Baby born face up myths
What Does It Mean to Have a Sunny Side Up Baby?
Sunny side up sounds intensely cheerful, conjuring images of bright morning breakfasts and summer days. But hearing that the baby you are carrying is positioned for a sunny side up delivery is far less cheerful.
Looking for information brings up stories of induction, intense back labor, and perineal tearing. Suddenly sunny side up doesn’t seem quite so happy.
But not to fear, only 5 to 8 percent of all births are sunny side up. While your baby may not be ideally positioned for birth there is plenty you can do to prepare for — and possibly even avoid — any issues.
Also known as the occiput posterior position (OP), or posterior position, a sunny side up baby is a baby positioned head down but facing mom’s abdomen, so the baby’s occipital bone (the skull) is against the back of your pelvis.
Because a baby birthed vaginally in this position enters the world facing up, the term “sunny side up” is often applied to these deliveries.
After 34 weeks of pregnancy, your prenatal care will include your healthcare practitioner, doctor, or midwife checking the position of your baby. They’ll often estimate the position by simply feeling the outside of your belly, but the most accurate and reliable way to determine the baby’s position is with an ultrasound.
At some point, they may tell you that your baby is in this position.
What about this position makes it less desirable?
In the sunny side up position, the baby’s back is extended along mom’s spine and baby’s chin is lifted, making the head seem larger as it enters the pelvis versus if the baby is in the anterior position. (The head circumference measures larger from the back than it does from the front).
If you learn that your baby is in this position, take a deep breath. It will be okay! You can still have an entirely successful vaginal delivery, despite the additional strain a face-up position may bring.
Also, keep in mind, while many women are told their near-term babies are in this position, most babies naturally move into the preferred anterior position before delivery.
There are several positions that your baby may be in over the course of your pregnancy.
Anterior
The best position for delivery is occiput anterior (OA), or “face-down.” This is also referred to as cephalic presentation. This is when baby is in a head-down position and the body is facing mom’s back. In this position, it is easier for the baby’s back to curl and chin to tuck as it travels through the pelvis.
Breech
If the baby is situated head-up in the mother’s uterus, feet aimed to enter the pelvis first, this is called the breech position. Most babies turn to head down naturally by 34 weeks.
But if the baby hasn’t turned by 36 weeks (when there is little to no room left to wiggle around), your healthcare provider will want to discuss the options for turning the baby and for delivery.
Transverse lie
Extremely rare and also known as the sideways or shoulder position, when the baby is transverse lie, he or she is laying horizontally (crosswise) in the uterus.
This means the baby’s shoulder may enter the pelvis first, causing the baby to potentially sustain more birth trauma. If an examination finds that your baby is still in this position by 38 weeks, your doctor or midwife will discuss the delivery options available for you.
As with everything in life, labor comes with some risks. The sunny side up, or posterior position, puts baby’s head where it is more likely to get wedged against the pubic bone.
When this happens, pressure is placed on your spine and sacrum and can cause a longer and more painful delivery.
The potential complications of a sunny side up delivery include:
- back labor (more pain in the back than in the abdomen)
- prolonged labor and delivery
- severe perineal tearing
- increased risk for assisted vaginal delivery (forceps or vacuum)
- increased need for a cesarean delivery
- start and stop labor pattern
- less engagement from baby during pushing stage
- longer neonatal stay (admission to NICU) in the hospital
If too much strain is placed on you or your baby during labor, your healthcare practitioner, doctor, or midwife will decide if an assisted vaginal delivery or cesarean delivery is necessary.
If you’re nearing full term and your baby is in the occiput posterior position, try not to stress. The human body is capable of many things. Do spend some time discussing the potential risks for both you and your baby in detail with your healthcare provider before agreeing to any procedure.
Pay attention to your body. Your anatomical structure, your posture, and your level of activity all play an important role in how you progress through labor and delivery.
First-time mothers and women with an android pelvis (a narrow pelvic canal) are more likely to have a sunny side up baby. While you can’t change your pelvic shape, you can be aware of possible challenges and discuss options with your doctor.
Likely to be present in taller women, an android shaped pelvis has a heart-shaped or triangular inlet, which can make childbirth more difficult. Unlike women with a gynaecoid pelvis (optimal pelvic shape for having babies), women with an android pelvis typically have to push harder, move around more, and may encounter more labor and delivery difficulties.
Good posture also plays is a key role in how the baby’s position presents at the time of labor and delivery.
Staying in proper alignment while moving your hip and pelvic joints will help the baby move into a more optimal position. To help facilitate a natural rotation of position, stand up straight and keep active. Use an exercise ball instead of a chair (it forces proper alignment). Take a walk around the block.
If you sit for hours throughout the day, keep both feet firmly on the ground, lengthen your spine like a giraffe’s neck, and keep your shoulders back
Once active labor has begun, don’t feel like you have to stay in one laboring position. One 2014 study found that rotation to anterior position is less likely to occur in women who spend at least 50 percent of laboring time in a recumbent position (lying on your back or side).
Women who favor other positions, such as on all fours, squatting, and sitting on a ball, may have a better chance of rotating the baby to an anterior position before delivery. As an added bonus, hands-and-knees positioning, where you’re relieving pressure of the baby pushing against your spine, can help provide pain relief, too.
As an added bonus, hands-and-knees positioning, where you’re relieving pressure of the baby pushing against your spine, can help provide pain relief, too.
It’s possible during labor that your doctor may suggest using forceps or a vacuum when a sunny side up baby gets stuck against the pelvic bone. Some doctors and midwives will even perform manual rotation from a posterior to an anterior position at full dilation.
Every woman, every baby, and every delivery is different.
Despite the difficulties, you can have a healthy vaginal delivery with a sunny side up baby. Working with your healthcare provider and discussing your options is key to your success.
If you have a sunny side up baby, it will be okay! Stay positive.
And don’t forget to stand up straight.
What Does It Mean to Have a Sunny Side Up Baby?
Sunny side up sounds intensely cheerful, conjuring images of bright morning breakfasts and summer days. But hearing that the baby you are carrying is positioned for a sunny side up delivery is far less cheerful.
Looking for information brings up stories of induction, intense back labor, and perineal tearing. Suddenly sunny side up doesn’t seem quite so happy.
But not to fear, only 5 to 8 percent of all births are sunny side up. While your baby may not be ideally positioned for birth there is plenty you can do to prepare for — and possibly even avoid — any issues.
Also known as the occiput posterior position (OP), or posterior position, a sunny side up baby is a baby positioned head down but facing mom’s abdomen, so the baby’s occipital bone (the skull) is against the back of your pelvis.
Because a baby birthed vaginally in this position enters the world facing up, the term “sunny side up” is often applied to these deliveries.
After 34 weeks of pregnancy, your prenatal care will include your healthcare practitioner, doctor, or midwife checking the position of your baby. They’ll often estimate the position by simply feeling the outside of your belly, but the most accurate and reliable way to determine the baby’s position is with an ultrasound.
At some point, they may tell you that your baby is in this position.
What about this position makes it less desirable?
In the sunny side up position, the baby’s back is extended along mom’s spine and baby’s chin is lifted, making the head seem larger as it enters the pelvis versus if the baby is in the anterior position. (The head circumference measures larger from the back than it does from the front).
If you learn that your baby is in this position, take a deep breath. It will be okay! You can still have an entirely successful vaginal delivery, despite the additional strain a face-up position may bring.
Also, keep in mind, while many women are told their near-term babies are in this position, most babies naturally move into the preferred anterior position before delivery.
There are several positions that your baby may be in over the course of your pregnancy.
Anterior
The best position for delivery is occiput anterior (OA), or “face-down. ” This is also referred to as cephalic presentation. This is when baby is in a head-down position and the body is facing mom’s back. In this position, it is easier for the baby’s back to curl and chin to tuck as it travels through the pelvis.
” This is also referred to as cephalic presentation. This is when baby is in a head-down position and the body is facing mom’s back. In this position, it is easier for the baby’s back to curl and chin to tuck as it travels through the pelvis.
Breech
If the baby is situated head-up in the mother’s uterus, feet aimed to enter the pelvis first, this is called the breech position. Most babies turn to head down naturally by 34 weeks.
But if the baby hasn’t turned by 36 weeks (when there is little to no room left to wiggle around), your healthcare provider will want to discuss the options for turning the baby and for delivery.
Transverse lie
Extremely rare and also known as the sideways or shoulder position, when the baby is transverse lie, he or she is laying horizontally (crosswise) in the uterus.
This means the baby’s shoulder may enter the pelvis first, causing the baby to potentially sustain more birth trauma. If an examination finds that your baby is still in this position by 38 weeks, your doctor or midwife will discuss the delivery options available for you.
As with everything in life, labor comes with some risks. The sunny side up, or posterior position, puts baby’s head where it is more likely to get wedged against the pubic bone.
When this happens, pressure is placed on your spine and sacrum and can cause a longer and more painful delivery.
The potential complications of a sunny side up delivery include:
- back labor (more pain in the back than in the abdomen)
- prolonged labor and delivery
- severe perineal tearing
- increased risk for assisted vaginal delivery (forceps or vacuum)
- increased need for a cesarean delivery
- start and stop labor pattern
- less engagement from baby during pushing stage
- longer neonatal stay (admission to NICU) in the hospital
If too much strain is placed on you or your baby during labor, your healthcare practitioner, doctor, or midwife will decide if an assisted vaginal delivery or cesarean delivery is necessary.
If you’re nearing full term and your baby is in the occiput posterior position, try not to stress. The human body is capable of many things. Do spend some time discussing the potential risks for both you and your baby in detail with your healthcare provider before agreeing to any procedure.
The human body is capable of many things. Do spend some time discussing the potential risks for both you and your baby in detail with your healthcare provider before agreeing to any procedure.
Pay attention to your body. Your anatomical structure, your posture, and your level of activity all play an important role in how you progress through labor and delivery.
First-time mothers and women with an android pelvis (a narrow pelvic canal) are more likely to have a sunny side up baby. While you can’t change your pelvic shape, you can be aware of possible challenges and discuss options with your doctor.
Likely to be present in taller women, an android shaped pelvis has a heart-shaped or triangular inlet, which can make childbirth more difficult. Unlike women with a gynaecoid pelvis (optimal pelvic shape for having babies), women with an android pelvis typically have to push harder, move around more, and may encounter more labor and delivery difficulties.
Good posture also plays is a key role in how the baby’s position presents at the time of labor and delivery.
Staying in proper alignment while moving your hip and pelvic joints will help the baby move into a more optimal position. To help facilitate a natural rotation of position, stand up straight and keep active. Use an exercise ball instead of a chair (it forces proper alignment). Take a walk around the block.
If you sit for hours throughout the day, keep both feet firmly on the ground, lengthen your spine like a giraffe’s neck, and keep your shoulders back
Once active labor has begun, don’t feel like you have to stay in one laboring position. One 2014 study found that rotation to anterior position is less likely to occur in women who spend at least 50 percent of laboring time in a recumbent position (lying on your back or side).
Women who favor other positions, such as on all fours, squatting, and sitting on a ball, may have a better chance of rotating the baby to an anterior position before delivery. As an added bonus, hands-and-knees positioning, where you’re relieving pressure of the baby pushing against your spine, can help provide pain relief, too.
It’s possible during labor that your doctor may suggest using forceps or a vacuum when a sunny side up baby gets stuck against the pelvic bone. Some doctors and midwives will even perform manual rotation from a posterior to an anterior position at full dilation.
Every woman, every baby, and every delivery is different.
Despite the difficulties, you can have a healthy vaginal delivery with a sunny side up baby. Working with your healthcare provider and discussing your options is key to your success.
If you have a sunny side up baby, it will be okay! Stay positive.
And don’t forget to stand up straight.
Six Hollywood misconceptions about childbirth
- Lucia Blasco
- BBC News Mundo
Image copyright, Universal Studios/BBC Mundo
Image caption,The character Katherine Heigl in Knocked Up (2007)
Hollywood loves to insert childbirth into its films, portraying the process to its own standards. However, births in American films tend not to be very similar to what actually happens in maternity wards. nine0020
However, births in American films tend not to be very similar to what actually happens in maternity wards. nine0020
Remember the panic-stricken women whose waters began to break so suddenly and at the most inopportune moment, remember the husbands who have no idea how to behave and end up fainting from the experience and unexpected sight - right in the maternity ward ... Such shots can be listed endlessly.
And then, from under a delicately placed sheet, a lovely child with a delightfully cute face is pulled out, staring at the ceiling or at the cameraman's camera. nine0011
Building on the book This is Going to Hurt, in which British physician Adam Key details exactly what happens in the delivery room, and with the help of three other specialists, we dispel six myths about childbirth that have been created and immortalized by the Hollywood Dream Factory.
Image copyright, Getty Images
Image caption,The depiction of childbirth in Hollywood movies can be very different from how it happens in real life
1.
 We are not born face up
We are not born face up During most births, the baby's head emerges first from the vagina. This is what happens in the movies.
However, on the screen, the newborn's face is most often turned up - so that we can see it. In reality, this is not the case.
More than 90% of babies before birth are positioned in the womb head down (so-called head presentation), buttocks up, chin pressed to the chest, and legs and arms bent and pressed to the body.
In this case, the baby's face is turned towards the mother's back, and the camera will not be able to see it at the moment of birth.
Image copyright, Getty Images
Image caption,When we're born, we don't look perfect
"This is the most natural position for a baby during labor - face down or at least sideways," says an OB/GYN in Barcelona Damian Dexeus.
"The reason for this orientation is simple - so the baby takes up less space and feels freer in the womb," he explains. nine0011
nine0011
"In films, babies are often born face up, with their eyes open and even smiling! Of course, this is very unusual," adds the doctor.
Besides, babies are not born as clean as they are portrayed in the movies. "I don't know if that's the aesthetic of cinema or it's an anachronism," comments Dr. Dexeus.
Image copyright, Getty Images
Image caption,Vernix caseosa - lubrication on the skin of a newborn - is unlikely to be seen in movies
Why an anachronism? The doctor explains that in the past it was customary in hospitals to wash the baby immediately after birth and remove the vernix caseosa, the primordial lubricant (a greyish-white substance with a curdled consistency that covers the skin of the newborn), after which the baby was handed over to the mother - already completely clean.
That doesn't happen anymore in advanced medical countries, the obstetrician explains, because studies have shown that it's good for a baby's health to have the lube on his skin for several hours after birth. nine0011
nine0011
2. How amniotic fluid actually drains
The fetal bladder that forms around the embryo is filled with amniotic fluid, often referred to as amniotic fluid. In films, we often see scenes of a "sudden" departure of these waters, after which the pregnant woman almost immediately begins childbirth.
An example from the TV series Sex and the City: Charlotte's water breaks when she fights outside a restaurant. Then he runs to catch a taxi.
Image copyright Getty Images
Image caption,Sex and the City: Charlotte's water breaks. But in real life, this does not mean at all that she is about to give birth
"There is nothing unusual about this - after the waters began to break, you should actually rush to the doctor for an examination to confirm whether the fetal bladder has really burst because the woman knows she's losing fluid, but she doesn't see what it is," says Dr. Dexeus.
Examination is necessary because it is not always so easy to determine whether it is amniotic fluid or urine, especially if it is a few drops or a little moisture. nine0011
- Medical myths about childbirth: the exact date, spicy food, and the waste of water
- "Age is one day": the first hours of a new life , as is often the case in films. In fact, this is only part of the processes taking place in the body of the expectant mother.
"It's much more common for a woman to realize after a few contractions that she's in the process of having a baby. It's part of the natural progression of childbirth," says Ann Yates of the International Confederation of Midwives (ICM), who has delivered throughout more than 40 years in various regions of the world. nine0011
"Actually, if the amniotic sac ruptured long before delivery, long before the baby is ready to be born, it could mean a complication," she adds.

3. Birth position
Another common scene in films: a woman giving birth sits on a high delivery table.
Image copyright, Getty Images
Photo caption,This is a comfortable position for childbirth, but not the most common in the world
There are plenty of examples too, from Katherine Heigl's character in "Knocked Up" to Jennifer Aniston's character in "Friends". nine0011
Indeed, this is a comfortable position for childbirth, but not the most common in the world.
"It's common in the UK and the US for the woman to be semi-sitting with her feet on the birthing table, with her legs elevated," says Dr. Dexeus.
"But in countries like Spain, for example, the most common birthing position is lying down, with knees supported, but the legs are not raised like that."
This position is the most common in Brazil, and this is how women are examined by gynecologists.
 nine0011
nine0011 There are a few other positions women give birth in that are rarely seen in movies or on TV: standing, squatting, sitting on a bench, or lying on their side.
In addition, the position depends on the stage of labor in which the woman is - she can change position during labor to speed up the birth of the child.
Image copyright, Getty Images
Photo caption,The positions in which women can give birth vary from country to country and culture to culture
Yates believes Hollywood's portrayal of childbirth creates problems in real life.
"It can be difficult for women to give birth in one position or another - and the cinema imposes on them the idea of \u200b\u200bhow it supposedly should be."
4. Where did the postpartum period go?
The postpartum period is usually referred to as the first six weeks after the birth of a baby. "The postpartum period is the most important thing that is forgotten in the movies," emphasizes Dr.
 Dexeus. nine0011
Dexeus. nine0011 Much of what happens after childbirth is rarely shown in Hollywood films.
- Postpartum psychosis: "I was always afraid to go crazy, but this happened after the birth of my son"
Naturally, you will not see the separation of the placenta or the suturing of tears that occur during childbirth. But not only that.
Image copyright, Getty Images
Image caption,Actress Brooke Shields speaks at an event to raise awareness of postpartum depression
"Postpartum depression is shown very superficially in movies," says a gynecologist of the condition experienced by at least one in every ten women who have given birth (according to WHO statistics).
Movies generally don't mention how difficult it can be to start breastfeeding, how having a baby can affect bladder and bowel health, and dozens of other bodily changes that can be very challenging for a woman.

"These films don't show how difficult the physical recovery from a C-section can be," adds Dr. Dexeus.
"All these movie images, pushing us to think that childbirth is something simple, are actually very dangerous, because it just doesn't always happen," says the doctor.
5. Heart-rending screams of pain
And here is another classic situation for childbirth scenes invented by filmmakers: a woman in labor screams in pain.
"In the past, laboring mothers weren't given anesthetics," explains Cuban doctor Josephine Lopez.
- Why is it much harder for women to give birth than for their distant ancestors?
"Yes, it's true that contractions are painful, and when they last a long time, a woman is exhausted. However, these pains do not necessarily make a woman scream. Although, of course, everyone has their own pain threshold," says Lopez.
 epidural anesthesia is used, this usually does not happen. nine0011
epidural anesthesia is used, this usually does not happen. nine0011 Image copyright, Getty Images
Image caption,Experts say women actually scream much less during childbirth than in movies. "Women are strong. It's kind of a common trait," the midwife emphasizes.
"And often they go through labor - which is no doubt painful - without a single scream. Yes, they sometimes moan, but almost never you will hear such heart-rending screams as in the movies," Yates adds. nine0011
6. Helpless, confused fathers
The image of a clumsy and fearful husband giving birth is another cinematic cliché.
Example: Hugh Grant's character in the comedy melodrama Nine Months, who does exactly what a man shouldn't do when his wife is in labor.
- Dad's Day, or Who and what needs to know about childbirth?
"We are shown horribly frightened men, pale as death when labor begins.
 Some even faint," says Dr. Dexeus. This is by no means the norm." nine0011
Some even faint," says Dr. Dexeus. This is by no means the norm." nine0011 Image copyright, Getty Images
Image caption,Are men in a situation where their wife is in labor really like the character Hugh Grant in Nine Months?
According to Yeats, in Hollywood films, the man is often portrayed as a nuisance or as someone who has absolutely no idea how to behave during childbirth.
"In fact, many of those who accompany the woman in labor are in perfect harmony with her," the midwife emphasizes. nine0011
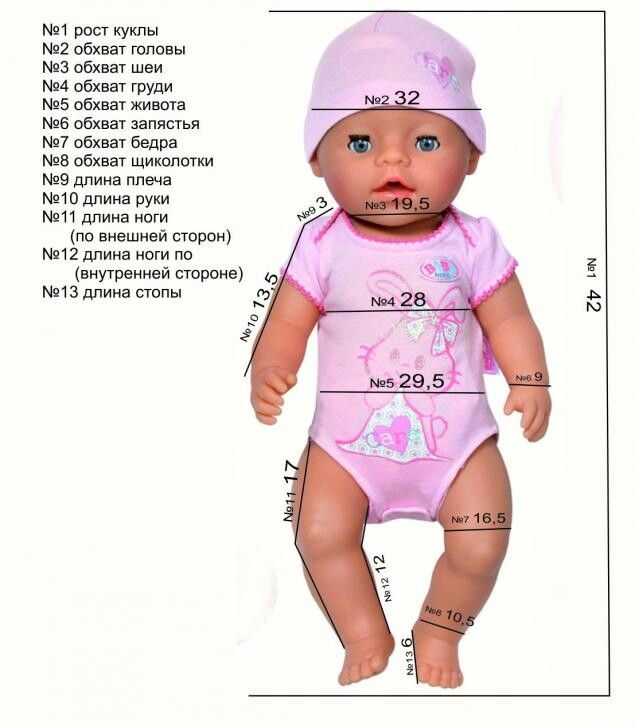
Orthopedist for the baby - articles from the specialists of the clinic "Mother and Child"
Bobrova Marina Igorevna
Obstetrician-gynecologist, Reproductologist
Clinic "Mother and Child" South-West
the sooner the better
It would seem, why show the baby to an orthopedist, because he still does not sit, does not get up, does not walk. It turns out that there is no load on the bones and muscles, so it seems that the baby has nothing to look at yet.
 Some parents think so and for some reason are in no hurry to show their child to an orthopedist. Other moms and dads don't go for counseling because they think their baby is developing normally. After all, he has no noticeable changes: his arms and legs are in place, seemingly of the same length, his back is even - it means that everything is in order with the baby. nine0019 In fact, some diseases of the musculoskeletal system are not always obvious and are usually not noticeable to parents. And it is generally impossible to independently determine, for example, whether a baby has the same leg length without being a specialist. And even a pediatrician, if the pathology is not expressed, may not detect it, especially if the disease does not bother the child. But as the baby grows, orthopedic problems can intensify and cure the disease will be much more difficult than at an early age. Therefore, the newborn should be shown to the orthopedist as early as possible. nine0011
Some parents think so and for some reason are in no hurry to show their child to an orthopedist. Other moms and dads don't go for counseling because they think their baby is developing normally. After all, he has no noticeable changes: his arms and legs are in place, seemingly of the same length, his back is even - it means that everything is in order with the baby. nine0019 In fact, some diseases of the musculoskeletal system are not always obvious and are usually not noticeable to parents. And it is generally impossible to independently determine, for example, whether a baby has the same leg length without being a specialist. And even a pediatrician, if the pathology is not expressed, may not detect it, especially if the disease does not bother the child. But as the baby grows, orthopedic problems can intensify and cure the disease will be much more difficult than at an early age. Therefore, the newborn should be shown to the orthopedist as early as possible. nine0011 what the doctor sees
An orthopedist should be visited when the child is 1 month old, and then several more times - at 3, 6 and 12 months.
 At the first consultation, the doctor will carefully examine the baby, literally from top to toe, assess the size and shape of all parts of the body, also check how proportional and symmetrical they are to each other, and see how the arms and legs move. The orthopedist carefully examines all joints for mobility, he will especially carefully examine the hip joints and be sure to check whether the baby's legs are the same length. nine0020
At the first consultation, the doctor will carefully examine the baby, literally from top to toe, assess the size and shape of all parts of the body, also check how proportional and symmetrical they are to each other, and see how the arms and legs move. The orthopedist carefully examines all joints for mobility, he will especially carefully examine the hip joints and be sure to check whether the baby's legs are the same length. nine0020 But even if there was no orthopedic pathology in 1 month, the baby still needs to be regularly shown to the doctor. During repeated examinations, some diseases can be identified that did not manifest themselves during the first visit to the doctor.
possible problems
What are the most serious diseases that an orthopedist should exclude in children of the first year of life?
- Hip dysplasia and congenital dislocation of the hip - these diseases occur due to congenital underdevelopment of the hip joint.
 If the disease is not detected in time, then it can progress rapidly, one leg will be much shorter than the other and the gait will be seriously disturbed. Pathology can be detected already in 1-3 months. nine0011
If the disease is not detected in time, then it can progress rapidly, one leg will be much shorter than the other and the gait will be seriously disturbed. Pathology can be detected already in 1-3 months. nine0011 - Congenital torticollis - immediately after birth, it becomes noticeable that the baby's head is constantly tilted to the side and to the side. Torticollis must be treated, otherwise the child develops asymmetry of the face, facial skull, shoulders, and spine.
- Congenital clubfoot - the baby's feet "clubfoot" like a bear cub: e If the newborn could stand up, he would lean on the outer surface of the foot. Without treatment, if a child begins to walk on such legs, the deformation of the damaged foot intensifies, the relationship of bones is disturbed, gait and posture suffer, and difficulties arise with the selection of shoes. nine0011
These three major diseases should be identified as early as possible (and they can be detected as early as 1-3 months), because the sooner they are treated, the better the result will be.
we distribute the load
But even if the child has no orthopedic pathology, the doctor will still advise parents what to do so that the bones and muscles of the baby develop properly. For example, even healthy children can often turn their heads to one side. This is usually because they are attracted to the side of the crib with a colorful toy or other interesting item. nine0019 Often, parents simply do not notice this, but the orthopedist will immediately pay attention to which direction the child most often tilts his head. He will also quickly see how the child turns over - again in one direction or both. All this may be a variant of the norm, but sometimes it indicates that the child has a different muscle tone on the left and right. In this case, the orthopedist will advise massage, swimming and special exercises with an emphasis on a specific muscle group. The doctor will tell you how to strengthen other muscle groups: for example, the abdomen, back - all this will help the baby start sitting, getting up and walking in time in the future.
 nine0011
nine0011 don't rush the baby
The child is growing and seems to be ready to sit. He should sit down on his own at 7 months, stand on his feet - at 9, at 10-11 take his first steps, holding on to a support. Until this age, doctors recommend not to encourage the baby to sit or stand (it is especially harmful to put him in pillows). The bones and muscles of the baby are not yet ready for new movements, and if the child’s muscle corset does not have time to get stronger before he starts to sit down on his own, this can lead to a curvature of the spine. If the time has come, and the baby has not yet mastered a new skill, the orthopedist will tell you how to stimulate the baby (massage and gymnastics will help here again). nine0011
help with the first steps
When the child tries to take the first steps, the orthopedist will tell you what shoes to buy for the baby. It will help to evenly load the ankle joint, which means that the load will be distributed correctly on all other joints.
 Usually, doctors advise learning to walk not barefoot or in socks, booties, but in boots or shoes: leather, with a hard heel, small heels, laced or Velcro . If the baby has some kind of foot or ankle pathology, the orthopedist will select special shoes or orthopedic insoles. nine0011
Usually, doctors advise learning to walk not barefoot or in socks, booties, but in boots or shoes: leather, with a hard heel, small heels, laced or Velcro . If the baby has some kind of foot or ankle pathology, the orthopedist will select special shoes or orthopedic insoles. nine0011 By clicking on the send button, I consent to the processing of personal data
Attention! Prices for services in different clinics may vary. To clarify the current cost, select a clinic
Clinical Hospital MD GROUPClinical Hospital Lapino-1 "Mother and Child"Children's Clinic KG "Lapino" on New Riga (branch)Clinic "Mother and Child" KuntsevoClinic "Mother and Child" SavelovskayaClinic "Mother and Child" South-WestClinic "Mother and Child" » Novogireevo
All directions
01.
Kinesiotherapy for children
02.