Pregnant mothers with diabetes
Type 1 or Type 2 Diabetes and Pregnancy
Problems of Diabetes in Pregnancy
Blood sugar that is not well controlled in a pregnant woman with Type 1 or Type 2 diabetes could lead to problems for the woman and the baby:
Birth Defects
The organs of the baby form during the first two months of pregnancy, often before a woman knows that she is pregnant. Blood sugar that is not in control can affect those organs while they are being formed and cause serious birth defects in the developing baby, such as those of the brain, spine, and heart.
An Extra Large Baby
Diabetes that is not well controlled causes the baby’s blood sugar to be high. The baby is “overfed” and grows extra large. Besides causing discomfort to the woman during the last few months of pregnancy, an extra large baby can lead to problems during delivery for both the mother and the baby. The mother might need a C-Section to deliver the baby. The baby can be born with nerve damage due to pressure on the shoulder during delivery.
C- Section (Cesarean Section)
A C-section is a surgery to deliver the baby through the mother’s belly. A woman who has diabetes that is not well controlled has a higher chance of needing a C-section to deliver the baby. When the baby is delivered by a C-section, it takes longer for the woman to recover from childbirth.
High Blood Pressure (Preeclampsia)
When a pregnant woman has high blood pressure, protein in her urine, and often swelling in fingers and toes that doesn’t go away, she might have preeclampsia. It is a serious problem that needs to be watched closely and managed by her doctor. High blood pressure can cause harm to both the woman and her unborn baby. It might lead to the baby being born early and also could cause seizures or a stroke (a blood clot or a bleed in the brain that can lead to brain damage) in the woman during labor and delivery. Women with type 1 or type 2 diabetes have high blood pressure more often than women without diabetes.
Early (Preterm) Birth
Being born too early can result in problems for the baby, such as breathing problems, heart problems, bleeding into the brain, intestinal problems, and vision problems. Women with type 1 or type 2 diabetes are more likely to deliver early than women without diabetes.
Women with type 1 or type 2 diabetes are more likely to deliver early than women without diabetes.
Read about one woman’s experience with being pregnant and diabetic »
Low Blood Sugar (Hypoglycemia)
People with diabetes who take insulin or other diabetes medications can develop blood sugar that is too low. Low blood sugar can be very serious, and even fatal, if not treated quickly. Seriously low blood sugar can be avoided if women watch their blood sugar closely and treat low blood sugar early.
If a woman’s diabetes was not well controlled during pregnancy, her baby can very quickly develop low blood sugar after birth. The baby’s blood sugar must be watched for several hours after delivery.
Miscarriage or Stillbirth
A miscarriage is a loss of the pregnancy before 20 weeks. Stillbirth means that after 20 weeks, the baby dies in the womb. Miscarriages and stillbirths can happen for many reasons. A woman who has diabetes that is not well controlled has a higher chance of having a miscarriage or stillbirth.
7 Tips for Women with Diabetes
If a woman with diabetes keeps her blood sugar well controlled before and during pregnancy, she can increase her chances of having a healthy baby. Controlling blood sugar also reduces the chance that a woman will develop common problems of diabetes, or that the problems will get worse during pregnancy.
Steps women can take before and during pregnancy to help prevent problems:
- Plan for Pregnancy
Before getting pregnant, see your doctor. The doctor needs to look at the effects that diabetes has had on your body already, talk with you about getting and keeping control of your blood sugar, change medications if needed, and plan for frequent follow-up. If you are overweight, the doctor might recommend that you try to lose weight before getting pregnant as part of the plan to get your blood sugar in control. - See Your Doctor Early and Often
During pregnancy, a woman with diabetes needs to see the doctor more often than a pregnant woman without diabetes. Together, you and your doctor can work to prevent or catch problems early.
Together, you and your doctor can work to prevent or catch problems early. - Eat Healthy Foods
Eat healthy foods from a meal plan made for a person with diabetes. A dietitian can help you create a healthy meal plan. A dietitian can also help you learn how to control your blood sugar while you are pregnant.
Tasty Recipes for People with Diabetes and Their Families »
To Find a Dietitian:
American Dietetic Association
1–800–877–1600
www.eatright.org (click on “Find an Expert”) - Exercise Regularly
Exercise is another way to keep blood sugar under control. It helps to balance food intake. After checking with your doctor, you can exercise regularly before, during, and after pregnancy. Get at least 30 minutes of moderate-intensity physical activity at least five days a week. This could be brisk walking, swimming, or actively playing with children.
Learn more about physical activity during pregnancy » - Take Pills and Insulin as Directed
If diabetes pills or insulin are ordered by your doctor, take them as directed in order to help keep your blood sugar under control.
- Control and Treat Low Blood Sugar Quickly
Keeping blood sugar well controlled can lead to a chance of low blood sugar at times. If you are taking diabetes pills or insulin, it’s helpful to have a source of quick sugar, such as hard candy, glucose tablets or gel, on hand at all times. It’s also good to teach family members and close co-workers or friends how to help in case of a severe low blood sugar reaction. - Monitor Blood Sugar Often
Because pregnancy causes the body’s need for energy to change, blood sugar levels can change very quickly. You need to check your blood sugar often, as directed by your doctor. It is important to learn how to adjust food intake, exercise, and insulin, depending on the results of your blood sugar tests.
Learn how to take control of your diabetes »
More Information
Got diabetes? Thinking about having a baby? [PDF – 1 MB]
View, download, and print this brochure about diabetes and pregnancy.
For information on how to keep blood sugar well controlled, visit the American Diabetes Association website.
- Diabetes
- Before Pregnancy
- Healthy Pregnancy
- Birth Defects
- CDC’s National Center on Birth Defects and Developmental Disabilities
Gestational Diabetes and Pregnancy | CDC
Gestational diabetes is a type of diabetes that is first seen in a pregnant woman who did not have diabetes before she was pregnant. Some women have more than one pregnancy affected by gestational diabetes. Gestational diabetes usually shows up in the middle of pregnancy. Doctors most often test for it between 24 and 28 weeks of pregnancy.
Often gestational diabetes can be managed through eating healthy foods and regular exercise. Sometimes a woman with gestational diabetes must also take insulin.
Learn more about Diabetes Self-Management Education and Support Services
Blood sugar that is not well controlled in a woman with gestational diabetes can lead to problems for the pregnant woman and the baby:
An Extra-Large Baby
Diabetes that is not well controlled causes the baby’s blood sugar to be high.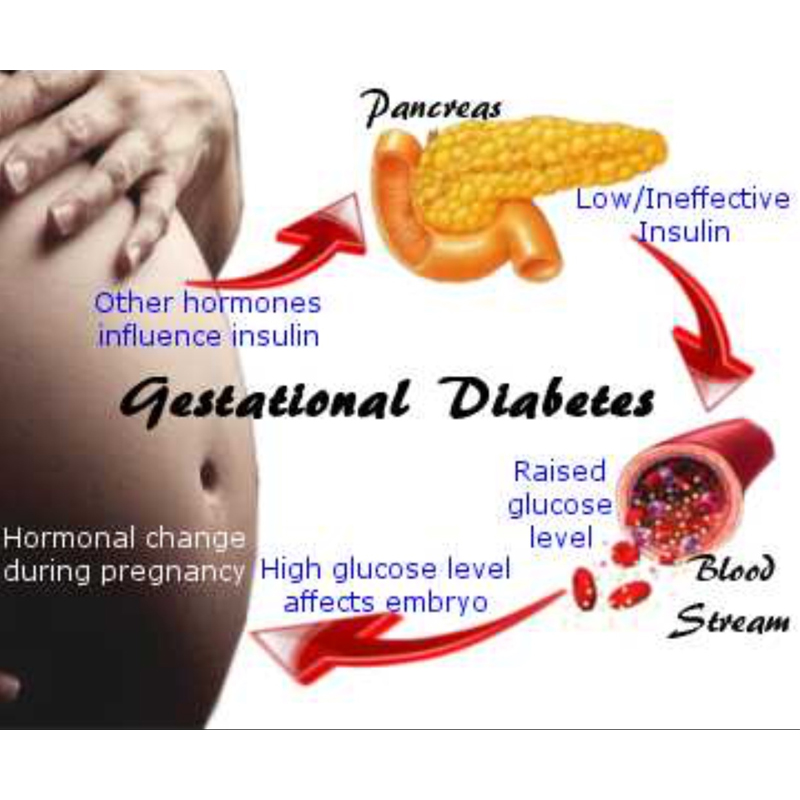 The baby is “overfed” and grows extra-large. Besides causing discomfort to the woman during the last few months of pregnancy, an extra-large baby can lead to problems during delivery for both the mother and the baby. The mother might need a C-Section to deliver the baby. The baby can be born with nerve damage due to pressure on the shoulder during delivery.
The baby is “overfed” and grows extra-large. Besides causing discomfort to the woman during the last few months of pregnancy, an extra-large baby can lead to problems during delivery for both the mother and the baby. The mother might need a C-Section to deliver the baby. The baby can be born with nerve damage due to pressure on the shoulder during delivery.
C-Section (Cesarean Section)
A C-section is an operation to deliver the baby through the mother’s belly. A woman who has diabetes that is not well controlled has a higher chance of needing a C-section to deliver the baby. When the baby is delivered by a C-section, it takes longer for the woman to recover from childbirth.
High Blood Pressure (Preeclampsia)
When a pregnant woman has high blood pressure, protein in her urine, and often swelling in fingers and toes that doesn’t go away, she might have preeclampsia. It is a serious problem that needs to be watched closely and managed by her doctor. High blood pressure can cause harm to both the woman and her unborn baby. It might lead to the baby being born early and also could cause seizures or a stroke (a blood clot or a bleed in the brain that can lead to brain damage) in the woman during labor and delivery. Women with diabetes have high blood pressure more often than women without diabetes.
It might lead to the baby being born early and also could cause seizures or a stroke (a blood clot or a bleed in the brain that can lead to brain damage) in the woman during labor and delivery. Women with diabetes have high blood pressure more often than women without diabetes.
Low Blood Sugar (Hypoglycemia)
People with diabetes who take insulin or other diabetes medications can develop blood sugar that is too low. Low blood sugar can be very serious, and even fatal, if not treated quickly. Seriously low blood sugar can be avoided if women watch their blood sugar closely and treat low blood sugar early.
If a woman’s diabetes was not well controlled during pregnancy, her baby can very quickly develop low blood sugar after birth. The baby’s blood sugar must be watched for several hours after delivery.
5 Tips for Women with Gestational Diabetes
- Eat Healthy Foods
Eat healthy foods from a meal plan made for a person with diabetes. A dietitian can help you create a healthy meal plan. Learn more about diabetes meal planning.
Learn more about diabetes meal planning. - A dietitian can also help you learn how to control your blood sugar while you are pregnant. To find a registered dietician near you, please visit The Academy of Nutrition and Dietetics website.
- Exercise Regularly
Exercise is another way to keep blood sugar under control. It helps to balance food intake. After checking with your doctor, you can exercise regularly during and after pregnancy. Get at least 30 minutes of moderate-intensity physical activity at least five days a week. This could be brisk walking, swimming, or actively playing with children.Learn more about physical activity during pregnancy » - Monitor Blood Sugar Often
Because pregnancy causes the body’s need for energy to change, blood sugar levels can change very quickly. Check your blood sugar often, as directed by your doctor. - Take Insulin, If Needed
Sometimes a woman with gestational diabetes must take insulin. If insulin is ordered by your doctor, take it as directed in order to help keep blood sugar under control.
If insulin is ordered by your doctor, take it as directed in order to help keep blood sugar under control. - Get Tested for Diabetes after Pregnancy
Get tested for diabetes 6 to 12 weeks after your baby is born, and then every 1 to 3 years.For most women with gestational diabetes, the diabetes goes away soon after delivery. When it does not go away, the diabetes is called type 2 diabetes. Even if the diabetes does go away after the baby is born, half of all women who had gestational diabetes develop type 2 diabetes later. It’s important for a woman who has had gestational diabetes to continue to exercise and eat a healthy diet after pregnancy to prevent or delay getting type 2 diabetes. She should also remind her doctor to check her blood sugar every 1 to 3 years.
Women who had gestational diabetes or who develop prediabetes can also learn more about the National Diabetes Prevention Program (National DPP), CDC-recognized lifestyle change programs. To find a CDC-recognized lifestyle change class near you, or join one of the online programs.
To find a CDC-recognized lifestyle change class near you, or join one of the online programs.
More Information
Gestational Diabetes and Pregnancy [PDF – 1 MB]
View, download, and print this brochure about gestational diabetes and pregnancy.
For more information on gestational diabetes, visit the American Diabetes Association’s website.
- Diabetes
- Before Pregnancy
- Healthy Pregnancy
- Birth Defects
- CDC’s National Center on Birth Defects and Developmental Disabilities
Gestational diabetes mellitus | Shchelkovsky perinatal center
Gestational diabetes mellitus is a disease characterized by hyperglycemia (increased blood glucose levels) that was first diagnosed during pregnancy. Most often, a woman's glycemia normalizes after childbirth, but there is a high risk of developing diabetes in subsequent pregnancies and in the future.
Gestational diabetes during pregnancy is a fairly common disease in Russia and the world as a whole. The incidence of hyperglycemia during pregnancy, according to international studies, is up to 18%.
The incidence of hyperglycemia during pregnancy, according to international studies, is up to 18%.
Disturbance of carbohydrate metabolism can develop in any pregnant woman, taking into account those hormonal and metabolic changes that consistently occur at different stages of pregnancy. But most high risk of developing gestational diabetes in pregnant women with:
- Overweight/obese and over 25 years of age
- The presence of diabetes in the immediate family
- Impaired carbohydrate metabolism identified prior to present pregnancy (impaired glucose tolerance, impaired fasting glycemia, gestational diabetes in previous pregnancies
- Birth of a child weighing more than 4000 g
In a healthy pregnant woman, in order to overcome physiological insulin resistance and maintain a normal blood glucose level for pregnancy, a compensatory increase in insulin secretion by the pancreas occurs approximately three times (the mass of beta cells increases by 10-15%).
However, in pregnant women, especially those with a hereditary predisposition to diabetes mellitus, obesity (BMI over 30 kg/m2), etc., the existing secretion of insulin does not always allow overcoming the physiological insulin resistance that develops in the second half of pregnancy. This leads to an increase in blood glucose levels and the development of gestational diabetes. With the blood flow, glucose is immediately and freely transferred through the placenta to the fetus, contributing to its production of its own insulin.
Fetal insulin, having a "growth-like" effect, leads to stimulation of the growth of its internal organs against the background of a slowdown in their functional development, and excess glucose coming from the mother through its insulin is deposited from the 28th week of pregnancy in the subcutaneous depot in the form of fat. As a result, chronic maternal hyperglycemia harms the development of the fetus and leads to the formation of the so-called "diabetic fetopathy".
These are fetal diseases that occur from the 12th week of intrauterine life until birth:
- Large fruit weight; violation of body proportions - large belly, wide shoulder girdle and small limbs
- Anticipation of intrauterine development - with ultrasound, an increase in the main dimensions of the fetus in comparison with gestational age
- Edema of fetal tissues and subcutaneous fat
- Chronic fetal hypoxia (impaired blood flow in the placenta as a result of prolonged uncompensated hyperglycemia in a pregnant woman)
- Delayed formation of lung tissue
- Birth injuries
- High risk of perinatal mortality
At birth, children with diabetic fetopathy are more common:
- Macrosomia (newborn weight ≥4000 g, or ≥90 percentile in preterm pregnancy)
- Violation of adaptation to extrauterine life, which is manifested by the immaturity of the newborn, even with a full-term pregnancy and its large size
- Respiratory disorders
- Asphyxia
- Neonatal hypoglycemia
- Organomegaly (enlarged spleen, liver, heart, pancreas)
- Cardiomyopathy (primary lesion of the heart muscle)
- Jaundice
- Disorders in the blood coagulation system, increased content of erythrocytes (red blood cells) in the blood
- Metabolic disorders (low blood glucose, calcium, potassium, magnesium levels)
Children born to mothers with undiagnosed, uncompensated gestational diabetes mellitus are more likely to:
- Neurological diseases (cerebral palsy, epilepsy) due to birth trauma
- During puberty and thereafter, the risk of developing obesity, metabolic disorders (in particular, carbohydrate metabolism), and cardiovascular diseases is increased
On the part of a pregnant woman with gestational diabetes mellitus, the following are more common:
- Polyhydramnios
- Infections of the urinary system
- Toxicosis of the second half of pregnancy (a pathological condition that develops in the second half of pregnancy and is manifested by the appearance of edema, increased blood pressure)
- Pre-eclampsia, eclampsia
- Prematurity
- Anomalies of labor activity
- Birth injuries
- Delivery by caesarean section
Gestational diabetes mellitus does not have any clinical manifestations associated with hyperglycemia (dry mouth, thirst, increased urine output per day, itching, etc. ), and therefore active detection of this disease in all pregnant women is required.
), and therefore active detection of this disease in all pregnant women is required.
Analysis and testing for diabetes in pregnant women
It is mandatory for all pregnant women to test fasting venous blood plasma glucose, in the laboratory - against the background of a normal diet and physical activity - at the first visit to the antenatal clinic or perinatal center, no later than 24 weeks of pregnancy.
If the results of the study correspond to normal indicators during pregnancy, then an oral glucose tolerance test - OGTT ("load test" with 75 g of glucose) is mandatory at 24-28 weeks of gestation in order to actively identify possible disorders in carbohydrate metabolism.
OGTT with 75 g of glucose is a safe and the only diagnostic test for detecting carbohydrate metabolism disorders during pregnancy.
Rules for conducting OGTT:
- OGTT is performed with a normal diet (at least 150 g of carbohydrates per day) and physical activity for at least 3 days prior to the study
- The test is performed in the morning on an empty stomach after 8-14 hours of overnight fasting
- The last meal must necessarily contain at least 30-50 g of carbohydrates
- Drinking plain water is not prohibited
- During the test, the patient must be seated
- Drugs that affect blood glucose levels (multivitamins and iron preparations containing carbohydrates, glucocorticoids, β-blockers), if possible, should be taken after the end of the test
- Determination of venous plasma glucose is performed only in the laboratory on biochemical analyzers or on glucose analyzers.
 The use of portable self-monitoring devices (glucometers) for testing is prohibited
The use of portable self-monitoring devices (glucometers) for testing is prohibited
Stages of implementation of PGTT
After taking the first sample of venous blood plasma on an empty stomach, the patient drinks a glucose solution for 5 minutes, consisting of 75 g of dry glucose dissolved in 250-300 ml of non-carbonated drinking water, or 82.5 mg of glucose monohydrate. The start of taking a glucose solution is considered the beginning of the test. The next blood samples to determine the level of venous plasma glucose are taken 1 and 2 hours after the glucose load.
Norms of venous plasma glucose for pregnant women:
- Fasting
- 1 hour after glucose load
- 2 hours after glucose load
Diagnosis of gestational diabetes mellitus is established by detecting glycemia above or equal to the above indicators. To establish a diagnosis, it is enough to obtain an abnormal result in one of the three points.
After the diagnosis of gestational diabetes mellitus is established, all women need constant monitoring by an obstetrician-gynecologist, a general practitioner together with an endocrinologist
Management of pregnancy in case of diagnosed gestational diabetes mellitus:
In women with gestational diabetes mellitus, taking into account the characteristics of the course of the pathological condition , nutrition should be adjusted.
Diet for diabetes in pregnancy
Easily digestible carbohydrates are completely excluded from the diet (they are quickly absorbed from the intestines and increase blood glucose levels within 10-30 minutes after ingestion):
- Sugar, fructose, jam, honey, caramel, lozenges, chocolate
- Fruit juices (including juices dispensed at antenatal clinics)
- Lemonades
- Ice cream, cakes, cakes, condensed milk
- High-grade flour baked goods
- Sweet pastries (buns, buns, pies)
Foods with a high glycemic index are completely excluded from the diet .
Glycemic index (GI) is a measure of the effect of food on blood sugar levels. Each food is assigned a score from 0 to 100 based on how quickly it raises blood glucose levels. Glucose has a GI of 100, which means it enters the bloodstream immediately, a benchmark against which other foods are compared.
Another indicator that helps predict how high blood sugar will rise after eating and how long it will stay at this level - glycemic load (GL)
Calculated using the formula:
GL = [GI (%) x amount of carbohydrates per serving (g)] / 100
Glycemic load indicates that eating a food with a low glycemic index , but a large amount of carbohydrates will not be effective in maintaining normal blood sugar after a meal.
For example, let's compare the glycemic load of different foods:
Watermelon:
GI - 75, carbohydrates - 6.8 g per 100 g of product, GL \u003d (75x6. 8) / 100 \u003d 6.6 g. g per 100 g of the product, GN = (76x38.8) / 100 = 29.5 g. 6)/100 = 15.3 g. products increases with an increase in the amount of carbohydrates consumed and the glycemic index. Accordingly, it is possible to control the glycemic load by eating low GI foods in small portions several times a day.
8) / 100 \u003d 6.6 g. g per 100 g of the product, GN = (76x38.8) / 100 = 29.5 g. 6)/100 = 15.3 g. products increases with an increase in the amount of carbohydrates consumed and the glycemic index. Accordingly, it is possible to control the glycemic load by eating low GI foods in small portions several times a day.
Glycemic load scale:
During one meal
- Low to 10 g
- Medium 11 to 19 g
- High - more than 20
During the day
- Low to 80 g
- Medium 100 to 120 g
- High - more than 120
It is necessary to give preference to foods with a medium and low glycemic load, eating food in small portions, several times a day, excluding the intake of easily digestible carbohydrates.
Avoid high GI foods:
- Sweet fruits and berries: grapes, bananas, persimmons, figs, cherries, melons, dates
- Vegetables: Potatoes, parsnips, pumpkin, boiled beets, boiled carrots, canned sweet corn and peas
- Cereals - millet, wheat groats, semolina, millet, polished rice varieties, and all instant porridges
- Homemade noodles, rice noodles
- Milk
- White or brown breads made from premium quality flour
Also, do not eat foods containing a large amount of hidden fat, so as not to put on too much weight:
- Meat delicacies
- Sausages
- Sausages
- Sausages
- Carbonates
- Ham
- Salo
- Baked ham
- Offal
Preference is given to products with medium and low GI:
- Vegetables: Any cabbage (white cabbage, broccoli, cauliflower, Brussels sprouts, leafy, kohlrabi), salads, greens (onion, dill, parsley, cilantro, sorrel, mint, basil, asparagus, spinach, wild garlic, tarragon), eggplant, zucchini, pepper, radish, radish, cucumber, tomato, asparagus, onion, garlic, squash, turnip, paprika, capsicum, raw carrot
- Legumes: peas, beans, lentils, beans
- Mushrooms
- Fruits: Grapefruit, lemon, lime, kiwi, orange, apples, pears, tangerines
- Berries: chokeberry, lingonberry, blueberry, blueberry, blackberry, feijoa, currant, wild strawberry, strawberry, raspberry, gooseberry, cranberry, cherry
- Fermented milk products - kefir, fermented baked milk, curdled milk, ayran, tan (no more than 1 glass at a time), yogurt, cottage cheese, cheese
- Meat, chicken, fish.
 During cooking, visible fat is removed and it is melted as much as possible. Best Food Processing—Boiling, Steaming, Roasting, Open Fire
During cooking, visible fat is removed and it is melted as much as possible. Best Food Processing—Boiling, Steaming, Roasting, Open Fire
How to lower your glycemic index and glycemic load:
- Pair medium GI starchy foods with low GI vegetables
- Pasta made from durum wheat flour without vegetables is worse than the same pasta with vegetables
- Do not cook durum wheat pasta until sticky
- Eat cereals made from whole grains (preference is given to barley, buckwheat, oatmeal, wheat, spelt, bulgur) and wholemeal bread with bran
- Kashi (buckwheat, oatmeal) is better to just brew with boiling water and keep warm for several hours. Then the starch under the influence of water and high temperature will not go into a state easily and quickly absorbed by the body
- The more crushed the product, the higher its glycemic index. Nothing Not to Puree
- Eat whole fruits (unlike juices, they contain fiber, which lowers the GI)
- Prefer raw vegetables.
 Vegetables subjected to heat treatment should not be boiled. Fiber is not destroyed during such processing
Vegetables subjected to heat treatment should not be boiled. Fiber is not destroyed during such processing - Try, whenever possible, to consume vegetables and fruits together with the skin, which consists of whole fiber
- Combine protein foods with vegetables, eat starches at the same time as proteins
- Dress salads with a little olive oil (1 tablespoon) with lemon juice
- Fat also lowers the glycemic index
- If you really want something sweet, eat it along with proteins and foods rich in fiber and fat
- High-fiber carbohydrate foods should not exceed 45% of the daily calorie intake and should be evenly distributed throughout the day (3 main meals and 2-3 snacks) with a minimum carbohydrate content for breakfast as . the contra-insular effect of increased levels of maternal hormones and the feto-placental complex in the morning enhances tissue insulin resistance
- Breakfast should be "protein" (cottage cheese, egg, meat, fish, chicken with vegetables).
 This improves blood sugar levels in the morning after breakfast, before and after lunch
This improves blood sugar levels in the morning after breakfast, before and after lunch
Gestational diabetes in pregnancy - treatment and diagnosis of gestational diabetes in Moscow, Clinical Hospital on Yauza
Get a consultation from a gynecologist
Service in two languages: Russian, English.
Leave your phone number and we will call you back.
Contents
IMPORTANT!
The information in this section should not be used for self-diagnosis or self-treatment. In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests. For diagnosis and proper treatment, you should contact your doctor.
Specialists of the Yauza Clinical Hospital diagnose and treat gestational diabetes and its complications. For a comfortable pregnancy and the safety of the expectant mother and baby, we exercise strict control over the blood sugar level of a pregnant woman, if necessary, prescribe a specially designed diet and medications.

Make an appointment with a gynecologist
- About 7% of pregnant women have manifestations of gestational diabetes. In 50% of cases, the disease is asymptomatic
- Gestational diabetes in pregnancy significantly increases the risk of pregnancy complications for both mother and fetus
- Perinatal mortality increases by 2-3% with a combination of diabetes mellitus and pregnancy
Pregnancy diabetes (gestational diabetes) is an increase in blood glucose that first occurs during pregnancy but is not high enough to warrant a diagnosis of diabetes mellitus. These are hidden disorders of carbohydrate metabolism that threaten to develop into diabetes mellitus.
Pregnant blood glucose norm
During pregnancy, all women experience changes in insulin sensitivity and glucose tolerance. This is fine. The difference between the norm and pathology in the degree of change.
Blood tests for diabetes during pregnancy - norm and pathology
- If the examination of venous blood taken on an empty stomach shows a glucose level of more than 5.
 1 mmol / l, this is the norm for pregnant women.
1 mmol / l, this is the norm for pregnant women.
- From 5.1 to 7.0 mmol / l - gestational diabetes.
- If 7.0 mmol / l or more - diabetes mellitus.
- Testing capillary blood (taken from a finger) for the diagnosis of gestational diabetes mellitus is not recommended.
- If during an oral glucose tolerance test (when 75 g of glucose is taken orally during the study) after an hour the glucose level is more than 10.0 mmol/l, and after two hours the blood glucose level is in the range of 7.8-8.5 mmol/l - then for pregnant women this is a normal indicator.
To better understand what gestational diabetes, or diabetes in pregnancy, is, you need to talk a little about hormonal changes in the body in pregnant women.
Causes of gestational diabetes
Hormonal changes that occur during pregnancy are associated with increased production of large amounts of steroid hormones. Some of them, such as cortisol and progesterone, have a significant effect on cell receptors, increasing their resistance to insulin.
This leads to an increase in blood glucose levels and requires a significant increase in insulin production by the pancreas. In cases where the compensatory capacity of the pancreas is not enough, sugar metabolism gets out of control and a condition called gestational diabetes or gestational diabetes develops.
This condition occurs quite often. Between 3 and 10% of pregnant women develop pathological insulin resistance leading to gestational diabetes.
Unlike diabetes mellitus diagnosed before pregnancy, pathological insulin resistance that occurs during pregnancy does not cause fetal malformations and in most cases does not require insulin treatment. But, nevertheless, uncompensated gestational diabetes can significantly complicate the course of pregnancy.
Specialists of the Yauza Clinical Hospital diagnose, treat and prevent diabetes in pregnant women and its complications, such as impaired fetal growth. The doctors of the Clinical Hospital on the Yauza strictly control the blood sugar level of a pregnant woman, if necessary, prescribe a specially designed diet. This ensures a comfortable pregnancy and the safety of the expectant mother and baby.
This ensures a comfortable pregnancy and the safety of the expectant mother and baby.
Pregnancy diabetes - consequences for the child
Large disproportionate fruit. The most important and frequent complication of gestational diabetes is fetal growth failure. Developing in conditions of increased blood glucose levels, which penetrate the fetoplacental barrier, the fetus is forced to compensate for the increased sugar level with its own insulin. Due to the fact that the structure of insulin and growth hormone are very similar, high levels of insulin stimulate the growth of the fetus. The problem is that a large fetus develops. In such a fetus, body proportions differ from those of normally developing newborns, in which the volume of the head is larger than the volume of the shoulder girdle. In fetuses with uncompensated gestational diabetes, the size of the shoulder girdle predominates, and the size of the abdomen increases. This leads to the fact that during childbirth after the fetus's head passes through the birth canal, the shoulders can get stuck (shoulder dystocia) and the child, along with the mother, can be severely injured or die.
Polyhydramnios or oligohydramnios. In addition, with gestational diabetes, the balance of the amount of amniotic fluid may be disturbed and either polyhydramnios or oligohydramnios develops. This is a serious risk factor for intrauterine fetal death or premature birth.
Underdevelopment of the lungs. In gestational diabetes, the lungs of the fetus mature later, as the production of surfactant (a special lubrication of the inner walls of the alveoli, where oxygen is exchanged in the lungs) is disrupted. Therefore, premature birth in gestational diabetes is especially dangerous.
Hypoglycemia and metabolic disorders in the fetus. Due to the constant increased production of its own insulin during pregnancy, immediately after birth, the child is in a state of hypoglycemia with electrolyte imbalance, which threatens his life.
All this dictates the need for the earliest possible detection of gestational diabetes in pregnant women, the level of sugar in the blood of a pregnant woman and to prevent the development of complications.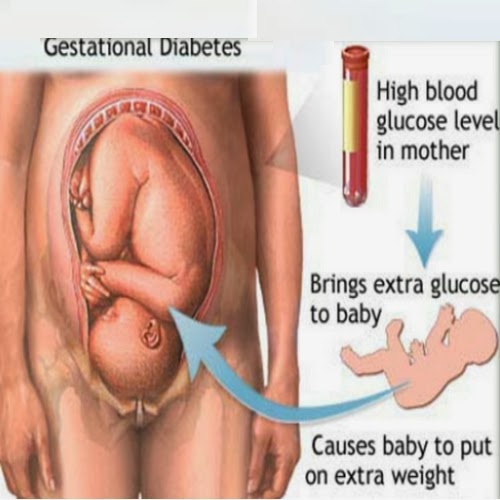
.
Diagnosis of diabetes in pregnant women at the Yauza Clinical Hospital
Signs of diabetes in pregnant women
Gestational diabetes in pregnancy is not usually associated with the classic symptoms of diabetes, such as thirst or excessive urination (polyuria).
Pregnancy tests for diabetes mellitus
First phase. At the first visit of a pregnant woman to a doctor at any time, she is tested for glucose levels in venous blood - fasting glucose, regardless of food intake, glycated hemoglobin. This is the first phase of research to detect diabetes mellitus or gestational diabetes in pregnant women. If diabetes mellitus is detected, the patient is referred for observation and treatment to an endocrinologist.
Second phase. For a period of 24-28 weeks, all patients who did not show identified disorders of carbohydrate metabolism at the first study are called for a glucose tolerance test (OGTT) to detect "hidden diabetes". This is done because the occurrence of gestational diabetes is associated with the development of insulin resistance under the influence of hormones produced by the placenta. Therefore, in the vast majority of cases, gestational diabetes develops in the second half of pregnancy after 24 weeks, when there is a peak in the production of placental hormones.
This is done because the occurrence of gestational diabetes is associated with the development of insulin resistance under the influence of hormones produced by the placenta. Therefore, in the vast majority of cases, gestational diabetes develops in the second half of pregnancy after 24 weeks, when there is a peak in the production of placental hormones.
Glucose tolerance test
It is carried out to detect pathological insulin resistance, characteristic of latent diabetes in pregnant women. Pregnant women undergo a two-hour test, only in the laboratory.
During the 3 days leading up to the test, the woman should eat her usual diet, including carbohydrates (>150 g of carbohydrates per day), maintain her usual physical activity. The evening before testing, dinner should include 30-50 grams of carbohydrates.
On the day of the study, before the analysis, you should not smoke and take medications that can affect the level of glucose (vitamins, glucocorticoid hormones, iron preparations, which include carbohydrates, beta-agonists, beta-blockers). You can drink water.
You can drink water.
Venous blood is taken on an empty stomach (after 8-14 hours of fasting, usually in the morning, before breakfast).
Then the patient takes a glucose solution (75 g).
And they take blood in an hour and two after the sugar load. Normally, the level of glucose in the blood after a sugar load should not exceed an hour later - 10 mmol / l, after 2 hours - 8.5 mmol / l.
If manifest diabetes mellitus is detected, the patient is referred to an endocrinologist, gestational diabetes mellitus is treated by an obstetrician-gynecologist or therapist.
Glucose tolerance test contraindications
- Strict bed rest prescribed for a pregnant woman (until doctor's permission).
- Severe toxicosis of pregnant women (with nausea and vomiting).
- Acute infectious or inflammatory disease.
- Exacerbation of chronic pancreatitis.
- Dumping syndrome (syndrome of resected stomach).
Prenatal diabetes monitoring
Blood glucose monitoring, self-monitoring diary
When diagnosing gestational diabetes, it is necessary to establish strict control of sugar levels throughout the subsequent pregnancy and during childbirth.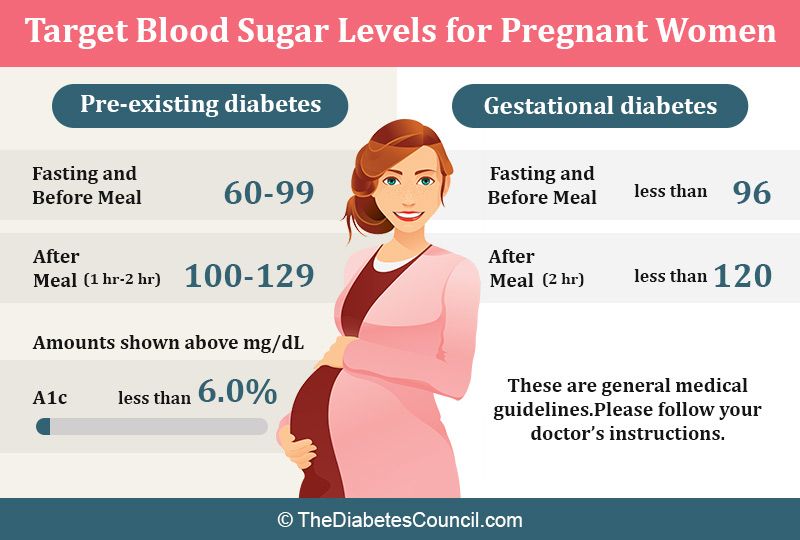 To do this, regularly examine the blood for sugar (glucose). In addition, the patient conducts self-monitoring using a glucometer.
To do this, regularly examine the blood for sugar (glucose). In addition, the patient conducts self-monitoring using a glucometer.
It is recommended that a pregnant woman keep a diary of observations in which to record:
- blood glucose level (normal <5.1 mmol/l),
- the presence of ketone bodies in the urine, which is determined by test strips sold in a pharmacy (normally, ketone bodies are absent),
- blood pressure readings (normal <130|80 mmHg),
- fetal movements,
- body weight,
- diet.
Expert ultrasound
Conducting an expert ultrasound examination reveals signs of intrauterine suffering of the fetus (diabetic fetopathy), polyhydramnios. Most often, this is a sign of chronically elevated blood glucose levels, penetrating into the blood of the fetus. This requires urgent correction of the diet and normalization of the level of glycemia (blood sugar). If necessary, insulin therapy.
Make an appointment
Treatment of gestational diabetes
Diet for gestational diabetes
In most cases, it is sufficient to follow a special diet recommended by a nutritionist based on the body mass index of the pregnant woman and her taste preferences. The effectiveness of diet therapy is determined by the maintenance of normal blood glucose levels. Diet in pregnancy diabetes recommends:
The effectiveness of diet therapy is determined by the maintenance of normal blood glucose levels. Diet in pregnancy diabetes recommends:
- Eliminate simple carbohydrates - sweets, pastries, white bread, honey, sugar, jam, sugary drinks and fruits, ice cream.
- Limit complex carbohydrates - cereals (semolina, rice - exclude), potatoes, corn, legumes, durum wheat pasta. Distribute their intake evenly over several meals throughout the day to eliminate starvation (causes the formation of ketone bodies).
- Eat enough protein - meat, fish, seafood, poultry, mushrooms, eggs, hard cheese, dairy and sour-milk products of medium fat content (3-5%).
- It is necessary to enrich the diet with fiber and vitamins - greens, vegetables (except for boiled carrots and beets), sweet and sour berries (excluding grapes).
- Correctly choose fats, do not exceed their amount recommended by the doctor - vegetable oils (add to ready-made meals), nuts, seeds.
 Animal fats (butter, sausages) - limit.
Animal fats (butter, sausages) - limit. - When cooking, boil, stew, steam and bake dishes. Don't fry. Do not deep fry.
A detailed menu for a pregnant woman with gestational diabetes will be compiled by a doctor, taking into account the individual characteristics of each particular woman.
It is not worth using table No. 9 in its pure form for pregnant women with diabetes mellitus due to a significant restriction of its calorie content.
In detail, what you can eat with diabetes in pregnant women will be told by the doctor at an in-person consultation.
Pharmacotherapy
In cases where the diet fails to achieve the desired control of the level of glycemia in the blood, there are signs of a negative effect on the fetus - they resort to prescribing drugs - insulin. In case of diabetes in pregnant women, antidiabetic drugs in tablets should not be used. Insulin therapy is prescribed by an endocrinologist. Pregnant women with diabetes who are on insulin therapy are jointly managed by an endocrinologist, an internist and an obstetrician-gynecologist.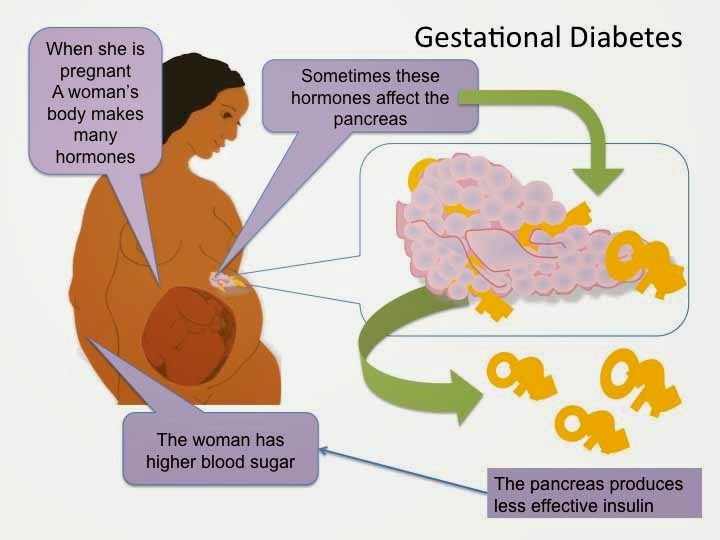
Physical activity
Patients are recommended regular physical activity - walking in the fresh air (at least 150 minutes per week), swimming.
Prenatal diabetes - childbirth
With a compensated course of gestational diabetes, normal development of the fetus and the condition of the woman, childbirth is carried out in time in a natural way. The question of early delivery, caesarean section may arise if there are relevant indications from the mother or fetus.
Specialists of the Yauza Clinical Hospital have included mandatory fetal development screenings and tests to diagnose sugar metabolism disorders in the pregnancy monitoring program. Recommendations are given on a special diet for women with manifestations of gestational diabetes. If necessary, strict glycemic control is carried out throughout pregnancy, ensuring its successful completion and the birth of a healthy child.
Make an appointment
Cost of services
Prices for services you can see in the price list or check by phone listed on the site.