What does retained placenta look like
Retained placenta | Pregnancy Birth and Baby
Retained placenta | Pregnancy Birth and Baby beginning of content3-minute read
Listen
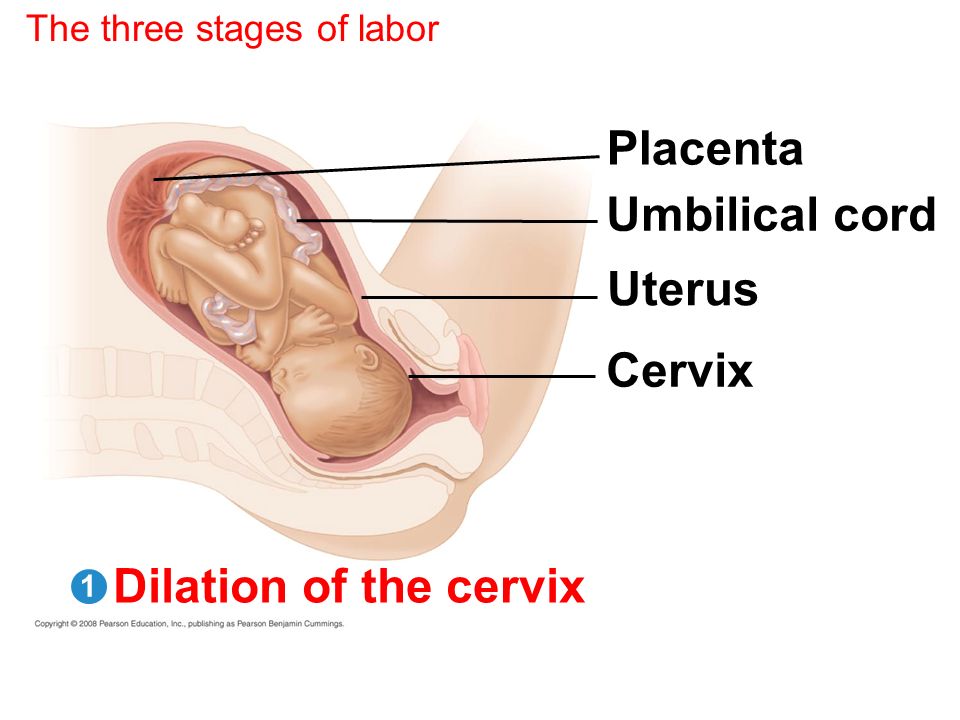
A retained placenta is when the placenta is not delivered within 30 minutes of the baby’s birth. It is a serious problem since it can lead to severe infection or life-threatening blood loss.
Retained placenta is not a common condition, but because it’s serious, it will need to be managed by a medical team.
What causes retained placenta?
A placenta can be retained if your contractions aren’t strong enough to expel it, or if the cervix closes and traps the placenta inside your uterus.
You are more at risk of a retained placenta if you are over the age of 30, have a premature baby or if your first and second stages of labour were very long. It can also happen if you have a fibroid or another problem with your uterus.
Many women will have an injection of syntocinon (a synthetic version of the hormone oxytocin), which not only helps deliver the placenta but also helps reduce the risk of postpartum bleeding. Having this injection is called ‘active management’. If the mother chooses not to have the injection, it is called ‘expectant management’.
What are the symptoms of retained placenta?
The main symptom of retained placenta is that the placenta doesn’t completely come out of the uterus after the baby is born. Another symptom can be bleeding before the placenta comes out.
If a piece of placenta is left behind, you may develop symptoms days or weeks after the birth. These may include:
- fever
- a bad smelling discharge from the vagina
- heavy bleeding
- large pieces of tissue coming out of the vagina
- pain
What is the treatment for a retained placenta?
Sometimes retained placenta can be treated simply if you empty your bladder, change position and have the doctor or midwife gently pull on the umbilical cord.
If that doesn’t work, you will need a procedure to remove the placenta. You will be taken into surgery after the birth and given an epidural or anaesthetic so you don’t feel anything. Your doctor will use an instrument called a curette to scrape away the lining of the uterus.
While you’re waiting for surgery, the medical team will keep a close eye on you to check you're not bleeding heavily (postpartum haemorrhage). The procedure itself is quick, but you will need to be monitored for several hours after to make sure you are not bleeding.
If you do start to experience some of the symptoms mentioned above in the days and weeks after you have had your baby, it’s important to see your doctor immediately. It is not always obvious after the placenta has been delivered that some tissue may have been left behind and this can lead to infection and bleeding. If you are bleeding heavily after the birth, you will need surgery to investigate the cause.
Sources:
RANZCOG (Management of Postpartum Haemorrhage (PPH)), King Edward Memorial Hospital (Retained placenta), Women's and Newborn Health Westmead Hospital (The birth of your placenta), International Journal of Women's Health (Retained placenta after vaginal delivery: risk factors and management)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: February 2020
Back To Top
Related pages
- Placenta complications in pregnancy
- About the placenta
Need more information?
Labour complications
Even if you’re healthy and well prepared for childbirth, there’s always a chance of unexpected problems. Learn more about labour complications.
Read more on Pregnancy, Birth & Baby website
Asherman Syndrome
Read more on RANZCOG - Royal Australian and New Zealand College of Obstetricians and Gynaecologists website
Why do some mums stop breastfeeding before 6 months?
Most new parents know 'breast is best', but while more than 9 out of 10 babies are breastfed at birth, few mums are breastfeeding exclusively 5 months later.
Read more on Pregnancy, Birth & Baby website
What is freebirth?
Freebirth is when a woman chooses to birth her baby without medical or midwifery assistance, but this greater independence comes with some risks.
Read more on Pregnancy, Birth & Baby website
About the placenta
The placenta develops inside the uterus (womb) during pregnancy. It gives your baby nutrients and oxygen. Find out more about the placenta here.
Read more on Pregnancy, Birth & Baby website
Postpartum haemorrhage
Postpartum haemorrhage is when you bleed more than normal after giving birth. It can be very serious and requires medical attention right away.
Read more on Pregnancy, Birth & Baby website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.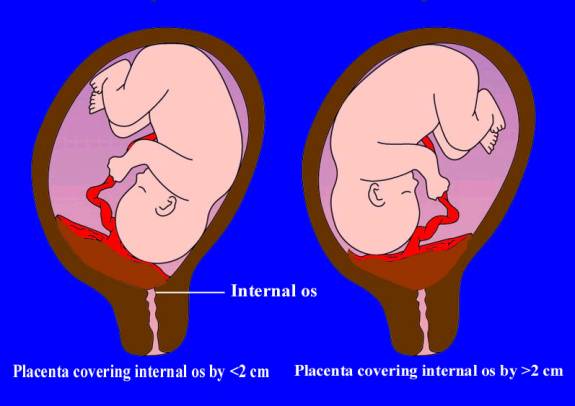
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
What You Should Know About a Retained Placenta
Written by WebMD Editorial Contributors
In this Article
- Causes of a Retained Placenta
- Symptoms of a Retained Placenta
- Risks of a Retained Placenta
- Treatment for Retained Placenta
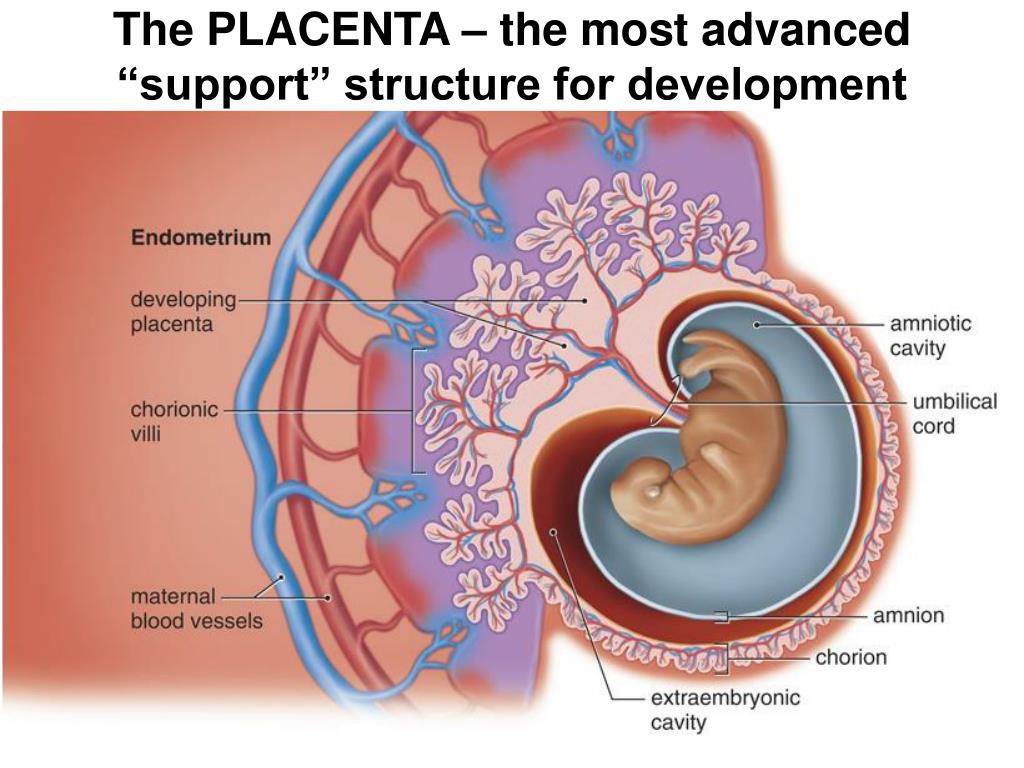
The placenta is a temporary organ that grows during pregnancy to filter oxygen, blood, and nutrients to your baby.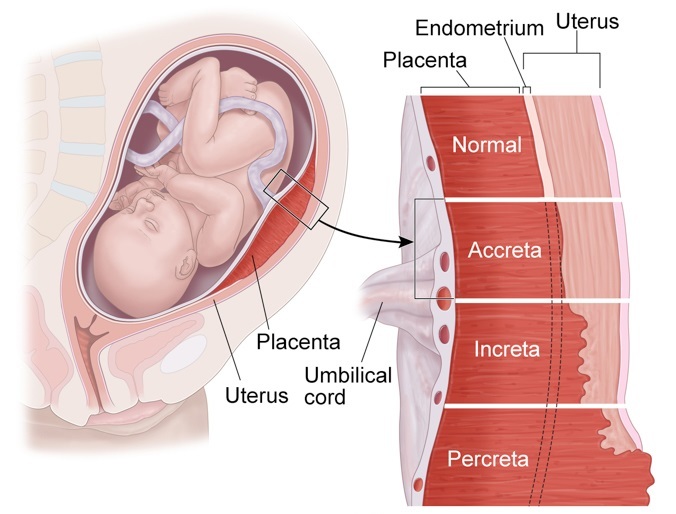 After you give birth, you will also deliver your placenta shortly after.
After you give birth, you will also deliver your placenta shortly after.
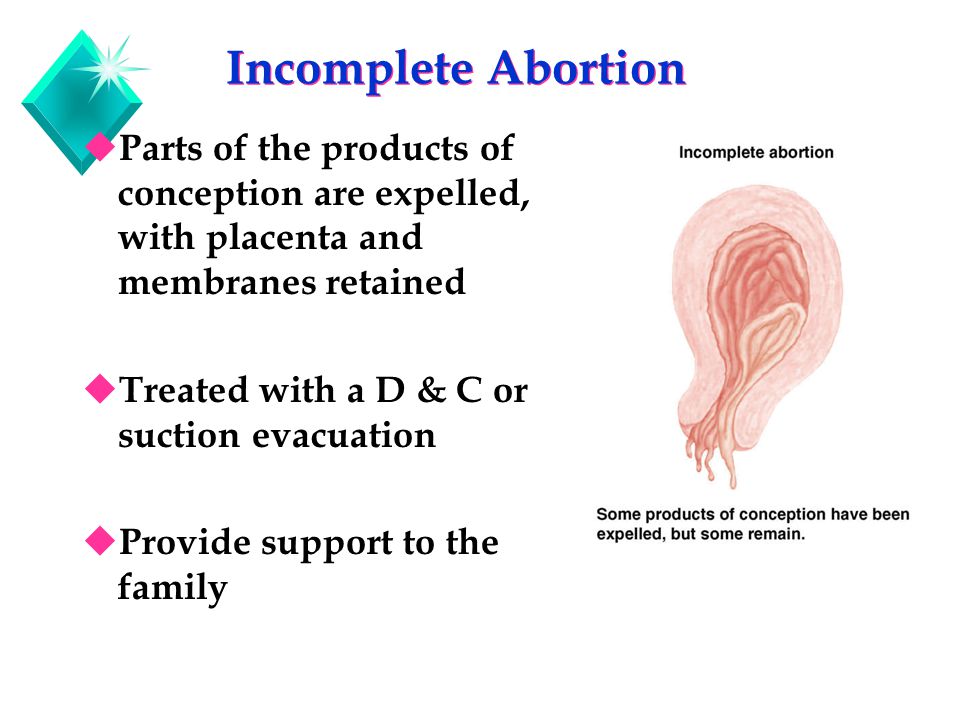
Sometimes all or part of the placenta stays in the womb. This is called a retained placenta and it can have serious side effects.
Causes of a Retained Placenta
After your baby is born, you will usually deliver your placenta within 18 to 60 minutes. Your uterus contracts, which pulls the placenta away from the wall of your uterus and pushes it out. Sometimes this doesn’t happen and can be caused by different things, including:
- Not enough contractions
- The placenta grows into the uterus wall
- The cervix closes
- Early delivery
- Giving birth many times
- Previous surgery in the uterus
- Conceiving by in vitro fertilization
- Having a retained placenta in another pregnancy
- Being born with uterus deformities
- Having oxytocin medication for too long
The most common reason for a retained placenta is not enough contractions in the uterus. Contractions can slow down or the uterus can have trouble contracting for different reasons. These include:
Contractions can slow down or the uterus can have trouble contracting for different reasons. These include:
- Having large babies
- Giving birth many times
- Too much oxytocin medication
- A long labor
- A fast labor
- Fibroids
- Having twins or multiples
- Magnesium sulfate infusions
Symptoms of a Retained Placenta
The most obvious sign of a retained placenta is that you don’t deliver it. The most common symptom of a retained placenta after birth is sudden blood loss and life-threatening bleeding.
At times you might push out most of it, however, some pieces of the placenta can be stuck inside. This can cause symptoms that take a while to show up such as:
- Delayed and heavy bleeding
- Blood clots
- Fever
- Chills
- Feeling sick or flu-like
- Foul-smelling vaginal discharge
If you have heavy bleeding and blood clots at home, make sure to keep your pads and show them to your doctor right away. They may want to check for placenta tissue.
They may want to check for placenta tissue.
Risks of a Retained Placenta
Most women safely deliver the placenta after having a baby, but sometimes it can stay inside the womb. This can cause serious side effects.
Life-threatening bleeding. If your placenta is not delivered, it can cause life-threatening bleeding called hemorrhaging.
Infection. If the placenta, or pieces of the placenta, stay inside your uterus, you can develop an infection.
A retained placenta or membrane has to be removed and you will need to see your doctor right away. If you have major bleeding, this is a medical emergency and you should go to your nearest hospital immediately.
Treatment for Retained Placenta
Some conditions can make it more likely that your uterus won’t contract properly. This can lead to a retained placenta. Your doctor will carefully check your medical history and consider how many births you’ve had and what kind of births.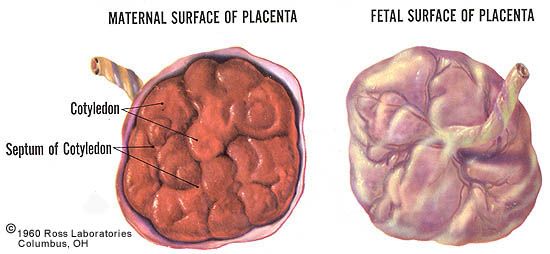 They might make plans during your pregnancy that can help ensure you won't have a retained placenta or prepare for retained placenta treatment.
They might make plans during your pregnancy that can help ensure you won't have a retained placenta or prepare for retained placenta treatment.
Your doctor or midwife will also usually ask you to do a few things right after giving birth that can help prevent a retained placenta.
Breastfeeding. Your doctor, midwife, or nurse will likely ask you to start breastfeeding your baby as soon as possible after you give birth. This is because breastfeeding makes your uterus contract and is a natural process that will help prevent a retained placenta.
Changing positions. Your doctor might ask you to roll to the side or to squat. Changing positions can help your uterus contract and push out your placenta.
Massage. After delivery, your doctor might massage your abdomen to help it contract. This can feel uncomfortable but can be helpful. Abdominal massage is often used after your second birth. This is because your uterus might not contract very well if you’ve had several births.
Medication. If these methods don’t work, your doctor might give you a shot of medicine that will make the uterus contract and help you deliver your placenta.
Manual removal. If your doctor diagnoses you with a retained placenta, they may want to remove the placenta by hand. They will often try another method first. Your doctor will give you an epidural or anesthetic medicine and manually separate the placenta inside the uterus.
Surgery. If massage, medication, or other options don’t work, your doctor might decide to do surgery. You will have an operation to safely remove the placenta. If the placenta has grown into the uterus wall and invaded other tissues, you may need to have your uterus removed.
Having surgery or a manual placenta removal can have risks, including infection and life-threatening bleeding. It can also cause endometritis, which is inflammation in the uterine lining. Your doctor may give you antibiotics to help stop infection and endometritis.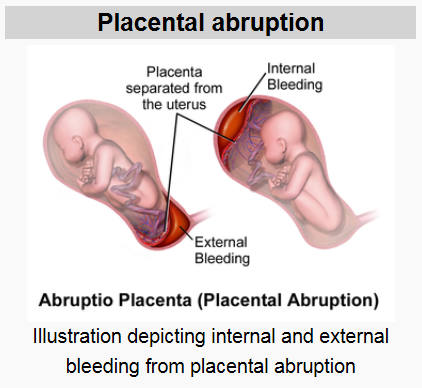
A retained placenta is not very common, but it can happen. Part of giving birth to a baby is also pushing out your placenta and your doctor will closely watch for it to come.
Delayed placenta separation - causes, symptoms, diagnosis and treatment
Delayed placenta separation is a complication of the third stage of labor, a condition in which the placenta does not fully or partially exfoliate from the uterine walls. Clinically, it can be manifested by pathological bleeding or the absence of bloody discharge normal for this period, soreness, or the absence of attempts. In this case, the standing of the bottom of the uterus corresponds to the period after the expulsion of the fetus, the connection of the umbilical cord with the uterus is indirectly determined. The diagnosis is established on the basis of the results of a physical examination, ultrasound. Most often, manual separation of the placenta or surgical treatment is performed.
General
According to the WHO definition, retained placenta is diagnosed if separation does not occur within half an hour after the end of the second stage of labour.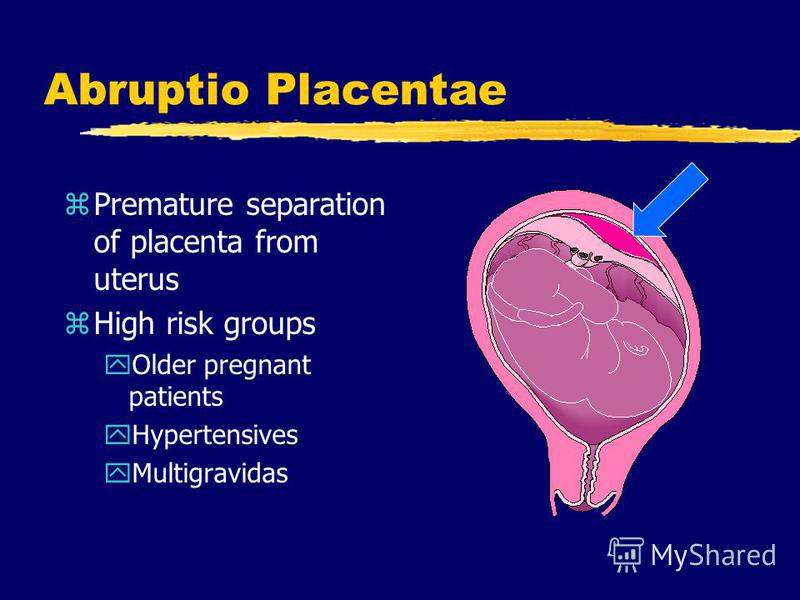 The incidence of pathology is 0.8-1.2% of all births. This complication is more often recorded in multiparous, especially those with a history of caesarean section. The disease is a serious problem of modern obstetrics, as it is often accompanied by postpartum hemorrhage. Bleeding is the cause of maternal death in a quarter of cases, 30% of which are the result of delayed separation of the placenta.
The incidence of pathology is 0.8-1.2% of all births. This complication is more often recorded in multiparous, especially those with a history of caesarean section. The disease is a serious problem of modern obstetrics, as it is often accompanied by postpartum hemorrhage. Bleeding is the cause of maternal death in a quarter of cases, 30% of which are the result of delayed separation of the placenta.
Delayed separation of the placenta
Causes
The etiology of delayed separation of the placenta has not been fully understood. Violations of detachment of the placenta and its parts in the afterbirth period, on the one hand, may be due to defects in uterine contractile activity, on the other hand, due to excessively tight attachment of the child's place. Most women in labor fail to detect any visible disorders. The main causes of pathology include:
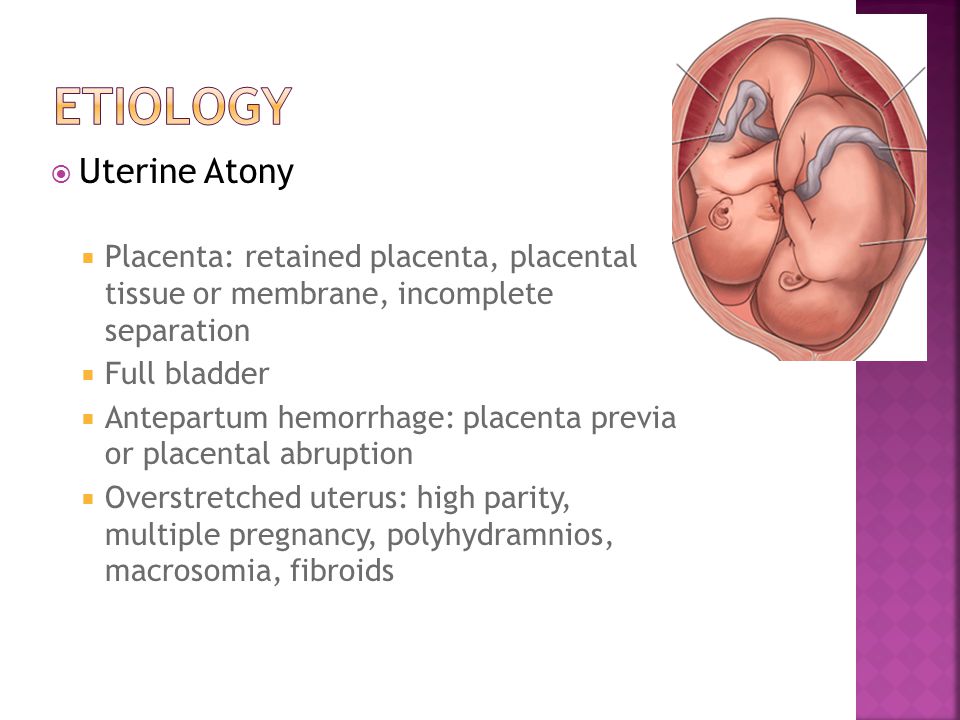
- Hypotension of the uterus. Weak contractions of the uterine muscles are not enough to start the process of separation of the placenta, even if the placenta does not have specific features that prevent detachment.
 In the presence of predisposing conditions, a slight decrease in contractile function can become a trigger for the development of pathology.
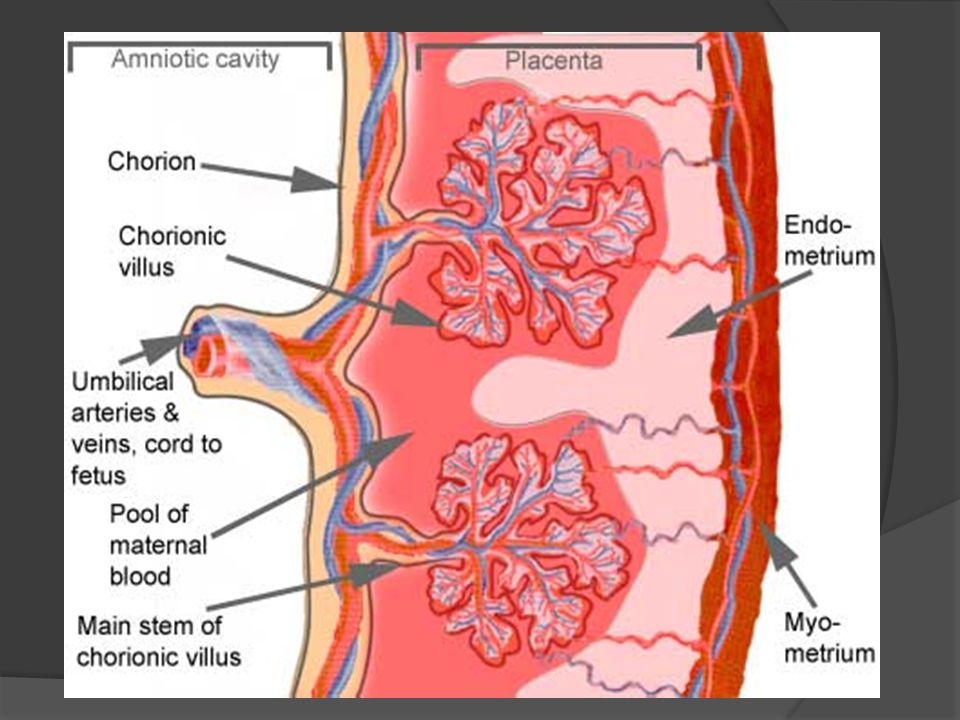
In the presence of predisposing conditions, a slight decrease in contractile function can become a trigger for the development of pathology. - Tight attachment of the placenta. Due to the depletion of the basal layer of the decidua and is characterized by a stronger than normal connection with the uterine walls without the germination of the chorionic villi into the myometrium. With the pathology under consideration, the force of uterine contractions is not enough to completely separate the placenta, which leads to bleeding.
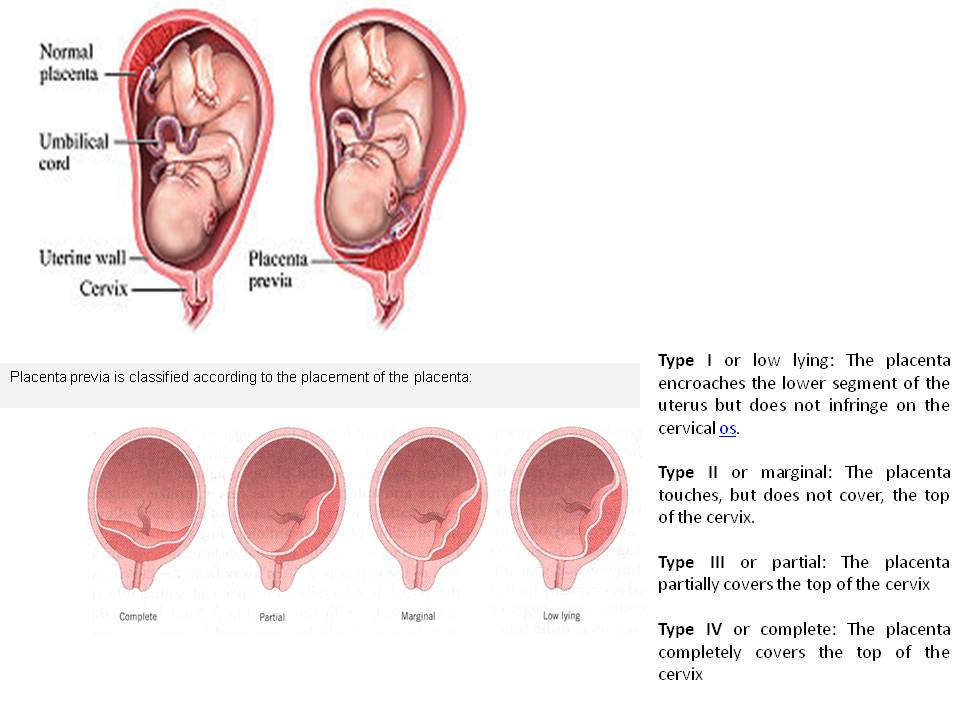
- True placental accreta. Also associated with underdevelopment of the basal layer, however, in this case, there is invasion of the villi into the muscle tissue, and in rare cases, the serosa of the uterus. More common with placenta previa. Spontaneous detachment of the adherent child's place is impossible, manual separation can lead to perforation of the uterine wall.
- Anomalies in the development of the placenta.
 Delayed detachment is often observed with developmental anomalies (lobed, two- and three-lobed or with additional lobules) of the placenta. The separation of the afterbirth is difficult with the so-called "membraneous" placenta, which is characterized by a slight thickness and a large attachment area, often extending to the entire uterine wall.
Delayed detachment is often observed with developmental anomalies (lobed, two- and three-lobed or with additional lobules) of the placenta. The separation of the afterbirth is difficult with the so-called "membraneous" placenta, which is characterized by a slight thickness and a large attachment area, often extending to the entire uterine wall.
The most significant risk factors are the endometritis transferred before the onset of pregnancy, obstetric history (surgery on the uterus, abortions, multiple births), indicating traumatic injuries. Inflammation and trauma lead to anatomical and histological changes in the uterus, which negatively affects placentogenesis and myometrial tone. Predisposing conditions include hyperandrogenism, malformations of the uterus (bicornuate uterus, intrauterine septum), volumetric formations (myoma, nodular adenomyosis).
Pathogenesis
Normally, after the birth of the fetus, afterbirth contractions appear, in which contractions spread to the entire uterus, including the placental site (previously, the muscles of this zone did not function).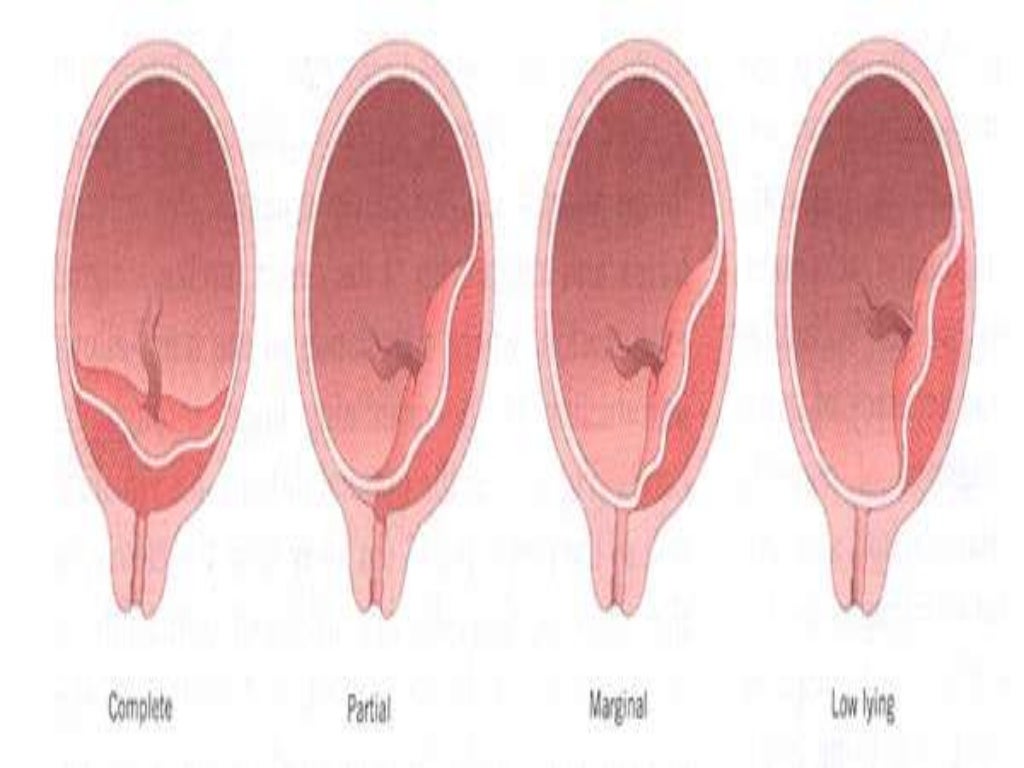 Labor activity leads to detachment of the child's place in the area of the spongy layer of the mucosa (with the preservation of the basal layer), and then to its exit to the outside. The separation of the placenta is accompanied by damage to blood vessels, physiological bleeding. After his birth, the uterus contracts, which helps to stop the bleeding.
Labor activity leads to detachment of the child's place in the area of the spongy layer of the mucosa (with the preservation of the basal layer), and then to its exit to the outside. The separation of the placenta is accompanied by damage to blood vessels, physiological bleeding. After his birth, the uterus contracts, which helps to stop the bleeding.
In the presence of unfavorable factors and predisposing conditions, detachment is difficult. With partial detachment, if the process started, but for some reason stopped, the gaping vessels of the uncontracted uterus become a source of pathological blood loss. Ingrown chorionic villi deep into the myometrium lead to thinning of the uterine wall, so an attempt to manually separate the placenta quickly ends in trauma, accompanied by intense bleeding.
Symptoms
Subjective signs of delayed separation of the placenta include prolonged, painful, ineffective attempts after the birth of a child or their complete absence.![]() An objective sign is intense bleeding observed with partial separation. If detachment of the placenta does not occur at all, even in a partial volume (for example, with a complete increment), bloody discharge from the birth canal may be absent.
An objective sign is intense bleeding observed with partial separation. If detachment of the placenta does not occur at all, even in a partial volume (for example, with a complete increment), bloody discharge from the birth canal may be absent.
Complications
The most common complication of delayed separation of the placenta is bleeding. Significant blood loss leads to such a potentially fatal complication as hemorrhagic shock, accompanied by multiple organ failure. Massive bleeding often develops when professional medical care is not provided in time (the risk increases sharply during childbirth outside a medical institution).
Other frequent complications of this pathology include purulent-inflammatory diseases (postpartum endometritis, pelvioperitonitis, obstetric sepsis), which can be the result of both surgical treatment and retention of placenta fragments in the uterine cavity. In addition, the remaining ingrown placenta can become a source of late postpartum hemorrhage, uterine rupture during a subsequent pregnancy.
Diagnosis
The diagnosis of retained placenta is made by the obstetrician if there is no discharge of the placenta within thirty minutes after the birth of the infant with appropriate results of the physical examination. To establish the causes of the pathological condition (which determines the choice of treatment tactics), an ultrasound examination is additionally used.
- Clinical examination. Signs of delayed separation of the placenta are determined by the shape and location of the uterus, the mobility of the umbilical cord. If separation has not occurred, the uterus is rounded, the bottom is located at the navel (Schroeder's sign), the outer segment of the umbilical cord does not lengthen (Alfeld's sign). The umbilical cord retracts with pressure over the womb (Kyustner-Chukalov's sign), after inhalation (Dovzhenko's sign), straining (Klein's sign).
- Ultrasonography. Ultrasound of the uterus is prescribed for the diagnosis of placenta accreta.
 Ultrasound signs of this pathology include deformation of the internal contour of the uterine cavity, its uneven expansion, and the absence of a hypoechoic layer between the myometrium and the placenta. Ultrasound angiography reveals hypervascularization of the anterior wall, chaotic branching of vessels.
Ultrasound signs of this pathology include deformation of the internal contour of the uterine cavity, its uneven expansion, and the absence of a hypoechoic layer between the myometrium and the placenta. Ultrasound angiography reveals hypervascularization of the anterior wall, chaotic branching of vessels.
If the placenta is retained, the volume of blood lost is estimated (abnormal blood loss is more than 400-500 ml). If a surgical operation is necessary, a coagulogram and a clinical blood test are examined. Differential diagnosis is carried out with a delay in the birth of the separated placenta, primarily with its infringement due to uneven or spastic contractions of the myometrium.
Treatment of delayed separation of the placenta
Conservative therapy
Therapeutic measures to promote the separation of the placenta are carried out only in the absence of pathological bleeding, and can last for 20-30 minutes. With the ineffectiveness of conservative treatment, surgical methods are used; in case of pathological blood loss, replacement blood transfusion is performed. Therapy is aimed at strengthening uterine contractions and includes:
With the ineffectiveness of conservative treatment, surgical methods are used; in case of pathological blood loss, replacement blood transfusion is performed. Therapy is aimed at strengthening uterine contractions and includes:
- Bladder catheterization. Since the muscular layer of the bladder is closely connected with the nerve fibers of the uterine muscles, irritation of the urothelial receptors leads to a reflex contraction of the myometrium. Catheterization normalizes the course of the afterbirth period of childbirth, contributes to the timely separation and release of the placenta.
- Medicines. Intravenous or intramuscular administration of uterotonic drugs (oxytocin preparations are preferred) in combination with cord traction is indicated to enhance labor activity. In parallel, intravenous transfusion of crystalloid solutions is performed to correct possible blood loss.
Surgical treatment
Surgical treatment of delayed separation can be performed non-surgical or operatively.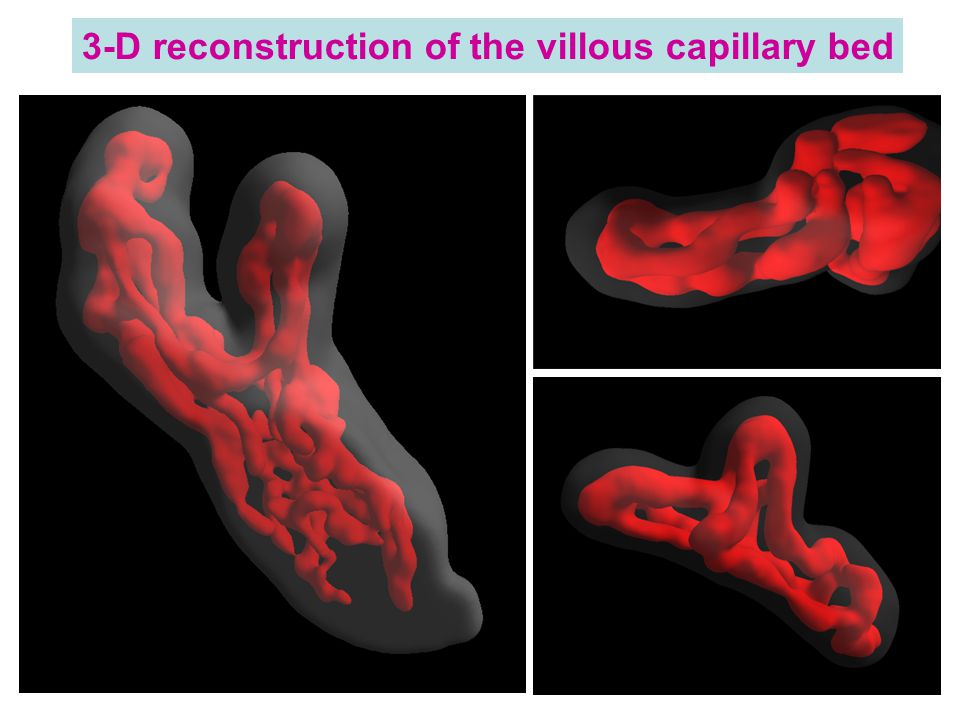 Treatment tactics depend on the cause of the pathology. Surgical intervention should be carried out in a timely manner, before the onset of generalized coagulopathy against the background of massive bleeding (otherwise, the operation aggravates the severity of the condition). In order to stop bleeding, embolization of the uterine vessels, the imposition of hemostatic sutures are used.
Treatment tactics depend on the cause of the pathology. Surgical intervention should be carried out in a timely manner, before the onset of generalized coagulopathy against the background of massive bleeding (otherwise, the operation aggravates the severity of the condition). In order to stop bleeding, embolization of the uterine vessels, the imposition of hemostatic sutures are used.
- Handbook. In case of tight attachment of the child's place or other reasons for the delay in its detachment (with the exception of true increment), manual separation of the placenta is performed with its subsequent removal to the outside. To avoid traumatic shock, intravenous anesthesia is performed before manipulation. Antibiotics (penicillin, cephalosporin) are used to prevent septic complications.
- Surgery. Indicated for failure of conservative bleeding management, true increment. The volume can vary from organ-preserving surgery (excision of the area of a partially ingrown child with affected myometrium and subsequent plasty) to radical (extirpation of the uterus, supravaginal amputation) with complete ingrowth, intractable bleeding.
Forecast and prevention
In case of timely started adequate treatment, the prognosis for life is favorable. The possibility of further implementation of the reproductive function largely depends on the presence of complications, the cause of the delay in the separation of the placenta. Primary prevention consists in the fight against abortion, the treatment of inflammatory diseases and the correction of endocrine disorders at the stage of preconception preparation. An important aspect of secondary prevention is a planned obstetric ultrasound during the gestation period, which allows early detection of placental accreta and the choice of tactics of labor management.
Delayed placenta - causes, symptoms, diagnosis and treatment
Delayed placenta is a complication of the third stage of labor, a condition in which the placenta does not fully or partially exfoliate from the uterine walls. Clinically, it can be manifested by pathological bleeding or the absence of bloody discharge normal for this period, soreness, or the absence of attempts. In this case, the standing of the bottom of the uterus corresponds to the period after the expulsion of the fetus, the connection of the umbilical cord with the uterus is indirectly determined. The diagnosis is established on the basis of the results of a physical examination, ultrasound. Most often, manual separation of the placenta or surgical treatment is performed.
In this case, the standing of the bottom of the uterus corresponds to the period after the expulsion of the fetus, the connection of the umbilical cord with the uterus is indirectly determined. The diagnosis is established on the basis of the results of a physical examination, ultrasound. Most often, manual separation of the placenta or surgical treatment is performed.
General
According to the WHO definition, retained placenta is diagnosed if separation does not occur within half an hour after the end of the second stage of labour. The incidence of pathology is 0.8-1.2% of all births. This complication is more often recorded in multiparous, especially those with a history of caesarean section. The disease is a serious problem of modern obstetrics, as it is often accompanied by postpartum hemorrhage. Bleeding is the cause of maternal death in a quarter of cases, 30% of which are the result of delayed separation of the placenta.
Delayed separation of the placenta
Causes
The etiology of delayed separation of the placenta has not been fully understood.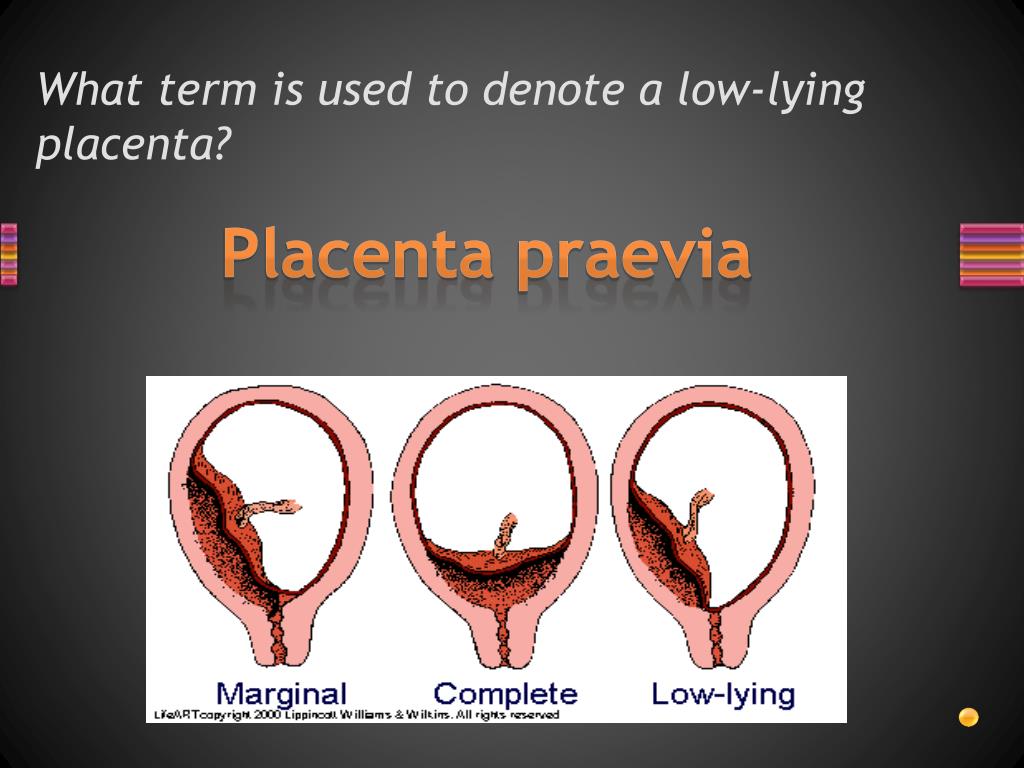 Violations of detachment of the placenta and its parts in the afterbirth period, on the one hand, may be due to defects in uterine contractile activity, on the other hand, due to excessively tight attachment of the child's place. Most women in labor fail to detect any visible disorders. The main causes of pathology include:
Violations of detachment of the placenta and its parts in the afterbirth period, on the one hand, may be due to defects in uterine contractile activity, on the other hand, due to excessively tight attachment of the child's place. Most women in labor fail to detect any visible disorders. The main causes of pathology include:
- Hypotension of the uterus. Weak contractions of the uterine muscles are not enough to start the process of separation of the placenta, even if the placenta does not have specific features that prevent detachment. In the presence of predisposing conditions, a slight decrease in contractile function can become a trigger for the development of pathology.
- Tight attachment of the placenta. Due to the depletion of the basal layer of the decidua and is characterized by a stronger than normal connection with the uterine walls without the germination of the chorionic villi into the myometrium. With the pathology under consideration, the force of uterine contractions is not enough to completely separate the placenta, which leads to bleeding.
- True placental accreta. Also associated with underdevelopment of the basal layer, however, in this case, there is invasion of the villi into the muscle tissue, and in rare cases, the serosa of the uterus. More common with placenta previa. Spontaneous detachment of the adherent child's place is impossible, manual separation can lead to perforation of the uterine wall.
- Anomalies in the development of the placenta. Delayed detachment is often observed with developmental anomalies (lobed, two- and three-lobed or with additional lobules) of the placenta. The separation of the afterbirth is difficult with the so-called "membraneous" placenta, which is characterized by a slight thickness and a large attachment area, often extending to the entire uterine wall.
The most significant risk factors are the endometritis transferred before the onset of pregnancy, obstetric history (surgery on the uterus, abortions, multiple births), indicating traumatic injuries. Inflammation and trauma lead to anatomical and histological changes in the uterus, which negatively affects placentogenesis and myometrial tone. Predisposing conditions include hyperandrogenism, malformations of the uterus (bicornuate uterus, intrauterine septum), volumetric formations (myoma, nodular adenomyosis).
Inflammation and trauma lead to anatomical and histological changes in the uterus, which negatively affects placentogenesis and myometrial tone. Predisposing conditions include hyperandrogenism, malformations of the uterus (bicornuate uterus, intrauterine septum), volumetric formations (myoma, nodular adenomyosis).
Pathogenesis
Normally, after the birth of the fetus, afterbirth contractions appear, in which contractions spread to the entire uterus, including the placental site (previously, the muscles of this zone did not function). Labor activity leads to detachment of the child's place in the area of the spongy layer of the mucosa (with the preservation of the basal layer), and then to its exit to the outside. The separation of the placenta is accompanied by damage to blood vessels, physiological bleeding. After his birth, the uterus contracts, which helps to stop the bleeding.
In the presence of unfavorable factors and predisposing conditions, detachment is difficult.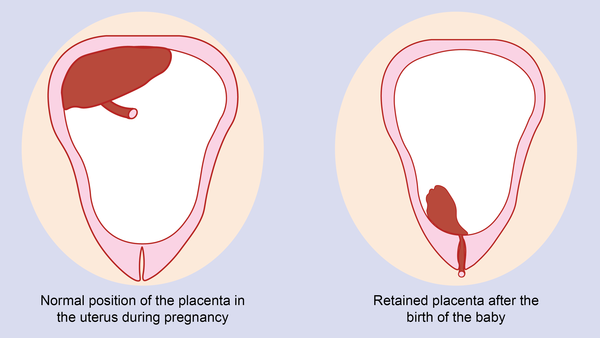 With partial detachment, if the process started, but for some reason stopped, the gaping vessels of the uncontracted uterus become a source of pathological blood loss. Ingrown chorionic villi deep into the myometrium lead to thinning of the uterine wall, so an attempt to manually separate the placenta quickly ends in trauma, accompanied by intense bleeding.
With partial detachment, if the process started, but for some reason stopped, the gaping vessels of the uncontracted uterus become a source of pathological blood loss. Ingrown chorionic villi deep into the myometrium lead to thinning of the uterine wall, so an attempt to manually separate the placenta quickly ends in trauma, accompanied by intense bleeding.
Symptoms
Subjective signs of delayed separation of the placenta include prolonged, painful, ineffective attempts after the birth of a child or their complete absence. An objective sign is intense bleeding observed with partial separation. If detachment of the placenta does not occur at all, even in a partial volume (for example, with a complete increment), bloody discharge from the birth canal may be absent.
Complications
The most common complication of delayed separation of the placenta is bleeding. Significant blood loss leads to such a potentially fatal complication as hemorrhagic shock, accompanied by multiple organ failure. Massive bleeding often develops when professional medical care is not provided in time (the risk increases sharply during childbirth outside a medical institution).
Massive bleeding often develops when professional medical care is not provided in time (the risk increases sharply during childbirth outside a medical institution).
Other frequent complications of this pathology include purulent-inflammatory diseases (postpartum endometritis, pelvioperitonitis, obstetric sepsis), which can be the result of both surgical treatment and retention of placenta fragments in the uterine cavity. In addition, the remaining ingrown placenta can become a source of late postpartum hemorrhage, uterine rupture during a subsequent pregnancy.
Diagnosis
The diagnosis of retained placenta is made by the obstetrician if there is no discharge of the placenta within thirty minutes after the birth of the infant with appropriate results of the physical examination. To establish the causes of the pathological condition (which determines the choice of treatment tactics), an ultrasound examination is additionally used.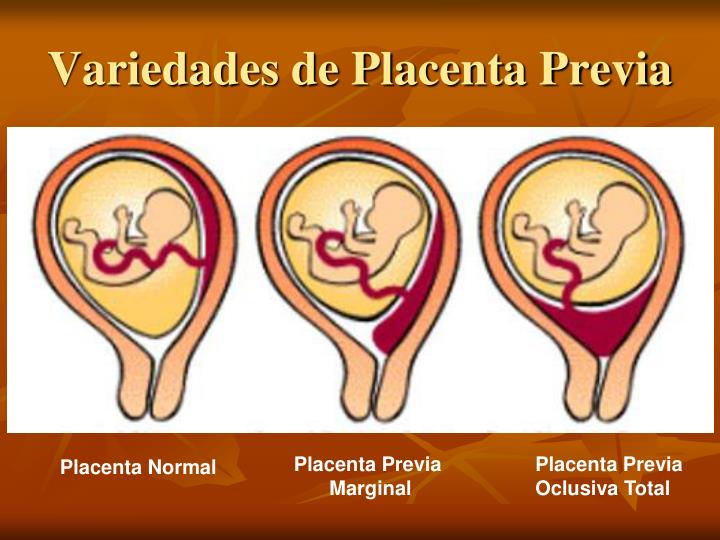
- Clinical examination. Signs of delayed separation of the placenta are determined by the shape and location of the uterus, the mobility of the umbilical cord. If separation has not occurred, the uterus is rounded, the bottom is located at the navel (Schroeder's sign), the outer segment of the umbilical cord does not lengthen (Alfeld's sign). The umbilical cord retracts with pressure over the womb (Kyustner-Chukalov's sign), after inhalation (Dovzhenko's sign), straining (Klein's sign).
- Ultrasonography. Ultrasound of the uterus is prescribed for the diagnosis of placenta accreta. Ultrasound signs of this pathology include deformation of the internal contour of the uterine cavity, its uneven expansion, and the absence of a hypoechoic layer between the myometrium and the placenta. Ultrasound angiography reveals hypervascularization of the anterior wall, chaotic branching of vessels.
If the placenta is retained, the volume of blood lost is estimated (abnormal blood loss is more than 400-500 ml). If a surgical operation is necessary, a coagulogram and a clinical blood test are examined. Differential diagnosis is carried out with a delay in the birth of the separated placenta, primarily with its infringement due to uneven or spastic contractions of the myometrium.
If a surgical operation is necessary, a coagulogram and a clinical blood test are examined. Differential diagnosis is carried out with a delay in the birth of the separated placenta, primarily with its infringement due to uneven or spastic contractions of the myometrium.
Treatment of delayed separation of the placenta
Conservative therapy
Therapeutic measures to promote the separation of the placenta are carried out only in the absence of pathological bleeding, and can last for 20-30 minutes. With the ineffectiveness of conservative treatment, surgical methods are used; in case of pathological blood loss, replacement blood transfusion is performed. Therapy is aimed at strengthening uterine contractions and includes:
- Bladder catheterization. Since the muscular layer of the bladder is closely connected with the nerve fibers of the uterine muscles, irritation of the urothelial receptors leads to a reflex contraction of the myometrium.
 Catheterization normalizes the course of the afterbirth period of childbirth, contributes to the timely separation and release of the placenta.
Catheterization normalizes the course of the afterbirth period of childbirth, contributes to the timely separation and release of the placenta. - Medicines. Intravenous or intramuscular administration of uterotonic drugs (oxytocin preparations are preferred) in combination with cord traction is indicated to enhance labor activity. In parallel, intravenous transfusion of crystalloid solutions is performed to correct possible blood loss.
Surgical treatment
Surgical treatment of delayed separation can be performed non-surgical or operatively. Treatment tactics depend on the cause of the pathology. Surgical intervention should be carried out in a timely manner, before the onset of generalized coagulopathy against the background of massive bleeding (otherwise, the operation aggravates the severity of the condition). In order to stop bleeding, embolization of the uterine vessels, the imposition of hemostatic sutures are used.
- Handbook. In case of tight attachment of the child's place or other reasons for the delay in its detachment (with the exception of true increment), manual separation of the placenta is performed with its subsequent removal to the outside. To avoid traumatic shock, intravenous anesthesia is performed before manipulation. Antibiotics (penicillin, cephalosporin) are used to prevent septic complications.
- Surgery. Indicated for failure of conservative bleeding management, true increment. The volume can vary from organ-preserving surgery (excision of the area of a partially ingrown child with affected myometrium and subsequent plasty) to radical (extirpation of the uterus, supravaginal amputation) with complete ingrowth, intractable bleeding.
Forecast and prevention
In case of timely started adequate treatment, the prognosis for life is favorable. The possibility of further implementation of the reproductive function largely depends on the presence of complications, the cause of the delay in the separation of the placenta.