Baby fragile x syndrome
What is Fragile X Syndrome: A Guide for Parents
Fragile X syndrome (FXS) is one of the more common known causes of intellectual disability that can run in families (inherited). FXS is caused by a change in the genetic material in each cell of the body. This change in genetic material makes it hard for cells to produce a protein that is necessary for normal brain development and normal brain function. As an inherited condition, FXS can be passed on to the next generation.
FXS Symptoms:
People with FXS may have some or all of the following symptoms:
- Walking, talking, or toilet training later than other children of the same age
- Problems with learning
- Trouble making eye contact
- Frequent ear infections
- Trouble sleeping
- Seizures
- Autism
- Sensory difficulties (trouble with what a person sees, hears, smells, tastes, and touches)
Currently there is no cure for FXS, but an early diagnosis can help a family get treatment and services for their child sooner, and having a diagnosis may provide valuable information for other family members.
Myth Busters for Families:
MYTH: I thought my child was tested for FXS when I was pregnant or after my child was born?
MYTH: I thought girls couldn't have FXS, and boys always have severe symptoms.
MYTH: Does everyone with FXS have large ears or a long, narrow face?
FACT: Many people with FXS do not have certain physical traits that textbooks attribute to FXS. However, some people with FXS do have some of these physical features. These features can be seen in younger children, but some may not show up until puberty.
MYTH: If there is no cure for FXS, why does my child need a diagnosis?
FACT: Even though there is no cure for FXS, there are educational, behavioral, and therapeutic services which can help. A diagnosis may also help families with family planning and connecting with support groups of other families affected by FXS.
MYTH: How can my child have FXS? We don't have a family history of FXS.
FACT: FXS is caused by a change in genetic material that ranges in size, and can become bigger from one generation to the next. Small size changes typically do not cause FXS, but large size changes often do cause FXS. Therefore, a person can have FXS without a family history if that person inherits a large change in the size of the genetic material while everyone else in the family has small size changes. Families who do not have FXS but have small size changes can have other signs that FXS could occur in future generations. These families have members that may have fragile X-associated disorder symptoms, such as tremors and early menopause, which could be identified through a more thorough evaluation of family history.
What to Do If You Think Your Child Might Have FXS:
Talk to your doctor about genetic testing if your child is not sitting, walking, or talking at the same time as other children the same age, has trouble learning new skills, or has social and behavioral problems like not making eye contact, anxiety, trouble paying attention, hand flapping, acting and speaking without thinking, and being very active.
Talk to your family to see if anyone remembers a history of "Parkinson-like" tremors in older men on the mother's side of the family, or a history of early menopause or fertility problems in women on the mother's side of the family. These are symptoms of fragile X-associated disorders, which suggest that FXS could run in the family.
What to Do If Your Child Has Been Diagnosed with FXS:
Early intervention services in each state help children from birth to 3 years old learn important skills. You can ask to have your child evaluated, and these services may improve your child's development. Even if your child has not been diagnosed with FXS, he or she may still be eligible for services.
Work with your child's pediatrician to get care and services for your child.
Contact the organizations who work with FXS families and become familiar with FXS resources.
Consider joining a local group of FXS families to share information and support each other.
Additional Information & Resources:
Fragile X Syndrome Myth Busters for Patients & Families (PDF)
Children with Intellectual Disabilities
Ethical and Policy Issues in Genetic Testing and Screening of Children (AAP Policy Statement)
Health Supervision for Children with Fragile X Syndrome (AAP Policy Statement)
National Fragile X Foundation
FRAXA Research Foundation
Centers for Disease Control and Prevention
This document was supported by the Cooperative Agreement Number 5 U38 OT000183-02, funded by the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
- Last Updated
- 5/25/2016
- Source
- American Academy of Pediatrics Fragile X Syndrome Expert Group
The information contained on this Web site should not be used as a substitute for the medical care and advice of your pediatrician.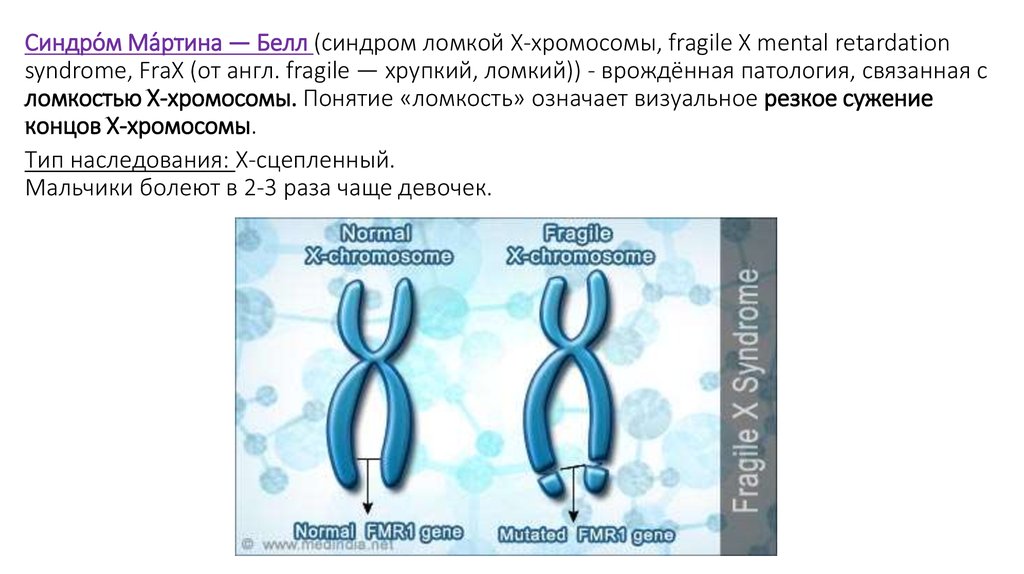 There may be variations in treatment that your pediatrician may recommend based on individual facts and circumstances.
There may be variations in treatment that your pediatrician may recommend based on individual facts and circumstances.
Fragile X syndrome – symptoms and support
Fragile X syndrome – symptoms and support | Pregnancy Birth and Baby beginning of content7-minute read
Listen
Key facts
- Fragile X is the most common inherited cause of intellectual disability, and also the most common genetic cause of autism.
- It is caused by a faulty gene in one of your X chromosomes.
- Symptoms of fragile X syndrome include speech and language delays, intellectual disabilities and learning difficulties, as well as behavioural and emotional problems.
- Fragile X is diagnosed with a genetic test. Genetic testing can be done prior to or during pregnancy.

- Fragile X has no cure, but there are effective treatments.
What is fragile X syndrome?
Fragile X syndrome gets its name from the X chromosome — 1 of the 2 chromosomes that determine your sex at the time of conception. Chromosomes carry DNA (deoxyribose nucleic acid). A gene is a small section of that DNA and contains the chemical information for our inherited characteristics. Sometimes, the X chromosome develops a fault — its DNA changes or mutates.
People can be carriers of this faulty gene without having any symptoms, while others will be born with symptoms of fragile X syndrome.
Fragile X syndrome is more common and more severe in males than in females. This is because males have one X chromosome and one Y chromosome, so if they have a mutation on their X chromosome, they will not have any functioning copies of the fragile X gene. Females have two X chromosomes, so even if they carry the fragile X mutation, they will usually have one functioning copy of the gene on their other X chromosome.
People with fragile X syndrome have intellectual disability, behavioural and learning difficulties, as well as certain physical characteristics. Fragile X syndrome is the most common inherited cause of intellectual disability, and also the most common genetic cause of autism.
It affects around 1 in 3600 males and around 1 in 6000 females.
What are the symptoms of fragile X syndrome?
Some people with fragile X have very few symptoms, while others have significant health problems. The main symptoms of fragile X syndrome are:
- speech and language delays
- intellectual disabilities and learning difficulties
- physical features such as low muscle tone
- problems with coordination
- a heart murmur
People with fragile X syndrome may also have behavioural and emotional problems including:
- shyness, aggression and mood swings
- attention deficit hyperactivity disorder (ADHD) or autism spectrum disorder
- anxiety and related problems such as obsessive-compulsive disorder
Females with fragile X syndrome or who carry the gene might experience early menopause.
Male carriers (and occasionally females) might experience fragile X tremor ataxia syndrome. The symptoms are similar to those of Parkinson’s disease and include unsteadiness (ataxia), intention tremor (shaking) and memory problems.
How do I know if I am a carrier for fragile X?
If you have a family history of fragile X, you can be tested before becoming pregnant to see if you are a carrier of the gene for fragile X. If you are a carrier, there is a chance that you can pass the gene on to your children.
Even if you don’t have a family history of fragile X, you can still do a genetic test to find out if you are a carrier for the condition.
If you are a carrier of the fragile X gene, a genetic counsellor can help you explore ways of having a healthy baby.
Can fragile X syndrome be detected during pregnancy?
If you are a known carrier for fragile X, your baby can be tested in pregnancy using amniocentesis or chorionic villous sampling.
If your baby is found to have fragile X, you will need to decide whether to continue with the pregnancy or consider a termination. Your doctor can refer you to a genetic counsellor who specialises in helping people in your situation. You can also call Pregnancy, Birth and Baby for advice and support.
Your doctor can refer you to a genetic counsellor who specialises in helping people in your situation. You can also call Pregnancy, Birth and Baby for advice and support.
What if my child has fragile X syndrome?
If you have a child of any age showing symptoms of fragile X syndrome, your doctor can ask for a DNA blood test to see if they have the condition. Having a diagnosis can help your child get the help they need.
It can be overwhelming to receive a diagnosis of fragile X syndrome. It’s a good idea to think about seeking support from family or friends as you process the diagnosis.
It’s a good idea to find out as much as you can about fragile X syndrome. The The Fragile X Association of Australia provides information and real-life stories about living with this condition.
There is no cure for fragile X but there are effective treatments for problems your child may experience. You can help your child reach their potential by getting them help as soon as possible after diagnosis. This is called early intervention. A team of different specialists work together to look after your child’s educational, behavioural and medical needs. This team may also include a psychologist to help your family work through some of the difficulties of living with a person with a disability.
This is called early intervention. A team of different specialists work together to look after your child’s educational, behavioural and medical needs. This team may also include a psychologist to help your family work through some of the difficulties of living with a person with a disability.
Raising a child with a disability is not easy, but help is available.
- Call the Carer Gateway on 1800 422 737 for support and services.
- The Fragile X Association has a helpline on 1300 394 636 and provides advice on treatments and early intervention.
Speak to a maternal child health nurse
Call Pregnancy, Birth and Baby to speak to a maternal child health nurse on 1800 882 436 or video call. Available 7am to midnight (AET), 7 days a week.
Sources:
Centre for Genetics Education (Fact sheet 54: Fragile X syndrome), Fragile X association of Australia (How does fragile X syndrome affect people?), Australian Family Physician (Fragile X associated conditions: don’t miss them), Fragile X association of Australia (Testing for fragile X), Fragile X association of Australia (Treatments and early intervention), Fragile X association of Australia (Family support and counselling)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: October 2022
Back To Top
Related pages
- Disability and chronic illness
- What is a congenital disorder?
Need more information?
Fragile X syndrome - Better Health Channel
The facts about fragile X syndrome are complicated, and parents and family members are invited to ask their doctor to refer them to a genetics clinic.
Read more on Better Health Channel website
Fragile X syndrome in children | Raising Children Network
Fragile X syndrome causes intellectual disability and other challenges. Early intervention and support helps children with Fragile X explore their abilities.
Read more on raisingchildren.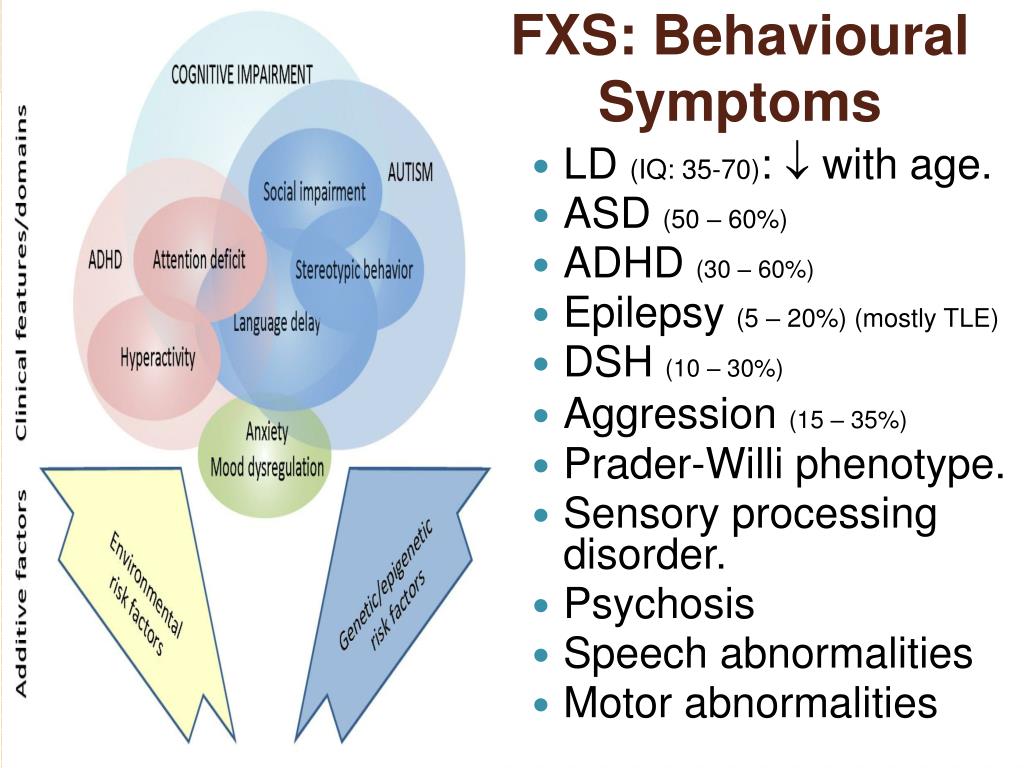 net.au website
net.au website
What is a childhood disability?
Learn more about childhood disabilities such as congenital disorders, disabilities developed after birth and disabilities caused by injury.
Read more on Pregnancy, Birth & Baby website
How pathology helps IVF parents get pregnant | Know Pathology Know Healthcare
For IVF parents, pathology testing is vital from fertility tests before conception to ensuring a healthy pregnancy
Read more on Know Pathology Know Healthcare website
Pregnancy tests amniocentesis - Better Health Channel
Amniocentesis is a prenatal procedure performed on a pregnant woman to withdraw a small amount of amniotic fluid from the sac surrounding the fetus.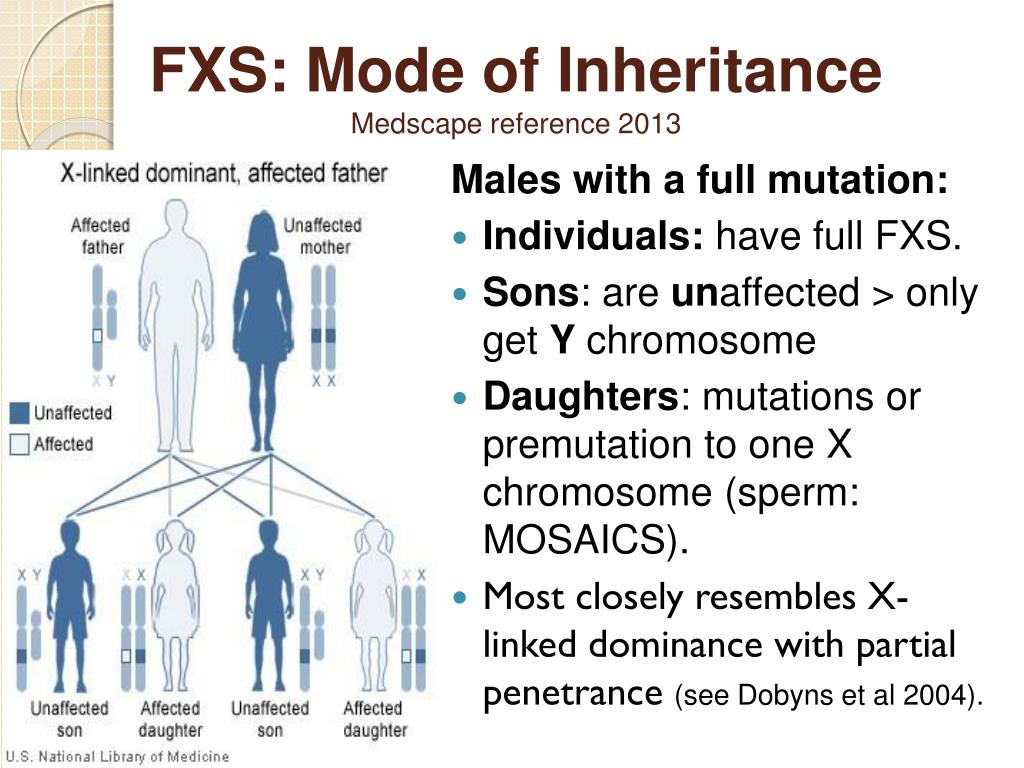
Read more on Better Health Channel website
Genetic counselling
Genetic counselling may be recommended for people who have a history of hereditary disorders. Find out when genetic counselling can be helpful and what to expect.
Read more on Pregnancy, Birth & Baby website
Screening for carrier status
Screening for carrier status assesses whether you and your partner carry genes that could mean your baby is born with a health condition. Find out more here about whether the test might be right for you.
Read more on Pregnancy, Birth & Baby website
What is a congenital disorder?
Congenital disorder, also known as congenital disease or birth defects, are conditions present from birth.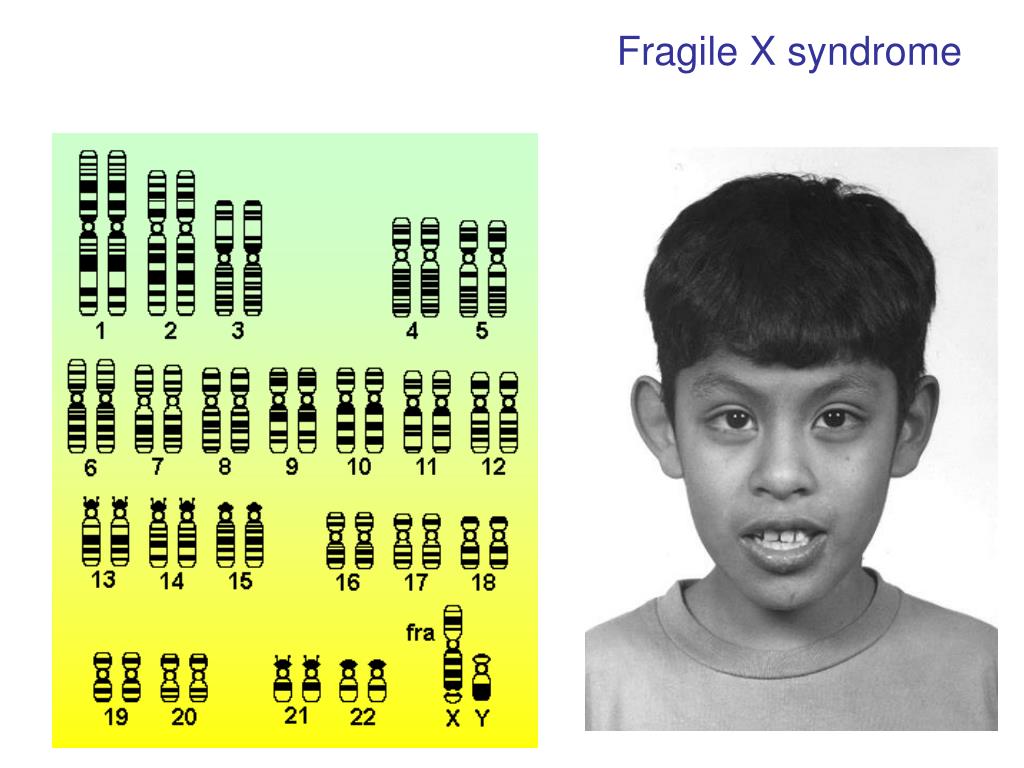 Find out more about congenital disorders.
Find out more about congenital disorders.
Read more on Pregnancy, Birth & Baby website
Intellectual disability | Sydney Children's Hospitals Network
What is intellectual disability? A child with an intellectual disability learns and develops slower than other children
Read more on Sydney Children's Hospitals Network website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Subscribe to newsletters
- Sign in
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.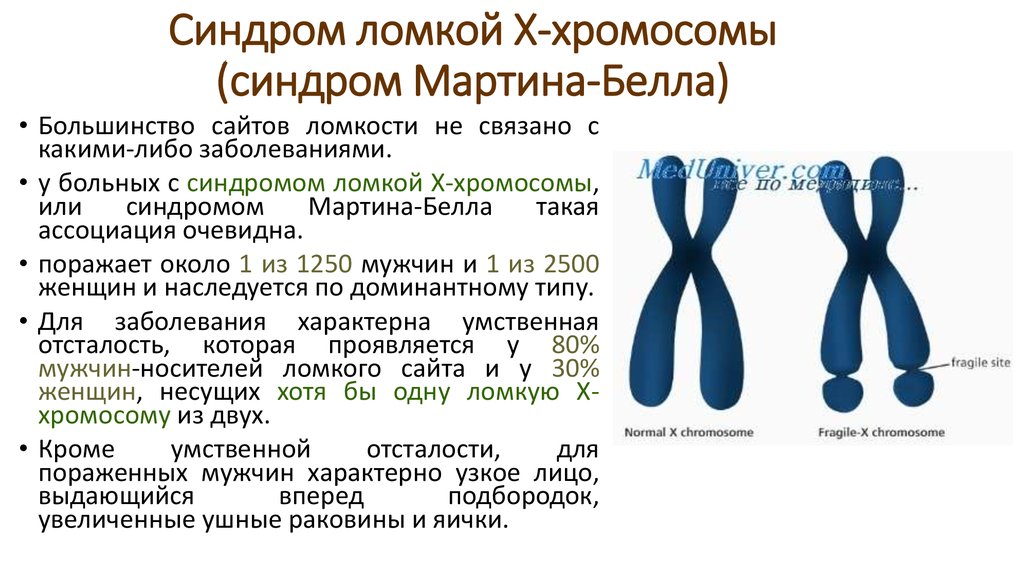
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
Healthdirect Australia acknowledges the Traditional Owners of Country throughout Australia and their continuing connection to land, sea and community. We pay our respects to the Traditional Owners and to Elders both past and present.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Genetic features of fragile X syndrome Genetico Center for Genetics and Reproductive Medicine
March 16, 2017
Among the group of hereditary diseases, there are two diseases related to the most common causes of intellectual disability.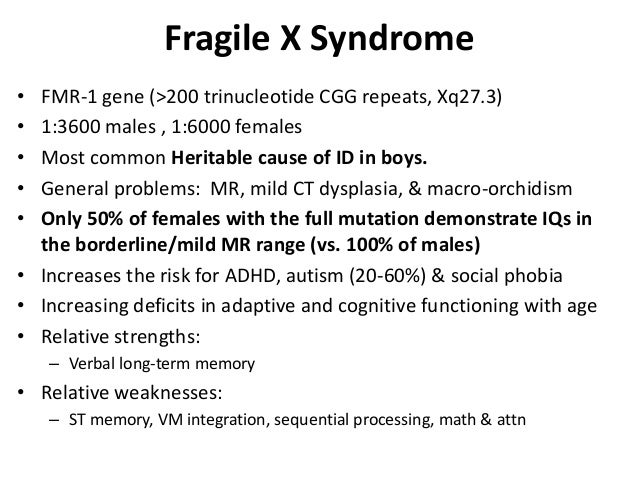 The most famous and most common pathology is Down syndrome, associated with the presence of an extra 21st chromosome in the human genome. In this article, we will talk about the second most common hereditary disease that leads to mental retardation, and may also be accompanied by other clinical manifestations.
The most famous and most common pathology is Down syndrome, associated with the presence of an extra 21st chromosome in the human genome. In this article, we will talk about the second most common hereditary disease that leads to mental retardation, and may also be accompanied by other clinical manifestations.
Fragile X syndrome or Martin-Bell syndrome is the result of a disorder in the FMR1 (fragile X mental retardation-1) gene, which is located on the X chromosome and plays an important role in the emergence and development of neural connections, learning and memory. The frequency of this syndrome among boys is 1:4000.
The so-called “fragility” of the X chromosome is manifested in the fact that the chromosome looks atypical with special staining, as if one piece has separated, although physically it remains intact. The genetic basis for this phenomenon is an increase in the number of CGG trinucleotide repeats in the FMR1 gene located on the X chromosome.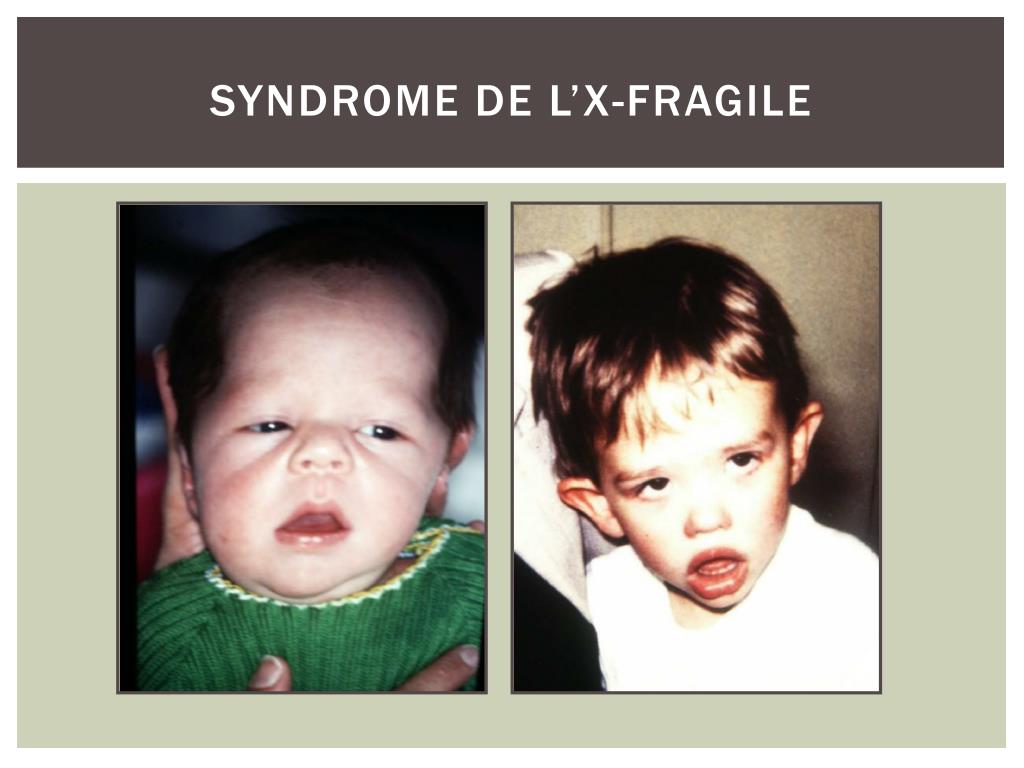
In healthy people, the number of repeats in this gene ranges from 5 to 54. If the repeats are more than 200, then the protein production from the FMR1 gene is disrupted, which leads to the development of Martin-Bell syndrome and the clinical manifestation of the disease. A premutational state is the number of CGG repeats from 55 to 200. In this state, the disease does not typically manifest in humans, but the more repeats a carrier has in this gene, the more likely it is that her or his children will have a repeat count greater than 200. and the disease will develop. In the case of a carrier of a premutation during the formation of germ cells, the number of repeats may increase, therefore, if the parent has a number of repeats from 55 to 200, then the probability of having a child with a mutant FMR1 gene and Martin-Bell syndrome is high. At the same time, the carriage of the premutational state by the future father and mother is not equivalent in terms of the probability of the occurrence of a mutant allele in their children: if the mother is the carrier, then the probability of a significant increase in the number of repeats is much higher.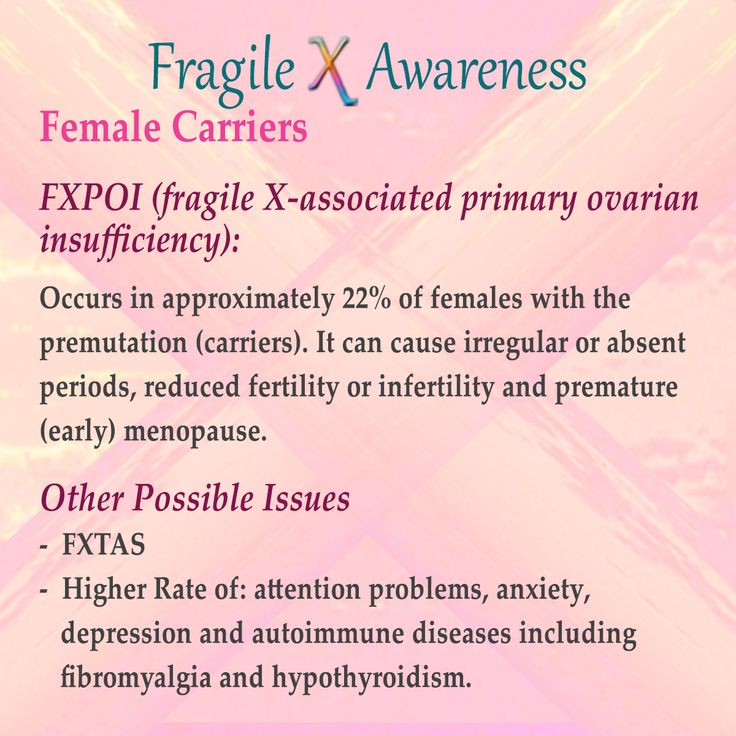 The number of repeats from 45 to 54 is an intermediate form that has no effect on human health, but can lead to problems in future generations, as in the case of a premutational state of the gene.
The number of repeats from 45 to 54 is an intermediate form that has no effect on human health, but can lead to problems in future generations, as in the case of a premutational state of the gene.
It is important to consider that the inheritance and development of the disease depends on gender, since the FMR1 gene is located on the X chromosome. Men have only one X chromosome, which they receive from their mother. Therefore, if this one chromosome turned out to be “fragile”, they have a disease. Women have two X chromosomes, but only one of them is active. Therefore, the presence of one X chromosome with a mutant FMR1 gene may not manifest itself clinically, in the case of inactivation of the “fragile” chromosome, or lead to the development of the disease in 30-50% of cases. A man with a fragile X chromosome can pass it on to all his daughters, but not to any of his sons. A woman with a mutant chromosome has a chance to pass it on to both sons and daughters with equal probability.
The premutation state of a gene affects both the fate of the descendants of the carrier of such a gene and directly on his health:
-
Development of primary ovarian failure (FXPOI) (decrease in ovarian reserve and menopause before age 40). The FMR1 mutation is responsible for premature ovarian failure in 5% of women with this diagnosis. Among carriers of the premutation, about a quarter develop this condition. It affects not only the general reproductive possibilities, but also the selection of the stimulation protocol for ART, as it often causes a poor ovarian response to stimulation. Interestingly, according to Genetico data, although poor ovarian response to stimulation affects the number of embryos produced per cycle, it does not lead to an increase in the proportion of aneuploid embryos.
-
Fragile X tremor/ataxia (FXTAS). This condition develops more often in men: when the premutation is carried by a man, it manifests itself in 33% of cases, and when the premutation is carried by a woman - only in 5-10%.
 FXTAS syndrome begins to manifest in old age. There is a tremor, a wobbly gait, speech may suffer.
FXTAS syndrome begins to manifest in old age. There is a tremor, a wobbly gait, speech may suffer.
The diagnostic method used in the Genetico laboratory is based on the use of a polymerase chain reaction with a special set of primers, which allows not only to detect normal, premutational and mutational states, but also to accurately determine the number of repeats in cases where they are less than 200. This diagnostic allows you to identify Fragile X syndrome at the molecular level, as well as to assess the likelihood of having a child with this syndrome and the possibility of the patient developing disorders associated with an increased number of repeats in the FMR1 gene. Such diagnostics also allows detection of the presence of AGG repeats among CGG repeats. It is believed that AGG regions that interrupt a long sequence of CGG repeats confer DNA stability and reduce the risk of an increase in the number of repeats in the next generation.
A genetic test that determines the number of repeats in the FMR1 gene is recommended primarily for women with premature ovarian failure syndrome or with identified non-random inactivation of the X chromosome (indirect sign), families with sons with intellectual disabilities. Also analysis of the state of the FMR1 gene is required:
Also analysis of the state of the FMR1 gene is required:
1) women with reproductive problems or fertility disorders associated with increased levels of follicle-stimulating hormone (FSH)
2) Patients with intellectual disability and their relatives
3) Those with a family history of Fragile X Syndrome or mental retardation without a definite diagnosis FMR1
5) patients with late-onset tremors and cerebellar ataxia (disorders in muscle coordination due to damage to the brain systems that control muscle movement).
If an asymptomatic carrier of a mutation in the FMR1 gene is detected in a woman, the use of donor oocytes or preimplantation genetic diagnosis (PGD) may be recommended in order to exclude the possibility of the syndrome in a child. It is also important to correctly assess the risk of having a sick child in the case of a premutational state of the FMR1 gene in future parents. In this case, according to the results of the test, it is recommended to consult a geneticist.
Author: Ochir Migyaev
Genetico laboratory intern
NSU molecular biologists looking for the causes of fragile X syndrome
Website Novosibirsk State University July 29, 2015
Website Science in Siberia July 29, 2015
Novosibirsk scientists are conducting unique research to determine the mechanism and causes of a common genetic disease that leads to mental retardation. Now they are trying to establish a comprehensive method for diagnosing the disease, starting from the molecular level in cell cultures and ending with a tomographic analysis of changes occurring in the brain of patients.
NSU lecturer Dmitry Yudkin told the university press service what their research is about, whether it will be possible to develop a comprehensive algorithm for diagnosing the disease, and whether it will be possible to find a new, more effective therapy for patients suffering from this incurable disease.
Dmitry Yudkin – Candidate of Biological Sciences, Senior Lecturer, Novosibirsk State University, lecturer on "Molecular Biology" at the Faculty of Natural Sciences, part-time researcher0054 .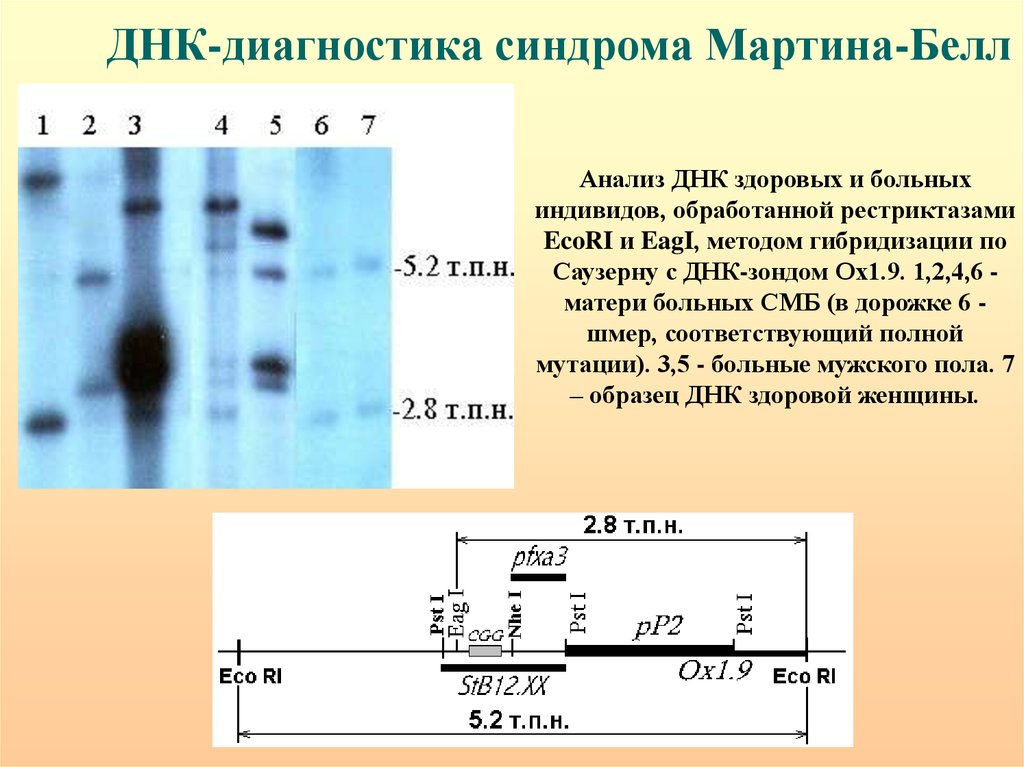 From 2011-2013 he worked at the US National Institutes of Health in Bethesda.
From 2011-2013 he worked at the US National Institutes of Health in Bethesda.
Fragile X syndrome is a very common hereditary disease (approximately one case per 2000-6000 people), for which medicine today does not know either a cure or even a perfect diagnosis.
– We have DNA in our body, some parts of which are repeated many times. However, they must be of a strictly defined size. But sometimes something happens, and one of the repeated areas increases dramatically! Because of this, the work of a gene that is nearby and is responsible for something specific is disrupted. For example, in fragile X syndrome, the repeat located before the beginning of the FMR1 gene increases - the gene starts to work harder, the chromosome becomes fragile, the tip breaks off and some kind of disease develops because of this. Over time, when the repetition becomes even larger, the gene is generally "turned off" completely, which leads to severe changes - up to and including mental retardation, the researcher said.
Medical practice shows that now only symptomatic therapy is applied to patients with such chromosomal abnormalities:
- On the basis of conventional clinics, diagnostics are not carried out to the end - and mainly only by clinical methods. That is, according to the symptoms, doctors put that this is presumably a syndrome of a fragile X chromosome. But no one can say for sure whether this is so until molecular diagnostics are made. Therefore, patients are constantly given folic acid in childhood. That allows them to develop relatively normally and even study a little in special groups, - Dmitry Yudkin explained.
Also, various methods are now used in the world, which lead to the “turning on” of the FMR1 gene back into operation:
- Such studies are carried out on cell cultures, with the addition of certain substances that reactivate the gene. But the main problem with these substances is that they are so toxic that they kill many cells. That is, of course, they "turn on" this gene, but most of the cells die. By the way, another of the areas in which we have already begun work is the search for harmless methods of gene activation in patients.
By the way, another of the areas in which we have already begun work is the search for harmless methods of gene activation in patients.
The team of Dmitry Yudkin and the International Tomography Center of the Siberian Branch of the Russian Academy of Sciences received a grant for a comprehensive study, which is precisely what is not enough for a complete comprehensive diagnosis of this disease.
- What is the point: we will see what happens in patients at the molecular level (what is the size of the repeat, how it has changed, how much it has increased and how the work of the gene has been disrupted), and at the same time the tomographers will do a functional MRI (analyze how the structure of the brain has changed , his work as a whole). That is, patients will perform some simple tasks (see pictures, draw), and at this time, MRI will register how signals are transmitted in the brain. Then we will compare the results of the study with data on healthy people and begin to understand what exactly is broken and why changes in the brain depend on the DNA level.
Scientists plan to solve this problem over the next three years. After this time, they hope to prepare an algorithm for complex diagnostics and a model for the development of the disease.
The biologist notes that they are not only concerned with the problem of this particular disease, they are trying to understand the reasons for the expansion itself (a sharp increase in the number of copies of repetitive sections of the DNA molecule in individuals in subsequent generations of the pedigree) in general:
– The real reason for the expansion is not yet known. For example, researchers have shown in cell cultures that potassium borate in food increases the ability of the repeat to grow. (In America, this substance is added to baked goods in order to make them fluffier). But how much this happens in real life, and not in a Petri dish, is still unknown. We will work in this direction as well.
Dmitry Yudkin believes that fragile X syndrome deserves close attention because of its prevalence:
– We had a problem of access to patients, and when we turned to the Novosibirsk Regional Diagnostic Center, saying that we needed so many people, they said that such volumes were very small by their standards! After all, children with mental retardation are the most common patients in genetic counseling.
It turns out that such statistics could have been avoided if the parents had carried out the necessary tests before pregnancy. According to the scientist, a woman needs to donate blood, since it is she who is the carrier of the disease, which may not affect her, but will be transmitted from her to her son.
“Usually parents go to the hospital after the fact, when the baby already has symptoms of mental retardation (around the age of 3 years), the molecular biologist explains. - When I worked in America, doctors spoke at one of the conferences devoted to this syndrome. They complained that many mothers, even after the birth of a child with symptoms of the disease, do not do the necessary tests, but calmly give birth to a second and even third son - they all turn out to be sick! These are, as a rule, representatives of the poor, uneducated segments of the population ...
Now the sector of chromosomal pathologies has already begun full-fledged work: researchers have begun to work out the first steps in diagnostics on test DNA samples.