Symptoms preeclampsia during pregnancy
Preeclampsia - Symptoms and causes
Overview
Preeclampsia is a complication of pregnancy. With preeclampsia, you might have high blood pressure, high levels of protein in urine that indicate kidney damage (proteinuria), or other signs of organ damage. Preeclampsia usually begins after 20 weeks of pregnancy in women whose blood pressure had previously been in the standard range.
Left untreated, preeclampsia can lead to serious — even fatal — complications for both the mother and baby.
Early delivery of the baby is often recommended. The timing of delivery depends on how severe the preeclampsia is and how many weeks pregnant you are. Before delivery, preeclampsia treatment includes careful monitoring and medications to lower blood pressure and manage complications.
Preeclampsia may develop after delivery of a baby, a condition known as postpartum preeclampsia.
Products & Services
- Book: Mayo Clinic Guide to a Healthy Pregnancy
Symptoms
The defining feature of preeclampsia is high blood pressure, proteinuria, or other signs of damage to the kidneys or other organs. You may have no noticeable symptoms. The first signs of preeclampsia are often detected during routine prenatal visits with a health care provider.
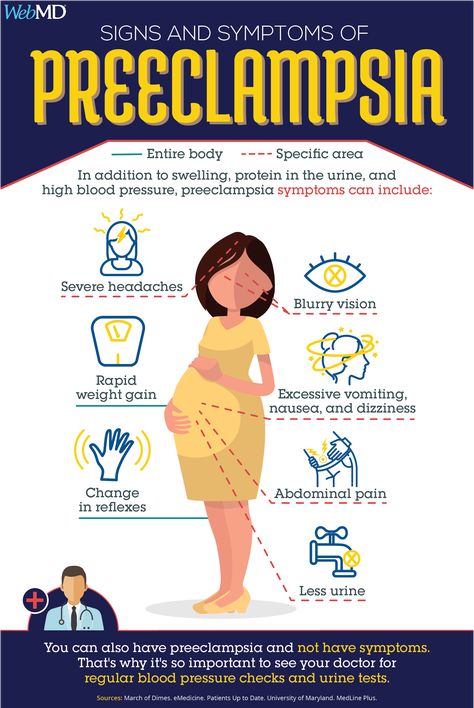
Along with high blood pressure, preeclampsia signs and symptoms may include:
- Excess protein in urine (proteinuria) or other signs of kidney problems
- Decreased levels of platelets in blood (thrombocytopenia)
- Increased liver enzymes that indicate liver problems
- Severe headaches
- Changes in vision, including temporary loss of vision, blurred vision or light sensitivity
- Shortness of breath, caused by fluid in the lungs
- Pain in the upper belly, usually under the ribs on the right side
- Nausea or vomiting
Weight gain and swelling (edema) are typical during healthy pregnancies. However, sudden weight gain or a sudden appearance of edema — particularly in your face and hands — may be a sign of preeclampsia.
When to see a doctor
Make sure you attend your prenatal visits so that your health care provider can monitor your blood pressure.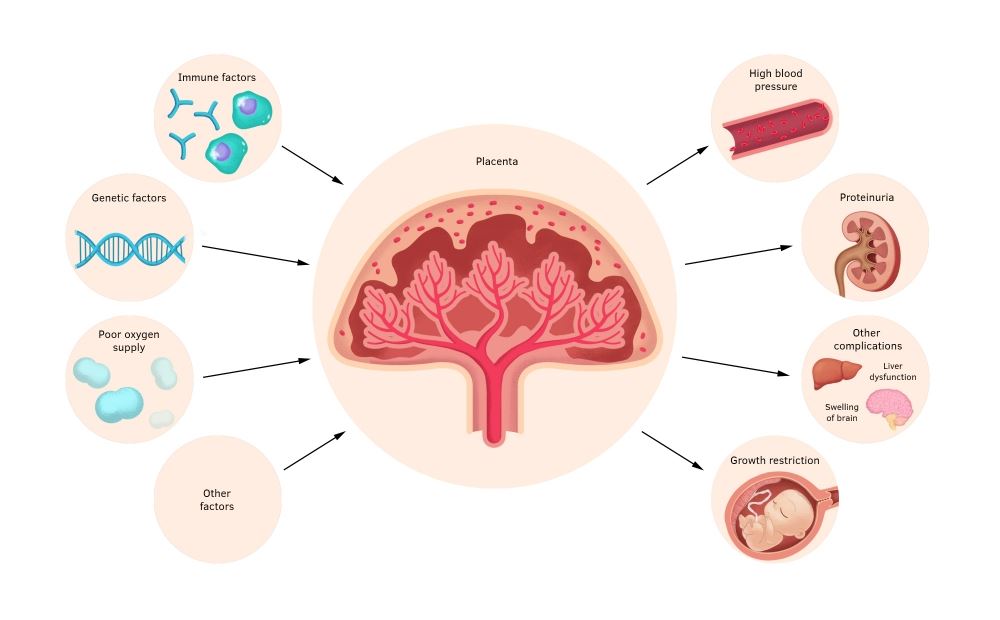 Contact your provider immediately or go to an emergency room if you have severe headaches, blurred vision or other visual disturbances, severe belly pain, or severe shortness of breath.
Contact your provider immediately or go to an emergency room if you have severe headaches, blurred vision or other visual disturbances, severe belly pain, or severe shortness of breath.
Because headaches, nausea, and aches and pains are common pregnancy complaints, it's difficult to know when new symptoms are simply part of being pregnant and when they may indicate a serious problem — especially if it's your first pregnancy. If you're concerned about your symptoms, contact your doctor.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which
information is beneficial, we may combine your email and website usage information with
other information we have about you. If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
Causes
The exact cause of preeclampsia likely involves several factors. Experts believe it begins in the placenta — the organ that nourishes the fetus throughout pregnancy. Early in a pregnancy, new blood vessels develop and evolve to supply oxygen and nutrients to the placenta.
In women with preeclampsia, these blood vessels don't seem to develop or work properly.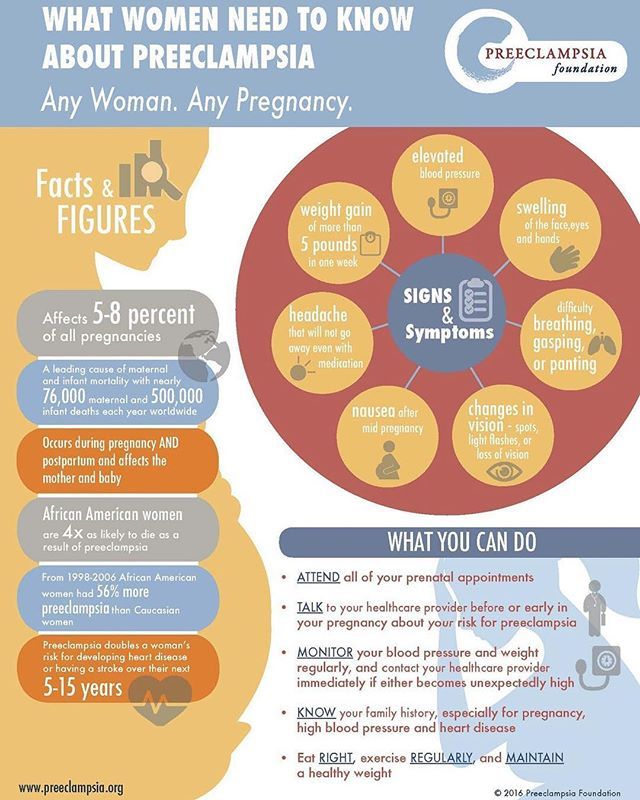 Problems with how well blood circulates in the placenta may lead to the irregular regulation of blood pressure in the mother.
Problems with how well blood circulates in the placenta may lead to the irregular regulation of blood pressure in the mother.
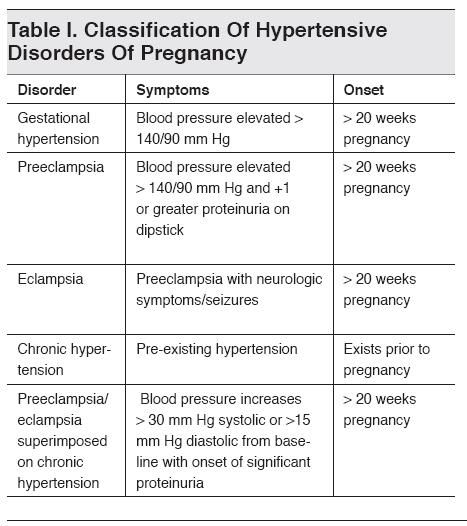
Other high blood pressure disorders during pregnancy
Preeclampsia is one high blood pressure (hypertension) disorder that can occur during pregnancy. Other disorders can happen, too:
- Gestational hypertension is high blood pressure that begins after 20 weeks without problems in the kidneys or other organs. Some women with gestational hypertension may develop preeclampsia.
- Chronic hypertension is high blood pressure that was present before pregnancy or that occurs before 20 weeks of pregnancy. High blood pressure that continues more than three months after a pregnancy also is called chronic hypertension.
- Chronic hypertension with superimposed preeclampsia occurs in women diagnosed with chronic high blood pressure before pregnancy, who then develop worsening high blood pressure and protein in the urine or other health complications during pregnancy.

Risk factors
Conditions that are linked to a higher risk of preeclampsia include:
- Preeclampsia in a previous pregnancy
- Being pregnant with more than one baby
- Chronic high blood pressure (hypertension)
- Type 1 or type 2 diabetes before pregnancy
- Kidney disease
- Autoimmune disorders
- Use of in vitro fertilization
Conditions that are associated with a moderate risk of developing preeclampsia include:
- First pregnancy with current partner
- Obesity
- Family history of preeclampsia
- Maternal age of 35 or older
- Complications in a previous pregnancy
- More than 10 years since previous pregnancy
Other risk factors
Several studies have shown a greater risk of preeclampsia among Black women compared with other women. There's also some evidence of an increased risk among indigenous women in North America.
A growing body of evidence suggests that these differences in risk may not necessarily be based on biology. A greater risk may be related to inequities in access to prenatal care and health care in general, as well as social inequities and chronic stressors that affect health and well-being.
Lower income also is associated with a greater risk of preeclampsia likely because of access to health care and social factors affecting health.
For the purposes of making decisions about prevention strategies, a Black woman or a woman with a low income has a moderately increased risk of developing preeclampsia.
Complications
Complications of preeclampsia may include:
- Fetal growth restriction. Preeclampsia affects the arteries carrying blood to the placenta. If the placenta doesn't get enough blood, the baby may receive inadequate blood and oxygen and fewer nutrients. This can lead to slow growth known as fetal growth restriction.
- Preterm birth.
 Preeclampsia may lead to an unplanned preterm birth — delivery before 37 weeks. Also, planned preterm birth is a primary treatment for preeclampsia. A baby born prematurely has increased risk of breathing and feeding difficulties, vision or hearing problems, developmental delays, and cerebral palsy. Treatments before preterm delivery may decrease some risks.
Preeclampsia may lead to an unplanned preterm birth — delivery before 37 weeks. Also, planned preterm birth is a primary treatment for preeclampsia. A baby born prematurely has increased risk of breathing and feeding difficulties, vision or hearing problems, developmental delays, and cerebral palsy. Treatments before preterm delivery may decrease some risks. - Placental abruption. Preeclampsia increases your risk of placental abruption. With this condition, the placenta separates from the inner wall of the uterus before delivery. Severe abruption can cause heavy bleeding, which can be life-threatening for both the mother and baby.
-
HELLP syndrome. HELLP stands for hemolysis (the destruction of red blood cells), elevated liver enzymes and low platelet count.
 This severe form of preeclampsia affects several organ systems. HELLP syndrome is life-threatening to the mother and baby, and it may cause lifelong health problems for the mother.
This severe form of preeclampsia affects several organ systems. HELLP syndrome is life-threatening to the mother and baby, and it may cause lifelong health problems for the mother.Signs and symptoms include nausea and vomiting, headache, upper right belly pain, and a general feeling of illness or being unwell. Sometimes, it develops suddenly, even before high blood pressure is detected. It also may develop without any symptoms.
-
Eclampsia. Eclampsia is the onset of seizures or coma with signs or symptoms of preeclampsia. It is very difficult to predict whether a patient with preeclampsia will develop eclampsia. Eclampsia can happen without any previously observed signs or symptoms of preeclampsia.
Signs and symptoms that may appear before seizures include severe headaches, vision problems, mental confusion or altered behaviors.
 But, there are often no symptoms or warning signs. Eclampsia may occur before, during or after delivery.
But, there are often no symptoms or warning signs. Eclampsia may occur before, during or after delivery. - Other organ damage. Preeclampsia may result in damage to the kidneys, liver, lung, heart, or eyes, and may cause a stroke or other brain injury. The amount of injury to other organs depends on how severe the preeclampsia is.
- Cardiovascular disease. Having preeclampsia may increase your risk of future heart and blood vessel (cardiovascular) disease. The risk is even greater if you've had preeclampsia more than once or you've had a preterm delivery.
Prevention
Medication
The best clinical evidence for prevention of preeclampsia is the use of low-dose aspirin. Your primary care provider may recommend taking an 81-milligram aspirin tablet daily after 12 weeks of pregnancy if you have one high-risk factor for preeclampsia or more than one moderate-risk factor.
It's important that you talk with your provider before taking any medications, vitamins or supplements to make sure it's safe for you.
Lifestyle and healthy choices
Before you become pregnant, especially if you've had preeclampsia before, it's a good idea to be as healthy as you can be. Talk to your provider about managing any conditions that increase the risk of preeclampsia.
By Mayo Clinic Staff
Related
Associated Procedures
News from Mayo Clinic
Products & Services
Symptoms, Causes, Treatments & Prevention
Overview
What is preeclampsia?
Preeclampsia is a serious blood pressure condition that develops during pregnancy. People with preeclampsia often have high blood pressure (hypertension) and high levels of protein in their urine (proteinuria). Preeclampsia typically develops after the 20th week of pregnancy. It can also affect other organs in the body and be dangerous for both the mom and her developing fetus. Because of these risks, preeclampsia needs to be treated by a healthcare provider.
What happens when you have preeclampsia?
When you have preeclampsia, your blood pressure is elevated (higher than 140/90 mmHg), and you may have high levels of protein in your urine. Preeclampsia puts stress on your heart and other organs and can cause serious complications. It can also affect the blood supply to your placenta, impair liver and kidney function or cause fluid to build up in your lungs. The protein in your urine is a sign of kidney dysfunction.
Preeclampsia puts stress on your heart and other organs and can cause serious complications. It can also affect the blood supply to your placenta, impair liver and kidney function or cause fluid to build up in your lungs. The protein in your urine is a sign of kidney dysfunction.
How common is preeclampsia?
Preeclampsia is a condition unique to pregnancy that complicates up to 8% of all deliveries worldwide. In the United States, it's the cause of about 15% of premature deliveries (delivery before 37 weeks of pregnancy).
Who gets preeclampsia?
Preeclampsia may be more common in first-time mothers. Healthcare providers are not entirely sure why some people develop preeclampsia. Some factors that may put you at a higher risk are:
- History of high blood pressure, kidney disease or diabetes.
- Expecting multiples.
- Family history of preeclampsia.
- Autoimmune conditions like lupus.
- Obesity.
Symptoms and Causes
What are the symptoms?
Many people with preeclampsia do not have any symptoms. For those that do, some of the first signs of preeclampsia are high blood pressure, protein in the urine and retaining water (this can cause weight gain and swelling).
For those that do, some of the first signs of preeclampsia are high blood pressure, protein in the urine and retaining water (this can cause weight gain and swelling).
Other signs of preeclampsia include:
- Headaches.
- Blurry vision or light sensitivity.
- Dark spots appearing in your vision.
- Right side abdominal pain.
- Swelling in your hands and face (edema).
- Shortness of breath.
It's essential to share all of your pregnancy symptoms with your healthcare provider. Many people are unaware they have preeclampsia until their blood pressure and urine are checked at a prenatal appointment.
Severe preeclampsia may include symptoms like:
- Hypertensive emergency (blood pressure is 160/110 mmHg or higher).
- Decreased kidney or liver function.
- Fluid in the lungs.
- Low blood platelet levels (thrombocytopenia).
- Decreased urine production
If your preeclampsia is severe, you may be admitted to the hospital for closer observation or need to deliver your baby as soon as possible. Your healthcare provider may give you medications for high blood pressure or to help the fetus's lungs develop before delivery.
Your healthcare provider may give you medications for high blood pressure or to help the fetus's lungs develop before delivery.
What causes preeclampsia?
No one is entirely sure. Preeclampsia is believed to come from a problem with the health of the placenta (the organ that develops in the uterus during pregnancy and is responsible for providing oxygen and nutrients to the fetus). The blood supply to the placenta might be decreased in preeclampsia, and this can lead to problems with both you and the fetus.
Does stress cause preeclampsia?
While stress may impact blood pressure, stress is not one of the direct causes of preeclampsia. While some stress is unavoidable during pregnancy, avoiding high-stress situations or learning to manage your stress is a good idea.
What week of pregnancy does preeclampsia start?
Preeclampsia typically occurs after 20 weeks of pregnancy, but it can come earlier. Most preeclampsia occurs at or near term (37 weeks gestation).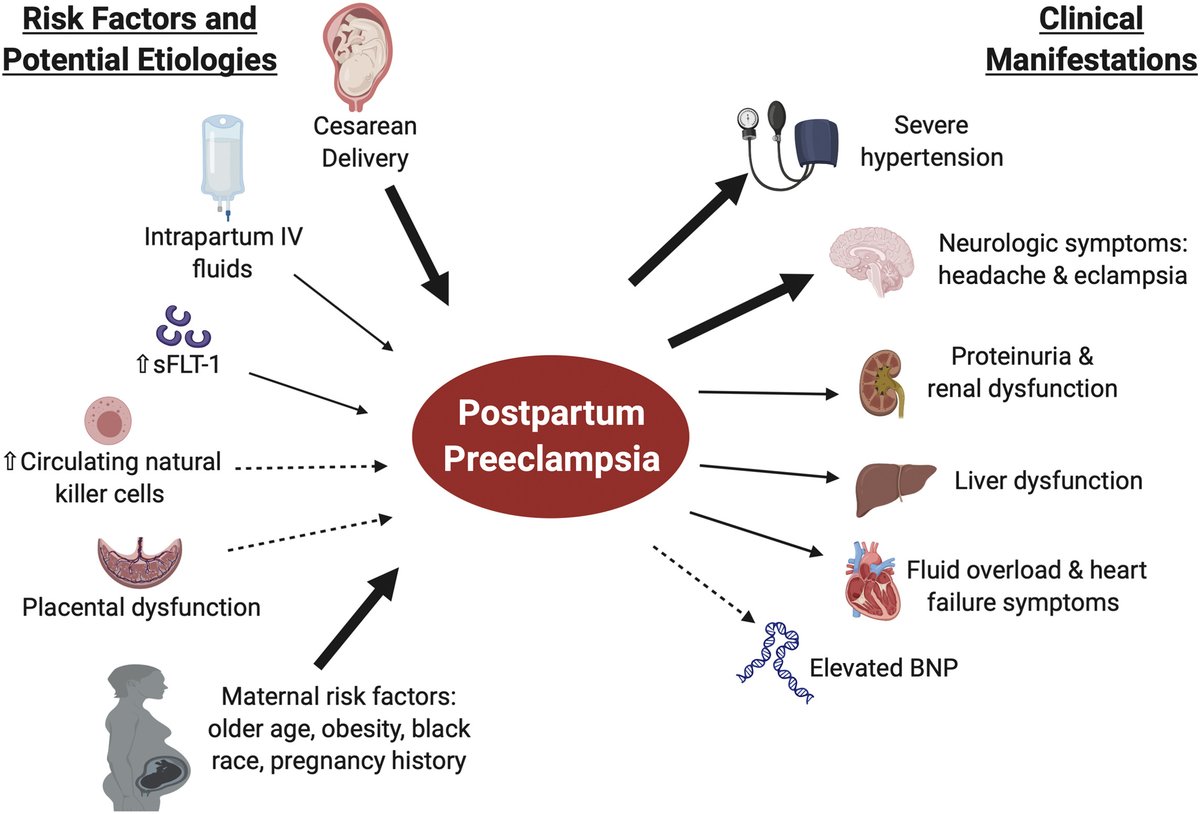 Preeclampsia can also come after delivery (postpartum preeclampsia), which usually occurs between the first few days to one week after delivery. In rare cases, it begins weeks after delivery.
Preeclampsia can also come after delivery (postpartum preeclampsia), which usually occurs between the first few days to one week after delivery. In rare cases, it begins weeks after delivery.
Will preeclampsia affect my baby?
Preeclampsia can cause preterm delivery (your baby needing delivered early). Premature babies are at increased risk for health complications like low birth weight and respiratory issues.
Diagnosis and Tests
How is it diagnosed?
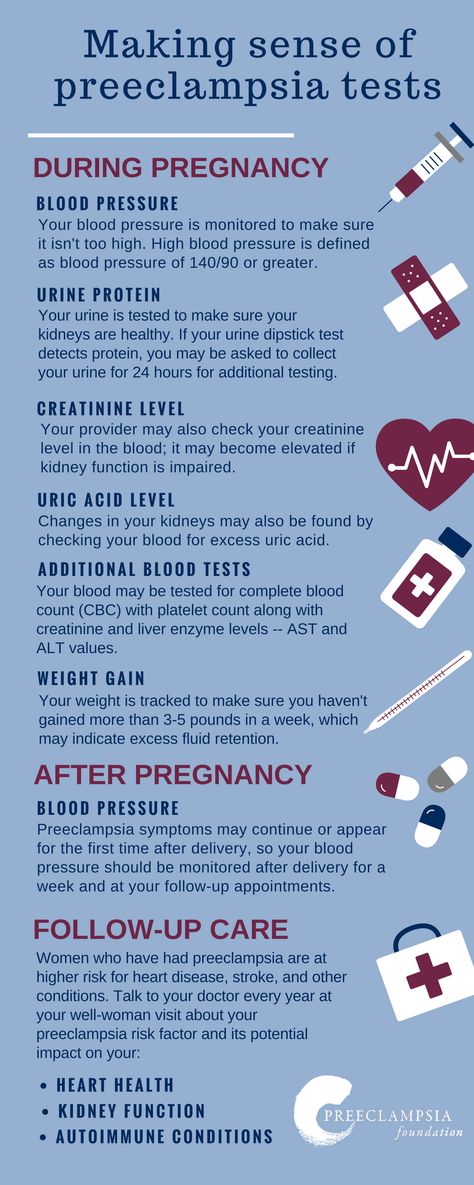
Preeclampsia is often diagnosed during routine prenatal appointments when your healthcare provider checks your weight gain, blood pressure and urine.
If preeclampsia is suspected, your healthcare provider may:
- Order additional blood tests to check kidney and liver functions.
- Suggest a 24-hour urine collection to watch for proteinuria.
- Perform an ultrasound and other fetal monitoring to look at the size of the fetus and assess the amniotic fluid volume.
Preeclampsia can be categorized as mild or severe. You may be diagnosed with mild preeclampsia if you have high blood pressure plus high levels of protein in your urine.
You may be diagnosed with mild preeclampsia if you have high blood pressure plus high levels of protein in your urine.
You are diagnosed with severe preeclampsia if you have symptoms of mild preeclampsia plus:
- Signs of kidney or liver damage (seen in blood work).
- Low platelet count
- Fluid in your lungs.
- Headaches and dizziness.
- Visual impairment or seeing spots.
Management and Treatment
How is preeclampsia treated?
Your healthcare provider will advise you on the best way to treat preeclampsia. Treatment generally depends on how severe your preeclampsia is and how far along you are in pregnancy.
If you're close to full term (37 weeks pregnant or greater), your baby will probably be delivered early. You can still have a vaginal delivery, but sometimes a Cesarean delivery (C-section) is recommended. Your healthcare provider may give you medication to help the fetus's lungs develop and manage your blood pressure until the baby can be delivered. Sometimes it is safer to deliver the baby early than to risk prolonging the pregnancy.
Sometimes it is safer to deliver the baby early than to risk prolonging the pregnancy.
When preeclampsia develops earlier in pregnancy, you'll be monitored closely in an effort to prolong the pregnancy and allow for the fetus to grow and develop. You'll have more prenatal appointments, including ultrasounds, urine tests and blood draws. You may be asked to check your blood pressure at home. If you are diagnosed with severe preeclampsia, you could remain in the hospital until you deliver your baby.
If the preeclampsia worsens or becomes more severe, your baby will need to be delivered.
During labor and following delivery, people with preeclampsia are often given magnesium intravenously (directly into the vein) to prevent the development of eclampsia (seizures from preeclampsia).
Is there a cure for preeclampsia?
No, there isn't a cure for preeclampsia. Preeclampsia can only be cured with delivery. Your healthcare provider will still want to monitor you for several weeks after delivery to make sure your symptoms go away.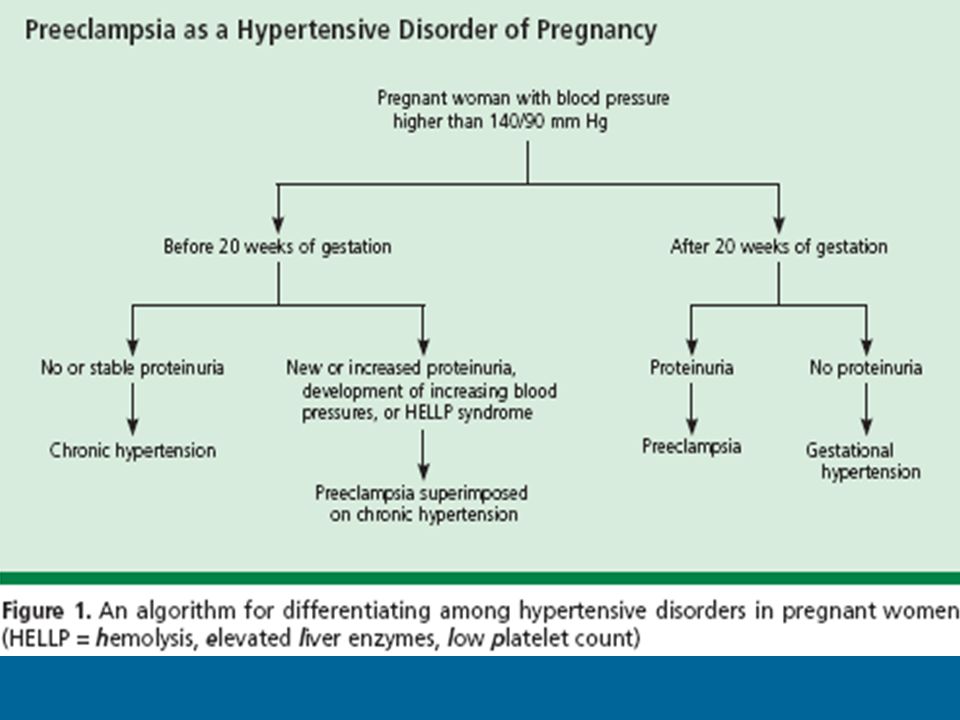
Prevention
How can I reduce my risk of getting preeclampsia?
For people with risk factors, there are some steps that can be taken prior to and during pregnancy to lower the chance of developing preeclampsia. These steps can include:
- Losing weight if you have overweight/obesity (prior to pregnancy-related weight gain).
- Controlling your blood pressure and blood sugar (if you had high blood pressure or diabetes prior to pregnancy).
- Maintaining a regular exercise routine.
- Getting enough sleep.
- Eating healthy foods that are low in salt and avoiding caffeine.
Can you prevent preeclampsia?
Taking a baby aspirin daily has been demonstrated to decrease your risk of developing preeclampsia by approximately 15%. If you have risk factors for preeclampsia, your healthcare provider may recommend starting aspirin in early pregnancy (by 12 weeks gestation).
Outlook / Prognosis
What are the most common complications of preeclampsia?
If left untreated, preeclampsia can be potentially fatal to both you and the fetus.
Before delivery, the most common complications are preterm birth, low birth weight or placental abruption.
Preeclampsia can cause HELLP syndrome (hemolysis, elevated liver enzymes and low platelet count). This happens when preeclampsia damages your liver and red blood cells and interferes with blood clotting. Other signs of HELLP syndrome are blurry vision, chest pain, headaches and nosebleeds.
After you've delivered your baby, you may be at an increased risk for:
- Kidney disease.
- Heart attack.
- Stroke.
- Developing preeclampsia in future pregnancies.
Does preeclampsia go away after delivery?
Preeclampsia typically goes away within days to weeks following delivery. Sometimes, your blood pressure can remain high for a few weeks after delivery, requiring treatment with medication. Your healthcare provider will work with you after your pregnancy to manage your blood pressure. People with preeclampsia — particularly those who develop the condition early in pregnancy — are at greater risk for high blood pressure (hypertension) and heart disease later in life. Knowing this information, those individuals can work with their primary care provider to take steps to reduce these risks.
Knowing this information, those individuals can work with their primary care provider to take steps to reduce these risks.
Living With
When should I see my healthcare provider?
Preeclampsia can be a fatal condition during pregnancy. If you're being treated for this condition, make sure to see your healthcare provider for all of your appointments and blood or urine tests. Contact your obstetrician if you have any concerns or questions about your symptoms.
Go to the nearest hospital if you're pregnant and experience the following:
- Symptoms of a seizure-like twitching or convulsing.
- Shortness of breath.
- Sharp pain in your abdomen (specifically the right side).
- Blurry vision.
- Severe headache that won't go away.
- Dark spots in your vision that don't go away.
What questions should I ask my doctor?
If your healthcare provider has diagnosed you with preeclampsia, it's normal to have concerns. Some common questions to ask your healthcare provider are:
Some common questions to ask your healthcare provider are:
- Do I need to take medication?
- Do I need to restrict my activities?
- What changes should I make to my diet?
- How often will you need to monitor my health during pregnancy?
- Will I need to deliver my baby early?
- How can I best manage preeclampsia?
Frequently Asked Questions
What's the difference between preeclampsia and eclampsia?
Eclampsia is severe preeclampsia that causes seizures. It's considered a complication of preeclampsia, but it can happen without signs of preeclampsia. In rare cases, it can lead to coma, stroke or death.
What is postpartum preeclampsia?
Postpartum preeclampsia is when you develop preeclampsia after your baby is born. It typically happens within two days of giving birth but can also develop several weeks later. The signs of postpartum preeclampsia are similar to preeclampsia and include swelling in your limbs and extremities, headaches, seeing spots, stomach pains and nausea. It's a serious condition that can cause seizures, stroke and organ damage.
It's a serious condition that can cause seizures, stroke and organ damage.
A note from Cleveland Clinic
Preeclampsia is a serious condition that you may not be aware you even have. It's important to go to all your prenatal appointments and be open about all the symptoms you feel during pregnancy. When preeclampsia is caught early, it can be treated and managed to keep both you and the fetus safe and healthy. Most people with preeclampsia go on to have healthy babies.
Preeclampsia and pregnancy | Ida-Tallinna Keskhaigla
The purpose of this leaflet is to provide the patient with information about the nature, occurrence, risk factors, symptoms and treatment of preeclampsia.
What is preeclampsia?
Pre-eclampsia is a disease that occurs during pregnancy and is characterized by high blood pressure and protein in the urine.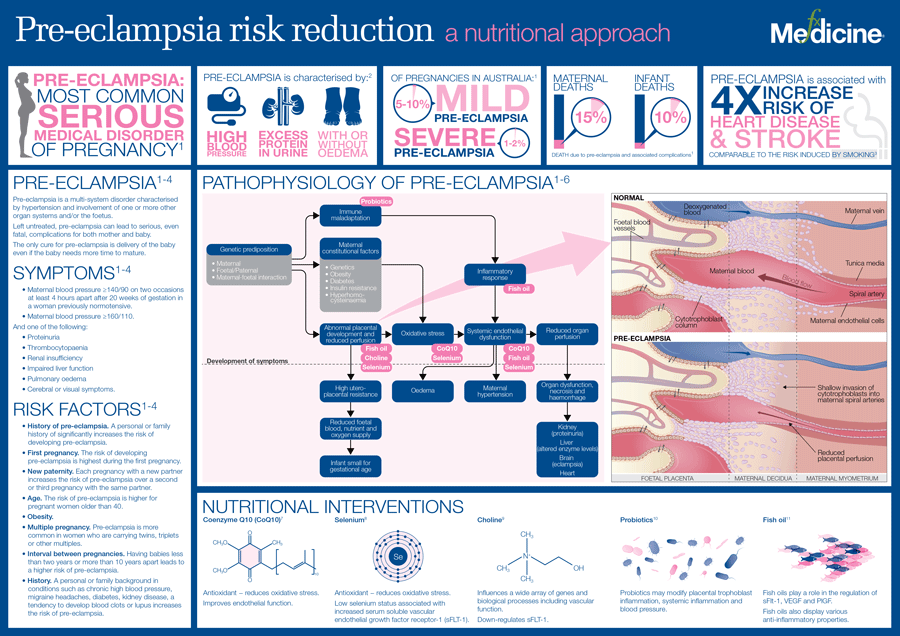 Preeclampsia is one of the most common complications of pregnancy. Epilepsy-like seizures occur in severe preeclampsia and are life-threatening.
Preeclampsia is one of the most common complications of pregnancy. Epilepsy-like seizures occur in severe preeclampsia and are life-threatening.
What symptoms may indicate the development of preeclampsia?
High blood pressure - blood pressure values are 140/90 mmHg. Art. or higher. If systolic (upper) or diastolic (lower) blood pressure rises by 30 mm Hg. Art. or more, then such an increase cannot be ignored.
Protein in urine - 300 mg in urine collected over 24 hours, or +1 value on a rapid test.
Swelling of the arms, legs or face , especially under the eyes or if the swelling leaves a depression in the skin when pressed. Edema can occur in all pregnant women and is generally harmless, but rapidly developing edema should be taken into account.
Headache that does not improve after taking pain medication.
Visual disturbances - double vision or blurred vision, dots or flashes before the eyes, auras.
Nausea or pain in the upper abdomen - These symptoms are often mistaken for indigestion or gallbladder pain. Nausea in the second half of pregnancy is not normal.
Sudden weight gain - 2 kg or more per week.
As a rule, there is a mild course of the disease that occurs at the end of pregnancy and has a good prognosis. Sometimes, preeclampsia can worsen quickly and be dangerous to both mother and fetus. In such cases, rapid diagnosis and careful monitoring of the mother and child are of paramount importance.
Unfortunately, most women show symptoms in the final stages of the disease. If you experience any of the above symptoms, you should contact your midwife, gynecologist, or the Women's Clinic emergency department.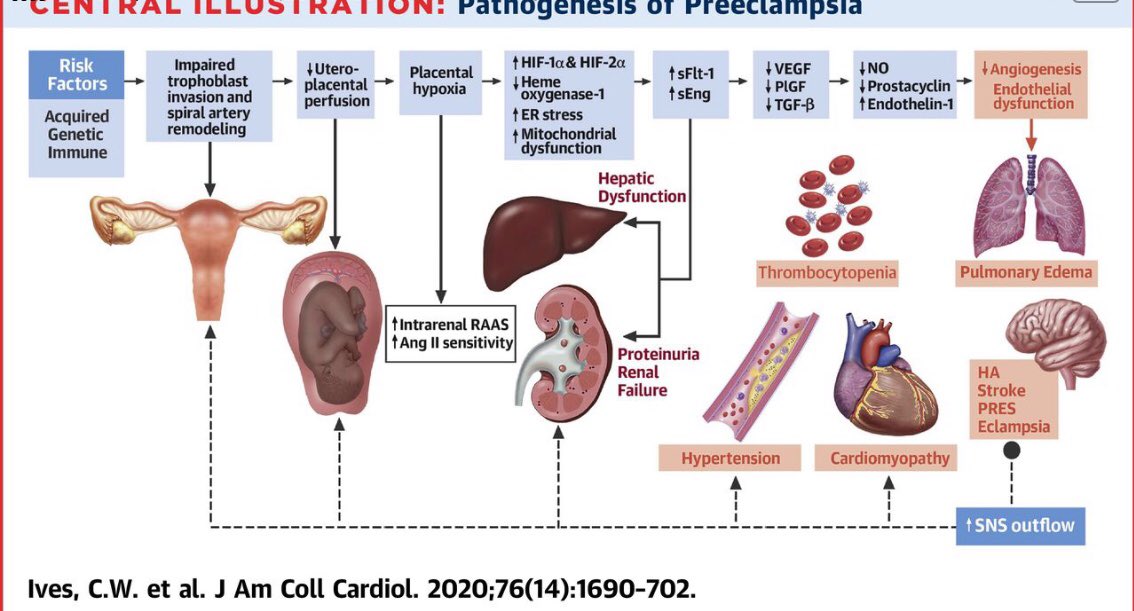
Is preeclampsia called toxemia of pregnancy?
Previously, pre-eclampsia was really called toxicosis, or toxemia, since it was believed that the cause of the disease was toxins, that is, poisons in the blood of a pregnant woman.
What is the difference between preeclampsia and gestational hypertension?
Pregnancy hypertension is an increase in blood pressure above normal after the 20th week of pregnancy. With hypertension of pregnant women, protein in the urine is not observed.
What is HELLP syndrome?
HELLP syndrome is one of the most severe forms of preeclampsia. HELLP syndrome is rare and sometimes develops before symptoms of preeclampsia appear. Sometimes the syndrome is difficult to diagnose, as the symptoms resemble gallbladder colic or a cold.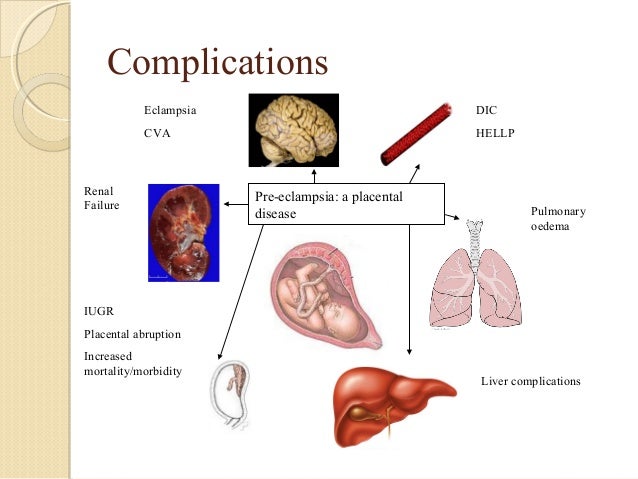
When does preeclampsia occur?
Preeclampsia usually occurs after the 20th week of pregnancy. As a rule, preeclampsia goes away after delivery, but complications can occur up to six weeks after delivery, during which careful monitoring of the condition is necessary. If by the sixth week after birth, blood pressure does not return to normal, then you need to contact a cardiologist, who will begin treatment against hypertension.
What is the cause of preeclampsia?
The causes of the disease are still not clear, there are only unproven hypotheses.
How does the disease affect pregnant women and pregnancy?
Most preeclamptic pregnancies have a favorable outcome and a healthy baby is born. However, the disease is very serious and is one of the most common causes of death of the child and mother.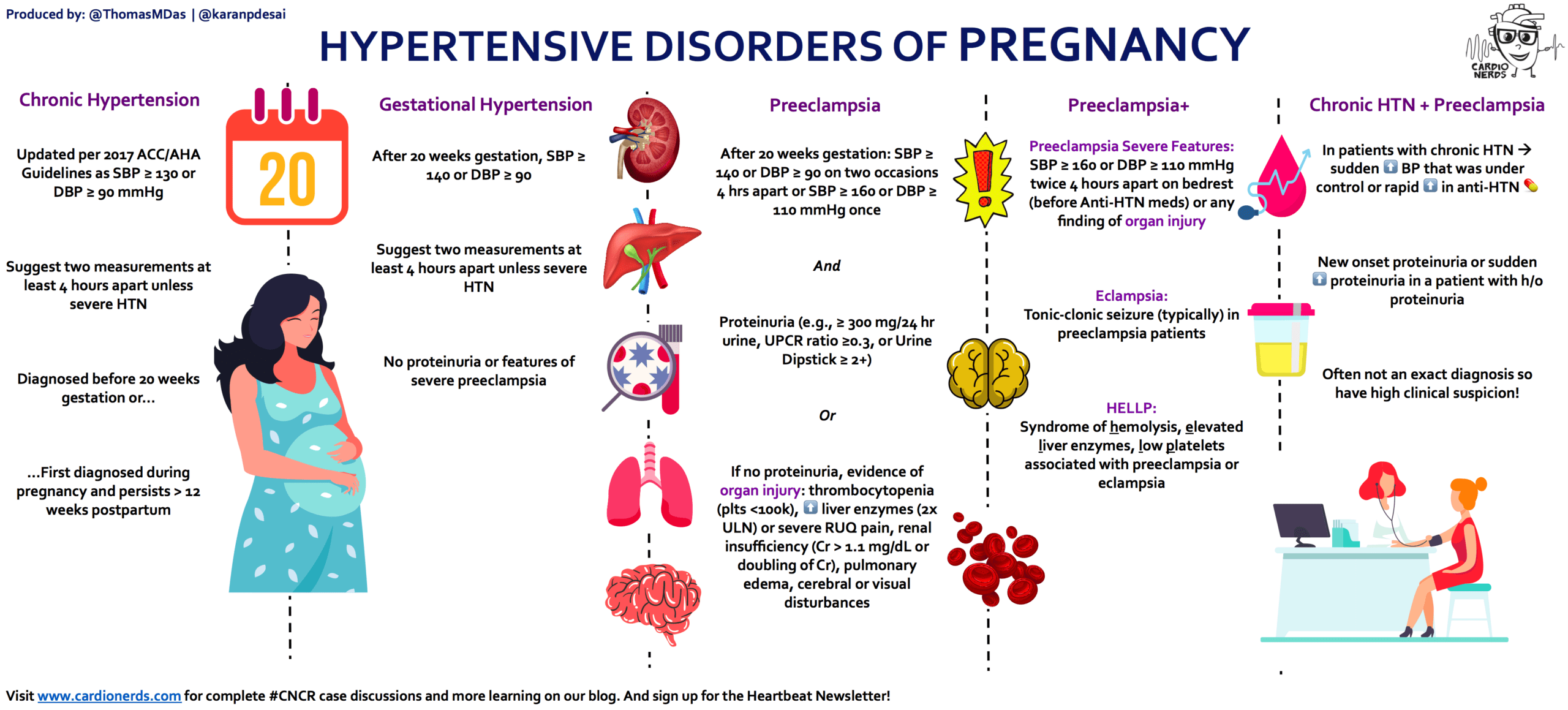 Preeclampsia affects a woman's kidneys, liver, and other vital organs, and if left untreated, it can cause seizures (eclampsia), cerebral hemorrhage, multiple organ failure, and death.
Preeclampsia affects a woman's kidneys, liver, and other vital organs, and if left untreated, it can cause seizures (eclampsia), cerebral hemorrhage, multiple organ failure, and death.
How does the disease affect the fetus?
In preeclampsia, the fetus does not receive enough oxygen and nutrients to grow, and intrauterine growth retardation may occur. In addition, the placenta may separate from the uterine wall before the baby is born. Since the only treatment for preeclampsia is childbirth, sometimes a pregnancy has to be terminated prematurely. Until the 34th week of pregnancy, the lungs of the fetus have not yet matured, and steroid hormones are administered intravenously to the pregnant woman to prepare her lungs. In addition to the immaturity of the lungs, the health of a premature baby is threatened by many other diseases.
Who is at risk of developing preeclampsia?
Preeclampsia occurs in approximately 8% of pregnant women, many of whom have no known risk factors.
What are the risk factors for preeclampsia?
Patient-related risk factors
-
First pregnancy
-
Pre-eclampsia during a previous pregnancy
-
Age over 40 or under 18
-
High blood pressure before pregnancy
-
Diabetes before or during pregnancy
-
Multiple pregnancy
-
Overweight (BMI> 30)
-
Systemic lupus erythematosus or other autoimmune disease
-
Polycystic ovary syndrome
-
Long interval between two pregnancies
Risk factors associated with the patient's family
What is the prevention and treatment of preeclampsia
During the first trimester screening, or Oscar test, in addition to the most common chromosomal diseases, the risk of preeclampsia is also calculated. In case of high risk, pregnant women are advised to take aspirin (acetylsalicylic acid) at a dose of 150 mg in the evenings until the 36th week of pregnancy. This helps reduce the chance of preeclampsia by the 34th week of pregnancy by up to 80%.
In case of high risk, pregnant women are advised to take aspirin (acetylsalicylic acid) at a dose of 150 mg in the evenings until the 36th week of pregnancy. This helps reduce the chance of preeclampsia by the 34th week of pregnancy by up to 80%.
Childbirth is the only treatment for preeclampsia. Sometimes a child can be born naturally, but sometimes, if the disease is very acute, an emergency caesarean section is necessary. The best time to have a baby is after the 37th week of pregnancy. Bed rest, medications, and, if necessary, hospitalization can sometimes help bring the condition under control and prolong the pregnancy. Often, a doctor will refer a woman with preeclampsia to the hospital for observation, as the condition of the fetus and pregnant woman may suddenly worsen.
Does bed rest help?
Sometimes bed rest is enough to bring mild preeclampsia under control. In this case, the patient often visits a doctor who measures blood pressure, does blood and urine tests, and monitors the course of the disease. The condition of the fetus is also often examined using a cardiotocogram (CTG) and ultrasound.
In this case, the patient often visits a doctor who measures blood pressure, does blood and urine tests, and monitors the course of the disease. The condition of the fetus is also often examined using a cardiotocogram (CTG) and ultrasound.
Are drugs used to treat preeclampsia?
High blood pressure sometimes requires medication. The medications used have few side effects, the drugs prescribed do not have much effect on the fetus, but are very important in the treatment of maternal high blood pressure.
Seizures are a rare but very serious complication of preeclampsia. Magnesium sulfate is sometimes given intravenously to prevent seizures in a pregnant woman with preeclampsia both during and after childbirth. It is safe for the fetus, but the mother may experience side effects such as hot flashes, sweating, thirst, visual disturbances, mild confusion, muscle weakness, and shortness of breath. All these side effects disappear when the drug is discontinued.
All these side effects disappear when the drug is discontinued.
Can preeclampsia recur?
Preeclampsia does not necessarily recur in the next pregnancy, but the main risk factor for preeclampsia is the presence of preeclampsia in a previous pregnancy(s). Risk factors for relapse include the severity of the previous case and the woman's overall health during pregnancy. A woman who has previously had preeclampsia should consult a gynecologist during a new pregnancy or when planning a pregnancy.
ITK1013
The information material was approved by the Health Care Quality Committee of East-Tallinn Central Hospital on 27.01.2021 (Minutes No. 2-21).
Pre-eclampsia: symptoms and treatment
Preeclampsia of pregnant women is a special complication of the second half of the waiting period for a baby, it is based on an increase in the permeability of the vascular wall. This pathology is manifested by an increase in blood pressure, edema, the appearance of protein in the urine and insufficiency of internal organs.
This pathology is manifested by an increase in blood pressure, edema, the appearance of protein in the urine and insufficiency of internal organs.
In the absence of timely medical care, the condition poses a serious threat to the health and life of the expectant mother and her baby.
Pay attention! Every pregnant woman is at risk of preeclampsia, but this condition is fortunately rare.
Causes of preeclampsia
The reason for this dangerous condition is the pregnancy itself. Usually in the second half of the waiting period for a child, the body "adjusts" and "rebuilds" the circulatory system. In this case, no problems develop. But if such adaptation does not occur, preeclampsia develops.
Fertile ground for the development of pathology are arterial hypertension, kidney disease, diabetes mellitus, multiple pregnancy, obesity, hereditary predisposition, as well as a large weight gain during the period of expectation of the baby and the age of the expectant mother 40 years and older.
Signs of pathology
In the development of pathology, several significant symptoms are observed:
1. Arterial hypertension
Systolic pressure rises to 140 mm Hg or more, and diastolic pressure is based on numbers of 90 mm Hg or more. The indicator is measured regularly, and 24-hour blood pressure monitoring (ABPM) is also recommended.
2. Proteinuria
Proteinuria, or the appearance of protein in the urine, may indicate impaired kidney function. To do this, you need to collect a daily portion of urine and determine the level of proteins in it, you can think about pathology when the indicator rises above 0.3 g / l.
According to the level of protein increase, there are:
| Type of pathology | Protein content in urine |
| Moderate proteinuria | More than 0. |
| Severe proteinuria | More than 0.3 g/l in two urine samples collected 6 hours apart. |
 3 g/l in two urine samples collected 6 hours apart.
3 g/l in two urine samples collected 6 hours apart. 3. Edema syndrome
Currently, edema is not an indicative symptom for the diagnosis of eclampsia. However, it is important to consider the severity of this symptom. In the normal course of pregnancy, edema occurs in at least half of expectant mothers. As a rule, this condition does not cause concern and is subject to outpatient monitoring.
In the case of generalized and recurrent edema, combined with arterial hypertension and proteinuria, one can speak of preeclampsia.
Pay attention! To determine the true cause of the appearance of protein in the urine, it is important to exclude urinary tract infections.
Sequelae of pre-eclampsia
In the absence of timely medical care, the patient's health deteriorates and the condition becomes severe, and sometimes life-threatening.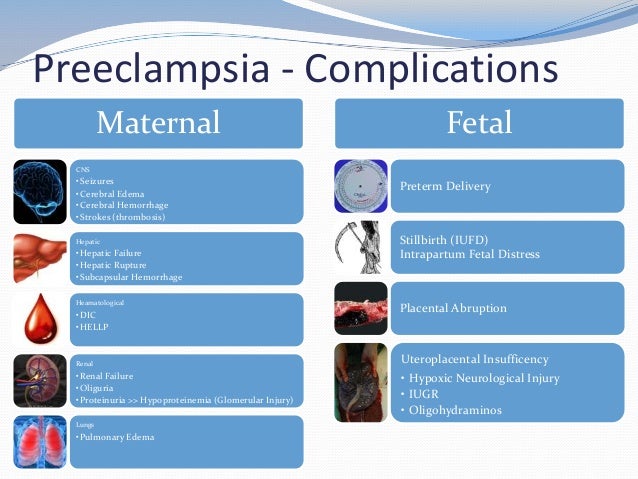
Complications and consequences of preeclampsia can be considered:
- hemorrhagic stroke
- DIC
- encephalopathy
- acute hypoxia, that is, oxygen starvation, fetus
- liver hematoma
- insufficiency of the liver, kidneys and other internal organs
- postpartum psychosis
Differential diagnosis of disease
In the diagnosis of this pathology, the collection of complaints and anamnesis, as well as laboratory and instrumental research methods, confirming an increase in blood pressure and the appearance of protein in the urine, are important.
High blood pressure? Do you feel a deterioration in well-being? You can get an initial consultation with a doctor remotely through our service. Specialists will help determine the cause of the ailment, advise medications and tell you what tests to take in order to make an accurate diagnosis.
Treatment of preeclampsia
1. Delivery is the most effective treatment for preeclampsia.
Delivery is the most effective treatment for preeclampsia.
With moderate preeclampsia, the expectant mother is hospitalized to clarify the diagnosis and carefully monitor the condition of the woman and fetus. In this case, pregnancy can be maintained up to 37 weeks in a hospital and constant monitoring. With a deterioration in the condition of the mother and fetus, stimulation of labor is indicated.
In severe preeclampsia, doctors stabilize the condition of the expectant mother, prevent DIC in the child, and then raise the issue of delivery. 2. Help with high blood pressure
The task of the doctor at this stage is to maintain normal figures for utero-fetal blood flow and reduce the risk of developing such a life-threatening condition as eclampsia.
Pay attention! Antihypertensive therapy is carried out, while constantly monitoring the condition of the fetus. The fact is that a decrease in placental blood flow provokes the progression of functional disorders in a child.
3. Convulsive syndrome
With preeclampsia, there is a high chance of having an attack of seizures. It is very important to "keep ready" drugs that relieve convulsive syndrome and prevent the transition of the pathological condition into real eclampsia. 4. Restoration of the volume of circulating fluid and prevention of deficiencies, treatment of pulmonary edema and stabilization of the central nervous system 5. Improvement of the rheological properties of blood and fetal blood flow
What is the prognosis for this pathology
In order to prevent the development of serious complications, it is important to act immediately when the blood pressure rises or the state of health worsens.
The tasks of gynecologists and obstetricians include:
- Early detection and identification of expectant mothers at risk and prone to the formation of preeclampsia
- Proper management of pregnancy, prevention of the formation of complications and conditions dangerous to health and life
- The correct tactics of the obstetrician after preeclampsia has formed
Unfortunately, there are currently no specific tests and analyzes for the early diagnosis of preeclampsia.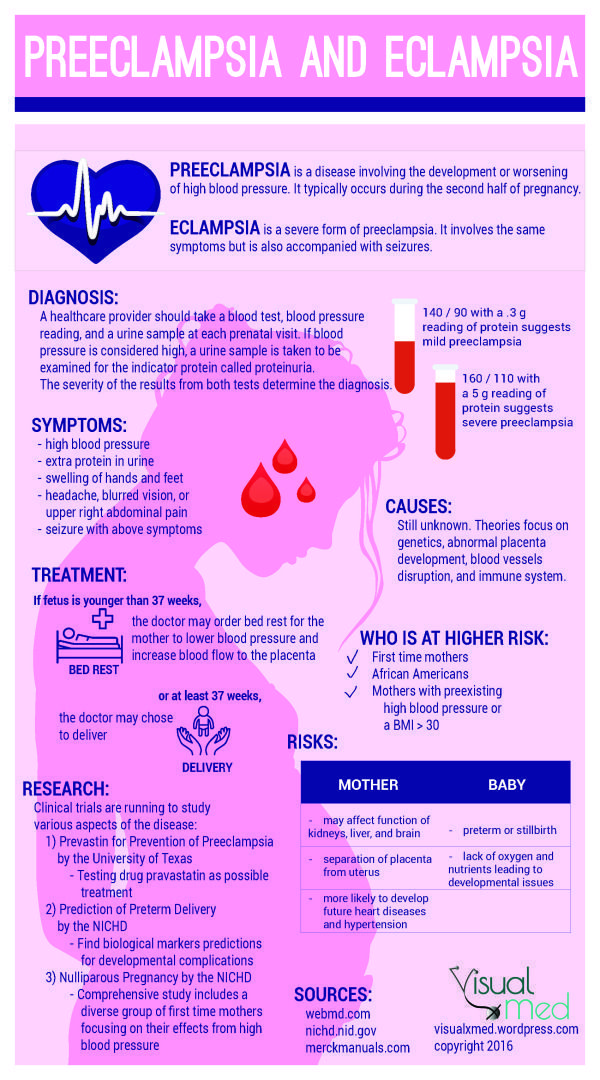 Therefore, it is very important for expectant mothers to scan their well-being and, if any complaints and symptoms appear, seek help from competent specialists in a timely manner!
Therefore, it is very important for expectant mothers to scan their well-being and, if any complaints and symptoms appear, seek help from competent specialists in a timely manner!
FAQ
How does mild preeclampsia manifest itself?
+
This condition is characterized by episodes of periodic increase in blood pressure, a tendency to edema, and "jumps of feeling unwell."
What is fetal preeclampsia?
+
There is no such concept. Preeclampsia develops in a pregnant woman, however, a significant deterioration in her well-being invariably affects the condition of the fetus.
How to suspect early preeclampsia?
+
According to pressure surges, deviations in the results of urine tests, a tendency to pastiness and swelling.
What symptoms of preeclampsia are observed during pregnancy in the 2nd trimester?
+
The risk of developing preeclampsia is actually a very individual story, this problem does not always develop and not every woman. But among the symptoms, attention is always drawn to an increase in blood pressure, swelling, deterioration of well-being and even convulsions in severe cases.
But among the symptoms, attention is always drawn to an increase in blood pressure, swelling, deterioration of well-being and even convulsions in severe cases.
How does severe preeclampsia in pregnancy develop?
+
Pre-eclampsia of severe severity is accompanied by an increase in blood pressure, edema and the development of multiple organ failure. Such an acute condition requires active and quick help from doctors, as it poses a serious threat to the health and life of both the mother and the child.
Does preeclampsia always develop during pregnancy?
+
No, not always. Toxicosis of the first half with nausea and mild malaise develops much more often. But preeclampsia is a serious condition, and, fortunately, it still develops quite rarely.
How to treat pregestosis and gestosis?
+
There are such concepts in obstetrics, but they do not need to be treated.