Are c sections optional
Is a Planned C-Section Right for Me?
Series Cesarean Section (C-Section)
Written by Joanne Barker
A woman may want a planned cesarean section to give birth for many reasons. For some, it's the best choice. But C-sections have risks of their own.
As long as there's no emergency, don't let yourself be rushed. Take the time to make a decision that feels right to you, for now as well as for your future.
Why You Might Have a C-Section
Sometimes a doctor will switch to this surgical procedure after a woman has started labor and then has problems.
Planned C-sections are different. Your doctor or midwife has found a medical reason for you to have one, but it's not an emergency. Two examples are that you've had a previous C-section and that you have a baby who's facing the wrong way. You and your doctor may even decide later that a vaginal birth is a better choice.
Some healthy women want the surgery so they can pick their delivery date or avoid a vaginal delivery. Those aren't medical reasons, and their doctors may disagree with that choice.
Experts from the American College of Obstetrics and Gynecology don't recommend these elective C-sections. They say you definitely shouldn't have one before 39 weeks. And they strongly discourage it if you want more children.
How It Affects the Birth
While C-sections are generally very safe, they're still major surgeries. Your recovery time will be longer than with a normal vaginal delivery, both in the hospital and afterward. And they carry risks for you and the baby.
You have a greater chance of:
- Heavy bleeding
- Blood clots
- Infection
- Injury to other organs
Some women will need a blood transfusion.
Babies delivered by C-section are more likely to have breathing problems after birth. When they do, they may need to spend time in the neonatal intensive care unit, usually for a few days.
Impacts Later in Life
Each C-section tends to be more difficult than the one before. If you're planning to have another baby, and particularly if you want a large family, talk with your doctor about how the procedure could affect your plans.
If you're planning to have another baby, and particularly if you want a large family, talk with your doctor about how the procedure could affect your plans.
It could complicate future pregnancies. The placenta might not attach to your uterus the right way. This means you would have a greater chance for bleeding and could need a hysterectomy. The scar in your uterus could split open.
Depending on why you had a C-section and how it went, you may be able to give birth vaginally later. But if you've had more than one of these surgeries, vaginal birth may not be an option.
Kids born by C-section may be more prone to have asthma, diabetes, allergies, and obesity when they grow up.
What to Consider
Talk to your doctor or midwife about why they think you should have a C-section. If the baby's size is the reason, ask how accurate the weight estimates are. Find out if you have any other options to address their concern.
Will you be able to wait until 39 or 40 weeks, as the American College of Obstetrics and Gynecology recommends?
Make sure you understand what harm could come to you and your infant if you don't have a C-section.
If having more children is important to you, find out if you'll need the procedure for future deliveries.
Think about whether or not the benefits of this surgery clearly outweigh the risks. It's OK to get a second opinion to help you decide.
Caesarean section - NHS
A caesarean section, or C-section, is an operation to deliver your baby through a cut made in your tummy and womb.
The cut is usually made across your tummy, just below your bikini line.
A caesarean is a major operation that carries a number of risks, so it's usually only done if it's the safest option for you and your baby.
Around 1 in 4 pregnant women in the UK has a caesarean birth.
Why caesareans are carried out
A caesarean may be recommended as a planned (elective) procedure or done in an emergency if it's thought a vaginal birth is too risky.
Planned caesareans are usually done from the 39th week of pregnancy.
A caesarean may be carried out because:
- your baby is in the breech position (feet first) and your doctor or midwife has been unable to turn them by applying gentle pressure to your tummy, or you'd prefer they did not try this
- you have a low-lying placenta (placenta praevia)
- you have pregnancy-related high blood pressure (pre-eclampsia)
- you have certain infections, such as a first genital herpes infection occurring late in pregnancy or untreated HIV
- your baby is not getting enough oxygen and nutrients – sometimes this may mean the baby needs to be delivered immediately
- your labour is not progressing or there's excessive vaginal bleeding
If there's time to plan the procedure, your midwife or doctor will discuss the benefits and risks of a caesarean compared with a vaginal birth.
Asking for a caesarean
Some women choose to have a caesarean for non-medical reasons.
If you ask your midwife or doctor for a caesarean when there are not medical reasons, they'll explain the overall benefits and risks of a caesarean to you and your baby compared with a vaginal birth.
If you're anxious about giving birth, you should be offered the chance to discuss your anxiety with a healthcare professional who can offer support during your pregnancy and labour.
If after discussing all the risks and hearing about all the support on offer you still feel that a vaginal birth is not an acceptable option, you should be offered a planned caesarean. If your doctor is unwilling to perform the operation, they should refer you to a doctor who will.
What happens during a caesarean
Most caesareans are carried out under spinal or epidural anaesthetic.
This mean you'll be awake, but the lower part of your body is numbed so you will not feel any pain.
During the procedure:
- a screen is placed across your body so you cannot see what's being done – the doctors and nurses will let you know what's happening
- a cut about 10 to 20cm long will usually be made across your lower tummy and womb so your baby can be delivered
- you may feel some tugging and pulling during the procedure
- you and your birth partner will be able to see and hold your baby as soon as they have been delivered if they're well – a baby born by emergency caesarean because of foetal distress may be taken straight to a paediatrician for resuscitation
The whole operation normally takes about 40 to 50 minutes.
Occasionally, a general anaesthetic (where you're asleep) may be used, particularly if the baby needs to be delivered more quickly.
Find out more about how a caesarean is carried out
Recovering from a caesarean
Recovering from a caesarean usually takes longer than recovering from a vaginal delivery.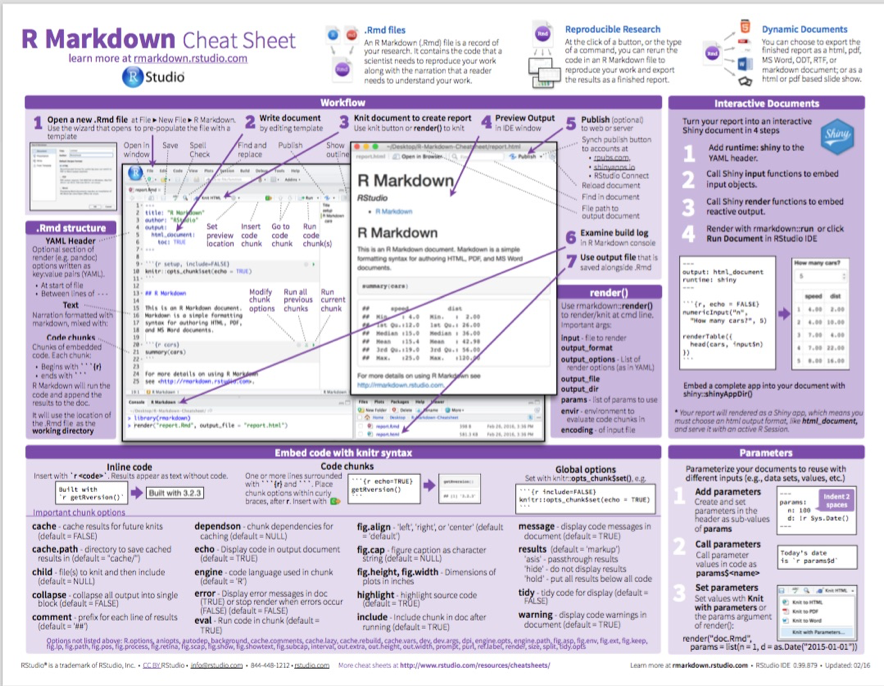
The average stay in hospital after a caesarean is around 3 or 4 days, compared with an average of 1 or 2 days for a vaginal birth.
You may experience some discomfort in your tummy for the first few days. You'll be offered painkillers to help with this.
When you go home, you'll need to take things easy at first. You may need to avoid some activities, such as driving, until you have had your postnatal check-up with the doctor at 6 weeks.
The wound in your tummy will eventually form a scar. This may be obvious at first, but it should fade with time and will often be hidden in your pubic hair.
Find out more about recovering from a caesarean
Risks of a caesarean
A caesarean is generally a very safe procedure, but like any type of surgery it carries a certain amount of risk.
It's important to be aware of the possible complications, particularly if you're considering having a caesarean for non-medical reasons.
Possible complications include:
- infection of the wound or womb lining
- blood clots
- excessive bleeding
- damage to nearby areas, such as the bladder or the tubes that connect the kidneys and bladder
- temporary breathing difficulties in your baby
- accidentally cutting your baby when your womb is opened
Find out more about the risks of a caesarean
Future pregnancies after a caesarean
If you have a baby by caesarean, it does not necessarily mean that any babies you have in the future will also have to be delivered this way.
Most women who have had a caesarean section can safely have a vaginal delivery for their next baby, known as vaginal birth after caesarean (VBAC).
But you may need some extra monitoring during labour just to make sure everything is progressing well.
Some women may be advised to have another caesarean if they have another baby.
This depends on whether a caesarean is still the safest option for them and their baby.
For more information, the Royal College of Obstetricians and Gynaecologists has a leaflet on birth options after previous caesarean section (PDF, 357kb).
Page last reviewed: 27 June 2019
Next review due: 27 June 2022
Mandatory and optional header files
Twitter LinkedIn Facebook E-mail address
- Article
- Reading takes 2 minutes
The description of each run-time routine includes a list of required and optional include header (. H) files for that routine. Required header files must be included to get a function declaration for a routine, or a definition used by another internally called routine. Optional header files are often included to use predefined constants, type definitions, or built-in macros. The following table shows examples of the contents of optional header files:
H) files for that routine. Required header files must be included to get a function declaration for a routine, or a definition used by another internally called routine. Optional header files are often included to use predefined constants, type definitions, or built-in macros. The following table shows examples of the contents of optional header files:
| Definition | Example |
|---|---|
| Macro definition | If a library subroutine is implemented as a macro, the macro definition may be in a different header file than the source routine's header file. For example, the macro _toupper is defined in the header file CTYPE.H, while the function toupper is declared in STDLIB.H. |
| Predefined constant | Many library routines refer to constants defined in header files. For example, the routine _open uses constants such as _O_CREAT , which is defined in the FCNTL. H header file. H header file. |
| Type definition | Some library routines return a structure or take a structure as an argument. For example, stream I/O routines use a structure like FILE , which is defined in STDIO.H. |
The run-time library header files provide function declarations in the style recommended by the ANSI/ISO C standard. The compiler performs type checking on any subroutine reference encountered after the corresponding function declaration. Function declarations are especially important for routines that return a value of some type other than the default int . Subroutines that do not specify an appropriate return value in the declaration will be considered by the compiler to return int , which may cause unexpected results. For more information, see Type Checking.
C runtime (CRT) and C++ Standard Library (STL) .lib files
How to use optional features of the GNU FDL - GNU Project free software
Richard Stallman The GNU FDL (Free Documentation License) GNU) includes two optional features: unchangeable sections and cover texts which you can desire to use.
The simplest case is when you do not use these opportunities. Then it should be stated in the license notice, something like this:
Permission is granted to copy, distribute and/or modify this document under the terms of the GNU Free Documentation License, version 1.3, or any later version published by the Free Software Foundation security; no Invariant Sections, no Front Side Texts covers and without Texts for the back cover. A copy of the license is located in section entitled "GNU Free Documentation License".
But if you want to take advantage of these opportunities, then here we are. explain what they are for and how to use them.
Invariant sections
The point of immutable sections is that they give you a way to express personal non-technical opinion on the subject.
A classic example of an immutable non-technical section in free manual - The GNU Manifesto, which is included in the GNU Emacs Handbook. In the GNU Manifesto nothing is said about how to edit with Emacs, but there explains the reason why I wrote GNU Emacs - so that it was an important part of the GNU operating system, which would give users computers the freedom to collaborate in the community. Since the GNU Manifesto reflects the principles of the GNU project rather than the specifics of GNU Emacs, we decided that others should not remove or modify it for further distribution "Manuals for Emacs", and we wrote this requirement into license. In fact, we have turned the GNU Manifesto into an immutable section, although did not use this term. To do this today with GNU FDL, we would write something like this license notice:
In the GNU Manifesto nothing is said about how to edit with Emacs, but there explains the reason why I wrote GNU Emacs - so that it was an important part of the GNU operating system, which would give users computers the freedom to collaborate in the community. Since the GNU Manifesto reflects the principles of the GNU project rather than the specifics of GNU Emacs, we decided that others should not remove or modify it for further distribution "Manuals for Emacs", and we wrote this requirement into license. In fact, we have turned the GNU Manifesto into an immutable section, although did not use this term. To do this today with GNU FDL, we would write something like this license notice:
Permission is granted to copy, distribute and/or modify this document under the terms of the GNU Free Documentation License, version 1.3, or any later version published by the Free Software Foundation security; only the “Manifest” applies to Invariant sections. GNU", without Texts for the front cover and without Texts for back cover.
A copy of the license is located in the section entitled "GNU Free Documentation License".
It says that the GNU Manifesto section is the only unchangeable section.
The old Emacs Handbook license did not allow others to people who modified and distributed the manual further, to add new invariant sections. But when we formulated a more general version of the concept for the GNU FDL, I thought it would make more sense ethically if those who change the manual will be able to write invariant sections exactly like this the same as the original authors. FDL allows this.
But this possibility requires precautionary measures to prevent abuse that would jeopardize free status guides. Person B who changes a manual written by person A does not should be able to make any kind of documentation of person A immutable, because that would be refusing person B permission to change it farther. Similarly, if person B adds documentation for additional subtopics, this additional documentation should not be immutable; others should be able to change themselves documentation. The conditions imposed by the FDL on adding immutable sections are put in place such precautionary measures.
The conditions imposed by the FDL on adding immutable sections are put in place such precautionary measures.
The manual does not need to have invariant sections. In the simplest case they don't exist at all. You don't need to list the GNU FDL itself as immutable section because the FDL explicitly states that the FDL itself cannot be modified. FDL also distinguishes sections with certain headings, such as "History", "Dedications" and others. You do not need list these sections as immutable because the rules are already given in the FDL for these sections.
Cover texts
The cover text is the short text you require print on the cover of a manual when it is published, even if it is published someone else. You can specify “text for the front side covers” to be printed on the front side, and “back cover text”, which should be printed on the back. You can enter one text for each of these two kinds.
Cover texts are a new feature, so I can't give examples of their use in the past, but their purpose is simple. They are intended to give the original publisher some editorial is a way to ask or encourage people to buy copies that published by him, not copies of someone who reprinted the manual. For example, we can imagine that as text for the reverse side covers will be indicated like this:
They are intended to give the original publisher some editorial is a way to ask or encourage people to buy copies that published by him, not copies of someone who reprinted the manual. For example, we can imagine that as text for the reverse side covers will be indicated like this:
OAO Free Guides paid for the work of M. Lomonosov on writing this guide and asks for your support through the purchase our edition of this guide.
This could help Free Guides to succeed in business publishing free manuals - at least that is idea. To indicate this as text for the back cover, OAO Free Guides could write something like this license notice:
Permission is granted to copy, distribute and/or modify this document under the terms of the GNU Free Documentation License, version 1.3, or any later version published by the Free Software Foundation security; no Invariant Sections, no Front Side Texts cover and with one Text for the back cover: “OAO Svobodnye management paid for the work of M.