Preeclampsia in pregnancy 35 weeks
Signs, Causes, Risk Factors, Complications, Diagnosis, and Treatment
Written by WebMD Editorial Contributors
In this Article
- What Is Preeclampsia?
- Preeclampsia Symptoms
- When Do Symptoms Show Up?
- Preeclampsia Causes
- Other High Blood Pressure Disorders in Pregnancy
- Preeclampsia Risk Factors
- Preeclampsia Complications
- Preeclampsia Diagnosis
- Preeclampsia Treatment
- Preeclampsia Prevention
What Is Preeclampsia?
Preeclampsia, formerly called toxemia, is when pregnant women have high blood pressure, protein in their urine, and swelling in their legs, feet, and hands. It can range from mild to severe. It usually happens late in pregnancy, though it can come earlier or just after delivery.
Preeclampsia can lead to eclampsia, a serious condition that can have health risks for mom and baby and, in rare cases, cause death. If your preeclampsia leads to seizures, you have eclampsia.
The only cure for preeclampsia is to give birth. Even after delivery, symptoms of preeclampsia can last 6 weeks or more.
You can help protect yourself by learning the symptoms of preeclampsia and by seeing your doctor for regular prenatal care. Catching preeclampsia early may lower the chances of long-term problems for both mom and baby.
Preeclampsia Symptoms
In addition to swelling (also called edema), protein in the urine, and blood pressure over 140/90, preeclampsia symptoms include:
- Weight gain over 1 or 2 days because of a large increase in bodily fluid
- Shoulder pain
- Belly pain, especially in the upper right side
- Severe headaches
- Change in reflexes or mental state
- Peeing less or not at all
- Dizziness
- Trouble breathing
- Severe vomiting and nausea
- Vision changes like flashing lights, floaters, or blurry vision
Some women with preeclampsia don’t have any symptoms, so it’s important to see your doctor for regular blood pressure checks and urine tests.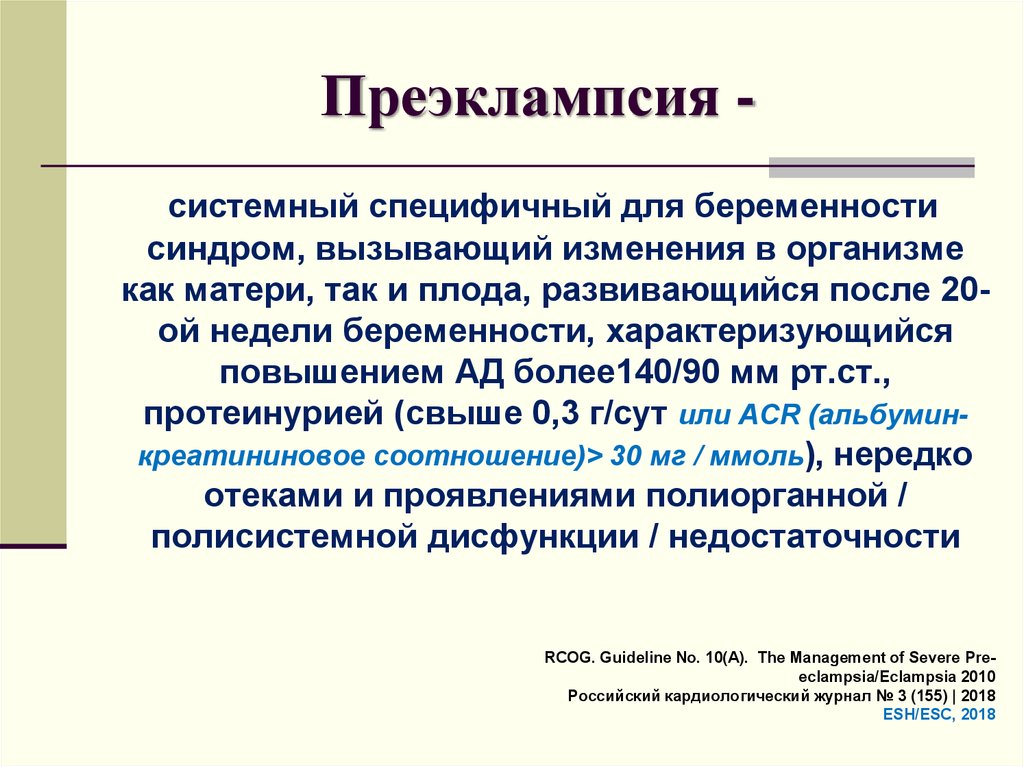
When Do Symptoms Show Up?
Preeclampsia can happen as early as 20 weeks into pregnancy, but that’s rare. Symptoms often begin after 34 weeks. In a few cases, symptoms develop after birth, usually within 48 hours of delivery. They tend to go away on their own.
Preeclampsia Causes
Many experts think preeclampsia and eclampsia happen when a woman’s placenta doesn’t work the way it should, but they don’t know exactly why. Some think poor nutrition or high body fat might contribute. A lack of blood flow to the uterus could play a role. Genes are also a factor.
Other High Blood Pressure Disorders in Pregnancy
Preeclampsia is one of four blood pressure disorders in pregnant women. The other three are:
- Gestational hypertension. This is high blood pressure that starts after the 20th week of pregnancy but doesn’t cause high amounts of protein in a woman’s urine. It usually goes away after delivery.
- Chronic hypertension.
 This is high blood pressure that starts before a woman gets pregnant or before the 20th week of pregnancy.
This is high blood pressure that starts before a woman gets pregnant or before the 20th week of pregnancy. - Chronic hypertension with superimposed preeclampsia. This is chronic high blood pressure that gets worse as pregnancy goes on, causing more protein in urine and other complications.
Preeclampsia Risk Factors
Things that can increase your chance of getting preeclampsia include:
- Being a teen or woman over 40
- Being African American
- Being pregnant for the first time
- Having babies less than 2 years apart or more than 10 years apart
- Pregnancy with a new partner instead of the father of your previous children
- High blood pressure before getting pregnant
- A history of preeclampsia
- A mother or sister who had preeclampsia
- A history of obesity
- Carrying more than one baby
- In-vitro fertilization
- A history of diabetes, kidney disease, lupus, or rheumatoid arthritis
Preeclampsia Complications
Preeclampsia can keep your placenta from getting enough blood, which can cause your baby to be born very small. This is called fetal growth restriction.
This is called fetal growth restriction.
It’s also one of the most common causes of premature births and the complications that can follow, including learning disabilities, epilepsy, cerebral palsy, and hearing and vision problems.
Preeclampsia can cause rare but serious complications that include:
- Stroke
- Seizure
- Fluid buildup in your chest
- Heart failure
- Reversible blindness
- Bleeding from your liver
- Bleeding after you've given birth
When preeclampsia or eclampsia damages your liver and blood cells, you can get a complication called HELLP syndrome. That stands for:
- Hemolysis. This is when the red blood cells that carry oxygen through your body break down.
- Elevated liver enzymes. High levels of these chemicals in your blood mean liver problems.
- Low platelet counts. This is when you don’t have enough platelets, so your blood doesn’t clot the way it should.

HELLP syndrome is a medical emergency. Call 911 or go to the emergency room if you have symptoms including:
- Blurry vision
- Chest or belly pain
- Headache
- Fatigue
- Upset stomach or vomiting
- Swelling in your face or hands
- Bleeding from your gums or nose
Preeclampsia can also cause your placenta to suddenly separate from your uterus, which is called placental abruption. This can lead to stillbirth.
Preeclampsia Diagnosis
You have preeclampsia if you have high blood pressure and at least one of these other signs:
- Too much protein in your urine
- Not enough platelets in your blood
- High levels of kidney-related chemicals in your blood
- High levels of liver-related chemicals in your blood
- Fluid in your lungs
- A new headache that doesn’t go away when you take medication
To confirm a diagnosis, your doctor might give you tests including:
- Blood tests to check your platelets and to look for kidney or liver chemicals
- Urine tests to measure proteins
- Ultrasounds, nonstress tests, or biophysical profiles to see how your baby is growing
Preeclampsia Treatment
The only cure for preeclampsia and eclampsia is to give birth.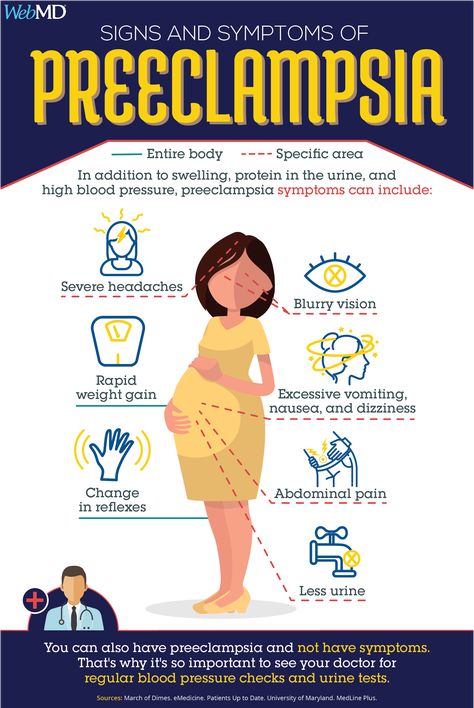 Your doctor will talk with you about when to deliver based on how far along your baby is, how well your baby is doing in your womb, and the severity of your preeclampsia.
Your doctor will talk with you about when to deliver based on how far along your baby is, how well your baby is doing in your womb, and the severity of your preeclampsia.
If your baby has developed well, usually by 37 weeks or later, your doctor may want to induce labor or do a cesarean section. This will keep preeclampsia from getting worse.
If your baby isn’t close to term, you and your doctor may be able to treat mild preeclampsia until your baby has developed enough to be safely delivered. The closer the birth is to your due date, the better it is for your baby.
If you have mild preeclampsia, also known as preeclampsia without severe features, your doctor may prescribe:
- Bed rest, either at home or in the hospital; resting mostly on your left side
- Careful monitoring with a fetal heart rate monitor and frequent ultrasounds
- Medicines to lower your blood pressure
- Blood and urine tests
Your doctor also may tell you to stay in the hospital so they can watch you closely.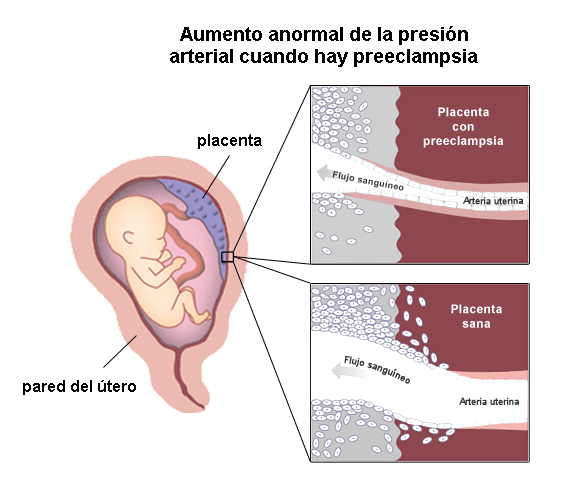 In the hospital, you might get:
In the hospital, you might get:
- Medicine to help prevent seizures, lower your blood pressure, and prevent other problems
- Steroid injections to help your baby's lungs develop faster
Other treatments include:
- Injections of magnesium to prevent eclampsia-related seizures
- Hydralazine or another blood pressure drug
For severe preeclampsia, your doctor may need to deliver your baby right away, even if you're not close to term. Afterward, symptoms of preeclampsia should go away within 1 to 6 weeks but could last longer.
Preeclampsia Prevention
If you have a greater chance of getting preeclampsia, talk to your doctor about making lifestyle changes that can help keep you healthy. You might need to:
- Lose some weight if you’re overweight
- Stop smoking
- Exercise regularly
- Get your blood pressure or blood sugar under control
Your doctor might also tell you to take a low-dose (81 milligram) aspirin each day./3/4.jpg) But don’t take any medications, vitamins, or supplements without talking to them first.
But don’t take any medications, vitamins, or supplements without talking to them first.
Symptoms, Causes, Treatments & Prevention
Overview
What is preeclampsia?
Preeclampsia is a serious blood pressure condition that develops during pregnancy. People with preeclampsia often have high blood pressure (hypertension) and high levels of protein in their urine (proteinuria). Preeclampsia typically develops after the 20th week of pregnancy. It can also affect other organs in the body and be dangerous for both the mom and her developing fetus. Because of these risks, preeclampsia needs to be treated by a healthcare provider.
What happens when you have preeclampsia?
When you have preeclampsia, your blood pressure is elevated (higher than 140/90 mmHg), and you may have high levels of protein in your urine. Preeclampsia puts stress on your heart and other organs and can cause serious complications. It can also affect the blood supply to your placenta, impair liver and kidney function or cause fluid to build up in your lungs. The protein in your urine is a sign of kidney dysfunction.
The protein in your urine is a sign of kidney dysfunction.
How common is preeclampsia?
Preeclampsia is a condition unique to pregnancy that complicates up to 8% of all deliveries worldwide. In the United States, it's the cause of about 15% of premature deliveries (delivery before 37 weeks of pregnancy).
Who gets preeclampsia?
Preeclampsia may be more common in first-time mothers. Healthcare providers are not entirely sure why some people develop preeclampsia. Some factors that may put you at a higher risk are:
- History of high blood pressure, kidney disease or diabetes.
- Expecting multiples.
- Family history of preeclampsia.
- Autoimmune conditions like lupus.
- Obesity.
Symptoms and Causes
What are the symptoms?
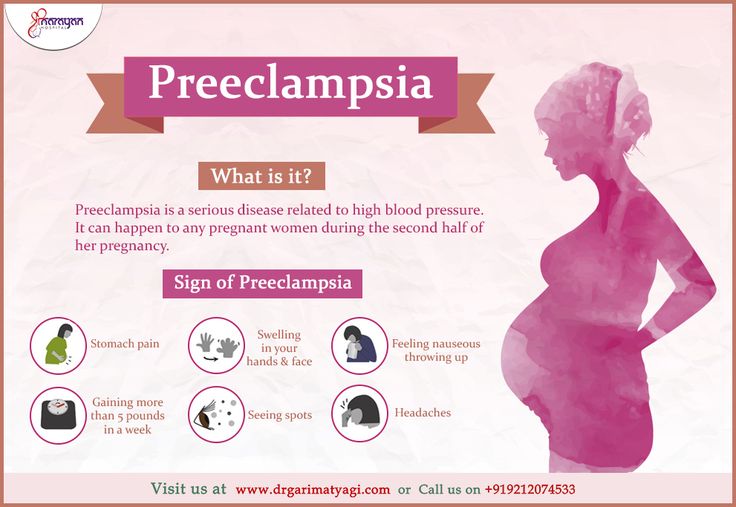
Many people with preeclampsia do not have any symptoms. For those that do, some of the first signs of preeclampsia are high blood pressure, protein in the urine and retaining water (this can cause weight gain and swelling).
Other signs of preeclampsia include:
- Headaches.
- Blurry vision or light sensitivity.
- Dark spots appearing in your vision.
- Right side abdominal pain.
- Swelling in your hands and face (edema).
- Shortness of breath.
It's essential to share all of your pregnancy symptoms with your healthcare provider. Many people are unaware they have preeclampsia until their blood pressure and urine are checked at a prenatal appointment.
Severe preeclampsia may include symptoms like:
- Hypertensive emergency (blood pressure is 160/110 mmHg or higher).
- Decreased kidney or liver function.
- Fluid in the lungs.
- Low blood platelet levels (thrombocytopenia).
- Decreased urine production
If your preeclampsia is severe, you may be admitted to the hospital for closer observation or need to deliver your baby as soon as possible. Your healthcare provider may give you medications for high blood pressure or to help the fetus's lungs develop before delivery.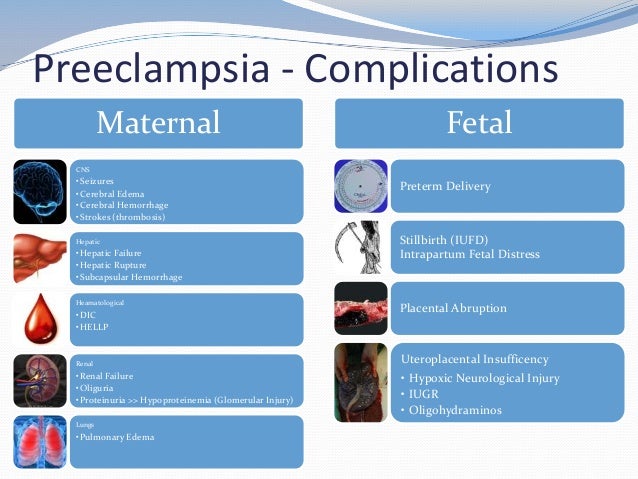
What causes preeclampsia?
No one is entirely sure. Preeclampsia is believed to come from a problem with the health of the placenta (the organ that develops in the uterus during pregnancy and is responsible for providing oxygen and nutrients to the fetus). The blood supply to the placenta might be decreased in preeclampsia, and this can lead to problems with both you and the fetus.
Does stress cause preeclampsia?
While stress may impact blood pressure, stress is not one of the direct causes of preeclampsia. While some stress is unavoidable during pregnancy, avoiding high-stress situations or learning to manage your stress is a good idea.
What week of pregnancy does preeclampsia start?
Preeclampsia typically occurs after 20 weeks of pregnancy, but it can come earlier. Most preeclampsia occurs at or near term (37 weeks gestation). Preeclampsia can also come after delivery (postpartum preeclampsia), which usually occurs between the first few days to one week after delivery.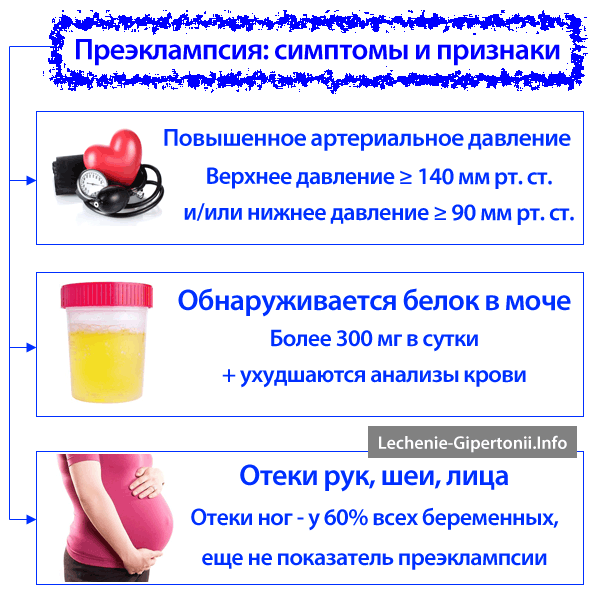 In rare cases, it begins weeks after delivery.
In rare cases, it begins weeks after delivery.
Will preeclampsia affect my baby?
Preeclampsia can cause preterm delivery (your baby needing delivered early). Premature babies are at increased risk for health complications like low birth weight and respiratory issues.
Diagnosis and Tests
How is it diagnosed?
Preeclampsia is often diagnosed during routine prenatal appointments when your healthcare provider checks your weight gain, blood pressure and urine.
If preeclampsia is suspected, your healthcare provider may:
- Order additional blood tests to check kidney and liver functions.
- Suggest a 24-hour urine collection to watch for proteinuria.
- Perform an ultrasound and other fetal monitoring to look at the size of the fetus and assess the amniotic fluid volume.
Preeclampsia can be categorized as mild or severe. You may be diagnosed with mild preeclampsia if you have high blood pressure plus high levels of protein in your urine.
You are diagnosed with severe preeclampsia if you have symptoms of mild preeclampsia plus:
- Signs of kidney or liver damage (seen in blood work).
- Low platelet count
- Fluid in your lungs.
- Headaches and dizziness.
- Visual impairment or seeing spots.
Management and Treatment
How is preeclampsia treated?
Your healthcare provider will advise you on the best way to treat preeclampsia. Treatment generally depends on how severe your preeclampsia is and how far along you are in pregnancy.
If you're close to full term (37 weeks pregnant or greater), your baby will probably be delivered early. You can still have a vaginal delivery, but sometimes a Cesarean delivery (C-section) is recommended. Your healthcare provider may give you medication to help the fetus's lungs develop and manage your blood pressure until the baby can be delivered. Sometimes it is safer to deliver the baby early than to risk prolonging the pregnancy.
When preeclampsia develops earlier in pregnancy, you'll be monitored closely in an effort to prolong the pregnancy and allow for the fetus to grow and develop. You'll have more prenatal appointments, including ultrasounds, urine tests and blood draws. You may be asked to check your blood pressure at home. If you are diagnosed with severe preeclampsia, you could remain in the hospital until you deliver your baby.
If the preeclampsia worsens or becomes more severe, your baby will need to be delivered.
During labor and following delivery, people with preeclampsia are often given magnesium intravenously (directly into the vein) to prevent the development of eclampsia (seizures from preeclampsia).
Is there a cure for preeclampsia?
No, there isn't a cure for preeclampsia. Preeclampsia can only be cured with delivery. Your healthcare provider will still want to monitor you for several weeks after delivery to make sure your symptoms go away.
Prevention
How can I reduce my risk of getting preeclampsia?
For people with risk factors, there are some steps that can be taken prior to and during pregnancy to lower the chance of developing preeclampsia.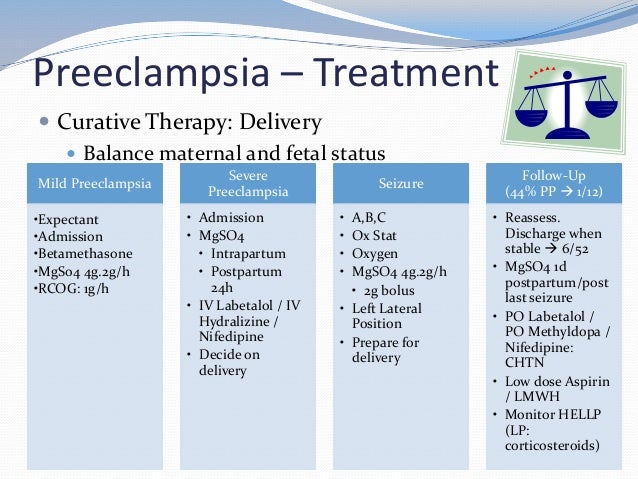 These steps can include:
These steps can include:
- Losing weight if you have overweight/obesity (prior to pregnancy-related weight gain).
- Controlling your blood pressure and blood sugar (if you had high blood pressure or diabetes prior to pregnancy).
- Maintaining a regular exercise routine.
- Getting enough sleep.
- Eating healthy foods that are low in salt and avoiding caffeine.
Can you prevent preeclampsia?
Taking a baby aspirin daily has been demonstrated to decrease your risk of developing preeclampsia by approximately 15%. If you have risk factors for preeclampsia, your healthcare provider may recommend starting aspirin in early pregnancy (by 12 weeks gestation).
Outlook / Prognosis
What are the most common complications of preeclampsia?
If left untreated, preeclampsia can be potentially fatal to both you and the fetus.
Before delivery, the most common complications are preterm birth, low birth weight or placental abruption.
Preeclampsia can cause HELLP syndrome (hemolysis, elevated liver enzymes and low platelet count). This happens when preeclampsia damages your liver and red blood cells and interferes with blood clotting. Other signs of HELLP syndrome are blurry vision, chest pain, headaches and nosebleeds.
After you've delivered your baby, you may be at an increased risk for:
- Kidney disease.
- Heart attack.
- Stroke.
- Developing preeclampsia in future pregnancies.
Does preeclampsia go away after delivery?
Preeclampsia typically goes away within days to weeks following delivery. Sometimes, your blood pressure can remain high for a few weeks after delivery, requiring treatment with medication. Your healthcare provider will work with you after your pregnancy to manage your blood pressure. People with preeclampsia — particularly those who develop the condition early in pregnancy — are at greater risk for high blood pressure (hypertension) and heart disease later in life.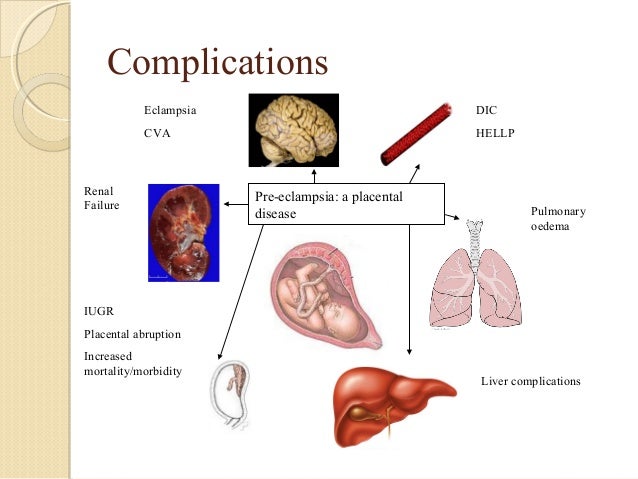 Knowing this information, those individuals can work with their primary care provider to take steps to reduce these risks.
Knowing this information, those individuals can work with their primary care provider to take steps to reduce these risks.
Living With
When should I see my healthcare provider?
Preeclampsia can be a fatal condition during pregnancy. If you're being treated for this condition, make sure to see your healthcare provider for all of your appointments and blood or urine tests. Contact your obstetrician if you have any concerns or questions about your symptoms.
Go to the nearest hospital if you're pregnant and experience the following:
- Symptoms of a seizure-like twitching or convulsing.
- Shortness of breath.
- Sharp pain in your abdomen (specifically the right side).
- Blurry vision.
- Severe headache that won't go away.
- Dark spots in your vision that don't go away.
What questions should I ask my doctor?
If your healthcare provider has diagnosed you with preeclampsia, it's normal to have concerns.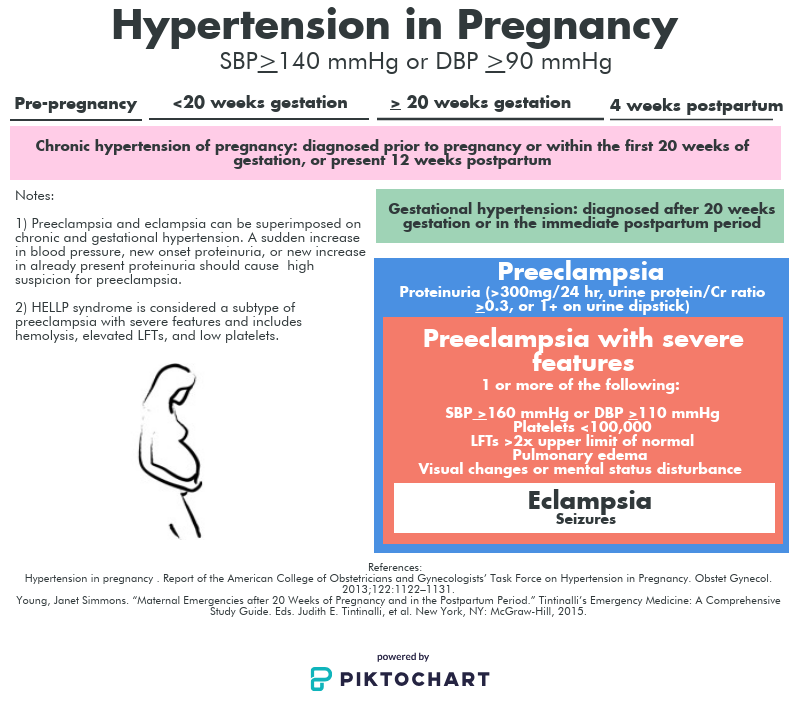 Some common questions to ask your healthcare provider are:
Some common questions to ask your healthcare provider are:
- Do I need to take medication?
- Do I need to restrict my activities?
- What changes should I make to my diet?
- How often will you need to monitor my health during pregnancy?
- Will I need to deliver my baby early?
- How can I best manage preeclampsia?
Frequently Asked Questions
What's the difference between preeclampsia and eclampsia?
Eclampsia is severe preeclampsia that causes seizures. It's considered a complication of preeclampsia, but it can happen without signs of preeclampsia. In rare cases, it can lead to coma, stroke or death.
What is postpartum preeclampsia?
Postpartum preeclampsia is when you develop preeclampsia after your baby is born. It typically happens within two days of giving birth but can also develop several weeks later. The signs of postpartum preeclampsia are similar to preeclampsia and include swelling in your limbs and extremities, headaches, seeing spots, stomach pains and nausea. It's a serious condition that can cause seizures, stroke and organ damage.
It's a serious condition that can cause seizures, stroke and organ damage.
A note from Cleveland Clinic
Preeclampsia is a serious condition that you may not be aware you even have. It's important to go to all your prenatal appointments and be open about all the symptoms you feel during pregnancy. When preeclampsia is caught early, it can be treated and managed to keep both you and the fetus safe and healthy. Most people with preeclampsia go on to have healthy babies.
preeclampsia
Every mother-to-be wants her pregnancy to be a time of joyful anticipation. But the fear of preeclampsia can darken the joy.
What is preeclampsia?
Pre-eclampsia is a potentially life-threatening disease that occurs during pregnancy and affects multiple organ systems and is characterized by high maternal blood pressure and protein in the urine, or in the absence of the latter, dysfunction of other organ systems.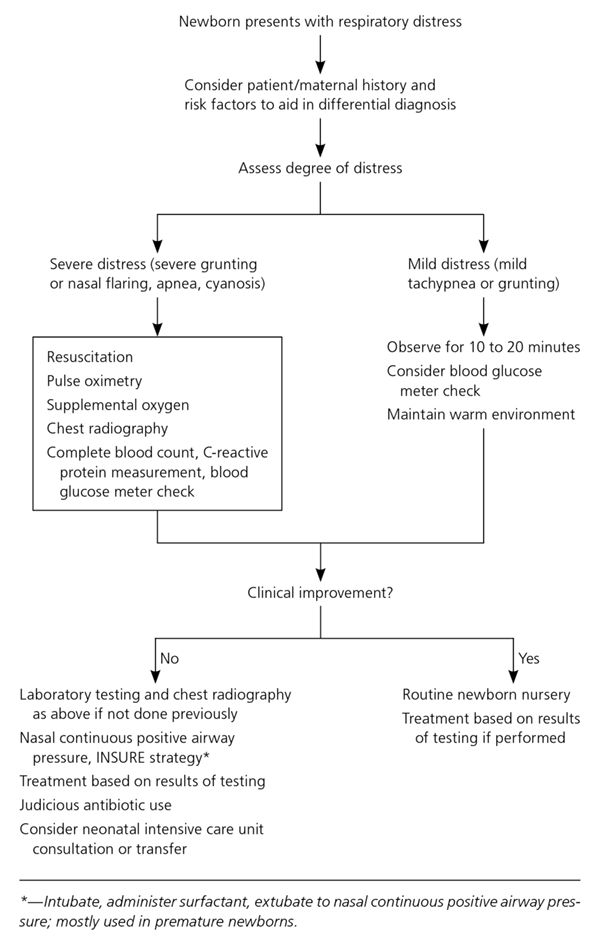 This can affect both you and your unborn child. If the risk of preeclampsia is known in advance, it can be prevented. nine0003
This can affect both you and your unborn child. If the risk of preeclampsia is known in advance, it can be prevented. nine0003
How common is preeclampsia?
Most women have a normal pregnancy. At the same time, pre-eclampsia is a relatively common disease during pregnancy, which occurs in two out of a hundred women in Estonia.
When does preeclampsia occur?
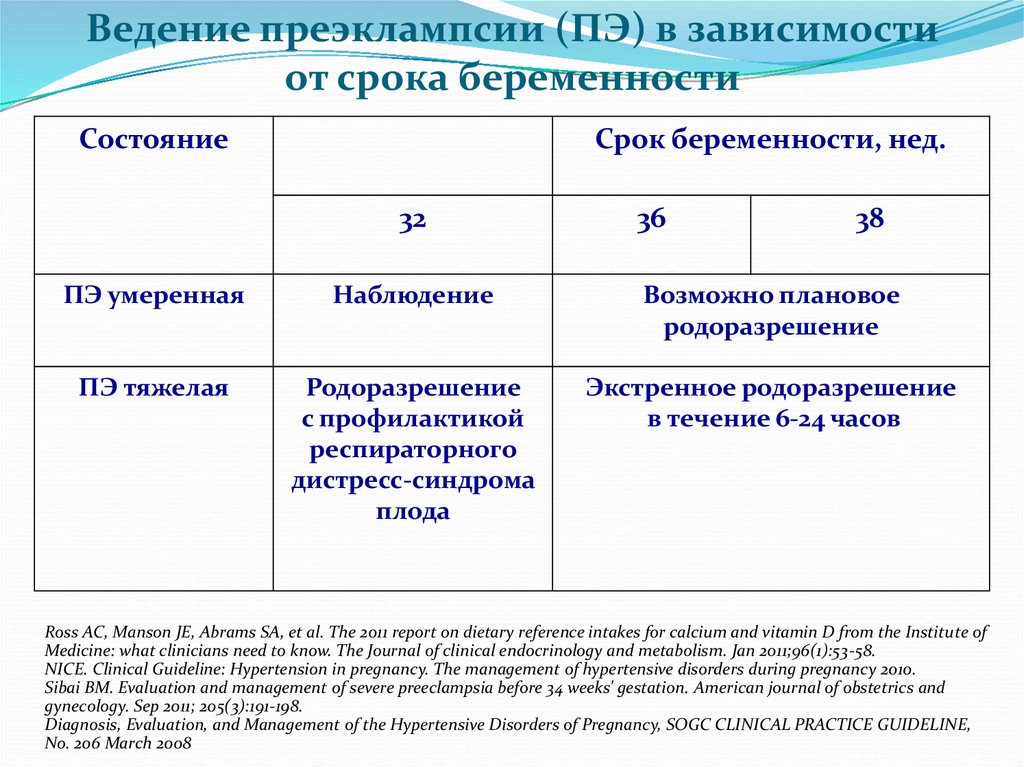
Pre-eclampsia occurs after the 20th week of pregnancy or up to six weeks after delivery. Most often, preeclampsia occurs between the 32nd and 36th weeks of pregnancy. The earlier in pregnancy the disease occurs, the more severe its course, and the more dangerous it is for the mother and child. nine0003
What causes preeclampsia?
The exact causes of preeclampsia are unknown, but it is believed that they lie in the violation of the attachment of the developing placenta to the uterus, as a result of which there is no reliable connection between the circulatory systems of the mother and child. At the same time, a rapidly developing fetus requires oxygen and nutrients from the mother's circulatory system for its growth. If oxygen deficiency occurs in the developing placenta, toxic substances are released into the mother's circulatory system, which damage the lining of the mother's blood vessels. This is how a systemic lesion of the internal organs of the mother is formed. In order to save the lives of mother and child, the child must be born. If this happens at a very early stage of pregnancy, the baby is not yet ready for extrauterine life. nine0003
At the same time, a rapidly developing fetus requires oxygen and nutrients from the mother's circulatory system for its growth. If oxygen deficiency occurs in the developing placenta, toxic substances are released into the mother's circulatory system, which damage the lining of the mother's blood vessels. This is how a systemic lesion of the internal organs of the mother is formed. In order to save the lives of mother and child, the child must be born. If this happens at a very early stage of pregnancy, the baby is not yet ready for extrauterine life. nine0003
How will this affect me?
Mostly there is a mild form of the disease that occurs at the end of pregnancy and the prognosis for which is good. But sometimes pre-eclampsia can get worse very quickly and begin to threaten the lives of the mother and child. Preeclampsia also has a long-term effect on a woman's health, as it doubles the incidence of cardiovascular disease in the future.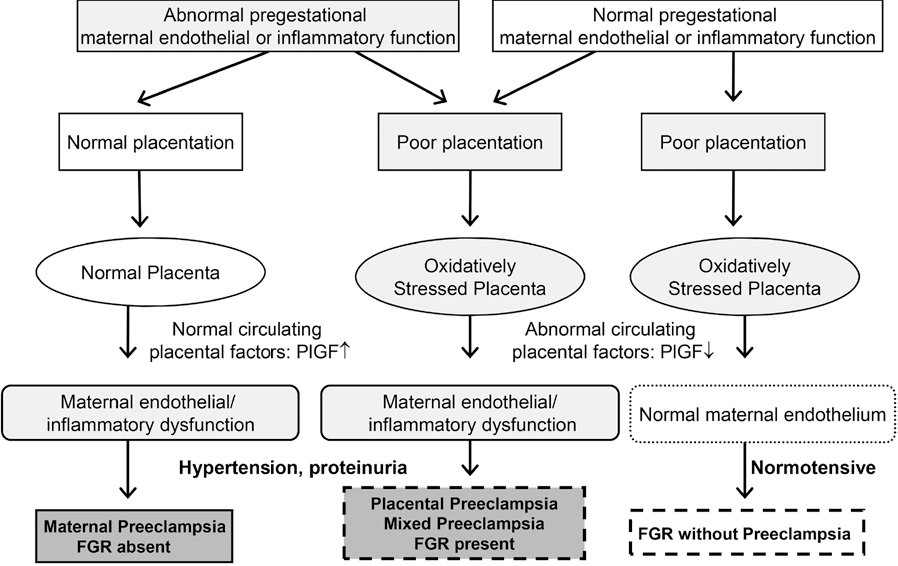 Most women with preeclampsia are hospitalized, and often their children have to be born prematurely. If the health of the mother or child is at risk, labor is induced or a caesarean section is performed. nine0003
Most women with preeclampsia are hospitalized, and often their children have to be born prematurely. If the health of the mother or child is at risk, labor is induced or a caesarean section is performed. nine0003
How will this affect my child?
Most children remain healthy even when their mothers have severe preeclampsia. But sometimes preeclampsia can threaten the life and health of both the fetus and the newborn. Maternal preeclampsia doubles the risk of a surviving child suffering from cerebral palsy, that is, brain damage that results in delayed physical and sometimes mental development. In addition, surviving children are more likely to develop cardiovascular disease, obesity and diabetes in the future. In preeclampsia, there is not enough oxygen and nutrients for the growth of the fetus, and intrauterine growth retardation occurs. Since the only treatment for preeclampsia is childbirth, sometimes the pregnancy has to be terminated. Until the 34th week of pregnancy, the lungs of the fetus have not yet fully developed, and steroid injections are given to the pregnant woman to stimulate them. nine0003
Until the 34th week of pregnancy, the lungs of the fetus have not yet fully developed, and steroid injections are given to the pregnant woman to stimulate them. nine0003
How to recognize preeclampsia?
Unfortunately, in most women, the symptoms of the disease appear only at an advanced stage.
- Chronic headache not responding to painkillers
- Severe nausea and vomiting
- Visual disturbances, tinnitus
- Pain in the right hypochondrium
- Feeling short of breath, shortness of breath
- Infrequent urge to urinate (less than 500 ml per day)
- Edema of hands, face and eyelids
- Rapid weight gain (more than 1 kg per week)
If you experience any of the above symptoms, contact your obstetrician, gynecologist or hospital doctor on call.
Am I at risk?
Although all pregnant women can develop preeclampsia, some women are more at risk than others.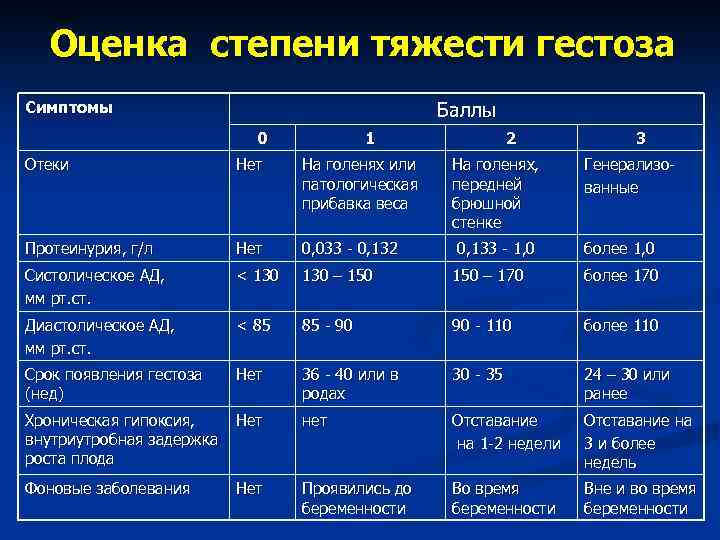
You are more at risk if
- this is your first pregnancy;
- you had preeclampsia during a previous pregnancy;
- your sister or mother had preeclampsia;
- Your body mass index is 35 kg/m 2 or more;
- You are at least 40 years old;
- the time between births was more than 10 years;
- You are expecting twins;
- You have become pregnant in vitro; nine0084
- you have any medical problem, such as hypertension, kidney problems, lupus, diabetes;
- You developed diabetes during this pregnancy.
At what stage of pregnancy is screening performed?
Pre-eclampsia screening can be performed in all three trimesters.
- First trimester, 11–13 weeks +6 weeks (as part of the OSCAR test)
- Second trimester, 19-21 weeks +6 weeks (as part of fetal anatomy screening)
- Third trimester, 34-36 weeks (as part of fetal growth and condition study)
A three-stage screening test for preeclampsia can prevent it from occurring or move it to a later stage of pregnancy.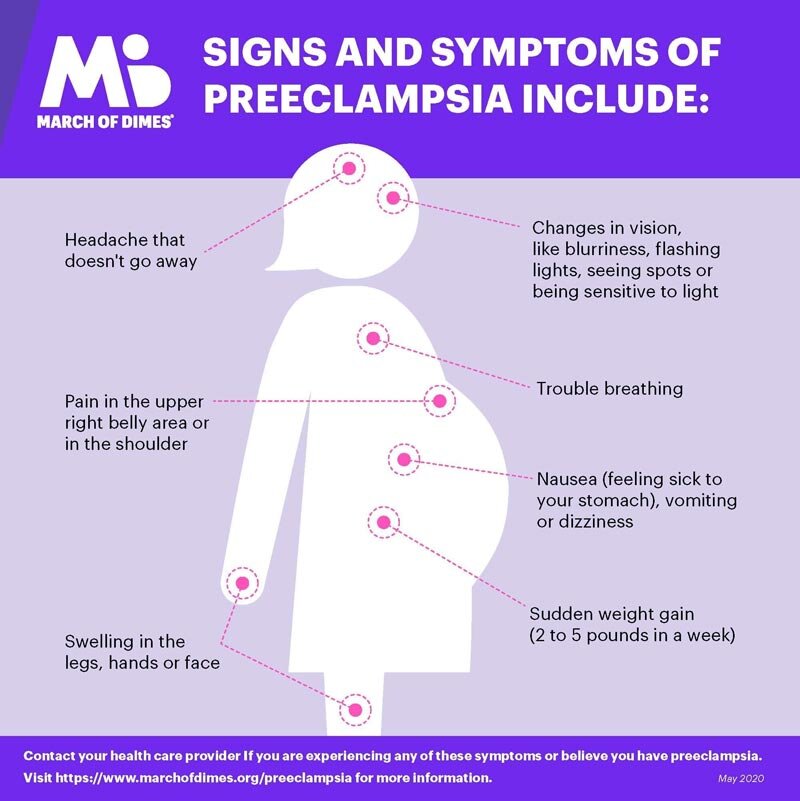
How reliable is screening for preeclampsia? nine0016
In the first trimester, the OSCAR test can identify women at risk of developing early preeclampsia with 76% accuracy before the 37th week of pregnancy. Among pregnant twins, all women who can develop early preeclampsia can be identified before the 37th week of pregnancy.
In the second trimester, fetal anatomy screening can identify women at risk of developing early preeclampsia with an accuracy of 85% before the 37th week of pregnancy. nine0003
In the third trimester, growth and fetal ultrasound can detect with 85% accuracy women at risk for developing late preeclampsia after 37 weeks of pregnancy.
Why should I assess my risk for preeclampsia?
The best way to assess the risk of early preeclampsia is in the first trimester with the OSCAR test, when at-risk women will benefit from the anti-preeclampsia effect of aspirin. Studies have shown that small doses of aspirin before the 16th week of pregnancy in 62% of cases reduce the risk of early preeclampsia, which may require delivery before the 37th week. Therefore, women with an increased risk of preeclampsia are advised to take 150 milligrams of aspirin once a day, in the evenings, until the 36th week of pregnancy. The goal of prophylactic treatment for women at high risk of preeclampsia is either to avoid the development of preeclampsia or to postpone its occurrence until later in pregnancy, when the child is ready for birth. nine0003
Studies have shown that small doses of aspirin before the 16th week of pregnancy in 62% of cases reduce the risk of early preeclampsia, which may require delivery before the 37th week. Therefore, women with an increased risk of preeclampsia are advised to take 150 milligrams of aspirin once a day, in the evenings, until the 36th week of pregnancy. The goal of prophylactic treatment for women at high risk of preeclampsia is either to avoid the development of preeclampsia or to postpone its occurrence until later in pregnancy, when the child is ready for birth. nine0003
In the second trimester, fetal anatomy screening may reassess the risk of preeclampsia obtained from OSCAR or recommend screening for preeclampsia in women who were not assessed for risk by OSCAR.
In the third trimester, ultrasound examination of the growth and condition of the fetus can assess the risk of late preeclampsia. This is very important as 75% of preeclampsia cases develop after the 37th week of pregnancy.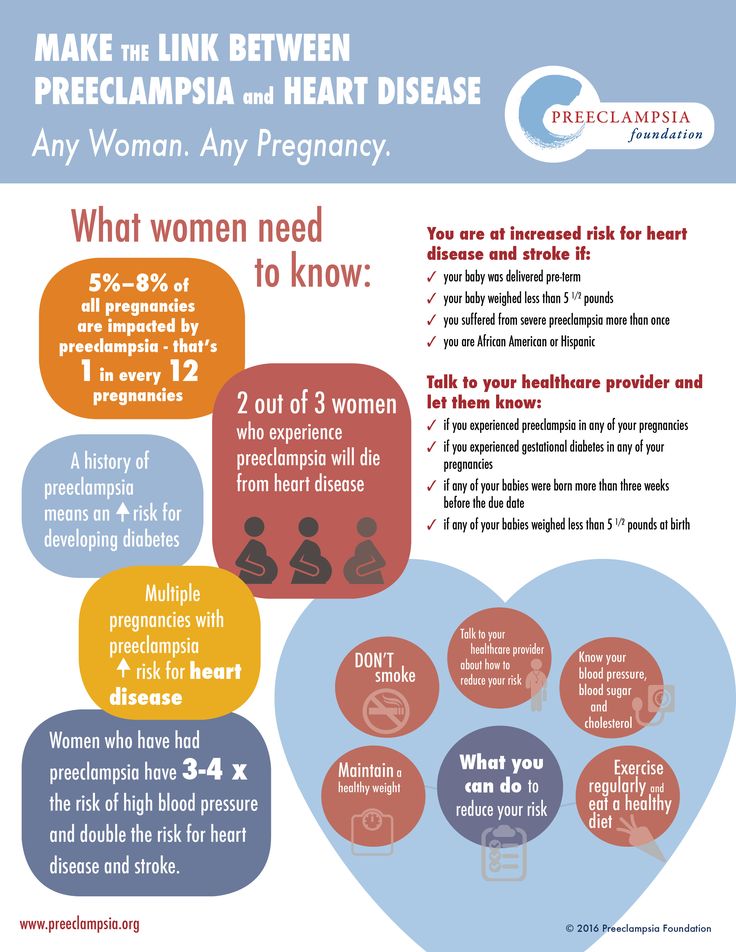 This makes it possible to more intensively examine women with an increased risk of preeclampsia and to detect the disease in a timely manner, as well as to prepare the baby's lungs for an early birth. nine0003
This makes it possible to more intensively examine women with an increased risk of preeclampsia and to detect the disease in a timely manner, as well as to prepare the baby's lungs for an early birth. nine0003
How is preeclampsia screened?
Screening for pre-eclampsia consists of an appointment with a nurse and an ultrasound examination by a gynecologist. The nurse interviews the pregnant woman, measuring her blood pressure, height and weight, and doing a blood test. The gynecologist performs an ultrasound examination and measures the blood flow indices of the uterine arteries feeding the placenta. Based on the blood test values of hormone levels and associated risk factors for preeclampsia, blood pressure parameters, body mass index and uterine arterial blood flow indices, the gynecologist uses a special computer program to assess the individual risk of early or late preeclampsia. nine0003
- The risk of preeclampsia can be assessed in one day.
- The risk of preeclampsia can also be assessed for women who are expecting twins.
Preeclampsia screening makes you feel safe
Most of the women who participate in preeclampsia screening are at low risk. At increased risk, a three-stage screening test for preeclampsia provides an opportunity, if necessary, to prevent its occurrence or shift it to a later stage of pregnancy. Reducing the risk of pre-eclampsia and careful, evidence-based monitoring of your health and that of your baby gives you the much-needed sense of security. So the child will be able to safely be born when he is ready for this, and you will enjoy a healthy child. nine0003
Read more:
- Pre-eclampsia screening at 11-14 weeks of gestation
- Pre-eclampsia screening at 19-22 weeks of gestation
- Screening for pre-eclampsia at 35-37 weeks of gestation
- Preeclampsia Screening Information Sheet
- Preeclampsia Risk Calculator
Preeclampsia and pregnancy | Ida-Tallinna Keskhaigla
The purpose of this leaflet is to provide the patient with information about the nature, occurrence, risk factors, symptoms and treatment of preeclampsia.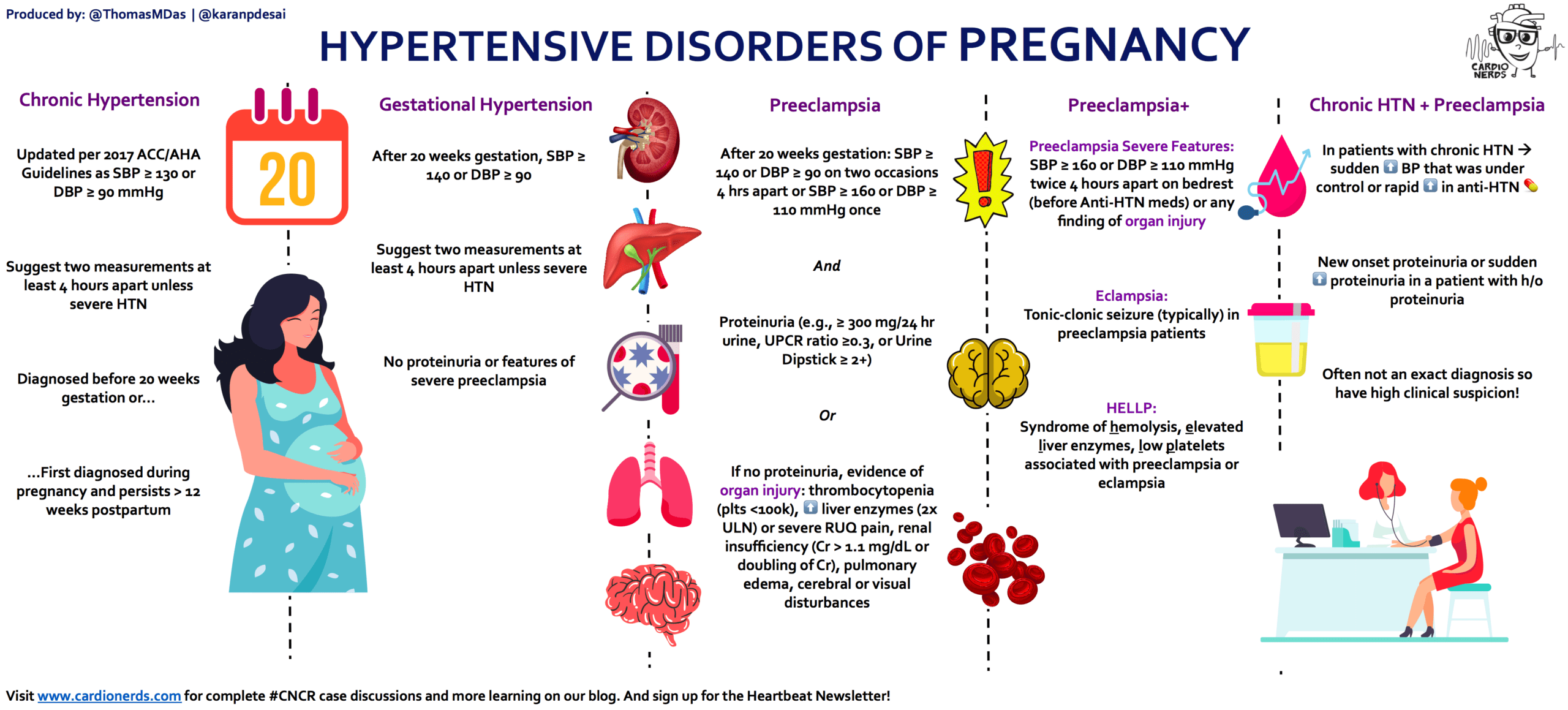 nine0003
nine0003
What is preeclampsia?
Pre-eclampsia is a disease that occurs during pregnancy and is characterized by high blood pressure and protein in the urine. Preeclampsia is one of the most common complications of pregnancy. Epilepsy-like seizures occur in severe preeclampsia and are life-threatening.
What symptoms may indicate the development of preeclampsia?
High blood pressure - Blood pressure values are 140/90 mm Hg. Art. or higher. If systolic (upper) or diastolic (lower) blood pressure rises by 30 mm Hg. Art. or more, then such an increase cannot be ignored.
Protein in urine - 300 mg in urine collected over 24 hours, or +1 value on a rapid test.
Swelling of the arms, legs or face , especially under the eyes, or if the swelling leaves a depression in the skin when pressed. Edema can occur in all pregnant women and is generally harmless, but rapidly developing edema should be taken into account. nine0003
Edema can occur in all pregnant women and is generally harmless, but rapidly developing edema should be taken into account. nine0003
Headache that does not improve after taking pain medication.
Visual disturbances - double vision or blurred vision, dots or flashes before the eyes, auras.
Nausea or upper abdominal pain - These symptoms are often mistaken for indigestion or gallbladder pain. Nausea in the second half of pregnancy is not normal.
Sudden weight gain - 2 kg or more per week. nine0003
As a rule, there is a mild course of the disease that occurs at the end of pregnancy and has a good prognosis. Sometimes, preeclampsia can worsen quickly and be dangerous to both mother and fetus. In such cases, rapid diagnosis and careful monitoring of the mother and child are of paramount importance.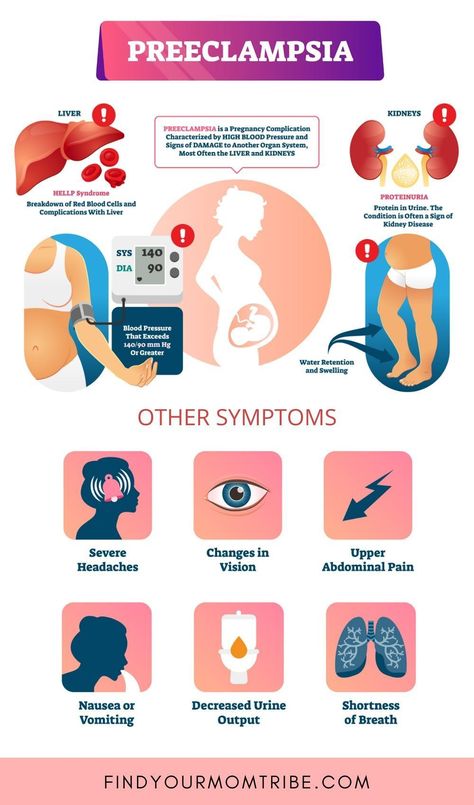
Unfortunately, most women show symptoms in the final stages of the disease. If you experience any of the above symptoms, you should contact your midwife, gynecologist, or the Women's Clinic emergency department. nine0003
Is preeclampsia called toxemia of pregnancy?
Previously, pre-eclampsia was indeed called toxicosis, or toxemia, since it was believed that the cause of the disease was toxins, that is, poisons in the blood of a pregnant woman.
What is the difference between preeclampsia and gestational hypertension?
Pregnancy hypertension is an increase in blood pressure above normal after the 20th week of pregnancy. With hypertension of pregnant women, protein in the urine is not observed. nine0003
What is HELLP syndrome?
HELLP syndrome is one of the most severe forms of preeclampsia.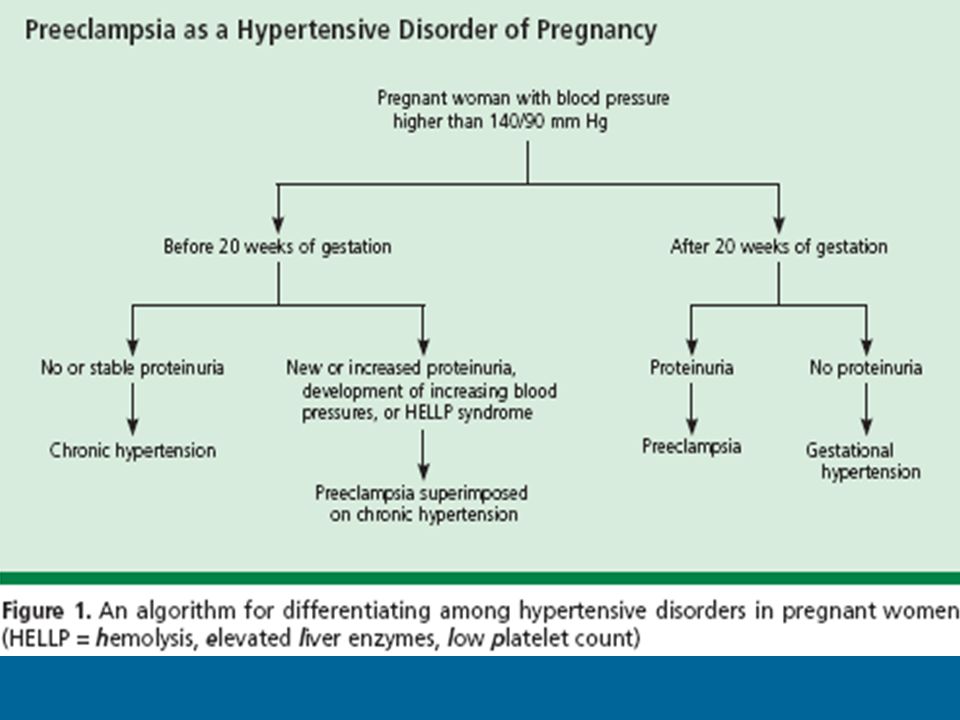 HELLP syndrome is rare and sometimes develops before symptoms of preeclampsia appear. Sometimes the syndrome is difficult to diagnose, as the symptoms resemble gallbladder colic or a cold.
HELLP syndrome is rare and sometimes develops before symptoms of preeclampsia appear. Sometimes the syndrome is difficult to diagnose, as the symptoms resemble gallbladder colic or a cold.
When does preeclampsia occur?
Preeclampsia usually occurs after the 20th week of pregnancy. As a rule, preeclampsia goes away after delivery, but complications can occur up to six weeks after delivery, during which careful monitoring of the condition is necessary. If by the sixth week after birth, blood pressure does not return to normal, then you need to contact a cardiologist, who will begin treatment against hypertension. nine0003
What is the cause of preeclampsia?
The causes of the disease are still not clear, there are only unproven hypotheses.
How does the disease affect pregnant women and pregnancy?
Most preeclamptic pregnancies have a favorable outcome and a healthy baby is born. However, the disease is very serious and is one of the most common causes of death of the child and mother. Preeclampsia affects a woman's kidneys, liver, and other vital organs, and if left untreated, it can cause seizures (eclampsia), cerebral hemorrhage, multiple organ failure, and death. nine0003
However, the disease is very serious and is one of the most common causes of death of the child and mother. Preeclampsia affects a woman's kidneys, liver, and other vital organs, and if left untreated, it can cause seizures (eclampsia), cerebral hemorrhage, multiple organ failure, and death. nine0003
How does the disease affect the fetus?
In preeclampsia, the fetus does not receive enough oxygen and nutrients to grow, and intrauterine growth retardation may occur. In addition, the placenta may separate from the uterine wall before the baby is born. Since the only treatment for preeclampsia is childbirth, sometimes a pregnancy has to be terminated prematurely. Until the 34th week of pregnancy, the lungs of the fetus have not yet matured, and steroid hormones are administered intravenously to the pregnant woman to prepare her lungs. In addition to the immaturity of the lungs, the health of a premature baby is threatened by many other diseases.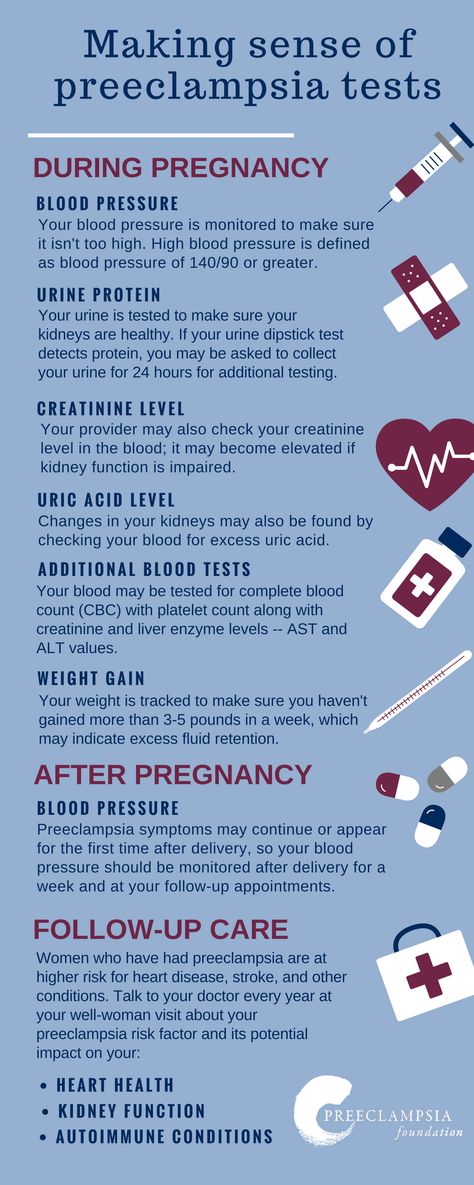 nine0003
nine0003
Who is at risk for preeclampsia?
Pre-eclampsia occurs in approximately 8% of pregnant women, many of whom have no known risk factors.
What are the risk factors for preeclampsia?
Patient-related risk factors
-
First pregnancy
-
Pre-eclampsia during a previous pregnancy
-
Age over 40 or under 18
-
High blood pressure before pregnancy
-
Diabetes before or during pregnancy
-
Multiple pregnancy
-
Overweight (BMI> 30)
-
Systemic lupus erythematosus or other autoimmune disease
-
Polycystic ovary syndrome
-
Long interval between two pregnancies
Risk factors associated with the patient's family
What is the prevention and treatment of preeclampsia
During the first trimester screening, or Oscar test, in addition to the most common chromosomal diseases, the risk of preeclampsia is also calculated.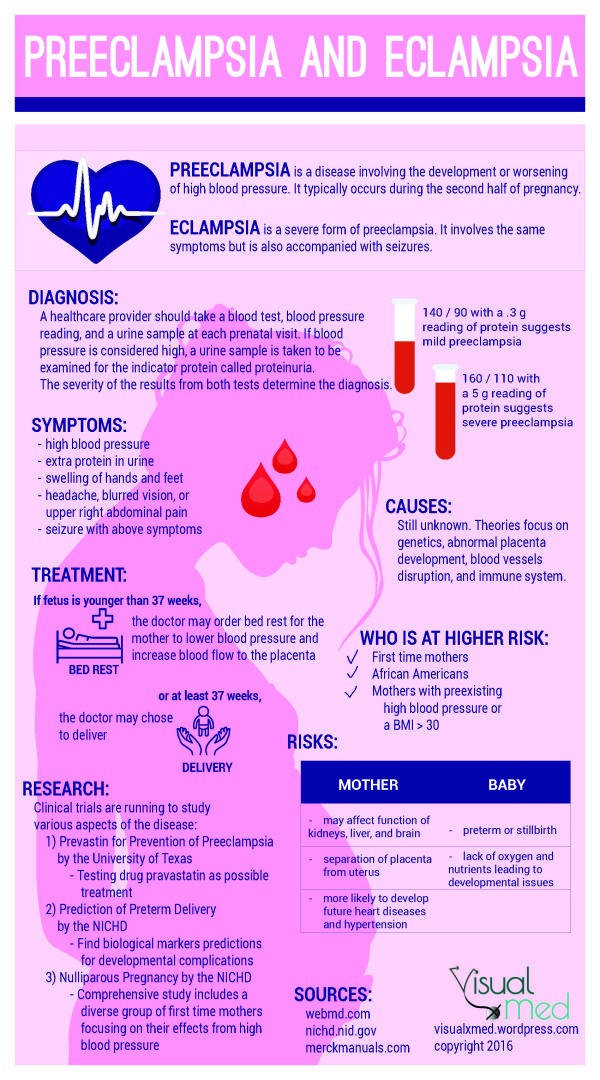 In case of high risk, pregnant women are advised to take aspirin (acetylsalicylic acid) at a dose of 150 mg in the evenings until the 36th week of pregnancy. This helps reduce the chance of preeclampsia by the 34th week of pregnancy by up to 80%. nine0003
In case of high risk, pregnant women are advised to take aspirin (acetylsalicylic acid) at a dose of 150 mg in the evenings until the 36th week of pregnancy. This helps reduce the chance of preeclampsia by the 34th week of pregnancy by up to 80%. nine0003
Childbirth is the only treatment for preeclampsia. Sometimes a child can be born naturally, but sometimes, if the disease is very acute, an emergency caesarean section is necessary. The best time to have a baby is after the 37th week of pregnancy. Bed rest, medications, and, if necessary, hospitalization can sometimes help bring the condition under control and prolong the pregnancy. Often, a doctor will refer a woman with preeclampsia to the hospital for observation, as the condition of the fetus and pregnant woman may suddenly worsen. nine0003
Does bed rest help?
Sometimes bed rest is enough to control mild preeclampsia.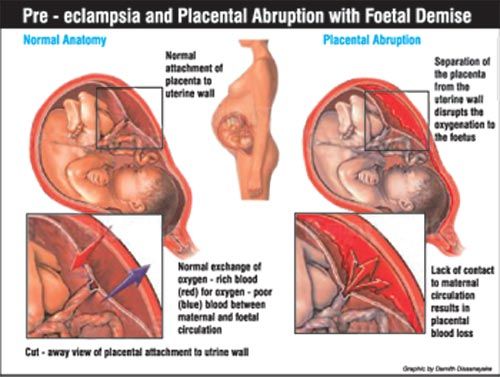 In this case, the patient often visits a doctor who measures blood pressure, does blood and urine tests, and monitors the course of the disease. The condition of the fetus is also often examined using a cardiotocogram (CTG) and ultrasound.
In this case, the patient often visits a doctor who measures blood pressure, does blood and urine tests, and monitors the course of the disease. The condition of the fetus is also often examined using a cardiotocogram (CTG) and ultrasound.
Are medications used to treat preeclampsia?
High blood pressure sometimes requires medication. The medications used have few side effects, the drugs prescribed do not have much effect on the fetus, but are very important in the treatment of maternal high blood pressure. nine0003
Seizures are a rare but very serious complication of preeclampsia. Magnesium sulfate is sometimes given intravenously to prevent seizures in a pregnant woman with preeclampsia both during and after childbirth. It is safe for the fetus, but the mother may experience side effects such as hot flashes, sweating, thirst, visual disturbances, mild confusion, muscle weakness, and shortness of breath.