Purpose of umbilical cord
Anatomy, Abdomen and Pelvis, Umbilical Cord - StatPearls
Introduction
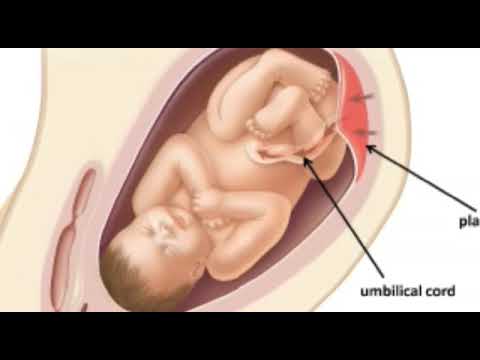
The umbilical cord is considered both the physical and emotional attachment between mother and fetus. This structure allows for the transfer of oxygen and nutrients from the maternal circulation into fetal circulation while simultaneously removing waste products from fetal circulation to be eliminated maternally. On the other hand, mothers associate an emotional connection to the fetus through the cord. It may merit consideration as the route of love and care during pregnancy. Thus, some poets call it the string of life.
The umbilical cord is a bundle of blood vessels that develops during the early stages of embryological development. It is enclosed inside a tubular sheath of amnion and consists of two paired umbilical arteries and one umbilical vein. During development, the umbilical arteries have a vital function of carrying deoxygenated blood away from the fetus to the placenta.[1] However, after birth, a significant distal portion of the umbilical artery degenerates. These remnants later obliterate, forming the medial umbilical ligament.[2] At the same time, the proximal portion of each umbilical artery serves as a branching point for the development of the anterior internal iliac arteries. The internal iliac arteries later give rise to the superior vesical arteries that supply the urinary bladder and ureters as well as the ductus deferens and seminal vesicles in males.[3][4] The umbilical cord is a vital structure for the entire period of development since it functions to tether the fetus to the placenta and the uterine wall while also acting as the primary route to enable blood to circulate between the fetus and placenta.[5]
Structure and Function
Anatomical Features of an Umbilical Cord
The umbilical cord is a soft, tortuous cord with a smooth outer covering of amnion. It extends from the umbilicus of the fetus to the center of the placenta. Its length ranges from 50 cm to 60 cm, with a diameter of about 1 cm.[6] The umbilical cord is composed of a gelatinous ground substance called Wharton's jelly or substantia gelatinea funiculi umbilicalis.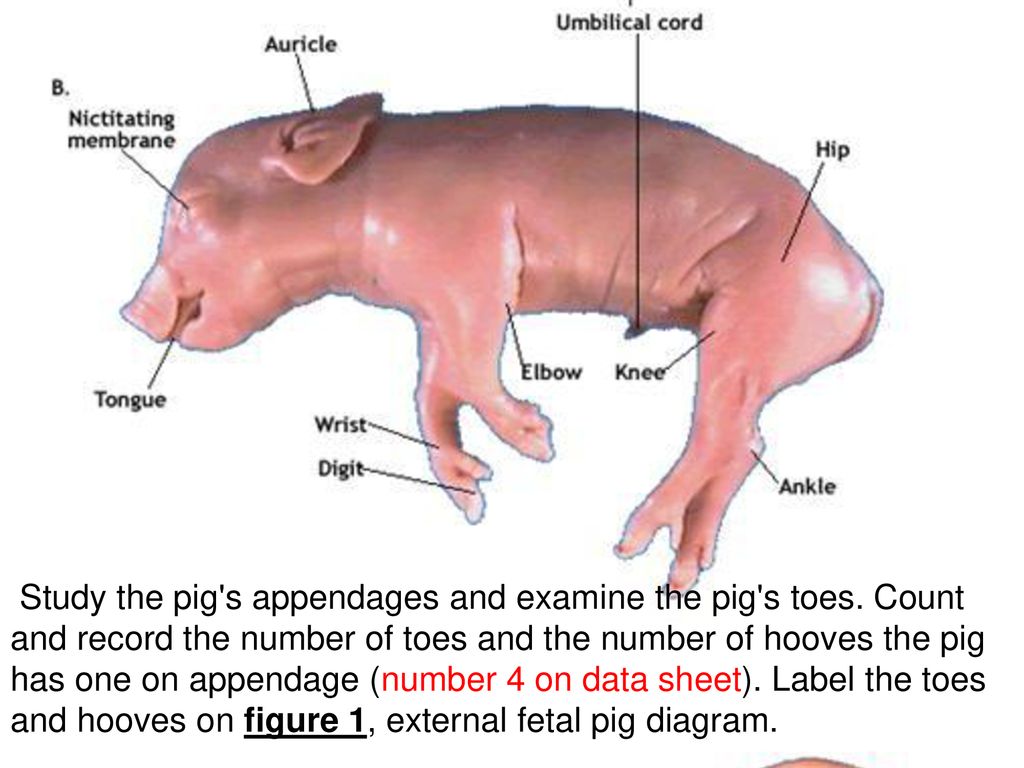 It is composed of mucopolysaccharides from the conjugation of hyaluronic acid and chondroitin sulfate. As previously mentioned, three vessels comprise the umbilical cord: two umbilical arteries and one umbilical vein. It also encloses the urachus (a remnant of allantois).[7] The urachus is a fibrous remnant of the allantois that extends through the umbilical cord and is located in the space of Retzius between the peritoneum posteriorly and the transverse fascia anteriorly. The urachus serves as a drainage canal for the urinary bladder of the fetus.[8]
It is composed of mucopolysaccharides from the conjugation of hyaluronic acid and chondroitin sulfate. As previously mentioned, three vessels comprise the umbilical cord: two umbilical arteries and one umbilical vein. It also encloses the urachus (a remnant of allantois).[7] The urachus is a fibrous remnant of the allantois that extends through the umbilical cord and is located in the space of Retzius between the peritoneum posteriorly and the transverse fascia anteriorly. The urachus serves as a drainage canal for the urinary bladder of the fetus.[8]
Function
The umbilical arteries carry deoxygenated blood from fetal circulation to the placenta. The two umbilical arteries converge together about at 5 mm from the insertion of the cord, forming a type of vascular connection called the Hyrtl's anastomosis.[9] The primary function of Hartl's anastomosis is to equalize blood flow and pressure between the umbilical and placental arteries.[10] As the arteries enter the placenta, each bifurcates into smaller branches called the chorionic vessels.
Embryology
During the early stages of embryonic development, gastrulation occurs and differentiates germinal tissues into three distinct layers: outer ectoderm, intra-embryonic mesoderm, and inner endoderm.[11] The formation of the umbilical cord occurs over three stages and coincides with the gastrulation process.
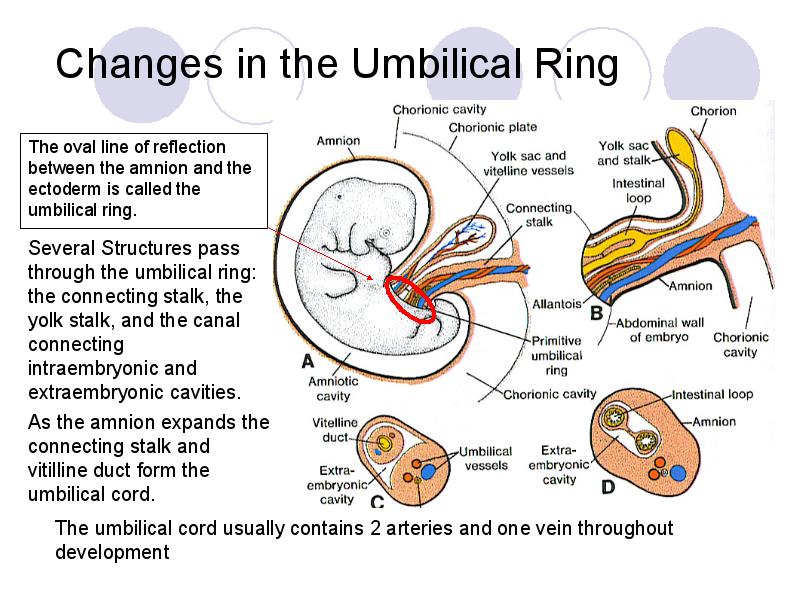
I. Formation of the Primitive Umbilical Ring
This developmental stage happens together with the folding of the embryonic disc. During this stage, the embryonic disc bulges into the amniotic cavity as a result of folding. At the same time, the amnio-ectodermal junction, which is the tight connection between the embryonic amnion and the ectodermal layer, becomes the ventral aspect of the embryo. Then, the line of reflection between the amnion and the ectoderm acquires an oval outline called the primitive umbilical ring.
II. Formation of the Primitive Umbilical Cord
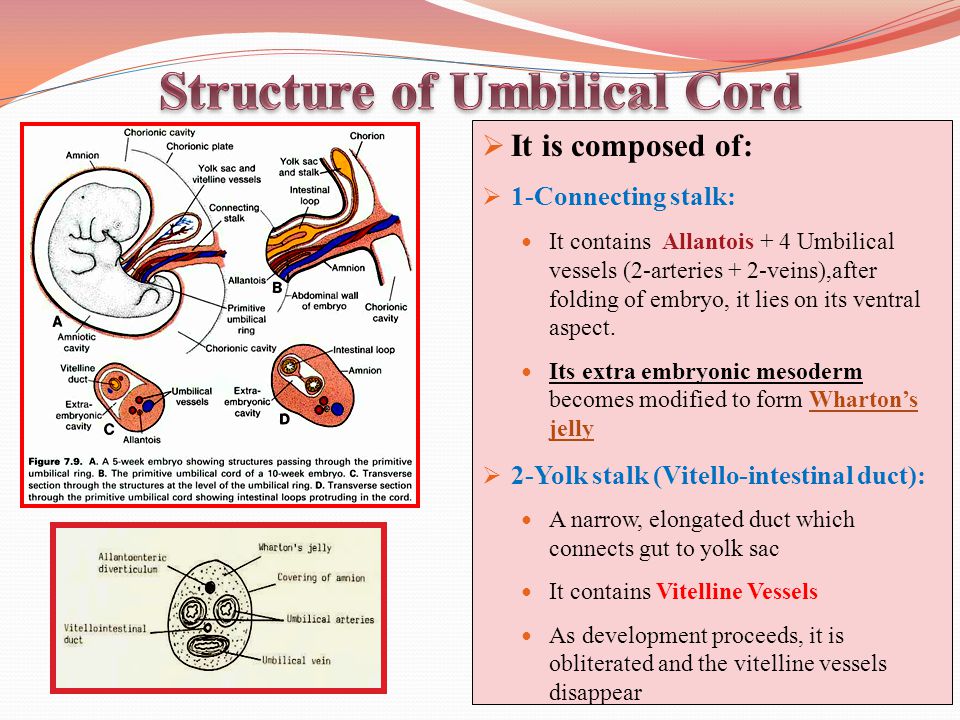
This stage of development starts in the fifth week of pregnancy, during which the primitive umbilical ring constricts to form a tubular sheath.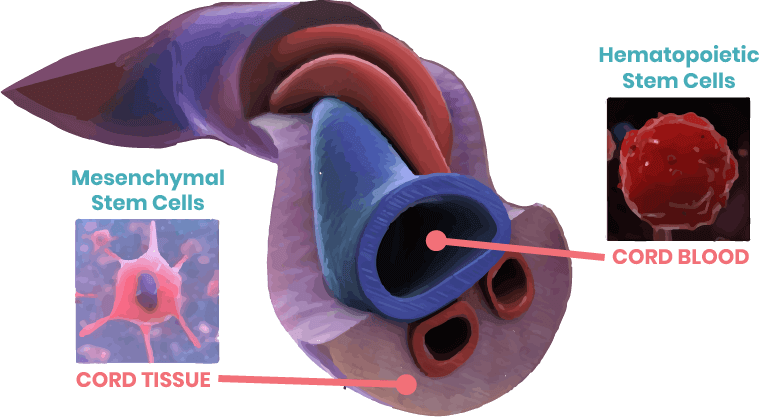 The tubular sheath is called the primitive umbilical cord. It encloses the body stalk, the yolk sac, and its vessels, as well as a part of the allantois.
The tubular sheath is called the primitive umbilical cord. It encloses the body stalk, the yolk sac, and its vessels, as well as a part of the allantois.
III. Formation of the Definitive Umbilical Cord
During this stage, the umbilical cord elongates, and its fundamental structures undergo primary changes. For instance, The extraembryonic mesoderm of the body stalk starts to differentiate into a mucoid substance called Wharton's jelly. Wharton's jelly develops gradually and forms the main bulk of the umbilical cord. The remnants of the extraembryonic coelom inside the umbilical cord progressively degenerate. The yolk sac becomes obliterated together with the vitellointestinal duct that connects the yolk sac with the midgut. Similarly, the distal part of the allantois becomes obliterated. However, the allantoic vessels persist and elongate to form the umbilical vessels. Finally, during the sixth week, a part of the midgut loop enters the umbilical cord developing a physiological hernia. That physiological hernia is usually corrected when that part of the midgut returns to the abdominal cavity after the tenth week of pregnancy.[12]
That physiological hernia is usually corrected when that part of the midgut returns to the abdominal cavity after the tenth week of pregnancy.[12]
Blood Supply and Lymphatics
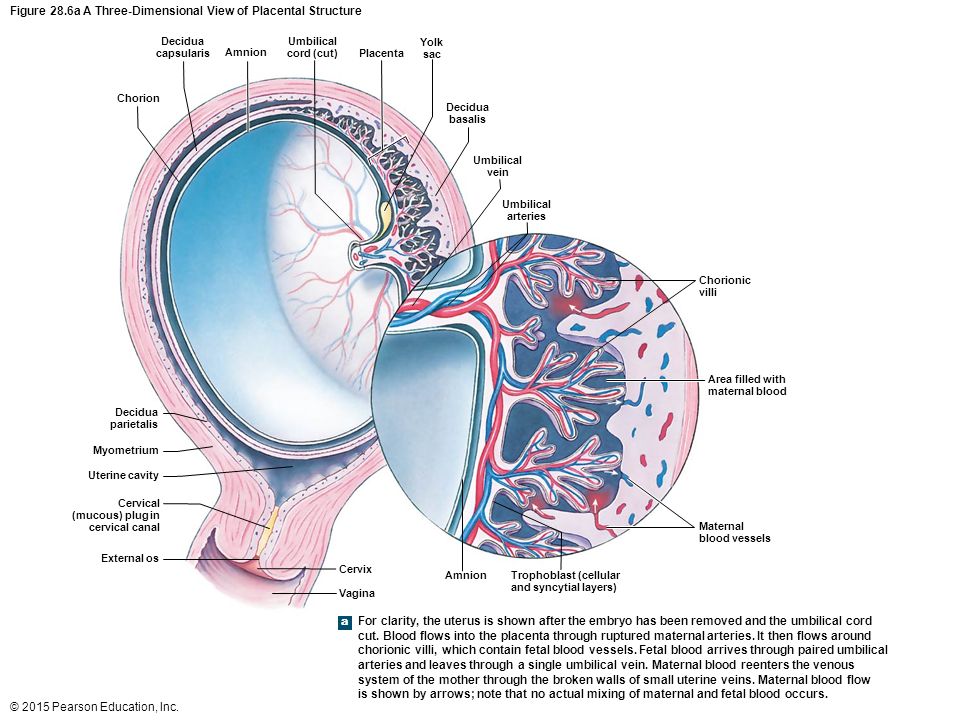
The umbilical cord, together with the placenta, contributes to the flow and regulation of fetal circulation. The two umbilical arteries arise from the internal iliac arteries of the fetus and enter the umbilical cord before further branching at the level of the placenta. At the placental level, each umbilical artery bifurcates into smaller arterioles that continue to branch further to distribute blood to the chorionic villi. The capillaries of the villi fuse to form venules that converge to form the umbilical vein. The umbilical vein carries oxygenated blood and nutrients from the mother to the fetus.[13]
As fetal growth ensues, both placental intervillous circulation and umbilical circulation develop gradually, until maturation is complete at the end of the first trimester. At midgestation, the percentage of umbilical blood in fetal circulation is about 30% of the fetal cardiac output.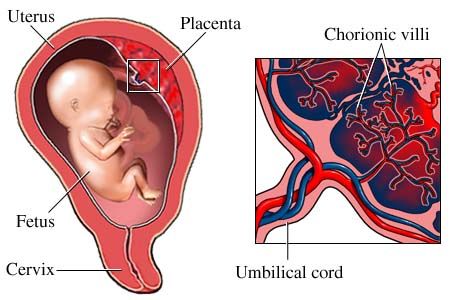 During the last trimester of pregnancy, umbilical blood flow declines significantly as it becomes inversely proportional to the fetal weight measured in kilograms. That percentage decreases considerably during the last trimester till it reaches less than 20%. The umbilical vein enters the abdominal region of the fetus. It carries the oxygenated blood with nutrients to the fetal liver parenchyma and ductus venosus. Then, blood flows to the inferior vena cava and foramen ovale of the fetal heart.[14]
During the last trimester of pregnancy, umbilical blood flow declines significantly as it becomes inversely proportional to the fetal weight measured in kilograms. That percentage decreases considerably during the last trimester till it reaches less than 20%. The umbilical vein enters the abdominal region of the fetus. It carries the oxygenated blood with nutrients to the fetal liver parenchyma and ductus venosus. Then, blood flows to the inferior vena cava and foramen ovale of the fetal heart.[14]
On the other hand, the role and distribution of lymphatic drainage for the placenta, as well as the umbilical cord, has been scarcely discussed in scientific resources. However, recent research has shown D2-40 expression at the level of placental stromal has a vital role in the fetal lymphatic drainage. This expression links to podoplanin-expressing cells whose function is related to forming a lymphatic-like reticular network. The thinking is that those cells are responsible for providing lymphatic drainage for the umbilical cord and the placenta.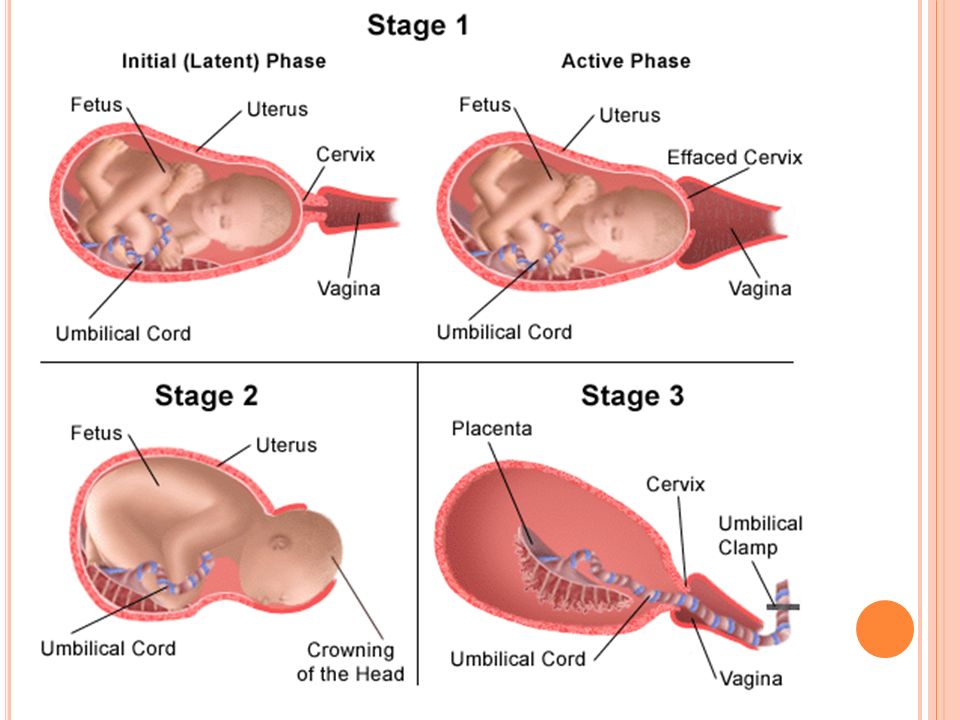 [15]
[15]
Nerves
The umbilical cord lacks intrinsic and extrinsic innervations during all stages of embryonic development. Vasoactive substances secreted locally within the umbilical vessels wall or carried through the fetal circulation are responsible for regulating the smooth muscle tension within the umbilical vasculature. For instance, nitrous oxide and prostacyclin play an essential role in maintaining the low vascular resistance within the umbilical and placental circulation. Furthermore, catecholamines are primary contributors for vasoconstriction of the umbilical vessels immediately after parturition.[16]
Muscles
The bulk of the umbilical cord consists of Wharton's jelly since it does not have any voluntary skeletal muscles. However, the umbilical vasculature has several smooth muscle layers of various compositions and thicknesses. The walls of umbilical vessels consist mainly of three layers: tunica externa, tunica media, and tunica interna.
Tunica externa
Also referred to as the tunica adventitia, it is the outermost layer of the umbilical vessels that consists of fibrous and elastic connective tissue with varying amounts of collagen and elastic fibers.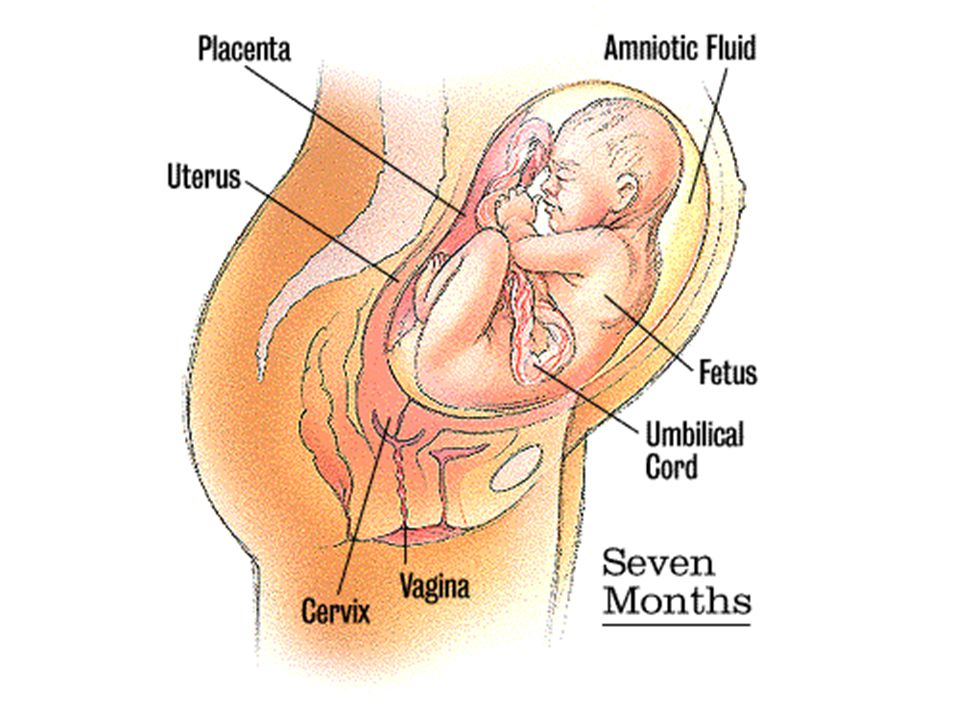 The connective tissue of this layer is quite dense near the tunica media. It transitions to loose connective tissue as it extends toward the periphery of the umbilical vessels. The umbilical arteries have denser connective tissue in their tunica externa compared to that of the umbilical vein.[17]
The connective tissue of this layer is quite dense near the tunica media. It transitions to loose connective tissue as it extends toward the periphery of the umbilical vessels. The umbilical arteries have denser connective tissue in their tunica externa compared to that of the umbilical vein.[17]
Tunica media
This section is the intermediate layer within the wall of the umbilical vessels. It represents the muscular bulk of the vessels and consists mainly of smooth muscle. It provides structural support for the vessels. It is also responsible for changing the diameter of the umbilical vessels. Thus, it contributes primarily to regulate blood flow and blood pressure. It is commonly the thickest layer within the vascular wall. It is much thicker in the umbilical arteries compared to the umbilical vein. Moreover, tunica media of the umbilical arteries contain well-defined internal and external elastic membranes that may be less defined or absent in the umbilical vein wall.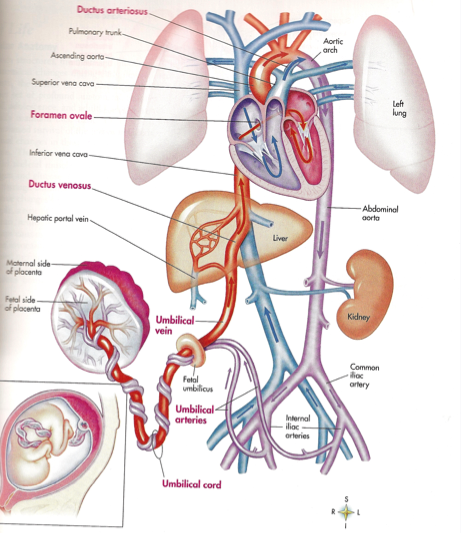 [18]
[18]
Tunica interna
Also called the tunica intima, it is the innermost layer of the umbilical vasculature. It is composed of simple squamous epithelium resting on a basement membrane consists of connective tissue rich in elastic fibers. Those layers together form the endothelium of the umbilical vessels. The tunica interna of the umbilical vein contains valves that direct the blood flow in one direction and prevent its regurgitation in the opposite direction. Those valves are absent in the wall of the umbilical arteries.[19]
Physiologic Variants
Umbilical Cord Coiling Patterns
One of the most common morphological variations of the umbilical cord is its different helical coiling patterns. The degree of coiling is measured by the umbilical cord index (UCI). Commonly, the umbilical cord coiling pattern has a UCI of 0.2 coil/cm. The rope model is considered the most common pattern of umbilical cord coiling. On the other hand, hyper-coiling of the umbilical cord is defined as having a UCI greater than 0. 3 coil/cm and a relatively high incidence of about 6% to 21% of all pregnancies.[20] Also, the umbilical cord can coil in an undulating pattern that has a relatively high incidence compared to other coiling patterns, such as segmented or linked coiling of the umbilical cord. It was found clinically that abnormal coiling of the umbilical cord is closely associated with the fetal vascular obstruction, which in its role can eventually lead to fetal thrombi, avascular villi or villous stromal vascular karyorrhexis that commonly occur with segmented coiling pattern of the umbilical cord [21].
3 coil/cm and a relatively high incidence of about 6% to 21% of all pregnancies.[20] Also, the umbilical cord can coil in an undulating pattern that has a relatively high incidence compared to other coiling patterns, such as segmented or linked coiling of the umbilical cord. It was found clinically that abnormal coiling of the umbilical cord is closely associated with the fetal vascular obstruction, which in its role can eventually lead to fetal thrombi, avascular villi or villous stromal vascular karyorrhexis that commonly occur with segmented coiling pattern of the umbilical cord [21].
False Knots of the Umbilical Cord
False knots are bulging masses located on the surface of the umbilical cord. Sometimes, excessive torsion of the umbilical cord inside the uterus can cause these bulging masses to appear as knots on uterine ultrasonography grossly. The knot appearance of this condition forms via the excessive accumulation of Wharton's Jelly bulks alternating with areas with relatively less amount of jelly composing constrictions after each bulging. Hence, they were identified as false knots of the umbilical cord. This physiologic variation does not affect the stability of the fetal position, nor does it affect umbilical blood flow and pressure. Thus, false knots do not represent a considerable risk to the fetus.[22]
Hence, they were identified as false knots of the umbilical cord. This physiologic variation does not affect the stability of the fetal position, nor does it affect umbilical blood flow and pressure. Thus, false knots do not represent a considerable risk to the fetus.[22]
Single Umbilical Artery
The incidence of having a single umbilical artery is very low overall. However, It is known to be more common in multiparous females compared to nulliparous ones. Many studies have reported that the left umbilical artery is more often absent than the right.[23] The side of umbilical artery absence has very minimal significance with the exception that one study concluded that infants with a single umbilical artery identified by ultrasound in utero had reported the presence of congenital abnormalities, including cardiac, renal, intestinal, and skeletal anomalies when the left umbilical artery was absent.[23][24][25][26][27] Also, it is noted that the incidence of urinary tract infection is higher in infants with a single umbilical artery. [28]
[28]
Surgical Considerations
Anesthetic Considerations
Placental and umbilical blood flow impact fetal oxygen delivery. Myometrial tone and maternal blood pressure have a direct correlation with uterine artery blood flow. Volatile anesthetics usually decrease myometrial tone and tend to reduce maternal blood pressure. Subsequently, there is a decrease in fetal oxygenation due to a reduction in placental blood flow. Maintenance of patent umbilical arteries and baseline maternal arterial blood pressure is essential for maintaining sound cardiac output for the fetus. For example, maternal hypercapnia leads to fetal hypoxia and metabolic acidosis as a result of umbilical venous flow reduction. Similarly, maternal hypocapnia should be avoided during all maternal or fetal procedures since it has a direct correlation with fetal hypoxia. Consequently, inhalation anesthesia is the best option for fetal and intrauterine procedures. Moreover, epidural anesthesia plays a critical role in the prevention of premature labor during the postoperative period of maternal surgeries.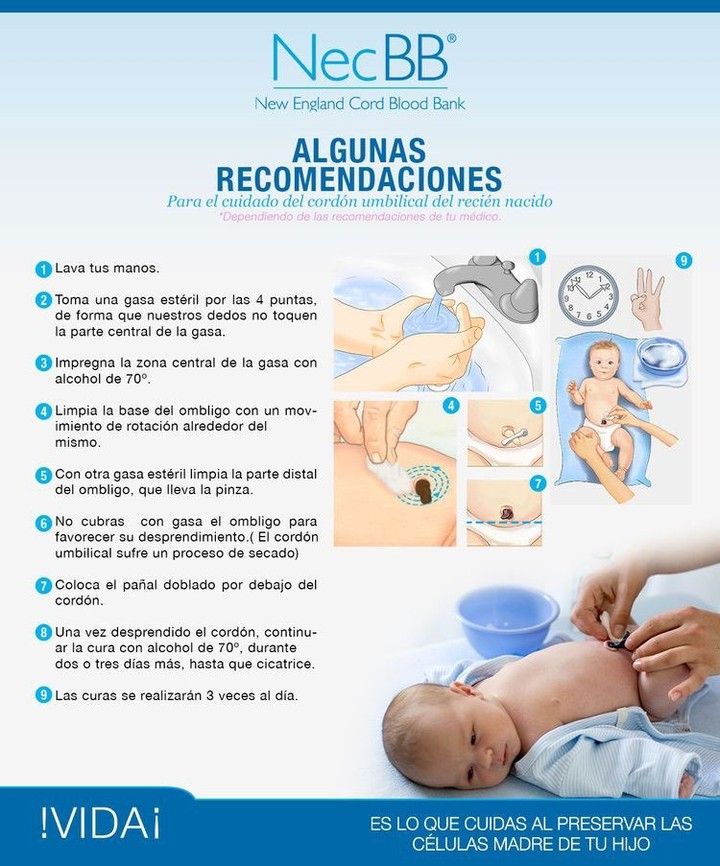 [29]
[29]
Intravenous Administration/Catheterization
The umbilical vein is considered the primary site for cannulation. The umbilical vein remains open for approximately one week after labor, and it can be useful for administering intravenous fluids and medications for newborns requiring more aggressive resuscitation efforts. The umbilical vein has a larger lumen than the umbilical arteries due to its thinner tunica media—catheterization through the umbilical vein to the ductus venosus. Finally, the catheter arrives at the inferior vena cava below the right atrium.[30] Furthermore, umbilical artery lines may also be used for resuscitative efforts during the first week after delivery. Umbilical artery catheterization is routinely used for direct access to monitor arterial blood gas, arterial blood pressure, and angiography. In the neonatal intensive care, umbilical artery catheterization is typically used to provide blood samples for laboratory testings.[31]
Clinical Significance
Different types of umbilical cord abnormalities may be potentially fatal or pose a severe threat to fetal health.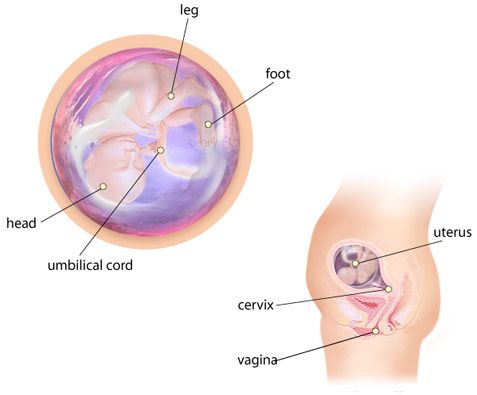 Thus, it is of great clinical significance to have early detection of these malformations to be able to provide a proper diagnosis and plan of care.
Thus, it is of great clinical significance to have early detection of these malformations to be able to provide a proper diagnosis and plan of care.
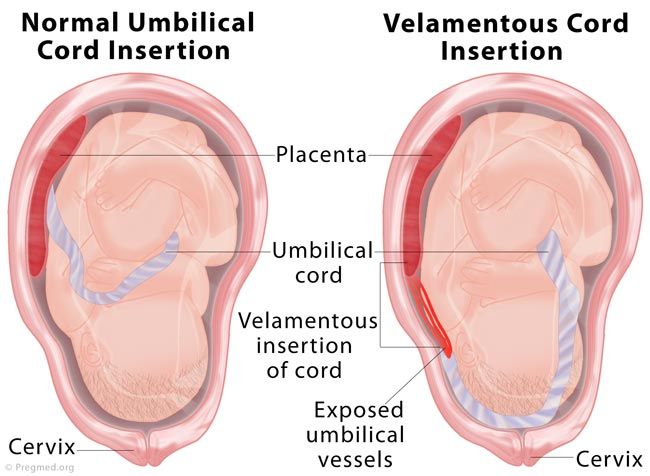
Velamentous Insertion
The incidence of velamentous insertion of the umbilical cord is significantly high for in vitro fertilization(IVF)-induced pregnancies compared to naturally-conceived pregnancies. It happens in about 10% of pregnancies and 20% of IVF pregnancies.[32] Velamentous insertion of the umbilical cord occurs when the placental end of the umbilical cord consists of umbilical arteries and vein surrounded by fetal membranes without Wharton's jelly. The exact reason for this condition is still unclear. However, the most current hypothesis suggests that during IVF pregnancy, half of the placenta undergoes excessive proliferation making the site of the insertion of the umbilical cord move peripherally away from its center. Conversely, the other pole of the placenta involutes and the umbilical cord becomes unable to follow the migration of the placenta.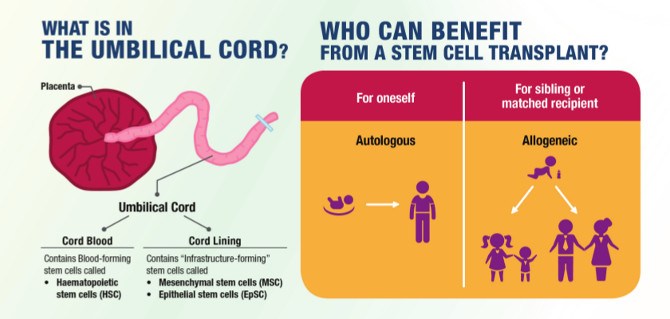 This condition casts risk for the fetus during delivery.[33]
This condition casts risk for the fetus during delivery.[33]
Four-Vessel Umbilical Cord
Normal umbilical cord anatomy consists of three vessels represented by two umbilical arteries and one umbilical vein. By the seventh week of gestation, the right umbilical vein usually obliterates, leaving a single (left) umbilical vein patent. However, there have been documented cases of umbilical cords containing four-vessels. The persistence of two umbilical veins and two umbilical arteries within the umbilical cord is associated with multiple cardiovascular and gastrointestinal anomalies.[34] When both the right and left umbilical veins remain open, a condition called persistent right umbilical vein (PRUV). This condition usually happens due to a deficiency in folic acid during the first trimester of pregnancy. This condition may cause teratogenic effects for the fetus and act as a risk factor for its overall physical health.[35]
True Knots of the Umbilical Cord
These are real tangling nodules of the umbilical vessels along the length of the umbilical cord.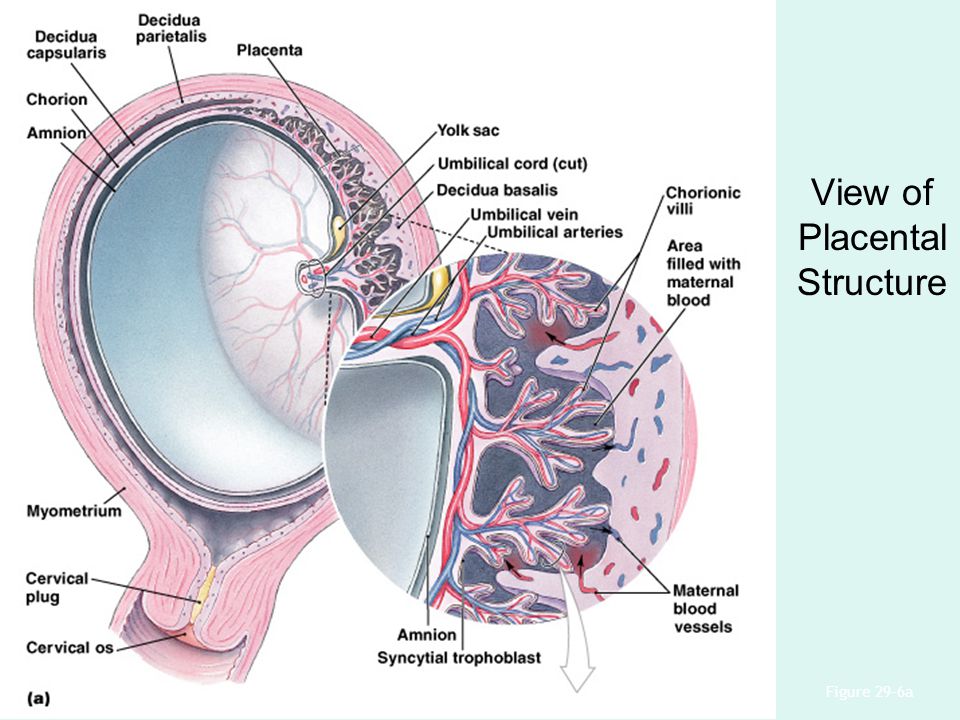 They usually occur early in pregnancy as a result of various predisposing factors. Most commonly, the development of true knots is associated with the presence of excessive amniotic fluid, causing high pressure on the umbilical cord vessels, increasing their torsional force, causing deep knots of those vessels. Also, an increase in the movement of the fetus in utero plays a vital role in creating that teratogenic deformity as supercoils of the umbilical cord can cause it to knot over itself. True knot deformities of the umbilical cord are very dangerous because they may obstruct the blood flow in the umbilical vessels, which may eventually lead to fetal demise.[36]
They usually occur early in pregnancy as a result of various predisposing factors. Most commonly, the development of true knots is associated with the presence of excessive amniotic fluid, causing high pressure on the umbilical cord vessels, increasing their torsional force, causing deep knots of those vessels. Also, an increase in the movement of the fetus in utero plays a vital role in creating that teratogenic deformity as supercoils of the umbilical cord can cause it to knot over itself. True knot deformities of the umbilical cord are very dangerous because they may obstruct the blood flow in the umbilical vessels, which may eventually lead to fetal demise.[36]
Very Short Umbilical Cord
An umbilical cord is considered significantly short when its length is less than approximately 40 cm. A short umbilical cord can lead to premature separation from the placenta resulting in an interruption in fetal circulation and, as a result, intrauterine bleeding followed by fetal death.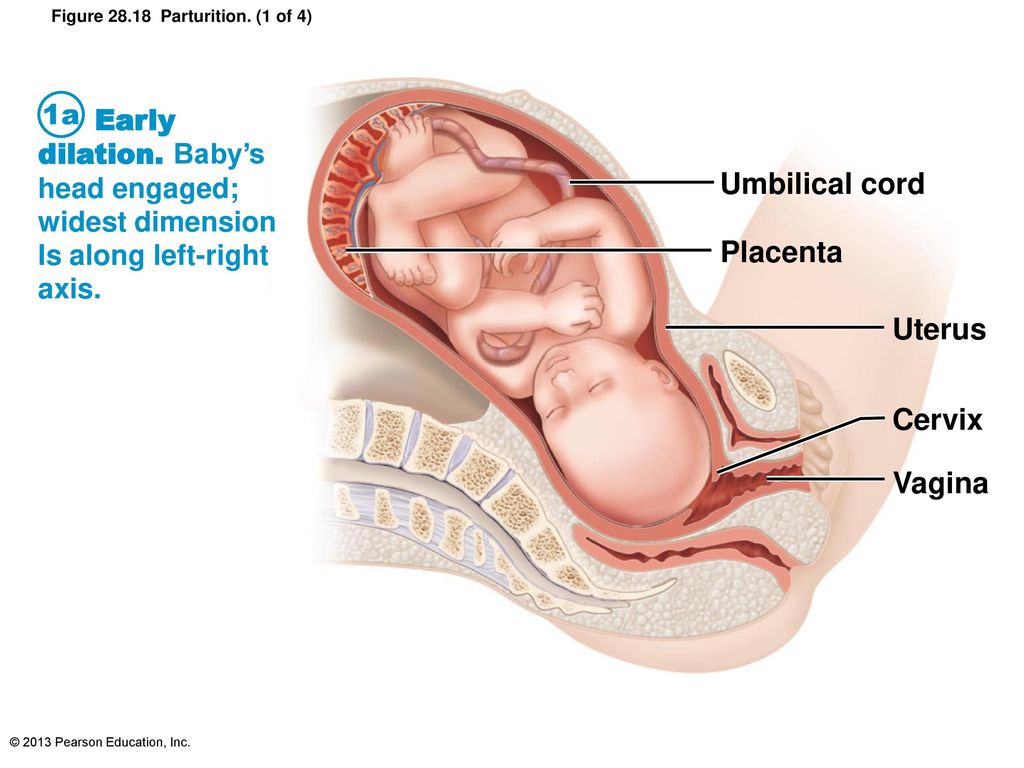 [37]
[37]
Very Long Umbilical Cord
If an umbilical cord is longer than 65 to 70 cm, it is clinically considered long. An abnormally long umbilical cord has the greater potential wind around the neck of the fetus multiple times contribute to fetal death, or it may also protrude from the mother's cervix.[37]
Omphalocele
Also referred to as exomphalos, an omphalocele is an abdominal wall defect that causes the herniation of bowel and sometimes other organs into the umbilical cord. The pathophysiology behind this condition is due to the failure of the reduction of the physiological umbilical hernia.[38] Surgical correction is considered for such conditions to prevent intestinal obstruction of the neonate.
Abnormal attachment of the umbilical cord to the placenta
Sometimes, the umbilical cord may have an abnormal attachment site on the placenta. For example, the umbilical cord may attach to the placenta significantly off-center, giving rise to eccentric attachment deformity. The placenta may take a deformed shape called battledore placenta. This deformity results from the marginal attachment of the umbilical cord to the placenta.[39] It closely correlates with abnormal hyper-coiling of the umbilical cord in most cases.
Delayed Umbilical Cord Separation
Normal separation of the umbilical cord can occur anytime after delivery with no reliable, constant timeline. However, generally speaking, separation of the umbilical cord is considered delayed if it happens later than the first three weeks after delivery. There are many factors and pathological conditions associated with the incidence of delayed cord separation. For instance, the topical application of antibiotics, alcohol, and triple dye after delivery has a significant contribution to delayed cord separation. Moreover, pathological conditions such as; infections, immune disorders, and the presence of urachal remnants can also delay umbilical cord separation. Interestingly, researchers found a correlation between each low birth weight, cesarian delivery, and prematurity and the increased risk of delayed umbilical cord separation.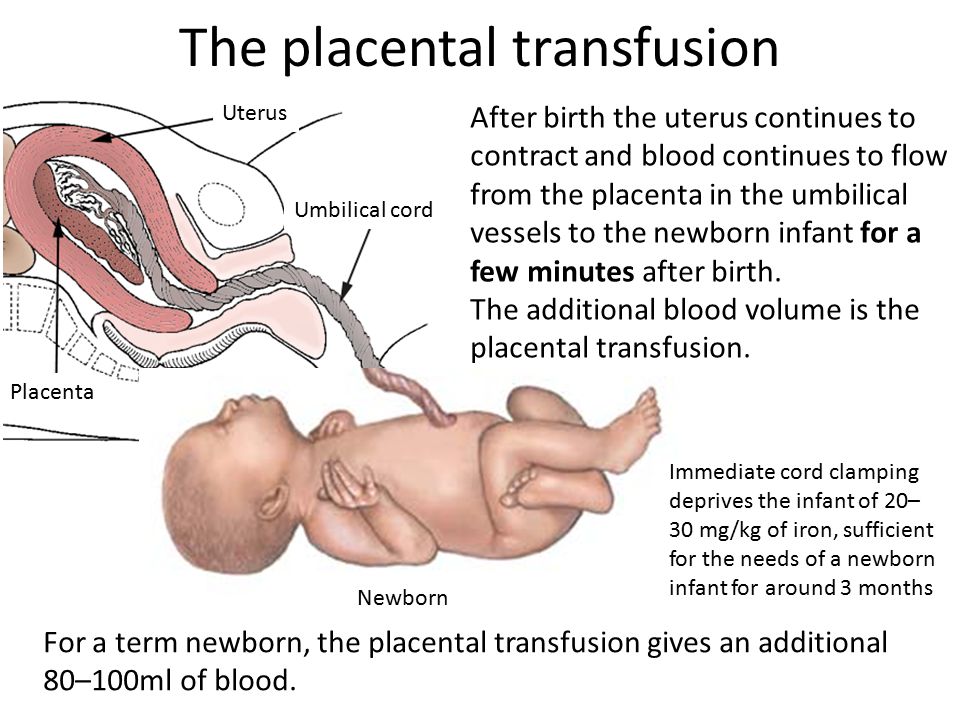 It is clinically significant to consider further workup in newborns with delayed umbilical cord separation and skin infections or those with persistent urachal remnants. These infants most likely have an underlying immunologic disorder.[40]
It is clinically significant to consider further workup in newborns with delayed umbilical cord separation and skin infections or those with persistent urachal remnants. These infants most likely have an underlying immunologic disorder.[40]
Umbilical Cysts
Cysts classify into two main categories: true cysts and pseudocysts. They usually occur near or around the insertion of the cord into the fetal umbilicus. Umbilical cord cysts generally develop during the first trimester with a standard resolution by the end of the twelfth week of gestation. Umbilical cysts have an incidence of 3.4% of all pregnancies. The exact etiology of umbilical cysts is not defined clinically. However, they appear to be closely related to chromosomal abnormalities, including trisomies of chromosomes 13 and 18, imperforate anus, and angiomyxoma of the cord.[41] The most frequently encountered type of cyst is a pseudocyst. Pseudocysts are also known as Wharton's jelly cysts. They lack epithelial tissue and occur commonly as a result of focal edema of Wharton's jelly.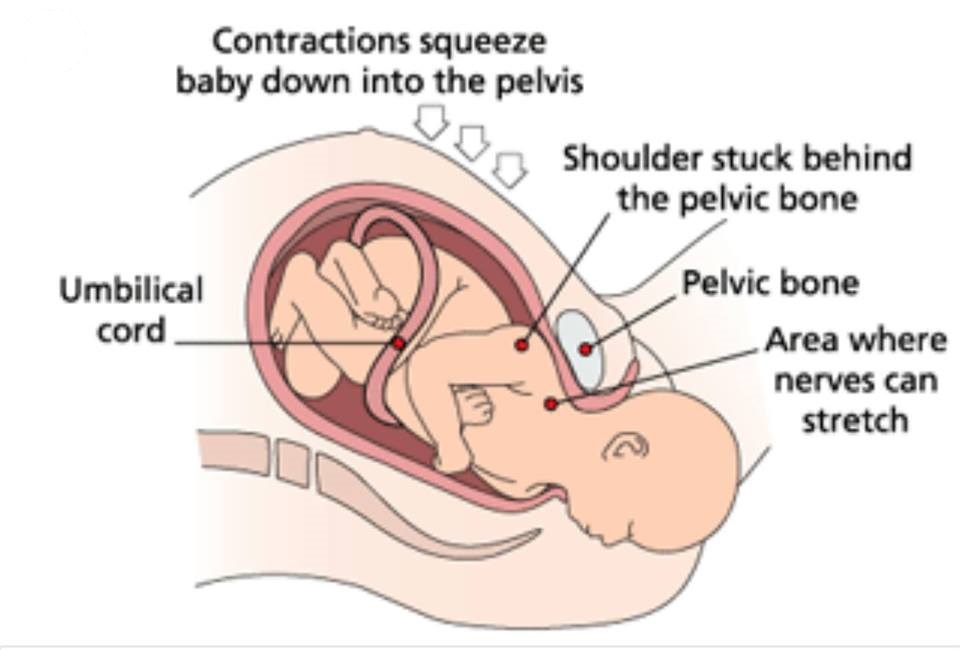 Also, they can develop as a result of mucoid degeneration inside the cord. It is not uncommon to see single cysts or multiple focal lesions. The diameter of these lesions is less than 2 cm approximately.
Also, they can develop as a result of mucoid degeneration inside the cord. It is not uncommon to see single cysts or multiple focal lesions. The diameter of these lesions is less than 2 cm approximately.
On the contrary, true cysts of the umbilical cord develop commonly from the omphalomesenteric duct or other primitive embryonic structures, including the allantois. True cysts have a distinct epithelial lining; hence they are known as true cysts.[42] In general, umbilical cysts are considered clinically significant. They serve as an early indicator of chromosomal abnormalities, especially if cysts persist during the second and third trimester of pregnancy. Thus, fetal karyotyping and amniocentesis are useful diagnostic procedures to determine any underlying conditions associated with them.
Umbilical Granuloma
An umbilical granuloma is a red nodule that may develop after the umbilical cord has separated from the naval of a newborn. On average, the diameter of a granuloma is about five mm. [40] The development of this lesion involves an abnormal proliferation of fibroblasts at the umbilicus forming thick layers of granulation tissue and endothelium. The vessels enclosed within the lesion have a dotted or strawberry-like appearance.[43] The mainstay of treatment is chemical cauterization with silver nitrate. Extra caution is needed to avoid injury or chemical burns of the surrounding skin. However, it is of great clinical significance to provide further evaluation of persistent umbilical granulomas as they can be mistaken for polyps that may require surgical removal.
[40] The development of this lesion involves an abnormal proliferation of fibroblasts at the umbilicus forming thick layers of granulation tissue and endothelium. The vessels enclosed within the lesion have a dotted or strawberry-like appearance.[43] The mainstay of treatment is chemical cauterization with silver nitrate. Extra caution is needed to avoid injury or chemical burns of the surrounding skin. However, it is of great clinical significance to provide further evaluation of persistent umbilical granulomas as they can be mistaken for polyps that may require surgical removal.
Review Questions
Access free multiple choice questions on this topic.
Comment on this article.
Figure
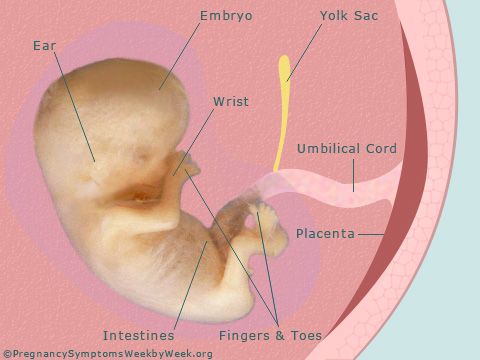
Development of the Fetal membrane and the Placenta, Diagram illustrating a later stage in the development of the umbilical cord, Placental villi, Umbilical cord, Allantois, Heart, Embryo. Contributed by Gray's Anatomy Plates
Figure
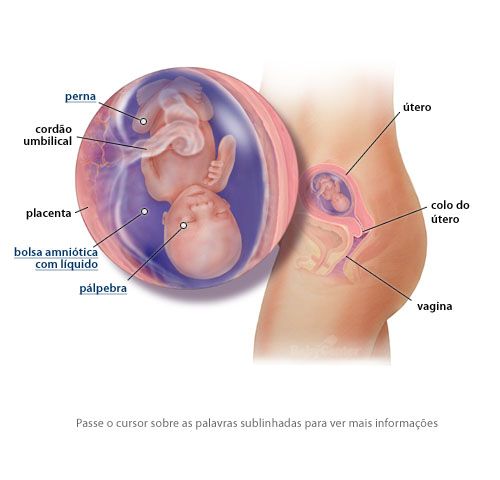
Development of Fetal Membranes and Placenta, Fetus in utero; between fifth and sixth months, Umbilical cord, Cervix uteri.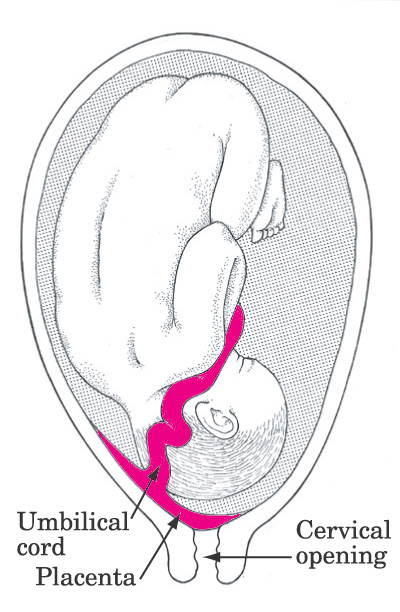 Contributed by Gray's Anatomy Plates
Contributed by Gray's Anatomy Plates
Figure
The Branchial Region, Embryo of about six weeks, Umbilical cord, Embryology. Contributed by Gray's Anatomy Plates
Figure
Umbilical cord. Image courtesy S Bhimji MD
References
- 1.
Barrios-Arpi LM, Rodríguez Gutiérrez JL, Lopez-Torres B. Histological characterization of umbilical cord in alpaca (Vicugna pacos). Anat Histol Embryol. 2017 Dec;46(6):533-538. [PubMed: 28884482]
- 2.
Tokar B, Yucel F. Anatomical variations of medial umbilical ligament: clinical significance in laparoscopic exploration of children. Pediatr Surg Int. 2009 Dec;25(12):1077-80. [PubMed: 19727772]
- 3.
Mamatha H, Hemalatha B, Vinodini P, Souza AS, Suhani S. Anatomical Study on the Variations in the Branching Pattern of Internal Iliac Artery. Indian J Surg. 2015 Dec;77(Suppl 2):248-52. [PMC free article: PMC4692843] [PubMed: 26730003]
- 4.
Hooper SB, Polglase GR, te Pas AB.
 A physiological approach to the timing of umbilical cord clamping at birth. Arch Dis Child Fetal Neonatal Ed. 2015 Jul;100(4):F355-60. [PubMed: 25540147]
A physiological approach to the timing of umbilical cord clamping at birth. Arch Dis Child Fetal Neonatal Ed. 2015 Jul;100(4):F355-60. [PubMed: 25540147]- 5.
Di Naro E, Ghezzi F, Raio L, Franchi M, D'Addario V. Umbilical cord morphology and pregnancy outcome. Eur J Obstet Gynecol Reprod Biol. 2001 Jun;96(2):150-7. [PubMed: 11384798]
- 6.
Fathi AH, Soltanian H, Saber AA. Surgical anatomy and morphologic variations of umbilical structures. Am Surg. 2012 May;78(5):540-4. [PubMed: 22546125]
- 7.
Parada Villavicencio C, Adam SZ, Nikolaidis P, Yaghmai V, Miller FH. Imaging of the Urachus: Anomalies, Complications, and Mimics. Radiographics. 2016 Nov-Dec;36(7):2049-2063. [PubMed: 27831842]
- 8.
Umeda S, Usui N, Kanagawa T, Yamamichi T, Nara K, Ueno T, Owari M, Uehara S, Oue T, Kimura T, Okuyama H. Prenatal and Postnatal Clinical Course of an Urachus Identified as an Allantoic Cyst in the Umbilical Cord. Eur J Pediatr Surg.
 2016 Apr;26(2):200-2. [PubMed: 26981767]
2016 Apr;26(2):200-2. [PubMed: 26981767]- 9.
Ullberg U, Sandstedt B, Lingman G. Hyrtl's anastomosis, the only connection between the two umbilical arteries. A study in full term placentas from AGA infants with normal umbilical artery blood flow. Acta Obstet Gynecol Scand. 2001 Jan;80(1):1-6. [PubMed: 11167180]
- 10.
Ullberg U, Lingman G, Ekman-Ordeberg G, Sandstedt B. Hyrtl's anastomosis is normally developed in placentas from small for gestational age infants. Acta Obstet Gynecol Scand. 2003 Aug;82(8):716-21. [PubMed: 12848642]
- 11.
Coetzee AJ, Castro E, Peres LC. Umbilical Cord Coiling and Zygosity: Is there a Link? Fetal Pediatr Pathol. 2015;34(5):336-9. [PubMed: 26291249]
- 12.
Hubbard LJ, Stanford DA. The Umbilical Cord Lifeline. J Emerg Nurs. 2017 Nov;43(6):593-595. [PubMed: 29100578]
- 13.
Kiserud T, Acharya G. The fetal circulation. Prenat Diagn. 2004 Dec 30;24(13):1049-59.
 [PubMed: 15614842]
[PubMed: 15614842]- 14.
Strong A, Gračner T, Chen P, Kapinos K. On the Value of the Umbilical Cord Blood Supply. Value Health. 2018 Sep;21(9):1077-1082. [PubMed: 30224112]
- 15.
Jin ZW, Nakamura T, Yu HC, Kimura W, Murakami G, Cho BH. Fetal anatomy of peripheral lymphatic vessels: a D2-40 immunohistochemical study using an 18-week human fetus (CRL 155 mm). J Anat. 2010 Jun;216(6):671-82. [PMC free article: PMC2952380] [PubMed: 20408907]
- 16.
Marx GF, Joshi CW, Orkin LR. Placental transmission of nitrous oxide. Anesthesiology. 1970 May;32(5):429-32. [PubMed: 5445031]
- 17.
DeFreitas MJ, Mathur D, Seeherunvong W, Cano T, Katsoufis CP, Duara S, Yasin S, Zilleruelo G, Rodriguez MM, Abitbol CL. Umbilical artery histomorphometry: a link between the intrauterine environment and kidney development. J Dev Orig Health Dis. 2017 Jun;8(3):349-356. [PubMed: 28260559]
- 18.
Hardy KJ, Nye DH. The anatomy of the umbilical vein.
 Aust N Z J Surg. 1969 Nov;39(2):127-32. [PubMed: 5264514]
Aust N Z J Surg. 1969 Nov;39(2):127-32. [PubMed: 5264514]- 19.
Baudin B, Bruneel A, Bosselut N, Vaubourdolle M. A protocol for isolation and culture of human umbilical vein endothelial cells. Nat Protoc. 2007;2(3):481-5. [PubMed: 17406610]
- 20.
Kashanian M, Akbarian A, Kouhpayehzadeh J. The umbilical coiling index and adverse perinatal outcome. Int J Gynaecol Obstet. 2006 Oct;95(1):8-13. [PubMed: 16860802]
- 21.
Ernst LM, Minturn L, Huang MH, Curry E, Su EJ. Gross patterns of umbilical cord coiling: correlations with placental histology and stillbirth. Placenta. 2013 Jul;34(7):583-8. [PubMed: 23642640]
- 22.
Feliks M, Howorka E. [Functional value of false knots of the umbilical cord]. Ginekol Pol. 1968 Jun;39(6):617-24. [PubMed: 5675023]
- 23.
Lubusky M, Dhaifalah I, Prochazka M, Hyjanek J, Mickova I, Vomackova K, Santavy J. Single umbilical artery and its siding in the second trimester of pregnancy: relation to chromosomal defects.
 Prenat Diagn. 2007 Apr;27(4):327-31. [PubMed: 17286313]
Prenat Diagn. 2007 Apr;27(4):327-31. [PubMed: 17286313]- 24.
Geipel A, Germer U, Welp T, Schwinger E, Gembruch U. Prenatal diagnosis of single umbilical artery: determination of the absent side, associated anomalies, Doppler findings and perinatal outcome. Ultrasound Obstet Gynecol. 2000 Feb;15(2):114-7. [PubMed: 10775992]
- 25.
Blazer S, Sujov P, Escholi Z, Itai BH, Bronshtein M. Single umbilical artery--right or left? does it matter? Prenat Diagn. 1997 Jan;17(1):5-8. [PubMed: 9021822]
- 26.
Budorick NE, Kelly TF, Dunn JA, Scioscia AL. The single umbilical artery in a high-risk patient population: what should be offered? J Ultrasound Med. 2001 Jun;20(6):619-27; quiz 628. [PubMed: 11400936]
- 27.
Abuhamad AZ, Shaffer W, Mari G, Copel JA, Hobbins JC, Evans AT. Single umbilical artery: does it matter which artery is missing? Am J Obstet Gynecol. 1995 Sep;173(3 Pt 1):728-32. [PubMed: 7573234]
- 28.
Sepulveda W, Peek MJ, Hassan J, Hollingsworth J. Umbilical vein to artery ratio in fetuses with single umbilical artery. Ultrasound Obstet Gynecol. 1996 Jul;8(1):23-6. [PubMed: 8843614]
- 29.
Hoagland MA, Chatterjee D. Anesthesia for fetal surgery. Paediatr Anaesth. 2017 Apr;27(4):346-357. [PubMed: 28211140]
- 30.
Tomek S, Asch S. Umbilical vein catheterization in the critical newborn: a review of anatomy and technique. EMS World. 2013 Feb;42(2):50-2. [PubMed: 23469464]
- 31.
Umbilical-artery catheters. N Engl J Med. 1979 Feb 08;300(6):316-7. [PubMed: 759887]
- 32.
Shevell T, Malone FD, Vidaver J, Porter TF, Luthy DA, Comstock CH, Hankins GD, Eddleman K, Dolan S, Dugoff L, Craigo S, Timor IE, Carr SR, Wolfe HM, Bianchi DW, D'Alton ME. Assisted reproductive technology and pregnancy outcome. Obstet Gynecol. 2005 Nov;106(5 Pt 1):1039-45. [PubMed: 16260523]
- 33.
Yanaihara A, Hatakeyama S, Ohgi S, Motomura K, Taniguchi R, Hirano A, Takenaka S, Yanaihara T.
 Difference in the size of the placenta and umbilical cord between women with natural pregnancy and those with IVF pregnancy. J Assist Reprod Genet. 2018 Mar;35(3):431-434. [PMC free article: PMC5904058] [PubMed: 29134477]
Difference in the size of the placenta and umbilical cord between women with natural pregnancy and those with IVF pregnancy. J Assist Reprod Genet. 2018 Mar;35(3):431-434. [PMC free article: PMC5904058] [PubMed: 29134477]- 34.
Painter D, Russell P. Four-vessel umbilical cord associated with multiple congenital anomalies. Obstet Gynecol. 1977 Oct;50(4):505-7. [PubMed: 904818]
- 35.
Kim JH, Jin ZW, Murakami G, Chai OH, Rodríguez-Vázquez JF. Persistent right umbilical vein: a study using serial sections of human embryos and fetuses. Anat Cell Biol. 2018 Sep;51(3):218-222. [PMC free article: PMC6172587] [PubMed: 30310717]
- 36.
Sepulveda W, Shennan AH, Bower S, Nicolaidis P, Fisk NM. True knot of the umbilical cord: a difficult prenatal ultrasonographic diagnosis. Ultrasound Obstet Gynecol. 1995 Feb;5(2):106-8. [PubMed: 7719859]
- 37.
Olaya-C M, Bernal JE. Clinical associations to abnormal umbilical cord length in Latin American newborns.
 J Neonatal Perinatal Med. 2015;8(3):251-6. [PubMed: 26485559]
J Neonatal Perinatal Med. 2015;8(3):251-6. [PubMed: 26485559]- 38.
Wakhlu A, Wakhlu AK. The management of exomphalos. J Pediatr Surg. 2000 Jan;35(1):73-6. [PubMed: 10646778]
- 39.
Hoopmann M, Kagan KO. Abnormal Placentation and Umbilical Cord Insertion. Ultraschall Med. 2020 Apr;41(2):120-137. [PubMed: 32259863]
- 40.
Muniraman H, Sardesai T, Sardesai S. Disorders of the Umbilical Cord. Pediatr Rev. 2018 Jul;39(7):332-341. [PubMed: 29967078]
- 41.
Hannaford K, Reeves S, Wegner E. Umbilical cord cysts in the first trimester: are they associated with pregnancy complications? J Ultrasound Med. 2013 May;32(5):801-6. [PubMed: 23620322]
- 42.
Whipple NS, Bennett EE, Kaza E, O'Connor M. Umbilical Cord Pseudocyst in a Newborn. J Pediatr. 2016 Oct;177:333. [PubMed: 27473880]
- 43.
Ancer-Arellano J, Argenziano G, Villarreal-Martinez A, Cardenas-de la Garza JA, Villarreal-Villarreal CD, Ocampo-Candiani J.
 Dermoscopic findings of umbilical granuloma. Pediatr Dermatol. 2019 May;36(3):393-394. [PubMed: 30811653]
Dermoscopic findings of umbilical granuloma. Pediatr Dermatol. 2019 May;36(3):393-394. [PubMed: 30811653]
Umbilical cord: Anatomical structure and function
Author: Sophie Stewart • Reviewer: Dimitrios Mytilinaios MD, PhD
Last reviewed: November 14, 2022
Reading time: 1 minute
Umbilical cord
Funiculus umbilicalis
1/5
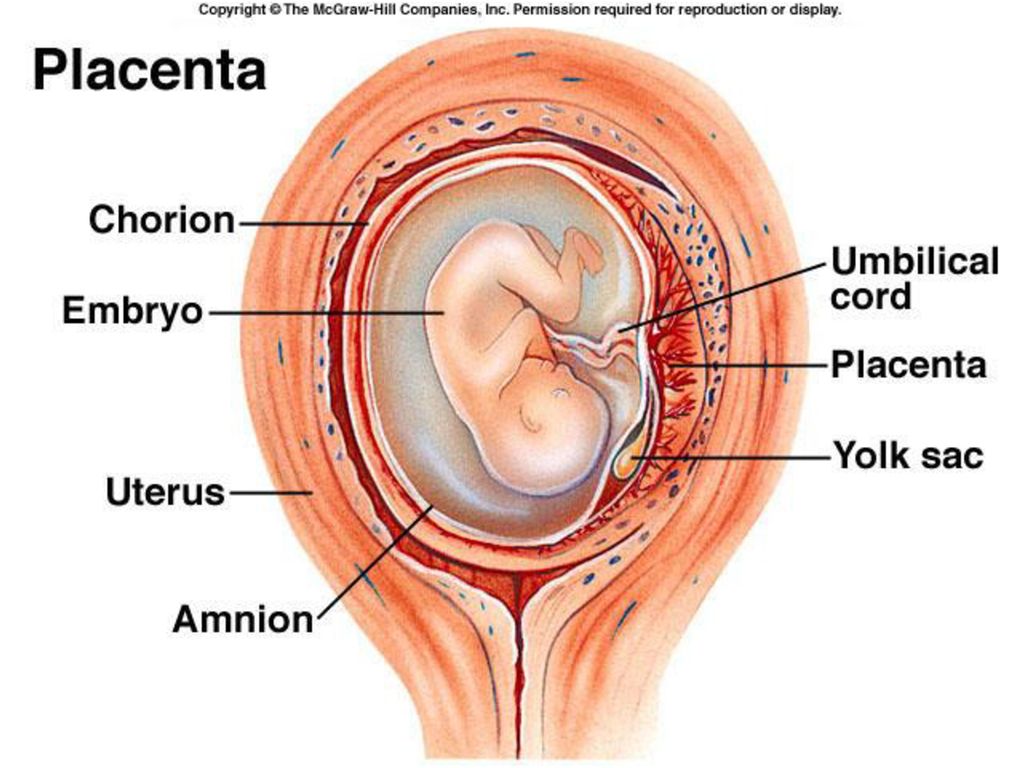
The umbilical cord is a fetal organ connecting the placenta to the developing fetus. This structure allows for the passage of oxygen and nutrients from the maternal circulation to the fetal circulation. In doing so, it also functions to remove waste products from fetal circulation.
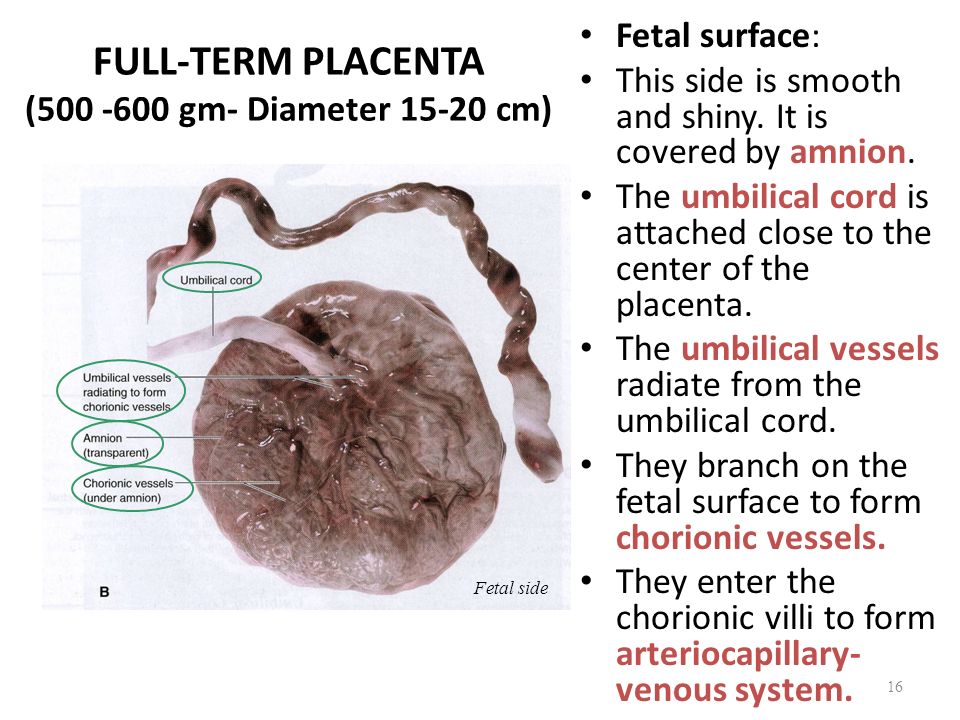
The umbilical cord attaches to the fetus at the umbilicus and extends to insert onto the center of the placental bulk. On average it measures 55-60 cm in length and has a diameter of 1-2cm.
The umbilical cord is a bundle of blood vessels contained within a tubular sheath of amnion and consists of two paired umbilical arteries and one umbilical vein.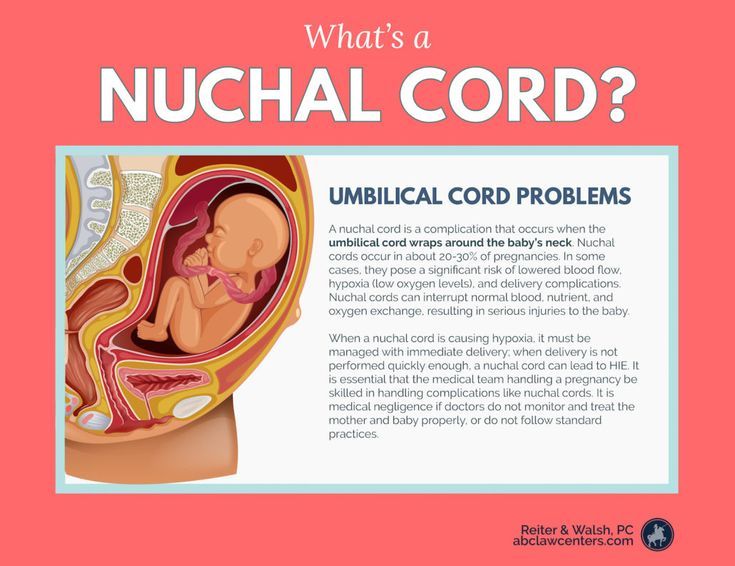 The paired umbilical arteries function to carry deoxygenated blood from the fetus to the placenta while the umbilical vein carries oxygenated blood from the placenta to the fetus.
The paired umbilical arteries function to carry deoxygenated blood from the fetus to the placenta while the umbilical vein carries oxygenated blood from the placenta to the fetus.
| Terminology | English: Umbilical cord Latin: Funiculus umbilicalis |
| Location | Attaches to the fetus at the umbilicus and center of the placental bulk |
| Structure | Blood vessel bundle surrounded by a tubular sheath of amnion Composed of: Two paired umbilical arteries and one umbilical vein |
| Function | Vital passage for nutrients, oxygen and waste products to and from the fetus |
Take a closer look at the structures of the fetus in utero using the study unit below.
Fetus in utero Explore study unit
All content published on Kenhub is reviewed by medical and anatomy experts.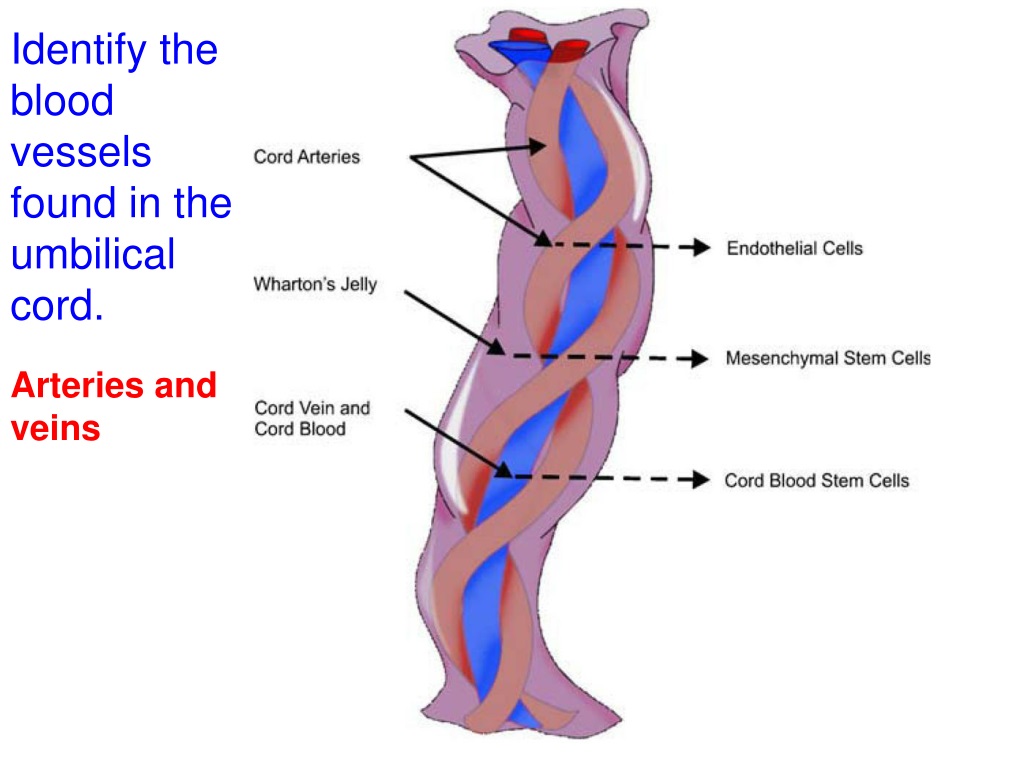 The information we provide is grounded on academic literature and peer-reviewed research. Kenhub does not provide medical advice. You can learn more about our content creation and review standards by reading our content quality guidelines.
The information we provide is grounded on academic literature and peer-reviewed research. Kenhub does not provide medical advice. You can learn more about our content creation and review standards by reading our content quality guidelines.
Jauniaux E, Burton GJ. Implantation and placentation. In: Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 41st ed. Elsevier; 2016. p. 189.
Umbilical cord: want to learn more about it?
Our engaging videos, interactive quizzes, in-depth articles and HD atlas are here to get you top results faster.
What do you prefer to learn with?
Videos Quizzes Both
“I would honestly say that Kenhub cut my study time in half.” – Read more. Kim Bengochea, Regis University, Denver
© Unless stated otherwise, all content, including illustrations are exclusive property of Kenhub GmbH, and are protected by German and international copyright laws. All rights reserved.what is dangerous and what may be the consequences - article of the reproductive center "For the Birth"
Take the first step
make an appointment with a doctor!
The umbilical cord is a rather simple organ in structure, but very important in meaning.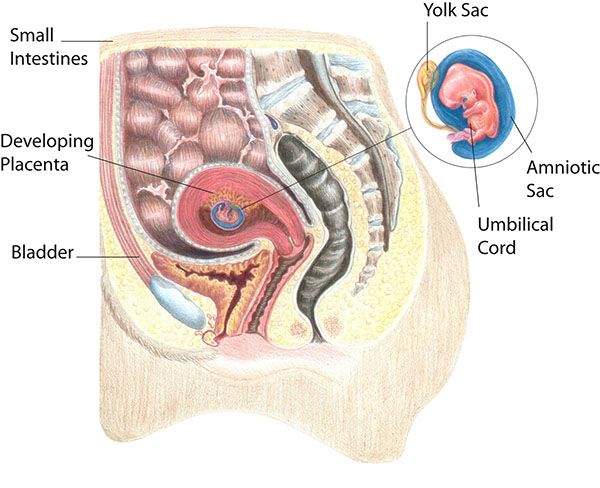 It plays an important role in ensuring the normal functioning of the baby during the gestation period. Accordingly, various anomalies and pathologies of its structure adversely affect the condition of the child, can lead to birth defects and even death. One of the problems that pregnant women face is a short umbilical cord in the fetus. This is a rather serious pathology that can seriously complicate gestation and childbirth, up to their complete impossibility. nine0006
It plays an important role in ensuring the normal functioning of the baby during the gestation period. Accordingly, various anomalies and pathologies of its structure adversely affect the condition of the child, can lead to birth defects and even death. One of the problems that pregnant women face is a short umbilical cord in the fetus. This is a rather serious pathology that can seriously complicate gestation and childbirth, up to their complete impossibility. nine0006
The umbilical cord and its role in childbearing
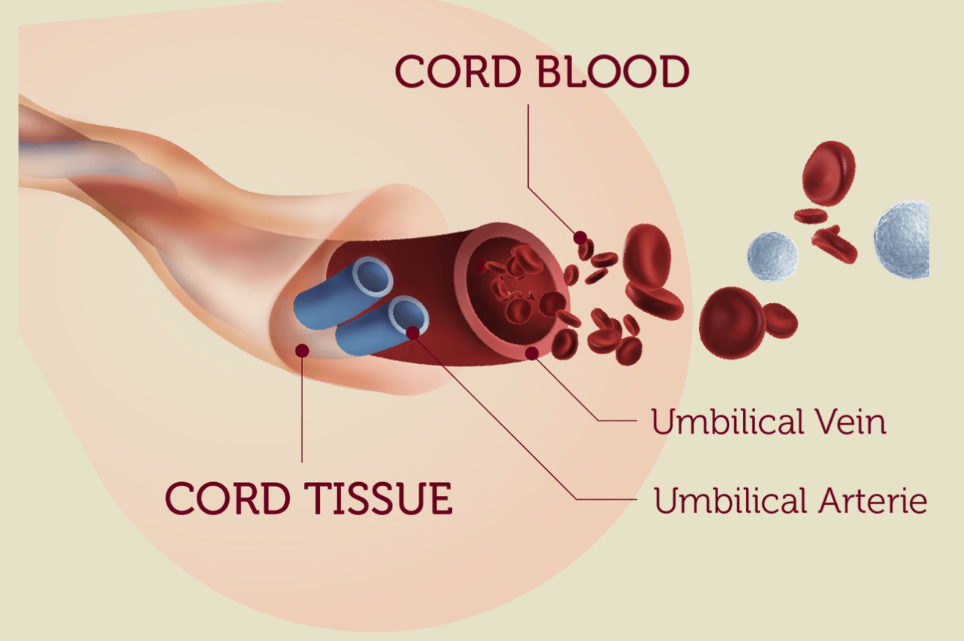
The umbilical cord is a hollow, flexible tube that connects the abdominal wall of the fetus to the placenta. Inside it runs:
- 1 vein, through which the baby from the maternal circulation receives blood enriched with oxygen and nutrients;
- 2 arteries through which fetal waste products (urea, carbon dioxide, etc.) are excreted back;
- Yolk duct, connecting the intestines of the embryo with the yolk sac, which contains a supply of nutrients; nine0015
- Urachus is a duct that connects the fetal bladder with the placenta and serves to remove metabolic products.
The outer shell (amnion) consists of strong connective tissue and protects blood vessels from damage. The space between it, the artery and the veins is filled with Wharton's jelly - a jelly-like or mucous substance consisting of polysaccharides. It gives the umbilical cord elasticity and prevents it from twisting, thereby protecting the veins from the formation of kinks and mechanical damage. nine0006
Thus, the purpose of the umbilical cord is to provide nutrition, respiration and metabolism of the fetus during the gestation period. Since his own organs and systems are just being formed, their function is shifted to the mother's body. During childbirth, the blood vessels in the umbilical cord, under the influence of the hormone oxytocin, "collapse", gradually blocking the blood flow. This is how the atrophy of the umbilical cord begins, which normally ends completely a few hours after the birth of the child. Under natural conditions, the umbilical cord dies and falls off by itself, but in the maternity hospital it is cut 1-3 minutes after birth.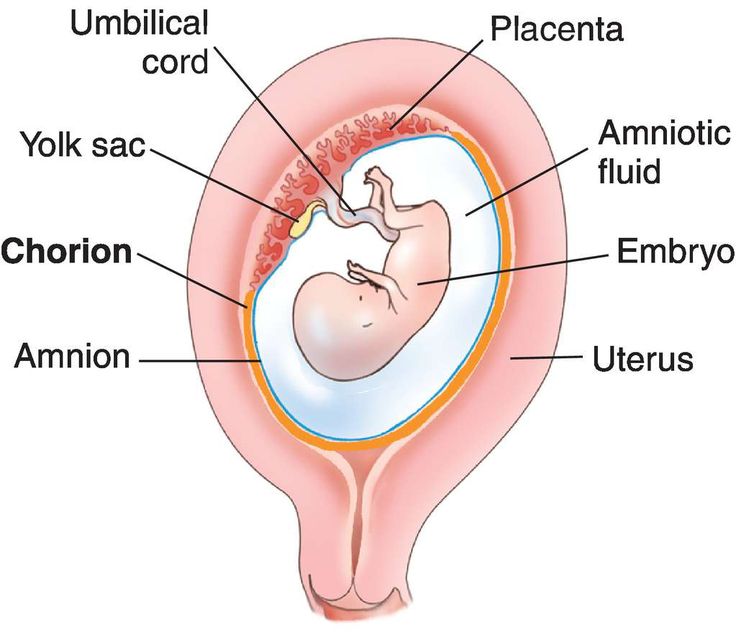 This minimizes the risk of infection. nine0006
This minimizes the risk of infection. nine0006
Take the first step
make an appointment with a doctor!
Short umbilical cord during pregnancy
: causes and symptomsNormally, the length of the umbilical cord in humans is 50-70 cm. This size reduces the likelihood of its twisting, due to which hypoxia and nutritional deficiencies can occur in the fetus. However, quite often in pregnant women there are violations of the length of the umbilical cord - in particular, its shortening. If the length of the organ is less than 50-40 cm, it is considered abnormally short. Depending on the causes of the pathology and the size of the umbilical cord, two types of anomalies are distinguished: nine0006
- Relatively short cord. It initially has a normal size, but in the process of gestation it shortens due to twisting or entwining around the fetus, the formation of varicose nodes on the organ.
 Most often this happens if the expectant mother does not eat well, uses alcohol and drugs, smokes, experiences constant stress, suffers from chronic systemic and gynecological diseases. Such a pathology poses a danger to the health and life of the child due to impaired blood circulation and the accompanying hypoxia. However, a shortened umbilical cord can unravel on its own, and therefore has a more favorable prognosis. nine0015
Most often this happens if the expectant mother does not eat well, uses alcohol and drugs, smokes, experiences constant stress, suffers from chronic systemic and gynecological diseases. Such a pathology poses a danger to the health and life of the child due to impaired blood circulation and the accompanying hypoxia. However, a shortened umbilical cord can unravel on its own, and therefore has a more favorable prognosis. nine0015 - Absolutely short umbilical cord. This is a genetic pathology associated with a violation of the mechanism of formation of the placenta. Factors contributing to this condition are hereditary diseases, chromosomal mutations. It occurs in most cases, also carries a great threat to the fetus. However, unlike the pathology of the previous type, an absolutely short umbilical cord cannot be treated.
The danger of this pathological condition is that outwardly it does not give itself away. The expectant mother does not experience any inconvenience and pain, nothing threatens her life.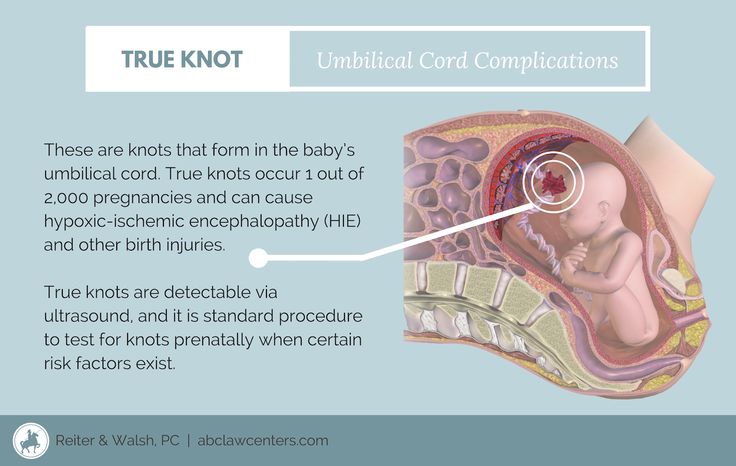 Very often, a woman finds out that she has an abnormally short umbilical cord already during childbirth. Typical signs of this pathology: nine0006
Very often, a woman finds out that she has an abnormally short umbilical cord already during childbirth. Typical signs of this pathology: nine0006
- Extended delivery time. In patients giving birth for the first time, they can last up to 20 hours, in those who have already given birth again - up to 15 hours.
- Early delivery of the placenta. Normally, she is born within 20-50 minutes after the fetus leaves the woman's birth canal. If the umbilical cord is too short, the child "pulls" it along, which is often accompanied by its separation and bleeding.
- Fetal hypoxia. This symptom is not direct evidence of an abnormally short length of the umbilical cord, since this condition is also observed in some other intrauterine pathologies. However, in combination with the above symptoms, fetal hypoxia may indicate a violation of the development or structure of the umbilical cord. nine0015
- Fetal hyperactivity.
 With acute hypoxia, the child begins to make energetic movements. His heart rate first increases to 160 beats per minute, then becomes slow (no more than 120 heartbeats). In addition, as a result of increased activity of the intestines of the fetus, meconium may appear in the amniotic fluid - the primary feces, consisting of bile, mucus, prenatal hair, and amniotic fluid digested by it.
With acute hypoxia, the child begins to make energetic movements. His heart rate first increases to 160 beats per minute, then becomes slow (no more than 120 heartbeats). In addition, as a result of increased activity of the intestines of the fetus, meconium may appear in the amniotic fluid - the primary feces, consisting of bile, mucus, prenatal hair, and amniotic fluid digested by it.
Thus, it is possible to judge the presence of a short umbilical cord in the fetus either by the fact of birth, or using modern diagnostic tools that allow you to track the condition of the baby in the prenatal period. nine0006
Take the first step
make an appointment with a doctor!
Why is a short umbilical cord dangerous ?
Both absolutely and relatively short umbilical cord are pathological anomalies, potentially dangerous for the life and health of the child. Chronic hypoxia causes the greatest damage to it, which develops due to insufficient oxygen supply to the tissues (including the brain). Its result is the death of the baby during gestation or during childbirth, as well as congenital pathologies caused by the death of neurons in the brain or spinal cord. Also, a short umbilical cord during childbirth can cause the following complications: nine0006
Chronic hypoxia causes the greatest damage to it, which develops due to insufficient oxygen supply to the tissues (including the brain). Its result is the death of the baby during gestation or during childbirth, as well as congenital pathologies caused by the death of neurons in the brain or spinal cord. Also, a short umbilical cord during childbirth can cause the following complications: nine0006
- Slow progression of the child through the genital tract, which again causes hypoxia and too long compression of the skull bones, leading to death or developmental disorders;
- Placental abruption, which is accompanied by intrauterine bleeding, hemorrhagic shock due to large blood loss, DIC, which simultaneously leads to the formation of blood clots and massive hemorrhages that threaten the life of both the fetus and the woman herself;
- Incorrect presentation of the fetus in the uterus, which can lead to various birth injuries - ruptures, sprains, etc.
Thus, the consequences that arise with a short umbilical cord concern not only the child himself, but also the mother.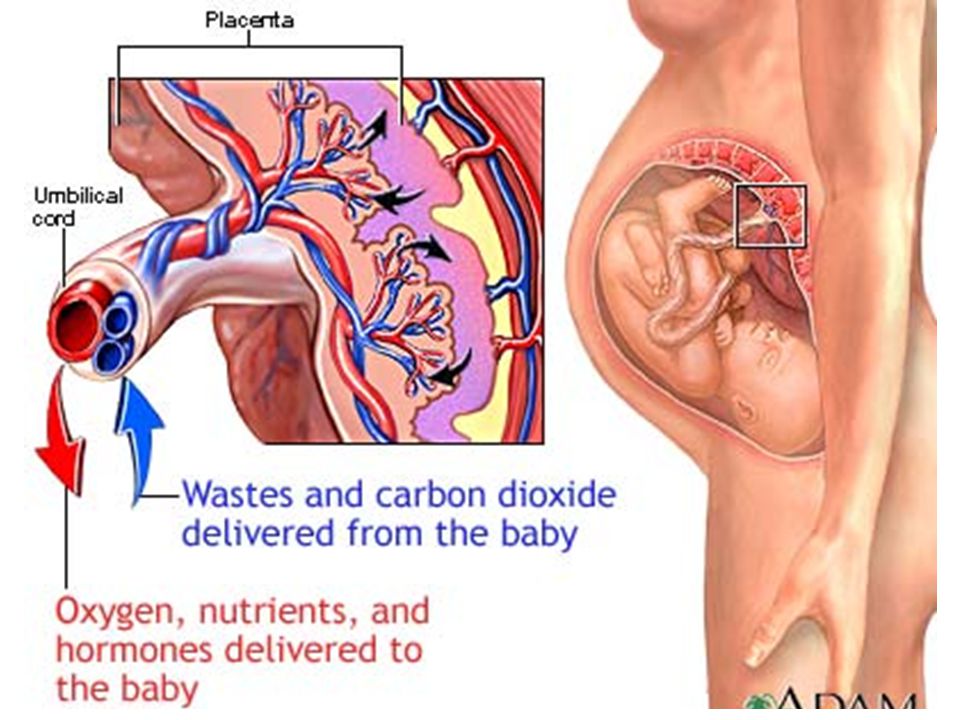 In severe cases, this pathology can lead to the loss of a newborn, infertility and death of the woman herself.
In severe cases, this pathology can lead to the loss of a newborn, infertility and death of the woman herself.
Take the first step
make an appointment with a doctor!
Diagnosis of the short umbilical cord
As already mentioned, this pathology during pregnancy does not affect the condition of the woman herself, which significantly complicates her diagnosis. Often they learn about it only directly during childbirth, when complications begin. However, a short umbilical cord directly affects the condition of the fetus, and its changes can be fixed by modern diagnostic tools: nine0006
- Ultrasound. Ultrasound examination allows you to get a visual picture of the umbilical cord, which can be used to judge the presence of knots and entanglements around the fetus on it. Unfortunately, this method does not accurately measure the length of the umbilical cord and, therefore, accurately diagnose the pathology.
- UZDG.
 Doppler ultrasound is a type of ultrasound, but fixes the parameters of dynamic (moving) objects, while conventional ultrasound is used to study mostly static ones. This method is based on the fact that sound waves are reflected from moving objects with a change in frequency. Ultrasound, in particular, allows you to determine the speed and direction of blood flow in the umbilical vessels. However, as in the previous case, these are only indirect signs that do not allow an accurate diagnosis. nine0015
Doppler ultrasound is a type of ultrasound, but fixes the parameters of dynamic (moving) objects, while conventional ultrasound is used to study mostly static ones. This method is based on the fact that sound waves are reflected from moving objects with a change in frequency. Ultrasound, in particular, allows you to determine the speed and direction of blood flow in the umbilical vessels. However, as in the previous case, these are only indirect signs that do not allow an accurate diagnosis. nine0015 - KTG. One of the manifestations of a short umbilical cord in a child is hypoxia, which is accompanied by a reduction in his heart rate. To measure the heart rate of the embryo, cardiotocography is used - a type of Doppler ultrasound, with which the heartbeat is recorded. In addition to it, this method also allows you to measure the frequency of uterine contractions. By synchronizing these two indicators, the doctor can judge the state of chronic fetal hypoxia and, therefore, the possible presence of a short umbilical cord.
 nine0015
nine0015 - Gynecological examination. The standard for this procedure includes a visual examination of the cervix, which can be used to judge the position of the fetus, as well as an ultrasound scan, which monitors its heartbeat. Practice shows that a gynecological examination often reveals indirect signs of a short umbilical cord.
The disadvantage of all these methods for diagnosing a short umbilical cord is that they do not give an accurate result. However, by combining them with each other, the doctor can, with a fairly high degree of probability, make the correct diagnosis of a short umbilical cord. nine0006
Take the first step
make an appointment with a doctor!
Short cord treatment
Effective treatment of the pathology itself (both of its forms) does not currently exist. If a short umbilical cord is suspected during pregnancy, the patient is hospitalized in a hospital under constant supervision. Doctors use a wait-and-see approach, carefully monitoring fetal heart rate and mobility with ultrasound, ultrasound, and CTG.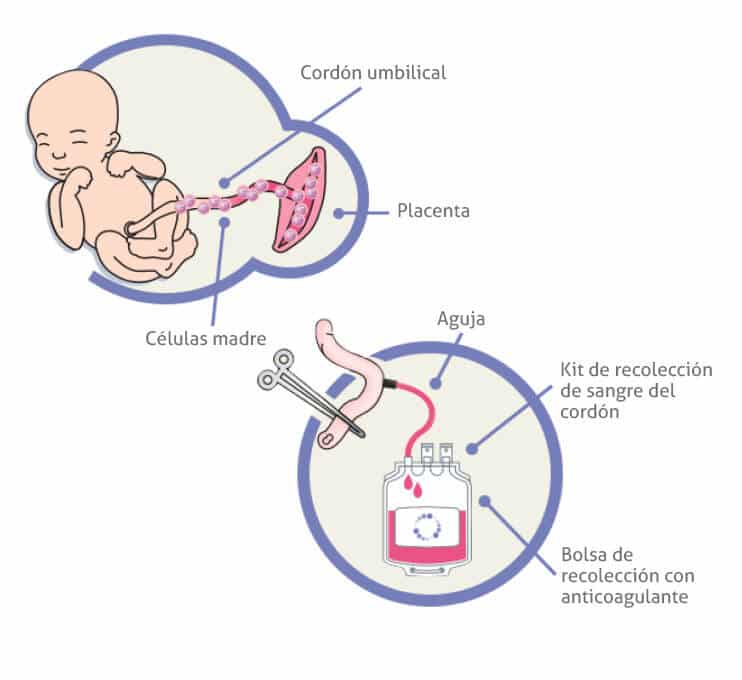 As maintenance therapy are prescribed: nine0006
As maintenance therapy are prescribed: nine0006
- Antispasmodics and mild sedatives to prevent vigorous fetal movements and cord torsion;
- Magnesium and iron preparations that improve blood oxygen supply and compensate for fetal hypoxia;
- Medicines that improve blood flow in the umbilical vessels.
Depending on the severity of the pathology, the predicted consequences of a short umbilical cord for the child and the woman herself, as well as the time of detection, the following options are possible: nine0006
- Caesarean section - it is prescribed for proven short umbilical cord and fetal hypoxia to prevent placental abruption and other complications during childbirth;
- Perineal incision - this method is used to prevent fetal hypoxia in cases where a short umbilical cord is already detected during natural childbirth.
A caesarean section can also be emergency - for example, if bleeding occurs during natural childbirth with a short umbilical cord, acute fetal hypoxia and other complications.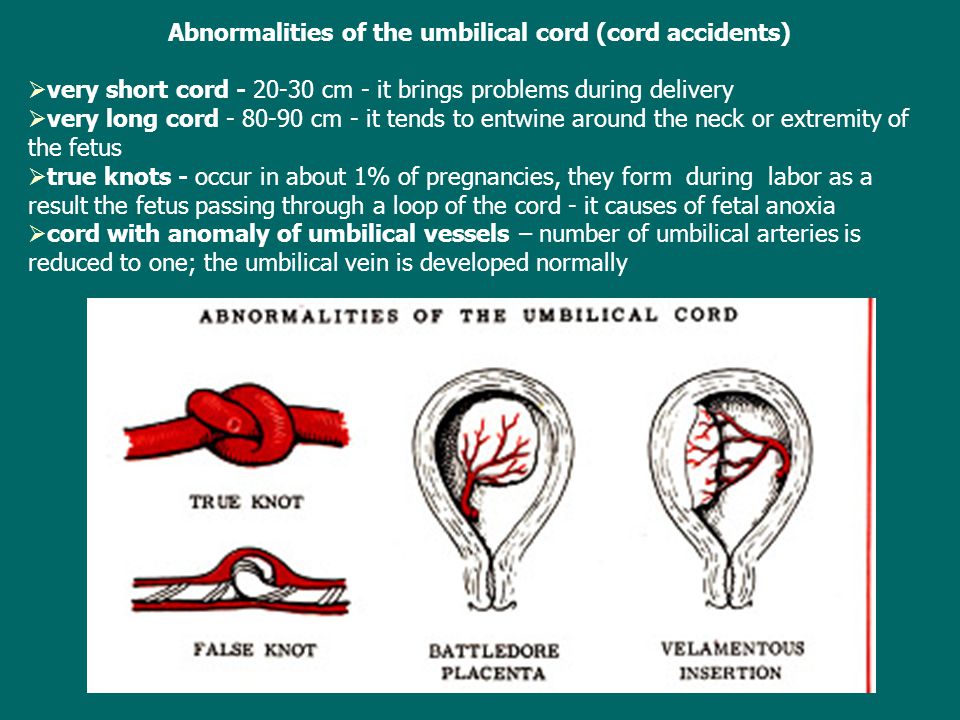 In general, even with late detection of pathology, timely and correct use of CS allows to minimize the risks for both the woman and her child. nine0006
In general, even with late detection of pathology, timely and correct use of CS allows to minimize the risks for both the woman and her child. nine0006
Take the first step
make an appointment with a doctor!
Short cord prophylaxis
Since there is currently no effective treatment for this pathology, doctors recommend reducing the risk of its development even when planning a pregnancy. If a woman cannot do anything with the hereditary physiological characteristics of her own body, then the following actions are quite within her power:
- Avoid smoking, drinking alcohol and drugs that can cause impaired development of the placental apparatus; nine0015
- Prevent fetal hyperactivity by reducing consumption of stimulant foods such as coffee, cocoa, chocolate, etc.;
- More often to be in the open air in order to saturate your own blood with fresh oxygen as much as possible, which will at least partially compensate for possible fetal hypoxia;
- Do not come into contact with toxic chemicals (varnishes, paints, industrial gases, etc.
 ) during the period of preparation for pregnancy and gestation; nine0015
) during the period of preparation for pregnancy and gestation; nine0015 - Eliminate or reduce stressful situations as much as possible - for example, change jobs, leave for a while from a dangerous urban area, etc.;
- Make your diet more varied, rich in vitamins and other useful substances - especially iron and magnesium compounds, which will improve blood oxygen saturation;
- Avoid strenuous physical activity and trauma, as they can lead to hyperdynamia of the fetus and entanglement of the umbilical cord around it. nine0015
Regular passage of scheduled medical examinations during pregnancy allows you to diagnose a possible pathology in the early stages. If the expectant mother has relatives who were born with a short umbilical cord, or she herself had this anomaly, it is recommended to be examined by a geneticist.
If you suspect a short umbilical cord in the fetus, it is important to use quality medical care. It can be provided only in licensed clinics where qualified doctors work. Also, the mother herself is required to fully trust the attending doctor and carefully follow his recommendations. Do not be afraid of such radical steps as a caesarean section - this is a long-established and simple operation that significantly reduces the likelihood of complications. nine0006
Also, the mother herself is required to fully trust the attending doctor and carefully follow his recommendations. Do not be afraid of such radical steps as a caesarean section - this is a long-established and simple operation that significantly reduces the likelihood of complications. nine0006
What are umbilical clamps used for? — Articles
The umbilical clamp avoids the complications that can occur when cutting off the umbilical cord in newborns. The umbilical anchor for babies is easy to use, sterile and environmentally friendly.
After the birth of a child, the umbilical cord, through which the fetus is fed throughout the entire gestation period, becomes unnecessary for him. The umbilical cord is cut, and an umbilical clamp is applied to the place of the cut, called the "stump". This manipulation is done right in the delivery room. nine0006
Design and purpose of the umbilical clamp
The umbilical clamp consists of two elements, the inner part of which has a slightly curved shape.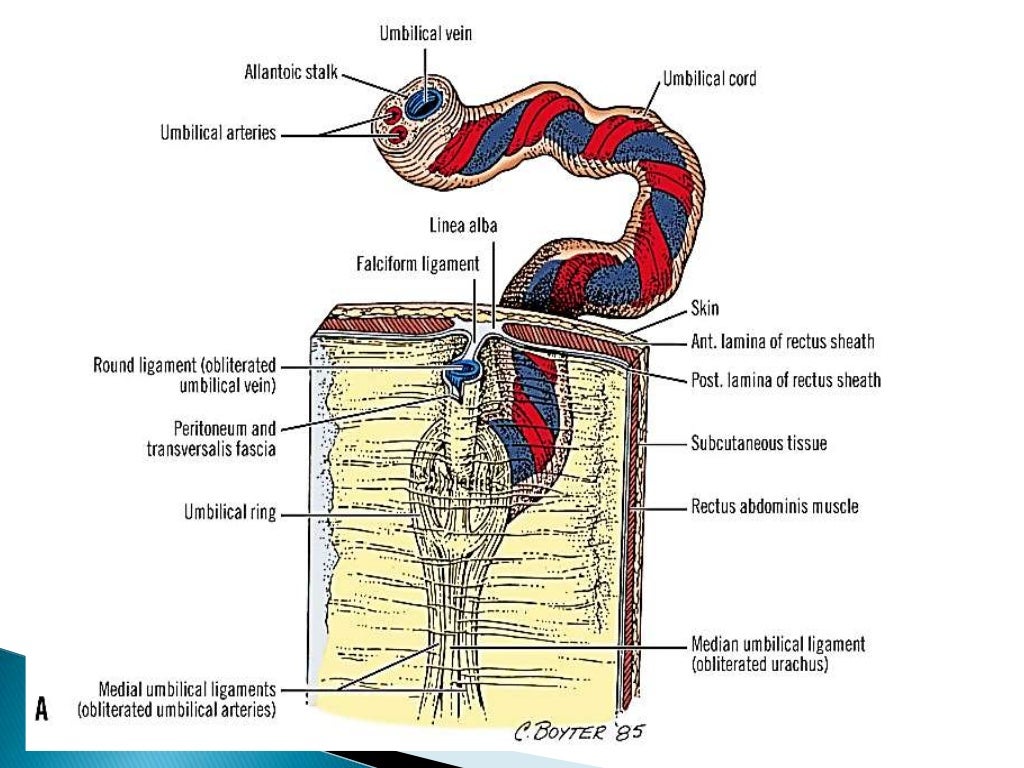 Both parts are interconnected by a ring into a movable structure. The product is made of durable and resilient polypropylene, medically tested, non-toxic and safe in every respect.
Both parts are interconnected by a ring into a movable structure. The product is made of durable and resilient polypropylene, medically tested, non-toxic and safe in every respect.
The main purpose of the product is to clamp the umbilical cord (ligature fixation of vessels) of a child after his birth. Reliable and strong compression is due to the presence of atraumatic teeth on the inner surfaces of the jaws, which prevent sliding along the soft tissue of the umbilical cord. The branches have longitudinal grooves, the presence of which is necessary for the uniform distribution of the jelly-like mass present in the umbilical cord and surrounding the blood vessels. nine0006
After the doctor fixes the clamp, the device remains in one position until the dried navel falls off. To ensure that the doctor's fingers do not slip on the outer surfaces of the branches at the moment of fixation, the latter are provided with corrugation.
The clip has a special lock that prevents accidental opening.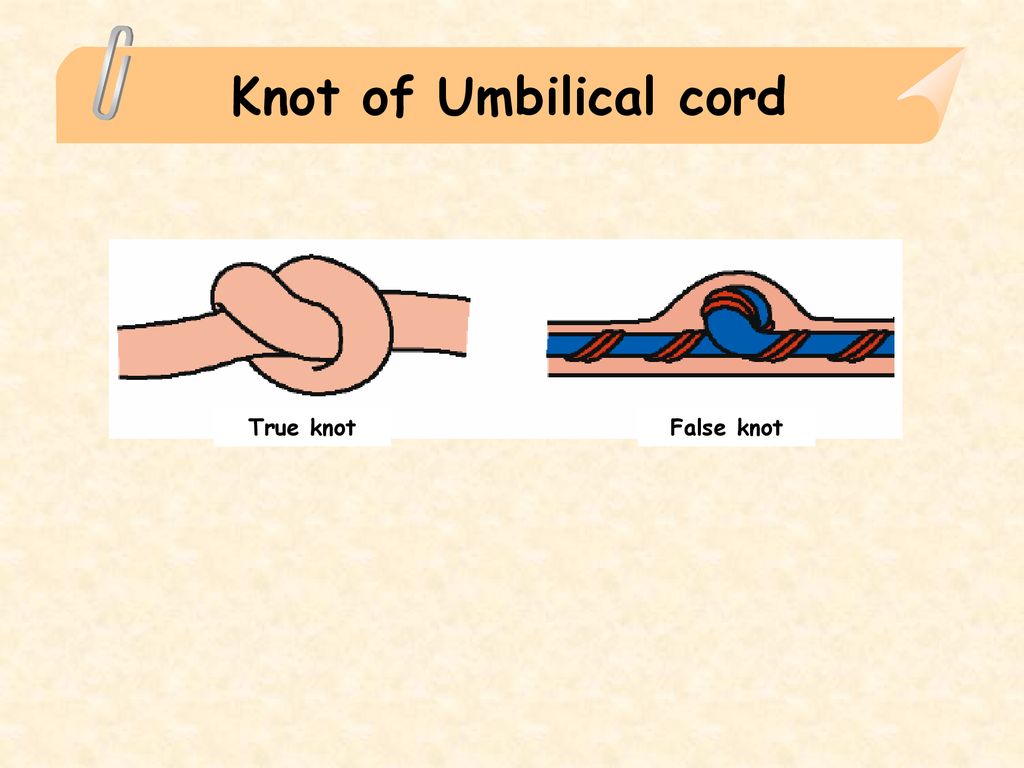 Each product undergoes an ethylene oxide sterilization process and is packaged in an individual bag. Umbilical clips are not intended for multiple use - they are disposable products that must be disposed of. nine0006
Each product undergoes an ethylene oxide sterilization process and is packaged in an individual bag. Umbilical clips are not intended for multiple use - they are disposable products that must be disposed of. nine0006
How to treat the navel with a clip
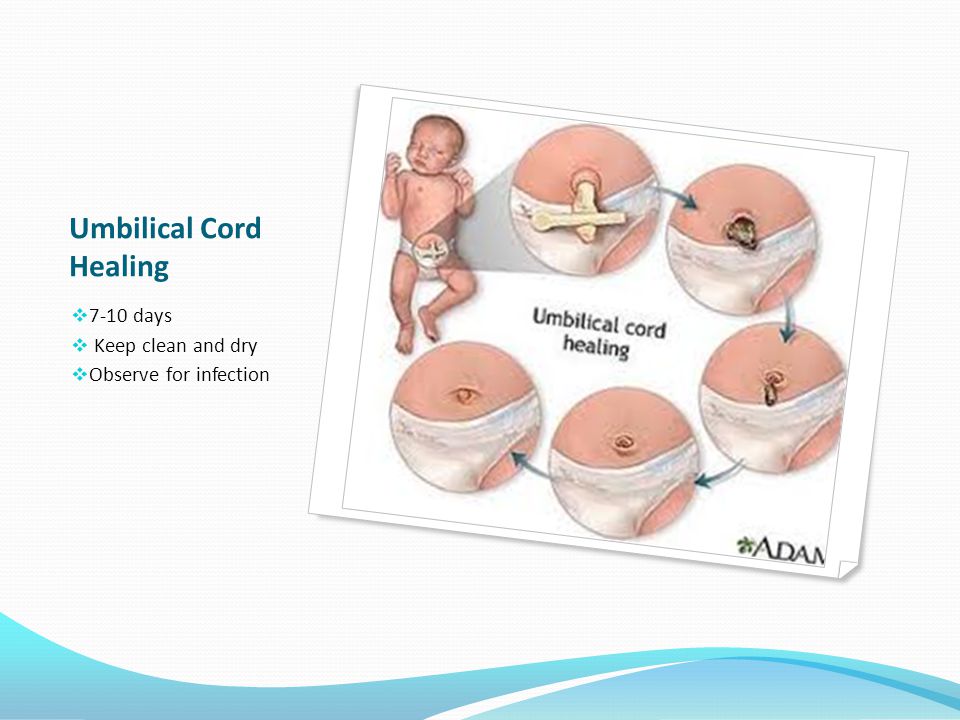
Umbilical clips are used in perinatal centers and all maternity hospitals. The purpose of using the product is to stop bleeding in the umbilical vessels and prevent umbilical infections. The umbilical clamp ensures proper healing of the navel and prevents the development of complications.
After cutting and processing the umbilical cord, it is subjected to medical treatment. As a result, a two-centimeter process remains from the long umbilical cord. Then they put a plastic clip on it. Previously, metal fixators were used for these purposes, but they quickly fell out of use because they were unsafe and could injure the child. nine0006
After the wound heals, a full-fledged navel will form in its place. However, in order for the healing process to proceed without complications, the stump must be properly processed.