Pregnancy without fetus
Blighted Ovum: Causes, Symptoms, and More
Written by Annie Stuart
Reviewed by Traci C. Johnson, MD on April 19, 2021
In this Article
- What Causes a Blighted Ovum?
- Signs of a Blighted Ovum
- Diagnosing a Blighted Ovum
- What Happens After a Miscarriage?
A blighted ovum occurs when a fertilized egg implants in the uterus but doesn't develop into an embryo. It is also referred to as an anembryonic (no embryo) pregnancy and is a leading cause of early pregnancy failure or miscarriage. Often it occurs so early that you don't even know you are pregnant.
A blighted ovum causes about one out of two miscarriages in the first trimester of pregnancy. A miscarriage is when a pregnancy ends on its own within the first 20 weeks.
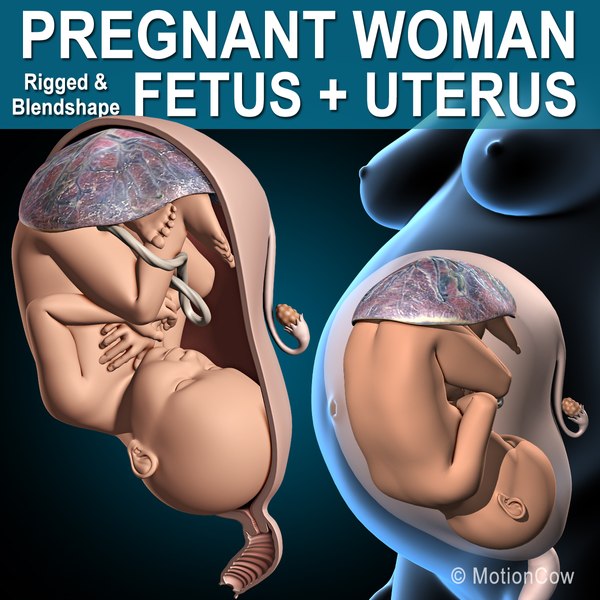
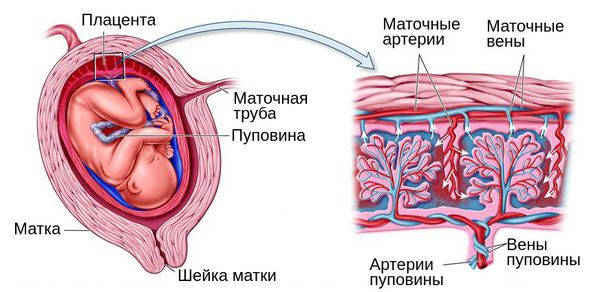
When a woman becomes pregnant, the fertilized egg attaches to the uterine wall. At about five to six weeks of pregnancy, an embryo should be present. At about this time, the gestational sac -- where the fetus develops -- is about 18 millimeters wide. With a blighted ovum, though, the pregnancy sac forms and grows, but the embryo does not develop. That's why a blighted ovum is also called an anembryonic pregnancy.
What Causes a Blighted Ovum?
Miscarriages from a blighted ovum are often due to problems with chromosomes, the structures that carry genes. This may be from a poor-quality sperm or egg. Or, it may occur due to abnormal cell division. Regardless, your body stops the pregnancy because it recognizes this abnormality.
It's important to understand that you have done nothing to cause this miscarriage and you almost certainly could not have prevented it. For most women, a blighted ovum occurs only once.
Signs of a Blighted Ovum
With a blighted ovum, you may have experienced signs of pregnancy. For example, you may have had a positive pregnancy test or a missed period.
Then you may have signs of a miscarriage, such as:
- Abdominal cramps
- Vaginal spotting or bleeding
- A period that is heavier than usual.
If you're experiencing any of these signs or symptoms, you may be having a miscarriage. But not all bleeding in the first trimester ends in miscarriage. So be sure to see your doctor right away if you have any of these signs.
Diagnosing a Blighted Ovum
If you thought you had a normal pregnancy, you're not alone; many women with a blighted ovum think so because their levels of human chorionic gonadotropin (hCG) may increase. The placenta produces this hormone after implantation. With a blighted ovum, hCG can continue to rise because the placenta may grow for a brief time, even when an embryo is not present.
For this reason, an ultrasound test is usually needed to diagnose a blighted ovum -- to confirm that the pregnancy sac is empty.
What Happens After a Miscarriage?
If you have received a diagnosis of a blighted ovum, discuss with your doctor what to do next. Some women have a dilation and curretage (D and C). This surgical procedure involves dilating the cervix and removing the contents of the uterus. Because a D and C immediately removes any remaining tissue, it may help you with mental and physical closure. It may also be helpful if you want a pathologist to examine tissues to confirm the reason for the miscarriage.
Because a D and C immediately removes any remaining tissue, it may help you with mental and physical closure. It may also be helpful if you want a pathologist to examine tissues to confirm the reason for the miscarriage.
Using a medication such as misoprostol on an outpatient basis may be another option. However, it may take several days for your body to expel all tissue. With this medication, you may have more bleeding and side effects. With both options, you may have pain or cramping that can be treated.
Other women prefer to forego medical management or surgery. They choose to let their body pass the tissue by itself. This is mainly a personal decision, but discuss it with your doctor.
After a miscarriage, your doctor may recommend that you wait at least one to three menstrual cycles before trying to conceive again.
Blighted ovum | Pregnancy Birth and Baby
Blighted ovum | Pregnancy Birth and Baby beginning of content4-minute read
Listen
Key facts
- A blighted ovum is a type of miscarriage that can happen early in a pregnancy.

- A blighted ovum is when a sac and placenta grow, but a baby does not.
- A miscarriage can be extremely upsetting, and you may need support and time to grieve.
- Having a blighted ovum in one pregnancy does not change your chance of having a successful pregnancy in the future.
What is a blighted ovum?
A blighted ovum is a type of miscarriage that can happen early in a pregnancy. It is also called an 'anembryonic pregnancy' as there is no embryo (developing baby). In this type of miscarriage, a sac and placenta grow, but there is no baby. Because a blighted ovum still makes pregnancy hormones, it may still show up as a positive pregnancy test.
A blighted ovum will eventually cause a miscarriage, usually at 7 to 12 weeks of pregnancy. Your body realises that the pregnancy is not developing properly and starts to shed blood and tissue from the uterus. You may notice pain in your lower abdomen, or bleeding from your vagina.
How common is miscarriage?
Miscarriage is very common, and up to 1 in 5 people who know that they are pregnant will miscarry before 20 weeks of gestation. The actual rate of miscarriage is even higher, as a very early miscarriage may happen before you even realise that you’re pregnant.
What causes a blighted ovum?
When the egg is fertilised, cells that make the pregnancy sac and placenta start multiplying. But occasionally, the cells that are supposed to develop into a baby don’t multiply.
The cause isn’t known. It isn’t caused by anything you have done.
How and when is blighted ovum diagnosed?
Sometimes, it is picked up during a routine ultrasound. This can be particularly difficult if you’ve gone for an ultrasound expecting good news.
At other times, there may have been bleeding at the start of the pregnancy and an ultrasound is used to investigate the cause.
How is blighted ovum treated?
Your doctor will discuss the options with you. You might choose to allow a natural miscarriage to happen. Once this starts, it can take days or weeks for the bleeding to finish. If the bleeding is getting heavier, if you are in pain or you feel unwell, see your doctor.
You might choose to allow a natural miscarriage to happen. Once this starts, it can take days or weeks for the bleeding to finish. If the bleeding is getting heavier, if you are in pain or you feel unwell, see your doctor.
You could also have a termination by taking medicines or by having a type of surgery known as D & C.
Does it affect my chances of having a baby?
No. Having a blighted ovum in one pregnancy does not alter your chance of having a successful pregnancy in the future.
If you have had one miscarriage, your next pregnancy is likely to be normal. If you have had 3 miscarriages in a row, you should see your doctor to rule out any problems.
Where can I go for support and information?
Speak with your doctor if you are concerned that you may have a blighted ovum.
A miscarriage can be extremely upsetting. If you’ve experienced a miscarriage you may need support and time to grieve. There is no right way to feel after a miscarriage. Different people react to a miscarriage with different emotions, including anger, guilt or relief.
Different people react to a miscarriage with different emotions, including anger, guilt or relief.
Pregnancy, Birth and Baby helpline can offer emotional support and trusted advice to anyone who is dealing with pregnancy loss. Call Pregnancy, Birth and Baby on 1800 882 436 anytime of the day or night.
Sources:
Raising Children (Miscarriage : what it is and how to cope), Pink Elephants Network (What is miscarriage?), Red Nose (Reasons for miscarriage)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: June 2022
Back To Top
Related pages
- Fathers and miscarriage
- Emotional support after miscarriage
- Miscarriage
- Pregnancy loss
Need more information?
Reasons for Miscarriage | Red Nose Australia
Read more on Red Nose website
Experiencing a pregnancy loss
Losing a baby at any stage of pregnancy can be devastating. Remember, pregnancy loss is more common than you probably think – and it’s not your fault. This article aims to help you deal with the many emotions you will be feeling.
Remember, pregnancy loss is more common than you probably think – and it’s not your fault. This article aims to help you deal with the many emotions you will be feeling.
Read more on Pregnancy, Birth & Baby website
Miscarriage
A miscarriage is the loss of a baby, usually during the first three months or first trimester of pregnancy.
Read more on Pregnancy, Birth & Baby website
Pregnancy: miscarriage & stillbirth | Raising Children Network
Have you experienced a miscarriage or stillbirth? Find articles and videos about coping with the grief of losing a pregnancy or having a stillbirth.
Read more on raisingchildren.net.au website
Miscarriage: a guide for men | Raising Children Network
This Dads Guide to Pregnancy covers miscarriage, the grief men might experience after miscarriage, and how to support partners after pregnancy loss.
Read more on raisingchildren.net.au website
The Pink Elephants Support Network - Supporting Your Physical Wellbeing After Miscarriage
Physical Wellbeing can be an important factor when trying to conceive
Read more on Pink Elephants Support Network website
The Pink Elephants Support Network - Supporting Your Emotional Wellbeing After Miscarriage
It can be challenging to maintain a positive outlook after early pregnancy loss
Read more on Pink Elephants Support Network website
The Pink Elephants Support Network - Holistic Options for Miscarriage Management
Some women may find holistic options can help them feel nurtured and empowered on their journey to future pregnancy
Read more on Pink Elephants Support Network website
The Pink Elephants Support Network - Causes of Miscarriage - Pink Elephants
There are a number of possible reasons that a miscarriage may occur, and often it’s not until extensive testing is done that you may find out why
Read more on Pink Elephants Support Network website
The Pink Elephants Support Network - Pregnancy After Loss - Pink Elephants
Pregnancy after loss is a time that can be fraught with many conflicting emotions
Read more on Pink Elephants Support Network website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
Need further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari.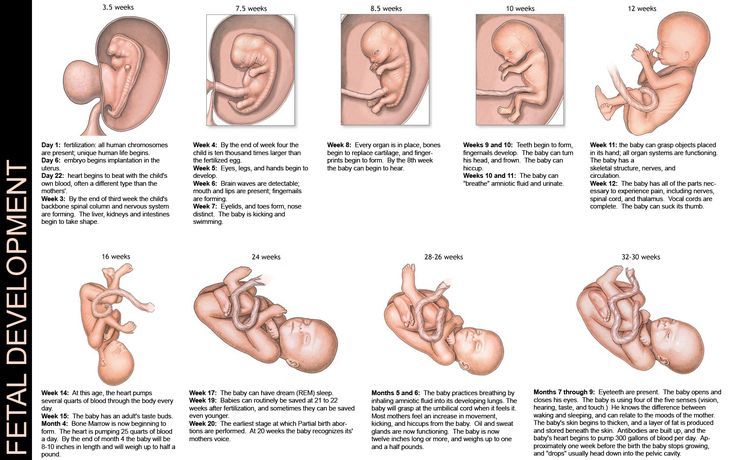 For more information, please visit the links below:
For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Anembryony - pregnancy or not?
Unfortunately, not all pregnancies end in childbearing. Reproductive losses in this case can be due to various reasons. And one of them is a non-developing or missed pregnancy. The proportion of this pathology accounts for up to 15-20% of reproductive losses. Currently, there are 2 variants of missed pregnancy: death of the embryo and anembryony. It is important to understand that the differential diagnosis between them does not affect the subsequent treatment tactics, but is taken into account when assessing the prognosis. Anembryony is more often determined, and this condition in many cases is not accompanied by spontaneous abortion and therefore requires artificial termination of a missed pregnancy. nine0005
nine0005
Anembryony – what is it?
Anembryony - is the absence of an embryo in a developing fetal egg. This condition is also called the empty gestational sac syndrome. This is by no means a rare pathology that can be diagnosed in primigravida and in women who already have healthy children.
Many possible causes of anembryony have now been identified. These include:
- Genetic anomalies , which are observed in almost 80% of the pathological condition. They are usually associated with gross and/or multiple chromosomal abnormalities. Moreover, with anembryony, such anomalies are of a qualitative nature, and with the death of the embryo and its abortion, they are predominantly quantitative. Unviable combinations of parental genes or mutations in key areas responsible for the early stages of embryogenesis and the synthesis of the main structural proteins of cell membranes are also possible. nine0020
- Some acute viral and bacterial diseases occurring in early pregnancy and leading to damage to embryonic tissues or trophoblast.
 The most dangerous in this regard are TORCH infections, although other pathogens can also be embryotropic.
The most dangerous in this regard are TORCH infections, although other pathogens can also be embryotropic. - Persistent viral-bacterial infections of the organs of the reproductive system, leading to the development of chronic endometritis . And in most cases, such a pathology occurs without obvious clinical symptoms and is detected after a frozen pregnancy. nine0020
- Radiation exposure of to a developing embryo.
- Exogenous intoxications : taking drugs with embryotoxic action, drug addiction, exposure to certain industrial and agricultural poisons (toxins).
- Endocrine disorders in a pregnant woman. And the most critical is the deficiency of progesterone and disorders of its metabolism, which is the main cause of the pathology of endometrial decidualization and abnormal implantation of the fetal egg. nine0020
In general, the causes of pathology in most cases remain undiagnosed. Usually it is possible to determine only a presumptive etiology.
Usually it is possible to determine only a presumptive etiology.
Genetic diagnosis of aborted tissues can reveal obvious anomalies of hereditary material. But such a study, unfortunately, is carried out in a very small percentage of cases. Basically, it is indicated with a burdened obstetric history in a woman, when she already had frozen or spontaneously interrupted in the early stages of gestation in the past. But even such a diagnosis is not always informative enough, which is associated with the limited possibilities of modern genetics and the high probability of the impact of other etiological factors. nine0005
Pathogenesis
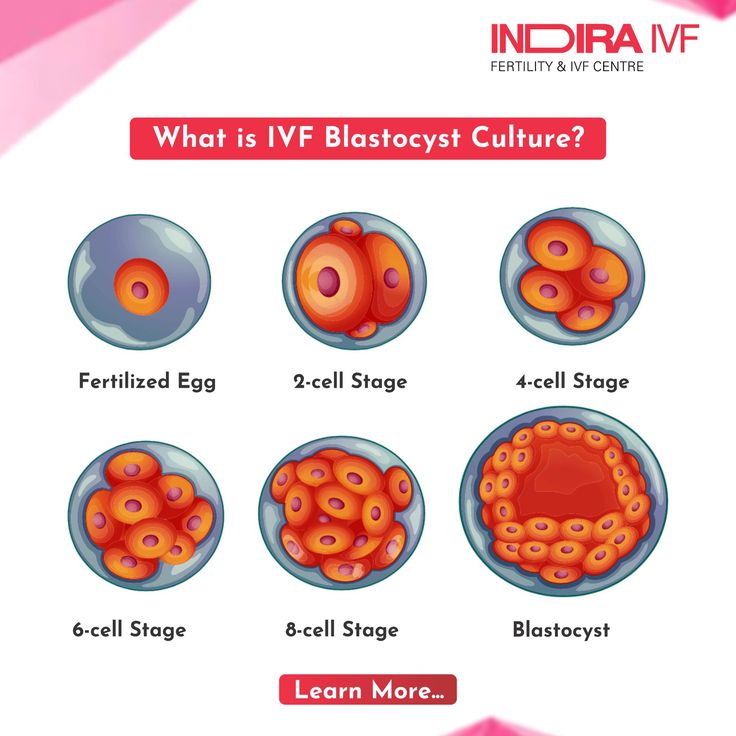
Anembryony is a consequence of the cessation of reproduction and differentiation of the embryoblast or inner cell mass - a group of cells that normally give rise to fetal tissues. And this happens at the earliest stages of pregnancy (usually at 2-4 weeks of gestation), and without disturbing the development of the fetal membranes from the trophoblast. As a result, a so-called empty fetal egg is formed, which continues to grow even in the absence of an embryo in it.
As a result, a so-called empty fetal egg is formed, which continues to grow even in the absence of an embryo in it.
Pathogenetically important factors in the development of the disease include:
- Inherited or acquired chromosome aberrations and other genetic abnormalities. They can lead to a gross desynchronization of the development of embryonic tissues, critical changes in the structure of collagen and other proteins, disruption of the induction of differentiation and migration of dividing cells. The most common autosomal trisomy, monosomy, triploidy, tetraploidy.
- Excessive formation of circulating immune complexes in a woman's body . Their deposition in the walls of small vessels leads to thromboembolism and other critical microcirculation disorders in the area of the implanting egg. Antiphospholipid antibodies are of the greatest clinical importance.
- Excessive activation of T-helpers with an increase in the concentration and aggression of the cytokines secreted by them.
 These substances are able to have a direct and indirect damaging effect on embryonic tissues with a violation of their proliferation and differentiation. In fact, the fetal egg in this case acts as a target for the cellular link of immunity. The reason for such an abnormal immune response of a woman's body may be a chronic infection of the endometrium, hormonal abnormalities, and some other endogenous factors. nine0020
These substances are able to have a direct and indirect damaging effect on embryonic tissues with a violation of their proliferation and differentiation. In fact, the fetal egg in this case acts as a target for the cellular link of immunity. The reason for such an abnormal immune response of a woman's body may be a chronic infection of the endometrium, hormonal abnormalities, and some other endogenous factors. nine0020
It is important to understand that with anembryony in the body of a woman, substances are produced that contribute to the prolongation of pregnancy. Therefore, in a significant proportion of cases, spontaneous abortion does not occur. The patient develops and maintains signs of pregnancy, there is an increase in hCG in the blood serum. Therefore, the basal temperature during anembryony usually does not have characteristic features. And on the first early ultrasound, the fact of successful implantation of the fetal egg in the uterine cavity is confirmed. After all, pregnancy does occur, but it develops without a key component - the embryo. nine0005
nine0005
In the future, rejection of the abnormal fetal egg is possible. In this case, the threat of termination of pregnancy (including with the formation of exfoliating retrochorial hematomas) or spontaneous abortion (miscarriage) can be diagnosed. But often anembryony is diagnosed only during a routine examination, in which case the diagnosis is absolutely unexpected and shocking news. Such a pregnancy requires an artificial interruption.
How does this manifest itself?
Anembryony does not have its own clinical symptoms , all emerging disorders are usually associated with the threat of termination of such a pathological pregnancy. And the warning signs include the presence of clinical manifestations of relative progesterone deficiency, which creates the prerequisites for spontaneous abortion. Therefore, pain in the lower abdomen and bloody discharge can become a reason for contacting a doctor; with anembryony, they can appear at almost any time during the 1st trimester. But often a woman learns about the existing pathology only when conducting a screening ultrasound for a period of 10-14 weeks. nine0005
But often a woman learns about the existing pathology only when conducting a screening ultrasound for a period of 10-14 weeks. nine0005
Diagnosis
Like other forms of miscarriage, anembryony is detected in the first trimester of gestation. And the main diagnostic tool in this case is ultrasound , because it is this study that allows you to visualize the existing deviations.
At the same time, symptoms can be reliably detected only after the 8th week of gestation. At earlier dates, visualization is often insufficient due to the too small size of the ovum, so an erroneous diagnosis is not ruled out. Therefore If a missed pregnancy and anembryony are suspected, it is recommended to conduct an examination several times, repeating the procedure on expert-class equipment with an interval of 6-8 days. At the same time, the initial diagnosis of an empty fetal egg can be removed if subsequent ultrasound scans can visualize an embryo with signs of a heartbeat and sufficient developmental dynamics.
The main echographic features:
- absence of the yolk sac when the diameter of the fetal egg is 8-25 mm; nine0020
- absence of an embryo in a fetal egg with a diameter of more than 25 mm.
Additional signs of a missed pregnancy include an irregular shape of the fetal egg, an insufficient increase in its diameter in dynamics, a weak severity of the decidual reaction, and the absence of a heartbeat at a gestational age of 7 or more weeks. And signs of the threat of its interruption are a change in the tone of the uterus and the appearance of areas of chorion detachment with the appearance of subchorial hematomas.
Anembryony can also be suspected by a dynamic assessment of the level of hCG in the blood. An increase in the level of this hormone along the lower limit of the norm should be the basis for further examination of a woman with an ultrasound scan. It is important to understand that hCG is also produced in the syndrome of an empty ovum. Moreover, its level in this pathology will be almost normal, in contrast to a frozen pregnancy with the death of a normally developing embryo. Therefore, monitoring of indirect signs of pregnancy and the growth of hCG during anembryony cannot be attributed to reliable diagnostic methods. nine0005
Moreover, its level in this pathology will be almost normal, in contrast to a frozen pregnancy with the death of a normally developing embryo. Therefore, monitoring of indirect signs of pregnancy and the growth of hCG during anembryony cannot be attributed to reliable diagnostic methods. nine0005
Varieties
Several variants of the empty ovum syndrome are possible:
- Type I anembryony. The embryo and its remains are not visualized, the size of the fetal egg and uterus does not correspond to the expected gestational age. The diameter of the egg is usually no more than 2.5 mm, and the uterus is enlarged only up to 5-7 weeks of gestation.
- Type II anembryony. There is no embryo, but the fetal egg and uterus correspond to the gestational age. nine0020
- Resorption of one or more embryos in multiple pregnancies. At the same time, normally developing and regressing fetal eggs are visualized.
 According to this type, anembryony often occurs after IVF, if several embryos were implanted in a woman.
According to this type, anembryony often occurs after IVF, if several embryos were implanted in a woman.
All these varieties are determined only with the help of ultrasound, they do not have characteristic clinical features .
What to do?
Confirmed anembryony is an indication for abortion. This does not take into account the gestational age, the woman's well-being and the presence of signs of a possible spontaneous abortion. An exception is the situation when the anembryony of the second fetal egg is diagnosed in a multiple pregnancy. In this case, a wait-and-see strategy is taken, evaluating the dynamics of the development of the preserved embryo. nine0005
Termination of a missed pregnancy is carried out only in a hospital. After the procedure for the evacuation of the fetal egg, the woman should be under medical supervision. In many cases, after it, additional medication and sometimes physiotherapy are prescribed, aimed at normalizing the hormonal background, preventing inflammatory and hemorrhagic complications, and eliminating the detected infection.
Several techniques can be used to perform a medical abortion for this pathology. Can be used:
- medical abortion - termination of pregnancy with the help of hormonal drugs that provoke rejection of the endometrium along with an implanted fetal egg;
- vacuum aspiration of the contents of the uterine cavity;
- curettage is an operation involving the mechanical removal of the fetal egg and endometrium with a special instrument (curette) after the forced expansion of the cervical canal with bougie.
Medical abortion for anembryos is possible only for a period of 6-8 weeks. In later periods of gestation, preference is given to mechanical methods, which requires the use of general anesthesia. The choice of the method of artificial abortion depends on whether the stomach hurts after an abortion, the length of the rehabilitation period, the likelihood of early and late complications. nine0005
Examination after induced abortion necessarily includes ultrasound control. This allows you to confirm the complete evacuation of the membranes and endometrium, to exclude undesirable consequences of abortion in the form of hematomas, perforation and endometritis.
This allows you to confirm the complete evacuation of the membranes and endometrium, to exclude undesirable consequences of abortion in the form of hematomas, perforation and endometritis.
Prediction
Can anembryony recur? Can I still have children? These questions concern all patients who have undergone this pathology. Fortunately, in most cases, the condition does not recur, the woman subsequently manages to safely become pregnant and bear the child. But at the same time, she is classified as a risk group for the possible development of complications of pregnancy and childbirth. Therefore, in the first trimester, she is usually assigned dynamic ultrasound control of the development of the fetal egg, determination of the hormonal profile and assessment of the state of the hemostasis system. nine0005
Pregnancy after anembryos is theoretically possible already in the next ovarian-menstrual cycle. But it is desirable to let the body recover. Therefore, it is recommended to start planning for re-conception not earlier than 3 months after the induced abortion . If it proceeded with complications, the rehabilitation period, while maintaining reproductive rest, is extended for up to six months. If a woman has chronic endometritis and various infections, 2 months after the completion of treatment, a control examination is carried out and only then the possible timing of re-conception is determined. nine0005
Therefore, it is recommended to start planning for re-conception not earlier than 3 months after the induced abortion . If it proceeded with complications, the rehabilitation period, while maintaining reproductive rest, is extended for up to six months. If a woman has chronic endometritis and various infections, 2 months after the completion of treatment, a control examination is carried out and only then the possible timing of re-conception is determined. nine0005
Barrier method and hormonal contraception are preferred to prevent pregnancy. The selection of funds in this case is carried out individually. Intrauterine devices immediately after a frozen pregnancy are not used in order to avoid the development of endometritis.
Prevention
Primary prevention of anembryonia includes careful planning of pregnancy with a comprehensive examination. If deviations are found, they are corrected. Of course, such preparation does not allow 100% to exclude the possibility of pathology, but reduces the risk of its development. nine0005
nine0005
Secondary prophylaxis is carried out if the woman has a history of spontaneous abortions and anembryos. The first pregnancy with empty ovum syndrome is a reason for a subsequent examination of a woman for infections and hemostasis disorders. When the situation repeats, a genetic examination of the spouses is also shown to exclude anomalies in their hereditary material. In some cases, subsequent conception is preferably carried out using IVF, which will allow the use of preimplantation diagnosis to detect chromosomal abnormalities in embryos. nine0005
Anembryony is diagnosed quite often. And, unfortunately, at present it is not yet possible to completely exclude such a pathology already at the stage of pregnancy planning. After all, it can develop even in completely healthy and examined patients. At the same time, a missed missed pregnancy does not mean the impossibility of a repeated successful conception; most women after anembryony manage to safely give birth to a healthy child.
Anembryony - causes, symptoms | Diamed
Anembryony is a pathology of pregnancy, also known as "premature miscarriage" or "missed pregnancy". This type of miscarriage is one of the most common due to the difficulty of detection. In 60% of cases, this pathology can manifest itself for years without causing discomfort to a woman, especially if during this period of time the woman does not plan pregnancy and does not contact an obstetrician-gynecologist on this issue. Women suffering from disorders of the regularity of the menstrual cycle are more susceptible to this pathology. nine0005
Anembryony is a type of abnormal pregnancy in which conception occurs but the embryo does not develop.
Obstetrics, as a science, cannot always answer questions about the causes of this pathology. With anembryony, an empty fetal egg is diagnosed. That is, conception occurs, but the embryo in the early stages stops developing and dies for some reason, and ultrasound diagnostics give the impression of the absence of an embryo due to its small size. Most often, this pathology develops between the 5th and 9thth week of pregnancy.
Most often, this pathology develops between the 5th and 9thth week of pregnancy.
If after this period the pregnancy is not interrupted and the embryo continues to develop, this pathology can no longer develop. If a woman did not go to the doctor or did not detect pregnancy in a timely manner, then in the event of the development of anembryonia, the embryo that stopped developing and died, along with the fetal egg, will leave the uterus naturally during the next menstrual bleeding, without causing inconvenience or discomfort to the woman. Anembryony, regardless of detection, leads to the independent exit of a dead embryo from the body of a woman and does not provoke inflammatory or infectious processes. nine0005
There is only one way to diagnose this pathology - ultrasound examination of the pelvic organs. If an ultrasound scan detects an empty fetal egg or the absence of embryo development, anembryonia is diagnosed.
Reasons for the development of anembronia
Obstetrics at this stage of development can not always establish the causes of the development of pathology, the most common are:
- Pathology at the genetic level.
 Currently considered the main cause of anembryos. The pathology of the female or male genetic material (eggs or sperm, respectively) causes anembryony. Even if the genetic material of one of the parents is normal, the pathogenic cell of the second will provoke a stop in the development of the embryo. Thus, in the treatment of this type of miscarriage, both partners should be diagnosed. nine0020
Currently considered the main cause of anembryos. The pathology of the female or male genetic material (eggs or sperm, respectively) causes anembryony. Even if the genetic material of one of the parents is normal, the pathogenic cell of the second will provoke a stop in the development of the embryo. Thus, in the treatment of this type of miscarriage, both partners should be diagnosed. nine0020 - Virus, infection, inflammation. A bacterial or viral infection, as well as an inflammatory process in any part of the female body, can cause an arrest in the development of the embryo. Colds, dental diseases, inflammation of the genital organs, etc. promote the spread of pathogenic bacteria throughout the body. With reduced immunity, the risk of infection and subsequent death of the embryo increases.
- External factors. Ecological conditions, clean air, background radiation and other external factors can also cause anembryony. nine0020
- Hormonal causes.
 Any disturbances and failures in the work of the endocrine system trigger the mechanisms of destruction of the embryo. If the mother does not suffer from endocrinological disorders, but the father has a hormonal imbalance, fetal death occurs due to sperm pathologies.
Any disturbances and failures in the work of the endocrine system trigger the mechanisms of destruction of the embryo. If the mother does not suffer from endocrinological disorders, but the father has a hormonal imbalance, fetal death occurs due to sperm pathologies.
Prevention of anembronia
Prevention of pathology consists primarily in a woman's attentive attitude to her health and monitoring changes in her state of health and condition. Since anembryony develops in the earliest stages of pregnancy, in some cases, women will find out that they were pregnant after the death of the fetus or not at all. Such latent miscarriage is fraught with aggravation of the situation in the future, since it is impossible to cure a pathology that has not been detected. nine0005
The main prevention tip is early detection of pregnancy through a blood test, ultrasound or rapid test. If pregnancy is detected, you should immediately register and undergo a full diagnosis.