Pregnancy induction methods
Inducing Labor (for Parents) - Nemours KidsHealth
It's common for many pregnant women, especially first-time mothers, to watch their baby's due date come and go without so much as a contraction. The farther away from the expected delivery date (called the EDD) you get, the more anxious you might become. You may start to wonder — is this baby ever going to come?
Late pregnancy can be challenging — you may feel large all over, your feet and back might hurt, you might not have the energy to do much of anything, and you're beyond ready to meet the little one you've nurtured all this time. Which is why waiting a little longer than you'd expected can be particularly hard.
Still, being past your due date doesn't guarantee that your doctor (or other health care provider) will do anything to induce (or artificially start) labor — at least not right away.
What Is It?
Labor induction is what doctors use to try to help labor along using medications or other medical techniques. Years ago, some doctors routinely induced labor. But now it's not usually done unless there's a true medical need for it. Labor is usually allowed to take its natural course. However, in some situations, a health care provider may recommend induction.
Why It's Done
Your doctor might suggest an induction if:
- your water broke but you are not having contractions
- your baby still hasn't arrived by 2 weeks after the due date (when you're considered post-term — more than 42 weeks into your pregnancy)
- you have an infection in the uterus (called chorioamnionitis)
- you have certain risk factors (e.g., gestational diabetes or high blood pressure)
- there is not enough amniotic fluid
- there is a problem with the placenta
- the baby is not growing appropriately
Induction also can be appropriate under certain circumstances, as with a mother who is full term and has a history of rapid deliveries or lives far from a hospital.
Some mothers request elective inductions for convenience, but these do come with risks. Doctors try to avoid inducing labor early because the due date may be wrong and/or the woman's cervix might not be ready yet.
Page 2
How It's Done
Some methods of induction are less invasive and carry fewer risks than others. Ways that doctors may try to induce labor by getting contractions started include:
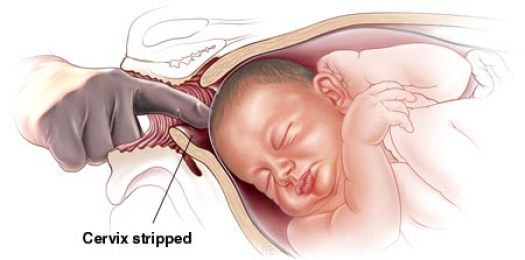
- Stripping the membranes. The doctor puts on a glove and inserts a finger into the vagina and through the cervix (the opening that connects the vagina to the uterus). He or she moves the finger back and forth to separate the thin membrane connecting the amniotic sac (which houses the baby and amniotic fluid) to the wall of the uterus. When the membranes are stripped, the body releases hormones called prostaglandins, which help prepare the cervix for delivery and may bring on contractions. This method works for some women, but not all.
- Breaking your water (also called an amniotomy).
 The doctor ruptures the amniotic sac during a vaginal exam using a little plastic hook to break the membranes. If the cervix is ready for labor, amniotomy usually brings on labor in a matter of hours.
The doctor ruptures the amniotic sac during a vaginal exam using a little plastic hook to break the membranes. If the cervix is ready for labor, amniotomy usually brings on labor in a matter of hours. - Giving the hormone prostaglandin to help ripen the cervix. A gel or vaginal insert of prostaglandin is inserted into the vagina or a tablet is given by mouth. This is typically done overnight in the hospital to make the cervix "ripe" (soft, thinned out) for delivery. Administered alone, prostaglandin may induce labor or may be used before giving oxytocin.
- Giving the hormone oxytocin to stimulate contractions. Given continuously through an IV, the drug (Pitocin) is started in a small dose and then increased until labor is progressing well. After it's administered, the fetus and uterus need to be closely monitored. Oxytocin is also frequently used to spur labor that's going slowly or has stalled.
What Will It Feel Like?
Stripping the membranes can be a little painful or uncomfortable, although it usually only takes a minute or so. You may also have some intense cramps and spotting for the next day or two.
You may also have some intense cramps and spotting for the next day or two.
It can also be a little uncomfortable to have your water broken. You may feel a tug followed by a warm trickle or gush of fluid.
With prostaglandin, you might have some strong cramping as well. With oxytocin, contractions are usually more frequent and regular than in a labor that starts naturally.
Page 3
Risks and Precautions
Inducing labor is not like turning on a faucet. If the body isn't ready, an induction might fail and, after hours or days of trying, a woman may end up having a cesarean delivery (C-section). This appears to be more likely if the cervix is not yet ripe.
If the doctor ruptures the amniotic sac and labor doesn't begin, another method of inducing labor also might be necessary because there's a risk of infection to both mother and baby if the membranes are ruptured for a long time before the baby is born.
When prostaglandin or oxytocin is used, there is a risk of abnormal contractions developing. In that case, the doctor may remove the vaginal insert or turn the oxytocin dose down. While it is rare, there is an increase in the risk of developing a tear in the uterus (uterine rupture) when these medications are used. Other complications associated with oxytocin use are low blood pressure and low blood sodium (which can cause problems such as seizures).
In that case, the doctor may remove the vaginal insert or turn the oxytocin dose down. While it is rare, there is an increase in the risk of developing a tear in the uterus (uterine rupture) when these medications are used. Other complications associated with oxytocin use are low blood pressure and low blood sodium (which can cause problems such as seizures).
Another potential risk of inducing labor is giving birth to a late pre-term baby (born after 34 and before 37 weeks). Why? Because the due date (EDD) may be wrong. Your due date is 40 weeks from the first day of your last menstrual period (LMP).
Babies born late pre-term are generally healthy but may have temporary problems such as jaundice, trouble feeding, problems with breathing, or difficulty maintaining body temperature. They may also be more likely than full term babies to have developmental or school problems later on.
Even though inductions do come with risks, going beyond 42 weeks of pregnancy can be risky, too. Many babies are born "post-term" without any complications, but concerns include:
Many babies are born "post-term" without any complications, but concerns include:
- A vaginal delivery may become harder as the baby gets bigger. As babies get bigger, the chance of an injury during delivery, such as a broken bone, increases.
- The placenta that helps to provide the baby with nourishment is deteriorating.
- The amniotic fluid can become low or contain meconium — the baby's first feces. If the baby breathes in meconium, it can cause breathing problems.
Old wives' tales abound about ways to induce labor, such as the use of castor oil. It is not safe to try to artificially start labor yourself by taking castor oil, which can lead to nausea, diarrhea, and dehydration. And herbs and herbal supplements meant to induce labor can be harmful. Breast stimulation can cause uterine contractions by causing the release of oxytocin. However, some studies have suggested that the baby might have abnormal heartbeats after breast stimulation. Some women feel that having sex in late pregnancy can induce labor, but there is no conclusion on this yet.
Talk to your doctor before doing anything to try to encourage your little one's arrival. Inducing labor is best left to medical professionals — you may cause more harm than good.
As frustrating as it can be waiting for your baby to finally decide to arrive, letting nature take its course is often best, unless your doctor tells you otherwise. Before you know it, you'll be too busy to remember your baby was ever late at all!
Labor induction - Mayo Clinic
Overview
Labor induction — also known as inducing labor — is prompting the uterus to contract during pregnancy before labor begins on its own for a vaginal birth.
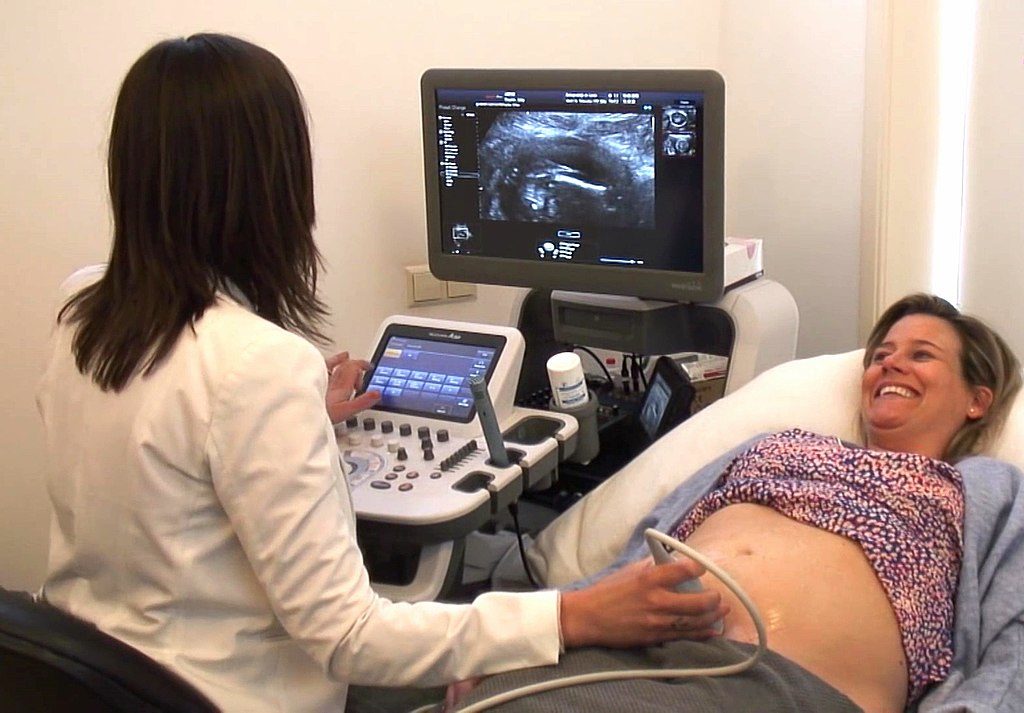
A health care provider might recommend inducing labor for various reasons, primarily when there's concern for the mother's or baby's health. An important factor in predicting whether an induction will succeed is how soft and expanded the cervix is (cervical ripening). The gestational age of the baby as confirmed by early, regular ultrasounds also is important.
If a health care provider recommends labor induction, it's typically because the benefits outweigh the risks. If you're pregnant, understanding why and how labor induction is done can help you prepare.
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Book: Mayo Clinic Guide to a Healthy Pregnancy
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Why it's done
To determine if labor induction is necessary, a health care provider will likely evaluate several factors. These include the mother's health and the status of the cervix. They also include the baby's health, gestational age, weight, size and position in the uterus. Reasons to induce labor include:
- Nearing 1 to 2 weeks beyond the due date without labor starting (postterm pregnancy).
- When labor doesn't begin after the water breaks (prelabor rupture of membranes).
- An infection in the uterus (chorioamnionitis).

- When the baby's estimated weight is less than the 10th percentile for gestational age (fetal growth restriction).
- When there's not enough amniotic fluid surrounding the baby (oligohydramnios).
- Possibly when diabetes develops during pregnancy (gestational diabetes), or diabetes exists before pregnancy.
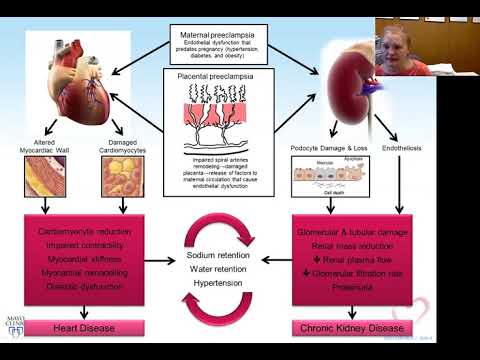
- Developing high blood pressure in combination with signs of damage to another organ system (preeclampsia) during pregnancy. Or having high blood pressure before pregnancy, developing it before 20 weeks of pregnancy (chronic high blood pressure) or developing the condition after 20 weeks of pregnancy (gestational hypertension).
- When the placenta peels away from the inner wall of the uterus before delivery — either partially or completely (placental abruption).
- Having certain medical conditions. These include heart, lung or kidney disease and obesity.
Elective labor induction is the starting of labor for convenience when there's no medical need. It can be useful for women who live far from the hospital or birthing center or who have a history of fast deliveries.
It can be useful for women who live far from the hospital or birthing center or who have a history of fast deliveries.
A scheduled induction might help avoid delivery without help. In such cases, a health care provider will confirm that the baby's gestational age is at least 39 weeks or older before induction to reduce the risk of health problems for the baby.
As a result of recent studies, women with low-risk pregnancies are being offered labor induction at 39 to 40 weeks. Research shows that inducing labor at this time reduces several risks, including having a stillbirth, having a large baby and developing high blood pressure as the pregnancy goes on. It's important that women and their providers share in decisions to induce labor at 39 to 40 weeks.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Risks
Uterine incisions used during C-sections
Uterine incisions used during C-sections
A C-section includes an abdominal incision and a uterine incision. After the abdominal incision, the health care provider will make an incision in the uterus. Low transverse incisions are the most common (top left).
After the abdominal incision, the health care provider will make an incision in the uterus. Low transverse incisions are the most common (top left).
Labor induction carries various risks, including:
- Failed induction. An induction might be considered failed if the methods used don't result in a vaginal delivery after 24 or more hours. In such cases, a C-section might be necessary.
- Low fetal heart rate. The medications used to induce labor — oxytocin or a prostaglandin — might cause the uterus to contract too much, which can lessen the baby's oxygen supply and lower the baby's heart rate.
- Infection. Some methods of labor induction, such as rupturing the membranes, might increase the risk of infection for both mother and baby. The longer the time between membrane rupture and labor, the higher the risk of an infection.
-
Uterine rupture. This is a rare but serious complication in which the uterus tears along the scar line from a prior C-section or major uterine surgery.
 Rarely, uterine rupture can also occur in women who have not had previous uterine surgery.
Rarely, uterine rupture can also occur in women who have not had previous uterine surgery.An emergency C-section is needed to prevent life-threatening complications. The uterus might need to be removed.
- Bleeding after delivery. Labor induction increases the risk that the uterine muscles won't properly contract after giving birth, which can lead to serious bleeding after delivery.
Labor induction isn't for everyone. It might not be an option if:
- You've had a C-section with a classical incision or major uterine surgery
- The placenta is blocking the cervix (placenta previa)
- Your baby is lying buttocks first (breech) or sideways (transverse lie)
- You have an active genital herpes infection
- The umbilical cord slips into the vagina before delivery (umbilical cord prolapse)
If you have had a C-section and have labor induced, your health care provider is likely to avoid certain medications to reduce the risk of uterine rupture.
How you prepare
Labor induction is typically done in a hospital or birthing center. That's because mother and baby can be monitored there, and labor and delivery services are readily available.
What you can expect
During the procedure
There are various ways of inducing labor. Depending on the circumstances, the health care provider might use one of the following ways or a combination of them. The provider might:
-
Ripen the cervix. Sometimes prostaglandins, versions of chemicals the body naturally produces, are placed inside the vagina or taken by mouth to thin or soften (ripen) the cervix. After prostaglandin use, the contractions and the baby's heart rate are monitored.
In other cases, a small tube (catheter) with an inflatable balloon on the end is inserted into the cervix. Filling the balloon with saline and resting it against the inside of the cervix helps ripen the cervix.
- Sweep the membranes of the amniotic sac.
 With this technique, also known as stripping the membranes, the health care provider sweeps a gloved finger over the covering of the amniotic sac near the fetus. This separates the sac from the cervix and the lower uterine wall, which might help start labor.
With this technique, also known as stripping the membranes, the health care provider sweeps a gloved finger over the covering of the amniotic sac near the fetus. This separates the sac from the cervix and the lower uterine wall, which might help start labor. -
Rupture the amniotic sac. With this technique, also known as an amniotomy, the health care provider makes a small opening in the amniotic sac. The hole causes the water to break, which might help labor go forward.
An amniotomy is done only if the cervix is partially dilated and thinned, and the baby's head is deep in the pelvis. The baby's heart rate is monitored before and after the procedure.
- Inject a medication into a vein. In the hospital, a health care provider might inject a version of oxytocin (Pitocin) — a hormone that causes the uterus to contract — into a vein. Oxytocin is more effective at speeding up labor that has already begun than it is as at cervical ripening.
 The provider monitors contractions and the baby's heart rate.
The provider monitors contractions and the baby's heart rate.
How long it takes for labor to start depends on how ripe the cervix is when the induction starts, the induction techniques used and how the body responds to them. It can take minutes to hours.
After the procedure
In most cases, labor induction leads to a vaginal birth. A failed induction, one in which the procedure doesn't lead to a vaginal birth, might require another induction or a C-section.
By Mayo Clinic Staff
Related
Products & Services
Induction of labor or induction of labor
The purpose of this informational material is to familiarize the patient with the induction of labor procedure and to provide information on how and why it is performed.
In most cases, labor begins between the 37th and 42nd weeks of pregnancy. Such births are called spontaneous. If drugs or medical devices are used before the onset of spontaneous labor, then the terms "stimulated" or "induced" labor are used in this case.
Labor should be induced when further pregnancy is for some reason unsafe for the mother or baby and it is not possible to wait for spontaneous labor to begin.
The purpose of stimulation is to start labor by stimulating uterine contractions.
When inducing labor, the patient must be in the hospital so that both mother and baby can be closely monitored.
Labor induction methods
The choice of labor induction method depends on the maturity of the cervix of the patient, which is assessed using the Bishop scale (when viewed through the vagina, the position of the cervix, the degree of its dilatation, consistency, length, and the position of the presenting part of the fetus in the pelvic area are assessed). Also important is the medical history (medical history) of the patient, for example, a past caesarean section or operations on the uterus.
The following methods are used to induce (stimulate) labor:
- Oral misoprostol is a drug that is a synthetic analogue of prostaglandins found in the body.
 It prepares the body for childbirth, under its action the cervix becomes softer and begins to open.
It prepares the body for childbirth, under its action the cervix becomes softer and begins to open. - Balloon Catheter - A small tube is placed in the cervix and the balloon attached to the end is filled with fluid to apply mechanical pressure to the cervix. When using this method, the cervix becomes softer and begins to open. The balloon catheter is kept inside until it spontaneously exits or until the next gynecological examination.
- Amniotomy or opening of the fetal bladder - in this case, during a gynecological examination, when the cervix has already dilated sufficiently, the fetal bladder is artificially opened. When the amniotic fluid breaks, spontaneous uterine contractions will begin, or intravenous medication may be used to stimulate them.
- Intravenously injected synthetic oxytocin - acts similarly to the hormone of the same name produced in the body. The drug is given by intravenous infusion when the cervix has already dilated (to support uterine contractions).
 The dose of the drug can be increased as needed to achieve regular uterine contractions.
The dose of the drug can be increased as needed to achieve regular uterine contractions.
When is it necessary to induce labor?
Labor induction is recommended when the benefits outweigh the risks.
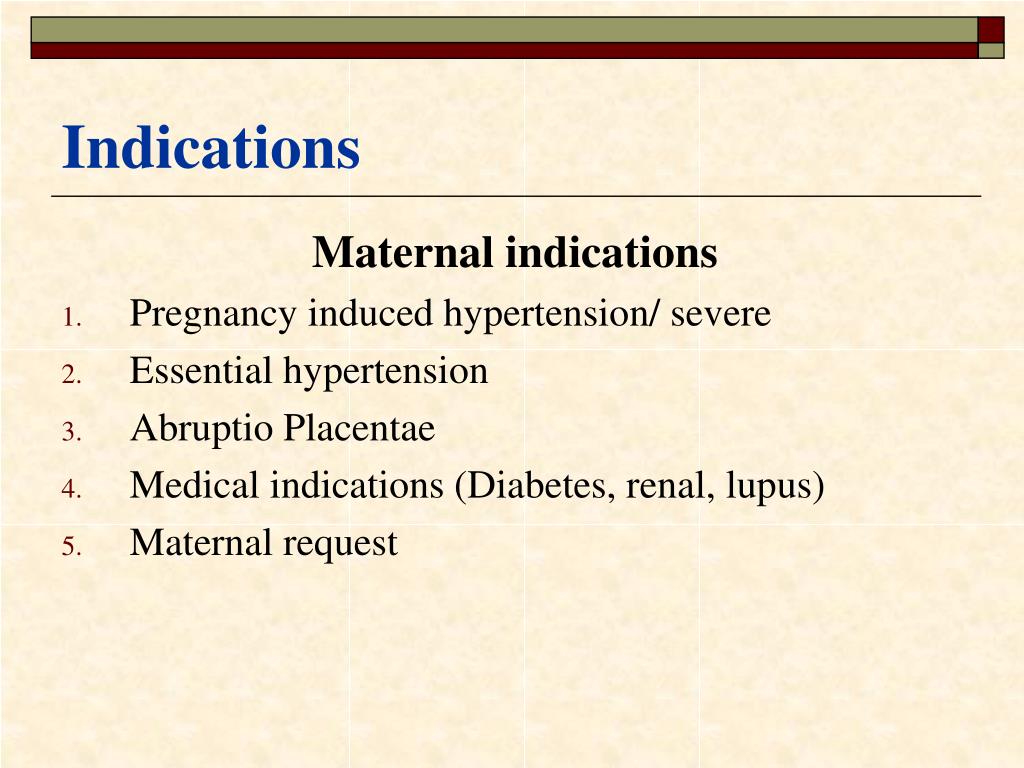
Induction of labor may be indicated in the following cases:
- The patient has a comorbid condition complicating pregnancy (eg, high blood pressure, diabetes mellitus, preeclampsia, or some other condition).
- The duration of pregnancy is already exceeding the norm - the probability of intrauterine death of the fetus increases after the 42nd week of pregnancy.
- Fetal problems, eg, problems with fetal development, abnormal amount of amniotic fluid, changes in fetal condition, various fetal disorders.
- If the amniotic fluid has broken and uterine contractions have not started within the next 24 hours, there is an increased risk of inflammation in both the mother and the fetus. This indication does not apply in case of preterm labor, when preparation of the baby's lungs with a special medicine is necessary before delivery.
- Intrauterine fetal death.
What are the risks associated with labor induction?
Labor induction is not usually associated with significant complications.
Occasionally, after receiving misoprostol, a patient may develop fever, chills, vomiting, diarrhea, and too frequent uterine contractions (tachysystole). In case of too frequent contractions to relax the uterus, the patient is injected intravenously relaxing muscles uterus medicine. It is not safe to use misoprostol if you have had a previous caesarean section as there is a risk of rupture of the uterine scar.
The use of a balloon catheter increases the risk of inflammation inside the uterus.
When using oxytocin, the patient may rarely experience a decrease in blood pressure, tachycardia (rapid heartbeat), hyponatremia (lack of sodium in the blood), which may result in headache, loss of appetite, nausea, vomiting, abdominal pain, depression strength and sleepiness.
Induction of labor, compared with spontaneous labor, increases the risk of prolonged labor, the need for instrumentation
(use of vacuum or forceps), postpartum hemorrhage, uterine rupture, the onset of too frequent uterine contractions and the associated deterioration of the fetus, prolapse umbilical cord, as well as premature detachment of the placenta.
If induction of labor is not successful
The time frame for induction of labor varies from patient to patient, on average labor begins within 24-72 hours. Sometimes more than one method is required.
The methods used do not always work equally quickly and in the same way on different patients. If the cervix does not dilate as a result of induction of labor, your doctor will tell you about your next options (which may include inducing labor later, using a different method, or delivering by caesarean section).
ITK833
This informational material was approved by the Women's Clinic on 01/01/2022.
Efficiency and outcomes of labor induction in prolonged and post-term pregnancy » Obstetrics and Gynecology
Purpose of the study. To evaluate the effectiveness of various methods of labor induction, the characteristics of the course of labor and factors affecting the success of induction in patients with prolonged and post-term pregnancy.
Material and methods. 71 women with singleton pregnancy 40 weeks 2 days or more and cephalic presentation of the fetus were examined. Depending on the method of labor induction, the patients were divided into three groups. In the 1st group, amniotomy was used, in the 2nd - the sequential use of dinoprostone and amniotomy, in the 3rd - intravenous drip administration of dinoprost with a whole fetal bladder. The 4th (control) group consisted of women with spontaneous onset of labor at the same time of pregnancy. Statistical data processing was carried out using the indicators of the risk ratio, the odds ratio, the Wilcoxon test.
Research results. The effectiveness of labor induction in patients with a tendency to prolong pregnancy was high and amounted to 80% with induction of labor by amniotomy, 86.7% with a combination of pgE2 analogues and amniotomy, and 100% with dinoprost. A characteristic feature of the course of labor during post-term pregnancy is the high frequency of labor anomalies, while the induction of labor does not increase the risk of developing this pathology. The fundamental factor affecting the success of labor induction is the condition of the cervix; therefore, induction of labor should be carried out only when she reaches maturity. With an increase in the gestational age of more than 41 weeks, the number of complications of induced labor increases, so the optimal gestational age for the preparation of the cervix and induction of labor is 40–41 weeks.
Development and improvement of methods for preparing the cervix for childbirth and labor induction
are an urgent task at the present stage of development of obstetrics. Rational pre-induction and induction of labor can be considered as one of the reserve options for reducing the frequency of caesarean sections. Labor induction is considered reasonable if its use improves maternal and perinatal outcomes and does not lead to an increase in the number of complications.
Rational pre-induction and induction of labor can be considered as one of the reserve options for reducing the frequency of caesarean sections. Labor induction is considered reasonable if its use improves maternal and perinatal outcomes and does not lead to an increase in the number of complications.
There is now a spectrum of both drugs and mechanical methods,
used for preparation of the birth canal and induction of labor. In this regard, the problem of their rational use and correct choice in a particular clinical situation is extremely important.
One of the most common indications for labor induction is the prolongation of pregnancy [5]. In the absence of opportunities to influence the pathogenetic factors leading to this condition, the only method for preventing adverse outcomes in this group of patients is the preparation of the cervix for childbirth and labor induction.
However, to date there is no consensus on the terms of pregnancy, at which
it is necessary to induce labor, the optimal methods of labor induction for patients with post-term pregnancy and the characteristic features of the
course of
induced labor have not been determined.
All of the above determined the purpose of this study: to compare the effectiveness of various methods of labor induction in patients with a tendency to over-term pregnancy, to study the features of the course of labor, as well as the outcomes of induced labor and labor with spontaneous
beginning, identify factors that affect the success of induction.
Material and research methods
71 patients were examined. Inclusion criteria: gestational age - 40 weeks 2 days or more, spontaneous pregnancy, singleton pregnancy, head presentation of the fetus, parity not more than 2, the presence of intact membranes, no contraindications to the use of prostaglandin E2 analogs (pgE2) and F2alpha (pgF2α). Exclusion criteria: the presence of contraindications to childbirth through the birth canal, a scar on the uterus, fetal malformations. In all cases, the indication for labor induction was a tendency to prolong pregnancy. The state of the cervix before labor induction was assessed using the Burnhill scale (modified by E. A. Chernukha). A score of 0 to 3 points corresponded to an immature cervix, 4–6 to
A. Chernukha). A score of 0 to 3 points corresponded to an immature cervix, 4–6 to
insufficiently mature, 7 points or more - mature cervix. When analyzing the effectiveness of labor induction, the course and outcomes of labor, the data of patients with insufficiently mature cervix were taken into account.
Depending on the method of labor induction, the patients were divided into three groups. In the 1st
group, amniotomy was used; in the 2nd group, the sequential use of the pgE2 analogue (dinoprostone) and amniotomy; in the 3rd group, intravenous drip administration of the pgF2α analogue (dinoprost)
with a whole fetal bladder. In the 2nd group of patients, amniotomy was performed against the background of regular
uterine contractions. The average interval between intracervical administration of dinoprostone
and amniotomy was 3.2 hours. Labor induction was performed under continuous cardiotocographic control. The 4th (control) group consisted of women with a tendency to overpregnancy and spontaneous onset of labor. Characteristics of patients in groups are shown in table. 1.
Characteristics of patients in groups are shown in table. 1.
Table 1. Characteristics of patients in the study groups.
Childbirth pain relief was performed using epidural analgesia. The frequency of its use was 78% in the 1st group of patients, 50% in the 2nd, 82% in the 3rd and 80% in the 4th groups. The rest
patients did not require medical anesthesia for childbirth.
Statistical data processing was carried out using relative
risk (RR), odds ratio (OR), modified Haldane formula for small numbers,
Wilcoxon test.
The results of the study
The analysis showed that in induced labor in patients with a tendency to prolong pregnancy, the average interval from the start of induction to the development of regular
labor activity depended on the methods used.
Its average duration was the shortest when using amniotomy and amounted to
32 minutes, while when using a combined technique (dinoprostone and amniotomy) and labor induction by intravenous administration of dinoprost, it was 60 minutes (Table 2).
Table 2 . The course of induced and spontaneous labor.
However, in a number of observations, the method used did not cause the development of regular labor activity. This situation was considered by us as the absence of the effect of labor induction and required the determination of further management tactics.
In particular, the isolated use of amniotomy did not work in 20% of cases, and the combined use of prostaglandin-containing gel and amniotomy was ineffective in 13% of patients. There were no such observations in the 3rd group.
It should be noted that when comparing the effectiveness of labor induction in primiparous and multiparous women, it was found that the lack of effect was more often noted in primiparous patients, and among them - mainly in the 1st group.
In most cases, with the ineffectiveness of the applied method, induction of labor was
continued with an infusion of dinoprost solution. And only in two patients, further labor induction was regarded as inappropriate due to the presence of signs of chronic fetal hypoxia (meconium staining of amniotic fluid). They were delivered by caesarean section.
They were delivered by caesarean section.
The study of the characteristics of the course of labor in patients with a tendency to prolong pregnancy
revealed the following patterns.
Induced labor was accompanied by the development of primary weakness of labor activity
in 41.7% of cases with the use of amniotomy, 33% with a combination of pgE2 analogs and amniotomy, 11% with labor induction with dinoprost (>0.05; Fig. 1). With a spontaneous onset of labor in
patients with a tendency to prolong pregnancy, the frequency of its occurrence was 20%.
Comparative analysis of the development of primary weakness of labor activity after labor induction, depending on the parity, revealed the following patterns. In the 1st group of patients in nulliparous 9In 0089 women, the risk of primary weakness was 4.4 times higher than in multiparous women. The opposite trend was
characteristic of the 2nd group of patients, in which multiparous women had a
greater risk of developing this complication (1. 7 times).
7 times).
Our results showed that secondary weakness of labor was also a characteristic complication of induced labor. With amniotomy and the combined use of dinoprostone and amniotomy, its frequency was 25 and 20%, respectively. However, most often this variant of labor anomalies occurred during labor induction with dinoprost (44% of women). In spontaneous childbirth, secondary weakness of labor activity was diagnosed in 26.6% of women.
To determine the relationship between labor induction and the development of weakness of labor
in patients with a tendency to prolong pregnancy, we conducted a comparative analysis of induced and spontaneous labor. Based on this, it was concluded that induction does not statistically significantly increase the chances of developing primary and secondary weakness of labor compared to labor with spontaneous onset (OR=1.7; p=0.4).
One of the fundamentally important characteristics of the labor induction method is the frequency of delivery by caesarean section, because it is this indicator that is often considered as fundamental in choosing not only the method of induction, but also the tactics of managing patients (active or expectant).
In our study, in patients with spontaneous onset of labor, the rate of caesarean section was 33%, with induction of labor by intravenous administration of dinoprost 9%, with the use of amniotomy and a combination of pgE2 analogue and amniotomy - 17 and 40%, respectively. However, these differences were not statistically significant (p>0.05). The main indications for emergency and urgent surgery were a clinically narrow pelvis, labor anomalies, acute fetal hypoxia, and no effect of labor induction (Fig. 2).
As a result of assessing the duration of induced labor, we found that the average value of the interval from induction to delivery using various methods of labor induction was from 6.7 to 11.0 hours (p>0.05). Regardless of the method used, the interval from induction to delivery was the longest in nulliparous patients (9.7–11 h). While in multiparous women it ranged from 6.8±2.6 to 8.30±1.03 h. 0.9h, in multiparous – 6.2±1.8 h (p>0.05; see Table 2).
Thus, we have identified the main features of the course of induced labor in patients with a tendency to prolong pregnancy. However, it is extremely important to identify their relationship with the initial clinical data before conducting labor induction. One of the main parameters that determine the body's readiness for childbirth is the condition of the cervix.
However, it is extremely important to identify their relationship with the initial clinical data before conducting labor induction. One of the main parameters that determine the body's readiness for childbirth is the condition of the cervix.
Taking into account the presence of a high frequency of anomalies in the contractile activity of the uterus, an analysis was made of the relationship between the state of the cervix before the induction of labor and the overall frequency of anomalies in labor activity. It was found that with an insufficiently mature cervix, the risk of their development was 4 times higher than with an initially mature cervix (RR - 4.0, 95% CI - 1.3–11.0,
p=0.01).
In addition, we suggested that not only the condition of the cervix, but also the duration of pregnancy can be a factor influencing the course of childbirth in case of post-pregnancy. With spontaneous onset of labor, there was a trend towards an increase in the overall incidence of anomalies of labor (ARD) and caesarean section if delivery occurred at ≥ 41 weeks of gestation. In turn, labor induction at ≥ 41 weeks of gestation was accompanied by a significant increase in the risk of labor anomalies by 2.7 times (RR=2.7, p=0.03, 95% CI - 1.1-7.0), while the frequency of caesarean section did not increase significantly.
In turn, labor induction at ≥ 41 weeks of gestation was accompanied by a significant increase in the risk of labor anomalies by 2.7 times (RR=2.7, p=0.03, 95% CI - 1.1-7.0), while the frequency of caesarean section did not increase significantly.
All the examined women had children in a satisfactory condition. Of these, 14% of newborns had signs of Bellentine-Runge syndrome, and the births that occurred were regarded as belated. Assessment of the condition of newborns according to the Apgar scale in the labor induction and control groups at the 1st minute ranged from 7.6 to 7.8, at the 5th minute from 8.6 to 8.9 points, but the differences were statistically insignificant. The average weight of newborns ranged from 3466 to 3774 g.
Discussion
The results of the study indicate the high efficiency of labor induction in patients with a tendency to prolong pregnancy. The effectiveness of amniotomy was 80%, which is consistent with the data of a retrospective study by S. M. Cooley et al. [8], who noted 90.1% of successful labor inductions using this method. However, E.A. Chernukha [4] described the effective use of amniotomy in only 45–50% of women. In his opinion, the method of labor induction by intravenous administration of a solution of dinoprost is the most effective, with the use of which it was possible to achieve a result of 95–100% of observations, which is consistent with our data. The method of labor induction by sequential use of dinoprostone and amniotomy was used in this study for the first time, so there are no literature data on its use. Noteworthy is the fact that primiparas often do not have the effect of labor induction. Our results are consistent with literature data, in which the first upcoming birth is considered as one of the predictors of unsuccessful induction [9, 10]. The analysis of the obtained data showed that anomalies of the contractile activity of the uterus are the predominant complication of the course of both induced and spontaneous labor in patients with a tendency to prolong pregnancy.
M. Cooley et al. [8], who noted 90.1% of successful labor inductions using this method. However, E.A. Chernukha [4] described the effective use of amniotomy in only 45–50% of women. In his opinion, the method of labor induction by intravenous administration of a solution of dinoprost is the most effective, with the use of which it was possible to achieve a result of 95–100% of observations, which is consistent with our data. The method of labor induction by sequential use of dinoprostone and amniotomy was used in this study for the first time, so there are no literature data on its use. Noteworthy is the fact that primiparas often do not have the effect of labor induction. Our results are consistent with literature data, in which the first upcoming birth is considered as one of the predictors of unsuccessful induction [9, 10]. The analysis of the obtained data showed that anomalies of the contractile activity of the uterus are the predominant complication of the course of both induced and spontaneous labor in patients with a tendency to prolong pregnancy.
We found that labor induction by amniotomy had the highest level of primary weakness of labor (41.7%). These data are confirmed by the study by D. Selo-Ojeme et al. [11], who found that it was in this group of patients that oxytocin was most often required. An interesting fact is that the maximum level of secondary weakness of labor was noted during labor induction with dinoprost. Perhaps this is due to a violation of the sequence and balance of action of pgE2 and pgF2α characteristic of the normal course of labor [2].
Currently, literature data on the frequency and risk of delivery by caesarean section
in patients with a tendency to prolong pregnancy are contradictory. In the study by B. Bodner-Adler [5], a significant increase in the frequency of caesarean section was noted in the group of patients with induction of labor during prolonged pregnancy, while A.B. Caughey et al. [6] indicate that labor induction reduces the risk of caesarean section compared to expectant management, which significantly increases the chances of caesarean section (OR=1. 22, 95% CI - 1.07-1.39), especially for a period of ≥41 weeks. The study did not reveal a statistically significant increase in the risk of caesarean section in patients with induced labor.
22, 95% CI - 1.07-1.39), especially for a period of ≥41 weeks. The study did not reveal a statistically significant increase in the risk of caesarean section in patients with induced labor.
Lack of biological readiness of the body for childbirth adversely affects both the development of regular labor activity and the course of childbirth [1, 3]. The results of the study showed that the initial state of the cervix is a factor of paramount importance for the successful induction of labor and the normal course of the birth process. It was found that insufficient cervical maturity before labor induction is associated with a 4-fold increase in the risk of developing anomalies in labor.
Particularly noteworthy is the fact that the factor influencing the outcome of labor induction is the gestational age at which it is performed. However, this position remains poorly understood to date. A.B. Caughey et al. [6] found that a shorter gestational age is associated with successful induction of labor, and based on a systematic review [7] showed that at a gestational age of 41 weeks or more, the risk of delivery by caesarean section increases. We did not find a significant increase in the risk of caesarean section, but we found an increase in the risk of labor anomalies during induction at ≥ 41 weeks (p>0.05). In contrast to labor with spontaneous onset, when there is only a tendency to an increase in the frequency of anomalies of labor activity (ARD) with increasing gestational age, a clear correlation between these indicators was found during induction of labor. Apparently, this necessitates earlier preparation of the cervix for childbirth and labor induction in patients with a tendency to prolong pregnancy. The effectiveness of labor induction depends to a greater extent on the body's readiness for childbirth and to a lesser extent on the medications used [4].
We did not find a significant increase in the risk of caesarean section, but we found an increase in the risk of labor anomalies during induction at ≥ 41 weeks (p>0.05). In contrast to labor with spontaneous onset, when there is only a tendency to an increase in the frequency of anomalies of labor activity (ARD) with increasing gestational age, a clear correlation between these indicators was found during induction of labor. Apparently, this necessitates earlier preparation of the cervix for childbirth and labor induction in patients with a tendency to prolong pregnancy. The effectiveness of labor induction depends to a greater extent on the body's readiness for childbirth and to a lesser extent on the medications used [4].
This statement was confirmed in our study. However, it should be noted that the isolated use of amniotomy was characterized by the maximum frequency of no effect, especially in nulliparous women. The use of labor induction by intravenous administration of dinoprost is highly effective, but is accompanied by a high level of development of secondary weakness of labor activity. In addition, it should be borne in mind that during pregnancy, oligohydramnios is often formed, in which the induction of uterine contractions with a whole fetal bladder can lead to premature detachment of a normally located placenta. The combined technique, including dinoprostone and amniotomy, had a good effect and a low rate of ARD compared to other methods, but a high rate of caesarean section was noted, which requires further study.
In addition, it should be borne in mind that during pregnancy, oligohydramnios is often formed, in which the induction of uterine contractions with a whole fetal bladder can lead to premature detachment of a normally located placenta. The combined technique, including dinoprostone and amniotomy, had a good effect and a low rate of ARD compared to other methods, but a high rate of caesarean section was noted, which requires further study.
The study did not reveal a method that is the "gold standard" for induction of labor in patients with a tendency to prolong pregnancy. At the same time, it allowed us to determine the range of means and methods available in our arsenal that are acceptable and effective for this group of women.
In summary, it should be noted that in most cases in patients with a tendency to post-pregnancy, induction of labor can be considered as preventive. However, the prevention of possible severe complications and adverse outcomes, including stillbirths, makes labor induction in this group of women justified and rational.
Based on the study, the following conclusions can be drawn:
1. The effectiveness of labor induction in patients with a tendency to prolong pregnancy was high and amounted to 80% with induction of labor by amniotomy, 86.7% with a combination of pgE2 analogues and amniotomy, and 100% with dinoprost.
2. A characteristic feature of the course of labor during post-term pregnancy is a high frequency of
ARD, while induction of labor does not increase the risk of developing this pathology. Differences
in the frequency of operative delivery and outcomes of newborns in patients after labor induction and with spontaneous onset of labor was not found.
3. The fundamental factor affecting the success of labor induction is the condition of the
cervix, therefore, induction of labor should be carried out only when it reaches maturity.
4. With an increase in the gestational age of more than 41 weeks, the number of complications of induced labor increases, so the optimal period for cervical preparation and induction of labor is 40-41 weeks.
1. Gasparyan N.D., Kareva E.N. Mifepristone in the preparation and induction of labor // midwife. and gin. ‒ 2008. ‒ No. 3. ‒ P. 50–53.
2. Sidorova I.S. Physiology and pathology of labor activity: Textbook. - M.: MIA, 2006.
3. Strizhakov A.N., Ignatko I.V., Timokhina E.V., Rybin M.V. Postponed pregnancy. - M.: Dynasty, 2006.
4. Chernukha E.A. Postterm and prolonged pregnancy. – M.: GEOTAR-Media, 2007.
5. Bodner-Adler B., Bodner K., Pateisky N. et al. Influence of labor induction on obstetric outcomes in patients with pregnancy: a comparison between elective labor induction and spontaneous onset of labor beyond term // Wien. Klin. Wschr. - 2005. - Bd 117, No. 7–8. – S. 287–292.
6. Caughey A.B., Sundaram V., Kaimal A.J. et al. Maternal and neonatal outcomes of elective induction of labor // Evid. Rep. Technol. Assess. - 2009. - Vol. 176. - P. 241-257.
7. Caughey A.B., Sundaram V., Kaimal A.J. et al. Systematic review: elective induction of labor versus expectant management of pregnancy// Ann.