great clever girl. In love? But not in me. Bazanchik, well, can there really be someone who is not in love with you? You seem to be hungry, let's go eat.
Lazarev comes to the laboratory and asks Olshanskaya to do one analysis. Olshanskaya asks Lazarev about Bakhmeteva. He says that he saw her briefly, but already on the first occasion it is clear that she is a maximalist, it is difficult with such people. Olshanskaya: see you on Friday? Lazarev: I have children on Friday. On Saturday? Olshanskaya: I don't know. I have a sports club, a massage, then a meeting with a childhood friend. If, of course, you squeeze in... Lazarev kisses Olshanskaya: I'm compact.
In the dining room, Bazanov and Bakhmetyeva ask each other what has happened in the seven years they have not seen each other. Bakhmetyeva answers questions about her personal life and reasons for leaving Moscow evasively. Her phone rings. There was an accident, eight cars. A pregnant woman is among the victims.
Bakhmetyeva answers questions about her personal life and reasons for leaving Moscow evasively. Her phone rings. There was an accident, eight cars. A pregnant woman is among the victims.
At the emergency department, Pavel and Sechenov are waiting for the arrival of a patient injured in an accident. Suitable couple. A pregnant woman says that her five-year-old daughter kicked her in the stomach last night: it hurts very badly. Sechenov instructs Pavel to do an ultrasound. Kashina, walking towards him, says that Pavel should start the inspection, she will come later.
A patient is brought in after an accident, she is 40 weeks pregnant, has a hip injury and is bleeding. Kashina believes that the placenta has exfoliated. Bakhmetyeva gives her an order: take her to the operating unit, first a caesarean section, then a hip, call a traumatologist. Pavel approaches Kashina: what to do with the woman whom her daughter kicked in the stomach? Oh, I totally forgot. What is an ultrasound? I did, nothing is visible, but it seems that something is wrong. She complains of pain. Bakhmetyeva decides to deal with the patient. On examination, the woman grimaces in sharp pain. Is that a caesarean scar? Yes. Were there other surgeries? Myoma was cut out.
She complains of pain. Bakhmetyeva decides to deal with the patient. On examination, the woman grimaces in sharp pain. Is that a caesarean scar? Yes. Were there other surgeries? Myoma was cut out.
Bakhmetyeva and Pavel drive the patient to the operating room. Near it is another gurney with a woman after the accident. Bakhmetyeva asks Kashina: why haven't they started yet? All the anesthesiologists are in surgery now, in an accident. Mishina: will be in 20 minutes, if they don't lie. Bakhmetyeva: we urgently need an operating room, her condition is critical. Kashina: We can't do two caesareans at the same time, the patient has a lot of blood loss. Bakhmeteva: yours can wait, she has a lot of damage, but the child is out of danger, and here we can lose both.
Bakhmetyeva believes that her patient had a uterine rupture. She performs a C-section on her under local anesthesia. As a result, both the child and the woman in labor remain alive. Mishina is delighted with the actions of Bakhmetyeva. Kashina believes that she was just lucky.
Kashina believes that she was just lucky.
Bazanov helps Bakhmeteva find an apartment in St. Petersburg. On the way to work, Bakhmetyeva asks him about her subordinates: which of them should I be afraid of? You can handle the rest yourself.
The pop diva Meridian (her real name is Marina) is brought to the clinic. At the appointment with Bakhmetyeva, she says that already in the late stages of pregnancy, the fetus was diagnosed with Down syndrome. The husband of the pop diva is an oligarch, he is waiting for a normal heir. Therefore, Marina hid the diagnosis from him. And now she doesn't want the baby to be born alive. Bakhmetyeva says that no doctor would agree to kill a child with a pathology. Marina intends to leave the clinic, but at the door she faints. Bakhmetyeva insists on the hospitalization of a VIP patient who has a fetal presentation.
Bazanov is trying to convince a patient who was undergoing IVF by his colleagues from another clinic to get rid of at least two out of four embryos. Giving birth to a healthy quadruple is very unlikely. The woman straightens up.
Giving birth to a healthy quadruple is very unlikely. The woman straightens up.
A prisoner from a pre-trial detention center is brought to the clinic. A woman (Anastasia) killed her husband - exceeding self-defense, he beat her. She has already started contractions. Despite the protests of Dina Rafailovna, Bakhmetyeva gives the order to register the patient and issue gowns to the guards accompanying her.
At the end of the working day, Samoryadov calls Bakhmetyeva and tells her to inform the management of her decisions in extraordinary situations.
Late in the evening, Meridian begins to bleed vaginally. She is rushed to the operating room.
Bakhmetyeva accepts Bazanov's invitation to dine at a restaurant. He orders champagne, expresses the hope that their relationship will become more than friendly. Bakhmetyeva flirts and laughs off.
Misha sees that Kashina cannot cope with Meridian's bleeding. She calls the head nurse and demands that she call Bakhmetyeva: otherwise we will have two VIP corpses.
Saying goodbye to Bazanov, Bakhmetyeva answers Diana Rafailovna's call and rushes to the clinic. She replaces Kashina and finishes the operation started by that one. The child is born premature. They are engaged in Lazarev. In the morning he tells Meridiana: your child is alive, a boy, genetic analysis has come, your son has Down syndrome. Thanks, I'm aware.
Meridian is visited by her producer Vladik. He says that a child down with a star can be a reason for crazy PR: everyone just swears. Meridiana declares: you would not go to the forest with such PR.
Bakhmetyeva delivers Anastasia. Pavel arrives. Bakhmetyeva smells a strong smell of fumes from the intern. She declares that Pavel has been demoted to the orderlies for three days, and drives him away.
A husband comes to Meridiana. Upon learning that the child was born with an incurable pathology, the oligarch declares: we are breaking up, you will receive everything that is written in the contract. And the child? We have a healthy child in the contract.