Symptoms of group b strep in pregnancy
Streptococcal infection – group B
Summary
Read the full fact sheet- Group B streptococcal bacteria can cause a wide range of illnesses.
- Between one and four out of every 1,000 newborns contract group B streptococcal disease (GBS disease) from their mothers during birth.
- Some of the life-threatening complications of GBS infection in newborns include bacterial infection of the bloodstream (septicaemia), pneumonia and meningitis.
- Many Australian maternity hospitals screen pregnant women for GBS infection to reduce the risk of GBS infection in newborn infants.
Group B streptococcal bacteria can cause a wide range of illnesses in susceptible people including newborns, the elderly and those with pre-existing medical conditions such as diabetes or cancer.
Out of every 1,000 newborns delivered vaginally, less than a third will become colonised with group B streptococci (GBS), and only one to four of those 1,000 will develop any illness from GBS. The rate of GBS disease is declining in Australia maternity hospitals, which is believed to be due to preventative screening programs and the use of antibiotics when required.
In most cases, pregnant women who are carriers of GBS shows no symptoms; they are usually not even aware that they are carrying the bacteria. Some of the life-threatening complications of GBS infection in newborns include bacterial infection of the bloodstream (septicaemia), pneumonia and meningitis. Many Australian maternity hospitals screen pregnant women for GBS infection to reduce the risk of GBS infection in newborn infants.
Symptoms of group B streptococcal infection
The signs and symptoms of GBS vary according to age, but can include:
- in non-pregnant adults – fever, headache, confusion, shortness of breath or cough (if pneumonia), a burning sensation when passing urine or frequent visits to the toilet to pass urine (if urinary tract infection), or red, swollen and painful skin (if cellulitis)
- in pregnant women – fever, abdominal swelling, uterine tenderness
- in newborns – shortness of breath or difficulty breathing, lethargy, low blood pressure
- in babies aged between one week and a few months – fever, lethargy, irritability, poor feeding, seizures.
Carriers of group B streptococcal infection
Some people are carriers of GBS, which means they harbour the bacteria but don’t show any symptoms of the infection. Common sites on the body where GBS may be carried include the vagina, bladder, the rectal (anal or back) passage and throat.
Infection is usually short term. It is thought that around 12 to 15 per cent of Australian pregnant women carry GBS in their vagina. A small proportion (less than two per cent) of babies born to these carriers will develop GBS disease. The risk of GBS infection is higher among premature babies. This risk can be reduced by giving the mother intravenous antibiotics during labour.
Onset of group B streptococcal infection in babies
The two types of GBS disease that affect babies include:
- early-onset – the newborn shows signs of illness shortly after birth or within one to two days of birth. Early-onset GBS disease is the most common type
- late-onset – infants show signs of illness one week to several months after birth.
 This form of GBS disease is comparatively rare. Only around half of all babies with late-onset GBS disease contract the illness from their infected mothers. For the remainder of cases, the source of infection is unknown.
This form of GBS disease is comparatively rare. Only around half of all babies with late-onset GBS disease contract the illness from their infected mothers. For the remainder of cases, the source of infection is unknown.
Diagnosis and treatment for group B streptococcal infection
GBS infection is diagnosed from specimens collected from blood, urine or spinal fluid. Vaginal swabs may be collected from pregnant women to determine if they are asymptomatic carriers of these bacteria.
The principal form of treatment for GBS is intravenous antibiotics, usually given in hospital. If the bacteria are found in a pregnant woman, intravenous antibiotics are given during the labour.
Screening methods for group B streptococcal infection
There is no standard screening procedure for GBS in Australia and the protocols vary from hospital to hospital. Some facilities screen only ‘at-risk’ pregnant women for GBS infection, while others screen all pregnant women at 35 to 37 weeks.
A recent Australian review of the published evidence reported lower rates of GBS disease among infants in hospitals where all pregnant women were screened for GBS. However, it acknowledged that there are advantages and disadvantages to each approach to screening. A recent statement from the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) listed both of the above approaches to GBS screening as being acceptable.
The main screening test is a swab of the vagina. A swab of the rectum (back passage) may also be taken. Research indicates that screening tests taken late in pregnancy are more reliable. For example, around 10 to 20 per cent of pregnant woman who have GBS-negative swabs at 28 weeks gestation are carrying the bacteria at the time of delivery.
Risk factors for group B streptococcal infection
If a pregnant woman is found to be a GBS carrier, the infection can easily be treated with intravenous antibiotics. Risk factors that may prompt your obstetrician to screen for GBS infection include:
- a GBS-positive swab in a previous pregnancy
- a previous baby with GBS infection
- pre-term labour
- rupturing of the membranes well before the onset of labour (18 hours or more)
- signs of infection around the time of labour or delivery (such as fever in the mother)
- prolonged labour.

For non-pregnant women and others, chronic diseases such as diabetes or cancer make you more vulnerable to getting GBS infection.
Where to get help
- Your doctor
- NURSE-ON-CALL. Tel. 1300 60 60 24 – for expert health information and advice (24 hours, 7 days)
- Your obstetrician or midwife
- Your maternity hospital.
- Maternal Group B Streptococcus in pregnancy: screening and management, 2016, Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG).
- Kurz E and Davis D 2015, ‘Routine culture-based screening versus risk-based management for the prevention of early-onset group B streptococcus disease in the neonate: a systematic review’, JBI Database of Systematic Reviews and Implementation Reports, vol. 13, no. 3, pp. 206–46.
This page has been produced in consultation with and approved by:
Department of Health - Public Health - Communicable Disease Prevention and Control
Group B Strep In Pregnancy: Test, Risks & Treatment
Overview
What is group B strep?
Group B strep infection (also GBS or group B Streptococcus) is caused by bacteria typically found in a person's vagina or rectal area. About 25% of pregnant people have GBS, but don't know it because it doesn't cause symptoms. A pregnant person with GBS can pass the bacteria to their baby during vaginal delivery. Infants, older adults or people with a weakened or underdeveloped immune system are more likely to develop complications from group B strep.
About 25% of pregnant people have GBS, but don't know it because it doesn't cause symptoms. A pregnant person with GBS can pass the bacteria to their baby during vaginal delivery. Infants, older adults or people with a weakened or underdeveloped immune system are more likely to develop complications from group B strep.
Most newborns who get GBS don't become sick. However, the bacteria can cause severe and even life-threatening infections in a small percentage of newborns. Healthcare providers screen for group B strep as part of your routine prenatal care. If you test positive, your provider will treat you with antibiotics.
How do you get group B strep?
GBS bacteria naturally occur in areas of your body like your intestines and genital and urinary tracts. Adults can't get it from person-to-person contact or from sharing food or drinks with an infected person. Experts aren't entirely sure why the bacteria spreads, but they know that it’s potentially harmful in babies and people with weakened immune systems.
When do you get tested for group B strep?
The Centers for Disease Control and Prevention (CDC) recommends routine screening for group B strep in all pregnancies. You're screened for GBS between 36 and 37 weeks of pregnancy. Group B strep testing involves your provider taking a swab of your vagina and rectum and then sending it to a lab for analysis.
Can Group B strep affect a developing fetus?
GBS doesn't affect the fetus baby while it's still inside your uterus. However, your baby can get GBS from you during labor and delivery. Taking antibiotics for GBS reduces your chances of passing it to your baby.
How does a baby get GBS?
There are two main types of Group B strep in babies:
- Early-onset infection: Most (75%) babies with GBS become infected in the first week of life. GBS infection is usually apparent within a few hours after birth. Premature babies face greater risk if they become infected, but most babies who get GBS are full-term.

- Late-onset infection: GBS infection can also occur in infants one week to three months after birth. Late-onset infection is less common and is less likely to result in a baby's death than early-onset infection.
How common is GBS?
Group B strep screening during pregnancy has decreased the number of cases. According to the CDC, about 930 babies get early-onset GBS, and 1,050 get late-onset GBS. About 4% of babies who develop GBS will die from it.
Symptoms and Causes
What are the symptoms of group B strep?
Most adults don't experience symptoms of group B strep. It can cause symptoms in older people or people with certain medical conditions, but this is rare. These symptoms include:
- Fever, chills and fatigue.
- Difficulty breathing.
- Chest pains.
- Muscle stiffness.
Newborns with GBS have symptoms like:
- Fever.
- Difficulty feeding.
- Irritability.
- Breathing difficulties.
- Lack of energy.
These symptoms can become serious quickly because newborns lack immunity. Group B strep infection can lead to severe problems like sepsis, pneumonia and meningitis in infants.
Can I pass group B strep to my partner?
Other people that live with you, including other children, aren't at risk of getting sick.
Diagnosis and Tests
Will I be tested for group B strep?
Yes, your healthcare provider will test you for GBS late in your pregnancy, around weeks 36 to 37.
Your obstetrician uses a cotton swab to obtain samples of cells from your vagina and rectum. This test doesn't hurt and takes less than a minute. Then, the sample is sent to a lab where it's analyzed for group B strep. Most people receive their results within 48 hours. A positive culture result means you're a GBS carrier, but it doesn't mean that you or your baby will become sick.
If you’re using a midwife, you might be given instructions on how to test yourself at home and submit the swab to a lab.
Is Group B strep an STI?
No, group B strep isn't an STI (sexually transmitted infection). The type of bacteria that causes GBS naturally lives in your vagina or rectum. It doesn't cause symptoms for most people.
Management and Treatment
What happens if you test positive for group B strep during pregnancy?
Healthcare providers prevent GBS infection in your baby by treating you with intravenous (IV) antibiotics during labor and delivery. The most common antibiotic to treat group B strep is penicillin or ampicillin. Giving you an antibiotic at this time helps prevent the spread of GBS from you to your newborn. It's not effective to treat GBS earlier than at delivery. The antibiotics work best when given at least four hours before delivery. About 90% of infections are prevented with this type of treatment.
One exception to the timing of treatment is when GBS is detected in urine. When this is the case, oral antibiotic treatment begins when GBS is identified (regardless of the stage of pregnancy). Antibiotics should still be given through an IV during labor.
Antibiotics should still be given through an IV during labor.
Any pregnant person who has previously given birth to a baby who developed a GBS infection or who has had a urinary tract infection in this pregnancy caused by GBS will also be treated during labor.
How is group B strep treated in newborns?
Some babies still get GBS infections despite testing and antibiotic treatment during labor. Healthcare providers might take a sample of the baby's blood or spinal fluid to see if the baby has GBS infection. If your baby has GBS, they're treated with antibiotics through an IV.
Prevention
How can I reduce my risk of group B strep?
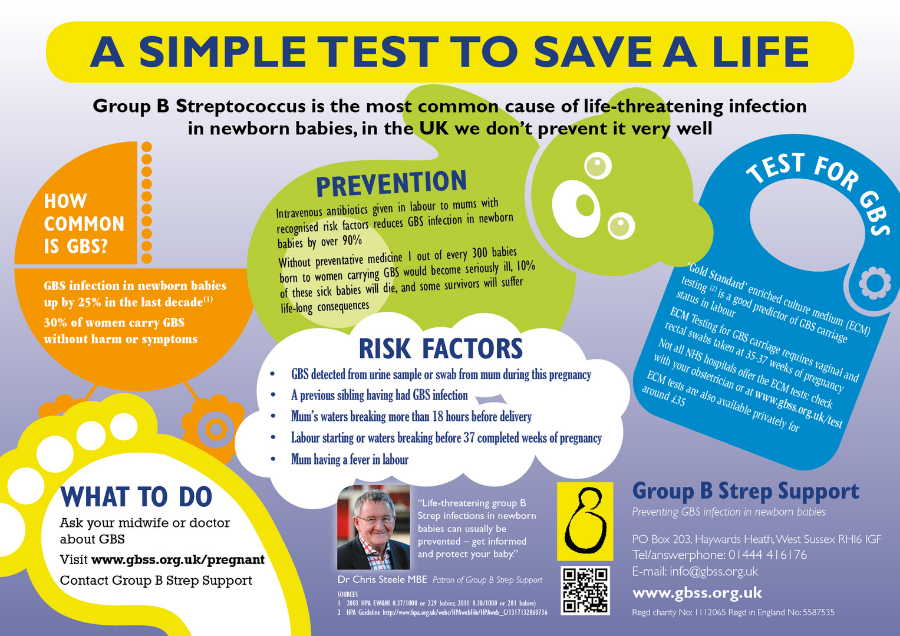
Anyone can get GBS. Some people are at higher risk due to certain medical conditions or age. The following factors increase your risk for having a baby born with group B strep:
- You tested positive for GBS.
- You develop a fever during labor.
- More than 18 hours pass between your water breaking and your baby being born.
- You have medical conditions like diabetes, heart disease or cancer.
Getting screened for GBS and taking antibiotics (if you're positive) is the best way to protect your baby from infection.
Outlook / Prognosis
What are long term problems of Group B strep in newborns?
Infants with GBS can develop meningitis, pneumonia or sepsis. These illnesses can be life-threatening. Most infants don't develop any long-term issues; however, about 25% of babies with meningitis caused by GBS develop cerebral palsy, hearing problems, learning disabilities or seizures.
Can I get tested for group B strep again?
No, once you test positive for GBS, you're considered positive for the rest of your pregnancy. You will not get re-tested.
Do I need treated for group B strep if I am having a c-section?
No, you don't need antibiotics if you're having a c-section delivery. However, you'll still be tested for GBS because labor could start before your scheduled c-section. If your water breaks and you're GBS positive, your baby is at risk of contracting the disease.
If your water breaks and you're GBS positive, your baby is at risk of contracting the disease.
Living With
When should I see my healthcare provider if I’m positive for group B strep?
In some cases, GBS causes infections during pregnancy. Symptoms of infection include fever, pain and increased heart rate. Let your provider know if you have any of those symptoms as it could lead to preterm labor.
GBS can also cause urinary tract infection (UTI), which requires oral antibiotics.
Talk to your provider about what you can expect during labor and delivery if you have group B strep.
A note from Cleveland Clinic
Try not to panic if your healthcare provider tells you you're positive for group B strep during pregnancy. It's caused by bacteria that occur naturally in your body, not by anything you did wrong. The chances of you passing group B strep to your baby are quite low, especially if you take antibiotics during labor. Talk to your provider about group B strep and share any concerns you have. In most cases, testing positive for GBS causes no problems, and your baby is healthy.
In most cases, testing positive for GBS causes no problems, and your baby is healthy.
Infections during pregnancy. Detection of group B streptococcus
05/16/2017
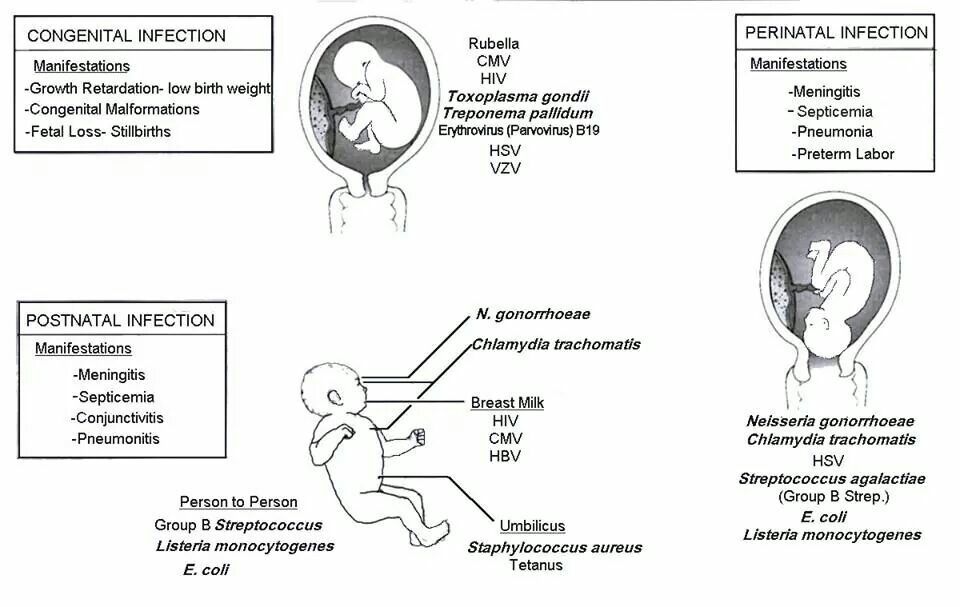
Infections during pregnancy that can be transmitted from mother to fetus deserve great attention, as they carry a potential risk of infection of the fetus or newborn and may lead to undesirable consequences. In addition, the diagnosis of infections during pregnancy has certain characteristics due to the asymptomatic course of most maternal infections or non-specific signs and symptoms. nine0003
Group B Streptococcus (GBS, Streptococcus agalactiae ) - Causes severe neonatal illness and poses a risk to certain patients in other age groups.
It has been estimated that GBS in 30% of pregnant women can be found in the vagina and often in the urethra of their sexual partners. Despite the fact that GBS can occur as part of the normal intestinal microflora of a woman, their colonization of the urogenital tract of a pregnant woman poses a significant risk to the fetus due to the possibility of ascending infection. There is a significant relationship between the carriage of GBS in the vagina, not only with early infection of newborns (sepsis, pneumonia and meningitis), but also with premature birth, premature discharge of amniotic fluid, urinary infection in pregnant women, development of chorioamnionitis during childbirth, endometritis. nine0003
There is a significant relationship between the carriage of GBS in the vagina, not only with early infection of newborns (sepsis, pneumonia and meningitis), but also with premature birth, premature discharge of amniotic fluid, urinary infection in pregnant women, development of chorioamnionitis during childbirth, endometritis. nine0003
In the USA, Canada and European countries, regulated National programs for the prevention and treatment of GBS infections have been adopted, which are mandatory for all medical institutions.
From 01.05.17, DILA ML introduces a new study “Identification of group B streptococcus (streptococcus agalactiae) with sensitivity to antibiotics”.
| Prompt identification of pregnant women who are positive for group B streptococcus and who have risk factors for an increased chance of infection in the newborn allows to conduct intravenous antibiotic prophylaxis with the onset of labor and prevent early infection of the newborn with group B streptococcus:
|

Rules for preparation : 24 hours before the use of intravaginal and rectal medications should be excluded, before taking the biomaterial, do not wash the external genital organs.
The biomaterial is taken from two points: the lower third of the vagina and the next - the rectum, the overall result is evaluated. nine0059 Detection of group B streptococcus is carried out by a cultural method with the determination of sensitivity to antibiotics.
Research period: 6 days (Kyiv), 7.5 days (Regions).
Adequate assessment of the risk of infection of the newborn with group B streptococcus will significantly reduce the possibility of complications and ensure a favorable pregnancy outcome.
Literature:
1. Australasian society for infectious diseases, 2014
2. Antibiotic Prevention for Maternal Group B Streptococcal Colonization on Neonatal GBS-Related Adverse Outcomes: A Meta-Analysis, Shunming Li, Jingya Huang, 2017.
3. Early onset Group B Streptococcal disease Queensland clinical guidelines, 2016
4. Effect of group B streptococci colonizing the urogenital tract of pregnant women on the course and outcome of pregnancy / Oganyan K.A., Zatsiorskaya S.L., Arzhanova O.N., Savicheva A.M. – St. Petersburg, 2014
5. Digest of professional medical information. Congenital and perinatal infections: prevention, diagnosis and treatment. / Catherine S. Peckham. - No. 1 (4). – 2008.
0 0
Rate satisfaction
DILA for you
Clinical consulting service for clinical support of doctors and patients before visiting a doctor
0-800-600-911
Bacterial infections during pregnancy
Among the inflammatory diseases of bacterial origin that occur during pregnancy, a significant place is occupied by conditions caused by disturbances in the normal microflora of the genitourinary tract. The microflora of the vagina is characterized by a wide variety of bacterial species and is divided into flora characteristic of healthy women (obligate) and pathological. With adverse external influences, in stressful situations, with a decrease in the body's immunological defense, with hormonal disorders, gynecological diseases, qualitative and quantitative changes in the microflora can occur in the genital tract. A decrease in the number of bacteria belonging to the normal microflora in the vagina leads to a decrease in protective barriers in the vagina, and to excessive reproduction of opportunistic microorganisms. Violations of the normal microflora of the birth canal pose a great danger to pregnant women, as they can lead to abortion, premature birth, intrauterine infection of the fetus and postpartum inflammatory complications in puerperas. nine0003
Physiological and biological changes that occur in the genital tract during pregnancy lead to the fact that the vaginal microflora becomes more homogeneous with a predominance of lactic acid bacilli (lactobacilli).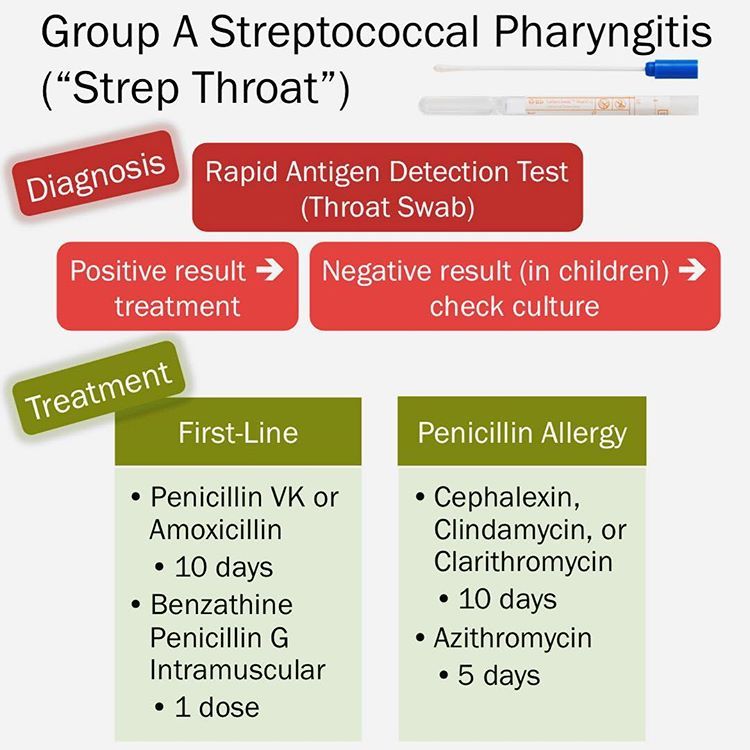
There are a number of factors that control and influence the composition of the normal vaginal microflora. The vaginal environment affects the microflora, providing conditions for the possible presence in certain quantities of various types of microorganisms. In general, the vaginal microflora includes various types of microorganisms. Vaginal discharge normally contains 108-1010 microorganisms per 1 ml, while aerobic bacteria are 105-108, anaerobic 108-109cfu/ml Lactobacilli dominate in the microbial flora of the vagina and cervix. It should be noted that bifidobacteria are more common in pregnant women than lactobacilli, and this fact is regarded as a reaction to the absence or inhibition of lactobacilli. In general, anaerobic organisms prevail over aerobic and facultative anaerobic organisms. Among aerobic bacteria, diphtheroids, staphylococci, streptococci are most often detected, and among anaerobic bacteria - lactobacilli, bifidobacteria, peptostreptococci, prevotella and bacteroids. nine0003
nine0003
streptococcal infection
The family of these microorganisms includes several genera of morphologically similar gram-positive cocci, which are facultative anaerobes. There are serological groups of streptococci A, B, C, D, E, F, G and H. According to the appearance of the colonies and the nature of hemolysis on blood agar, these pathogens are divided into hemolytic, green and non-hemolytic species. Three groups of streptococci can be present in the vagina of healthy women: streptococci of the viridans group (green streptococci), serogroup B streptococci, and serogroup D streptococci (enterococci). The frequency of detection and the number of streptococci belonging to these groups varies significantly and normally does not exceed 104 CFU / ml. During pregnancy, from the point of view of possible infection, pathogens such as Streptococcus pyogenes (group A beta-hemolytic streptococcus) and Streptococcus agalactiae (group B streptococcus, which has recently become the most common cause of infections in both newborns, especially premature ones, so do their mothers). nine0003
nine0003
Diseases caused by Streptococcus pyogenes
About 20% of pregnant women are carriers (nasopharynx, vagina and perianal area). A pregnant woman may experience: tonsillitis, pharyngitis, pyoderma, urinary infection, chorionamnionitis, endometritis, postpartum sepsis. The infection can be transmitted to the child at birth, with subsequent risk of neonatal sepsis increased, especially with prolonged anhydrous interval.
nine0108 The main diagnostic method is a culture method (on blood agar aerobically and anaerobically).
In the treatment prescribed antibiotics from the group of penicillins and cephalosporins for at least 10 days. In postpartum sepsis, high doses of parenteral benzylpenicillin or ampicillin are prescribed. Newborns with streptococcal infections are also given high doses of benzylpenicillin, ampicillin, or cephalosporins. nine0003
Due to the fact that Streptococcus pyogenes is transmitted by contact, prevention is to comply with the rules of asepsis during childbirth.
Diseases caused by Streptococcus agalactiae
This type of streptococcus is part of the vaginal microflora in 20% of pregnant women. With a disease in a pregnant woman, asymptomatic bacterial colonization of the vagina and perianal area, urinary tract infection, chorionamnionitis, endometritis can be observed. nine0003
The main diagnostic method is a cultural method. The more intense the infection of the pregnant woman, the more likely the infection of the child. With delivery through the natural birth canal, the frequency of transmission of infection to the child is 50-60%. The risk of disease in a full-term baby is 1-2%, and in a premature baby - 15--20%, with a period of less than 28 weeks of pregnancy - 100%. If a child is infected during childbirth, sepsis, pneumonia, meningitis, and severe neurological complications may develop. In severe cases, the disease begins immediately after birth and progresses rapidly. The risk for the child increases with premature rupture of the membranes, premature birth, symptoms of chorionamnionitis in the mother. nine0003
nine0003
When prescribing treatment it should be taken into account that group B streptococci are sensitive to all beta-lactam antibiotics, cephalosporins. If streptococci are detected in a pregnant woman, even without clinical symptoms, penicillin therapy is necessary for 10 days, cephalosporins and macrolides may be used.
Prevention. According to some studies, the appointment of ampicillin to a woman in labor prevents infection with Streptococcus agalactiae. The disadvantages of prophylactic administration of ampicillin include the need for a preliminary bacteriological study. It is advisable to screen all pregnant women in the third trimester for the presence of group B streptococci using gynecological culture. nine0003
Bacterial vaginosis
Among bacterial diseases in pregnant women, a large proportion are pathological conditions associated with violations of the normal microflora of the genital tract. Bacterial vaginosis is a clinical syndrome caused by a pathological change in the structure of the microbial environment of the vagina.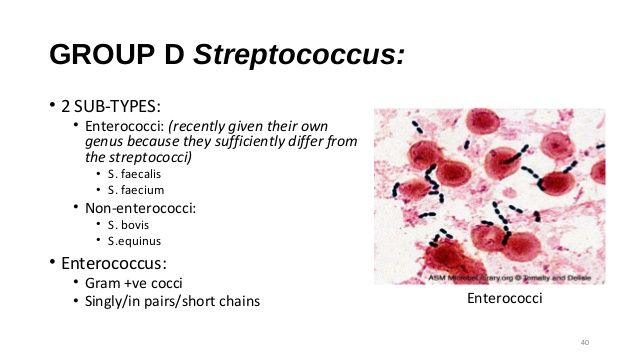 In patients with bacterial vaginosis, concentrations of facultative and anaerobic bacteria predominate to a large extent, which displace lactic acid bacilli, which leads to significant changes in the vaginal microflora. The main feature of the violation of the composition of the normal vaginal microflora in bacterial vaginosis is a significant decrease in the number of lactic acid bacilli and a pronounced colonization of the vagina by anaerobic bacteria (Prevotella/Porphyromonas spp., Peptostreptococcus spp., Fusobacteium spp., Mobiluncus spp.) and Gardnerella vaginalis. nine0003
In patients with bacterial vaginosis, concentrations of facultative and anaerobic bacteria predominate to a large extent, which displace lactic acid bacilli, which leads to significant changes in the vaginal microflora. The main feature of the violation of the composition of the normal vaginal microflora in bacterial vaginosis is a significant decrease in the number of lactic acid bacilli and a pronounced colonization of the vagina by anaerobic bacteria (Prevotella/Porphyromonas spp., Peptostreptococcus spp., Fusobacteium spp., Mobiluncus spp.) and Gardnerella vaginalis. nine0003
During pregnancy, the reasons for the violation of the normal composition of the microflora of the vagina may be the corresponding hormonal changes, the use of antibiotics, etc. More than half of all women with bacterial vaginosis have some kind of subjective complaints and pathological secretions from the genital tract (leucorrhoea) are absent, along with the available positive laboratory signs. Inflammatory reaction of the vaginal epithelium is not a characteristic sign bacterial vaginosis . In the clinical variant of the course of bacterial vaginosis with severe symptoms, prolonged abundant, liquid, milky or grayish-white homogeneous discharge (leucorrhoea), mainly with an unpleasant fishy odor, is noted. nine0003
In the clinical variant of the course of bacterial vaginosis with severe symptoms, prolonged abundant, liquid, milky or grayish-white homogeneous discharge (leucorrhoea), mainly with an unpleasant fishy odor, is noted. nine0003
Bacterial vaginosis occurs in 15 - 20% of pregnant women, and is a serious risk factor for the development of infectious complications. A pronounced relationship of bacterial vaginosis with premature termination of pregnancy and untimely rupture of the amniotic membranes was noted. The risk of developing these complications compared with healthy pregnant women in patients with bacterial vaginosis increases by 2.6 times. Approximately 10% of preterm women give birth to gardnerella and other microorganisms from the amniotic fluid, while normally the amniotic fluid is sterile. It was noted that in women who gave birth before 37 weeks. there is a high probability of having bacterial vaginosis. nine0003
Chorioamnionitis, detected in 1% of pregnant women, is a severe complication that threatens the life of the mother and fetus. The development of chorionamnionitis associated with bacterial vaginosis in the mother can subsequently lead to premature abortion or premature rupture of amniotic fluid. The presence of chorionamnionitis in patients with bacterial vaginosis is histologically confirmed by the identification of relevant pathogenic microorganisms in the placental tissue, which can also be the cause. premature birth . nine0003
The development of chorionamnionitis associated with bacterial vaginosis in the mother can subsequently lead to premature abortion or premature rupture of amniotic fluid. The presence of chorionamnionitis in patients with bacterial vaginosis is histologically confirmed by the identification of relevant pathogenic microorganisms in the placental tissue, which can also be the cause. premature birth . nine0003
There is also a relationship between the presence of bacterial vaginosis and the development of postpartum endometritis including after caesarean section. The risk of developing postpartum endometritis in pregnant women with bacterial vaginosis is 10 times higher than in healthy women. The microbial flora detected in the endometrium in patients with endometritis is often similar to that in bacterial vaginosis. This is especially true for anaerobic microorganisms. Mixed microflora in bacterial vaginosis can lead to the development of other inflammatory complications, such as breast abscess, inflammation of the umbilical wound, etc.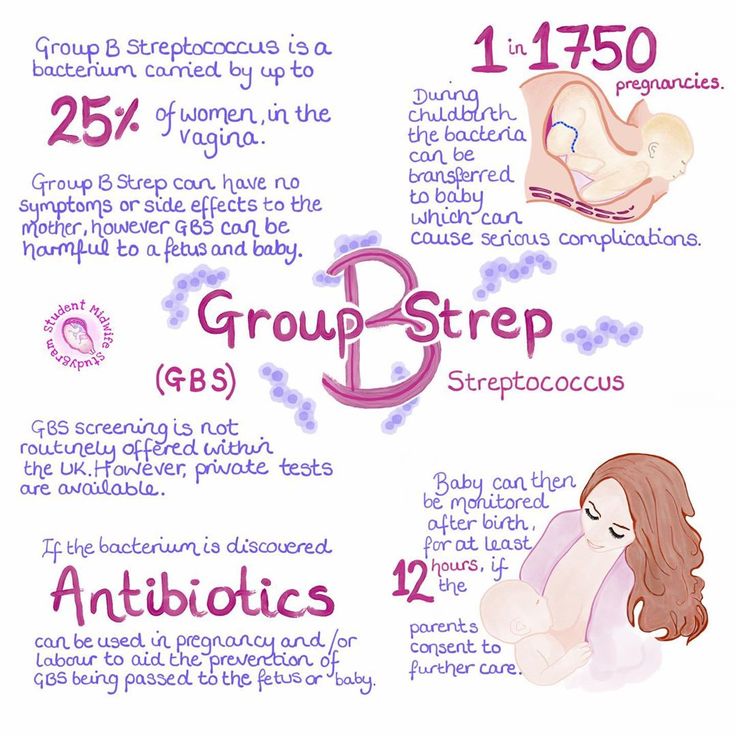 nine0003
nine0003
Thus, patients with bacterial vaginosis are at increased risk for the development of inflammatory diseases of the pelvic organs, premature termination of pregnancy, untimely rupture of amniotic fluid, the occurrence of chorionamnionitis, postpartum and postoperative endometritis. The high concentration of virulent microorganisms in the vagina of patients suffering from bacterial vaginosis is a risk factor for the penetration of bacteria into the higher parts of the genitourinary system. nine0003
Diagnostics - the complex includes four diagnostic tests
- during an external gynecological examination of the patient in the area of the vestibule of the vagina, leucorrhoea typical of bacterial vaginosis is noted. If the discharge is too profuse, it may also drain to the perineum. In this case, usually the external genital organs are not hyperemic and not edematous. However, in the presence of concomitant infection, edema and hyperemia of the vaginal mucosa are observed; nine0042
- PH value of vaginal discharge in patients with bacterial vaginosis is usually 5.
 0 - 6.0;
0 - 6.0; - a positive amine test, which is accompanied by the appearance of an unpleasant fishy odor when exposed to a 10% potassium hydroxide solution on a sample of the contents from the middle third of the vagina;
- detection by microscopy in the discharge from the vagina of "key cells", which are mature cells of the vaginal epithelium with microorganisms adhered to them in large numbers, which are located mostly chaotically. nine0042
Microscopic analysis of vaginal secretions is the method of final diagnosis, including Gram-stained smears.
Treatment of bacterial vaginosis
In the first trimester of pregnancy, for the treatment of bacterial vaginosis, it is possible to prescribe clindamycin 2% in the form of a vaginal cream of 5.0 g for 3-7 days or povidone-iodine 1 vaginal suppository per day for 14 days or from the 10th week Terzhinan 1 vaginal tablet 10 days. nine0003
In II trimester of pregnancy the arsenal of drugs for the treatment of bacterial vaginosis can be supplemented with Clotrimazole 1 vaginal tablet for 10 days, as well as oral administration of Clindamycin 300 mg 2 times - 7 days.
In the III trimester, in addition to the listed drugs, Ornidazole 500 mg 2 times - 5 days, or Metronidazole 500 mg 2 times - 7 days, as well as Viferon-2 Suppositories or KIP-feron 1 suppository 2 times 10 days rectally can be used. nine0003
Gonorrhea
The causative agent of the disease is Neisseria gonorrhoeae - Gram-negative bacteria sensitive to light, cold and dryness. Outside the human body, these pathogens are not able to live long. The infection is transmitted by sexual infection. When infected, gonococci are detected in the urethra, the large gland of the vestibule, the cervix, tubes and peritoneum. The infection can spread through the mucous membranes of the endometrium and pelvic organs. nine0003
In 80% of women, gonorrhea is asymptomatic, with cervical lesions observed in more than 50% of cases, rectum - more than 85%, pharynx - more than 90%. The presence of gonorrhea in a pregnant woman is a significant risk factor for adverse outcomes for both mother and fetus. In women who contract gonorrhea after 20 weeks of pregnancy or after childbirth increases the risk of developing gonococcal arthritis. In acute gonorrhea, there is an increased risk of premature rupture of amniotic fluid, spontaneous abortion, and preterm birth. Chronic gonorrhea may worsen immediately after childbirth, with an increased risk of gonococcal sepsis. nine0003
In women who contract gonorrhea after 20 weeks of pregnancy or after childbirth increases the risk of developing gonococcal arthritis. In acute gonorrhea, there is an increased risk of premature rupture of amniotic fluid, spontaneous abortion, and preterm birth. Chronic gonorrhea may worsen immediately after childbirth, with an increased risk of gonococcal sepsis. nine0003
Infection of the fetus occurs in utero or during childbirth. intrauterine infection manifested by gonococcal sepsis in the newborn and chorionamnionitis. Infection during childbirth can lead to gonococcal conjunctivitis, otitis externa, and vulvovaginitis.
If gonorrhea is suspected, a study is made of discharge from the vagina and cervix. An indicative diagnosis is established when pathogens of gonorrhea are detected in a smear. To confirm the diagnosis, sowing of the discharge on a special medium is used. Also use the PCR method. nine0003
Treatment of gonorrhea in pregnant women
Treatment of pregnant women at any gestational age should be carried out in a hospital. Treatment of disseminated gonorrhea should be carried out with the involvement of specialists of the appropriate profile. In the treatment of the disease, pregnant women with gonococcal urethritis, endocervicitis, proctitis or pharyngitis are prescribed ceftriaxone 250 mg intramuscularly or spectinomycin (trobicin) 2.0 g intramuscularly once. With gonococcal sepsis, ceftriaxone is prescribed 1 g intravenously or intramuscularly 1 time per day for 7-10 days. 7 days after the end of treatment, repeated crops are carried out. With ophthalmic rhea of newborns, ceftriaxone is used at a dose of 25-50 mg / kg intravenously or intramuscularly once and frequent washing of the conjunctiva with isotonic sodium chloride solution. nine0003
Treatment of disseminated gonorrhea should be carried out with the involvement of specialists of the appropriate profile. In the treatment of the disease, pregnant women with gonococcal urethritis, endocervicitis, proctitis or pharyngitis are prescribed ceftriaxone 250 mg intramuscularly or spectinomycin (trobicin) 2.0 g intramuscularly once. With gonococcal sepsis, ceftriaxone is prescribed 1 g intravenously or intramuscularly 1 time per day for 7-10 days. 7 days after the end of treatment, repeated crops are carried out. With ophthalmic rhea of newborns, ceftriaxone is used at a dose of 25-50 mg / kg intravenously or intramuscularly once and frequent washing of the conjunctiva with isotonic sodium chloride solution. nine0003
As a control for treatment, sowing is carried out after the end of treatment after 7 days and after 4 weeks.
As a preventive measure during the initial examination of a pregnant woman, it is necessary to sow the discharge from the cervix for gonorrhea.