Emotional abuse during pregnancy
Abuse During Pregnancy – Envision
Pregnancy can be a dangerous time for women and the children of women who are abused. Studies show that many women report that the abuse starts or increases during their pregnancy. There are many ways that an abusive partner can exert power and control over their partner before, during and after pregnancy.
Once a woman is pregnant, the abuser may:
- Force her to have an abortion
- Injure her with the intent of causing her to lose the baby
- Force her to continue an unwanted pregnancy
Statistics
- Pregnant women have a higher risk of experiencing violence during pregnancy than they do of experiencing problems such as high blood pressure, gestational diabetes or premature rupture of membranes.
- The incidence of violence in pregnancy may range from 4% to 17%. These figures may significantly underestimate the problem, as many women do not report their experiences of violence.
- Of women who had ever been married, were 18 years of age or over and who reported violence during pregnancy by a marital partner, 40% reported that it began while they were pregnant.
- 21% of women abused by a current or previous partner were assaulted during pregnancy.
- Women who were abused during pregnancy were four times as likely as other abused women to say they experienced very serious violence (beating, choking, gun/knife threats, sexual assault).
Abuse often begins or increases during pregnancy because of different reasons, such as:
- the woman focuses attention to her unborn child
- the woman receives attention from others
- other partner is no longer the center of attention
- she is too tired or ill to take care of the needs of the other in the way they demand
During pregnancy, the abuser may:
- start, continue or change the pattern of abuse
- control, limit, delay or deny her access to prenatal care
- use her pregnancy as a weapon for emotional abuse
- refusing sex on grounds that her pregnant body appears unattractive
- denying that the child is theirs
- refusing to support her emotionally throughout the pregnancy
- financially abuse her by refusing her access to money to buy food and supplies
- restrict her access to food
- threaten to leave her or report her to Social Services as an unfit mother
- force her to work beyond her endurance during pregnancy
The abusive partner most often directs their physical assaults at the women’s breasts, abdomen and/or genital area. The emotional responses triggered by abuse, such as anxiety, depression, drug use, sleeplessness, and reduced appetite can have health risks for a pregnant woman and her developing baby. Abuse during pregnancy can cause direct or indirect injury to the fetus.
The emotional responses triggered by abuse, such as anxiety, depression, drug use, sleeplessness, and reduced appetite can have health risks for a pregnant woman and her developing baby. Abuse during pregnancy can cause direct or indirect injury to the fetus.
The abuse can result in:
- miscarriage
- stillbirth
- separation of the placenta
- broken bones in the fetus
- preterm labour
- premature rupture of the membranes, increasing the risk of infection and preterm delivery
- hemorrhage in the fetus
- low birth-weight
During labour and birth, the abuser may:
- refuse to support her
- try to control decision-making around the use of pain medication or other interventions
- demand that doctors restore the woman’s vagina to the “way it was before” the birth
After the baby is born, the abuser may:
- increase the amount of abuse
- begin using the woman’s relationship with her baby as part of the abuse by:
- denying her access to her newborn child
- not supporting her or helping her when she comes home with the baby
- demanding sex soon after childbirth
- blaming her because the infant is the “wrong sex”
- sulking or trying to make her feel bad for time spent with the baby
- criticizing her parenting ability
- threatening to or abducting the baby
- telling her she will never get custody
- making her stay home with the baby
- prevent her from getting a job or make her take a job
- making, or threatening to make, false child abuse accusations to Social Services against her
- withholding money for supplies for the baby such as formula, food, diapers
- blaming her for the baby’s crying or other problems
- not allowing her to bathe or perform personal hygiene
- threatening to take the baby/other children and leave
- not allowing her to feed the baby during the night
Help is available for women who are being abused. Counselling for survivors can help you process what you’ve been through and learn how to build new and healthy relationships. There are also transition houses located throughout Saskatchewan for abused women and her children to find safety.
Counselling for survivors can help you process what you’ve been through and learn how to build new and healthy relationships. There are also transition houses located throughout Saskatchewan for abused women and her children to find safety.
Remember…
- You do not deserve to be abused.
- No one has the right to hurt you or your unborn child.
- You and your unborn child have a right to be free from the abuse.
- You can learn to take care of yourself and your children.
- There is help available. Please do not be afraid to ask for help.
Abuse during pregnancy | March of Dimes
Abuse, whether emotional or physical, is never okay. Unfortunately, some women experience abuse from a partner. Abuse crosses all racial, ethnic and economic lines. Abuse often gets worse during pregnancy. The American College of Obstetricians and Gynecologists (also called ACOG) says that 1 in 6 abused women is first abused during pregnancy. More than 320,000 women are abused by their partners during pregnancy each year.
More than 320,000 women are abused by their partners during pregnancy each year.
What is abuse?
Abuse can come in many forms. An abusive partner may cause emotional pain by calling you names or constantly blaming you for something you haven't done. An abuser may try to control your behavior by not allowing you to see your family and friends, or by always telling you what you should be doing. Emotional abuse may lead you to feel scared or depressed, eat unhealthy foods, or pick up bad habits such as smoking or drinking.
An abusive partner may try to hurt your body. This physical abuse can include hitting, slapping, kicking, choking, pushing or even pulling your hair. Sometimes, an abuser will aim these blows at a pregnant woman's belly. This kind of violence not only can harm you, but it also can put your unborn baby in grave danger. During pregnancy, physical abuse can lead to miscarriage and vaginal bleeding. It can cause your baby to be born too soon, have low birthweight or physical injuries.
What can trigger abuse during pregnancy?
For many families, pregnancy can bring about feelings of stress, which is normal. But it's not okay for your partner to react violently to stress. Some partners become abusive during pregnancy because they feel:
- Upset because this was an unplanned pregnancy
- Stressed at the thought of financially supporting a first baby or another baby
- Jealous that your attention may shift from your partner to your new baby, or to a new relationship
How do you know if you’re in an abusive relationship?
It's common for couples to argue now and then. But violence and emotional abuse are different from the minor conflicts that couples have.
Ask yourself:
- Does my partner always put me down and make me feel bad about myself?
- Has my partner caused harm or pain to my body?
- Does my partner threaten me, the baby, my other children or himself?
- Does my partner blame me for his actions? Does he tell me it's my own fault he hit me?
- Is my partner becoming more violent as time goes on?
- Has my partner promised never to hurt me again, but still does?
If you answered "Yes" to any of these questions, you may be in an unhealthy relationship.
What can you do?
Recognize that you are in an abusive relationship. Once you realize this, you've made the first step towards help. There are lots of things you can do.
Tell someone you trust. This can be a friend, a clergy member, a health care provider or counselor. Once you've confided in them, they might be able to put you in touch with a crisis hotline, domestic violence program, legal-aid service, or a shelter or safe haven for abused women.
Have a plan for your safety. This can include:
- Learn the phone number of your local police department and health care provider's office in case your partner hurts you. Call 911 if you need immediate medical attention. Be sure to obtain a copy of the police or medical record should you choose to file charges against the abuser.
- Find a safe place. Talk to a trusted friend, neighbor or family member that you can stay with, no matter what time of day or night, to ensure your safety.
- Put together some extra cash and any important documents or items you might need, such as a driver's license, health insurance cards, a checkbook, bank account information, Social Security cards and prescription medications. Have these items in one safe place so you can take them with you quickly.
- Pack a suitcase with toiletries, an extra change of clothes for you and your children, and an extra set of house and car keys. Give the suitcase to someone you trust who can hold it for you safely.
Remember: No one deserves to be physically or emotionally abused. Recognize the signs of abuse and seek help. You might feel very scared at the thought of leaving, but you've got to do it. You and your baby's life depends on it.
More information
- National domestic violence hotline: (800) 799-SAFE (7233) or (800) 787-3224 TTY
Domestic violence against pregnant mothers was linked to the deterioration of the intelligence of their children
British scientists found that domestic violence against a pregnant woman is associated with a deterioration in the mental abilities of her child. Children whose mothers were abused had an IQ that was 3 to 5 percent below normal. At the same time, indicators suffered more from physical abuse of the mother than from psychological abuse, scientists write in the journal Wellcome Open Research .
Children whose mothers were abused had an IQ that was 3 to 5 percent below normal. At the same time, indicators suffered more from physical abuse of the mother than from psychological abuse, scientists write in the journal Wellcome Open Research .
Partner violence is still widespread even in developed countries. At least as far back as 2013, the WHO reported that 23 percent of women in high-income countries experienced violence. If a woman is pregnant, then not only she herself suffers, but also her child. It is known, for example, that stress during pregnancy can lead to a variety of consequences for the fetus - from preterm birth to neurological abnormalities. However, there is little research on how violence against a mother during pregnancy is related to the cognitive abilities of her child.
A team of scientists led by Richard Emsley of King's College London set out to estimate how many British women are being abused and to see how it affects the intelligence of their children.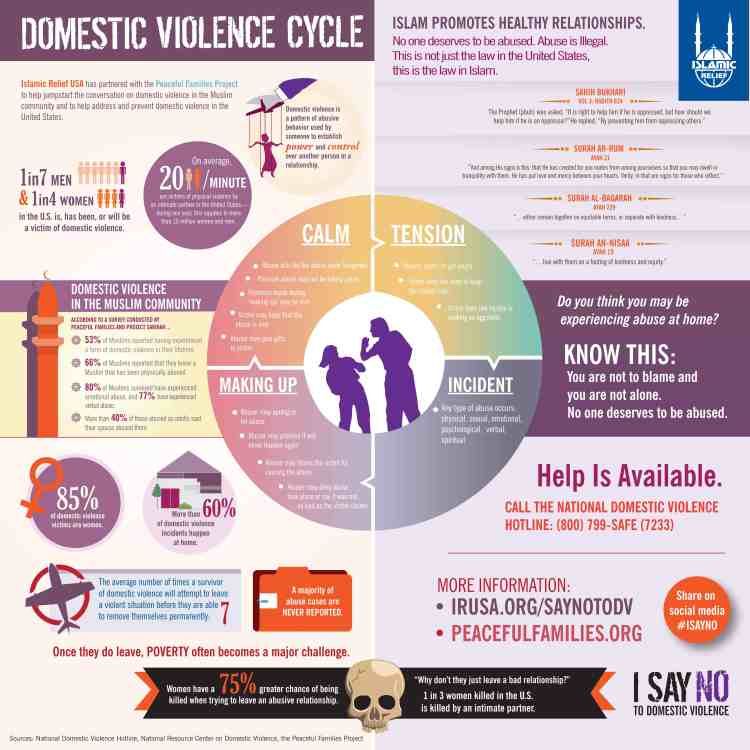
Scientists worked with data from the Avon Longitudinal Study of Parents and Children (ALSPAC). Of the 14,000 women who were pregnant in 1990–1992, 3,153 were selected who gave birth to one child, provided information about domestic violence, and agreed to have a child under 18 examined. The researchers assessed the level of intelligence of children using the Wechsler Intelligence Scale, a multi-level test that includes testing working memory, speech perception, understanding visual information and other skills.
18.6 percent of the women interviewed said they experienced violence between the start of pregnancy and up to six years after giving birth. At the same time, 17.6 percent reported psychological violence, and 6.8 percent physical. The researchers controlled for parental demographics and socioeconomic status, alcohol consumption and smoking during pregnancy, and maternal depression as side variables in evaluating the association between maternal abuse and child cognitive ability.
The researchers then counted the number of children with below average intelligence (less than 90 points) at age 8 in both groups. Among women who were not abused, 13 percent of children had below average general intelligence, 9.9 percent verbal intelligence, and 20.4 percent performative intelligence. Those who reported violence had 16.8, 12.1 and 25.6 percent, respectively. At the same time, physical violence, apparently, turned out to be more traumatic than psychological: from the first, children lost an average of 5.6 points compared to their peers, and from the second - 2.9 points..
In this way, scientists have demonstrated that the problem of domestic violence is still relevant in the UK and can even affect the mental abilities of the children of victims of women. However, the authors of the work note that not all cases of violence could be identified - due to the fact, for example, that women were afraid to talk about it or forgot when exactly it happened, so the real numbers may be different (most likely even more).
In 2018, scientists recorded a drop in the average level of intelligence - at least in Norway. Now there are technologies that allow you to choose a future child with the highest possible cognitive abilities based on genetic tests - however, as it turned out, they do not give a big win, and their accuracy is low. And about how intelligence is connected with other characteristics of a person, for example, appearance or love of music, we talked about in the material "Stop being clever."
Polina Loseva
Found a typo? Select the fragment and press Ctrl+Enter.
Psycho-emotional state of women with spontaneous pregnancy and after the use of assisted reproductive technologies
HEALTH OF WOMAN. 2019.10(146): 10–15; doi 10.15574/HW.2019.146.10
Benyuk V. A., Vigovskaya L. N., Maidannik I. V., Oleshko V. F.
National Medical University. A.A. Bogomolets, Kyiv
The article highlights the relationship of psychological processes that accompany physiological changes in the body of a pregnant woman. After all, pregnancy is a state of functional tension of all systems and organs of a woman. Of course, increased stress is reflected in the psychological state of the pregnant woman.
After all, pregnancy is a state of functional tension of all systems and organs of a woman. Of course, increased stress is reflected in the psychological state of the pregnant woman.
From the point of view of psychology, during pregnancy, a woman undergoes certain successive psychological changes - the decision to continue the pregnancy, the period of pregnancy before the movement of the fetus, the period after the onset of movement, the prenatal period and childbirth.
According to a literature review, each trimester of pregnancy has a certain psychological "portrait" of a pregnant woman. So, in the first trimester, many women are characterized by an increase in psychological passivity and the appearance of a sense of satisfaction and pleasure, other women note a feeling of depression and increased physical activity associated with the realization of the very fact of pregnancy.
The second trimester of pregnancy is characterized by the normalization of the mental state and increased efficiency. However, it is precisely at this time that a restructuring takes place in the system of worldview and the formation of motherhood motivation, and the appearance of fetal movements allows concretizing the image of the child and provides a basis for interpreting his subjective state.
However, it is precisely at this time that a restructuring takes place in the system of worldview and the formation of motherhood motivation, and the appearance of fetal movements allows concretizing the image of the child and provides a basis for interpreting his subjective state.
The third trimester of pregnancy is characterized by an increase in the level of anxiety and anxiety - fear of childbirth, regarding the health of the unborn child and an increase in the frequency of depressive disorders. Activity during this period is aimed at preparing for childbirth and the postpartum period, and activity not related to the birth of a child is reduced.
The prenatal period is characterized by a decrease in the activity of the pregnant woman, general relaxation and emotional "exhaustion", which protects the mother and child from unnecessary stress and worries. In a pregnant woman, the fear of childbirth decreases and the ability to concentrate on only one dominant essence increases, which will be extremely necessary during childbirth and postpartum interaction with the child.
The postpartum period is characterized by an adaptation to the feeling of emptiness and a feeling of inner emptiness.
The psychological state is of leading importance in carrying a pregnancy. Some researchers point out that it is impossible to explain preterm birth only in terms of physiological and chemical changes during pregnancy.
Taking into account a number of physiological changes in the psychological sphere of women with spontaneous onset of pregnancy, an analysis of the psychological state of 249 was carried outpregnant women after the use of assisted reproductive technologies and 50 pregnant women with spontaneous pregnancy.
A study of the psycho-emotional state of pregnant women after the use of assisted reproductive technologies revealed deviations in the level of personal and reactive anxiety that are inherent in women after the use of assisted reproductive technologies. With this in mind, we consider it appropriate to involve a psychologist in work with pregnant women after the use of assisted reproductive technologies in order to correct the identified deviations.
Key words: pregnancy, assisted reproductive technologies, psychological state, personal anxiety, reactive anxiety.
BIBLIOGRAPHY
1. Ayvazyan E.B. The development of a woman's bodily and emotional experience during pregnancy: Diss. … cand. psychol. Sciences. - M., 2005. - 319 p.
2. Bodyazhina V.I., Semenchenko I.B. (2005). Obstetrics [proc. allowance for medical students. colleges] / Ed. 4th. - Rostov-on-Don: Phoenix. - 477 p.
3. Broipgigam W., Christian I., Rad M. (1999). Psychosomatic medicine / Per. With him. – M.: Geotar medicine. – S. 295–310.
4. Brutman V.I., Varga A.Ya., Rodionova M.S. (1998). The study of the states of consciousness at various stages of the reproductive period of women. Social and mental health of the child and family: protection, assistance, return to life. - M. - S. 142-143.
5. Brutman V.I., Varga A.Ya. , Khamitova I.Yu. (2000). Influence of family factors on the formation of deviant behavior of the mother // Psychological journal. 2:48–57.
, Khamitova I.Yu. (2000). Influence of family factors on the formation of deviant behavior of the mother // Psychological journal. 2:48–57.
6. Brutman V.I., Pankratova M.G., Enikolonov S.N. (1995). Unwanted pregnancy of victims of sexual violence (psychological and psychiatric aspects) // Questions of psychology. 1:33–39.
7. Brutman V.I., Filippova G.G., Khamitova I.Yu. (2002). Dynamics of the psychological state of women during pregnancy and after childbirth // Questions of psychology. 6:49–57.
8. Volodin N.N. (2009). Perinatal psychology and psychiatry. - M.: Publishing Center "Academy". – 364 p.
9. Gusev A.N., Izmailov C.A., Mikhalevskaya M.B. (1997). Measurement in psychology: general psychological practice. - M.: "Meaning", 1997. - 280 p.
10. Grigorieva E.S. (2011). The role of a woman's personality traits in the occurrence of pregnancy pathology (a review of modern research). Psychology of corporeality: Theoretical and practical research. 4:177-185.
Psychology of corporeality: Theoretical and practical research. 4:177-185.
11. Dermanova I.B. (2002). Anxiety research (C.D. Spielberger, adaptation by Yu.L. Khanin). Diagnostics of emotional and moral development. - St. Petersburg. - S. 124-126.
12. Dobryakov I.V., Prokhorov V.N., Prokhorova O.V. (2016). Psychological diagnostics in perinatal psychology. Diagnostics in medical (clinical) psychology: current state and prospects / Collective monograph. - S. 118-132.
13. Dobryakov I.V. (2011). Perinatal psychology. - "Peter", 1st edition. - 272 p.
14. Eltsova-Strelkova V.I. (1987). Obstetrics (textbook) / Ed. E.V. Mareev. – M.: Ed. UDN. – 301 s.
15. Zalevsky G.V., Mamysheva N.L., Shelekhov I.L. (2005). Individual psychological characteristics of pregnant women in the prediction of the formation of deviant forms of maternal behavior. Siberian Journal of Psychology. 22:7–12.
16. Karaseva A.E., Kiselev V.D., Fadeeva N.I. (2001). Psychological features of women with a diagnosis of weakness of the birth forces // Obstetrics and Gynecology. 1:44-45.
Karaseva A.E., Kiselev V.D., Fadeeva N.I. (2001). Psychological features of women with a diagnosis of weakness of the birth forces // Obstetrics and Gynecology. 1:44-45.
17. Kopyl O.A., Baz L.L., Bazhenova O.V. (1994). Readiness for motherhood: identification of factors and conditions of psychological risk for the future development of the child // Zhurn. Synapse. 5:27–38.
18. Kochneva M.A. (1992). Features and role of mental reactions of pregnant women in the development of complicated pregnancy and childbirth: Dis. … cand. honey. Sciences. - M. - 191 s.
19. Krechetov A.B., Abramchenko V.V. (1968). On some neuropsychic reactions in pregnant women and women in childbirth // Journal of Neurology and Psychiatry named after Korsakov. 7:7-18.
20. Leskov G.A., Piskunova T.V., Zhabina T.P. (1992). Assessment of the level of neuroticism and psychopathization in women in the department of pathology of the reproductive function of women. - S-P. – S. 104–06.
- S-P. – S. 104–06.
21. Misyuk M.N., Kovalenko E.S. (2008). Anxiety and fears as a manifestation of the emotional sphere of pregnant women. Management in social and economic systems: materials of the XVII International Scientific and Practical Conference (June 2–6, 2008, Minsk) // Minsk Int. management; redol. - Minsk. - S. 413-414.
22. Noskova O.V. (2008). Features of the anxiety state of women during pregnancy and its psychocorrection // Medical psychology. 3:52-56.
23. Pines D. Unconscious use of her body by a woman. - S-P.: Ed. East European Institute of Psychoanalysis, 1997. - 196 p.
24. Plotnikov V.V., Mironova T.A., Kazarenko L.L. (1996). Psychophysiological factors in miscarriage. History of Saburova dacha: Advances in psychiatry, neurology, neurosurgery and narcology / Collection of scientific works of the Ukrainian Research Institute of Clinical and Experimental Neurology and Psychiatry and Kharkiv City Clinical Psychiatric Hospital No.