Contraindications of tens
Transcutaneous Electrical Nerve Stimulation - StatPearls
Dac Teoli; Jason An.
Author Information
Last Update: October 31, 2022.
Continuing Education Activity
Transcutaneous electrical nerve stimulation, known by its acronym TENS, is a modality that uses electric current to activate nerves in order to decrease pain. The TENS unit is a small device, often battery-operated, which can sometimes even fit into a pocket. It utilizes electrodes placed on the skin and which connect to the unit via wires to address pain in a target region. Pregnancy, epilepsy, and pacemaker are all contraindications for TENS. This activity describes the indications, contraindications, and clinical significance of transcutaneous electrical nerve stimulation and highlights the role of the interprofessional team in the management of pain.
Objectives:
Summarize the indications for transcutaneous electrical nerve stimulation.
Explain how transcutaneous electrical nerve stimulation reduces pain.
Recall the complications of transcutaneous electrical nerve stimulation.
Discuss interprofessional team strategies for improving care coordination and communication to advance the control of pain and improve outcomes.
Access free multiple choice questions on this topic.
Introduction
Transcutaneous electrical nerve stimulation, known by its acronym TENS, is a modality that uses electric current to activate nerves for therapeutic reasons. The TENS unit is a small device, often battery-operated, which can sometimes even fit into a pocket. It utilizes electrodes placed on the skin and which connect to the unit via wires to address a targeted therapeutic goal. The units are said to be titratable, permitting for a high degree of user tolerance with few side effects. Compared to many medications, the device is free from the risk of overdose. TENS units are often highly adjustable, allowing the user to control pulse width, intensity, and frequency. Low frequency of < 10Hz in conjunction with high intensity is used to produce muscle contractions. High frequencies of > 50 Hz are used with low intensity to produce paresthesia without muscle contractions. Overall, the concept of TENS throughout history has been the topic of vigorous debate within scientific circles in regards to efficacy. However, while this modality of pain management has proven itself in clinical investigations, there remains to this day disagreement over which pain syndromes and conditions TENS is appropriate.
TENS units are often highly adjustable, allowing the user to control pulse width, intensity, and frequency. Low frequency of < 10Hz in conjunction with high intensity is used to produce muscle contractions. High frequencies of > 50 Hz are used with low intensity to produce paresthesia without muscle contractions. Overall, the concept of TENS throughout history has been the topic of vigorous debate within scientific circles in regards to efficacy. However, while this modality of pain management has proven itself in clinical investigations, there remains to this day disagreement over which pain syndromes and conditions TENS is appropriate.
TENS, in its earliest conceptual form, is believed to date back to approximately 60 A.D. The Roman physician Scribonius Largus proposed symptomatic relief to patients by having the patient be exposed and in contact with an "electric fish" from the ocean. There are also ancient records of the use of electric eels for their pain management benefits — the use of electricity in managing human ailments propagated over time. By the 18th century, there were numerous devices developed to deliver electrostatic exposures with the belief of treating a wide array of conditions, from headaches to cancer, with even Benjamin Franklin being an eventual supporter.
By the 18th century, there were numerous devices developed to deliver electrostatic exposures with the belief of treating a wide array of conditions, from headaches to cancer, with even Benjamin Franklin being an eventual supporter.
The 19th century started with one particular machine, the "Electreat," leading the way in clinical therapeutic usage of electricity in managing patient disease. However, it had several constraints including large size and limited adjustments. It has been long since abandoned.
The TENS units and functionality as we think of it today are credited to American neurosurgeon Dr. C. Norman Shealy. After completing medical school at Duke University in North Carolina, he had additional training out of Barnes-Jewish Hospital and Massachusetts General Hospital. He spent several years subsequently researching spinal cord stimulators and transcutaneous electrical nerve stimulation, developing what developed into today's TENS units. His early work was an effort to arrive at an impactful therapy for several types of pain including migraines, back pain, and gout.
As the study of transcutaneous electrical nerve stimulation advanced, there came new techniques inherent to the modality, such as intense TENS, acupuncture TENS, and conventional TENS.[1][2][3][4]
Anatomy and Physiology
TENS is believed to be effective by selectively delivering an activating stimuli to large diameter non-noxious afferents (A-beta) which subsequently reduces pain (via decreased nociceptor activity) and unwanted sensation.[5][6]
Indications
The fundamental indication for TENS is seeking to manage pain, both acute and chronic. There is an overall divide across scientific literature regarding the efficacy of TENS application for particular types of pain or pain conditions. While a significant body of work exists which suggests that TENS is effective for neuropathic, nociceptive, and musculoskeletal pain, a notable portion of these studies were noted for methodological concerns.
A look at the three types of TENS is outlined below along with their conceptual indications.
Intense TENS is used primarily as a "counter-irritant." Aiming to target small diameter, high threshold cutaneous afferent (A-delta), this type of TENS specifically seeks to block transmission of nociceptive information in nerves while stimulating other analgesic mechanisms. Both high frequencies and intensities are used for short periods of time.
Acupuncture-like TENS (AL-TENS) is an approach at hyperstimulation and often used in patients that do not respond to conventional TENS. Titration is to low-frequency, higher intensity, longer pulse width. AL-TENS aims to stimulate small diameter, high threshold peripheral afferent (A-delta).
Conventional TENS utilizes high-frequency, low-intensity, small pulse width. The goal is to stimulate selectively large diameter, low threshold non-noxious afferent (A-beta). This approach enjoys use in the treatment of dermatomal pain distributions.[5][7][8]
Contraindications
Pregnancy, epilepsy, and pacemaker are all contraindications for TENS. Additionally, contraindications exist to the placement of the electrode pads in certain areas. Some of these placements include: over the eyes, trans-cerebrally, the front of the neck, simultaneously positioned anterior and posterior chest electrodes, internally, over broken skin or lesions, over tumors, directly over the spine, regions of severe paresthesia where the user might not recognize skin irritation.[6][9]
Additionally, contraindications exist to the placement of the electrode pads in certain areas. Some of these placements include: over the eyes, trans-cerebrally, the front of the neck, simultaneously positioned anterior and posterior chest electrodes, internally, over broken skin or lesions, over tumors, directly over the spine, regions of severe paresthesia where the user might not recognize skin irritation.[6][9]
Technique
It is imperative to read the manufacturer's instruction booklet, as each unit might have slight variances in recommendations. TENS units are now small and lightweight. Patients can place them in their pocket, on a desk, or hold them. Treatment sessions can take place at the convenience of the patient except while operating heavy machinery, driving, bathing, showering, or swimming. The unit should be powered off before placing the pads. Electrode pad placement is at least 1 inch apart in the appropriate dermatomal region of the targeted pain. The skin underlying pad placement must have intact sensation. After powering on the unit, the setting titration is to manufacturer recommendations. Red and black lead placement have little impact on clinical outcomes.[8]
After powering on the unit, the setting titration is to manufacturer recommendations. Red and black lead placement have little impact on clinical outcomes.[8]
Complications
Overall, for the vast majority of people, TENS is believed to be safe and well-tolerated with little to no side effects. However, manufacturers of TENS units universally warn individuals with pacemakers, epilepsy, or are pregnant that these conditions are contraindications to use as they can lead to potential complications. Nevertheless, this has been viewed as more of a medicolegal maneuver in high-risk populations, and TENS units are actually usable in these groups assuming close medical supervision and electrode placement is not in close vicinity to the chest, neck, or abdomen.
Furthermore, there have been some complications with impacting transdermal drug delivery systems if drug application is close to the TENS electrodes.
There have been documented dermatologic complications from using TENS units — the most of these cases relate to either allergic reactions to the electrode pads or contact dermatitis. Special hypoallergenic electrode pads are available for this population. Additionally, syncope and nausea have both been documented as complications of transcutaneous electrical nerve stimulation.
Special hypoallergenic electrode pads are available for this population. Additionally, syncope and nausea have both been documented as complications of transcutaneous electrical nerve stimulation.
Lastly, there are theoretical risks with using TENS units while driving or operating heavy machinery, so it is therefore recommended to avoid TENS during those activities to avoid the risk of further complication.[9][10]
Clinical Significance
There is no universal consensus concerning the efficacy of TENS in managing pain. However, there are indeed a number of studies which have found a positive impact on patients with an overall low risk of complications/side effects when using TENS appropriately and according to manufacturer instructions. As such, combining TENS with pharmacotherapy remains a worthwhile endeavor for interested patients willing to try the modality. More research needs to take place to arrive at a definitive position on the place of TENS in pain management. One characteristic that has universal agreement, however, is that if TENS does provide results, those are short-term in nature and rapid in onset and offset. TENS is not a cure for pain conditions or syndromes.
One characteristic that has universal agreement, however, is that if TENS does provide results, those are short-term in nature and rapid in onset and offset. TENS is not a cure for pain conditions or syndromes.
The positive impact in which TENS has on an individual might diminish over time. Habituation might even lead to a worsening of pain. Recommendations are that patients take breaks from treatment and vary their placement of electrode pads over time.[8][11]
Enhancing Healthcare Team Outcomes
TENS units are available in many different clinical settings. Practitioners utilize them in hospice and palliative care, pain management, orthopedic surgery, neurology, dentistry, chiropractic, and physical therapy. Units have found use in hospitals, clinics, and homes alike. However, before the first TENS treatment, individuals should have a formal pain assessment by an experienced and qualified professionals, as well as given full and clear instructions on how to use the TENS unit. It is just as important to review the medical conditions and contraindicated electrode pad placements. Instructions should be thorough, but easy to understand. The patient should undergo a monitored session of TENS therapy by a trained provider so that they can evaluate for adherence to and comprehension of directions, placement, and titrating the machine. Conventional TENS is the approach first used in individuals new to the modality, often with a continuous pulse pattern of midrange frequencies and durations.[12][6] An interprofessional team approach involving the nurse, allied health professional, and clinician in educating the patient and family and providing follow up will elicit the best results. [Level V]
It is just as important to review the medical conditions and contraindicated electrode pad placements. Instructions should be thorough, but easy to understand. The patient should undergo a monitored session of TENS therapy by a trained provider so that they can evaluate for adherence to and comprehension of directions, placement, and titrating the machine. Conventional TENS is the approach first used in individuals new to the modality, often with a continuous pulse pattern of midrange frequencies and durations.[12][6] An interprofessional team approach involving the nurse, allied health professional, and clinician in educating the patient and family and providing follow up will elicit the best results. [Level V]
Review Questions
Access free multiple choice questions on this topic.
Comment on this article.
Figure
TENS (Transcutaneous Electrical Nerve Stimulator). Contributed by Wikimedia Commons (CC by 2.0) https://creativecommons. org/licenses/by/2.0/
org/licenses/by/2.0/
References
- 1.
Francis J, Dingley J. Electroanaesthesia--from torpedo fish to TENS. Anaesthesia. 2015 Jan;70(1):93-103. [PubMed: 25348076]
- 2.
Kasat V, Gupta A, Ladda R, Kathariya M, Saluja H, Farooqui AA. Transcutaneous electric nerve stimulation (TENS) in dentistry- A review. J Clin Exp Dent. 2014 Dec;6(5):e562-8. [PMC free article: PMC4312687] [PubMed: 25674327]
- 3.
Slavin KV. History of peripheral nerve stimulation. Prog Neurol Surg. 2011;24:1-15. [PubMed: 21422772]
- 4.
Johnson MI, Jones G. Transcutaneous electrical nerve stimulation: current status of evidence. Pain Manag. 2017 Jan;7(1):1-4. [PubMed: 27641909]
- 5.
Gibson W, Wand BM, O'Connell NE. Transcutaneous electrical nerve stimulation (TENS) for neuropathic pain in adults. Cochrane Database Syst Rev. 2017 Sep 14;9(9):CD011976. [PMC free article: PMC6426434] [PubMed: 28905362]
- 6.

Sluka KA, Walsh D. Transcutaneous electrical nerve stimulation: basic science mechanisms and clinical effectiveness. J Pain. 2003 Apr;4(3):109-21. [PubMed: 14622708]
- 7.
Johnson M. Transcutaneous electrical nerve stimulation: review of effectiveness. Nurs Stand. 2014 Jun 10;28(40):44-53. [PubMed: 24894255]
- 8.
Johnson MI, Paley CA, Howe TE, Sluka KA. Transcutaneous electrical nerve stimulation for acute pain. Cochrane Database Syst Rev. 2015 Jun 15;2015(6):CD006142. [PMC free article: PMC8094447] [PubMed: 26075732]
- 9.
Miller MA, Palaniswamy C, Sharma D, Reddy VY. Inappropriate shock from a subcutaneous implantable cardioverter-defibrillator due to transcutaneous electrical nerve stimulation. Heart Rhythm. 2015 Jul;12(7):1702-3. [PubMed: 25889810]
- 10.
Jauregui JJ, Cherian JJ, Gwam CU, Chughtai M, Mistry JB, Elmallah RK, Harwin SF, Bhave A, Mont MA. A Meta-Analysis of Transcutaneous Electrical Nerve Stimulation for Chronic Low Back Pain.
 Surg Technol Int. 2016 Apr;28:296-302. [PubMed: 27042787]
Surg Technol Int. 2016 Apr;28:296-302. [PubMed: 27042787]- 11.
Khadilkar A, Odebiyi DO, Brosseau L, Wells GA. Transcutaneous electrical nerve stimulation (TENS) versus placebo for chronic low-back pain. Cochrane Database Syst Rev. 2008 Oct 08;2008(4):CD003008. [PMC free article: PMC7138213] [PubMed: 18843638]
- 12.
Young JD, Spence AJ, Power G, Behm DG. The Addition of Transcutaneous Electrical Nerve Stimulation with Roller Massage Alone or in Combination Did Not Increase Pain Tolerance or Range of Motion. J Sports Sci Med. 2018 Dec;17(4):525-532. [PMC free article: PMC6243624] [PubMed: 30479519]
Transcutaneous Electrical Nerve Stimulation - StatPearls
Dac Teoli; Jason An.
Author Information
Last Update: October 31, 2022.
Continuing Education Activity
Transcutaneous electrical nerve stimulation, known by its acronym TENS, is a modality that uses electric current to activate nerves in order to decrease pain. The TENS unit is a small device, often battery-operated, which can sometimes even fit into a pocket. It utilizes electrodes placed on the skin and which connect to the unit via wires to address pain in a target region. Pregnancy, epilepsy, and pacemaker are all contraindications for TENS. This activity describes the indications, contraindications, and clinical significance of transcutaneous electrical nerve stimulation and highlights the role of the interprofessional team in the management of pain.
The TENS unit is a small device, often battery-operated, which can sometimes even fit into a pocket. It utilizes electrodes placed on the skin and which connect to the unit via wires to address pain in a target region. Pregnancy, epilepsy, and pacemaker are all contraindications for TENS. This activity describes the indications, contraindications, and clinical significance of transcutaneous electrical nerve stimulation and highlights the role of the interprofessional team in the management of pain.
Objectives:
Summarize the indications for transcutaneous electrical nerve stimulation.
Explain how transcutaneous electrical nerve stimulation reduces pain.
Recall the complications of transcutaneous electrical nerve stimulation.
Discuss interprofessional team strategies for improving care coordination and communication to advance the control of pain and improve outcomes.
Access free multiple choice questions on this topic.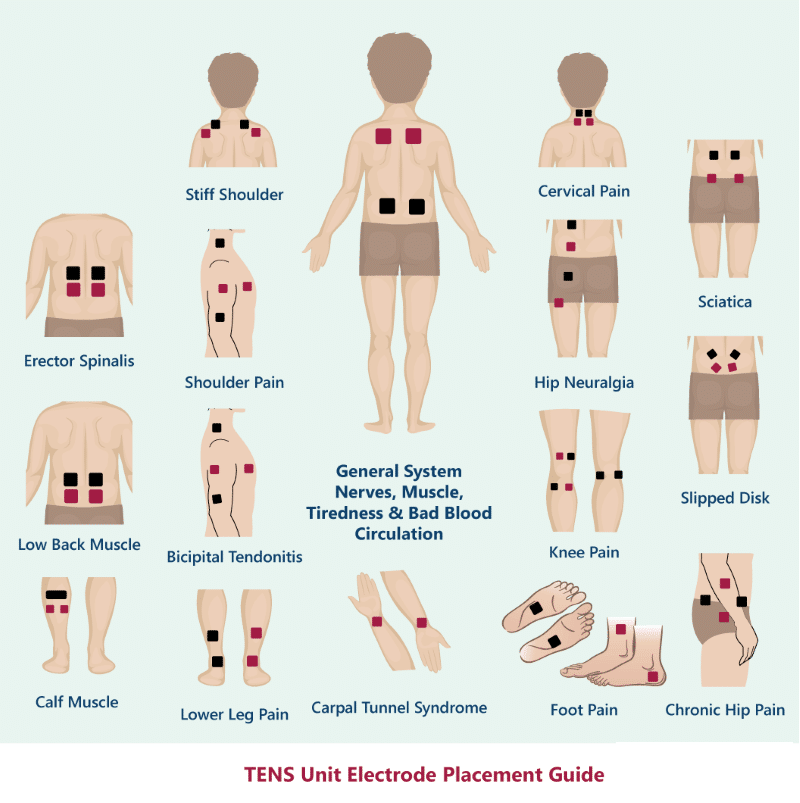
Introduction
Transcutaneous electrical nerve stimulation, known by its acronym TENS, is a modality that uses electric current to activate nerves for therapeutic reasons. The TENS unit is a small device, often battery-operated, which can sometimes even fit into a pocket. It utilizes electrodes placed on the skin and which connect to the unit via wires to address a targeted therapeutic goal. The units are said to be titratable, permitting for a high degree of user tolerance with few side effects. Compared to many medications, the device is free from the risk of overdose. TENS units are often highly adjustable, allowing the user to control pulse width, intensity, and frequency. Low frequency of < 10Hz in conjunction with high intensity is used to produce muscle contractions. High frequencies of > 50 Hz are used with low intensity to produce paresthesia without muscle contractions. Overall, the concept of TENS throughout history has been the topic of vigorous debate within scientific circles in regards to efficacy. However, while this modality of pain management has proven itself in clinical investigations, there remains to this day disagreement over which pain syndromes and conditions TENS is appropriate.
However, while this modality of pain management has proven itself in clinical investigations, there remains to this day disagreement over which pain syndromes and conditions TENS is appropriate.
TENS, in its earliest conceptual form, is believed to date back to approximately 60 A.D. The Roman physician Scribonius Largus proposed symptomatic relief to patients by having the patient be exposed and in contact with an "electric fish" from the ocean. There are also ancient records of the use of electric eels for their pain management benefits — the use of electricity in managing human ailments propagated over time. By the 18th century, there were numerous devices developed to deliver electrostatic exposures with the belief of treating a wide array of conditions, from headaches to cancer, with even Benjamin Franklin being an eventual supporter.
The 19th century started with one particular machine, the "Electreat," leading the way in clinical therapeutic usage of electricity in managing patient disease. However, it had several constraints including large size and limited adjustments. It has been long since abandoned.
The TENS units and functionality as we think of it today are credited to American neurosurgeon Dr. C. Norman Shealy. After completing medical school at Duke University in North Carolina, he had additional training out of Barnes-Jewish Hospital and Massachusetts General Hospital. He spent several years subsequently researching spinal cord stimulators and transcutaneous electrical nerve stimulation, developing what developed into today's TENS units. His early work was an effort to arrive at an impactful therapy for several types of pain including migraines, back pain, and gout.
As the study of transcutaneous electrical nerve stimulation advanced, there came new techniques inherent to the modality, such as intense TENS, acupuncture TENS, and conventional TENS.[1][2][3][4]
Anatomy and Physiology
TENS is believed to be effective by selectively delivering an activating stimuli to large diameter non-noxious afferents (A-beta) which subsequently reduces pain (via decreased nociceptor activity) and unwanted sensation. [5][6]
Indications
The fundamental indication for TENS is seeking to manage pain, both acute and chronic. There is an overall divide across scientific literature regarding the efficacy of TENS application for particular types of pain or pain conditions. While a significant body of work exists which suggests that TENS is effective for neuropathic, nociceptive, and musculoskeletal pain, a notable portion of these studies were noted for methodological concerns.
A look at the three types of TENS is outlined below along with their conceptual indications.
Intense TENS is used primarily as a "counter-irritant." Aiming to target small diameter, high threshold cutaneous afferent (A-delta), this type of TENS specifically seeks to block transmission of nociceptive information in nerves while stimulating other analgesic mechanisms. Both high frequencies and intensities are used for short periods of time.
Acupuncture-like TENS (AL-TENS) is an approach at hyperstimulation and often used in patients that do not respond to conventional TENS. Titration is to low-frequency, higher intensity, longer pulse width. AL-TENS aims to stimulate small diameter, high threshold peripheral afferent (A-delta).
Conventional TENS utilizes high-frequency, low-intensity, small pulse width. The goal is to stimulate selectively large diameter, low threshold non-noxious afferent (A-beta). This approach enjoys use in the treatment of dermatomal pain distributions.[5][7][8]
Contraindications
Pregnancy, epilepsy, and pacemaker are all contraindications for TENS. Additionally, contraindications exist to the placement of the electrode pads in certain areas. Some of these placements include: over the eyes, trans-cerebrally, the front of the neck, simultaneously positioned anterior and posterior chest electrodes, internally, over broken skin or lesions, over tumors, directly over the spine, regions of severe paresthesia where the user might not recognize skin irritation.[6][9]
Technique
It is imperative to read the manufacturer's instruction booklet, as each unit might have slight variances in recommendations. TENS units are now small and lightweight. Patients can place them in their pocket, on a desk, or hold them. Treatment sessions can take place at the convenience of the patient except while operating heavy machinery, driving, bathing, showering, or swimming. The unit should be powered off before placing the pads. Electrode pad placement is at least 1 inch apart in the appropriate dermatomal region of the targeted pain. The skin underlying pad placement must have intact sensation. After powering on the unit, the setting titration is to manufacturer recommendations. Red and black lead placement have little impact on clinical outcomes.[8]
Complications
Overall, for the vast majority of people, TENS is believed to be safe and well-tolerated with little to no side effects. However, manufacturers of TENS units universally warn individuals with pacemakers, epilepsy, or are pregnant that these conditions are contraindications to use as they can lead to potential complications. Nevertheless, this has been viewed as more of a medicolegal maneuver in high-risk populations, and TENS units are actually usable in these groups assuming close medical supervision and electrode placement is not in close vicinity to the chest, neck, or abdomen.
Furthermore, there have been some complications with impacting transdermal drug delivery systems if drug application is close to the TENS electrodes.
There have been documented dermatologic complications from using TENS units — the most of these cases relate to either allergic reactions to the electrode pads or contact dermatitis. Special hypoallergenic electrode pads are available for this population. Additionally, syncope and nausea have both been documented as complications of transcutaneous electrical nerve stimulation.
Lastly, there are theoretical risks with using TENS units while driving or operating heavy machinery, so it is therefore recommended to avoid TENS during those activities to avoid the risk of further complication.[9][10]
Clinical Significance
There is no universal consensus concerning the efficacy of TENS in managing pain. However, there are indeed a number of studies which have found a positive impact on patients with an overall low risk of complications/side effects when using TENS appropriately and according to manufacturer instructions. As such, combining TENS with pharmacotherapy remains a worthwhile endeavor for interested patients willing to try the modality. More research needs to take place to arrive at a definitive position on the place of TENS in pain management. One characteristic that has universal agreement, however, is that if TENS does provide results, those are short-term in nature and rapid in onset and offset. TENS is not a cure for pain conditions or syndromes.
The positive impact in which TENS has on an individual might diminish over time. Habituation might even lead to a worsening of pain. Recommendations are that patients take breaks from treatment and vary their placement of electrode pads over time.[8][11]
Enhancing Healthcare Team Outcomes
TENS units are available in many different clinical settings. Practitioners utilize them in hospice and palliative care, pain management, orthopedic surgery, neurology, dentistry, chiropractic, and physical therapy. Units have found use in hospitals, clinics, and homes alike. However, before the first TENS treatment, individuals should have a formal pain assessment by an experienced and qualified professionals, as well as given full and clear instructions on how to use the TENS unit. It is just as important to review the medical conditions and contraindicated electrode pad placements. Instructions should be thorough, but easy to understand. The patient should undergo a monitored session of TENS therapy by a trained provider so that they can evaluate for adherence to and comprehension of directions, placement, and titrating the machine. Conventional TENS is the approach first used in individuals new to the modality, often with a continuous pulse pattern of midrange frequencies and durations.[12][6] An interprofessional team approach involving the nurse, allied health professional, and clinician in educating the patient and family and providing follow up will elicit the best results. [Level V]
However, before the first TENS treatment, individuals should have a formal pain assessment by an experienced and qualified professionals, as well as given full and clear instructions on how to use the TENS unit. It is just as important to review the medical conditions and contraindicated electrode pad placements. Instructions should be thorough, but easy to understand. The patient should undergo a monitored session of TENS therapy by a trained provider so that they can evaluate for adherence to and comprehension of directions, placement, and titrating the machine. Conventional TENS is the approach first used in individuals new to the modality, often with a continuous pulse pattern of midrange frequencies and durations.[12][6] An interprofessional team approach involving the nurse, allied health professional, and clinician in educating the patient and family and providing follow up will elicit the best results. [Level V]
Review Questions
Access free multiple choice questions on this topic.

Comment on this article.
Figure
TENS (Transcutaneous Electrical Nerve Stimulator). Contributed by Wikimedia Commons (CC by 2.0) https://creativecommons.org/licenses/by/2.0/
References
- 1.
Francis J, Dingley J. Electroanaesthesia--from torpedo fish to TENS. Anaesthesia. 2015 Jan;70(1):93-103. [PubMed: 25348076]
- 2.
Kasat V, Gupta A, Ladda R, Kathariya M, Saluja H, Farooqui AA. Transcutaneous electric nerve stimulation (TENS) in dentistry- A review. J Clin Exp Dent. 2014 Dec;6(5):e562-8. [PMC free article: PMC4312687] [PubMed: 25674327]
- 3.
Slavin KV. History of peripheral nerve stimulation. Prog Neurol Surg. 2011;24:1-15. [PubMed: 21422772]
- 4.
Johnson MI, Jones G. Transcutaneous electrical nerve stimulation: current status of evidence. Pain Manag. 2017 Jan;7(1):1-4. [PubMed: 27641909]
- 5.
Gibson W, Wand BM, O'Connell NE. Transcutaneous electrical nerve stimulation (TENS) for neuropathic pain in adults.
 Cochrane Database Syst Rev. 2017 Sep 14;9(9):CD011976. [PMC free article: PMC6426434] [PubMed: 28905362]
Cochrane Database Syst Rev. 2017 Sep 14;9(9):CD011976. [PMC free article: PMC6426434] [PubMed: 28905362]- 6.
Sluka KA, Walsh D. Transcutaneous electrical nerve stimulation: basic science mechanisms and clinical effectiveness. J Pain. 2003 Apr;4(3):109-21. [PubMed: 14622708]
- 7.
Johnson M. Transcutaneous electrical nerve stimulation: review of effectiveness. Nurs Stand. 2014 Jun 10;28(40):44-53. [PubMed: 24894255]
- 8.
Johnson MI, Paley CA, Howe TE, Sluka KA. Transcutaneous electrical nerve stimulation for acute pain. Cochrane Database Syst Rev. 2015 Jun 15;2015(6):CD006142. [PMC free article: PMC8094447] [PubMed: 26075732]
- 9.
Miller MA, Palaniswamy C, Sharma D, Reddy VY. Inappropriate shock from a subcutaneous implantable cardioverter-defibrillator due to transcutaneous electrical nerve stimulation. Heart Rhythm. 2015 Jul;12(7):1702-3. [PubMed: 25889810]
- 10.
Jauregui JJ, Cherian JJ, Gwam CU, Chughtai M, Mistry JB, Elmallah RK, Harwin SF, Bhave A, Mont MA.
 A Meta-Analysis of Transcutaneous Electrical Nerve Stimulation for Chronic Low Back Pain. Surg Technol Int. 2016 Apr;28:296-302. [PubMed: 27042787]
A Meta-Analysis of Transcutaneous Electrical Nerve Stimulation for Chronic Low Back Pain. Surg Technol Int. 2016 Apr;28:296-302. [PubMed: 27042787]- 11.
Khadilkar A, Odebiyi DO, Brosseau L, Wells GA. Transcutaneous electrical nerve stimulation (TENS) versus placebo for chronic low-back pain. Cochrane Database Syst Rev. 2008 Oct 08;2008(4):CD003008. [PMC free article: PMC7138213] [PubMed: 18843638]
- 12.
Young JD, Spence AJ, Power G, Behm DG. The Addition of Transcutaneous Electrical Nerve Stimulation with Roller Massage Alone or in Combination Did Not Increase Pain Tolerance or Range of Motion. J Sports Sci Med. 2018 Dec;17(4):525-532. [PMC free article: PMC6243624] [PubMed: 30479519]
PET CT with gallium | Indications, contraindications and preparation
July 15, 2022
Leader in quality and safety of medical activity in Russia
International accreditation JCI Joint Commission International
PET CT with gallium is a kind of radionuclide diagnostics of cancers at all stages of their progression. Positron emission computed tomography aims to identify the foci of the spread of malignant tumors. The use of gallium in the form of its derivative component "gallium 68" allows you to accurately, accurately and quickly determine oncological diseases of the prostate gland. nine0003
Positron emission computed tomography aims to identify the foci of the spread of malignant tumors. The use of gallium in the form of its derivative component "gallium 68" allows you to accurately, accurately and quickly determine oncological diseases of the prostate gland. nine0003
The use of the radiopharmaceutical Gallium 68 makes it possible to combine all the advantages of PET and computed tomography for a correct diagnosis. This substance, introduced into the body about an hour before the examination, is concentrated in the prostate gland and is visible on the monitor in the form of colored foci. Fiery color indicates the presence of an oncological tumor. In the course of research by positron emission tomography, it becomes possible to obtain the following information: nine0003
- cessation or progression of tumor growth;
- involvement in oncological pathology of lymph nodes;
- the presence of metastases.
The method is used in cases of suspected oncological diseases of the reproductive organs, to control the dynamics of recovery and monitor the effectiveness of the therapeutic course.
Equipment
For diagnostics by PET CT with gallium, modern devices are used: nine0003
- cellular scanners;
- detectors of morphological changes in tissues;
- radiation generators;
- computer tomograph;
- positron emission tomograph.
There are dozens of models and design options for gallium PET CT equipment. Maximum efficiency is demonstrated by equipment operating on Exclusive Evolution technology. nine0003
Readings
An appointment for PET CT with gallium is issued to the patient based on the history, primary diagnosis, clinical examinations and laboratory tests. Reasons for carrying out such diagnostic measures are:
- primary PCa-PSA;
- the results of evaluation on the Gleason scale;
- the presence of tumors in other areas of the body;
- diagnosis of allergic anomalies; nine0013 kidney failure;
- confirmed hyperthyroidism.

Also, the identified disorders of the reproductive function and pathology of the urinary system can serve as indications. These include hematuria, nocturia, pain during ejaculation, erectile dysfunction and other pathologies.
Gallium PET CT is recommended 4-6 weeks after surgery or a course of chemotherapy. 2 weeks must pass before the examination after the course of PCT. After the last radiotherapy treatment, at least 6-8 weeks should elapse. nine0003
Contraindications
Significant restrictions on the conduct of positron emission computed tomography have not been established. At the same time, the features of the procedure sometimes exclude the possibility of its implementation. Since the patient will have to lie still for about 40 minutes, it is not recommended to perform PET CT with gallium in such cases:
- psychosomatic disorders in a patient;
- renal failure in the process of exacerbation; nine0014
- pregnancy in any trimester.

Also, contraindications apply to children under the age of 3-5 years, who will not be able to remain calm and the desired body position during the procedure. For older children, sanitation can be used for this, introducing a state of rest and sleep.
Study preparation
Before starting the examination, you need to get rid of metal objects, do not eat for 6 hours. A few days earlier, you need to take a blood test for creatinine. nine0003
It is also undesirable to overcool the body, at least for two days before the examination. A similar requirement applies to physical overload at work or training - within 24 hours. Before starting the procedure, it is advisable to drink plenty of water for several hours.
FAQ
How long does a PET CT procedure take?
Taking into account the preparation, all diagnostics by this method takes an average of one and a half hours. nine0003
Is gallium PET CT allowed for confirmed oncology?
Yes, this will allow us to more accurately determine the causes of the disease, conduct differential diagnostics, and track the intensity of tumor development.
Are there any side effects?
Since the radiopharmaceutical (gallium) has a short period of existence, the exposure period is limited and does not pose a threat to health. nine0003
WHERE YOU CAN GET THE PROCEDURE:
JSC "Medicina"
You can sign up for the procedure and find out its cost by calling +7 (495) 266-95-40 or during a personal visit to the clinic: Moscow, 2nd Tverskoy-Yamskoy pereulok, 10.
Contraindications to dental implantation - types of contraindications to the installation of dental implants
- Warranty 5 years in the contract nine0013 24/7 in touch with the clinic and the attending physician
- All treatments are carried out under the microscope Carl Zeiss
- Over 6300 happy smiles, thanks and recommendations in 12 years
- The financial plan drawn up at the beginning of treatment does not change until the end, and there are also no hidden fees
5 year warranty according to
agreement
Most dental clinics in the Moscow market give a 1 year warranty. We, TopSmile clinic, are confident in our work and in the contract
We, TopSmile clinic, are confident in our work and in the contract
we prescribe a 5-year guarantee for all types of work. For our patients, there is also a system for extending the five-year warranty to a lifetime one.
Before surgery, each patient undergoes a series of necessary examinations to assess their health status and identify possible contraindications. Implantation is a complex intervention that has clear indications. These include:
| Readings | Contraindications | |
|---|---|---|
| Absolute | Relative | |
| - Single defect (missing one tooth), presence of healthy neighboring teeth - Absence of the last teeth in a row - In the absence of two or three teeth in a row - With complete edentulism - Increased sensitivity of teeth to materials that are part of removable dentures, making them impossible to wear | - Diseases of the central nervous system, including mental - Tuberculosis - HIV infection - Diabetes mellitus - Oncological neoplasms - Severe hypertension, ischemic heart disease, heart failure | - The presence of carious cavities, especially on teeth that are located next to the missing one (it is necessary to sanitize the oral cavity beforehand) - Hard plaque on the teeth - Inflammation of the gums or tissues that are in close proximity to the problem area - Poor oral hygiene (professional cleaning by a dental hygienist is recommended) |
In some cases, the installation of implants does not bring the desired effect: the design does not take root, complications develop, etc. All contraindications are identified during the preliminary examination, the collection of an anamnesis by the doctor, and the study of the medical record. Absolute contraindications are the reason for the refusal of implantation for a long period, more often for life, as they are insurmountable. nine0003
All contraindications are identified during the preliminary examination, the collection of an anamnesis by the doctor, and the study of the medical record. Absolute contraindications are the reason for the refusal of implantation for a long period, more often for life, as they are insurmountable. nine0003
If there is any of the above diseases, which is included in the list of absolute contraindications for surgery, then, together with the dentist, you should choose another method of prosthetics.
There are also relative contraindications for dental implants. If there are any, the procedure is postponed until they are eliminated. These contraindications are eliminated without any problems at the stage of preparation for implantation.
- Specialists advise to pay special attention to oral hygiene for several months in order to minimize the risk of implant rejection and any other complications. nine0014
- A week before the proposed operation, it is undesirable to take any drugs that slow down clotting and thin the blood (these include aspirin, heparin, etc.
 ) They can cause severe bleeding - both during and after surgery. You should tell your doctor about any medications you are taking before surgery.
) They can cause severe bleeding - both during and after surgery. You should tell your doctor about any medications you are taking before surgery.
Implantation and diabetes mellitus
In diabetes mellitus, there is a violation of all types of metabolism, the hormonal background suffers: all this can contribute to the rejection of the implant. Also, in diabetes mellitus, the process of osteosynthesis is disrupted, which makes implantation almost impossible. With the help of modern technologies, it is possible to install implants even in patients with diabetes, but only a doctor should determine the possibility of using this method of restoring the dentition after examination and examination. nine0003
Implantation and pregnancy
During pregnancy, it is recommended to postpone implantation due to possible negative effects from anesthesia. Also, implantation is a certain stress for the body, which a pregnant woman does not need during this period.
Implantation and bad habits
Smoking and alcohol consumption are incompatible with implantation: these bad habits reduce the chances of engraftment. After the operation, it is strongly recommended to minimize smoking for 1-2 weeks so that at least the early period proceeds without complications. The fact is that when smoking and drinking alcohol, the formation of a blood clot is inhibited, which is necessary for the normal healing of tissues and their recovery after surgery. Also, nicotine contributes to vasoconstriction and increased blood pressure, which also adversely affects the effect of implantation. nine0003
After the operation, it is strongly recommended to minimize smoking for 1-2 weeks so that at least the early period proceeds without complications. The fact is that when smoking and drinking alcohol, the formation of a blood clot is inhibited, which is necessary for the normal healing of tissues and their recovery after surgery. Also, nicotine contributes to vasoconstriction and increased blood pressure, which also adversely affects the effect of implantation. nine0003
Possible complications after dental implantation
The most common complication that occurs most often in practice is implant rejection, when it simply does not take root in the bone. This rarely happens, especially if all contraindications are eliminated. If the implant does not take root, then the doctor removes it and installs a new design in its place.
After implantation, complications may occur if medical recommendations are not followed in good faith. Inflammatory foci may form around the implant, sometimes its intraosseous parts are exposed.